Dr Minh Alexander retired consultant psychiatrist 27 February 2026
This is a post to share a BBC item from yesterday.
Amanda Ford is a senior nurse and midwife who had a distinguished and unblemished career dating back to the days of pre-CQC, rigorous NHS regulation.
HSIB were lucky to recruit her as an investigator in their maternity programme, where she worked from 2019. Her experience and skills soon told as she identified care quality and governance failings in maternity services at Yeovil Hospital. But she then also became troubled by HSIB’s responses to her concerns.
She was not alone as other HSIB staff also had concerns about HSIB’s maternity investigations and they experienced problems raising concerns, as was revealed by internal and external reviews. Multiple, unnamed HSIB staff whistleblew to the media previously, but the significantly critical reports remained suppressed from public view. It required a later FOI process to release the reports.
Amanda eventually quit HSIB and lodged an Employment Tribunal claim for constructive dismissal in which she represented herself as a litigant in person, against the full resources of the NHS. This litigation did not succeed, but internal NHS processes upheld most of her grievances and recognised that she should have been treated as a whistleblower, which she clearly was.
Her concerns are sadly fully vindicated as years later, Yeovil Hospital is now one of the sites under a national investigation for maternity failings:
The timeline of events at Yeovil illustrates how valuable whistleblower intelligence is, if only the NHS has the maturity to respond to it constructively, to prevent unnecessary harm and suffering to patients and their families.
BBC Points West has now covered these issues. Health Correspondent Matthew Hill interviewed Amanda Ford for a broadcast yesterday. Amanda has also received an apology from the trust if not from her former employer.
These are some of the key passages from the BBC interview:
MH: “……She [AF] told me that if she been listened to properly then this service may well have closed and harm to other babies may have been prevented
AF: “…Within a month I just was appalled. There was a baby death. That’s a death that shouldn’t have occurred….And there was a lady who was put through labour…she’s lucky to have survived that and her baby survived…it was just appalling care”
MH: “…The hospital didn’t always want to hear what she had to say…”.
AF: “…there wasn’t enough consultant oversight or consultant ward rounds…not enough escalation…locums that didn’t seem to be orientated or supervised …didn’t seem to be prepared for emergencies or things going wrong…in obstetrics and maternity, things go rapidly wrong…a feeling of defensiveness to the concerns that I was raising”
MH: “…Amanda says she tried to feed back the problems she saw at Yeovil but felt the hospital and HSIB were too close.”
MH: “…..Do you think HSIB is fit for purpose?”
AF: “No I don’t. I don’t think they got it. And if that was happening in Yeovil, where else was it happening in the country?”
MH: “So she left HSIB feeling it wasn’t challenging the trust enough. She lost her case for constructive dismissal at an Employment Tribunal but did win most of her grievances in HSIB’s internal process. An independent report found she should have been treated as an HSIB whistleblower.”
AF: “It validated the fact that I was whistleblowing…also this piece was about the culture within HSIB. There was also a bullying culture”
MH: “How did that leave you?”
AF: “Destroyed”
MH: “Had you been listened to, would the unit still be open today, functioning safely?”
AF: “There would have had to have been a process where CQC would have gone in sooner. And HSIB would have escalated sooner.”
MH: “The Healthcare Safety Investigation Branch no longer exists. Its successors declined to comment. Yeovil said they strive to have an open and safe culture and acknowledge they didn’t always get this right.”
AF: “I ended up very unwell because of what I’d been put through, from not being listened to, and that moral injury as many NHS whistleblowers will realise… for doing my job and being honest.”
BBC Points West: “It must have been so hard for Amanda to speak out”
MH: “Yes, I was first in touch with Amanda a year ago, but it took her several months to decide to speak out because she was worried about the potential consequences of doing that. Now given her experience of not being listened to, and then resigning as a result, it’s a shame her former employer didn’t want to comment. But remarkably the hospital here has put up its hands and said “sorry””
Apology by Dr Melanie Iles, Chief Medical Officer since April 2024, on behalf of Somerset NHS Foundation Trust:
“I’m really sorry that Amanda wasn’t listened to and that she’s been put in this difficult situation. I’m passionate that for really high quality care we need to be listening to women, we need to be listening to our staff and acting on what we’re hearing. And I’m really sorry that on occasions that hasn’t happened, and those actions haven’t been taken or quickly enough.”
The BBC has also published an article touching on Amanda’s story:
These are previous posts relevant to HSIB’s serious failures of maternity investigation, NHS England’s cover ups and the arising investigations into these matters and Amanda Ford’s case, and a related item about previous HSIB leadership by Keith Conradi who was parachuted into the NHS from the Air Accidents Investigation Branch (AAIB):
By Dr Minh Alexander retired consultant psychiatrist 24 February 2026
Valdo Calocane was discharged after missing appointments
The statutory inquiry hearings into the attacks by Valdo Calocane, psychiatric patient, against the public in Nottingham opened on Monday 23 February 2026.
Counsel to the Inquiry set out the areas of concern.
Agonisingly, Valdo Calocane’s loss to follow up was recounted. He was discharged from specialist mental health services in September 2022 after missing appointments and after an outreach visit was mooted but did not take place. Compounding this, there was reportedly minimal information and guidance given to primary care upon discharge. There was no further contact with health services until the attacks in June 2023.
This situation of discharge because of disengagement from mental health services is more common than it should be.
Disengagement is a precursor to suicide and homicide, but trusts vary in their approach to discharge
Patients with severe mental illness (SMI) have been poorly served in that high intensity, specialist services that are proven necessary for flexible and proactive support, were scrapped or watered down.
Generic teams cannot offer the same level of care and may struggle with patients whom they experience as “challenging”, because they are not equipped to deal with their complex needs.
In particular, when generic teams are over-burdened, de-sensitised and/or poorly managed and supervised, patients may bear the brunt in terms of therapeutic rejection, premature discharges and failures to outreach or to appropriately mitigate risk.
And thus patients may be abandoned when they are chaotic due to relapse, and are at their most vulnerable, and when some also pose greater risk to others.
Disengagement by severely mentally ill patients should trigger concern, investigation and outreach, not discharge. The National Confidential Inquiry advises:
“Non-receipt of planned care is a crucial precursor of patient suicide. Services should place priority on follow-up efforts for patients losing contact with services or who are non-adherent with medication. These patients have multiple clinical and social problems that are likely to add to risk and that need to be addressed in their care plan. Involvement of the patient’s family or carers should form part of engagement efforts.” Annual report 2025
Disengagement is similarly a precursor to homicides:
“65 (32%) patients with schizophrenia were non-adherent with drug treatment in the month before the homicide, an average of 6 per year. There had been no fall since 2008. 75 (39%) patients with schizophrenia missed their final service contact before the homicide, an average of 7 per year, and again there had been no fall since 2008. In total 116 (59%) were either non-adherent or missed their final contact with services. There was a fall overall in this group over the report period.” Annual report 2017
A glance at NHS mental health trust discharge policies in the public domain shows a range of approaches. Most contain an element of risk management when dealing with non-attendance/ disengagement. But there are differences in tone and emphasis on caution and urgency of response to a possibly deteriorating patient.
The independent homicide investigation commissioned by NHS England into Valdo Calocane’s case concluded that Nottingamshire Healthcare’s discharge processes were not sufficiently robust and that staff in any case failed to involve his family as required by trust policy.
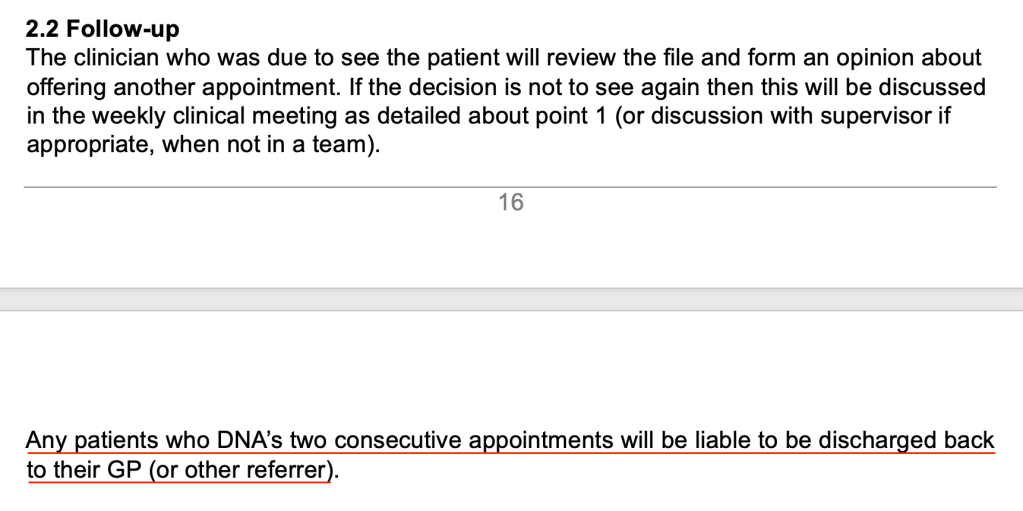
Some trusts’ discharge/ non-attendance policies are overly complex and sometimes downright confusing. For example, one policy contains a rigid “two strikes and out” clause whilst also featuring a plethora of caveats scattered in different places in the policy:
At the end of the day, policies and flow charts cannot compensate for insufficient clinical training and experience, in the context of cost-cutting and downskilled services.
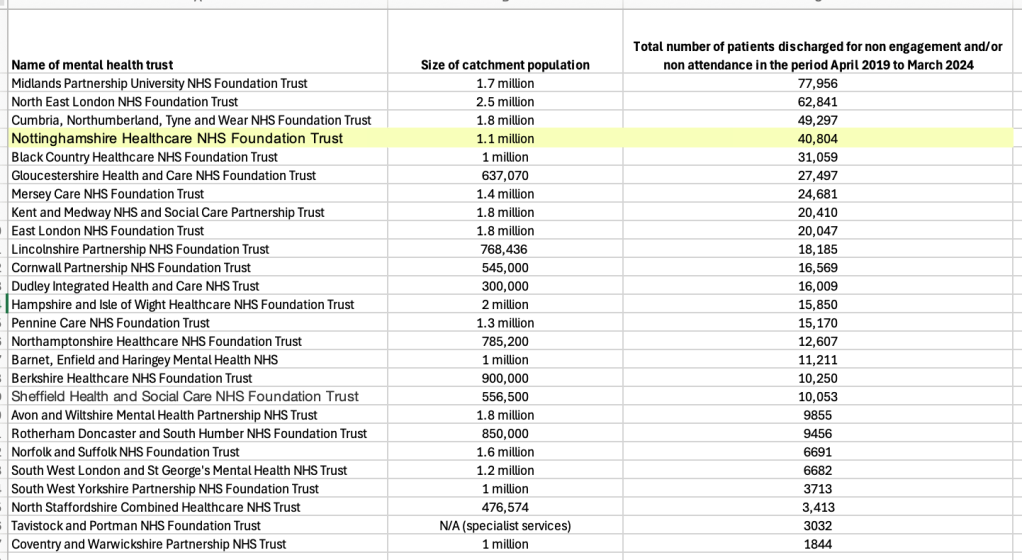
This revealed patterns of discharge due to non-attendance and non-engagement by patients. The data is incomplete for various reasons, including the fact that some trusts claimed that they did not routinely collect this data.
But of 26 mental health trusts that provided data for the five year period 2019-2024, there was quite a range in the number of patients discharged for non-attendance/non-engagement. The trusts vary in their range of services and comparison is rough.
According to this FOI data, Nottinghamshire Healthcare NHS Foundation Trust was at the higher end of the spectrum.
In total, the 26 trusts discharged 525,182 patients over the five year period for not attending/ not engaging.
And one trust pointed out that some patients may be discharged more than once in any given period, so the number of episodes of discharge may be slightly higher than the total number of patients discharged.
For completeness, I have loaded the more detailed results by year onto a spreadsheet. This also gives a list of the trusts which claimed not to collect data on discharges for disengagement.
Questions arise about the appropriateness of the many thousands of discharges for disengagement, and how well risk is managed and needs are met during such discharges.
Realistically, how often are such discharges clinically audited for safety, in our super-stressed NHS?
And what might the disengagement data say about the suitability of services provided?
All NHS mental health services operate under great pressure, including severe bed pressure after savage bed cuts. There is always potential for something to go badly wrong, and it is important to acknowledge that Nottinghamshire Healthcare NHSFT is not an isolated example.
One only has to glance at the immaculately maintained database of mental health homicides by the charity HundredFamilies to see that risk remains widespread and ongoing.
The issue is what will be done, if anything, to change this.
RELATED ITEMS
1) This is the independent homicide report commissioned from Theemis Consulting Ltd by NHS England into the attacks by Valdo Calocane:
This concluded that discharge due to disengagement had become “normalised”:
“Based on interviews with Trust staff and from the evidence reviewed by the independent investigation, VC’s discharge due to disengagement does not appear to have been an isolated event. Pressures on the service and a lack of oversight to understand whether the service was being delivered as intended, or whether ‘as intended’ is possible within the constraints of resources, meant that this practice had become normalised and accepted within the team.”
Theemis made this important finding about the provision of Assertive Outreach Services in NHS mental health trusts:
“Finding
NHS England’s recent review and guidance indicates that assertive outreach should be a discrete resource but recognises while some ICBs may already commission ‘assertive outreach’ teams or similar, others may not currently commission a specific team or service focused on intensive and assertive approaches. This aligns with the information and evidence provided to the independent investigation that suggested the majority of dedicated assertive outreach teams as a standalone function, were disbanded over 10 years ago. Alternative models for supporting service users who do not choose to or are unable to engage with mental health services have developed but there is variation in the approach, dedicated protected resources and in outcomes for patients. VC’s clinical records and interviews with community Trust staff do, to an extent, demonstrate an element of an assertive approach. However, this was constrained by the service model and workload within the team.”
2) After the Nottingham attacks, NHS England back tracked on the dangerous dismantling of specialist assertive outreach services and directed ICBs to review their provision. The reviews have been submitted to NHSE. What happens next is the question.
The failings that it described have been repeated over the years.
The Inquiry observed that care was inversely proportional to deterioration in Christopher Clunis’ mental state, and that this was a pattern that the panel had noted over the years:
The question is how much longer society tolerates these failures, and prioritises the changes that are needed to protect the public, and also to protect patients from catastrophic deterioration that changes their lives and prognosis indelibly.
My condolences to all the affected families and surviving victims.
“This Inquiry is not only about Barney, Grace and Ian, but it is also about Jonathan Zito (who died at the hands of the Christopher Clunis; about which killing, Jean Ritchie concluded her report in 1994)’ and each of the countless other unnecessarily bereaved, whose loved ones were lost to the unmanaged risk of people who were known to be ill and known to be a risk to public safety.”
The Department of Health made its opening submission at the Nottingham Inquiry yesterday and its written submission has been published here.
The Department acknowledged there was a failure to manage disengagement, emphasised the need for continuity of care at several points and touched somewhat ambiguously on the issue of resources, citing a need for resources but also claiming that it has made investments.
“43.Valdo Calocane was discharged from services and at times it appeared that he may have been non-compliant with medication and was reluctant to engage with mental health services, such as in September 2022 (WITNO084001). The Department recognises that non-engagement is a recurring problem. Those with severe mental illness often live with these illnesses for their whole lives, and the support of the health services needs to reflect this in the services provided and in being able to go back into the system efficiently and quickly should deterioration occur. As a result of the lack of information sharing and the absence of access to information, professionals did not monitor Valdo Calocane’s mental health deterioration over time. This led to, for example, a failure to actively manage Valdo Calocane in transfer between the community mental health team and his GP (WITN0084001). There should have been resources to carry out this exercise. Failing to engage with services, not turning up to appointments, not answering messages, are not often in this group of patients a sign of health or a conscious decision, but a sign of mental ill health and a lack of insight into how unwell they are. Help is needed for this group even if it is difficult to deliver and requires persistence, patience, and perseverance.”
By Dr Minh Alexander retired consultant psychiatrist 18 February 2026
This is a very brief note for anyone interested in the ever-deepening crisis affecting highly vulnerable patients and their families, who are forced to rely on one of the largest providers of private secure mental healthcare purchased by the NHS.
It is clear that St. Andrew’s Healthcare’s governance has been deplorable, and combined with ineffective regulation, this has allowed systemically abusive practices to flourish. It all now culminates in a substantial police investigation that has led to arrests for alleged wilful neglect and ill-treatment, assault, rape, and manslaughter.
Some of the incidents which have led to these arrests were captured on CCTV.
Many, many questions arise about why staff felt comfortable to abuse patients on camera.
Much of what went wrong is still hidden, and sadly I think much will remain secret and hidden.
But examining three coroners’ warning reports published in 2023 on St. Andrews Healthcare facilities shows some of the neglectful practices. These reports are only issued exceptionally when there are serious risks:
Jason Bayley died of constipation, a known side effect of his psychiatric medication. He is not the first St Andrew’s patient to have died in these circumstances. An alarm was raised years ago by the Healthwatch Chair with NHS England’s CEO after four St. Andrews patients died in similar circumstances and NHSE seemed reluctant to act robustly. St Andrews was, and still is, a powerful and well-connected institution, based in a county with reportedly the highest concentration of landed gentry. The fact that two of these previous deaths were not subject to inquest, that one was ruled a natural death and failure by the Care Quality Commission to investigate all raised eyebrows: Call for inquiry into deaths of four men at psychiatric hospital. The failure by St. Andrews to learn and the horrendous repetition in the death of Jason Bayley speaks volumes, but responsibility must surely be shared by the regulators.
Sasha Mishabi died with skin ulcers after a total failure to follow any sort of protocol for managing his high risk of pressure sores. No Datix incident report was submitted when ulcers developed, arguably a preventable failure of care in most cases. No serious incident investigation was undertaken when Sasha died. Staff claimed they “forgot” that there was a pressure sore policy:
“At inquest it was identified that [REDACTED] had forgotten that there was such a policy (he initially denied there was a policy/procedure for waterlow assessments and later, after the policy had been produced, said there was but he had forgotten about it).”
Steven Sanders It was thought from other patients’ reports and discovery of cocaine on the unit after his death that Steven may have smuggled an illicit drug onto the secure ward after leave, and that drug use may have been a factor in his death. Subsequent police investigation revealed several positive drug tests on the unit. There was also an unexplained death of another patient. The coroner was concerned about “endemic” illicit drug use and lack of mitigation by St Andrews Healthcare.
All three PFD reports relate to detained patients, making these failures all the more egregious, as the duty of care is even greater. Condolences to their families.
Declaration of interest:
I was a St. Andrews whistleblower.
RELATED ITEMS
On the regulatory revolving door….
Laingbuisson reported in October 2018 that a CQC manager joined the St Andrews Healthcare management team, having worked at the CQC overseeing regulation of St Andrews Healthcare:
Were there any other regulatory staff who joined St Andrews Healthcare?
I have collated PFDs on private mental healthcare providers whose services are purchased by the NHS, found upon search of the chief coroner’s database, into an Excel spreadsheet for anyone who might find it useful. There are some explanatory notes at the beginning.
Amongst these PFDs is an example of another death by constipation/bowel obstruction due to medication side effects. This occurred at the Priory Cheadle, where Wayne Millet died aged only 46:
I found a total of twenty two PFDs on Priory Group facilities, nine of which were in the Manchester or Greater Manchester area, at Priory Altrincham and Priory Cheadle.
By Dr Minh Alexander retired consultant psychiatrist 11 February 2026
SUMMARY
Paul Lipscombe an Associate Director at University Hospitals Coventry and Warwickshire NHS Trust was sentenced on 11 November 2025 to over twenty eight years in prison for extremely serious and sometimes violent sexual offending against female children. He was also sentenced for making and distributing indecent images. A transcript of the sentencing hearing shows that Lipscombe reportedly took “very high risks” in offending, sometimes even whilst taking work conference calls. By Lipscombe’s own report, he had been offending against young girls since his twenties. Sentencing Judge Raynor concluded that Lipscombe was “very highly dangerous”. FOI data shows the trust provided the police with information, but there is otherwise no evidence of meaningful NHS effort, by the trust or the regulator Care Quality Commission, to ensure safe, appropriate learning from these events. There was an alleged agreement, between the trust and the local CQC relationship manager, that Lipscombe’s initial arrest in April 2024 for suspected kidnap of a missing fifteen year old girl was not even a reportable incident. CQC published a brief Well Led inspection report in August 2025, shortly after the trust learnt Lipscombe had pleaded guilty to further offences. CQC concluded that UHCW was “Good” on the Well Led domain. The authors of this report are not disclosed.
INTRODUCTION
Paul Lipscombe was an Associate Director of Performance and Informatics at University Hospitals Coventry and Warwick NHS Trust who was sentenced on 11 November 2025 to over twenty-eight years in jail for a series of extremely serious, calculated sexual offences, including rapes, against female children aged twelve to fifteen. He was also convicted of making and distributing indecent images of children being abused, which related to an online side business that also sold advice to other/would-be sex offenders. The case was widely reported:
Reflecting the seriousness of his offending, Lipscombe’s sentence consists of a three year sentence which is to run consecutively with a twenty five year sentence. He is not eligible to apply for parole until two thirds of the twenty five year sentence has been served. He was 51 at the time of sentencing and so at the earliest will not be on licence until 70.
To put Lipscombe’s heavy sentence in context, the average sentence for child sex abuse between 2015 to 2019 was three years and four months. In 2019, only 124 people received sentences of more than twenty years (across all offence types), barring life sentences. In 2021, the Prison Reform Trust reported that there were a total of only 894 people across the prison estate who were serving determinate sentences of 20 years or longer.
Lipscombe was given an Extended sentence under section 280 of the Sentencing Act 2020, relating to rape of a child under age 13. In 2024, only 1200 people received extended sentences.
The police described Lipscombe’s crimes as “horrendous” and indicated that they were some of the most serious sex offences they had handled.
A summary of the police investigation and a helpful list of the specific offences can be found here.
Lipscombe’s case clearly raised issues of NHS managerial Fit and Proper Persons.
His former employing trust released a deflective statement, which emphasised that Lipscombe had an “administrative” and not a “patient facing” role.
UHCW also claimed to have carried out its “own internal review” and that “nothing has been identified at this stage to indicate this individual’s criminal activity was committed as part of their role”.
[UHCW] “Statement in relation to the sentencing of former employee, Paul Lipscombe 11 November 2025 We would like to praise the girls and their families, as well as Leicestershire Police, for their bravery and courage in bringing Paul Lipscombe to justice for his horrendous crimes. Following Lipscombe’s arrest in April 2024, we immediately suspended him before dismissing him from his administrative, non-patient facing role in June 2024. The Trust has and will continue to support Leicestershire Police with its investigations and has carried out its own internal review – nothing has been identified at this stage to indicate this individual’s criminal activity was committed as part of their role. For anyone who would like to report information or possible offences committed by Lipscombe, visit: public portal. You can also call Leicestershire Police on 101. In an emergency always call 999. For more information around spotting the signs of grooming and where to get further support, visit: https://www.leics.police.uk/advice/advice-and-information/gr/grooming/
JUDGE’S SENTENCING REMARKS
In an attempt to get a better sense of the case details, and especially the length of offending and potential relevance of Lipscombe’s offending to his NHS employment, I asked the Court for a transcript of the sentencing remarks.
Because of the extremely unpleasant material about Lipscombe’s offending therein, I am not posting the transcript.
I instead summarise and provide the most salient excerpts for the purposes of this post.
But the whole document is available as verification, if required.
It is clear from the sentencing hearing that Lipscombe was an entirely unsuitable person to be responsible for healthcare services, responsible for vulnerable people and/or people at vulnerable times in their lives, or responsible for overseeing staff and their welfare.
His offending was cold, intentionally degrading, manipulative and at times coercive and violent. At times he hurt his victims, and said that he intended to do so.
The Probation Officer who prepared the pre-sentence report concluded that the offences were planned and featured pre-meditation.
Lipscombe was controlling of victims and he engineered damaging attachments with victims to facilitate the sexual offences.
The defence attributed these attachments in part to victims’ pre-existing vulnerabilities:
“He developed, with a very small “r”, relationships with the girls, and it is right and fair to say that the girls, because of the level of grooming, and because of their vulnerabilities, believed at the relevant time that they were in such relationships with him.”
Another view is that offenders target the vulnerable.
In return for payment, Lipscombe also tutored other predators in his grooming methods. The minutely calculated nature of his grooming and manipulation of children is vividly illustrated in these communications.
The tone in these communications is one of pride and satisfaction in his achievements, by his own lights. In one communication, Lipscombe stated that the information he was selling was worth far more than the fee charged. In Lipscombe’s comments, victims are objectified, their feelings considered in so far as manipulation was a means to facilitating offending.
Victims’ privacy was violated by Lipscombe’s secret recordings, and the Court noted from the Probation pre-sentence report that images may still be circulating on the internet:
“…in some instances they were secretly recorded, thus violating privacy, and any images shared online may remain there permanently, and not be totally removed.”
Lipscombe was married and the Court noted that he also misled his wife, telling her that he was away on work trips when he was pursuing victims:
“…you lived in a nice house with your wife, and were proud of your wealth and the Tesla car parked up on your drive. You told your wive [sic], for instance, that you were going on business trips to London, but in truth you were travelling to engage in your obsession, namely sexually abusing young girls.”
According to the media, the prosecution also held that Lipscombe tried to blame others:
At sentencing, Judge Keith Raynor praised the thoroughness of the pre-sentence Probation report, which noted that even when on remand, Lipscombe wrote sexualised stories, which echoed elements of his own offending. He handed these stories to prison educational staff. Judge Raynor concluded from this behaviour that the sexual offending was “engrained” in Lipscombe.
Judge Raynor noted inconsistent expressions of remorse and that the pre-sentence Probation report had described victim-blaming by Lipscombe.
“When we deal with the question of remorse, he has expressed some remorse to a psychiatrist. To the pre-sentence report author he has victim blamed, and he has said that these offences in part occurred because the victims were promiscuous. That is not indicative, it seems to me, of anyone with genuine remorse.”
At the conclusion of proceedings, Judge Raynor noted a letter of apology by Lipscombe and decided: “In the circumstances I have decided to give him a morsel in respect of remorse.”
It is notable that Lipscombe’s defence barrister cited his NHS service as a factor in mitigation.
“So far as these matters are concerned, your Honour is dealing with a 51-year-old man. He has no criminal convictions before this date. He was also an award winning employee at the National Health Service because of the work he had done, particularly during covid, in reducing waiting times for patients, and in improving the computer systems, those are facts.
He did live, aside from this awful part of him, a good and decent life, and was a useful member of society. He did all of that whilst having ADHD and autism, and he continued to work.”
The defence also pointed to reported psychiatric factors of ADHD and “autism”. However, Lipscombe’s behaviours suggest high social functioning that may not be entirely consistent with the latter.
Judge Raynor noted that the pre-sentence Probation report described “sophisticated predatory behaviour”.
Indeed, the sentencing hearing also revealed that Lipscombe had obtained a position of responsibility and sensitivity in custody as a “Listener”, about which the reporting Probation officer had expressed some concern. Listeners in theory act as confidential emotional supports to other prisoners, who may be in crisis and or suicidal, and therefore a level of social function is needed.
In weighing the case at sentencing, Judge Raynor identified the following aggravating factors:
“manipulation”
“deviousness”
“controlling and obsessive behaviour”
“committing offences in a victim’s home”
“Telling L it had to be a secret”
“The distances you travelled to engage in your sexual activity”
“The fact that there was ejaculation”
“The spy camera 54-minute video”
“The upskirting”
“The grooming”
“The snapping of the Sim and the factory reset with S”
“The disparity of age”
“On occasions force being used”
“child known to the offender”
“severe psychological harm”
“Additional degradation, humiliation”
“Violence or threats of violence”
“Forced uninvited entry into a victim’s home”
“a child being particularly vulnerable due to personal circumstances”
“moving images”
“active involvement in a network which facilitates the sharing of images”
“profiting from the distribution”
Judge Raynor concluded that Lipscombe was “very highly dangerous”:
“The dangerousness of you, it shouts out from the evidence in this case, it then becomes utterly compounded by the contents of the pre-sentence report, and I have a firm view that you are very highly dangerous”
Importantly, Judge Raynor also noted that Lipscombe took “very high risks” in his offending:
“You were bold in your offending, and you took very high risks, which I am sure made things more exciting for you. You committed offences in your own home, at the same time as working from home and taking conference calls. You also sexually assaulted one victim in her own house.”
This raises questions about the degree to which there may have been signs during Lipscombe’s offending that others could have acted upon, to help stop him.
Also very importantly, during the preparation of the pre-sentence Probation report, Lipscombe reportedly disclosed that he had been offending against girls since he was in his twenties:
“…he has been committing sexual offending against young girls since he was in his 20s”
That is to say, it is possible that Lipscombe was offending through much or all of his NHS career.
This Probation evidence was supported by online chat data recovered by the police, in which Lipscombe informed another male of very longstanding sexual urges towards children.
It is of course possible that Lipscombe was so skilful in his deceptions that he functioned “normally” at work, at a superficial level, and that the NHS cannot be fairly criticised for not detecting any abnormality or risk to others.
And it is of course easy to criticise in hindsight.
But after such a catastrophe, it would be good practice to reflect and ensure organisational learning where relevant.
Moreover, systems weaknesses may be spotted upon review, even when there have not been failings.
UNIVERSITY HOSPITALS OF COVENTRY AND WARWICKSHIRE NHS FOUNDATION TRUST’S RESPONSE
I asked the trust about its internal response to Lipscombe’s case. Two FOI requests, and a note to the trust informing it that I had made referral to the ICO, were needed to elicit reasonable information. The trust appeared reluctant to answer supplementary questions which probed further, and it delayed in responding to the second FOI request.
It appears that despite the trust’s claim that it undertook “an internal review”, there was no meaningful learning exercise.
The trust admitted that it only checked devices and for evidence of any inappropriate access to patient information by Lipscombe as part of the police investigation.
“In liaison with the police, the Trust reviewed whether there was any evidence that PL had used any Trust devices to make contact with children and whether there was any inappropriate material on any of his Trust devices. The Trust also reviewed whether there was any evidence that PL had made any inappropriate access to patient information as part of his non patient contact role.”
There was no evidence that the trust fully considered its governance, human resources practice, possible failures to spot signs of a serious offender or the impact on colleagues of working with Lipscombe. In particular, the experience of female subordinates would have been important to review, one would have thought.
Moreover, the directors in charge of the trust’s response to the police were the Chief People Officer (Donna Griffiths) and Director of Performance & Informatics (Dan Hayes), who both arguably had conflicts of interest in the matter. This is because Lipscombe was an associate director in Performance and Informatics and his offending also raised questions about trust HR practice.
“The review was undertaken by the Director of Performance & Informatics, Director of ICT & Digital and Director of Workforce reporting to the Chief People Officer on behalf of the Trust Board”
In its first FOI response to me, the trust answered misleadingly when asked if it had checked processes for ensuring the fitness of its managers, especially directors, and whether there were Safeguarding issues arising from Lipscombe’s employment at the trust. It replied:
“There was no failings identified as part of the support to the criminal investigation or in relation to Trust processes”
when the scope of the trust’s actual response could not have answered or fully answered either of these questions.
The trust was more careful when asked if there has been evidence of other employees acting in concert with Lipscombe, and gave the following reply:
“As confirmed in our press statement we supported and continue to support the police in their criminal investigation. No concerns have been reported to the Trust and we continue to support their investigation.”
UHCW admitted that there had been three other cases in the last five years of alleged sexual offending by other trust employees, but maintained these were unrelated to the Lipscombe case.
UCWH revealed that it did not formally inform the regulator the Care Quality Commission (CQC) of Lipscombe’s arrest in April 2024, and only informed CQC about Lipscombe in August 2025.
On further questioning, UHCW claimed that the initial arrest in April 2024 did not trigger CQC reporting requirements and that the local CQC relationship manager agreed with this view:
“On 23rd April 2024, the Trust was informed that PL had been arrested for a serious criminal charge involving one person. The Trust made an initial assessment that the CQC would not need to be informed. A verbal conversation with the CQC relationship manager confirmed that the incident did not trigger Regulation 18.”
See here for information on CQC Regulation 18, which relates to staffing requirements. It is arguable that other CQC regulations were also relevant.
Interestingly though, UHCW indicated that it informed NHS England of events in June 2024, so there was recognition that Lipscombe’s arrest was a significant matter.
“The Trust also informed NHSE of this matter on 5th June 2024.”
I fail to see how the arrest of a senior NHS manager on a “serious criminal charge” (the trust’s words) is not reportable to the CQC and should not trigger a review of Fit and Proper Persons CQC Regulation 5 or other potentially relevant CQC Regulations, regardless of whether the offending is against one person or several people. The original arrest in April 2024 was for suspected kidnapping of a missing fifteen year old girl. If neither UHCW and CQC consider this a reportable matter, what hope is there? Moreover, after the police found the missing girl with Lipscombe and took her to a place of safety, she reportedly disclosed that he had raped her. Were UHCW and the CQC were aware of this?
The events above, as reported by UHCW, raise not only questions about the trust but also about the local CQC relationship manager.
The trust claims it was notified on 6 August 2025 that Lipscombe pleaded guilty to additional charges, and at that point it formally reported to CQC:
“On 6th August 2025, the Trust was informed that PL’s court case was due to commence in late August 2025 and that PL had pleaded guilty to further criminal charges. The CQC were formally notified on 6 August 2025.”
For accuracy, the police summary states that Lipscombe in fact pleaded guilty to the 34 offences in February 2025.
It is notable that only nine days after formal notification by UHCW of Lipscombe’s guilty plea to additional charges, the CQC conducted a Well Led assessment of UHCW on 15 August 2025. CQC somewhat dubiously concluded that the trust merited a rating of “Good”.
There is no indication by CQC in its report of why a Well Led assessment was triggered, and no reference to the fact that a senior trust employee was being prosecuted for multiple serious offences, or to the trust’s governance response to this. CQC concluded that the trust was compliant with the Fit and Proper Persons’s requirements. “The trust followed the NHS England guidance for ensuring those persons who met the criteria in Regulation 5 of the Health and Social Care Act 2008 (Regulated Activities) Regulations 2014 were fit and proper to carry out their roles.” This relates mainly to administrative processes.
The report of the CQC inspection was brief and directly published on CQC’s UHCW webpage, without details of the inspection team who had conducted the inspection. Was it led by the same CQC relationship manager who had failed to act when informed of Lipscombe’s arrest in 2024?
It is remarkable that there was silence about major criminality by a senior trust manager when CQC knew by that point that Lipscombe had pleaded guilty to so many serious offences. It is, as the police said, a horrendous case.
I will raise these various matters with CQC.
So, as Lipscombe embarks on his long prison sentence and drifts from public view, the NHS waters close over with barely a ripple.
It may be that there would not have been a great deal to learn, had a properly accountable and diligent learning process been launched.
But we will probably never know, will we?
RELATED ITEMS
Not many may be aware, but Carl Beech the notorious sex offender and source of bizarre, malicious allegations about a VIP sex ring was, incredibly, a CQC inspector.
He was imprisoned for his crimes in 2019, having been sentenced to eighteen years in prison, but released early last week.
The victims of his malicious allegations were reportedly given no warning of this.
The CQC informed me that it reviewed potential risks that Beech posed in his duties as a CQC inspector:
“…we have reviewed all records to identify any risks from the inspections and CQC activities that he was involved in and we have no information of concern about his conduct on any inspection. All of the providers have been notified of his involvement in the inspection of their services.”
Perhaps CQC should have applied similar expectations to UHCW’s response to Lipscombe’s offending.
Lipscombe’s victims’ and victims’ families’ statements published by Leicestershire police can be found here. Some of the victim impact evidence was also discussed towards the end of the sentencing hearing. Serious psychiatric injury and ongoing suffering, unsurprisingly, were reported.
CQC has advised that it will review FPPR issues at UHCW. Also, an NHS IT whistleblower has revealed to Computer Weekly magazine that analysts like Paul Lipscombe have untraceable access to NHS patients’ personal data. This could have been used to facilitate his crimes. NHSE has given deflective responses when asked to comment. UHCW has failed to respond at all. An update summary is provided here:
By Dr Minh Alexander retired consultant psychiatrist 31 January 2026
This is a brief update for whistleblowers.
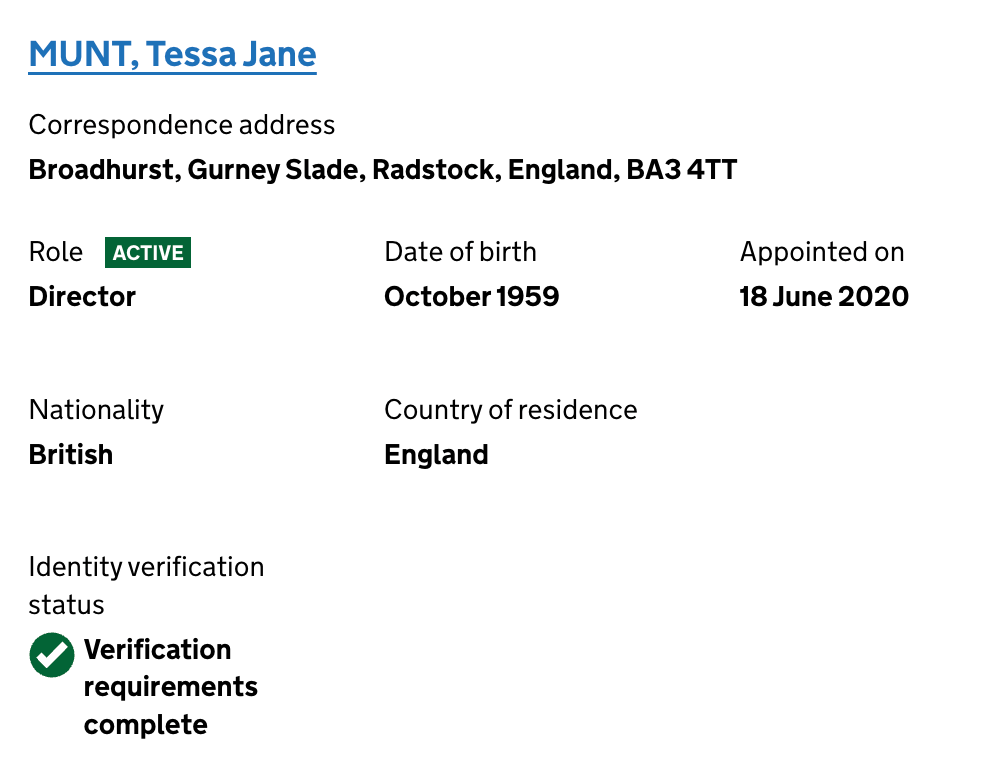
A citizen has done a public service by publicly establishing some accountability with regards to the troubling private company WhistleblowersUK, company number 09347927.
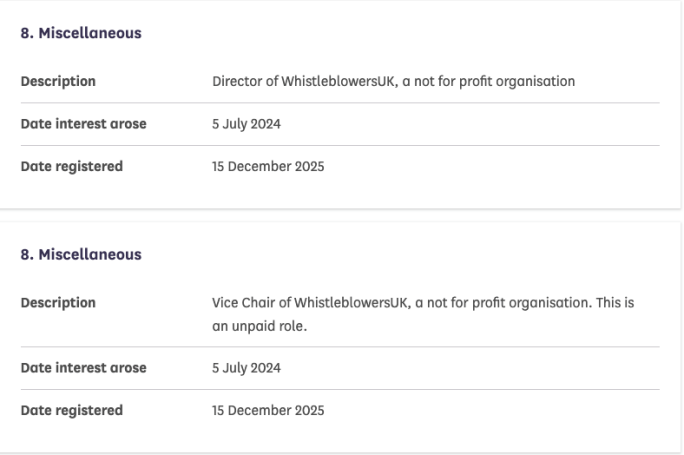
They successfully lodged a complaint to the Parliamentary Standards Commissioner about the fact that Tessa Munt MP had not registered her role as a director of the company.
The document provides a useful baseline in that Ms Munt has now committed to the public record her understanding of the nature of the company, which she presently characterises as “not for profit”.
She has stated that she is “deeply” and “truly sorry” for errors in not registering interests.
One matter jarred somewhat. The Commissioner determined that the failure to register was “inadvertent” and decided there was misapplication of the rules.
I reminded him that I wrote to him in early 2025 about a related but separate matter, in which I informed him that Tessa Munt had not registered her role as WhistleblowersUK’s Vice Chair, and that I had not received any response when I wrote to her about this.
I have now furnished him with the TWO unanswered emails that I sent Ms Munt on this matter and asked him if her failure to register her interest could really be “inadvertent”.
RELATED ITEMS
WhistleblowersUK is an entity which has an interest in establishing a US-type financial model of bounty hunting, to replace the mainstream of current UK whistleblowing law and practice. Many whistleblowers are very concerned about this,and see the move as part of private industry’s attempts to monetise what should be the public interest. There are fears that this will distort governance, waste public money and lead to exploitation and unfairness to whistleblowers and sectors which are not lucrative from the bounty hunting industry’s perspective.
There were also concerns about lobbying and access to parliament through a now defunct APPG, administrated by WhistleblowersUK, which received funding from US bounty hunting law firms. There is concern that another similar APPG will be established.
WhistleblowersUK charges whistleblowers for its services and seeks to recover a percentage of their settlements and awards. WhistleblowersUK’s documents have been revealed by a number of whistleblowers who have had dealings with the company.
By Dr Minh Alexander retired consultant psychiatrist 31 January 2026
Summary
I briefly report on the case of Dr Tim Noble who has been sacked by Doncaster and Bassetlaw Teaching Hospitals NHS Foundation Trust under a classic route of broken down relationships, sometimes applied to whistleblowers when no wrongdoing can be proven or manufactured. Shortly after Dr Noble’s dismissal, the trust published external reviews by the private company TheValueCircle on culture and leadership which concede shortcomings in whistleblowing practice but make ineffective recommendations with respect to this. These review reports also omit important governance failings, including the trust’s use of medical disciplinary procedures which is highly germane in Dr Noble’s case, where an excessively prolonged suspension was used and much criticised. The leadership review omitted other data which is unflattering to the trust and which suggests carelessness and/or cover ups, and the culture review instead emphasised that staff were proud of the trust’s services.
Dr Noble’s case
There has been a high profile dispute at Doncaster and Bassetlaw Teaching Hospitals NHS Foundation Trust in which the medical director Tim Noble, a respiratory physician, was subjected to prolonged suspension of over a year.
Dr Noble has been backed by the British Medical Association which has maintained that he was persecuted for raising concerns in the public interest, chiefly about bullying and harassment at the trust.
In other words, the route of dismissal known technically as “Some Other Substantial Reason” or SOSR, applied when there is no misconduct or incapability issue.
The NHS has abused this means of dismissal in some whistleblower cases and also more generally. Some idea of the NHS usage of this category of dismissal can be found here.
The regulator the Care Quality Commission noted in an inspection report of 28 March 2024 that there were issues with trust leadership and staff confidence in raising concerns:
“Not all staff felt leaders were visible. Staff in areas where there were greater pressures, due to challenges recruiting staff, financial restraints, and patient demand, felt less supported by the senior leadership.”
“However, during our discussions with staff groups not everyone felt respected supported and valued. We had received several whistleblowing concerns where employees felt a lack of respect, listening and ‘compassionate leadership’ from the trust. Staff in areas where there were greater pressures, due to challenges recruiting staff, financial restraints, and patient demand, felt less supported and listened to by the senior leadership.”
CQC criticised incomplete recording of staff concerns and noted staff concerns about the safety of the internal whistleblowing process:
“However, as the trust’s process encouraged staff to approach the FTSU [Freedom To Speak Up] partners rather than the guardian in the first instance, the report did not include the details of concerns raised directly to the partners. The trust did not have a process to capture these concerns centrally. This meant the Board were not fully sighted on the numbers of concerns raised by staff through the trust’s FTSU process. Following the inspection, the trust informed us they were undertaking further work to triangulate themes from concerns raised through different routes.
During the inspection most staff said they were aware of how to contact FTSU. However, we received several enquiries from staff who shared their negative opinion of speaking up, as such there was further work needed to ensure all staff felt safe to speak up.”
Two just published external reviews
This week, Doncaster and Bassetlaw published two external reviews, respectively on culture and leadership.
UHB remains as dogged by cultural problems as ever. One of UHB’s governors has recently revealed that he is being investigated by UHB for publicly engaging with discussion on a recent scandal about use of funds for recruiting overseas doctors:
The more recent culture review at Doncaster and Bassetlaw was reportedly based on twenty confidential interviews of senior staff (“Chair, CEO, Executive and Non-Executive members of the Board, and wider system partners”), surveys, walkabouts engaging 150 plus staff and listening groups with 67 staff.
The trust noted that about 10% of staff participated.
The authors say that their report was commissioned by the trust. The trust’s website states: “We commissioned the independent review to provide another safe and confidential place for colleagues to share their experiences openly”, and adds that the reviews were commissioned in “mid-2025”.
In the context of major allegations and disputes, NHS England usually has a hand in these matters, albeit this is not yet admitted in the current situation.
The report’s executive summary emphasised staff’s pride in care provided by the trust, acknowledged a “top down” dynamic, some disconnect between staff and senior management and noted improvements were needed. But I found the language somewhat euphemistic and the summary did not fully reflect the negative findings listed in the body of the report. These in fact showed:
* 27% staff did not feel respected by their immediate manager/local leader
* 46% staff did not feel respected by the trust as their employer
* 26% staff did not feel their work was valued by their immediate manager/ local leader
* 45% staff did not feel their work was valued by the trust
* 28% staff did not feel the trust was an employer which cared about their well being
* 47% staff did not feel their immediate manager/ local leader cared about their well being
Lending support to Dr Noble’s reported concerns,
* 49% staff had felt bullied or harassed in the workplace
Staff indicated that 62% of the bullying and harassment came from managers, whether from “senior management in the trust”, “senior managers in your own teams” and/or “immediate line manager/local leader”.
And very seriously,
* 54% staff did not feel confident that the trust would listen and consider their feedback
The review authors reported there were mixed views about internal whistleblowing process: “Some staff felt confident if they needed to use the FTSU route, that their concerns would be taken seriously and considered in an appropriately confidential manner. However, others felt a similar feeling to raising concerns of any kind to the Trust and doubted the process’ effectiveness. A small number of staff and some staff representatives expressed concerns regarding the perceived confidentiality of the FTSU process.”
Interestingly, reviewers noted “We were made aware that the Trust Executive team have commissioned a peer review of FTSU.”
In my view, the reviewers made largely anodyne recommendations. On whistleblowing governance they recommended:
“6.7 The review team recommends that the Trust ensures the FTSU process meets its intended purpose, assessing the effectiveness of that process, ensuring feedback is given to those raising concerns and the importance of confidentiality is understood by all.”
This is hardly going to change any abusive practices.
Nor will it assuage staff fears, when the workforce have just witnessed one of the most senior trust officers being bundled out of the door under SOSR, after a prolonged suspension.
It is necessary to acknowledge serious issues before there can be real change.
The Well Led review was also undertaken by TheValueCircle. It relied on some of the same evidence used in the culture review, as well as observation of meetings and also document review.
There were a slew of observations about trust process with some criticisms about failures to follow up and mitigate corporate risks, consistency in ensuring stated trust values, issues about communication and non executive challenge. Below average staff engagement was noted. Concerns from governors about access to some board sub-committee meetings and whether governors were heard was also raised.
Although governors’ concerns were mentioned, I found no mention of the major rupture behind the suspension of an executive director, and yet the mission includes “To identify the dynamics of the board”. Instead, the reviewers appeared to erase the fact that there had been a rupture and reported as if a member of the board was not currently suspended. They referred only to “respectful” and well chaired ongoing meetings.
Similar comments were made about whistleblowing governance as in the culture review, with the added detail that the trust had worked with the General Medical Council on whistleblowing matters, implying that at least some doctors were fearful:
“We acknowledge that the Trust has worked with the General Medical Council to strengthen perceptions of psychological safety in speaking up and to improve medical colleagues’ confidence in the process. However, listening groups identified that some colleagues still lacked confidence. In addition, some staff reported they were unsure how to access the FTSU service.”
Of note, despite the controversial and excessively long suspension of the medical director, I could find no comment by the reviewers about the trust’s application of formal NHS medical disciplinary process under MHPS (Maintaining High Professional Standards).
This seems to be a serious omission in the trust’s favour and potentially a point of criticism about impartiality of the review, or at best, its effectiveness.
The only reference that I found in the Well Led review report on trust disciplinary process was the inclusion of the policy “ORP/EMP 2– Disciplinary Procedure” in the list of documents reviewed.
Neither was disciplinary culture discussed in TheValueCircle’s culture review report, as far as I could see.
These seem to be inexplicable omissions given the high level of bullying and harassment flagged by staff.
Especially as staff reported that 62% of the bullying and harassment came from managers.
Neither could I find discussion of compliance with CQC Regulation 5 Fit and Proper Persons in the Well Led review report. This may be a limitation of the NHS England template for these types of reviews.
On general search, I also found past CQC fines against the trust for breach of candour and several serious and relevant coroners’ findings in 2025, that were not reflected in TheValueCircle’s well led review report. I list these at the end of this post. I would have hoped that these should have been considered under the banner “Is there a culture of high quality, sustainable care?”
In conclusion
We appear to have a classic NHS whistleblowing case of very harsh discipline following reported public interest disclosures and then dismissal on shaky grounds on breakdown of relationships. The latter is usually a last resort when employers are unable to make misconduct or incapability grounds stick. All accompanied by somewhat lacking employer-commissioned reviews which offer partial fig leaves by omission, throw up some vapour trails yet have not answered all the crucial questions.
None of which serves patients’ interests, and likely only leaves remaining staff in anxiety and doubt.
As well as the wasteful dismissal of an expensively trained and developed senior doctor who was not accused of misconduct or incapability, the prolonged suspension of Dr Noble was especially objectionable. Such torturous suspensions are wasteful and almost never justified. They are punitive and very harmful to individuals and their families. They were supposed to be actively tracked and phased out long ago after NAO recommendations in 2003, but harsh discipline and suppression in the NHS is too politically useful and so was retained.
Tim Noble may obviously lodge an Employment Tribunal claim against the trust in respect of his treatment, in which case more details will emerge about the nature of the governance concerns.
RELATED ITEMS
1) It is relevant to note that the CQC issued two fixed penalty notices against Doncaster and Bassetlaw in recent years for failing to comply with the legal Duty of Candour:
“In 2021 CQC completed an investigation of a serious incident at the trust. The fixed penalty notices relate to an incident in July 2018 where a patient, who cannot be named for legal reasons, died after complications during childbirth. These two breaches of duty of candour regulations were:
Failing to notify the family as soon reasonably possible that an incident had occurred
The trust did not provide the family with an account of the incident or offer an appropriate apology to them in a timely manner.”
These governance failings reflect on trust leadership.
2) Doncaster and Bassetlaw has also been issued several coroners’ Prevention of Future Deaths reports last year as follows, some of which raise issues about organisational learning and thus leadership.
In the case of John Bell, the coroner was concerned that no Datix incident report was filed and that six months after his untoward death, no investigation had taken place.
In the case of Marina Raisbeck, the coroner was concerned that the factors which contributed to her death had not been addressed, fifteen months after her death.
Distressingly, in the case of Walter Horton, the coroner concluded that staff did not understand cleanliness or aseptic technique.
In the death of Emily Hewerdine from neglect, the coroner noted fifteen months after her death that the system failings had not been rectified.
In the death of Khadija Kerri, radiological evidence of cervical and rib fractures were not passed on initially and clinical action was not taken to immobilise the fractures for 3 days. Eight months after the patient’s death, the coroner noted that there was no policy on disseminating addendum report findings.
It would seem to me that such governance failings should have been reflected in a report on whether the trust was well led.
NHS England’s expectations for Well Led reviews require:
“Senior leaders can evidence that there are appropriate and effective mechanisms for turning concerns/ incidents into improvement actions based on inquiry about the root causes of what has happened, where constructive challenge is welcome at all levels of the organisation, including the board.”
4) It is worth reminding ourselves that the lamentable architect of the NHS Freedom To Speak Up model, Robert Francis, claimed expansively over ten years ago in his 2015 Freedom to Speak Up report:
“The climate that can be generated by these measures will be one in which injustice to whistleblowers should become very rare indeed, but is redressed when it does occur.”
Neither of the risible claims in this statement is true.
I have spent the last ten years tracking and documenting the failures of Francis’ patently ineffective but government-pleasing policy.
It is clear that there continue to be no end of casualties. Redress for NHS whistleblowers is very patchy and usually only partial and inadequate when achieved. And redress very rarely comes in the form of resolution of the original whistleblowing concerns, which is so important to the majority of whistleblowers. In the NHS this is vital to public safety, which still limps in last.
Realistically, I usually have to advise whistleblowers to prepare themselves for loss, and to make choices about the level and type of losses.
The least risky whistleblowing strategy is NOT to follow the internal policy but to disclose to the media, either anonymously or with guarantee of anonymity. But it is best to take advice and each must make a personal decision.
And until UK policy and law are properly reformed, the situation will sadly not change.
5) At University Hospitals Birmingham, which also commissioned reviews from TheValueCircle after scandal, another whistleblower was severely victimised and the CQC failed to hold trust directors to account under the Fit and Proper Person provisions:
Accordingly, I asked HOLAC if it routinely checks nominees’ qualifications, or had arrangements for third parties to do so.
I also asked that if not, whether this would be corrected, and whether there would be any retrospective review to assess whether there were past cases where qualifications had not been checked. I also asked for documented reasons if there had been a decision not to undertake such a retrospective review.
The reply to my FOI request was that it would not be in the public interest to disclose how nominees’ qualifications are checked, with the following convoluted argument:
“The information that you have requested in question 1 falls within section 37(1)(b) of the Freedom of Information Act, which relates to the conferral of honours and dignities. A peerage is a dignity for the purposes of the Act. Section 37 is a qualified exemption which is subject to a public interest test. In favour of disclosing information, there is a strong public interest in knowing that the appointments process is accountable and transparent, and in maintaining public confidence in the peerage appointments system. In favour of maintaining the exemption, there is a strong public interest in limiting the level of detail about exactly what checks are carried out by the Commission, to ensure individuals are not able to tailor the information they provide once nominated. It would set a dangerous precedent to start providing precise detail of the checks conducted, which could allow individuals to selectively decide what information might be presented to both the Commission and the nominating Party.
Taking all of the relevant factors into consideration, including the fact that the Commission already places a great deal of information about its working practices and the checks it carries out in the public domain to reassure the public that these are sufficiently rigorous, I consider that the balance of the public interest lies in maintaining the section 37(1)(b) exemption in respect to confirming whether the Commission verifies individuals’ qualifications.”
I think this response would probably make even Sir Humphrey blush.
The rest of the world presents a curriculum vitae to prospective employers, which is checked, and educational qualifications are duly verified with the relevant institutions.
Straightforward, no?
But it seems that the arcane HOLAC is concerned that letting us know about its procedure for verifying qualifications will somehow give nominees some nebulous, nefarious advantage.
Or maybe they simply have no checking procedure and are too mortified, as very important individuals, to admit this to impertinent plebs.
Perhaps very important people are content to accept recommendations from other very important people. PLU to PLU.
With respect to the rest of the FOI request, it is maintained that:
“I have established that HOLAC does not hold any information in scope of questions 2,3 and 4 of your request”.
That is to say, there is no intention to correct any possible omission in HOLAC’s verification procedure nor to retrospectively review for any other naughty peers with non-existent qualifications. And there is no written record of the latter decision not to review.
All told, a very unsatisfactory and unaccountable position after such a major scandal.
This serf will now withdraw to her wattle and daub hut to appeal to the ICO and dispute HOLAC’s application of the public interest test.
Feudalism being what it is, the chances of success may be slim, but I was pleasantly surprised on a past occasion so we shall see.
Internal review request
Prior to appealing to the ICO, I have taken the preliminary step of requesting an internal review of the FOI response, which I have directed to Baroness Deech Chair of HOLAC:
FAO Baroness Deech
Chair House of Lords Appointments Commission
12 January 2026
Dear Baroness Deech,
Request for FOI internal review and query about governance on verification of nominees’ qualifications
I was concerned by the Sunday Times report about Ann Limb’s qualifications – or lack of – and asked for information via FOIA about HOLAC’s process, if any, for verifying nominees’ qualifications.
I received the attached FOI response which I take to mean that:
1) HOLAC does not wish to disclose the details of any verification process on grounds that it may somehow given undue advantage to nominees.
Indeed, the FOI response states: “It would set a dangerous precedent to start providing precise detail of the checks conducted, which could allow individuals to selectively decide what information might be presented to both the Commission and the nominating Party.”
I confess I do not understand this argument as past qualifications are something one possesses or does not, and that is the point of verification – to establish the truth of claimed qualifications.
What I am merely seeking is confirmation of whether or not HOLAC has within its process a means of checking that nominees have not fraudulently manufactured qualifications on their CV which they never earned. I do not see how providing confirmation of a process could prejudice the selection of nominees.
I would be very grateful if you could consider my query on this aspect to be a request for internal review under FOIA for disclosure of whether HOLAC has a procedure for verification of nominees’ qualifications, and for broad details of any procedure.
For example, does HOLAC (or a third party) routinely contact universities to establish that nominees hold the degrees that they claim to hold?
2) I further understand HOLAC does not intend to make any changes to its procedure – whatever it may be – or to retrospectively review for any cases where nominees’ qualifications may not have been verified. Also, there is no record of a decision not to retrospectively review for any cases where nominees’ qualifications may not have been verified.
If my understanding is correct, may I ask if this is the right approach in light of the seriousness of the Ann Limb matter?
HOLAC says that its purpose is to ensure the highest standards of propriety. Would not wider learning be important after such an incident?
Dr Minh Alexander retired consultant psychiatrist 6 January 2026
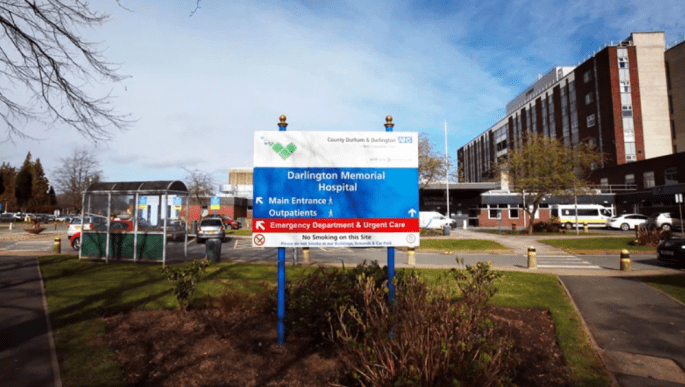
This is a post-script to my last post on the still unfolding breast cancer surgery scandal at County Durham and Darlington NHS Foundation Trust (CDDFT).
An independent investigation (the “Aubrey Report”) reported major governance failures by trust executives and failures to act on red flags over many years. These included concerns from multiple sources, including staff whistleblowers.
A missing element to the whole picture was any apparent contribution by the regulator, the Care Quality Commission (CQC), to the identification of the failures.
Accordingly, I asked the CQC via FOIA for information on public interest disclosures by trust staff about the breast cancer surgery service and other information. This is because the CQC is a ‘prescribed person’ under UK whistleblowing law, which is responsible for receiving concerns from the staff of regulated health and social care providers.
It seemed inconceivable that at least some staff who had been so concerned for so long would not have sought help from the key regulator responsible for overseeing health services.
Implausibly, the CQC denied that it had received any whistleblowing disclosures from CDDFT staff about the breast cancer surgery service. There is some wiggle room in that CQC advised it was unable to manually review the records within the FOIA cost limits and relied only on searching for key words. But even so, it is still remarkable that a key word search yielded nothing.
It should be noted that CQC is now aggregating provider staff whistleblowing disclosures with concerns from other sources, which inflates numbers and contributes to its claims of Section 12 cost exemptions under FOIA.
I further asked the CQC to confine its search to trust staff disclosures to the local CQC inspection team in the last five years. It denied that these were recorded any differently. CQC advised that it had received 520 concerns about CDDFT in the last five years and claimed that it would still exceed FOI cost limits for these to be manually reviewed for staff disclosures relating to breast surgery.
I am almost certain the CQC will have received disclosures about CDDFT breast surgery services at some point, given the level of concern and the very long period of time over which the problems occurred. We may receive confirmation in due course that such staff disclosures were made, especially if any of the staff who made disclosures about the breast cancer surgery service learn that CQC has denied receiving them/ avoided answering.
But in swerving the questions about staff whistleblowing at CDDFT, the CQC lays itself open to criticism of general negligence in tracking whistleblowing activity in NHS organisations – a vital governance task. If it has really stopped differentiating the various sources of concerns, as it now claims, it must have no grip. I will write to the latest CQC CEO about this. Alternatively, the CQC may eventually decide that it can tell us about whistleblowing at CDDFT after all.
CQC evaded a question about whether it had been alerted to the breast cancer surgery issues by other regulators:
“3. Please disclose if since 2012 the CQC has been alerted by other regulators such as Monitor, NHS Improvement or NHS England of any pf the problems in the breast cancer surgery services at CDDFT? If so, please give dates and relevant details.
We do not keep a central record of information that can easily answer this point.”
Although CQC did not clearly say whether it had specifically inspected breast cancer surgery in the years concerned, the CQC disclosed that it re-inspected the trust’s surgery services in October 2025, and has taken enforcement action.
“6. Has the CQC inspected the trust since 2019? Does the CQC have anyplans to inspect CDDFT in the next year?”
The trust’s surgical services were recently inspected by the Care Quality Commission. We carried out an inspection of surgery services in October, and due to concerns found, we have taken enforcement action against the trust to ensure the safety of people using services.”
As far as I can see, the report from this inspection has not yet been published on CQC’s website.
I asked CQC about data held on serious incidents relating to CDDFT’s breast cancer surgery service. CQC advised that data is held for only three years and not in a form which allows analysis of incidents specific to the breast cancer surgery service: “we cannot break it down to identify incidents specifically about breast cancer surgery services”.
This would obscure detection and monitoring of any patterns.
Regarding whether CQC has reviewed itself in the light of the Aubrey report, and has identified any lessons to learn from the breast surgery scandal, CQC replied thus:
“5. Please disclose if CQC has assessed whether it has any lessons to learnarising from events at CDDFT and the findings of the Royal College ofSurgeons invited review and the Aubrey report into breast cancer surgeryat CDDFT. If so, has the CQC conducted any internal review of itsinspection process at CDDFT or does it plan to do so?
Following reasonable searches, no recorded information has been located with which we can answer this specific part of your request.”
Dr Minh Alexander retired consultant psychiatrist 26 November 2025
Introduction
This is a brief report on the continuing failure of the wasteful Freedom To Speak Up model, which is being retained by the NHS despite abolition of the National Freedom To Speak Up Guardian’s Office.
An external review of failings in breast cancer care, the “Aubrey Report”, has this week been published by County Durham and Darlington NHS Foundation Trust (CDDFT).
About the author of the Aubrey Report Mary Aubrey the author is described in the report as Director and Specialist Expert Advisor in Governance. Her LinkedIn entry describes her as a part time NHS director “Providing specialist advice and support on progressing the NHS Trust to moving to excellence and exiting RSP 4 in 2026”. She is also listed on the website of the private company Quality Governance Solutions 15267661 where she is described as a CQC associate. A search shows that she has acted for CQC as an executive reviewer in past CQC inspections. For example, during the 2019 inspection of Royal Berkshire NHS Foundation Trust.
Care Failings
The Aubrey report found multiple failings spread over a long period of time, which resulted in poor care, summarised as follows:
“Patient harm due to outdated clinical practices and unnecessary procedures:
Patients experienced avoidable harm, including delayed diagnoses, unnecessary mastectomies and axillary clearance, and benign procedures that were not clinically indicated. These failures resulted in significant physical, emotional and psychological consequences for patients and staff”
“A lack of documented breast reconstruction planning in at least six cases highlights missed opportunities for shared decision making. Additionally, technical errors, including incorrect skin marking leading to repeat surgery, underscore preventable harm and resource inefficiencies.”
A local media report gives a devastating report of one patient who was left bed bound after sepsis:
“This has been totally devastating. It has ruined my life, without a doubt,” says Moira, who is in her 60s….I never thought this would be the case at this age. I have had a very busy life and career, but now I am dependent on the care of others.”
“She says she is completely bedbound unless hoisted into a chair by her carers.”
The patient describes a traumatic encounter with a surgeon:
“This surgeon was in his suit and put surgical gloves on – and without warning from him, and without any kind of anaesthetic, cut open my wound.”
“He began taking out handfuls of blood clots from my breast and putting them into a surgical bowl.
“While it wasn’t painful, it was uncomfortable and felt very concerning. Blood was pooling underneath me and down my left-hand side, which the nurses cleaned after the surgeon left the room.
“From the faces of the nurses who were present, I could tell this wasn’t normal.
“I didn’t know what to do, as I wanted my breast to get better, but the faces of the nurses told me everything I needed to know. They didn’t say anything about what he had done.
Related governance failings including whistleblowing failures
The Aubrey report also noted a failure of the legal, organisational duty of candour:
“Despite clear evidence of harm, including unnecessary axillary clearance, mastectomies, excessive surgery due to poor diagnostics, and benign procedures that were not clinically indicated, the Executive Medical Director and former Executive Director of Nursing delayed the initiation of Duty 12 of 232 of Candour. Action was only taken in February 2025, a nine-month gap that represented a significant breach of statutory obligations.”
According to his LinkedIn entry, the Executive Medical Director was in post from 2017 up to November 2025. The former Executive Director of Nursing according to his LinkedIn entry was in post 2015 to December 2024 and is now a NED at York and Scarborough Teaching Hospitals NHS Foundation Trust.
Mary Aubrey concluded that there were repeated missed opportunities to identify and correct the patient harm, with multiple red flags and warnings from different sources, including from senior personnel, which the trust board failed to act upon.
For example:
“Despite multiple early warnings from 2012 to 2025 including internal audits, external reviews, national surveys, and benchmarking data, effective action was not taken until 2025. This prolonged delay reflects deep-rooted leadership and governance failures, where Executive Directors, Care Group Triumvirate and Specialty leaders repeatedly failed to intervene, challenge poor practice, or implement improvement recommendations.”
“Concerns raised in 2017. 2018, 2019, 2021, 2023, and 2024 were either ignored or subject to delayed action, despite clear red flags. Service and Care Group leaders did not act on, or escalate warnings from colleagues across pathology, radiology, booking, MDT coordination, medical records, operational management and clinical nursing.”
These listed whistleblowing episodes all fall firmly within the period when the NHS Freedom To Speak Up arrangements should have been embedded. They were introduced in 2015 and it is reasonable to expect that by 2017, all trusts should have had compliant structures and informed boards. It was certainly what the central propaganda claimed. But there may have been issues of capacity, as a CQC report of 2019 stated:
“On our last inspection we raised concerns about the capacity of the Freedom to Speak Up Guardian (FTSUG). While two champions had been recruited and working hours increased there was still work to do to increase capacity and raise the profile of the role within the trust.”
Aubrey noted dysfunctional culture within trust breast surgery services with issues of bedside manner, rudeness within teams, insularity and resistance to feedback and change.
For example: “Cultural and behavioural issues, including poor communication, lack of psychological safety, and unprofessional conduct from some consultants, contributed to staff distress, high turnover, and reluctance to raise concerns.”
The RCS invited review noted problems with multidisciplinary decision making, challenge and leadership.
Moreover, Trust staff showed fear during Aubrey’s investigation and asked for anonymity.
Their fears proved justified when Trust executives tried to identify them. Aubrey wrote:
“Staff repeatedly expressed to the Reviewer their desire to remain anonymous, particularly where roles were unique and individuals could be easily identified. Attempts by some Executive Directors to identify contributors not only breached this understanding but also reflected a leadership approach perceived to prioritise control over accountability. This incident highlights broader cultural challenges within the Trust, where psychological safety appears compromised and staff remain apprehensive about potential retaliation or scrutiny when raising concerns.”
It is a measure of dysfunction that trust executives felt free to attempt to identify staff in plain view of an external investigator.
Clearly, whether or not the trust Freedom To Speak Up Guardian service was adequately resourced, it had no chance if the trust executives had no respect for staff confidentiality.
Unsurprisingly, the Aubrey report concludes that whistleblowing governance at the trust was flawed. There is possibly an implication that Freedom To Speak Up procedures – “formal mechanisms” – failed:
“As outlined above, staff reported feeling discouraged by managers from whistleblowing due to apprehension about retaliation, including warnings from managers that speaking up could adversely affect their careers. This culture of deterrence contributed to the persistence of harmful practices and undermined efforts to strengthen safety, transparency, and accountability within the service. Concerns were not escalated and the Trust Board did not have effective systems to detect and address suppression of concerns within the areas affected. While the Trust’s staff survey scores for ‘Raising Concerns’ are in line with national averages, qualitative feedback from interviews and helpline data suggests that formal mechanisms were not always experienced as psychologically safe or effective by staff” [my emphasis]
There was specific criticism of Non-Executive directors who should challenge, and who often hold “champion” roles for FTSU arrangements:
“The cultural factors outlined above combined with staff apprehension around whistleblowing and limited scrutiny from Non-Executive Directors, including the former Trust Chairs during their tenure. and assurance committees created conditions in which unsafe practices were able to persist unchallenged and without accountability.”
It is almost always the case that such summarised details do not convey the depth of suffering of individuals and their families who are at the butt end of such failures of whistleblowing governance. To be at the mercy of trust executives whose goal is “control”, above all else, can be a life-changing nightmare that may extend for years.
In short, Aubrey’s report sets out a fairly typical and familiar anatomy of an NHS scandal.
This “Good” rating is from 2019. One would have hoped that with all the concerns about the breast service and poor trust governance that the trust should have been inspected more recently.
But was CQC even aware of the breast service failings? The trust’s breast service lost training status as early as 2012 and the Aubrey report rightly concludes that the loss of training status was a red flag:
“The Breast Surgery Services was flagged for failing to meet the standards required for safe and effective medical education, and for not providing a supportive training environment which are both essential for surgical trainees. This led to the withdrawal of training accreditation in 2012. The loss of surgical trainees was a direct result of GMC action and serves as a fundamental indicator of breakdowns in supervision and clinical governance.”
“The loss of trainee status in the Breast Surgery Services represents a significant red flag for the organisation”
But as far as I can see, CQC did not specifically inspect the breast service in 2019. Or if it did, it raised no specific concerns.
Moreover, the CQC inspection report of 2019 claimed generally “It was easy for people to give feedback and raise concerns about care received. The service treated concerns and complaints seriously, investigated them and shared lessons learned with all staff.”
General ineffectiveness of the Freedom To Speak Up model and questions about the Fit and Proper Person Framework
In conclusion, this affair only reinforces concerns that the government’s Freedom To Speak Up project has been a wasteful, deflective propaganda exercise that has done very little to help NHS patients and staff.
At least the lead propagandist’s Office, the National Guardian’s Office has been disbanded. But the decision to continue wasting scarce public funds by continuing with a local model of Freedom To Speak Up Guardians is a classic but disappointing NHS fudge.
There has been little transparency about how the latter will work, only a few cryptic comments in a NGO’s newsletter and a brief NHSE update about how some central functions will transfer to NHS England. I have asked NHS England via FOI for more precise details.
I have also written to Jim Mackey NHSE CEO to ask if and how the findings of the Aubrey report will be used by NHS England with respect to new NHS Fit and Proper Person arrangements following the Kark review. This is with respect to general findings of executive failure to act upon red flags and safety indicators, the failure of organisational duty of candour and the reported attempts by trust executives to breach anonymity of staff reporting concerns to an investigator. It is unclear to me if the FPP framework and related database/ disbarring mechanism have been finalised six years after completion of the Kark Review on Fit and Proper Persons in the NHS, but I have asked NHSE for a completion date if not.
My wonderful husband Ian has died. I am not back at work at full strength and cannot respond to requests as much as usual, but will aim to post from time to time. All my very best.
RELATED ITEMS
CDDFT has as per NHS standard operating policy, announced a cultural reset. The trust also reports early progress in rectifying the safety issues.
This is considered to be a weighty indicator of the eventual ruling of the international court on the genocide case against Israel.
At present, the UN Commission considers there is a duty on all states parties to the genocide convention to do all they can to actively halt the Gaza genocide and restrain Israel. This includes the tool of economic pressure.
Concerns have been raised about NHS bodies purchasing supplies from Israeli companies.
A particular issue is that Kings are involved and the Chair of Kings is no other than David Behan the former regulatory chief of the Care Quality Commission. Who one might hope should take extra care to ensure a high level of legal and ethical compliance. Cough.
Campaigners, including trust staff, remain very concerned.
I have been sent this flyer for anyone with an interest in these matters:
All best wishes and see you when I see you.
A reported exchange between campaigners and Behan at Kings: