By Dr Minh Alexander NHS whistleblower and former consultant psychiatrist 22 August 2019
Last year the Health and Social Care watchdog the Care Quality Commission acknowledged that it had still not got whistleblowing governance right.
It agreed to consult again by the end of the year. I advised that this should be an open process.
To give due credit, Ted Baker Chief Inspector of Hospitals also agreed to revisit a request for audit of CQC’s handling of whistleblower confidentiality, despite Peter Wyman CQC Chair having arbitrarily dismissed the need for audit, after breaches.
CQC board minutes subsequently showed that CQC reviewed a series of cases and concluded that there had been no recent confidentiality breaches.
However, the general consultation on whistleblowing did not materialise.
CQC board papers from July this year revealed that CQC pressed on with internal review of its whistleblowing process.
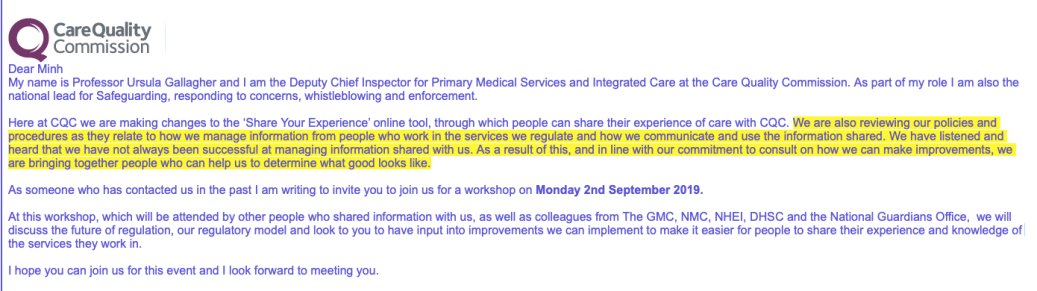
The CQC has now sent out, at short notice, invitations to a national event on 2 September 2019 which includes consultation on how its whistleblowing process might be improved:
“We are also reviewing our policies and procedures as they relate to how we manage information from people who work in the services we regulate and how we communicate and use the information shared. We have listened and heard that we have not always been successful at managing information shared with us. As a result of this, and in line with our commitment to consult on how we can make improvements, we are bringing together people who can help us to determine what good looks like.”
The Department of Health and Social Care, GMC, NMC, NHS England/ Improvement and the National Guardian will be represented.
Some whistleblowers have been invited, but I do not know how many in total.
There also does not appear to be clear open access to the consultation process by correspondence, and I am not aware that the consultation has been advertised.
There is no agenda for the 2 September workshop yet, but the event is scheduled for a five hour slot.
It is led by Professor Ursula Gallagher CQC Deputy Deputy Chief Inspector for Primary Medical Services and Integrated Care, who is the CQC lead on whistleblowing.
I have asked for sight of the policies about which the CQC is consulting. I am advised that these are the two relevant policies:
- Published 2013 guidance for providers on whistleblowing governance
Whistleblowing Guidance for providers who are registered with the Care Quality Commission
- Internal CQC guidance for its inspectors produced in June 2019, and currently in use
Guidance: Handling concerns raised by workers of providers registered with CQC
The 2019 internal guidance document replaces a document produced last year:
Handling concerns raised by workers of providers registered with CQC
Apart from a different title and a curious new section on RIPA powers, the 2019 CQC guidance for its inspectors looks much the same as the 2018 guidance.
|
The new section in 2019 CQC guidance on whistleblowing for its staff:
| 10. The Regulation of Investigatory Powers Act 2000 (RIPA) |
“CQC does not routinely as a matter of policy currently undertake or authorise providers or members of the public to undertake either directed covert surveillance or Covert Human Intelligence Sources (CHIS).
In addition, the Regulation of Investigatory Powers Act 2000 (RIPA) places restrictions upon the use of surveillance and covert intelligence sources by public bodies. Under RIPA, the Care Quality Commission does not have the power to undertake intrusive covert surveillance or to authorise providers or the public to undertake intrusive covert surveillance. This prohibits CQC from authorising the use of hidden cameras and listening devices in residential premises.
Therefore, CQC currently does not ask people to create recordings on its behalf. For further information about RIPA and covert activity including intrusive surveillance, directed surveillance or CHIS please visit the RIPA intranet page and RIPA awareness video in ED.” |
|
Inevitably, the CQC guidance to its staff toes the government line: UK whistleblowing law is protective, the National Guardian is leading culture change, blah blah blah…
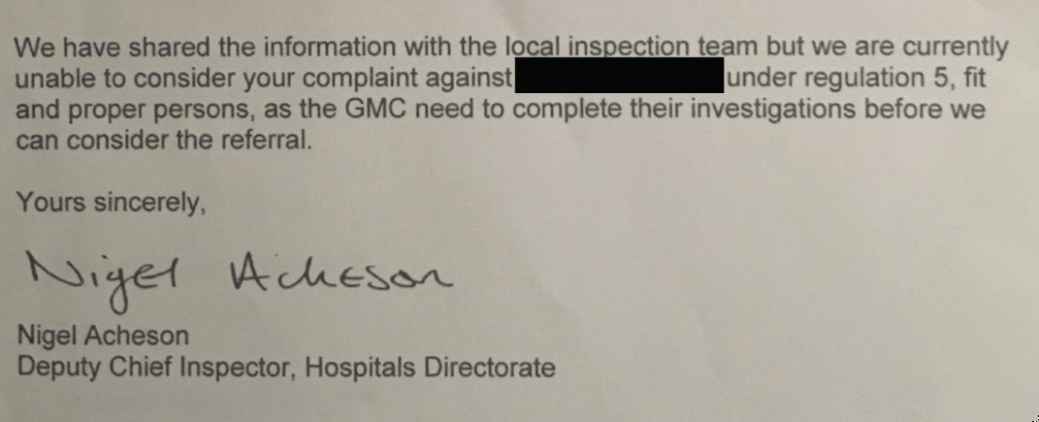
The key issue that is unspoken in these documents is the fact that the CQC declines to actually investigate whistleblowers’ concerns.
The government continues to avoid answering questions about whether CQC should do so under its current regulations, or whether new regulations will be drafted to ensure that CQC has clear powers to do so.
I have asked the DHSC to clarify its position in time for the event on 2 September 2019, but the correspondence fencing bout may well continue. The latest correspondence with the Department is copied below in the appendix.
The event on 2 September 2019 will be an expensive affair, and whilst CQC’s recent staff guidance documents are an improvement on past versions which were technically very rudimentary, little will be achieved until whistleblowers’ concerns are appropriately investigated.
If any Health or Social Care whistleblower who has not so far been invited to contribute wishes to send in comments on how CQC can improve its handling of whistleblowing, I would suggest sending written contributions to CQC FAO Professor Ursula Gallagaher.
UPDATE 24 AUGUST 2019
Some whistleblowers who have expressed interest in contributing to the consultation have received conflicting information about its scope. For clarity, this is the original correspondence from the CQC, sent on 14 August 2019:
RELATED ITEMS
Under UK whistleblowing law, CQC is part of a network of ineffectual ‘Prescribed Persons’:
Prescribed Persons or the Pretence of PIDA. How UK whistleblowers are ignored
The law needs to be urgently replaced:
Replacing the Public Interest Disclosure Act
Whistleblowers in Their Own Words: What’s wrong with UK whistleblowing law and how it needs to change
APPENDIX
Most recent correspondence with the Department of Health and Social Care about whether CQC will investigate whistleblowers’ concerns:
From: “Benjamin, Jennifer” <REDACTED>
Subject: RE: Will the government ensure that the Care Quality Commission investigates individual whistleblowers’ concerns?
Date: 16 August 2019 at 14:48:57 BST
To: Minh Alexander <REDACTED >
Cc: Caroline Dinenage <REDACTED>
Dear Minh
Thank you for your email. Just to confirm that your email to Alan has been picked up in his absence and we will be able to provide you with a response.
Jennifer
|
Jennifer Benjamin
Deputy Director – Quality, Patient Safety & Investigations
Department of Health and Social Care
Email: REDACTED |
From: Minh Alexander <REDACTED >
Sent: 15 August 2019 11:03
To: Benjamin, Jennifer <REDACTED>
Cc: Caroline Dinenage <REDACTED>
Subject: Will the government ensure that the Care Quality Commission investigates individual whistleblowers’ concerns?
Hi Jennifer,
I received an out of office message from Alan’s account, advising that he is away until the 5th September.
Are you able to help with my enquiry in his absence?
BW
Minh
From: Minh Alexander <REDACTED>
Subject: Will the government ensure that the Care Quality Commission investigates individual whistleblowers’ concerns?
Date: 15 August 2019 at 09:25:57 BST
To: Alan Addison
Cc: Jennifer Benjamin <REDACTED> Barbara Keeley <REDACTED> Caroline Dinenage <REDACTED> Laura Pidcock <REDACTED>
BY EMAIL
Alan Addison
Ministerial Correspondence
Department of Health and Social Care
15 August 2019
Dear Mr Addison,
Will the government ensure that the Care Quality Commission investigates individual whistleblowers’ concerns?
Since I last wrote on 9 August I have been invited by the Care Quality Commission to a consultation event on 2 September 2019, led by Ursula Gallagher Deputy Chief Inspector PMS and Integrated Care London, which includes reviewing how CQC manages whistleblowing by the staff of provider organisations:
“We are also reviewing our policies and procedures as they relate to how we manage information from people who work in the services we regulate and how we communicate and use the information shared. We have listened and heard that we have not always been successful at managing information shared with us. As a result of this, and in line with our commitment to consult on how we can make improvements, we are bringing together people who can help us to determine what good looks like.”
I also understand that the DHSC will be represented at this event.
In advance of the event, I have asked for sight of the relevant policy and procedural documents that are being consulted upon.
However, it would be surreal for this event to take place without a clear answer from the DHSC on its position on whether the CQC should investigate whistleblowers’ concerns.
I would therefore be very grateful if you could expedite your answer to the questions posed in my letter of 9 August below, before the event on 2 September, which are the subject of matters first put to the Department in December 2018.
Yours sincerely,
Dr Minh Alexander
Cc Caroline Dinenage Minister for Care
Jennifer Benjamin DHSC Deputy Director, Quality, CQC & Investigation
Barbara Keeley Shadow Minister for Mental Health and Social Care
From: Minh Alexander <REDACTED>
Subject: Your recent correspondence to the Department of Health and Social Care
Date: 9 August 2019 at 17:07:49 BST
To: Alan Addison <REDACTED>
Cc: Jennifer Benjamin <REDACTED> Caroline Dinenage <REDACTED>
BY EMAIL
Alan Addison
Ministerial Correspondence
9 August 2019
Dear Mr Addison,
Will the government ensure that the Care Quality Commission investigates individual whistleblowers’ concerns?
Thank you for your email regarding my query, first put to the Department eight months ago.
I asked if the Department would:
- Confirm that CQC has the powers to investigate, and should investigate, individual whistleblowers’ concerns
or
- Amend CQC’s regulations to make it unequivocally clear that CQC should investigate individual whistleblowers’ concerns.
I am unsure from your reply today whether the Department considers that CQC has the power to investigate individual whistleblowers’ concerns.
With regard to your comment:
“The CQC has the power to respond where a matter of concern raises any issues about patient safety or quality of care and will intervene in its capacity as a regulator. If, in the course of that action, it has concerns about the how a provider has responded to a whistleblower’s concerns, it can take regulatory action. A provider’s systems and processes in place to respond to complaints are assessed on inspection as part of the CQC’s ‘well-led’ key lines of enquiry.”
the CQC does ‘intervene’ sometimes in response to whistleblowers, largely superficially, and its actions are usually short of actual investigation. It tells whistleblowers it has no power to investigate.
Please can you clarify if your above advice means that the CQC has the power to investigate individual whistleblowers’ concerns about patient safety and or quality of care, and not just the way in which the provider responded to their concerns.
If what you are saying is that CQC has no powers to investigate individual whistleblowers’ primary, presenting concerns, as opposed to how their concerns were handled, please can you advise if the Department will amend CQC’s regulations to ensure that CQC has clear powers to investigate individual whistleblowers’ concerns about patient safety and or quality of care.
Yours sincerely,
Dr Minh Alexander
Cc Caroline Dinenage Minister for Care
Jennifer Benjamin DHSC Deputy Director, Quality, CQC & Investigation
From: Department of Health and Social Care
Subject: Your email to Caroline Dinenage
Date: 9 August 2019 at 16:30:20 BST
To: “Alexander, Minh” <REDACTED>
Our ref: DE-1185271
Dear Dr Alexander,
Thank you for your further correspondence of 1 August about the Care Quality Commission (CQC). I have again been asked to reply.
I was sorry to read that you were unhappy with my reply of 1 August (our ref: DE-1169259). I should clarify that it was a response to your correspondence of 5 March, 12 March and 28 May to Caroline Dinenage and 23 April to Matt Hancock.
I note your continuing concerns about the role of the CQC.
The CQC treats whistleblowing concerns as it would any other concern, and will use the information as part of its assessment of a provider.
The CQC has the power to respond where a matter of concern raises any issues about patient safety or quality of care and will intervene in its capacity as a regulator. If, in the course of that action, it has concerns about the how a provider has responded to a whistleblower’s concerns, it can take regulatory action. A provider’s systems and processes in place to respond to complaints are assessed on inspection as part of the CQC’s ‘well-led’ key lines of enquiry.
The CQC does not have the legal powers to intervene in, or investigate, an individual employment matter or how an individual is treated after raising a patient safety or quality issue.
I hope this reply is helpful.
Yours sincerely,
Alan Addison
Ministerial Correspondence and Public Enquiries
Department of Health and Social Care
From: Minh Alexander <REDACTED>
Subject: Your recent correspondence to the Department of Health and Social Care
Date: 1 August 2019 at 15:57:55 BST
To: Alan Addison <REDACTED>
Cc: Jennifer Benjamin <REDACTED> Caroline Dinenage <REDACTED>
BY EMAIL
Alan Addison
Ministerial Correspondence
1 August 2019
Dear Mr Addison,
Will the government ensure that the Care Quality Commission investigates individual whistleblowers’ concerns?
Thank you for your letter below.
Unfortunately, it is unclear to me to which of my letters you are replying.
Please could you clarify this.
If your letter is not a reply to my letter to Caroline Dinenage of 25 May 2019 about CQC investigation of whistleblowers’ concerns and related reminder letters of 19 June 2019 and 3 July 2019, none of which have been met with replies, please could the Department ensure a swift substantive response.
If your letter today is a reply to my above mentioned correspondence to Caroline Dinenage, it does not address the key issue that I have raised of whether the DHSC will either
- Confirm that CQC has the powers to investigate, and should investigate, individual whistleblowers’ concerns
or
- Amend CQC’s regulations to make it unequivocally clear that CQC should investigate individual whistleblowers’ concerns.
You will appreciate that this is a critical national patient safety issue.
CQC has avoided investigation of individual whistleblowers’ concerns since its inception 10 years ago, but with an admission to me last October that it might have been wrong to do so.
Your own Departmental lead for whistleblowing policy later advised me that CQC should be investigating individual whistleblowers’ concerns.
I first raised the issue with the Department eight months ago.
Please can the Department finally address this issue.
Yours sincerely,
Dr Minh Alexander
cc Caroline Dinenage Minister for Care
Jennifer Benjamin DHSC Deputy Director, Quality, CQC & Investigation