
| Please sign and share:
Petition to replace weak UK whistleblowing law to protect whistleblowers and the public |
By Dr Minh Alexander NHS whistleblower and former consultant psychiatrist, 1 June 2017
Ian Paterson the surgeon at the centre of a colossal NHS governance failure was yesterday sentenced to 15 years imprisonment. 1
These are the judge’s sentencing remarks:
r-v-paterson-sentencing-remarks-mr-justice-jeremy-baker-20170531
Both Paterson’s NHS and private practice has been subject to hundreds of negligence claims.
For years, he carried out so-called cleavage sparing mastectomies for breast cancer without patients’ consent, which were not accepted practice, and which raised concerns that he had left patients at greater risk of cancer recurrence. He was also found to have fraudulently carried out unnecessary surgery by deceiving patients and colleagues.
Paterson was made subject to restrictions on his practice, which included GMC restrictions introduced in 2011.
A 2013 review by Sir Ian Kennedy into Paterson’s NHS practice at the Heart of England NHS Foundation trust found that weak management failed to challenge Paterson or to ensure that he adhered to restrictions on his practice and that whistleblowers were repeatedly ignored: 2
“3.41 For the future, and reflecting on the past history of the NHS, Dr Stockdale’s dilemma could not be more challenging. He had taken what he, and contemporaries in the NHS, would see as a risk: he had drawn attention to the practice of a senior colleague, outside his specific area of expertise, and criticised it. He had blown a whistle. Whistleblowers do not fare well in the NHS. This is one of the major indictments of management in the NHS: that it is inwards-looking, over-defensive, and prone to destroy, by a variety of means, those who suggest that the Emperor has no clothes. This is not unique to this Review. It is a blight on the NHS and is one of the principal areas where lessons must be learned. This was the context in which Dr Stockdale and his colleagues had to wrestle with what to do.”
Kennedy also noted that Rex Polson Consultant Physician, who had been asked to investigate allegations against Paterson in 2007, 2b had made these comments about raising concerns in the NHS:
“Dr Polson, who was asked by the Trust to conduct a parallel investigation with Mr Hennessy in 2007, told me that he did not explore the challenge of raising concerns when he spoke to the oncologists. But, he told me, the prevailing culture at the time was that raising the issue “was probably as much as you were able to do, or you looked to move and change job”. It would be difficult to imagine a bleaker indictment of the reality of the time. And, he added, the patients were not complaining, because “they did not know that they should be complaining”, which made it that much more difficult for one professional to rock the boat by accusing another.” 2
A Verita report about Paterson’s private practice at Spire Parkway resulted in similar findings to Kennedy’s. 3
It was evident that concerns about Paterson’s breast surgery were raised from at least 2003 and other concerns were raised before that. 2 3 4
The trust was woefully slow in recalling patients 2 and there are doubts about whether HEFT has really come clean. The trust has given conflicting information on some occasions. Also, HEFT only recalled Paterson’s mastectomy patients but not those who had wide local excisions and lumpectomies. 5 10
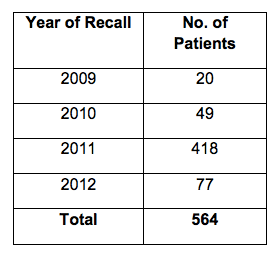
This is data from HEFT 10 on the numbers of Paterson’s NHS patients who attended HEFT’s recall clinic by year:
Debate continues about whether HEFT was correct to assert on some occasions that the cancer recurrence rate from Paterson’s cleavage sparing mastectomies was within the expected range.
Shockingly, Paterson’s private patients have been denied compensation as the private provider and Paterson’s former medical defence body the MDU have denied liability.6
Arguments have been made that the NHS may be liable for compensating Paterson’s private patients because it took insufficient action to warn private providers.
Some of the issues, FOI disclosures and other source documents are collated below.
Chief Executives at Heart of England throughout the period of interest
Mark Goldman 2001 to 2010
Mark Newbold 2010 to 2014
Andrew Foster January to October 2015
Julie Moore 2015 to present
What HEFT says about Paterson’s NHS patients
As of 30 May 2017, HEFT maintained via FOI 5224 7 that :
- 1207 trust patients had received a cleavage sparing mastectomy from Ian Paterson.
- At the time the trust recalls started, 387 of these 1207 patients had already died. (In FOI disclosure 5157 of 6 April 2017, HEFT advised that by 31 March 2017 an additional 288 of Paterson’s mastectomy patients had died. 8)
- Of the remaining patients who were still alive when recalls started, 697 were invited to a recall clinic, and 564 of these individuals attended.
- To HEFT’s knowledge so far 68 of as HEFT puts it, the ‘alive mastectomy cohort’, have experienced recurrence of breast cancer.
Verita reported that in September 2009:
“HEFT’s medical director writes to Ruth Paulin [Spire Health hospital director] to tell her that West Midlands Cancer Intelligence audit found that the five-year recurrence rates for invasive cancer for Mr Paterson’s patients were within acceptable limits. At the time these findings were accepted by Spire as assurance that Mr Paterson’s practice was safe.” 3
Crucially however, Kennedy and Verita noted that this was only half the story:
“1.24 In Sir Ian Kennedy’s Review of the response of HEFT to concerns about Mr Ian Paterson’s surgical practice (2013) he reported that HEFT’s medical director had been advised by the director of the West Midlands Cancer Intelligence Unit (WMCIU) on a number of occasions before 2009 that Mr Paterson’s rates of recurrence were not accurate because the WMCIU did not have all of Mr Paterson’s data.” 2 3
The Kennedy report detailed the warnings to HEFT from the WMCIU and Kennedy observed: “Mr Paterson was an outlier in terms of his general rate of recurrence and evidence was emerging that patients undergoing at least one particular procedure and, perhaps, others were at a high risk of suffering a recurrence.” 2
HEFT later produced a report on Paterson’s outcomes which conceded:
“The analysis suggests that in patients who underwent the unapproved procedure (CSM) there is an increased risk of the cancer returning to the same site (local recurrence) in the long term, requiring further treatment.” 9
BUT HEFT claimed on 6 April 2017 that:
“The figures suggest that the outcomes for Mr Paterson’s patients are not outside the expected norms” 8
On 11 April 2017, via FOI 5138, HEFT also incongruously claimed:
“The Trust is unable to provide any statistically meaningful interpretation of these recurrence figures. Mr Paterson’s first operations occurred in the early 1990s and he was not excluded from the Trust until 2011. National breast cancer survival figures have changed over this period.” 10
Moreover, HEFT now indicates that there has been no analysis of the cases of CSM patients who had died and whether their deaths were related to recurrence of breast cancer:
“There has not been an analysis of the deceased patients to determine who may have had a CSM or other type of incomplete mastectomy; the Trust’s efforts have been to focus on reviewing the patients who are alive to ensure that they are having the best individualised care and advice possible in these distressing circumstances.” 7
(This is despite a previous claim that it had undertaken “A review of all NHS patients believed to have had a mastectomy under the care of Mr. Paterson – 1071”. 9)
If no analysis has been conducted of the deaths, it is difficult to see how HEFT was able to conclude that Paterson’s outcomes were within the expected range.
HEFT now also admits that it did not inform its trust governors of the Paterson issues until 2010. 7
In terms of action taken to protect Paterson’s private patients, HEFT wrote to the private provider Spire Healthcare in 2007, but has refused to place the contents of the correspondence into the public domain. 11
Whistleblowing at HEFT
HEFT has a poor reputation in general for whistleblowing governance.
There have been numerous whistleblowers, who have raised concerns about Paterson’s practice but also other matters, some of whom have reported experiencing reprisal. 12 13
This was despite HEFT’s then chief executive Mark Newbold jumping onto the Speak Out Safely bandwagon in 2013, with an accompanying publicity splash in the Nursing Times. 15
Since CQC started publishing its so-called ‘intelligent monitoring’ reports, all five of the CQC intelligent monitoring reports on HEFT have flagged whistleblowing alerts (21 October 2013, 13 March 2014, July 2014, December 2014, May 2015). 16
The CQC holds data about concerns that it received from HEFT whistleblowers, but claims that it is unable to account for whistleblowing contacts from HEFT staff before 2011, as it did not keep central records before 2011. 17
In other words, the CQC has apparently not bothered to pull this vital pre-2011 whistleblowing information from its records, despite the great scandal and grave patient harm.
The CQC has disclosed that since 2011 it has received 51 whistleblowing contacts from HEFT staff. This number of external whistleblowing disclosures flags issues of troubled institutional culture. 17b
| Financial year | Number of whistleblowing contacts to CQC by HEFT staff |
| 2011/12 | 1 |
| 2012/13 | 9 |
| 2013/14 | 15 |
| 2014/15 | 12 |
| 2015/16 | 11 |
| 2016/17 year to date | 3 |
| Total | 51 |
Source: CQC database on whistleblowing by HEFT staff
The concerns raised with CQC about HEFT since 2011 have been diverse and included unsafe discharges, anomalies in recording of cancer waiting times, prioritisation of targets over quality, overcrowding to achieve targets, staffing levels and staff stress, nepotism and conflicts of interest.
According to CQC’s recorded outcomes on these whistleblowing incidents, CQC mostly either just noted whistleblowers’ concerns as information for future inspection, or accepted trust assurance that matters were in hand. This seems unacceptably lax given HEFT’s past failures.
HEFT itself responded incompletely to my FOI request about whistleblowing events at the trust by omitting data about the nature of whistleblowing concerns by staff and about its compliance with government standards.
Moreover, HEFT ignored a follow up request to disclose all of the requested data. 18
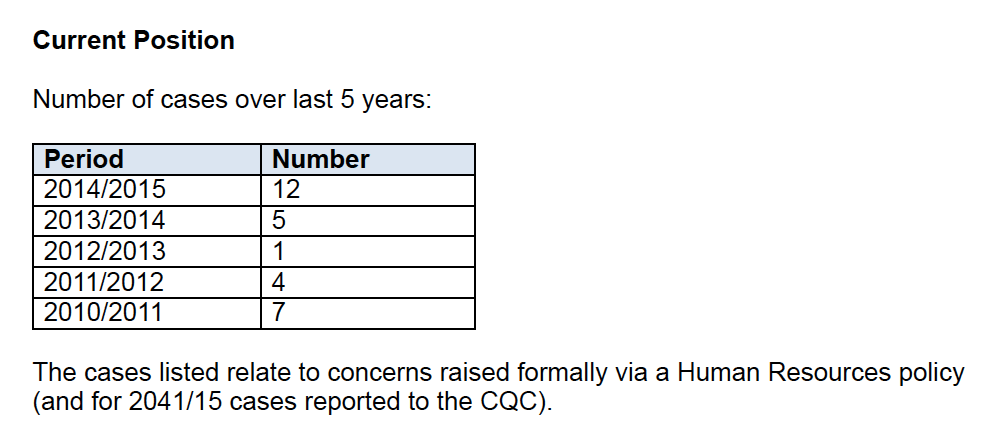
However, the trust admitted to at least 29 whistleblowing incidents between 2010/11 and 2014/15.
This figure includes only cases raised formally under HEFT’s whistleblowing policy, and is an underestimate of the real number.
In June 2014 HEFT appeared to mislead another FOI requester, informing the requester that there had been only three recorded whistleblowing events in 2013/14. 19 This contradicted what HEFT told me in 2015, as per the table above.
HEFT also appeared to incorrectly answer some questions that I asked about its use of compromise agreements between 2011 and 2015.
HEFT claimed to me that it could not disclose any data at all as the numbers were too small and might lead to identification of individuals:
“Q1-4 The Trust does hold the information you have requested. However, we are withholding this information under section 40(2) of the Freedom of Information Act 2000 as the numbers involved are so small that there is a high risk that disclosing the numbers would lead to identifying individuals.” 20
This was self-evidently not the case as HEFT had previously disclosed the following information in response to another FOI request on 21 May 2015, ref. 3754:
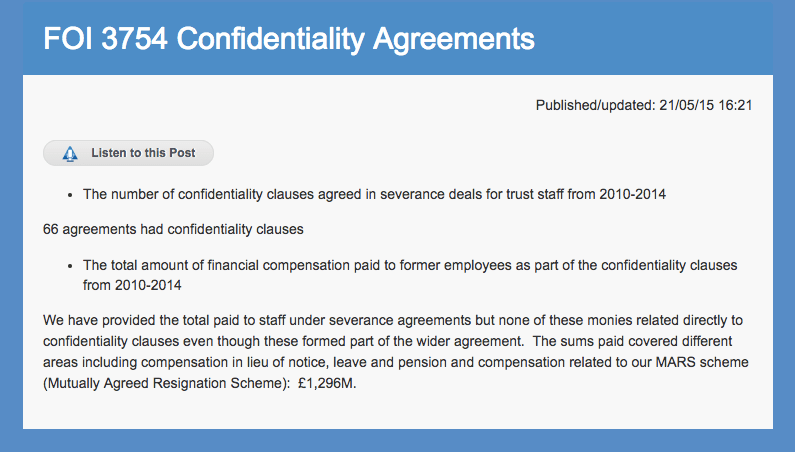
http://www.heartofengland.nhs.uk/foi-3754-confidentiality-agreements/
I questioned the anomaly but HEFT has continued evading clarity about this matter. No explanation has so far been provided, despite correspondence to the current chief executive and assurances from the trust that it would respond.
HEFT has attracted ICO attention previously for poor data handling and was the subject of a recent ICO audit. 21
The financial cost and NHS Resolution’s (formerly the NHS Litigation Authority’s) role
Approximately £18 million has been paid out to Paterson’s NHS patients in damages and legal costs. 22
In April 2017 HEFT disclosed in response to an FOI request by the Press Association 8 17 that there had been a total of 281 claims against the trust by Paterson’s patients, 256 of which had been resolved and that a total of £9,499,458 compensation had been paid to Paterson’s NHS patients.
NHSR has disclosed that it started receiving claims about treatment by Paterson seven years ago, in July 2010. 23
NHSR reported that it had received 281 claims about Paterson’s NHS patients, and
“Of the 281 claims received, 237 have resolved with a payment of damages and 19 discontinued with 25 outstanding”.
NHSR places the total legal costs at “£8,314,142.90 (combined claimant and defence costs)” and broke this down to £4,550,733.90 claimant costs and £3,763,409 defence costs. 24
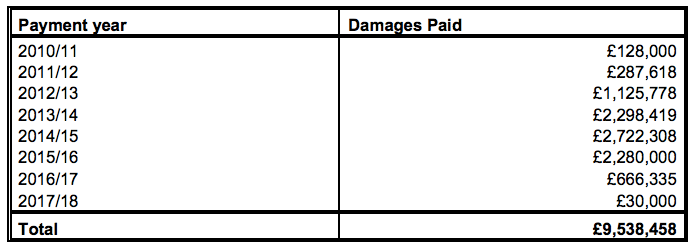
NHSR gave a similar overall total to HEFT in terms of compensation paid out on Paterson’s NHS patients – £9,538,458. The biggest reported award was £320,000. 24
According to NHSR, this is how the compensation payments were distributed by financial year:
A question arises about what steps since July 2010 NHSR has taken to flag concerns about Paterson’s practice to the rest of the system, and if it took such steps, what the system response was.
NHSR’s operating frameworks claim that it works closely with the DH and other bodies 25, and that the NHSR should ensure that the DH is “sighted” on NHSR’s work and not subject to any unpleasant surprises 26 :
“Ensure that DH is sighted on issues affecting NHSLA [NHSR] and share information to ensure that both organisations work together to form a ‘no surprises’ culture”.
Whatever the DH’s precise role in the Paterson business, it has refused to learn one of the key lessons from Paterson’s unchecked malpractice – that there must be real whistleblower protection. The DH remains inimical to whistleblowers:
https://minhalexander.com/2017/05/06/cqc-and-national-guardian-defend-fortress-dh/
As for NHSR, seven years after it first received claims about Paterson’s practice, it says:
“NHS Resolution are very sorry for the distress experienced by any patients affected by this case and remain committed to ensuring that any lessons are learnt in the interests of protecting patients in the future.” 27
The latest NHSR board papers of 17 May 2017 note that the NHS is facing claims by private patients on the basis that:
“The generic allegations against HEFT suggest a duty of care owed by the Trust to private patients; failing to stop the inappropriate and negligent surgery earlier; allowing IP to remain in post when it was known he was not competent to continue to treat “in and after 2004” when it was known he was performing incomplete mastectomies at Spire and Solihull; failure to monitor IP’s activities after December 2007 to ensure no CSM’s were carried out; knowing Spire relied on appraisals and monitoring from HEFT to ensure IP’s competency.” 27
The GMC and NCAS
The GMC has been tight-lipped about its role in the Paterson governance failures, and recently implausibly claimed that it could not answer any questions at all until the prosecution had concluded.
“I can confirm that we do hold the information that you have requested. However, the judicial process concerning Mr Paterson is ongoing. When that has concluded the GMC procedures will recommence. It is possible that once the criminal process and the GMC/MPTS process have ended, we will be able to disclose more information about Mr Paterson. At this time, however, I consider that the following FOI exemptions apply to the release of the information that you have requested [Section 40 and 41 FOIA exemptions]” 28
The Kennedy report noted that Paterson was referred to the National Clinical Assessment Service (NCAS) in 2007. NCAS has a remit for assessing doctors’ clinical performance and conduct in response to referrals about concerns. In Kennedy’s view, NCAS focused on re-integrating Paterson and failed to give sufficient weight to the patient’s perspective. 29
Kennedy and Verita reported that the GMC received the first complaint about Paterson’s practice in 2010. 2 3
The GMC did not impose conditions on Paterson’s registration until July 2011, and he was not suspended from practice by the GMC until October 2012.
Yesterday, immediately after Paterson’s sentencing, the GMC chair released a statement effectively blaming health professionals for not reporting the problems sooner:
“As soon as we were made aware of these issues we took action to curb his practice and then suspend him, but his practice went unchecked for so long because some of those in the health system – managers but also his colleagues – had their concerns but failed to report them to us.” 30
This is somewhat rich as the GMC has been criticised for not adequately protecting medical whistleblowers. Sir Anthony Hooper observed in his report about the GMC’s handling of whistleblowing matters that:
“26. In the context of this review, my concern is that employers may use the process of making an allegation to the GMC about a doctor’s fitness to practise as an act of retaliation against a doctor because he or she has raised concerns or, simply, as an inappropriate alternative to dealing with the matter in-house. If that happens, the GMC unwittingly becomes the instrument of the employer in its campaign against the doctor. If the doctor is then subject to an interim suspension order and, as it later turns out, he or she ought not to have been, the damage to the doctor can be lifelong.” 31
Moreover, the GMC has faced awkward questions about its role in ensuring that registrants have proper indemnity, following the Medical Defence Union’s refusal to indemnify Paterson’s illicit procedures. 31
The Care Quality Commission
According to the Kennedy report, in 2009 HEFT’s then chief executive Mark Goldman wrote to the CQC about the planned recall of some of Paterson’s patients, and the trust later updated the CQC, Monitor, SHA and NHSLA (now NHS Resolution) in 2011. 2
Kennedy reported that there was no evidence of a response from these central bodies:
“10.23 Outside the Trust, the Chief Executive had written to the Chief Executive of the Care Quality Commission (CQC) on July 1, 2009 advising her of the proposed recall of 12 patients and the possibility that this may attract the attention of the media. A subsequent letter from the new Medical Director, Dr Anwar on May 19, 2011 provided CQC with an update, with copies sent to Monitor, the Strategic Health Authority and the NHS Litigation Authority. I have not seen any evidence of a response from any of these bodies.” 2
The CQC carried out a review of HEFT’s serious untoward incidents in 2009. A letter from the CQC copied to Andrea Gordon, now a CQC Deputy Chief Inspector of Hospitals, about the CQC’s 2009 review suggests that the CQC carried out a box ticking exercise based on the trust’s paper trail. 32 There is no mention of Paterson or the harm that he had caused to patients.
CQC’s letter concludes thus:
There are two published CQC inspection reports on HEFT, of 14 January 2014 and 1 June 2015, both of which rated HEFT overall as ‘requires improvement’. 33
Neither report mentions Paterson or the patient harm that he caused, or the progress made in response to the recommendations of the Kennedy report.
In contrast to these CQC inspection reports on HEFT, CQC’s inspection report of 23 December 2015 on Spire Healthcare does acknowledge Paterson’s malpractice and the governance issues arising:
“Staff were aware of the duty of candour and a robust Duty of Candour Policy was in place for staff to access electronically and in paper form. Senior hospital staff recalled more than 600 patients at Spire Parkway Hospital relating to historic operations performed by a former breast care surgeon. The recall of patients was to provide a full explanation and apology for care and treatment which had gone wrong. The recall register was in place and the recall process was completed in June 2015.”
“Historical complaints relating to a former breast care surgeon had generated a significant volume of issues during the past few years. The hospital had reviewed its complaints’ procedure and the complaints’ policy and process was robust. Staff at all levels were aware of their responsibilities as to the management of service specific and hospital level complaints.”
“During the inspection we reviewed the 15 recommendations made by an independent review body as a result of a review commissioned by Spire Healthcare and completed in March 2014. The review had been commissioned in April 2013 to report on the governance arrangements at Spire Parkway and Spire Little Aston hospitals in the light of concerns raised about the surgical practice of a consultant surgeon who operated at those two locations.The consultant’s practice led to the Requires improvement ––– Summary of findings 6 Spire Parkway Hospital Quality Report 23/12/2015 consultant’s ultimate dismissal and the recall of more than 600 patients at Spire Parkway Hospital. We found evidence at this inspection to demonstrate that the majority of the recommendations made by the independent review had been implemented at the hospital. In addition to the 15 recommendations made by Verita, Corporate Spire had adopted a further eight actions across the Spire hospital network to improve governance and monitoring arrangements. We were assured all eight had been completed at Spire Parkway”
One has to ask why CQC has not used its powers under Section 48 of the Health and Social Care Act 2008 to investigate the large scale patient harm and governance failures arising from the Paterson case.
CQC’s role in mitigating the harm and risk related to the Paterson affair, especially with regards to CQC’s action or inaction over HEFT, remains to be fully elucidated.
Given the circumstances, it is not at all appropriate for CQC to draw a veil over the whistleblowing disclosures that it received about Paterson’s activities at HEFT prior to 2011.
In addition to CQC, GMC, NCAS and NHSR’s roles, unanswered questions remain about the role of commissioners, the notorious West Midlands Strategic Health Authority which allowed the failures at Mid Staffs and other regulators such as Monitor.
Public Inquiry
The Royal College of Surgeons has offered the services of its Invited Review Service. 34
A public inquiry is clearly needed, particularly in the light of continuing obfuscations by HEFT, and there have been repeated calls for such.
Hunt has stated that he intends to launch a “comprehensive and focused inquiry” if he is returned to power after the election, but he has not indicated that he will seek a public inquiry. 35
Even a public inquiry may not reveal all the important facts, given that past public inquiries have been criticised for protecting the most senior culprits:
http://drphilhammond.com/blog/wp-content/uploads/2013/03/Private-Eye-mid-staffs-final.pdf
The further handling of this scandal will help clarify the degree to which politicians and senior officials are willing to allow transparency about NHS failure and to stop the suppression of whistleblowers – or not.
UPDATE 2 JUNE 2017:
Heart of England NHS Foundation Trust has now admitted that it has super-gagged two whistleblowers (settled with confidentiality clauses that prevent signatories from even revealing the existence of the settlements, and non-disparagement clauses which prevent former employees from criticising the trust).
HEFT FOI response on compromise agreements 4561Review 2.06.2017
| Please sign and share:
Petition to replace weak UK whistleblowing law to protect whistleblowers and the public |
RELATED ITEMS
https://minhalexander.com/2017/01/06/national-clinical-assessment-disservice/
REFERENCES
1 Disgraced surgeon Ian Paterson jailed for 15 years. BBC 31 May 2017
http://www.bbc.co.uk/news/uk-england-birmingham-40108558
2 Kennedy report on the Review of the Response of Heart of England NHS Foundation Trust to Concerns about Mr Ian Paterson’s Surgical Practice; Lessons to be Learned; and Recommendations, 13 December 2013
https://minhalexander.com/wp-content/uploads/2016/09/kennedy-report-final.pdf
2b Dr Rex Polson’s investigation report on Ian Paterson, 29 April 2008
https://minhalexander.com/wp-content/uploads/2016/09/dr-polsons-report1.pdf
3 Verita Independent review of the governance arrangements at Spire Parkway and Little Aston hospitals, March 2014
4 Ian Paterson timeline of missed opportunities to uncover and stop him. Solihull Observer, editorial 4 March 2015
5 Ian Paterson case: disgraced surgeon’s patients ‘airbrushed’. BBC 3 May 2017
http://www.bbc.co.uk/news/uk-england-birmingham-39779438
6 Private patients to miss out on compensation from God complex breast surgeon as Spire and union refuse to cover costs , Robert Mendick, Telegraph 29 April 2017
7 HEFT FOI disclosure ref 5224, on 30 May 2017, about Paterson’s breast surgery and clinical outcomes
https://minhalexander.com/wp-content/uploads/2016/09/heft-disclosure-30-05-2017-foi-5224.pdf
8 HEFT FOI disclosure ref 5157, on 6 April 2017, about Paterson’s breast surgery and outcomes
https://minhalexander.com/wp-content/uploads/2016/09/heft-disclosure-foi-5157-breast-surgery.docx
9 HEFT paper on Paterson’s breast cancer surgical outcomes
Click to access heft-surgical-outcomes-and-practice-final.pdf
10 HEFT FOI disclosure ref 5138, on 11 April 2017, about Paterson’s breast surgery and outcomes
https://minhalexander.com/wp-content/uploads/2016/09/heft-disclosure-foi5138.pdf
11 HEFT FOI disclosure ref 2551, 27 February 2014, about Paterson and communication with Spire Healthcare
https://minhalexander.com/wp-content/uploads/2016/09/heft-disclosure-foi-2651-two-others.docx
12 Petition of HEFT whistleblower Shazada Hussain, Hansard 22 October 2014
https://www.publications.parliament.uk/pa/cm201415/cmhansrd/cm141022/petntext/141022p0001.htm
13 Account of Michael John HEFT whistleblower, 26 March 2017
https://antibullyingnhs.wordpress.com/2017/03/26/michael-andrews-story/
15 Staff must be free to raise safety concerns, says Heart of England chief exec, Shaun Lintern, Nursing Times 9 April 2013
16 CQC intelligent monitoring reports on HEFT:
21 October 2013
http://www.cqc.org.uk/sites/default/files/old_reports/RR1_101_WV.pdf
13 March 2014
http://www.cqc.org.uk/sites/default/files/old_reports/RR1_102v2_WV.pdf
July 2014
http://www.cqc.org.uk/sites/default/files/RR1_103v3_WV.pdf
December 2014
http://www.cqc.org.uk/sites/default/files/RR1_104v3_WV.pdf
May 2015
http://www.cqc.org.uk/sites/default/files/RR1_105v3_WV.pdf
17 CQC FOI disclosure 30 May 2017, ref. IAT 1718 0065
17b CQC FOI disclosure 30 May 2017, ref. IAT 1718 0065, spreadsheet:
18 HEFT FOI disclosure 11 September 2015, ref. 4008, about whistleblowing governance
19 HEFT FOI disclosure 20 June 2015, ref. 3124
https://minhalexander.com/wp-content/uploads/2016/09/heft-disclosure-foi-3124-whistleblowing.docx
20 HEFT FOI response of 15 July 2016 to FOI 4561
21 ICO audit of HEFT’s data handling February 2017
https://minhalexander.com/wp-content/uploads/2016/09/ico-heart-of-england-nhs-audit-201702.pdf
22 Hundreds seeking compensation over ops by convicted breast surgeon, York Press 29 April 2017
23 NHSR (formerly NHSLA) FOI disclosure 2970 on HEFT, 18 May 2017
https://minhalexander.com/wp-content/uploads/2016/09/nhsla-foi-disclosure-heft-2970-response.pdf
24 NHSR (formerly NHSLA) FOI disclosure 2953 on HEFT, 27 April 2017
25 Framework agreement between the DH and NHSLA (now NHSR) 2013. Annex D: Relationships with other bodies
26 Protocol for public and parliamentary accountability. Between the DH and NHSLA (now NHSR). February 2014
27 NHSR Board papers 17 May 2017
http://www.nhsla.com/aboutus/Documents/Master%20Board%20Papers%20May%202017%20-%20Part%201.pdf
28 GMC FOI response IAT/ME/F17/8858, of 12 May 2017 to Clare Sardari NHS whistleblower, @Sardari_Clare
29 Kennedy report page 6:
“21 The second important implication of pursuing an investigation through the disciplinary procedures was that senior managers worked within the approach adopted by the Department of Health’s National Clinical Assessment Service (NCAS). This approach concentrated on identifying the measures necessary to reintegrate Mr Paterson into the team and make sure that his surgery met appropriate standards. The perspective, therefore, was that of the clinician and his needs, all set out in an Action Plan.
22 There was another perspective which could and should have been adopted: that of the patient. Had that perspective been adopted, the question would have been: how can we act in the best interests of patients. This may have caused senior managers to require Mr Paterson to cease operating on women with breast cancer until the concerns that had been swirling around for several years could be calmly analysed. This perspective did not appear to be understood, far less adopted.”
https://minhalexander.com/wp-content/uploads/2016/09/kennedy-report-final.pdf
30 GMC statement about Paterson 31 May 2017
http://www.gmc-uk.org/news/30724.asp
31 Report by Sir Anthony Hooper on the handling by the GMC of cases involving whistleblowers
http://www.gmc-uk.org/Hooper_review_final_60267393.pdf
31 GMC FOI disclosure 24 February 2015, ref. IAT/F15/6854
“5. We do not check registrants indemnity arrangements when they pay their annual retention fee.
However, since August 2014, all new applications for registration, with a licence to practise, and restoration of a licence to practise do require the applicant to make a declaration that they will have, at the point of practise, appropriate cover under an indemnity arrangement.
In addition we have recently consulted on changes to the licence to practise and revalidation regulations which will provide the Registrar of the GMC with powers to:
- Request information from a doctor or third party about a doctor’s indemnity arrangements
b. Require a doctor to inform us if they cease to have appropriate indemnity or insurance cover or if their cover is provided by their employer
c. Refuse to grant or to withdraw a doctor’s licence to practise for failure to have appropriate cover or to comply with our requirements to complete the declaration or provide any further information”
https://www.whatdotheyknow.com/request/private_gmc_registered_doctor_in
32 CQC review closure letter to HEFT chief executive 8 January 2010
33 CQC inspection reports on HEFT:
14 January 2014
http://www.cqc.org.uk/sites/default/files/new_reports/AAAA0787.pdf
1 July 2015
http://www.cqc.org.uk/sites/default/files/new_reports/AAAD4967.pdf
34 Royal College of Surgeons statement 31 May 2017
35 Hunt announces plans for inquiry into rogue surgeon Ian Paterson, Frances Perraudin, Guardian 4 May 2017


Yet another instance where, but for the feet of clay regarding an independent, universal whistleblowing service, calls of alarm could have been raised.
LikeLike
Thank you for this Dr. A.
I shall only make two points.
First, I was astonished that Mr. Patterson was actually given a prison sentence. Others who have butchered to the same extent got away with it.
Second, as you so rightly point out, these atrocities didn’t occur in a vacuum but within, under and surrounded by, all of the checks and balances and oversights and safeguards that were required. But, as usual, all of the patient protections were not enforced as their reality is only as fig-leafs, P.R. and financial rewards for those who do not undertake their duties to any meaningful extent.
Regards,
Zara/
LikeLike