By Dr Minh Alexander retired consultant psychiatrist 25 July 2026
Summary: This post briefly reports on accumulating evidence which discredits Marianne Griffiths’ unsatisfactory review for NHS England on North East Ambulance Service’s fiddling of deaths reporting to coroners. The government relies on Griffiths’ report to deny bereaved families and whistleblowers a public inquiry, but it is steadily losing the moral high ground.
The inquest
The extraordinary inquest on Andrew Watson’s death, seven years ago, aged just 32, opened in June and resumed this week, with a conclusion that ambulance delay contributed to Andrew’s avoidable death from a throat abscess. The coroner determined that Andrew would probably have survived if ambulances had been more available.
Despite this, Griffiths inexplicably excluded Andrew’s case from her review of NEAS.
NHS England has been asked to account for this exclusion, but there is no substantive response yet.
Because the trust downgraded the level of harm suffered by Andrew, and withheld the true circumstances of his death from the senior coroner, an inquest in 2020 made a finding of death due to natural causes.
After Andrew’s family discovered that there had been ambulance delay and care failings, they pressed for the current inquest.
This second inquest has now heard that two paramedics and a trust manager were pressured to downgrade the harm that Andrew suffered. The former NEAS Head of Quality and Safety was accused of leaning on staff to ensure that harm was downgraded.
In returning his verdict yesterday, the coroner for Durham and Darlington pointedly noted evidence that the trust had gerrymandered evidence, retrospectively trimming the reported level of harm to fit the excessive ambulance response time.
He commended the integrity of paramedic staff who objected to the manipulation of evidence and noted that they did not agree to the downgrading of harm.
The coroner also indicated that he had given latitude within the inquest for the examination of NEAS’ handling of the death and its poor governance because this had an effect on the coronial process, and because a public inquiry had not been established which could examine these issues. He considered these were matters of public interest.
He intends to issue a Prevention of Future Deaths report regarding ambulance escalation process.
These are some of the media reports which covered the inquest:
The coroner’s comments and conclusions about NEAS’ cover up and manipulation of evidence with the effect of avoiding coronial scrutiny have significant implications for the Griffiths review, NHS England and the government.
The system response
Griffiths examined only four cases when NEAS whistleblowers had flagged at least ninety. Did she exclude Andrew Watson’s case because NHS England knew his case would reveal strong evidence of deliberate cover up?
Griffiths ended up claiming ridiculously that she could not make a finding of deliberate cover up by NEAS because, in terms, she wasn’t there.
At the top of this creaky edifice, the government has refused bereaved families and whistleblowers a public inquiry based on the claim that the Griffiths review was sufficient. It very clearly was not, now emphatically driven home by the Watson inquest.
Further demonstrating persisting poor culture, NEAS issued a disingenuous public statement in response to the inquest outcome.
It was issued by Karen O’Brien the Director of People and Development, also Deputy Chief Executive.
The statement claimed that relevant issues had been extensively reported by the Griffiths review in 2023.
This was misleading given that Griffiths did not even examine Andrew Watson’s case, and did not concede any deliberate cover up by NEAS.
The trust’s statement is in part a facile good news message. It fails to apologise for the deliberate cover up. It only apologises for the ambulance delay, and even then gracelessly claims that it has “always” acknowledged the delay.
In a dismal sort of circularity, it is relevant to remember that Griffiths claimed in her 2023 review report that everything was better at NEAS because it was under a new management team.
However, it seems from the disrespectful and less than truthful NEAS response to the inquest outcome, that some things are unchanged at the trust.
Even at this late hour, NEAS seems incapable of candour.
RELATED ITEMS
1.Fitness to practice proceedings continue against two senior NEAS nurse managers who are accused of bullying and withholding information from the coroner.
Distressingly for the affected bereaved families, a hearing was part heard earlier this year and will resume next year:
2. Karen O’Brien the NEAS Director of People and Development has been in post at NEAS since 2020.
She oversaw the trust’s attempt to unlawfully gag the coronial cover up whistleblowers with settlement agreements which restricted their ability to pursue public interest disclosures. One signed and one refused.
Griffiths later downplayed this serious breach, portraying it as a matter of poor governance instead of illegality.
As head of human resources, O’Brien obviously also had a large share of the responsibility for NEAS whistleblowing governance, which has been criticised.
By Dr Minh Alexander retired consultant psychiatrist 24 July 2026
Prompted by public statements by Liberal Democrat politicians about the “Office of the Whistleblower”, whilst many troubling questions remain about the private company WhistleblowersUK, I have written an open letter to Ed Davey leader of the Liberal Democrats. This is both to express concern and to seek clarification of his party’s policy position.
Two of his MPs are currently directors of WhistleblowersUK.
It seems important to have clarity, especially as there seem to be efforts to hitch their wagon to the Hillsborough Law as well.
By Dr Minh Alexander retired consultant psychiatrist 19 July 2026
Summary The troubling private company WhistleblowersUK was criticised in a recent documentary film by JAM Motion Pictures. Norman Lamb former MP contributed to these criticisms and specifically raised issues of transparency and accountability. He indicated that WhistleblowersUK refused to answer questions which he raised in 2019 on my behalf, about matters such as potential conflicts of interest. WhistleblowersUK later denied it had been given a right of reply to the film and also claimed that the then Co Chair of the Whistleblowing APPG Stephen Kerr MP, now MSP, referred these matters to the Parliamentary Commissioner for Standards. WhistleblowersUK published a 2019 email purportedly from Stephen Kerr, claiming that there had been a finding of “no case to answer”. A Subject Access Request to parliament for my personal data has not confirmed any such referral or finding from 2019. Mr Kerr has been asked for further information. WhistleblowersUK denied that they were given a right of reply to the recent documentary film. The filmmakers say they have supplied WhistleblowersUK’s Chair with their original email correspondence which repeatedly sought comments/responses to their film, and which were blind copied to the filmmaker’s lawyers. Following this WhistleblowersUK removed social media and website posts, some of which claimed that the filmmakers and a participating individual had lied. It is claimed that WhistleblowersUK has not apologised. I am not aware of any published apology.
Background
The private company WhistleblowersUK Companies House 09347927 was incorporated on 9 December 2014 . It was created after a split in the original entity, Whistleblowers UK Companies House 08112953 (incorporated 12 June 2012, dissolved 7 April 2015). This split followed conflict in which it is alleged that a co-founder, inter alia, took unilateral action to advocate for whistleblowing financial bounties. Those who say they objected to this, left.
The remaining nucleus set up the new entity with the similar name in 2014, WhistleblowersUK Companies House 09347927 . This company has advocated for US style bounties ever since. That is, financial rewards for whistleblowing. In the US, such financial rewards are open to anyone who provides requisite information for the State to recover money, and not just employees who whistleblow on their employers. Crooks who turn in other crooks may qualify for rewards. In some ways, the US model is more akin to a system of rewarding criminal informants. Vast sums may be awarded so long as monies recouped by the State exceed a given threshold. Much, much more money than any one person will ever need. Genuine whistleblowers who suffer major detriment but fall below this financial threshold are left in the cold. The model focuses on the financial sector. It is likely to disadvantage other whistleblowers and sectors such as Health and Social Care where there is very high public interest but little bounty to recoup.
The concept of bounties is repugnant to many, with concerns that it is damaging to true whistleblowers who are already marginalised and reviled by employers. It has therefore has been resisted for years in the UK despite the prolonged efforts of powerful (and wealthy) US bounty hunting law firms to introduce the model here.
As the Westminster APPG campaign was financed and grew more slick, it gathered more names for a while. This eventually fizzled out, and the APPG is now defunct. But this was not before a Bill which opened the door to the US bounty model was repeatedly introduced to parliament. The Bill was introduced by various MP/peer members of the APPG as a private members Bill and repeatedly fell, but it was a useful vehicle for publicity. It opened the door to the US bounty hunting model by redefining whistleblowers as all members of the public, and not just as employees meeting certain criteria. And whilst the Bill did not explicitly introduce financial rewards, it had room for future alteration: A Bounty Hunters’ Bill? A critique of the Whistleblowing APPG’s April 2022 Bill
Other concerns have also been raised about WhistleblowersUK besides its pursuit of financial bounties in the UK. It has asked whistleblowers seeking help for money and a percentage of awards and settlements, it charges money for associate membership which does not come with voting rights and there are concerns about how it has treated some whistleblowers. A recent documentary by JAM Motion Pictures reported that a large number of whistleblowers had reported mistreatment and the film makers obtained derogatory messages about whistleblowers. Norman Lamb former MP appeared in the documentary and spoke to his concerns about a lack of transparency and accountability by WhistleblowersUK. WhistleblowersUK has to my knowledge not so far answered the allegations of mistreatment.
Instead, WhistleblowersUK initially flatly denied that it had been given the right of reply to the film, posting several related items on social media and its website.
Later, after JAM Motion Pictures reported that they had furnished WhistleblowersUK’s Chair with the original, repeated emails showing repeated attempts to seek comments from WhistleblowersUK, which were bcc’d to the filmmaker’s lawyers at the material time, WhistleblowersUK removed its various denials.
Some of these denials had alleged that WhistleblowersUK’s accusers had lied. Via a tweet, WhistleblowersUK publicly accused one person of lying. Via a statement on its website, purportedly by its Chair Jo Gideon former MP, the company stated that the individual and the film company “are both joining in what is in fact a lie.” However after the removal of these denials and counter-accusations from WhistleblowersUK’s website and social media, the company reportedly issued no apologies. As far as I am aware, this remains the case. I have seen no published apologies.
Questions which WhistleblowersUK failed to answer and which Stephen Kerr MSP purportedly claimed he referred to the parliamentary Standards Commissioner
In 2019 I asked members of the then Whistleblowing APPG about the activities of the APPG’s questionable external secretariat WhistleblowersUK, its inconsistent/ un-evidenced claims and potential conflicts of interest.
The only response came from Norman Lamb MP, then an APPG member, who agreed to pass on my questions.
He eventually resigned from the Whistleblowing APPG. After I learnt of this and made enquiries, it transpired that he had given WhistleblowersUK’s failures to answers my questions as his reason for resignation:
Zipping forwards to the present day, after the recent release of the JAM Motion Pictures film in May about WhistleblowersUK, WhistleblowersUK published a 5 November 2019 email purportedly from Stephen Kerr MSP to Norman Lamb. This claimed that concerns raised about WhistleblowersUK at that time were all passed to the parliamentary Standards Commissioner:
“….all such allegations against the Secretariat of the APPG have been passed to the Parliamentary Standards Board [sic *] and that the Board continues to affirm that there is no case to answer.” *Parliament has confirmed that there is no such body as the “Parliamentary Standards Board”. It has worked on the assumption that Mr Kerr, or whoever wrote the email, was referring to the Parliamentary Commissioner for Standards.
The claim of onwards referral was unexpected as I never heard from Mr Kerr when I raised questions about WhistleblowersUK in 2019. One would have thought that if he had acted then upon my queries, and indeed presumably passed my personal data onwards, he would naturally have written back to me to discuss these matters.
In any case, I was largely asking questions rather than making allegations, so I do not understand on what basis Mr Kerr would have passed my correspondence/issues to the Standards Commissioner. I am also not sure what remit the Standards Commissioner would have to investigate an external APPG secretariat.
And neither did the Standards Commissioner nor anyone from his office contact me in 2019 about a referral by Mr Kerr, nor the outcome of any investigation exonerating WhistleblowersUK as claimed by the email attributed to Mr Kerr.
But to test the claims that my questions and concerns were passed to the Standards Commissioner, I asked parliament for my personal data as held by the Standards Commissioner.
On 15 July 2026 I received a reply, Subject Access Request D26-065, which confirmed that the Standards Commissioner did not hold:
1. Any correspondence from Stephen Kerr to the Standards Commissioner about me
2. Any of the correspondence from me to Kerr and other members of the Whistleblowing APPG in 2019, in which I asked questions and raised concerns about WhistleblowersUK’s potential conflicts of interest and other matters
That is to say, there was no evidence in the SAR disclosure to confirm that Stephen Kerr acted on my issues as his purported email of 5 November 2019 claimed.
I have now written to Mr Kerr to ask:
That he confirms whether or not the 5 November 2019 email that was previously reproduced on the WhistleblowersUK’s website (now removed) was an email that he sent in 2019
Whether or not he passed on my 2019 questions and concerns about WhistleblowersUK to the Standards Commissioner as the email claimed
For disclosure of my personal data relevant to any purported 2019 referral of my questions and concerns to the Standards Commissioner, if indeed a referral was made.
RELATED ITEMS
The bounty hunting model involves vast sums.
Unsurprisingly, it has led to regulatory corruption, as uncovered by Prof Platt after a prolonged FOI battle:
The model of litigation in US bounty hunting is known as Qui Tam, or in the name of the King.
It comes from a very rough, archaic form of governance in Ye Olde England which stemmed from shortage of public resources to run a more sophisticated model. Thugs and rogues were often deputised, and came to be feared and despised:
In the US, the model was introduced during civil war time due to exceptional exigency, and recognised as a lesser evil. The Union held its nose and dealt with criminals to control fraudulent defence sales:
“In short, I have based the…sections upon the old-fashioned idea of hold out a temptation,” and “setting a rogue to catch a rogue…a reward for the informer who comes into court and betrays his co-conspirator”
By Dr Minh Alexander retired consultant psychiatrist 17 July 2026
Summary
This is a brief post to share a report commissioned by Cambridge University Hospitals NHS Foundation Trust (CUH) into whistleblowing governance, as applied to consultants and SAS (specialty, associate specialists and specialist) doctors at the trust.
A low response rate and disturbing insights into the experiences of doctors raising concerns paint a dismal picture. Lowlights include a universal lack of faith that raising concern will lead to action, normalised patient safety risks due to this organisational inaction, passive aggressive managerial silence in the face of concerns raised and identification of several departments as managerial trouble spots. These are neurosciences, emergency medicine, paediatrics and some surgical specialities.
It was a mixed method exercise, including a survey.
The key lines of enquiry for the exercise were:
“The KLOEs span eight distinct themes related to medical voice. Section five aligns qualitativeand quantitative findings to these to outline consultant and SAS doctor experience.
1. Psychological safety and voice
2. Representation, credibility and fairness of voice
3. Risk, early warning and organisational intelligence
4. Learning, prioritisation and visible ownership
5. Follow-through, trust and confidence
6. Inclusion, belonging and equity of experience
7. Blind spots, strategic gaps and unmet priorities
8. Surfacing best practice
The authors claim:
“All data collected through this process was handled with strict attention to confidentiality and ethical principles. Contributions were analysed by a small team, to reduce the number of people reviewing outputs. Anonymous quotes found within this report have been included and signed off by interview participants themselves or by written consent via the survey. No raw data has been provided to CUH.”
I could find no other information on data handling/ storage.
Results
The exercise engaged only 19% of target staff, in itself an indication of poor culture and staff hesitancy.
The data gathered represented:
128 survey responses
45 interviews
7 meetings
The survey authors noted “Many participants have had poor experiences of previous organisational leadership within CUH.”
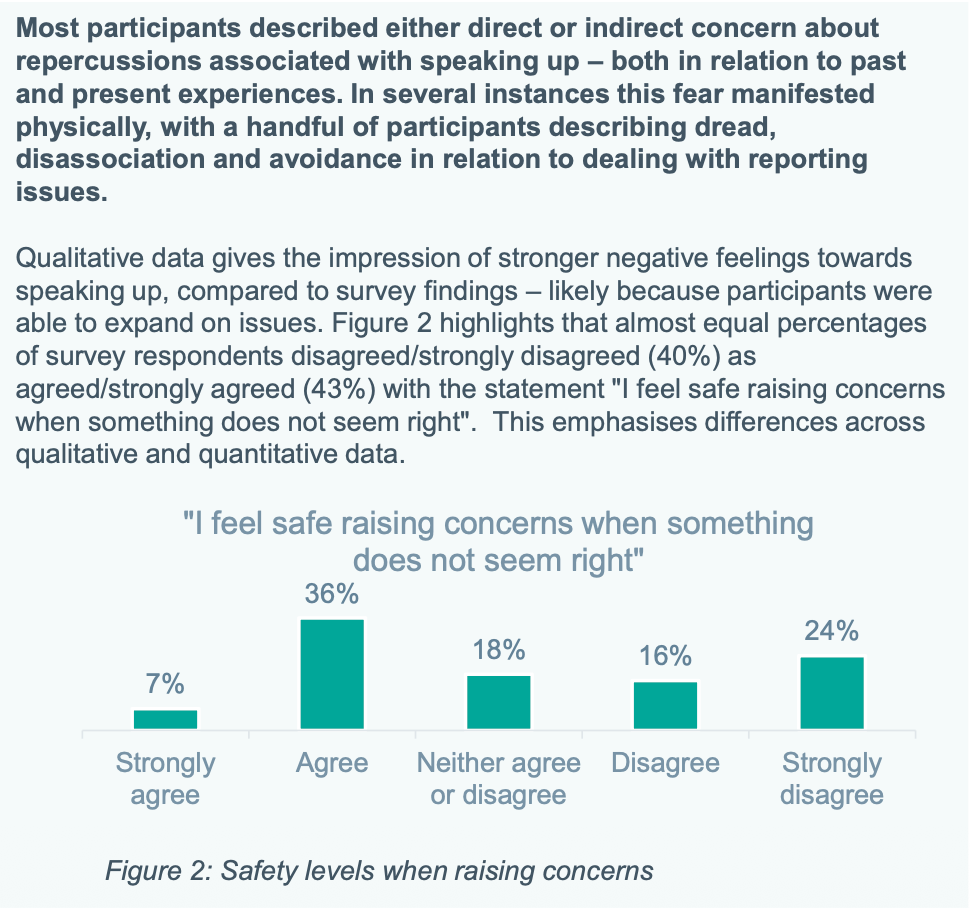
Importantly, crude survey responses gave a better impression of whistleblowing governance than detailed qualitative responses.
This has implications for the national NHS staff survey, which relies only on a few simple questionnaire indicators about staff whistleblowing experience.
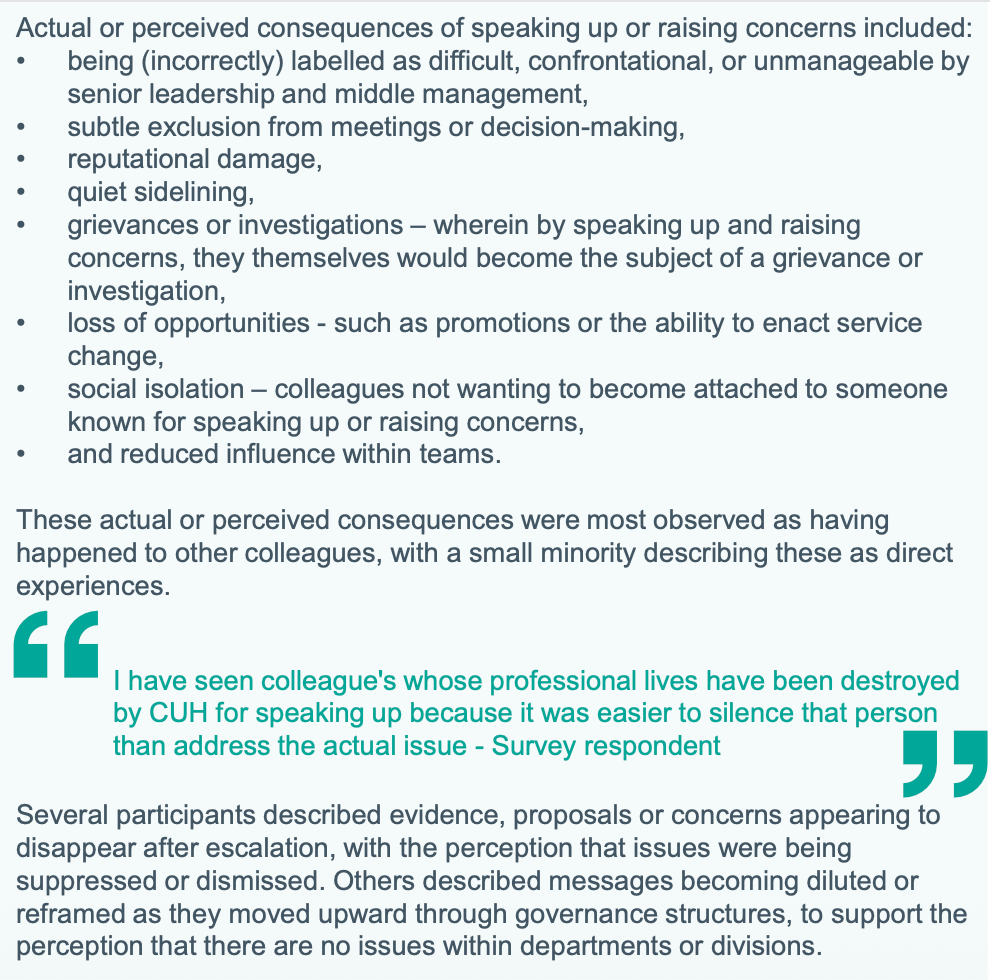
Some staff described severe symptoms of anxiety such as dissociation (feeling detached from reality and surroundings) with regards to whistleblowing. Others reported seeing colleagues “destroyed” for speaking up, as part of a range of typical whistleblower detriments.
Doctors are in an impossible situation because they are ethically obliged to raise concerns, but know that doing so carries risks, sometimes serious.
Importantly, according to respondents, CUH departments which were associated with particularly bad leadership and whistleblowing governance are neurosciences, emergency medicine, paediatrics and some surgical specialties:
Unsurprisingly, the Freedom To Speak Up model was questioned and staff expressed a lack of confidence in whether neutral support “genuinely” existed:
Echoing repeated national NHS staff survey findings, there was “universal” lack of confidence in whether speaking up led to change. The results at CUH were more extreme than the national staff survey:
Not unique by any means to CUH, some of the review participants reported that concerns were sometimes met with silence:
“Many talked about often not even getting a response or acknowledgement when they raised issues.”
As an aside, staff should understand that this silence is a form of passive aggression by managers, and is in effect a warning to desist.
Should the unfortunate member of staff press their concerns, the risk of active management reprisal increases.
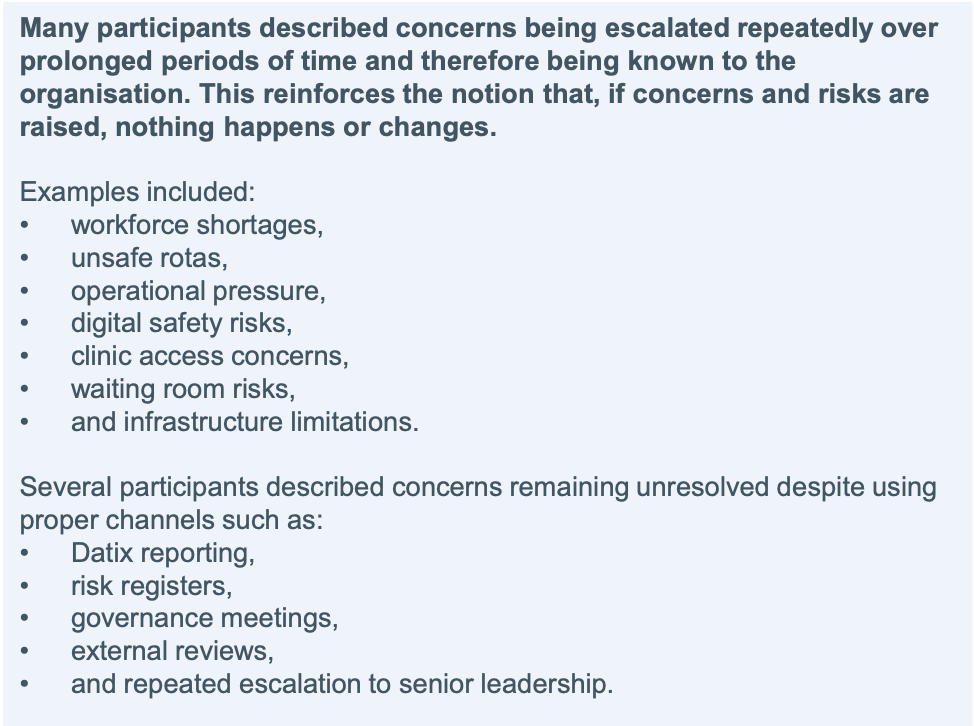
Respondents described a picture of unsafe conditions becoming normalised:
“Participants frequently linked deteriorating psychological safety with systemic workforce shortages, burnout, corridor care, service targets and on-going investigations/patient safety issues. The perception being these issues are never resolved and, worse, have become normalised.”
The typically normalised risks were as follows:
Doctors were concerned that CUH prioritised financial and reputational considerations:
“Many participants described concern that organisational prioritisation is perceived to be driven more strongly by operational, financial and reputational pressures than by frontline clinical experience.”
Related to the failures of listening up, doctors also reported serious flaws in trust consultations and investigations. For example:
The survey found that SAS doctors and internationally trained consultants had worse experiences of whistleblowing governance:
“….SAS doctors and internationally trained consultants were perceived as less likely to feel comfortable speaking up or being heard”
The authors felt their review uncovered additional issues that had not been identified by the Verita investigation into the Stohr scandal, and that cultural problems and organisational risks ran deeper:
Lastly, I must declare that I have fairly extensive experience of health services in this region as a carer. This includes, over the years, experience of care failures and cover ups. CUH has had its ignominious moments, but was not the worst. And at times it was much better than average. What on earth does that say about the health of our NHS?
ADDENDUM
I do not recommend that NHS staff use internal mechanisms for whistleblowing. The likely gain for the public interest set against potential harm to the whistleblower is unlikely to justify such a course. Instead, directing disclosures to the media either anonymously or with agreement of anonymity is safer. It is best to take advice as each individual’s circumstances are unique and it is a very personal decision. For example, someone earlier in their career with a young family to support has much more at stake than someone nearing retirement, who can afford to weather any financial consequences. It should also be noted that if you whistleblow externally and anonymously, and you are suspected and victimised, an employer may be able to claim that they did not know that you were a whistleblower. Take advice and consider options carefully. Equally, not all whistleblowing ends in disaster for whistleblowers, but whistleblowing about serious matters which threatens organisations or senior individuals is more likely to attract reprisal. Especially if a whistleblowers persists with their concerns.
RELATED ITEMS
At the Lampard public inquiry into failures at Essex Partnership University NHS Foundation Trust on 15 July 2026, Brian O’ Donnell clinical lead gave evidence that senior managers asked him to get rid of 4000 unresolved incident reports, dating back years:
Dr Minh Alexander retired consultant psychiatrist 8 July 2026
Summary: This is a very brief post to share an FOI response by the National Confidential Inquiry into Suicide and Homicide by People with Mental Illness
With the Nottingham public inquiry in progress, some media narratives have at times been sensationalised and stigmatising, and they have “othered” mental health patients, who have been portrayed as “them”.
To help illustrate that these are not simple, black and white issues, I post briefly here about mental health homicides against mental health patients.
There is a large literature on violence on mental health wards, with the victims often being patients. There are intermittent headlines about assaults on psychiatric units. But there is less specific data available on homicides in mental health settings.
I asked the National Confidential Inquiry into Suicide and Homicide by People with Mental Illness (NCISH)* if it had any data on mental health homicides committed against mental health patients.
*NCISH was renamed after NHS England pulled the funding for homicide research but this has been re-commissioned so I use the original name, to which the Inquiry will revert, for simplicity.
The Confidential Inquiry advised that it does not collect this data routinely, but it did examine this issue in a 2014 paper by Rodway et al. This found that 29 mental health patients over a three year period (1 January 2003-31 December 2005) had been killed by other mental health patients.
This is in the context that there are an average of 58 people a year who are the victims of mental health homicides, by NCISH’s methodology. (There is debate about this).
In total, the 2014 study found that 90 mental health patients were the victims of homicides in the three year period. The majority (86) of homicides occurred in the community and four occurred in hospital. Of the four homicides in hospital, three were committed by other patients.
This is the relevant part of the FOI response from NCISH:
“NCISH collect demographic characteristics and offence related information on victims of homicide but we do not routinely collect clinical data. We did undertake a more detailed analyses on patients as victims of homicide in our paper on ‘Patients with mental illness as victims of homicide: a national consecutive case series’ (Rodway et al., 2014). In this national consecutive case-series study, we obtained data for victims and perpetrators of all confirmed homicides between Jan 1, 2003, and Dec 31, 2005, in England and Wales. Patients were defined as people with contact with mental health services in the 12 months before death.
During this period 90 homicide victims (6% of all homicide victims) had contact with mental health services in the 12 months before their death. Of the 90 patient victims, 29 (32%) were killed by another patient with mental illness.
Overall most patient victims were community patients (n=86, 96%). Four (4%) were in-patients at the time of death. Three of these deaths were cases of homicide perpetrated by other inpatients at the same hospital. Information is not available on whether these patients were detained and whether the offence took place in a locked environment.”
This is the full FOI reply by NCISH which also gives helpful contextual information on other victim analyses:
Mental health homicides are horrific tragedies, overlying a complex lattice of many failures.
It is important that public protection is achieved with humanity, full understanding and the full range of evidenced-based and effective measures. I hope that the government will avoid the trap of simplistic, media-driven outcomes.
RELATED ITEMS
Examples follow of mental health patients who were victims of mental health homicides, both in hospital and in the community, in settings such as supported accommodation. The first four cases relate to East London NHS Foundation Trust.
2) The recently published public inquiry report on patient abuse at Muckamore Abbey Hospital in County Antrim by Tom Kark (previously Counsel to the Mid Staffs public inquiry) made significant findings and recommendations on the use of CCTV in the safeguarding of vulnerable populations.
It was recognised that but for CCTV, the serious abuse against patients at Muckamore would likely not have come to notice. However, there were also concerns about how some hospital managers handled CCTV evidence. Related to this, Kark made recommendations on ensuring the independent handling of CCTV evidence.
By Dr Minh Alexander retired consultant psychiatrist 15 June 2026
This is a brief post to raise awareness of a second inquest which opens tomorrow into the death of 32 year old Andrew Edward Watson
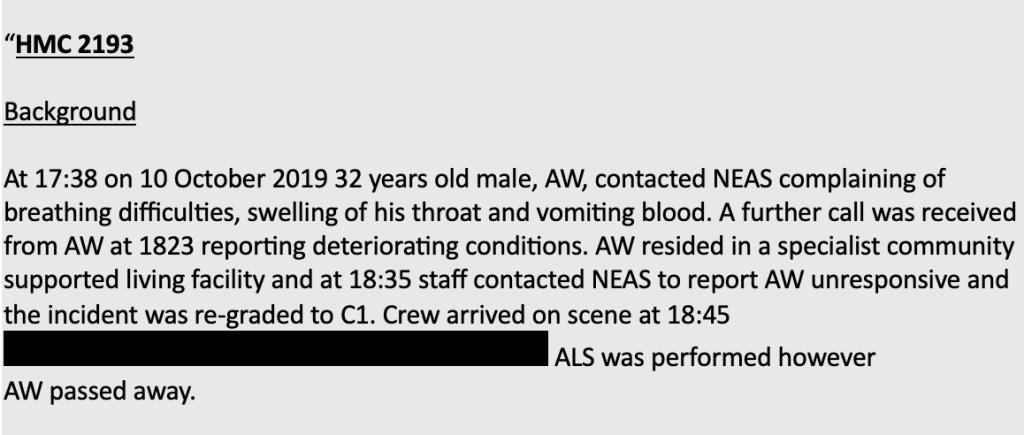
Andrew died on 10 October 2019 after being unable to breath due to a quinsy, which was an abscess in his throat related to severe tonsillitis.
The condition is a recognised emergency when signs of sepsis or airways obstruction, such as difficulty breathing, are present. It is in theory fully treatable.
An ambulance was called to Andrew’s home, but the response was delayed. He had become unresponsive by the time an ambulance arrived. He could not be revived despite attempts to resuscitate him.
North East Ambulance Service (NEAS) is accused of covering up its failings by withholding relevant information about the ambulance delay from the coroner:
As a result of the information about the circumstances of Andrew’s death being withheld, a previous inquest held in 2019 concluded that Andrew’s death was due to natural causes.
However, a second inquest was scheduled after whistleblowing disclosures by Paul Calvert, a coroner’s officer employed by NEAS, revealed that information had been withheld from the coroner:
The second inquest highlights that matters regarding NEAS’ governance are far from resolved.
Both NEAS and NHS England (NHSE) were implicated in the failures, as NHSE failed to respond adequately to whistleblower concerns. However, NHSE was allowed to oversee the investigation into NEAS’ failings, which was controversially contracted to Marianne Griffiths.
Griffiths was the former CEO of University Hospitals Sussex NHS Foundation Trust which had recurrent whistleblower scandals including maternity care whistleblowing, an ongoing police investigation into surgical harm and most recently a maternity care scandal necessitating inclusion in the national investigation programme.
Griffiths’ investigation into NEAS commanded little credibility, not least because NHS England’s highly restrictive terms of reference for the investigation excluded many relevant cases, focusing only on four cases when trust whistleblowers flagged more than ninety:
Griffiths failed to review Andrew Watson’s case despite it being one of the cases flagged by a previous report commissioned by NEAS, the so-called “Interim Audit One report”.
NEAS attempted to suppress the Audit One report for a long time, and it was only released into the public domain in 2025 in a very heavily redacted form after a prolonged FOI battle, involving an appeal to the Information Commissioner.
Both the Sunday Times and local media have confirmed that the Interim Audit One report covered Andrew’s case.
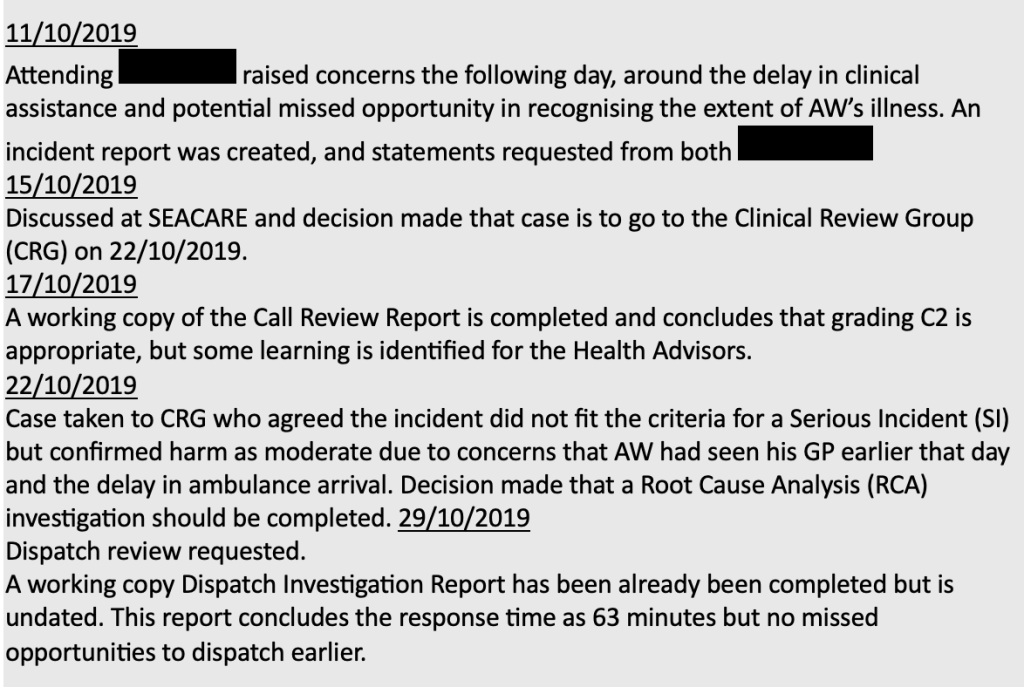
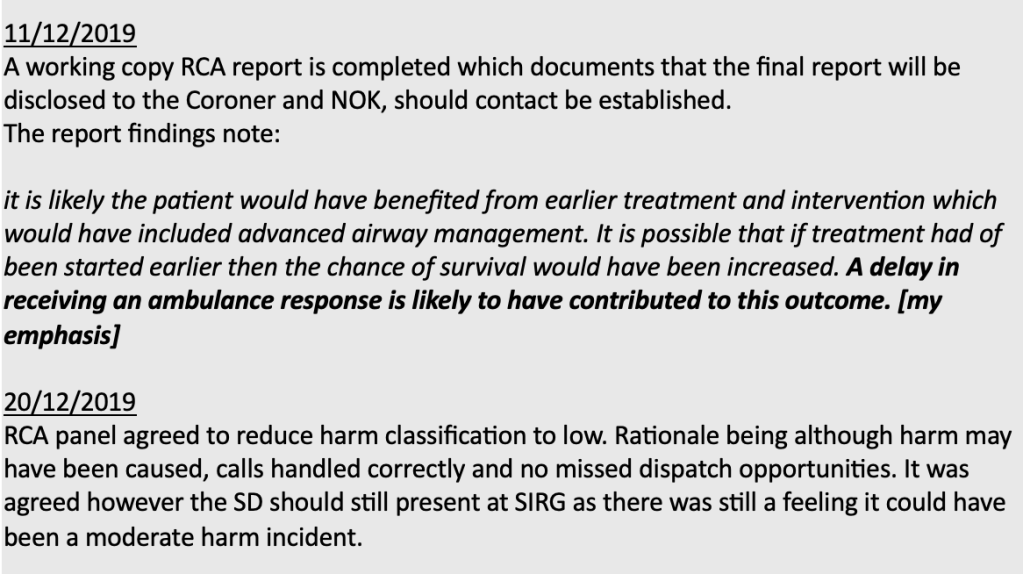
The relevant passage from the report crucially noted that an internal trust root cause analysis concluded ambulance delay contributed to Andrew’s death.
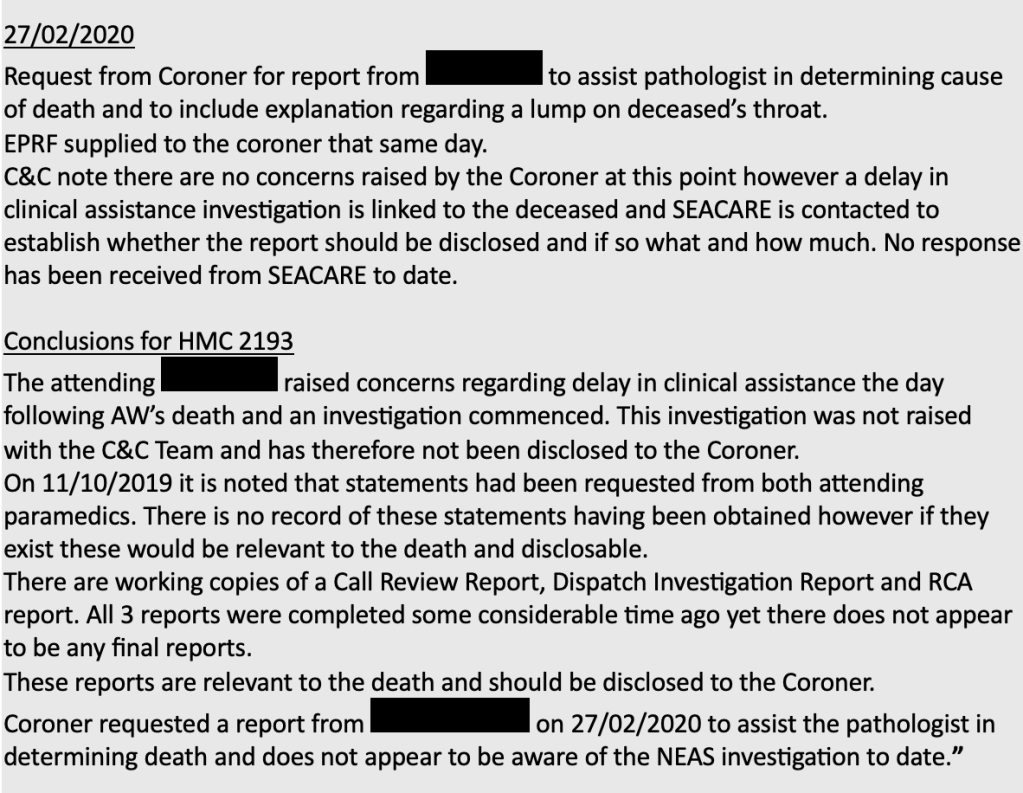
It also noted that this internal RCA report and other relevant documents were not disclosed to the coroner.
This is the crucial, relevant section from the Interim Audit One report on Andrew’s case:
They are accused of playing a key part in the minimisation of trust operational failures and subsequent failures to inform the coroner about these in relation to deaths. One of the accused registrants, SD, was reportedly party to the above decision on 20 December 2019 to downgrade Andrew’s death to a “low” harm classification.
Reclassification to “low harm” meant that the trust did not have to disclose these matters to Andrew’s family under the statutory Duty of Candour.
This is Care Quality Commission regulatory guidance which stipulates that provider organisations should disclose harm where the harm is classed as “moderate” or “severe”, and does NOT require disclosure when harm is classed as “low”:
The fitness to practice hearing was scheduled earlier this year but ended only part heard, and will resume next year.
The government has so far resisted calls for a public inquiry, which is an injustice in the face of the questions left unanswered and the serious failures of the Griffiths report and its commissioning.
UPDATE 25 JULY 2026
The inquest was heard in two tranches in June and July and has now concluded. Extraordinary evidence of a deliberate cover up was heard. Two paramedics and a NEAS manager were pressured to downgrade the level of harm suffered by Andrew Watson. The coroner has determined that Andrew would probably have survived if more ambulances had been available, and that ambulance delays contributed to his death. The coroner concluded that evidence had been manipulated and that this had an effect on the coronial process, delaying a proper hearing by seven years. He commended the paramedics’ integrity for objecting to the downgrading of harm:
Death of Mr Peter Coates – an example of manipulation of evidence by NEAS
On 23 March 2026 Paul Appleton the coroner for Teesside and Hartlepool issued a Prevention of Future Deaths report on the death of one of the victims of the NEAS scandal, Peter Coates.
Mr Coates died of asphyxiation due to a combination of severe respiratory disease and a power cut at his home which meant that he was unable to access his usual oxygen treatment. He called 999 but there was a delay in an ambulance reaching Mr Coates because a nearby vehicle could not get through electrically controlled gates because of the power outage (and because the crew did not know of a manual override), and because another vehicle stopped to refuel despite having sufficient fuel in the tank.
The coroner concluded this year that the ambulance delay may have been a contributory factor in Mr Coates’ death:
“Peter’s death was possibly contributed to by delays in the arrival of the ambulance crew to him.”
In 2023 the Griffiths report acknowledged the family’s concern that the delayed ambulance response was a contributory factor in Mr Coates death, but in my view Griffiths’ report did not make it sufficiently clear that an inquest was yet to make a finding on this issue.
Originally, when the coroner first opened an investigation into Mr Coates’ death, NEAS did not fully disclose the circumstances of the death, downgraded the level of harm to “low” and excised facts from evidential documents, as reported by the Sunday Times:
“Although an investigation began the same day, the coroner was not made aware of this at the time, or of the fact that there had been any delay in getting help. Despite the mistakes and delays, a decision was made by bosses to downgrade the incident to “low harm”, on the basis that the primary reason for Coates’s death had been the oxygen equipment malfunction. The coroner, in fact, “should have been notified” straight away about the death and about the delays, the AuditOne investigation found. The NEAS internal investigation soon found that the second ambulance had in fact had sufficient fuel to complete the journey. This raised questions as to why the stop occurred. A statement made by one of the paramedics involved, explaining the decision to refuel, was never disclosed to the coroner. Instead, the paramedic was asked by bosses to produce a new statement, which made no reference to the decision to refuel. The coroner was “only supplied with the [later] statement, which does not include any reference to the refuelling”, AuditOne found.”
Unless a statutory public inquiry is held, we will never know how many other cases were subject to such manipulation of evidence and self-interested under-estimation of harm.
By Dr Minh Alexander retired consultant psychiatrist 25 April 2026
This is a brief summary report to raise awareness of a recent case of NHS whistleblower retaliation and mobbing against a nurse who refused to fall in with medication administration practices that deviated from trust policy, and involved falsification of medical records.
In March 2023 Mr Thomson took up a substantive post as a nurse at University Hospitals Bristol and Weston NHS Foundation Trust and after three months switched to a bank contract to accommodate family circumstances, which included his wife’s ill health. For the purposes of UK whistleblowing law, he was still a “worker” under the Act.
Mr Thomson also had disabilities of autism and dyslexia.
In July 2023 he raised concerns about trust staff giving 08.00 iv medications at 06.00 am and falsely recording that the medications had been given on time. He refused to do this and continued to raise the matter.
Mr Thomson had other concerns about patients being woken up too early. For example: “…confused/dementia patients being made to get up, washed and dressed from 5am “to help the day shift staff”. There was also a concern about staffing levels.
A ward manager emailed the Modern Matron thus:
“The RN has refused to give the morning IV antibiotics between 06.00 and07.00 as they are prescribed for 08.00. The SOP for administration ofmedicines says all critical medications should be administered within onehour of the prescribed time, but practices are that 08.00 IV medicationsare given at the end of the night-shift as workload in the morning does notusually allow for tis [sic] to happen, normally being administered around 06.00.”
The Tribunal accepted that Mr Thomson’s concerns were protected public interest disclosures and observed:
“The Claimant said that he refused to do this as he felt it was incorrect practice and moreover was resulting in documentation being falsified, as the medications were being recorded as being administered at 8am. The Claimant was concerned that this was being done in order to reduce the workload of the day shift. Essentially, his view was that the convenience of the nursing staff was being prioritized over patient comfort and safety.”
Mr Thomson’s conscientious objection set off a cascade of events at the trust, with complaints made against him. The Tribunal determined that these were “exaggerated” and led to retaliatory restriction and then a ban from bank work in August 2024, which constituted whistleblower detriment.
The Tribunal emphasised that senior nurses were involved in exaggerating the allegations against Mr Thomson: “The nursing staff, including senior nursing staff, produced a complaint which was misleading.”
The Tribunal criticised the overall fairness of the process by which the trust arrived at the bank work ban, including failure to call all relevant witnesses.
The Tribunal also questioned the use of an exceptional mechanism for terminating Mr Thomson’s bank contract, which the trust’s former Associate Director of HR Operations indicated was used for “tricky cases”:
“145. The Tribunal was concerned about the fact that a DMG [Decision Making Group] was chosen as the appropriate vehicle for dealing with the matter. This appears to have been Sarah Dodds’ decision but there was no evidence about her reasons for this. Mr Dickson said that the DMG was used for “trickycases”. However, the Respondent’s policy makes clear that DMG meetings are used for serios [sic] and urgent cases. There did not appear to be anything urgent in relation to the situation.”
As NHS trusts are near-monopoly employers in any given area, such bans can have serious implications for any bank NHS worker. In Mr Thomson’s case, it was potentially even more serious because of his family circumstances and his own disabilities and issues with change.
The Tribunal concluded:
“The Claimant’s disclosure raised an issue which put pressure on the nursing staff, as it involved weighting the convenience of the staff against the comfort and safety of the patients. We consider that the nursing staff provided misleading information about the Claimant to the Bank and this is what resulted in the restriction and the subsequent ban on his working in the ED, which does not seem to have been properly recorded and for which no proper reasons are given.”
“The Respondent is liable for the detriment of restricting the Claimant form working in the ED caused by the misleading and exaggerated complaint raised by the nursing staff. We are satisfied that the complaint was materially influenced by the Claimant’s disclosures.”
The Tribunal was satisfied that Mr Thomson was a credible witness.
“16. We found the Claimant’s evidence to be clear and consistent. We considered that he was an honest witness, and indeed the Respondent did not suggest that he was being untruthful in relation to any matters.”
It was less content with the trust’s witnesses. For example:
“54. We are satisfied that the nursing staff in the ED exaggerated the seriousness of what the Claimant did when they raised the complaint and, in relation to the move to Sandford ward and his leaving at 2am, supplied false information to the Bank office.”
“20. In relation to Ms Cordeiro-Sorroche [Modern Matron], we did not consider that any proper explanation was given for her failure to mention that she was aware of the Claimant’s protected disclosures, in her meeting with him on 08 August 2024, despite the fact that the Claimant was seeking to discuss the fact that he had made these with her. Her witness statement also said that she discussed and agreed with Alex Rossiter, another manager, following the DMG meeting, that Alex Rossiter would send the letter notifying the Claimant’s of his removal from the Bank. However, Alex Rossiter had not attended the DMG meeting.”
“132. We had some difficulties with evidence of Sam Trumble [Clinical Lead for the Bank]. On many occasions she seemed vague and unclear in her evidence and did not appear to understand questions relating to it, even when they were explained to her.”
“18. For example, Ms Trumble’s evidence in her witness statement was that “several wards” had raised complaints about the Claimant and there was “a catalogue of complaints with a theme arising” about him. However, it was accepted that there were only two complaints, from the same ward, about the Claimant, and no evidence in relation to other complaints had been disclosed to either the Claimant or the Tribunal. When this discrepancy was put to Ms Trumble she seemed unable or unwilling to understand the question, and when it was eventually explained to her, after intervention from the Tribunal, was still unable to provide a coherent response.”
“143. The Respondent relied on the judgment of Sam Trumble, in support of its argument that what the Claimant did was serious and justified the termination of his Bank contract, but as stated above the Tribunal does not accept that Sam Trumble was a credible witness in relation to this and finds that the information she gave the panel [Decision Making Group which decided on the bank ban] about the Claimant was misleading and was affected by his protected disclosures.”
The Tribunal also determined that the trust discriminated against Mr Thomson on grounds of disability:
“The Respondent subjected the Claimant to direct discrimination because of the protected characteristic of disability (s.13 Equality Act 2010) by terminating his Bank contract.”
“The Respondent subjected the Claimant to discrimination arising from disability under s.15 Equality Act 2010 by restricting the Claimant from undertaking Bank shifts in November 2023 and thereafter when the restriction was lifted continuing to restrict him from undertaking any shifts in the Respondent’s Emergency Department until the termination of his contract.”
The Tribunal noted that before being sacked from the bank, Mr Thomson clearly identified himself as a whistleblower. For example: “The fact that the Claimant considered himself to be a whistleblower is referred to expressly in the email.”
Mr Thomson also reportedly escalated his concerns to the Trust’s Chief People Officer: “On 16 July 2024 the Claimant emailed Emma Wood, an Executive Director of the Respondent. His email stated, “I am currently trying to raisegrievance and discrimination harassment and bullying and alsowhistleblowing against the Trust.”
As is standard in the NHS, the trust’s whistleblowing policy promises that no one who whistleblows will lose their job and that victimisation of whistleblowers is never tolerated.
Will the trust take any meaningful action in light of the Tribunal’s finding of whistleblower detriment?
Dr Minh Alexander retired consultant psychiatrist 9 April 2026
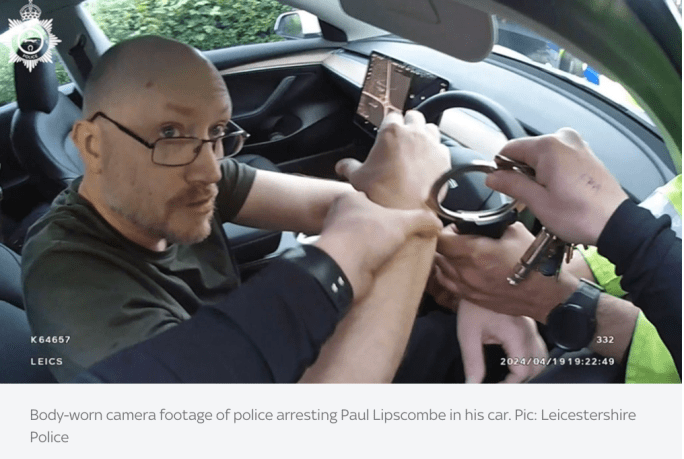
Paul Lipscombe former Associate Director of Performance and Informatics at University Hospitals of Coventry and Warwickshire NHS Trust (UHCW) was sentenced in November 2025 at Leicester Crown Court to over 28 years imprisonment for very serious sexual crimes against children, some violent.
He committed these crimes whilst employed by UHCW.
I examined the transcript of the sentencing proceedings and also requested FOIA data from the trust to better understand the trust’s governance of these matters.
Some troubling questions arose, such as why the trust delayed in reporting his arrest to the Care Quality Commission (CQC). There also appeared to be little attempt at organisational learning in response to his crimes:
Of note, UHCW explicitly claimed to me via FOIA that there was no evidence that Lipscombe had used trust systems in the furtherance of his crimes.
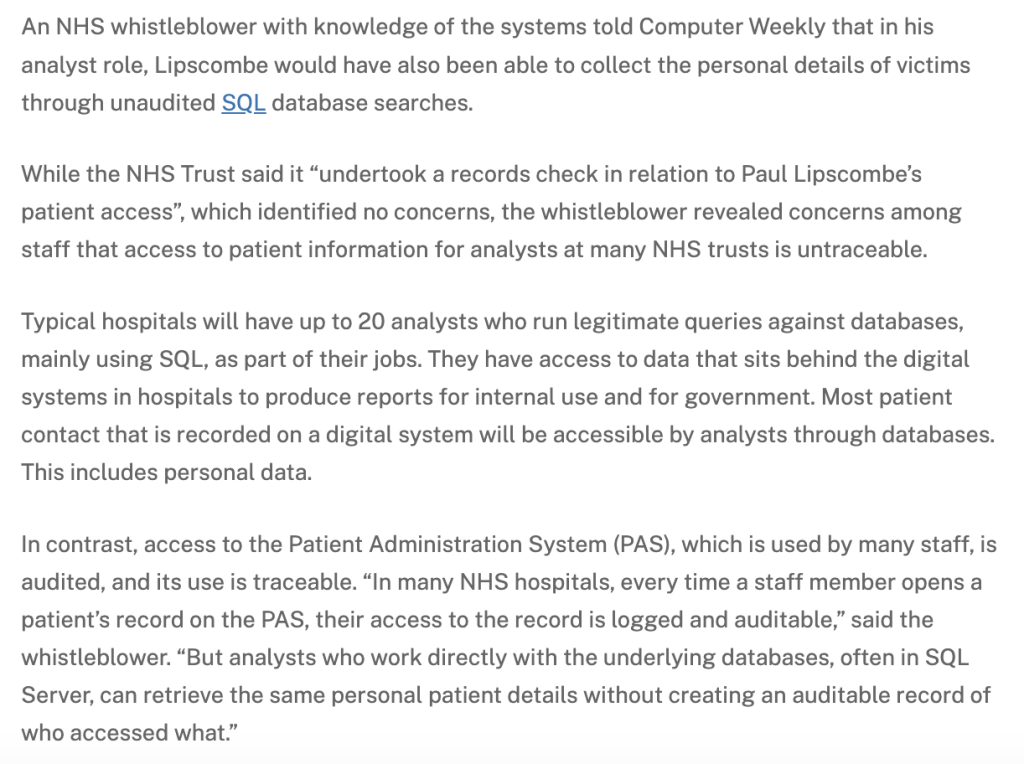
Since then, an NHS IT whistleblower has contacted the magazine Computer Weekly, well known for its long running work in exposing the Post Office Horizon computer scandal.
The NHS IT whistleblower told Computer Weekly that there are gaps in NHS IT governance which allow NHS analysts like Lipscombe to untraceably search for patient’s personal data, such as addresses. It seems therefore quite possible that Lipscombe could have used trust IT systems to identify and/or triangulate and locate his victims:
Of concern, UHCW reportedly failed to respond to Computer Weekly when asked for comment.
I have raised my concerns about trust governance with the CQC and also passed on the additional whistleblower intelligence as reported by Computer Weekly.
CQC says it has reviewed the matters at its FPPR (CQC Regulation 5 Fit and Proper Persons) committee and that it will raise these issues with the trust.
The FPPR process is unlikely to amount to any concrete action based on past history but at least there will be a degree of scrutiny, and it will be useful to see how the trust responds on the issue of IT traceability.
I have also asked UHCW directly via FOIA for a formal response about the issue of untraceable analyst access to patients’ personal data.
I have put it to the CQC that this unauditable activity appears to be a systemic safety issue that NHS system regulators should jointly address, and not just an issue for UHCW.
I note that NHS England gave a late and deflective response to Computer Weekly, which failed to address the issue of unaudited analyst access:
“An NHS England spokesperson said: “A patient’s full medical record can only be seen by healthcare professionalsdirectly involved in their care and there are strict controls and safeguards on how anyone else can access confidential patient information.
[my emphasis]
The insertion of the words “full medical record” adds another lawerly dimension of wriggle room.
These evasions by NHS England only serve to increase concern.
But NHSE does usefully also add:
“All trusts are required to meet the standards set out in the Data Security and Protection Toolkit, which include maintaining audit logs of access to information and putting in place controls to identify unauthorised access.”
By Dr Minh Alexander retired consultant psychiatrist 31 March 2026
This post provides an update on the NEAS scandal via the long awaited NMC hearing on two senior nurses accused of facilitating NEAS’ cover up of deaths.
Background
In 2022 North East Ambulance Service NHS Foundation Trust was exposed by whistleblowers as having covered up care failures by not passing relevant information to coroners.
It is surmised that the trust began doing this in 2019 in response to a period of sustained criticism after high profile care failures.
Staff protested and an investigation in 2020 into a small number of cases had confirmed that information had been wrongly withheld from coroners, but the trust withheld this from families.
But the problems continued and more than 90 cases were thought to be affected.
It is likely that the whole truth has not yet been revealed as arguably, a sufficiently independent and robust inquiry has not taken place.
Reviews were commissioned by the trust in 2020. An investigation was then commissioned by NHS England in 2022. The latter was led in 2023 by NHS insider Marianne Griffiths, former NHS trust CEO, whose own trust in Sussex has been mired in successive cover up scandals of whistleblower suppression and victimisation, unsafe surgical care with an ongoing police investigation and most recently a maternity care scandal.
NHS England’s terms of reference for the external investigation into NEAS severely limited the scope to only a small number of cases highlighted by the whistleblowers, instead of systematic investigation to fully identify all relevant breaches. It was felt to be a damage limitation exercise. Because of this Paul Calvert, the whistleblower who went public, declined to take part on principle.
Griffiths’ investigation spoke to only four affected families. The investigation refused to conclude that there was deliberate suppression by NEAS: “In some cases, the families believe that changes to reports and not sending original documentation to the Coroner was a deliberate act to avoid negative attention and accountability. We cannot say what the intent was of those individuals who authorised those changes or did not share information as we were not there”. [my emphasis]. This is an astonishing line of reasoning for investigators, who by that logic would never find any one culpable unless they had a signed confession.
The affected families have understandably had limited confidence in these investigations. But calls for a statutory, public inquiry were not heeded:
NEAS also persecuted the whistleblowers who raised the alarm, gagged one of them and also tried to gag the other but failed, and unlawfully required the whistleblowers not to pursue their public interest disclosures. Both were driven out of the organisation.
The trust also persisted in refusing to release some of the relevant documents into the public domain:
Two key trust managers involved in the trust’s process for managing information sent to coroners were senior nurses, Joanne Baxter and Shelley Dyson.
Joanne Baxter was NEAS’ then Chief Nurse and the Executive Director with primary responsibility for Quality and Safety, including the flow of information to coroners and trust whistleblowing governance. Shelley Dyson was NEAS’ Head of Quality and Patient Safety.
Both later moved on to other NHS trusts. Baxter became Chief Operating Officer at Gateshead Health NHS Foundation Trust and then retired. It is believed that Dyson remains employed by the NHS at Gateshead Health NHS Foundation Trust. According to various correspondence exchanged during several FOI requests on the What Do They Know website, her last known position at Gateshead was as Head of Risk and Patient Safety.
Baxter and Dyson were referred to the Nursing and Midwifery Council in May 2020 for alleged misconduct on grounds of bullying and improperly withholding information from the coroner.
There has been much delay in the NMC’s process and it has taken until this month for a hearing to be convened:
Shocking evidence was heard at the Fitness to Practice Tribunal about how evidence was reportedly withheld from coroners. Local media reported thus on the NMC hearing:
“A senior North East Ambulance Service (NEAS) boss has said that crucial information relating to patient deaths was “not disclosed” to coroners, as key legislation was challenged. Alan Gallagher, head of regulatory services at NEAS, spoke of “full evidence” including call logs and dispatch reports previously being withheld after deaths… The panel heard evidence from Mr Gallagher regarding a Rapid Process Improvement Workshop (RPIW) held in 2019, which centred around the coronial process.
According to a witness statement by Mr Gallagher, the meeting “quickly turned sour” as Ms Dyson began to question experts and suggested that legislation on what information is shared to coroners, including dispatch reports and call logs, be changed.
He said: “The experts were saying that we had a legal requirement to share relevant information with coroners that included information of staff involvement, and not to redact this was one of the points.
“At one stage, Ms Dyson stated that the legislation needed to change and stated that we should request changes to the law. Ms Dyson wasn’t happy with information being shared to the coroner.
“I had to explain that this was what was required by law.”
Mr Gallagher went on to discuss patient safety incidents, which he said were “not managed well” by the service and impacted what information was given to coroners.
He added that Ms Baxter had “very different views on NEAS processes”, and wanted to write a simpler, summary report to coroners instead of providing all details, saying NEAS had “changed processes” when it came to disclosure.
However, according to Mr Gallagher, this meant that full evidence on cases was not being given to coroners, and despite raising concerns, the ‘summaries’ were still sent.
He said: “We were not sharing full, relevant information with senior coroners.
“We were not disclosing full evidence to the coroner, which would result in the coroner not having full access to all relevant documentation and evidence to consider the case.”
This is a much more direct, alarming account of what happened than the guarded, hedged version given by NHSE’s Griffiths report. Baxter is not even named in Griffiths’ report. Upon searching, the phrase “Chief Nurse” appears only once.
The NMC Tribunal also heard evidence on alleged bullying at the trust:
As an additional caveat to NMC proceedings, Paul Calvert raises reservations about how Alan Gallagher reportedly responded to staff concerns about the problems at NEAS and the trust’s alteration of a report.
Moreover, he is concerned that Baxter and Dyson are convenient lightning rods to distract from what was a more widespread organisational failure, involving other senior NEAS staff who have escaped any consequences, some of whom remain in NHS posts.
The family of one of NEAS’ victims, 17 year old Quinn Beadle, were recognised participants in NMC’s process.
Quinn Beadle’s mother was devastated not only by the further delay in NMC’s proceedings, but by her general experience of the NMC process. She has posted publicly as follows:
“Tracey Beadle [27 March 2026]
Seven years.
Seven years of waiting.
Seven years of fighting to be heard.
Seven years of searching for answers about what happened to Quinn.
And now we’re being told there may still be no conclusion. The tribunal will pause and resume again in January 2027… more than eight years after Quinn’s death.
How is this justice?
Many of you will have seen the reporting in The Northern Echo and the Newcastle Chronicle about the toxic culture within the ambulance service. A culture where serious concerns have been raised again and again.
I was supposed to stand in London and give evidence in person at the @nursing and Midwifery Council hearing for 2 senior nurses.
I was ready to speak – not just for Quinn, but to give evidence against Baxter and Dyson, and to stand up for Andrew and Mr Coates too.
Two weeks before, it was moved online.
Then days before it began, I was told my evidence would only be read out.
My voice was taken away.
I was the only family member giving evidence. The only one.
And I wasn’t allowed to speak.
For 21 days, I have sat and listened, trying to follow complex evidence without even being given access to the documents being discussed. Listening to systems defend themselves while families are left on the outside.
This is not just about Quinn anymore.
This is about accountability.
This is about truth.
This is about Andrew, Mr Coates and all the families that don’t even know that their loved one died at the hands of @the north east ambulance service (They have blocked me from their page! How is that accountability)
How can there be accountability if key voices are silenced?
How can there be justice if families are pushed aside?
Seven years on, and we are still here. Still fighting. Still being denied answers.
It is completely unacceptable for the families’ suffering to be prolonged and exacerbated. In the context of all that has happened, the NMC should have ensured that there was no further postponement.
Does NMC’s postponement signify that the authorities realise that the cover up can no longer be denied?
What can we expect to happen during the postponement?
RELATED ITEMS
1) Death of Mr Peter Coates – an example of manipulation of evidence by NEAS
On 23 March 2026 Paul Appleton the coroner for Teesside and Hartlepool issued a Prevention of Future Deaths report on the death of one of the victims of the NEAS scandal, Peter Coates.
Mr Coates died of asphyxiation due to a combination of severe respiratory disease and a power cut at his home which meant that he was unable to access his usual oxygen treatment. He called 999 but there was a delay in an ambulance reaching Mr Coates because a nearby vehicle could not get through electrically controlled gates because of the power outage (and because the crew did not know of a manual override), and because another vehicle stopped to refuel despite having sufficient fuel in the tank.
Paul Calvert questions whether the crew in fact stopped for other reasons.
The coroner concluded that the ambulance delay may have been a contributory factor in Mr Coates’ death:
“Peter’s death was possibly contributed to by delays in the arrival of the ambulance crew to him.”
Originally, when the coroner first opened an investigation into Mr Coates’ death, NEAS did not fully disclose the circumstances of the death and excised facts from evidential documents, as reported by the Sunday Times:
“Although an investigation began the same day, the coroner was not made aware of this at the time, or of the fact that there had been any delay in getting help. Despite the mistakes and delays, a decision was made by bosses to downgrade the incident to “low harm”, on the basis that the primary reason for Coates’s death had been the oxygen equipment malfunction. The coroner, in fact, “should have been notified” straight away about the death and about the delays, the AuditOne investigation found. The NEAS internal investigation soon found that the second ambulance had in fact had sufficient fuel to complete the journey. This raised questions as to why the stop occurred. A statement made by one of the paramedics involved, explaining the decision to refuel, was never disclosed to the coroner. Instead, the paramedic was asked by bosses to produce a new statement, which made no reference to the decision to refuel. The coroner was “only supplied with the [later] statement, which does not include any reference to the refuelling”, AuditOne found.”
Unless a statutory public inquiry is held, we will never know how many other cases were subject to such manipulation of evidence and self-interested under-estimation of harm.
Dr Minh Alexander retired consultant psychiatrist 29 March 2026
Summary
There is a history of enculturated failure to carry out mental health observations and of falsification of records entries about observations at East London NHS Foundation Trust (ELFT). This is not unique to ELFT but there have been repeated, serious ELFT cases that have been criticised by inquest juries and coroners, which have been publicised. The trust’s reported governance response to these matters is examined here, and FOI material is provided. This includes a disclosed 2024 Human Factors review report commissioned by ELFT to shed light on how failures of observation arise. Supporting coroners’ concerns, the Human Factors review concluded that improvement measures by the trust did not fully address the issues of missed and falsified observations. Via FOIA, the trust reports that it has so far referred twelve staff to the Nursing and Midwifery Council in relation to the falsification of observations. Problems have persisted. As recently as May 2024, staff who were supposed to be conducting 1:1 observations were seated facing away from a patient, whilst using their personal mobile phone. The most recent coroner’s Prevention of Future Deaths warning about falsification of observation records was issued on 1 September 2025 and expressed concern about failure of the trust’s improvement initiatives. The trust countered with its own research evidence to demonstrate improved metrics and asserted that it had already done a “considerable amount of work”. It indicated that it was “reassured that no further action is required”. However, some questions and concerns remain. The Care Quality Commission is currently re-inspecting ELFT and has confirmed that it will take into account issues relevant to a recent coroners’ Prevention of Future Deaths report of 6 February 2026 which criticised ELFT’s serious incident process. In this case, an ELFT investigator had reportedly “neither sought the recollections of treating staff, nor communicated the findings of the report to the same staff”, raising additional concerns about the trust’s governance.
The full report and links to documents can be found here:
A coroner’s PFD warning of 5 March 2026 revealed serious failures in the mental health care of Nicholas Aina, who killed his mother and seriously injured his sister:
Another serious incident took place on ELFT premises on 28 February 2026, at the Tower Hamlets Centre for Mental Health, Mile End Hospital. A patient was attacked by another patient. The victim later died. Police announced on 6 March 2026 that a murder investigation had been opened.
ELFT’s comms over the years have perhaps been glossier than the actuality.
The latest trust Director of Comms was appointed late last year and has previously held central government and parliamentary posts. It remains to be seen how trust PR rolls henceforth.