
By Dr Minh Alexander, NHS whistleblower and former consultant psychiatrist, 22 September 2020
Summary: Professional regulators are not doing enough to identify, track and manage abusive employers who maliciously refer their staff to their professional regulators. Last month I reported that the Health and Care Professions Council had no systems at all for dealing with these issues, and that the regulators’ regulator, the Professional Standards Authority indicated to me that it would welcome evidence of malicious referrals. Since then, staff who have suffered malicious referrals or witnessed them have been sending in evidence. I provide here more detailed evidence on the HCPC’s systemic failings in respect to whistleblower registrants and to NHS ambulance trusts. There is an astonishing laxity by both the HCPC and employers on assuring the quality and probity of referrals. NHS staff may suffer severe personal injury as a result of oppressive workforce management. Several NHS whistleblowers have reported that they have experienced heart problems in the last year. These organisations are not holding themselves to the same professional and ethical standards that are so sternly heaped on the frontline. It is time for the unions and the PSA to do more to protect frontline staff from abuse. I have written to both.
Background
Professional regulators are supposed to keep the public safe by managing practitioners’ impaired fitness to practice and also to be fair to frontline health and care staff.
It is a challenging balancing act, and there have been failings in both directions.
There have been egregious examples of professional regulators’ failure to keep the public safe. For example, the repeated failures by the General Medical Council to stop Jane Barton the doctor associated with the suspicious opioid deaths at Gosport, Ian Paterson the breast surgeon who was eventually jailed and Zholia Alemi the fake doctor who was allowed to masquerade as a consultant psychiatrist despite not even having a basic medical degree, also jailed and expected in court again today on further charges. Whistleblowers repeatedly tried to raise the alarm on all three of these cases, but insufficient regulatory action resulted.
Juxtaposed against this is a serious failure to track rogue employers who misuse the professional revalidation and Fitness to Practice procedures as a tool for coercing staff and silencing whistleblowers. Professional regulators have very little in the way of systematic approaches to deter employer abuse. Their institutional focus is on erring staff, and as Mark Twain once said: “To a man with a hammer, everything looks like a nail”.
The HCPC
HCPC lets rogue employers off and does not track whistleblowers who are referred
I reported previously that the Health and Care Professions Council has no system whatsoever for tracking and tacking action against rogue employers, even though I am aware that whistleblowers have been vexatiously referred to the HCPC.
I contacted the Professional Standards Authority about this. PSA indicated that it would “welcome” evidence about vexatious referrals to professional regulators. I have since seen some of the submissions that affected whistleblowers and other workers have been sending in about professional regulators.
I will now report further on the HCPC’s handling of referrals by NHS ambulance trusts and its approach to whistleblowers.
In an FOI disclosure of 17 September 2020, the HCPC showed a lack of care and understanding about employers’ vexatious referrals on whistleblower registrants.
When I asked if HCPC had a policy on handling employers’ referrals on whistleblowers, it merely directed me to a generic policy for workers who wish to whistleblow to HCPC – a completely different issue.
Moreover, HCPC admitted that:
- It had not been aware of the 2015 Hooper report for the GMC on good practice in cases of whistleblower registrants who are referred
- It did not ask senior registrants who make referrals to declare whether the practitioner being referred is a whistleblower
- It held no central record of whistleblowers who are referred: “we do not hold a central record on whistleblowers who are referred to the HCPC”
Indeed, the HCPC previously admitted that it keeps no central register of malicious referrals.
I have seen recent correspondence from the HCPC to a vexatiously referred registrant in which HCPC declined to log a referral as malicious.
On 20 August 2020 I asked Christine Elliott Chair HCPC and her colleagues to do more to deter malicious referrals in general:
“I wonder if the HCPC can consider this very serious issue of power imbalance and unfairness and let me know whether and how it might be prepared to correct its omission.”
There has so far been silence in response to this request.
Shockingly, the HCPC has also been failing to fully meet its public sector equality duty under the Equality Act, to track how it is responding to people with different protected characteristics. An FOI disclosure to another party showed that HCPC bizarrely only collects data on age and gender. Nothing on other protected characteristics such as Race and Disability. Its board also looks distinctly white. This serious failure adds to the concerns about whether HCPC is protecting the workforce from unfairness by referring employers.
I have raised this major failure with the Professional Standards Authority, which responded to say that it recently added a requirement for professional regulators about diversity and equality. The correspondence with PSA can be found here.
Ambulance trusts
I am aware of vexatious referrals by NHS ambulance trusts to the HCPC, on whistleblowers and other staff.
One referred individual who has had a terrible ordeal commented that the HCPC’s handling of referrals can be a huge part of the problem:
““The HCPC are, without a doubt the most unprofessional organisation I have ever had to deal with.”
There are 10 English NHS ambulance trusts, which form a subculture of their own, with the highest levels of bullying in any category of NHS trusts.
Yet their workers carry out high pressure emergency work, sometimes in dangerous conditions, facing abuse or even assault by the public, and witness terrible, traumatic scenes. They need the best quality employer support.
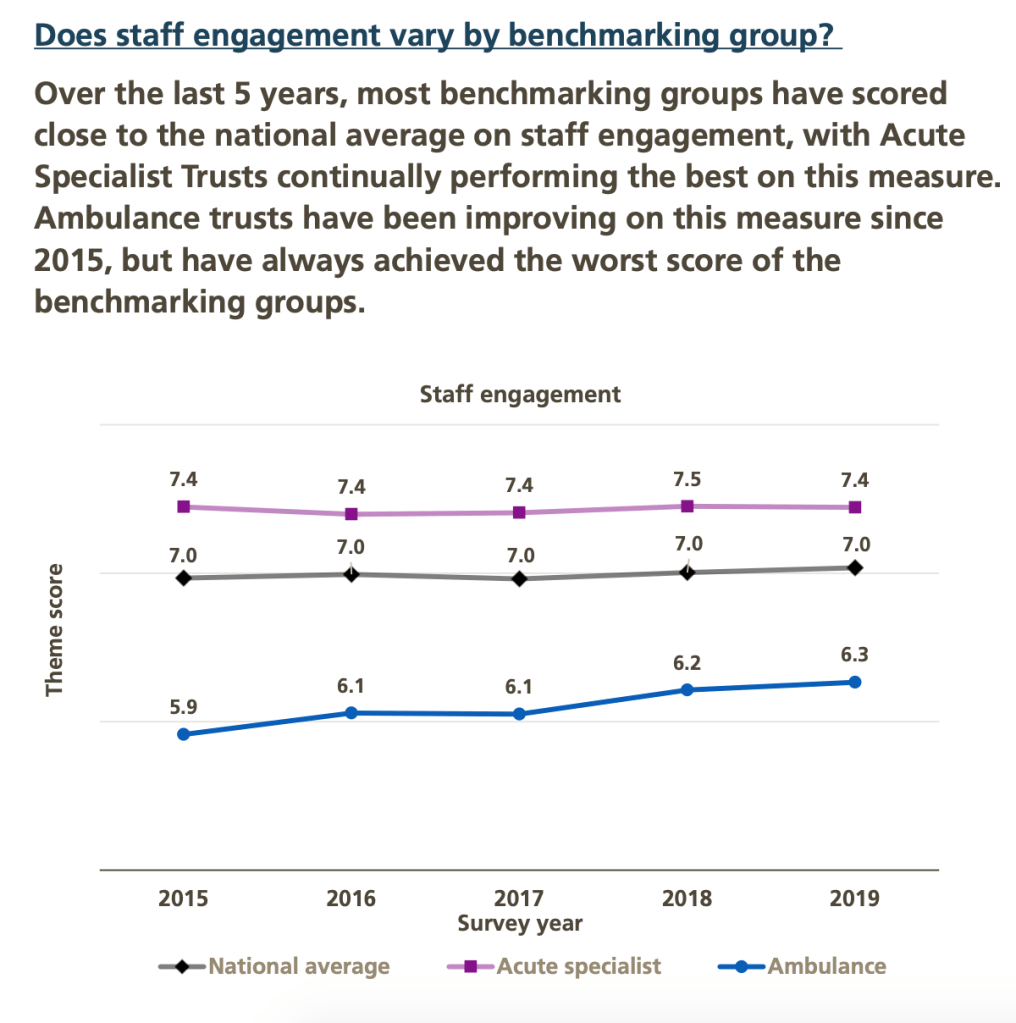
The last NHS staff survey continued to show what a difficult employment environment ambulance trust workers face.
Ambulance trusts have by far the lowest levels of staff engagement:
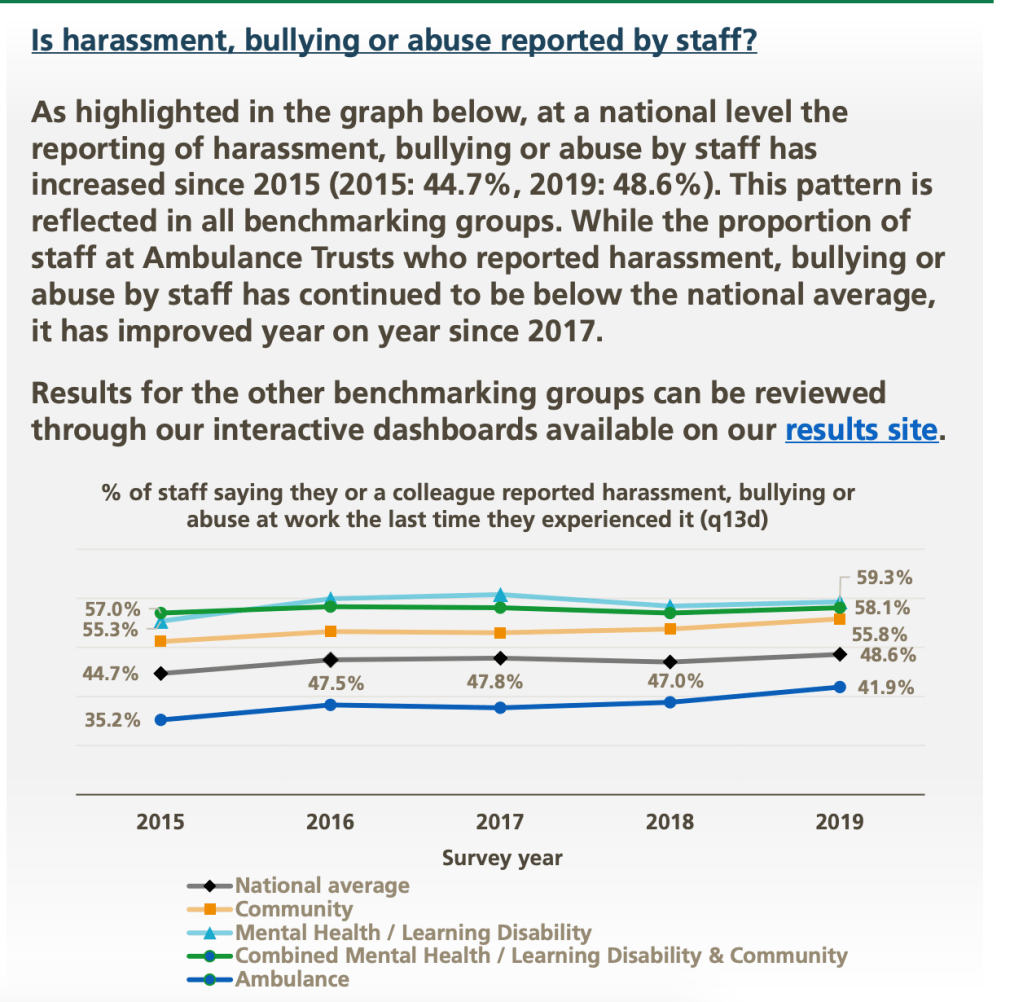
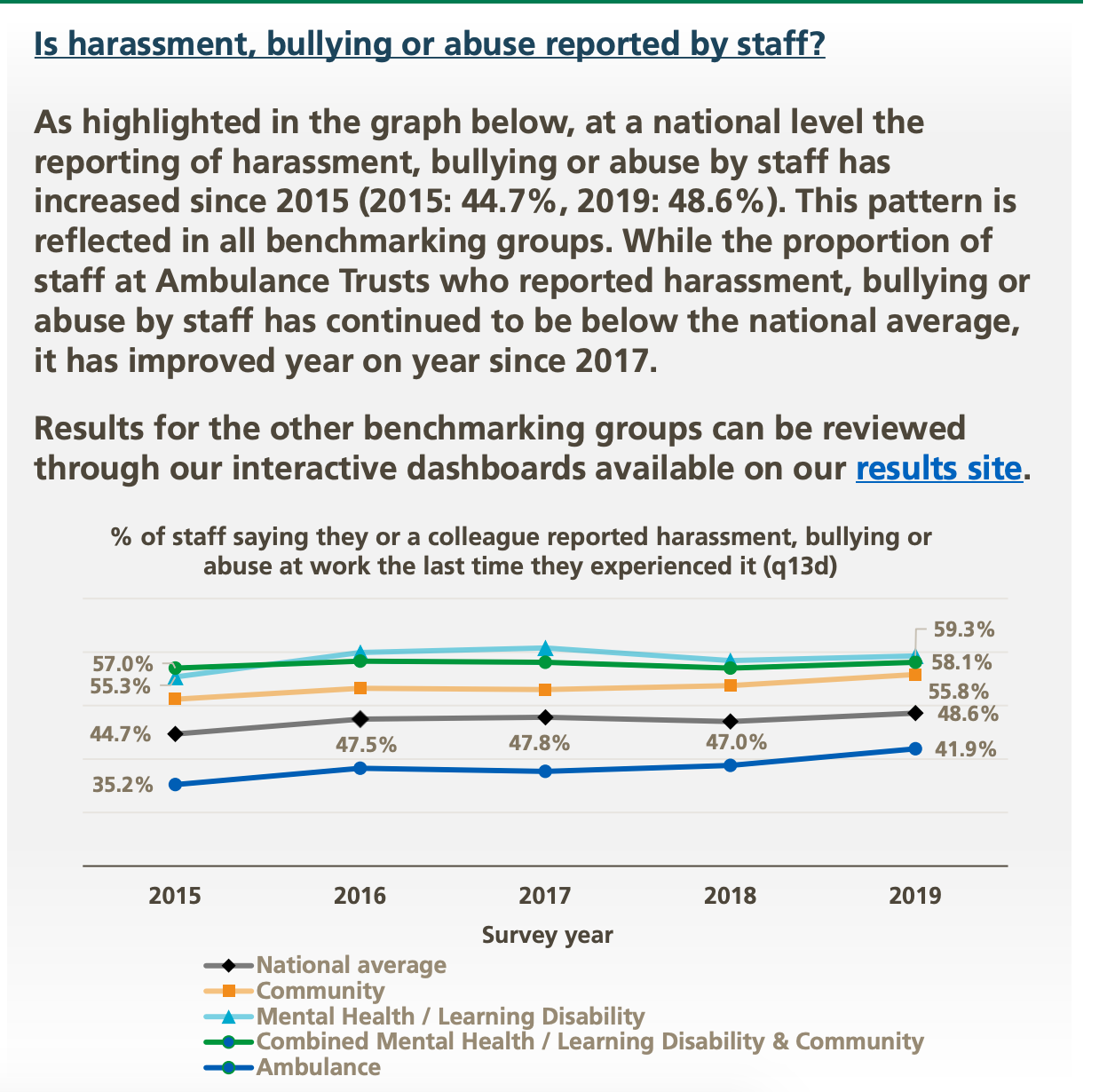
Ambulance trust staff report the highest levels of bullying:
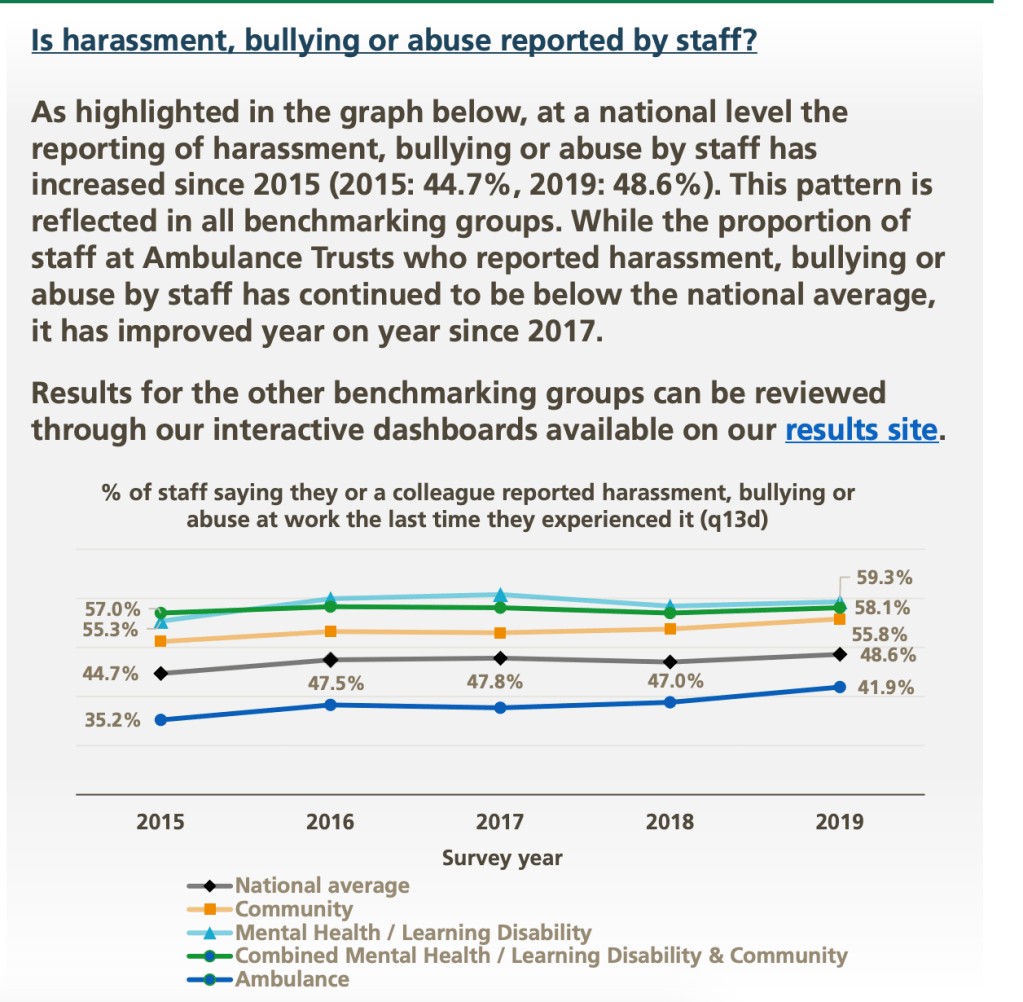
These high levels of disclosed bullying are despite ambulance trust staff being less ready than other groups to report bullying:
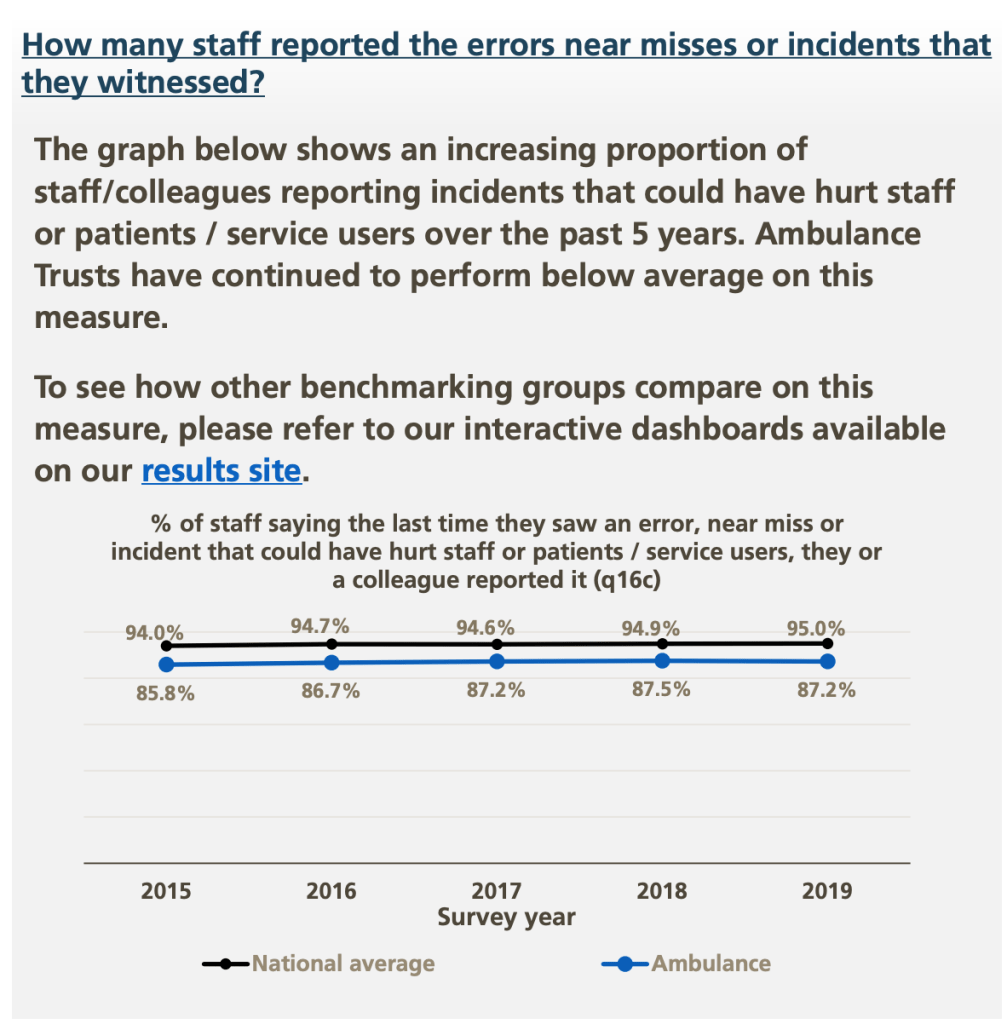
Ambulance trust staff are also less likely to report safety incidents:
Ambulance workers are also the least likely to feel secure when raising concerns about unsafe care:
| TYPE OF NHS TRUST | % of staff who agreed with the statement: “I would feel secure raising concerns about unsafe clinical practice.” |
| All trusts | 72% |
| Acute trusts | 70% |
| Combined acute and community trusts | 72% |
| Acute specialist trusts | 74% |
| Mental health and learning disability trusts | 72% |
| Combined mental health, learning disability and community trusts | 74% |
| Community trusts | 78% |
| Ambulance trusts | 68% |
Source: NHS Staff Survey 2019, detailed results https://minhalexander.com/wp-content/uploads/2020/08/nhs-staff-survey-2019-detailed-results-st19-detailed-spreadsheets_final.xlsx
Ambulance trust workers are the least confident that their employer would address concerns:
| TYPE OF NHS TRUST | % of staff who agreed with the statement: “I am confident that my organisation would address my concern.” |
| All trusts | 60% |
| Acute trusts | 58% |
| Combined acute and community trusts | 60% |
| Acute specialist trusts | 67% |
| Mental health and learning disability trusts | 59% |
| Combined mental health, learning disability and community trusts | 63% |
| Community trusts | 67% |
| Ambulance trusts | 55% |
Source: NHS Staff Survey 2019, detailed results https://minhalexander.com/wp-content/uploads/2020/08/nhs-staff-survey-2019-detailed-results-st19-detailed-spreadsheets_final.xlsx
To get some idea of the scale of meritless and or frankly abusive referrals to HCPC by ambulance trusts, I asked both the HCPC and ambulance trusts for data.
The HCPC response was very poor and claimed that the regulator held no central data by ambulance organisation on numbers and outcomes. This implied that HCPC fails to track referrals by individual organisations and is not actively assessing whether employers may be misapplying or abusing Fitness to Practice procedures. Alternatively, HCPC may be able to call up the data, but wishes to shield employers from scrutiny. HCPC decisions quite often refer to paramedic’s employing organisations, so it is surprising that the HCPC cannot produce the data.
This is the full FOI correspondence with HCPC:
HCPC FOI Numbers and outcomes of referrals to HCPC by NHS ambulance trusts
HCPC’s poor approach is of particular concern because concerns had already been raised that some groups of registrants, such as paramedics, are referred at disproportionately higher levels. The concerns had resulted in research being commissioned from Surrey University, reporting in 2017:
People like us? Understanding complaints about paramedics and social workers1
This report by Surrey noted that paramedics faced a “blame focussed” work environment.
Ambulance trusts’ FOI responses to my enquiries about HCPC referrals since 1 April 2018 showed:
- South Central Ambulance Service NHS Foundation Trust has not responded despite reminders
- Three ambulance trusts have not bothered at all to oversee and evaluate how they make HCPC referrals (South Western Ambulance Service NHS Foundation Trust, which had major bullying issues, and West Midlands Ambulance Service NHS Foundation Trust, dubiously rated ‘Outstanding’ by CQC, and Yorkshire Ambulance Service NHS Trust)
- Two trusts (North East Ambulance Service NHS Foundation Trust and London Ambulance Service NHS Trust) held numbers on referrals but not outcomes
- There was a great range in the numbers of referrals. South East Coast Ambulance Service NHS Foundation Trust had not referred any staff to HCPC in the period.
- North West Ambulance NHS Trust – a whistleblowing and severe bullying hotspot known to both regulators and the National Guardian – made 20 ‘personal misconduct’ referrals, with 4 ending in a “No case to answer” finding by the HCPC, and 9 ‘clinical practice/ patient care concerns’ referrals, with 3 ending in a “No case to answer” finding by the HCPC. Whistleblowers at this trust have continued to be harmed after an ineffective review by the National Guardian.
- East of England Ambulance Service Trust – which has had recent paramedic suicides answered in a muddled way, giving all sources of referral and thus obscuring the number of ‘no case to answer’ outcomes arising specifically from referrals by the trust
The FOI responses from ambulance trusts can be found linked below. I will add the overdue response from South Central as it arrives.
North West Ambulance Service NHS Foundation Trust
East of England Ambulance Service NHS Trust
West Midlands Ambulance Service NHS Foundation Trust
South Western Ambulance Service NHS Foundation Trust
Yorkshire Ambulance Service NHS Trust
East Midlands Ambulance Service NHS Trust
North East Ambulance Service NHS Foundation Trust
London Ambulance Service NHS Trust
South East Coast Ambulance Service NHS Foundation Trust
NHS Trusts and the HCPC should in particular actively track the ‘no case to answer’ referral outcomes for possible learning, and it is a concern that this is not happening most of the time.
This all paints a picture of neglect and casual abuse of the frontline. People who save lives, who work so hard and under such pressure, yet are so easily discarded upon employer whim, with regulatory complicity through lack of duty of care.
Alongside this is the still casual way in which NHS staff can be suspended with very few safeguards and no central tracking, despite a 2003 National Audit Office recommendation for substantial systemic improvements to be made.
The mistreatment of staff in these summary ways is extremely serious and causes personal injury, sometimes life threatening. I am in touch with several NHS whistleblowers who have experienced heart problems just in the last year. It is also not just staff but their family who suffer. Linda Faircliffe, North Tees and Hartlepool NHS Foundation Trust whistleblower, tragically lost her partner to a heart attack whilst the trust suspended her.
Innocent staff can be pinned down by vexatious referrals for years, especially where a professional regulator is especially incompetent.
It is inconceivable that a safety critical sector can lurch on in this dangerous way, with lazy tolerance of poor culture.
The NHS Chief People Office Prerana Issar’s office promised on 7 September 2020 that Issar would shortly respond to a prompt on 26 August 2020 about the much delayed implementation of the Kark Review on unfit NHS senior managers and continuing impunity for whistleblower reprisal but she has not done so yet.
The unions should be cracking down harder on these failures and so should PSA.
I have written to the PSA cc the unions, to forward the above further evidence of professional regulatory failure to deter employers’ abuses of power.
All the above is a glimpse into the weak systems that favour employers and allow whistleblowers to be silenced.
If you have not done so already, please sign and share the petition to reform UK whistleblowing law, so that there is a legal duty on bodies to protect whistleblowers and to deter reprisal with effective penalties.
Petition: Replace weak UK whistleblowing law, and protect whistleblowers and the public
APPENDIX
CORRESPONDENCE WITH PSA
BY EMAIL
David Martin, Concerns and Appointments Officer, Professional Standards Authority
22 September 2020
Dear David,
More examples of professional regulatory failure to deter vexatious Fitness to Practice referrals on frontline workers, as a means of intimidation and punishment
To follow up on my concerns about the Health and Care Professions Council admitting to having no systems whatsoever for identifying, tracking and managing rogue employers and its failure to fully track protected groups of registrants (it only tracks age and gender), please find via this link more evidence of HCPC failure to address employer abuses of the Fitness To Practice process as an improper means of punishment:
This additional evidence focuses on ambulance services, which have troubled culture and whose staff suffer the highest levels of bullying in the NHS.
Importantly, please note that as part of HCPC’s failures, it has little understanding of the importance of ensuring that whistleblower registrants who are referred need to be properly protected and that vexatious referrals on such registrants need to be identified and robustly deterred.
Thank you again for picking up the general issue of how professional regulators should manage vexatious/ malicious/ dishonest referrals.
I hope some improvements can be made in due course.
You will note amongst this latest evidence the fact that I have heard from several NHS whistleblowers who have suffered from heart problems in the last year relating to the immense stress of employer reprisals. There is the terrible case of Linda Fairhall, North Tees and Hartlepool NHS Foundation Trust whistleblower, whose partner died of a heart attack when she was suspended by her employer.
The problem is of course relevant to all workers, whistleblowers or not.
I hope this helps to illustrate the gravity of system and professional regulators allowing employers to get away with seriously abusive behaviour and coercing the workforce through this means.
With best wishes,
Minh
Dr Minh Alexander
Cc
Alan Clamp CEO PSA
Secretaries of TUC, Unison, Unite, GMB, HCSA, BMA, RCN, DAUK
NMCWatch Registrant Care
RELATED ITEMS


{kind=link}
Thank you for a deeply shocking report.
Yet again, we see those who are amongst the most responsible and involved in frontline activities being treated appallingly (whilst, I imagine those sheltering behind mahogany desks, being protected).
I can find nothing positive to say other than I am very glad you are on the case.
Kindest,
Z
LikeLike