Dr Minh Alexander retired consultant psychiatrist 5 September 2022
| Summary: The Care Quality Commission’s poor whistleblowing governance has been exposed by the case of Dr Shyam Kumar who was found by an Employment Tribunal to have suffered detriment by the CQC, explicitly linked to Mr Kumar’s whistleblowing. The case reveals that the CQC: – Failed to protect a whistleblower – Failed to act on his concerns – Failed to accept that his whistleblowing was valid, minimised his concerns and saw the whistleblowing as a nuisance and a threat – Mistreated the whistleblower seriously and smeared him with a number of unjust and false claims – When challenged by the whistleblower about this poor treatment, the regulator sought to portray him as a difficult and “challenging”, and ridiculed his claim of whistleblower reprisal by the CQC – Tried to dig dirt about the whistleblower to retrospectively manufacture a case justifying its mistreatment, abusing regulatory power in the process – Suggested falsely to the Employment Tribunal that Mr Kumar was attacking non-consultant grade doctors at his trust for financial gain, because he did not want them to do work which reduced the waiting list – Fed false information to the Ombudsman to shut down a legitimate complaint by the whistleblower about his mistreatment by the CQC – Claimed reasons for its treatment of the whistleblower which were not believed and were rejected by the ET, calling into questions the truthfulness of the claims – Operated oppressive HR policy and practice, but foolishly and incompetently maintained up to the last minute that its processes were fine. |
Introduction
The Health and Social Care regulator the Care Quality Commission has lost an important whistleblowing Employment Tribunal case against surgeon and NHS whistleblower Mr Shyam Kumar.
This is the judgment:
ET judgment 24 August 2022 Mr S Kumar v Care Quality Commission case number 2410174/2019
This important case reveals failures by the regulator on several levels, some of which arguably amounts to serious misconduct by CQC personnel.
The regulator is supposed to protect whistleblowers and ensure good whistleblowing governance by regulated bodies.
Moreover, the CQC is legally a Prescribed Person, which means that it is supposed to be a safe haven body, to which Health and Social Care whistleblowers can make protected disclosures.
But CQC has been found by the ET to have unfairly dismissed and seriously harmed a whistleblower.
A decade after the CQC was found by the MidStaffordshire Public Inquiry to have harmed its previous whistleblowers. by the MidStaffordshire Public Inquiry, the ET finding is highly relevant.
And the reason for this current failure is the same as the previous failure: CQC reacted badly to concerns about its poor regulatory performance.
CQC has clearly learnt little.
This matter raises serious questions about the honesty and probity of the regulator, which holds the welfare of so many patients and service users in its hands.
Mr Kumar’s role as a CQC Specialist Advisor
Mr Kumar is an experienced orthopaedic surgeon of unblemished record.
He has experience of assisting whistleblowers through a previous role as an active member of BAPIO. He has also has a legal qualification.
He was of good standing and hired by the Care Quality Commission as a Specialist Advisor in July 2014, on the basis of a secondment contract.
By 2015, he was in bad odour with the CQC’s senior managers, because he whistleblew to them about poor management of a CQC inspection and an experience of being bullied by the CQC inspection lead, who prevented him from talking to NHS trust whistleblowers during the inspection:
One of the concerns raised in this letter is of collusion by the CQC:
“There appears to remain a culture within the CQC, which results in some medical directors and chief executives being let off lightly when whistleblowers have raised concerns.
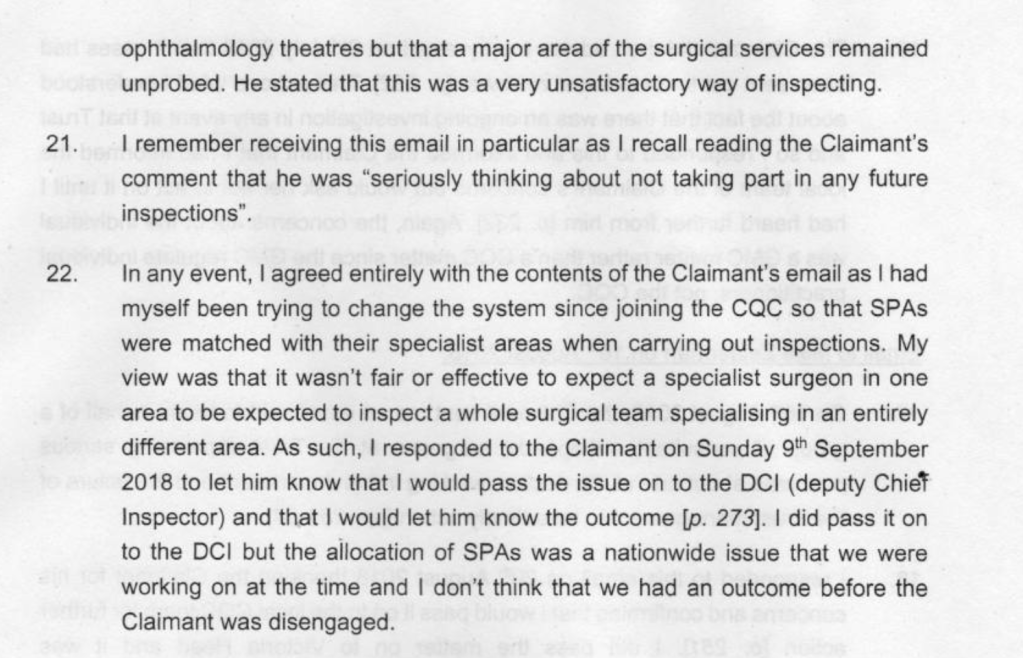
Mr Kumar is not aware that his concerns were ever investigated, despite a reminder. Neither has the CQC produced any records to prove that it investigated his concern.
Whistleblowing to the CQC in 2018
By June 2018 Mr Kumar had cause to whistleblow again to CQC managers, over two areas of concern:
1. CQC’s flawed inspection methodology which included using Specialist Advisors in inspections for which they were not expert. Mr Kumar’s concerns arose from a chaotic CQC inspection of East Lancashire Hospitals NHS Trust.
2. Issues about very serious patient safety at his own trust, University Hospitals Morecambe Bay NHS Foundation Trust.
These patient safety issues revolved around the poorly supervised orthopaedic practice of a Dr X, about which a number of consultants raised concerns. These safety concerns have been validated by two external investigations. The GMC imposed restrictions on dr X’s practice in 2018, as a result of whistleblowing by Mr Kumar and other colleagues.
As well as the patient safety concerns, Mr Kumar also raised concerns with the CQC about the governance at his trust, failure by the trust to act effectively on the patient safety issues and the fact that he had not been protected from severe whistleblowing reprisal.
The whistleblower reprisal included serious false allegations against him, including in group emails involving his peers. In one email Mr Kumar was dubbed a “traitor”.
“80. On 30 October 2018, Mr S [REDACTED], in an email to a broad recipient list, described individuals who were involved in activities against doctors of Indian origin as being ‘traitors of their community’ (p.393). Given that the claimant had raised complaints about the Dr X’s practice, and the close nexus in time that this comment is made to those complaints, on balance it is likely that this comment is about the claimant.”
Mr Kumar also raised concerns with the CQC about white consultants feeling intimidated to to raise patient safety concerns in case they would be subject to counter-allegations of racism
Mr Kumar’s concerns about the above governance failure at UHMBT have been vindicated by both external and internal investigations.
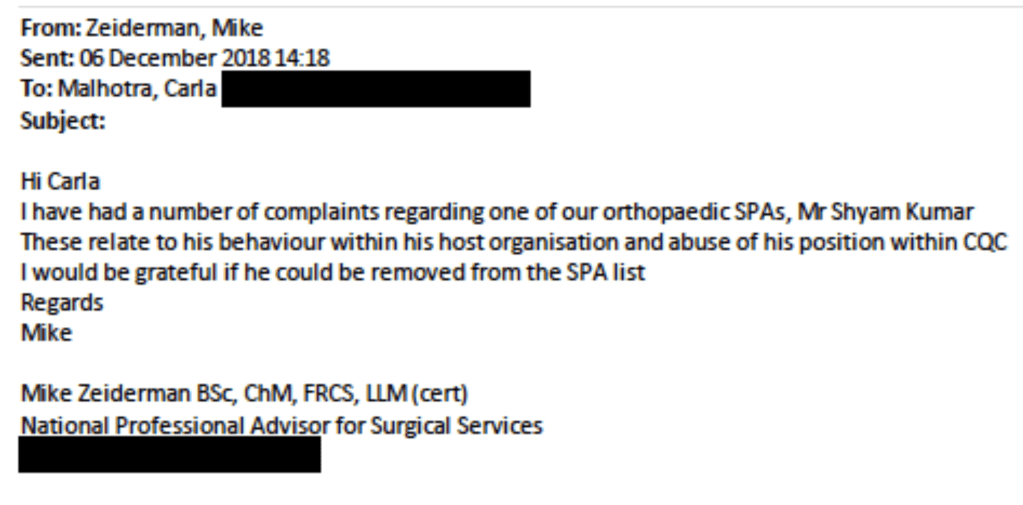
His disclosures to CQC were made primarily to the CQC National Professional Advisor, Mike Zeiderman, colorectal surgeon based at Southport and Ormskirk.
This is list of Mr Kumar’s disclosures that the ET ruled met the legal threshold of protected disclosures:
Instead of recognising the seriousness and validity of Mr Kumar’s concerns, it appears that the CQC regarded Mr Kumar’s disclosures as a nuisance and a threat.
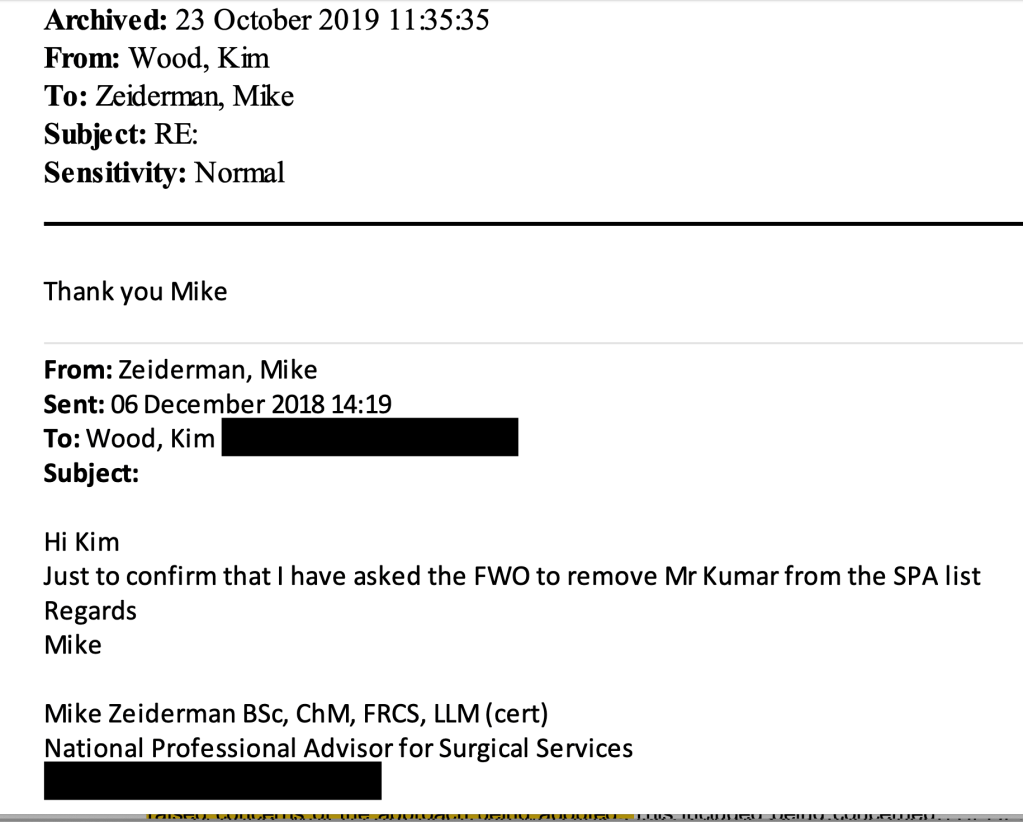
The ET considered that correspondence by Mike Zeiderman made it clear that a decision in December 2018 to sack Mr Kumar as a Specialist Advisor was explicitly linked to Mr Kumar’s disclosures to Mike Zeiderman.
These are examples of Mr Kumar’s disclosures:
The ET summarised another disclosure by Mr Kumar as follows:
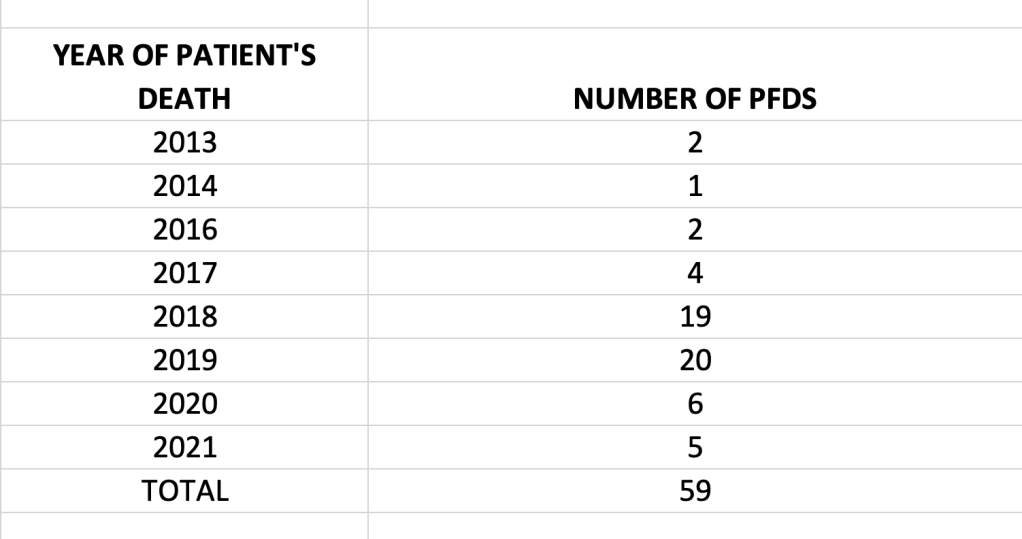
“On 29 June 2018, following up his email of 16 June 2018, the claimant called Mr Zeiderman. During this phone call, the claimant reiterated concerns that matters had been raised with the Trust’s Medical Director, but that the Trust was refusing to look into those concerns but was wanting to cover up the issues. The claimant also raised specific examples of to suspicious deaths, after which the Trust had not taken steps to prevent further harm. The claimant provided specific details of the two cases to Mr Zeiderman in this phone call. The claimant was disclosing information of serious and/or potential harm to patients. Mr Zeiderman accepted the claimant’s paragraph 38 as being the content of that phone call.”
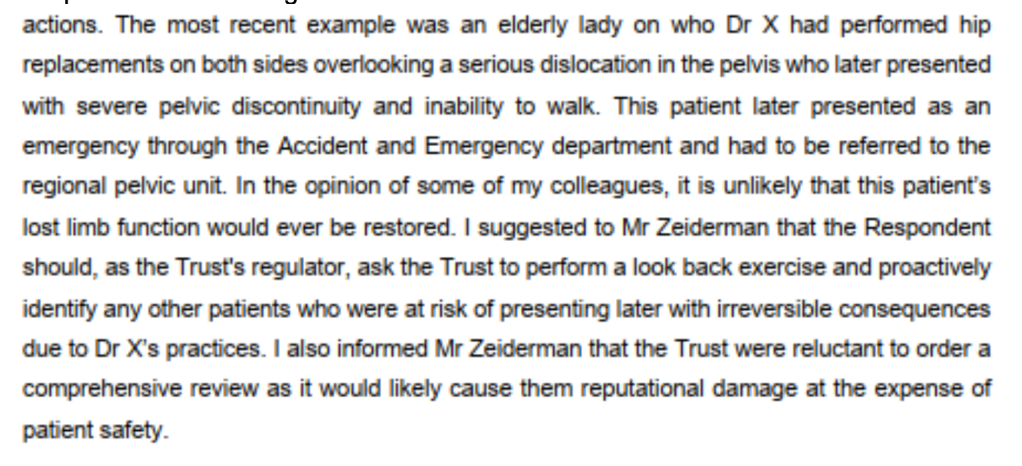
This is Mr Kumar’s account of another disclosure to Mike Zeiderman:
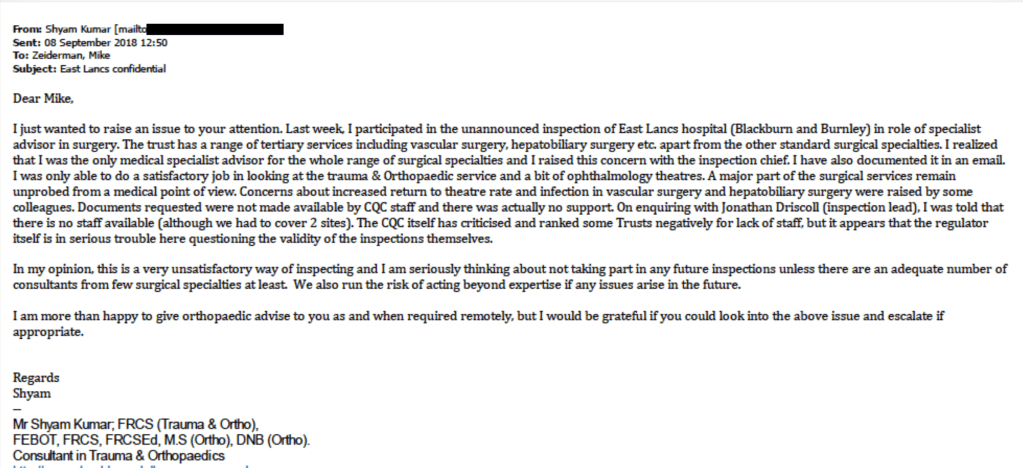
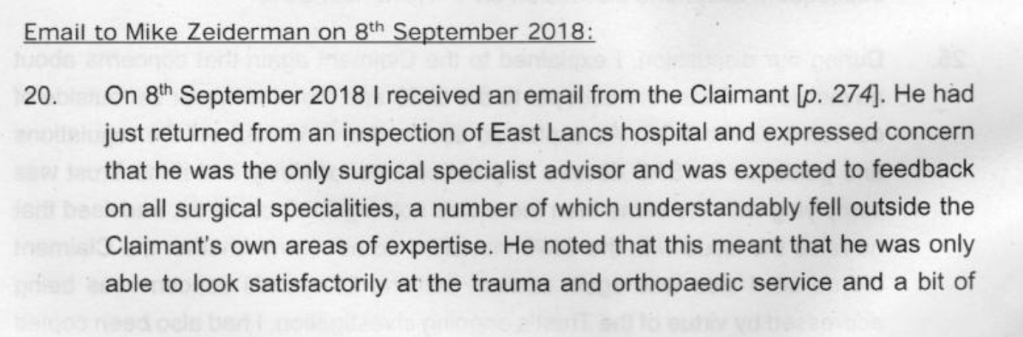
The most threatening of these disclosures from CQC’s point of view would have been the email of 8 September 2018, in which Mr Kumar made serious criticisms of CQC’s unsafe inspection methodology at East Lancashire.
Despite Mr Kumar’s concerns about CQC’s inspection methodology, CQC still rated Surgery at East Lancashire as “Good”.
The CQC later accepted that some of Mr Kumar’s communications were protected whistleblowing disclosures, but the regulator and Prescribed Person contested five significant disclosures (disclosures 2,3,4,8,10) right up to the point when the Employment Tribunal ruled that they were bona fide whistleblowing.
The ET judgment reveals that a witness statement by the local CQC inspector Kim Wood had a denigratory tone in that it referred to Mr Kumar’s valid disclosures as “persistent”:
“Ms Wood compounds this at paragraph 33 of her witness evidence, where she explains whilst discussing the decision to disengage and the letter to Mr S [REDACTED] that ‘This was particularly so against the background of the persistent emails to Mike about the use of SAS doctors and patients concerns…’ Ms Wood again refers to emails as part of the decision making process. These emails are protected disclosures 2-10.” [my emphasis]
In one email thread, Kim Wood dismissed correspondence from Mr Kumar as “largely irrelevant”.
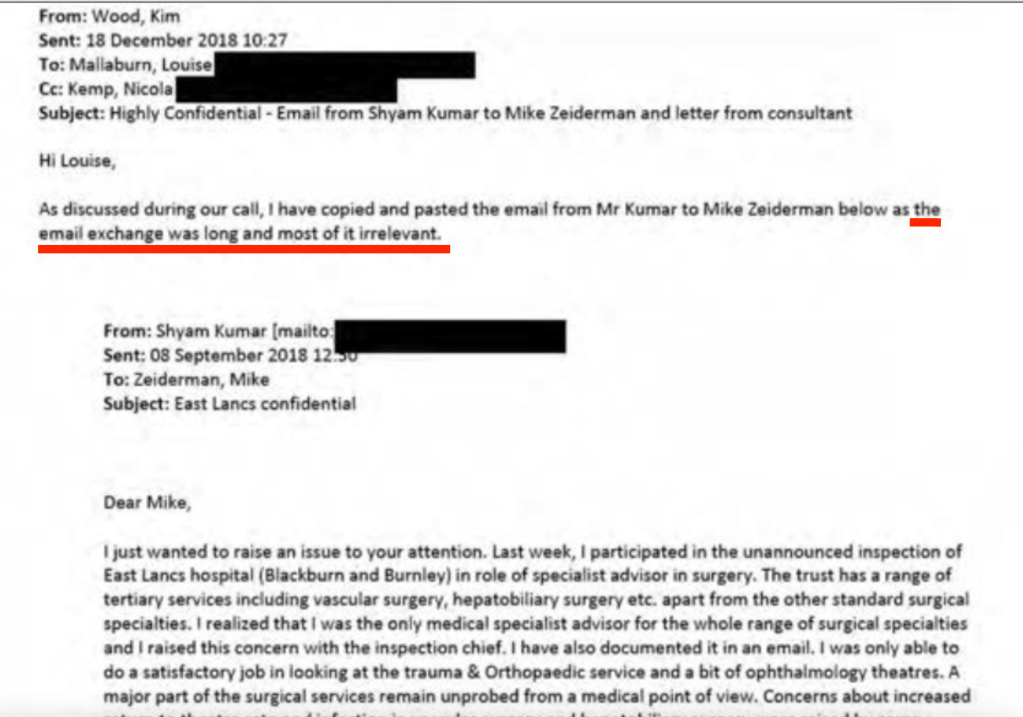
The ET later concluded that this correspondence by Mr Kumar, which Wood had so casually dismissed, was NOT irrelevant but were protected disclosures:
“The emails forwarded by Ms Wood were relevant and played a central role in this decision to disengage the claimant from his role with the respondent. The emails contained in this email were:
a. The 08 September 2018 email from the claimant to Mr Zeiderman (Protected Disclosure 7)
b. The 17 September 2018 email from the claimant to Mr Zeiderman (Protected Disclosure 8)
c. The letter of 29 November 2018 (wrongly dated as August) that Mr S [REDACTED] had sent to Ms Wood.”
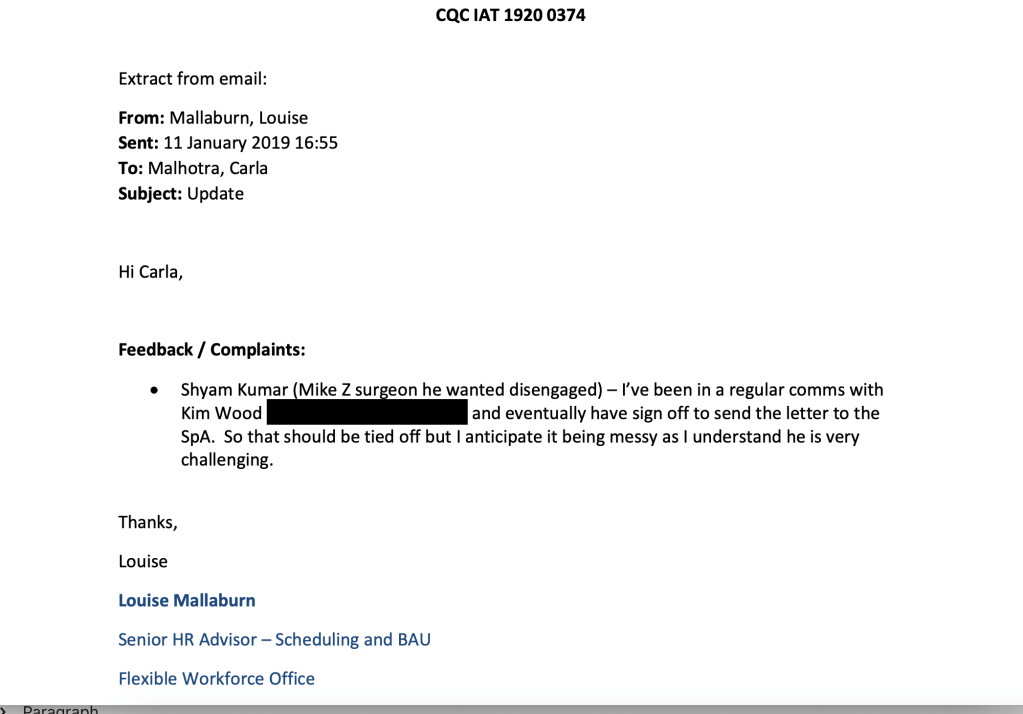
The dismissive and disrespectful attitude is echoed in later emails by Louise Mallaburn CQC Senior HR Advisor who wrote that Mr Kumar was “very challenging” and in another email made a sarcastic comment about him writing long emails.
The unfair dismissal by CQC
In November 2018 a CQC inspection took place at UHMBT, Mr Kumar’s trust.
Mr Kumar wrote to Kim Wood CQC inspector to express concerns that one of his persecutors at the trust, Dr S, might make inappropriate and damaging comments about him during the inspection.
This proved to be a realistic fear as Dr S did indeed make false and highly damaging claims about Mr Kumar during a CQC focus group.
The ET noted that Dr S’s remarks were inappropriate in that forum:
“In this meeting, Mr S [REDACTED] raised a number of issues which the Investigating Manager, Ms Helen Vine, considered were not appropriate for the Focus Group.”
The ET found that Mr Kumar was entitled to feel upset and injured by the serious attack on his character, probity and standing:
“The matters raised by the claimant, in his letter to Mr S [REDACTED], were serious issues. The claimant, if these matters were true, had the right to feel upset, in particular with the matters that were probity matters or race. All involved in this case accept that allegations concerning probity, bias and racism are serious matters and could have impacted on the claimant’s fitness to practise.”
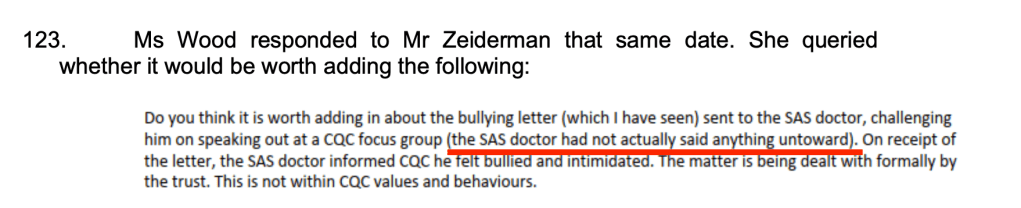
Extraordinarily though. Kim Wood later wrote to Mike Zeiderman on 6 May 2019, when they were deciding how to respond to a request for information by the CQC Chair’s office, that Dr S had not said “anything untoward”.
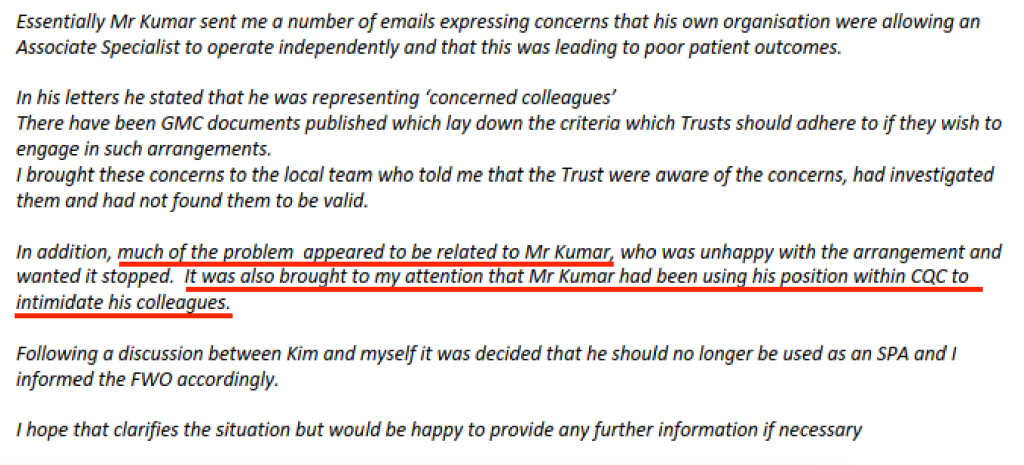
On the same day, Mike Zeiderman’s drafted a response to the CQC Chair, which cast Mr Kumar as the problem and undermined his credibility as a whistleblower:
This dismissal of Mr Kumar’s experience of whistleblowing reprisal contrasted with the CQC’s over reaction to counter-claims by Dr S.
After the above CQC focus group, Mr Kumar wrote a letter to Dr S with advice from the BMA, setting out his concerns about Dr S’s conduct. He proposed steps for resolution. The ET accepted that this was a good faith attempt to resolve the matter
“The letter sent by the claimant to Mr S [REDACTED] was an attempt to resolve matters informally, before making any decision as to whether to pursue a formal process. This is in line with the policies and procedures adopted by both the respondent and the employing Trust. We accept the claimant’s evidence on this, which is consistent with the wording in the letter that he sent to Mr S [REDACTED], in which he is seeking to resolve the situation. This is also consistent with the approach the claimant took after this letter was sent.”
However, the CQC seized on the fact that Mr Kumar had written a letter to Dr S as a means of dismissing him.
This is correspondence in which Mike Zeiderman instructed HR to sack Mr Kumar and informed Kim Wood of the sacking:
CQC sent a letter accusing him of several counts of poor conduct, of which three out of four were eventually withdrawn.
CQC’s line of attack thereafter focussed on a vague claim that Mr Kumar’s letter to Dr S proposing a resolution was in fact improper and a breach of CQC’s values.
CQC maintained this line of attack throughout the ET proceedings. During the June ET hearing, which I attended via web link, CQC’s witnesses made much of Dr S’ alleged response to Mr Kumar’s letter. The CQC contended that the definition of bullying includes the “victim’s” experience and it claimed that Dr S was so distressed by Dr K’s letter that the letter should be viewed as bullying.
The ET did not accept this.
In his evidence to the Employment Tribunal, Mike Zeiderman said that he had seen the letter from Mr Kumar to Dr S, before sacking him.
Damningly, the ET did not believe this:
“102. On balance we find that before 06 December 2018, Mr Zeiderman had not seen the letter that the claimant had sent to Mr S [REDACTED]. Although Mr Zeiderman in his oral evidence said he had seen the letter, the evidence before the tribunal suggests on balance that he did not see it by this date.“
That is, the central reason claimed by the CQC for dismissing Mr Kumar – his letter to Dr S – had not even been examined by Zeiderman at the point of the decision to dismiss Mr Kumar.
The ET determined that CQC’s dismissal of Mr Kumar was a “forgone conclusion” and therefore unfair.
“Disengaging the claimant was a foregone conclusion at the point the claimant was informed that he was placed on hold, and in those circumstances it is not plausible that it is a neutral act.”
The ET considered that Mr Kumar had been sacked by the CQC because he had whistleblown:
145. Given our findings above, it is very clear that the emails and concerns raised by the claimant in the form of protected disclosures had a material influence on the decision to disengage him. Amongst other reasons, this is particularly because of:
a. The reasons provided by Mr Zeiderman for disengaging the claimant appeared to develop throughout the period between the decision to disengage him on 06 December 2018 and his correspondence Mr Matt Wood from the Private Office Correspondence Unit, and into these proceedings. This and the lack of reference to the alleged offending letter to Mr S [REDACTED] a form the claimant, casts great doubt on that being the reason for disengagement and placing on hold of the claimant.
b. The correspondence with the claimant disengaging him provides little in terms of explaining in what way his behaviour fell below the expected behaviours or values of the respondent. And there was no detail as to what in the letter from the claimant to Mr S REDACTED] offended those principles. This again casts doubt on this being the sole reason, with other matters being trivial in the decision making process, for the decisions made.
c. During the phone call between Mr Zeiderman and Ms Wood in early December 2018, when Mr Zeiderman formed the view that the claimant could no longer be used as a special advisor, the claimant had at the forefront of his mind the emails which he had received from the claimant over the course of 2018. The emails that he is referring to include a number that are protected disclosures, or more specifically Protected Disclosures 2-10.”
The Tribunal determined that the CQC made no proper and reasonable investigation prior to dismissing Mr Kumar and that it failed to protect him as a whistleblower:
“Alongside this, this tribunal is mindful that this is a case where the claimant was being disengaged for having conducted himself in a manner not befitting of the respondent, without any proper and reasonable investigation. Where his professionalism was being questioned, and his action, which was later used as the reason for disengagement was in response to that. Where he had made the decision-makers aware of potential retaliatory action against him, and no safeguards were put in place. Against this backdrop, the decision to disengage him clearly reaches the level of detriment.”
CQC dismissed Mr Kumar without an appeal process, claiming that its policies allowed it to sack him without appeal, and that this was CQC’s normal practice.
The ET considered that this was unreasonable employer behaviour, and a detriment.
Thus it follows that the CQC is operating an oppressive employment practice, which takes no heed of natural justice.
CQC dug for dirt
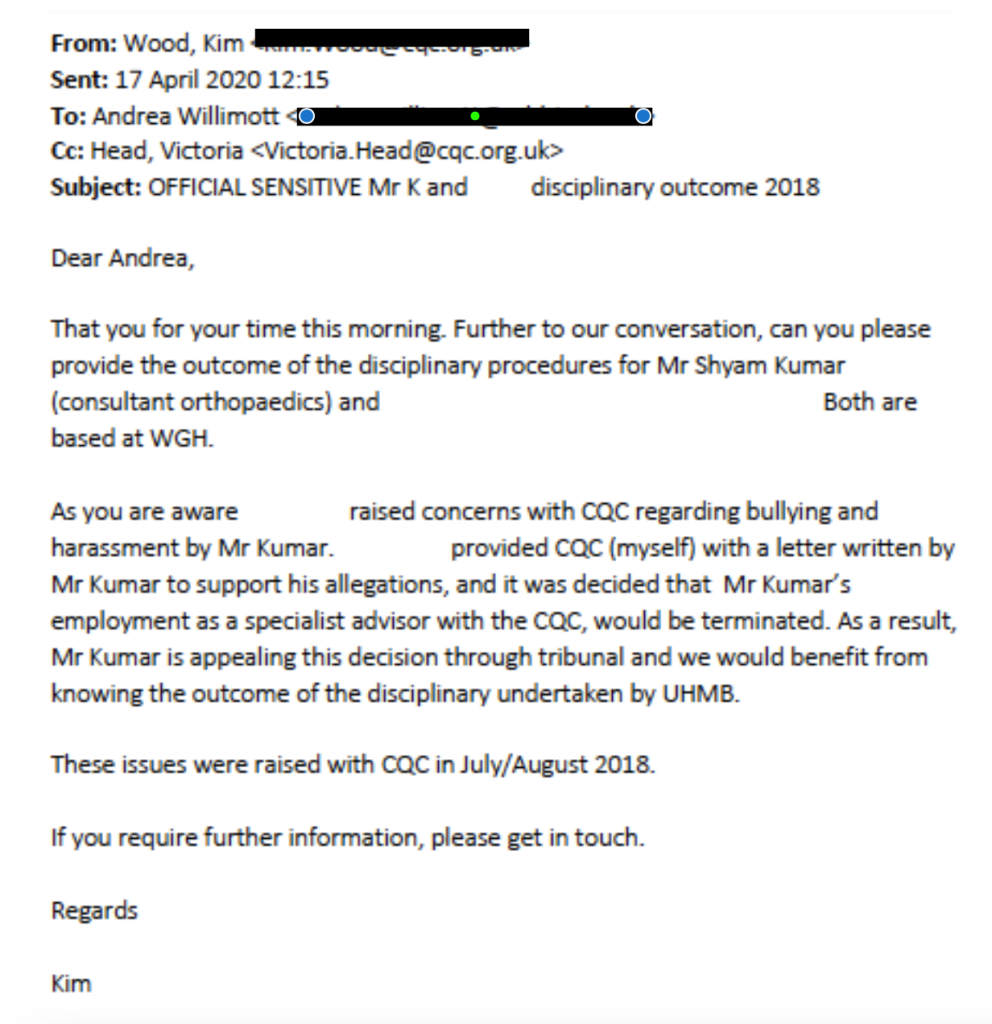
One of the most extraordinary aspects of this case is that CQC sought to retrospectively justify its arbitrary and unfair treatment of Mr Kumar by placing pressure on his employer (University Hospitals Morecambe Bay NHS Foundation Trust, UHMBT) to give it dirt on Mr Kumar.
After Mr Kumar filed an ET claim against CQC for whistleblower detriment, the CQC asked UHMBT for information about UHMBT’s disciplinary action against Mr Kumar for his letter to Dr S, when no such disciplinary action ever took place.
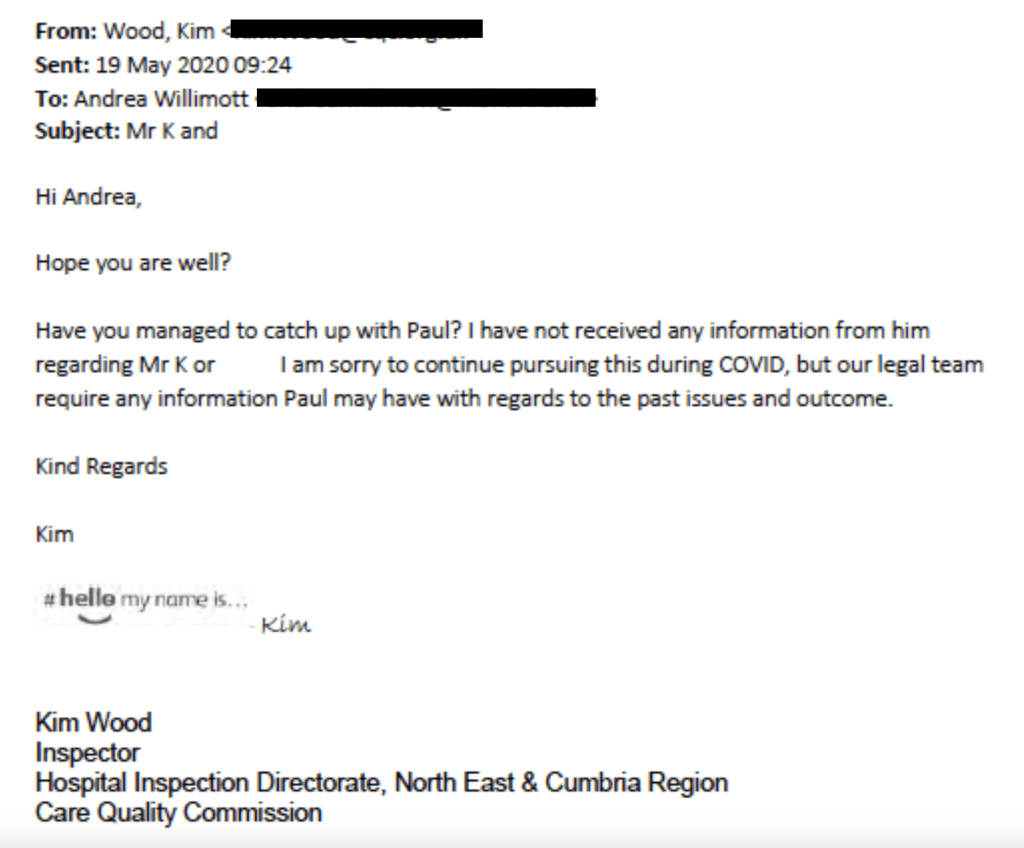
A month later, Kim Wood pursued UHMBT staff for “past issues” about Mr Kumar that could be useful to CQC’s lawyers:
In fact, the ET noted that Dr S, for all the CQC’s protestations of injury on his behalf, never even filed a grievance against Mr Kumar.
The fact that the regulator would ask a regulated body for information that was outwith the regulatory process, and was in fact requested for self-serving reasons, seems a most serious matter.
Especially when that purpose is to retrospectively justify the regulator’s poor treatment of a whistleblower.
This seems to me to be a gross abuse of power.
It would be for a lawyer to opine on whether it amounts to Misconduct In Public Office.
The CQC makes false counter-allegations against whistleblowers
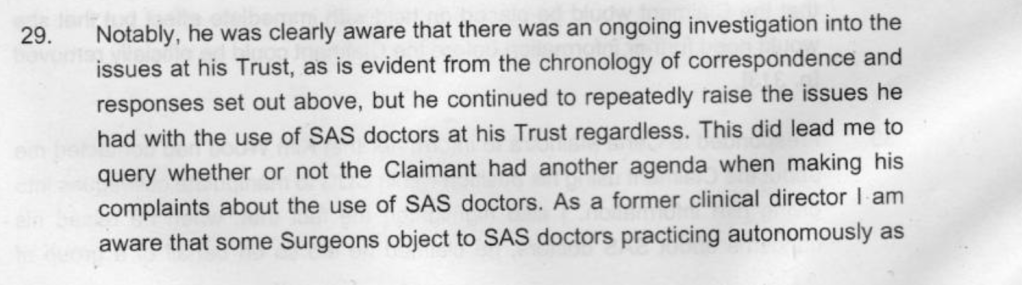
As part of its defence strategy against Mr Kumar’s claim to the Employment Tribunal, the CQC sought to portray his whistleblowing about the unsafe practice of a single doctor as an attack on all the SAS (non-consultant grade) doctors at his trust, for potential financial gain.
Mike Zeiderman’s witness statement to the Tribunal repeatedly claimed that Mr Kumar was “targeting” SAS doctors because some were allowed to work autonomously.
Zeiderman accused Mr Kumar of abusing his position as a CQC Specialist Advisor to intimidate others. Almost no particularisation was given of this alleged intimidation or the basis of the accusation.
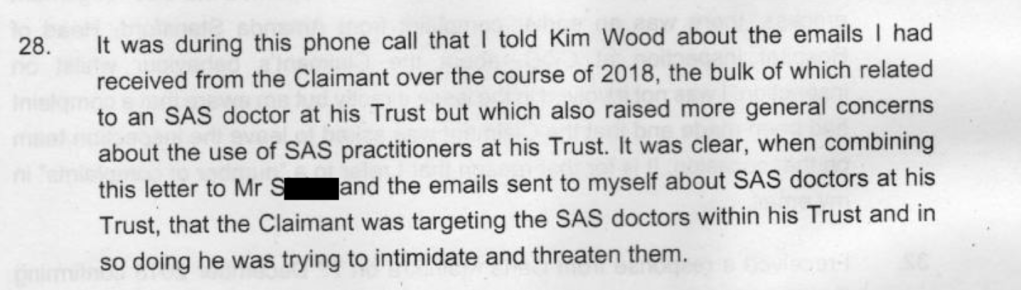
Zeiderman’s witness statement claimed that a motive for attacking SAS doctors might be that their work to reduce waiting lists affected on the private income of consultant surgeons, as waiting lists encouraged patients to seek private treatment.
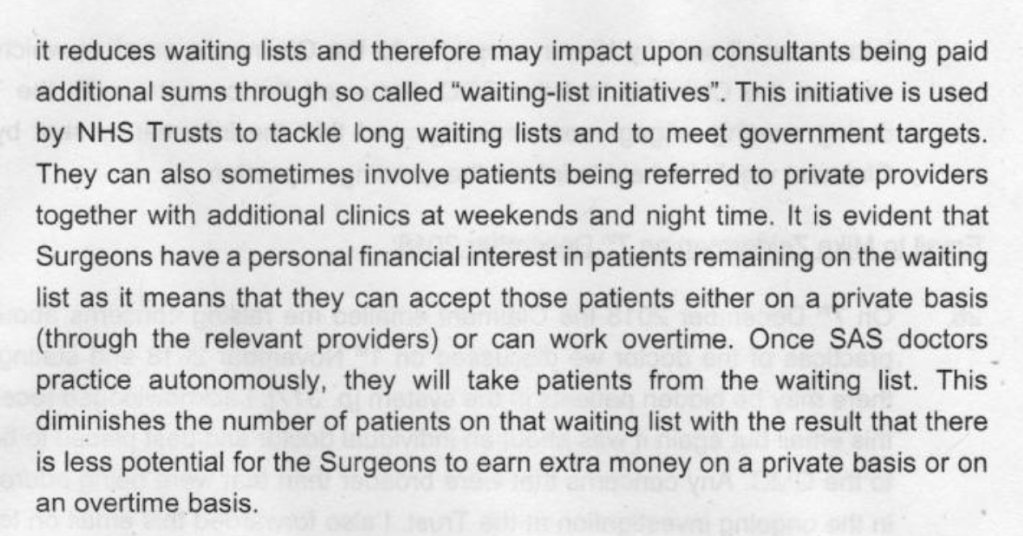
There was no basis for this suggestion that Mr Kumar might benefit financially. Dr X was helping to reduce trust waiting lists for LOWER limb cases such as hip and knee replacements. Mr Kumar is an UPPER limb surgeon.
But such a serious allegation about a doctor’s probity would normally require a fellow doctor to refer the individual to General Medical Council, as part of their professional obligations to safeguard patients. The CQC did NOT refer Mr Kumar to the GMC, despite Zeiderman stating clearly in his witness statement that CQC sacked Mr Kumar for reasons of probity:

Moreover, Louise Mallaburn repeated untrue claims about Mr Kumar in correspondence, which were very harmful to his reputation. The false claims are highlighted below:
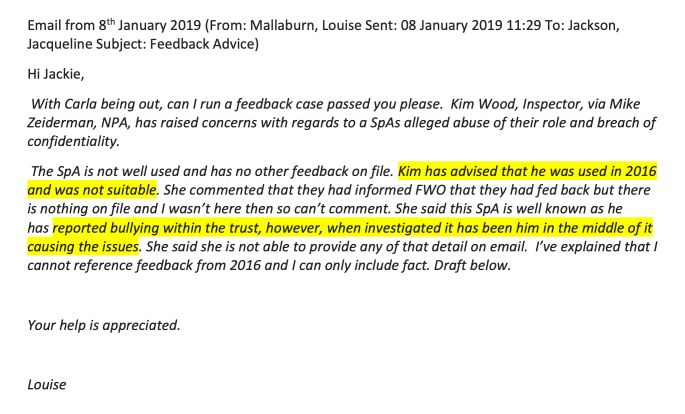
This is correspondence from Mr Kumar’s trust, UHMBT, which confirmed that there had never been any such record of bullying and harassment on his file:
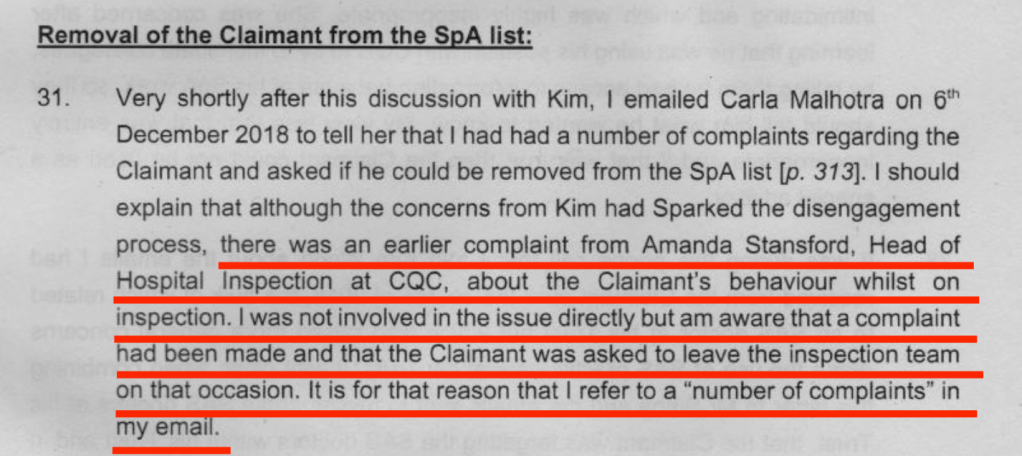
The false allegation by Louise Mallaburn in her email of 8 January 2019 that Mr Kumar was not often used by the CQC because he had previously been found to be “unsuitable”, was later echoed in Mike Zeiderman’s witness statement of 30 October 2020. In this statement, Zeiderman claims Mr Kumar was asked to leave a CQC inspection [in 2015]. This was false because it was Mr Kumar who made a complaint about Amanda Stanford’s conduct,, AFTER the end of the 2015 inspection.
The CQC doesn’t act on whistleblowers’ concerns
Mr Kumar has never received a satisfactory response from the CQC regarding the whistleblowing concerns that he raised with Mike Zeiderman and subsequently with other senior CQC managers.
This is an email of 16 May 2019 by Mr Kumar to the CQC noting this failure:
Months later a letter by the CQC Chief Executive to the Secretary of State in August 2019 conceded that the CQC had yet to address all of Mr Kumar’s concerns:
“I will ensure that where any of Mr Kumar’s concerns remain outstanding we address those as soon as possible.”
The CQC does not apologise or back down
More serious than an original failure are failures to learn and to take responsibility.
CQC directors rejected Mr Kumar’s complaint about his mistreatment. They stood by their man, Mike Zeiderman.
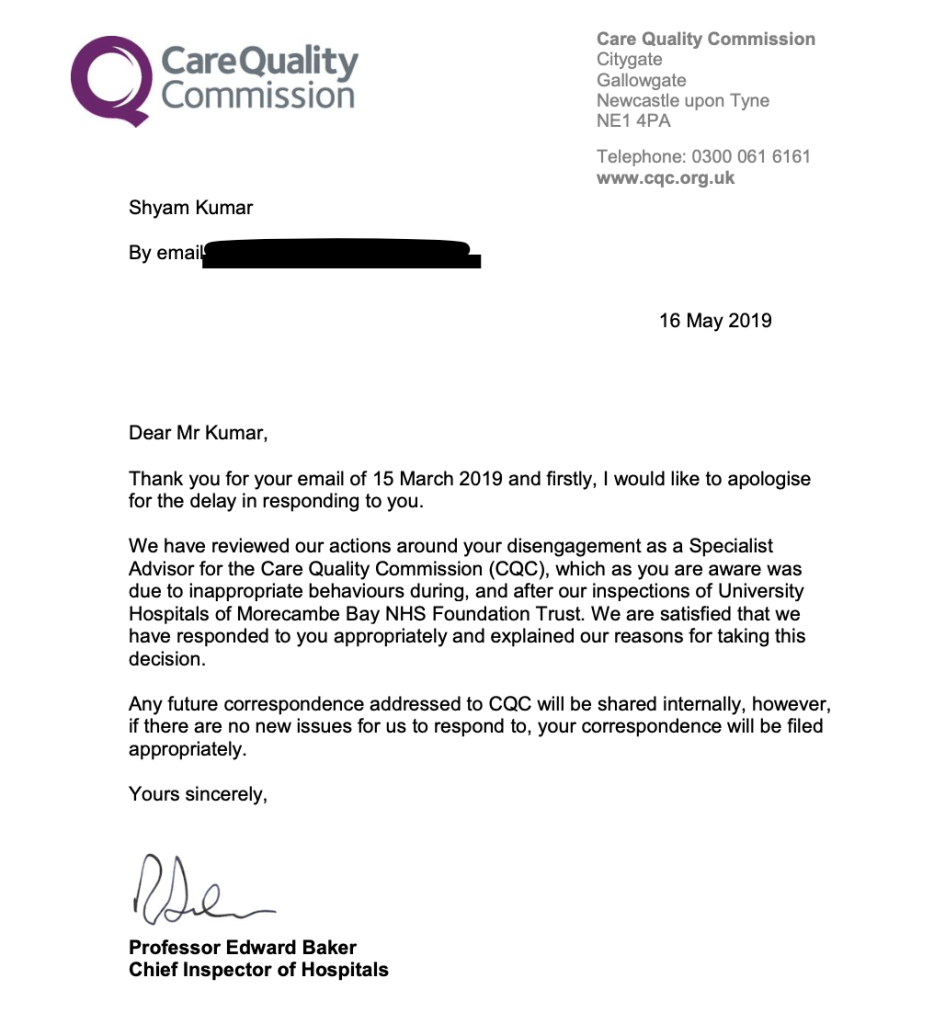
The final letter from CQC, sent by Ted Baker Chief Inspector of Hospitals, dismissing Mr Kumar’s complaint is painful to read:
By August 2019, CQC PR staff conferred on what “line” to take in explaining CQC’s conduct to Matt Hancock, then Health Secretary:
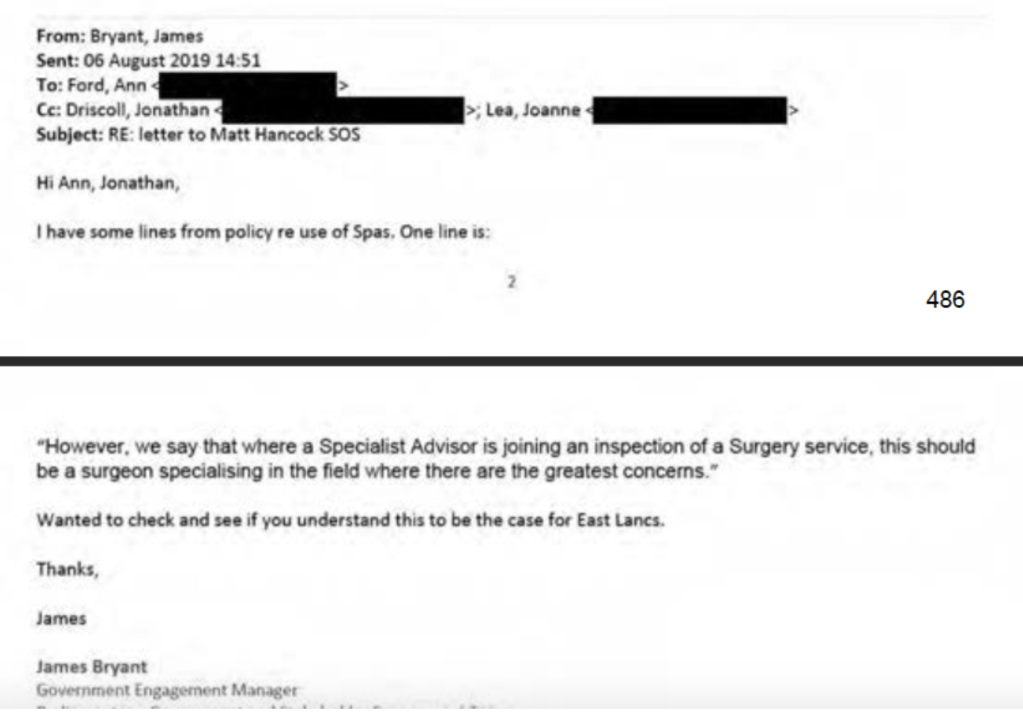
The CQC informed the Health Secretary that Mr Kumar had been dismissed because of poor behaviour. The regulator through its Chief Executive Ian Trenholm confirmed Mr Kumar had been expected to inspect areas where he was not expert, but it denied that there was anything wrong with its inspection methodology. This was despite CQC’s own National Professional Advisor Mike Zeiderman stating in his ET witness statement that he agreed with Mr Kumar that Specialist Advisors should not be asked to inspect areas in which they were not expert, and that this was an acknowledged problem nationally on which the CQC had been working.
Mr Kumar complained to the PHSO about his treatment by the CQC: The CQC fed false information to the PHSO about Mr Kumar being on a zero hours contract.
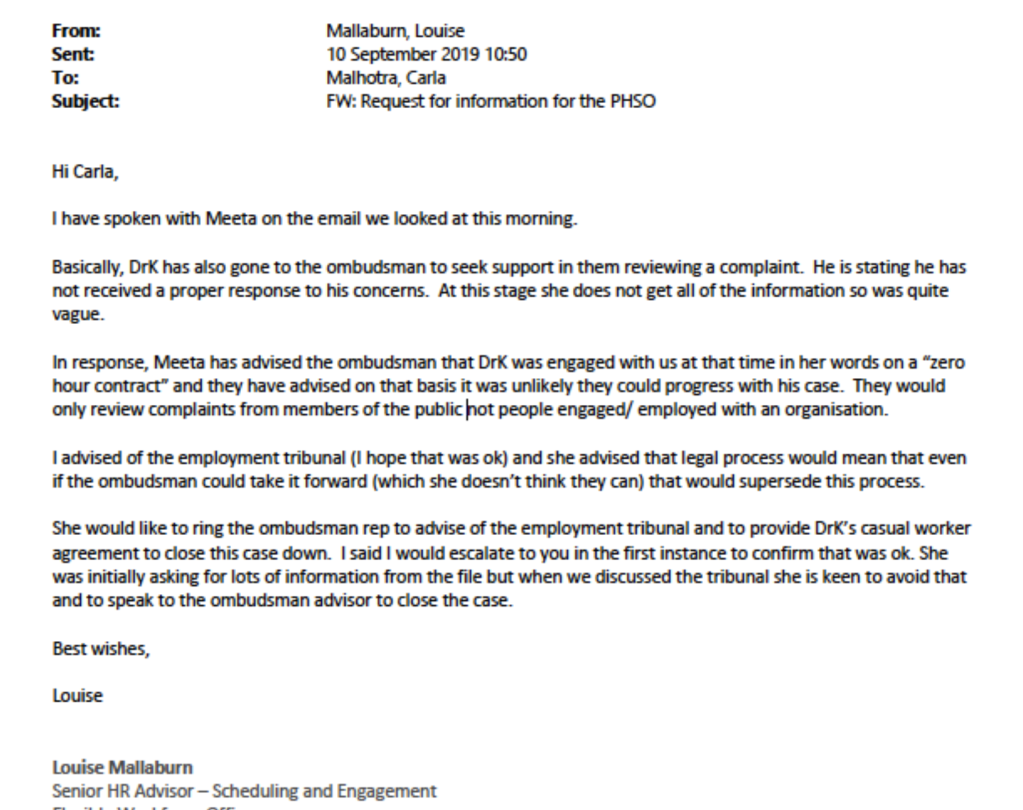
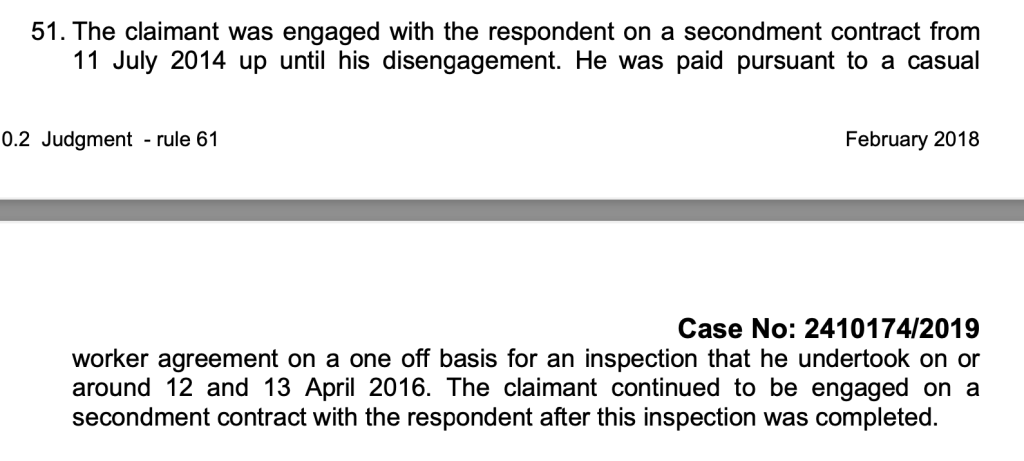
Mr Kumar was in fact on a secondment contract, as determined by the ET.
CQC continued to denigrate Mr Kumar during the initial ET proceedings in 2021, branding his claim of whistleblower detriment by the CQC as branding his claim of whistleblower reprisal by the CQC as “fanciful”. I witnessed similar tactics by the CQC during the June 2022 hearing.
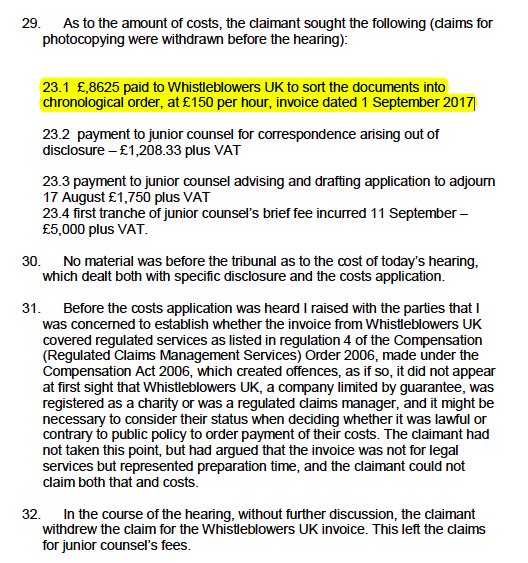
Also, in 2020 the CQC made an application for wasted costs but this was denied by the ET.
Accountability
So in short, it would seem that the CQC:
- Failed to protect a whistleblower
- Failed to act on his concerns
- Failed to accept that his whistleblowing was valid, minimised his concerns and saw the whistleblowing as a nuisance and a threat
- Mistreated the whistleblower seriously and smeared him
- When challenged by the whistleblower sought to portray him as a difficult and “challenging”, and ridiculed his claim of whistleblower reprisal by the CQC
- Tried to dig dirt about the whistleblower to retrospectively manufacture a case justifying its mistreatment, abusing regulatory power in the process
- Fed false information to the Ombudsman to shut down a legitimate complaint by the whistleblower about his mistreatment by the CQC
- Claimed reasons for its treatment of the whistleblower which were not believed and were rejected by the ET, calling into questions the truthfulness of the claims
- Operated oppressive HR policy and practice, but foolishly and incompetently maintained up to the last minute that its processes were fine.
I asked the CQC press office to comment on whether it believes it has anything to learn from Mr Kumar’s case, and whether the CQC personnel involved in these serious governance failures should continue in CQC’s employ and hold responsibility for vulnerable patients and service users. I received no reply. I then asked the new CQC Chair Ian Dilks to comment, and have not so far received a reply.
One also has to wonder, if the CQC as an organisation would have been quite so blind to Mr Kumar’s professional credentials and standing, and his professionalism in standing up for patients, or treated him so contemptuously, had he been a Caucasian doctor.
Although the CQC vilified him and caused Mr Kumar and his family so much hurt, it seems clear that he has done all whistleblowers, especially Health and Social Care whistleblowers, and the public a great service.
He defended the truth despite the huge strain involved. This was at a time of personal tragedy when his wife, a fellow senior medic, almost died of COVID and spent 107 traumatic days in ITU.
Mr Kumar has exposed the nature of the CQC, and a Court has resoundingly agreed with him.
The question now is, what accountability will there be for this almighty mess and injustice?
The CQC sacked Mr Kumar for purportedly breaching its values.
But it is in fact the CQC who has been found to have breached its values, which require CQC personnel to protect whistleblowers.
This is a key CQC value from the regulator’s internal whistleblowing policy, “The CQC Guardian and the Freedom to Speak Up. CQC’s policy on raising and dealing with concerns at work“:
Will anyone be disciplined or sacked for the harm to Mr Kumar as a whistleblower and the harm to the public interest?
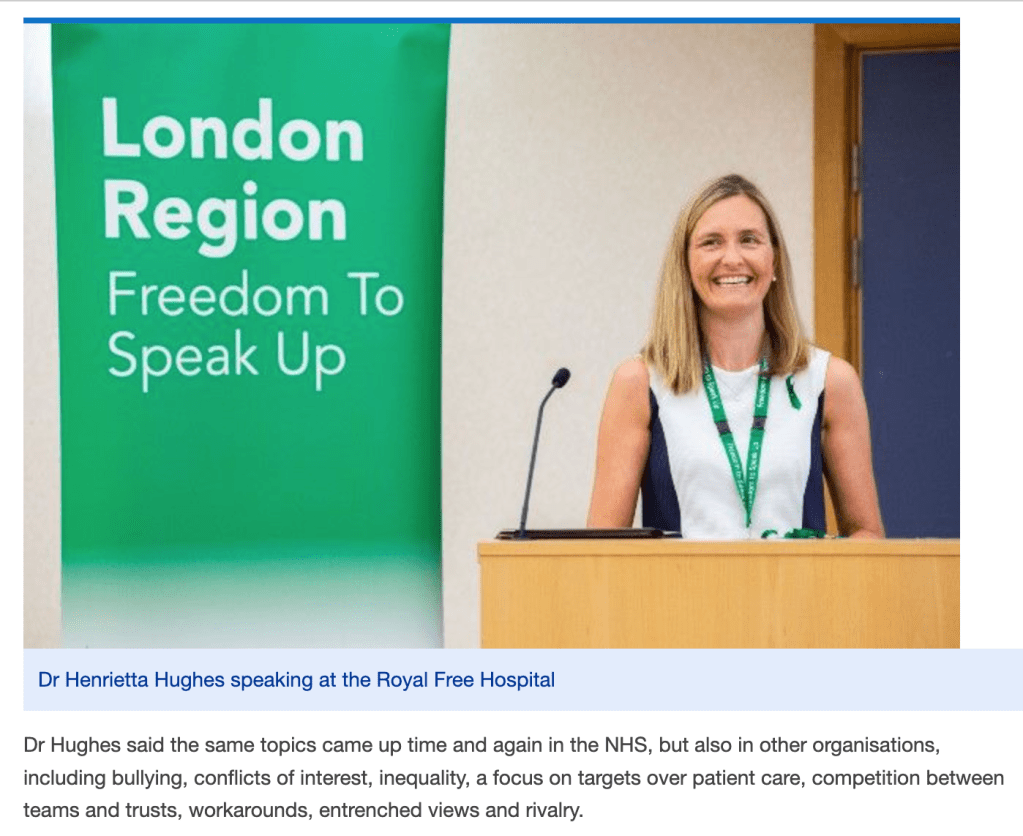
Mr Kumar and his BMA representative asked the then NHS National Freedom To Speak Up Guardian Henrietta Hughes to review the issues raised by his case, but no case review has ever materialised.
But then, why would the National Guardian seek to challenge her employer, the CQC?
That would take the courage of a whistleblower.
I have asked Steve Barclay the Health Secretary to protect Mr Kumar and his family from further trauma and to prevent a wasteful appeal against the ET judgment by the Care Quality Commission, an arms length body of the Department of Health and Social Care.

Appendix: CQC dramatis personae
These are individuals at the CQC who either took an active part in handling Mr Kumar’s case or were party to the case from being copied into correspondence.
Ian Trenholm CQC CEO
Ted Baker CQC then Chief Inspector of Hospitals, just selected by Steve Barclay the Health Secretary as the new Chair of the Healthcare Safety Investigation Branch, where he will join ex Chief Inspector of Primary Care, Rosie Benneyworth of FPPR mishandling fame.
Henrietta Hughes former National Freedom To Speak Up Guardian, now comfortably embedded at the DHSC as Patient Safety Commissioner for medicines and devices
Mike Zeiderman CQC National Professional Advisor, Consultant Colorectal Surgeon Southport and Ormskirk
Ann Ford CQC Deputy Chief Inspector of Hospitals
Victoria Head CQC Inspection Manager
Nicola Kemp CQC Hospital Inspection Manager
Kim Wood CQC inspector
Jonathan Driscoll CQC Inspection Manager
Carla Malhotra CQC Human Resources Business Partner
Jacqueline Jackson CQC Head of HR Services and Business Partners
Louise Mallaburn CQC Senior HR Advisor
James Bryant CQC Government Engagement Manager
And of course, the regrettable CQC legal department belong on this list.
It is also very likely that Peter Wyman the CQC Chair would have been apprised of Mr Kumar’s case, given the political sensitivity.
Amanda Stanford, about whom Mr Kumar raised concerns in 2015 regarding CQC obstruction of his efforts to speak to trust whistleblowers during an inspection, was in 2017 promoted to CQC Deputy Chief Inspector of Hospitals.
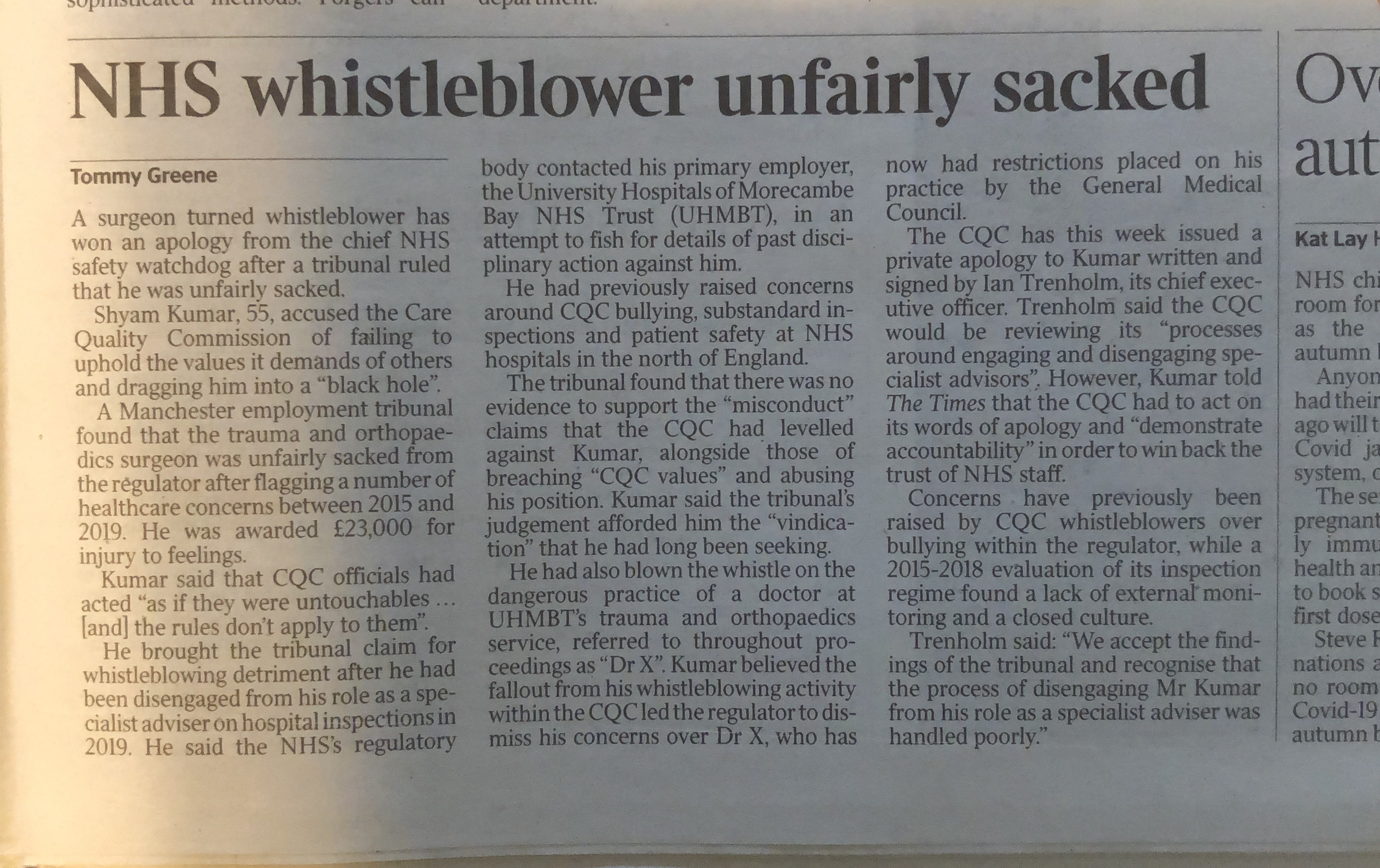
This is press coverage from July 2022 of Mr Kumar’s evidence to the ET about bullying culture at the CQC, and his complaint about Amanda Stanford’s conduct:
‘Bullying culture’ at NHS watchdog, says ex-inspector
In 2019, Amanda Stanford walked through the ever spinning CQC revolving door and became the Director for Quality and Patient Safety at Airedale NHS Foundation Trust and in 2021 she was appointed Chief Nurse of the trust.
In keeping with the grand traditions of the NHS, Amanda Stanford’s Airedale NHS Foundation Trust biographical profile states:
“Amanda has an active interest in developing compassionate leadership, quality improvement and how education and training and creating a just and learning culture.”
I have written to Steve Barclay Health Secretary to ask that he ensures Mr Kumar’s concerns about the CQC are properly addressed, and that he ensures that the CQC will not appeal against the ET judgment and inflict further suffering on Mr Kumar and his family.
Letter to Steve Barclay 5 September 2022 re Mr Shyam Kumar and CQC misconduct
The BBC has today broken the news of the ET’s decision in Mr Kumar’s favour:
NHS whistleblower Shyam Kumar wins case against regulator
UPDATE 6 SEPTEMBER 2022
I have written to the BEIS Secretary about serious failure of the ramshackle system of “Prescribed Persons” under flawed UK whistleblowing law, arising from Mr Kumar’s case and others. Prescribed Persons such as the CQC have minimal legal duties and are too often complicit or directly responsible for harm to whistleblowers.
UPDATE 8 SEPTEMBER 2022
The British Medical Journal has covered Mr Kumar’s case, including his comments on accountability for CQC’s terrible failure of governance:
This means that large swathes of the NHS workforce will be apprised of the regulatory failure and forewarned about CQC’s unreliability as a Prescribed Person.
In the current political and regulatory landscape, I advise whistleblowers to consider whistleblowing directly to the media, either on an anonymous basis or with protection of identity. Take careful advise before doing so, as there are legal tests to fulfil if you wish to maintain protected status under current UK whistleblowing law.
UPDATE 9 SEPTEMBER 2022
CQC has responded briefly only to the media breaking the scandal of Mr Kumar’s case. It claimed in correspondence and through a media statement that it had already learned lessons and made improvements. However, it provided little evidence of these claimed improvements.
Today, it responded to an enquiry that I made about learning lessons and whether those implicated in Mr Kumar’s whistleblower victimisation should remain in the CQC’s employ, and in positions of public trust.
The CQC response today was brief and minimal but of note, referred in the future tense to learning lessons from Mr Kumar’s case:
“We accept the findings of the Employment Tribunal and will consider lessons to be learned from the judgement.” (my emphasis)
UPDATE 13 SEPTEMBER 2022
On 12 September 2022 the Health Service Journal provided further coverage of Mr Kumar’s case, in which it highlighted the Employment Tribunal’s findings on evidence by Mike Zeiderman, CQC National Professional Advisor:
“The unimpressed tribunal judge, meanwhile, said Mr Zeiderman’s explanation for terminating the contract “appeared to develop” in the months after his decision “and into these proceedings”.
HSJ also drew attention to the fact that the ET revealed Mr Kumar’s trust had “hidden” evidence of serious patient harm:
Trust ‘hiding serious harm and death’ report
The Times also covered Kumar v Care Quality Commission on 12 September 2022:
UPDATE 22 SEPTEMBER 2022
The CQC has stated explicitly, in response to a question to the CQC board from @JadeTaylor8, that it will not be appealing Kumar v Care Quality Commission:
Starts 1:48 into the video:
Ian Trenholm CQC CEO: “Thanks very much Ian, this I think Jade is referring to the recent case involving Mr Kumar. Just for clarity we’re not appealing that judgment and I have no intention of doing that. I think it is worth saying we have very few Employment Tribunal cases. In the round, we have a handful at any one time and very few of them actually proceed to a Tribunal. I think it would be difficult for us to make a blanket statement that we were never going to appeal an ET but but U think it is something that would be really very much by exception. So I think it is something we take very seriously. Thank you for the question Jade. Thank you.”
Ian Dilks CQC Chair: “[Inaudible first few words]….it links to the public purse that is something we have to take account of. That means we have to look into each case on its merits rather than making blanket statements about what we would do.”
PETITION
Please click and add your signature to this petition to reform UK whistleblowing law – whistleblowers protect us all but weak UK law leaves them wholly exposed, lets abusers off the hook and it is a threat to public safety.
Replace weak UK whistleblowing law and protect whistleblowers and the public
RELATED ITEMS:
This is not the first time by far that seconded CQC Specialist Advisors have criticised CQC’s poor inspection methodology and chaotic approach.
I know of doctors who tried the role but resigned due to the problems described by Mr Kumar in his disclosures to the CQC.
Hugh Cannell a former CQC specialist advisor committed his experiences and concerns to paper, in this article of 2019, thus contemporaneous with Mr Kumar’s struggles with the CQC:
RCS Bulletin H Cannell, The CQC and Specialist Advisors. Who shall inspect the inspectors?
Importantly, Cannell notes that instances of trust staff whistleblowing were not always reflected in CQC inspection reports.
How many more doctors have raised concerns with the CQC about its poor regulatory performance, but have been ignored, silenced or harmed?
The CQC’s dreadful history of handling whistleblowing within both its own organisation and provider bodies speaks for itself.
The Tulloch review into orthpaedics safety issues at UHMBT – see page 60 onwards
Serious Case Review into Winterbourne Hospital Abuse
Witness statement of Amanda Pollard CQC whistleblower, to the Mid Staffs Public Inquiry
Resignation letter 26 January 2016 and disclosures by Barry Stanley Wilkinson, CQC whistleblower
Counting the cost of the CQC: Abuse, Whorlton Hall and CQC spin doctors
Mr Tristan Reuser’s whistleblowing case: Scandalous employer and regulatory behaviour on FPPR
CQC’s Victimisation of Whistleblowers: Failure to Investigate Concerns
More CQC denial about collusion with employers against whistleblowers
Carl Beech, CQC inspector, convicted child sex offender and fraudster: Activities at the CQC
CQC’s Asleep on the Night Shift
CQC case study. Snooping. Briefing. Porkies. And vexatiously applied ‘vexatious’ protocols.
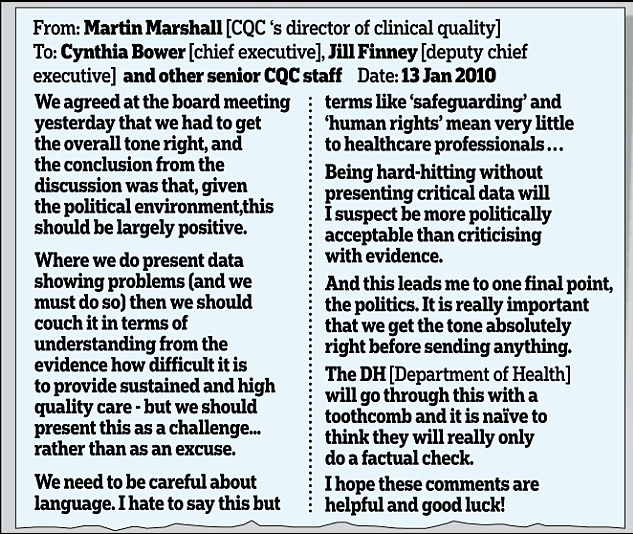
Source: https://www.dailymail.co.uk/news/article-2443051/Labours-cover-failing-hospitals-Ministers-tried-silence-watchdog-eve-general-election.html