Dr Minh Alexander retired consultant psychiatrist 23 August 2022
This is a post to share data extracted from the. Chief Coroner’s website on coroners’ safety warnings related to NHS ambulance trusts in England.
Emergency services have recently collapsed due to a confluence of many disastrous factors.
Some have suggested that thousands are now dying because of NHS ambulance delays.
The Times reported on 21 August 2022 that there has been a spike in non COVID deaths and that the South West is most affected by excess deaths:
“Since the start of May, about 7,400 more people have died of non-Covid reasons than would be expected in the same period, an analysis of data from the government’s Office for Health Improvement and Disparities suggests.
The increase in deaths has been highest in southwest England, where about 8 per cent more people have died than expected. The region’s ambulance services are also suffering the worst handover delays of any region, with nearly a third of all patients in July being forced to wait more than an hour to get into A&E, a report by the Association of Ambulance Chief Executives (AACE) suggests.”
The Department of Health and Social Care is reportedly investigating:
“Early enquiries suggest most of the excess deaths in recent months have been in heart attack, stroke and diabetes patients, officials said.”
A horrifying 35% of paramedics surveyed by the GMB union reported that they had witnessed deaths due to ambulance delays.
The Health Service Journal saw a leaked internal memo from Wrightington, Wigan, and Leigh NHS Foundation Trust, which noted increasing deaths in A&E.
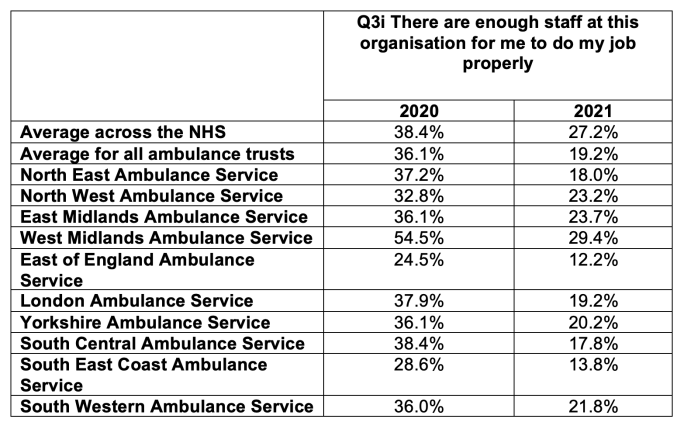
The proportion of NHS ambulance trust staff who feel there is safe staffing at their trust has dived between the 2020 and 2021 NHS staff survey. Extraordinarily, by the end of 2021 only 12.2% of staff at East of England Ambulance Service felt that there was adequate staffing
Coroners’ reports to Prevent Future Deaths are issued variably depending on individual coroners’ approaches, and they are only issued exceptionally.
The Chief Coroner’s published database of PFD reports does not represent a complete dataset as there is sometimes a lag in publishing.
The database is not user friendly and there is no search function. This obscures patterns from public view, and therefore reduces accountability to the public.
Previously, it was necessary to laboriously search the whole database manually in order to extract data for analysis. In recent years, cases have been loosely grouped under a few categories, which allows greater public access. This is not fool proof as the indexing sometimes does not capture all cases that belong in a particular category. Nevertheless, it is now possible to manually sift each category.
I have done a rough and ready search for PFDs related to English NHS ambulance trusts under the category ‘Emergency services related deaths’.
The data in this series dates back only to 2019.
I found 59 coroners’ PFD reports that related to some aspect of NHS ambulance trust function.
This the breakdown of numbers of PFDs by each ambulance trust:
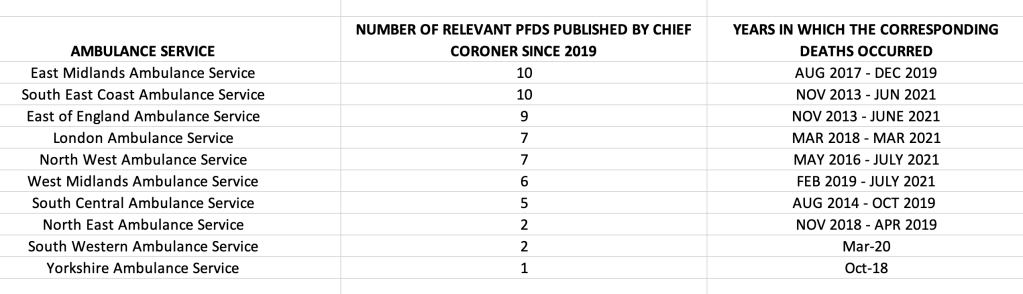
The low numbers for some trusts may represent under-reporting to the coroner, as has been the case at North East Ambulance Service (NEAS).
The NHS ambulance trust related PFDS published since 2019 relate mostly to deaths which occurred in 2018 and 2019:
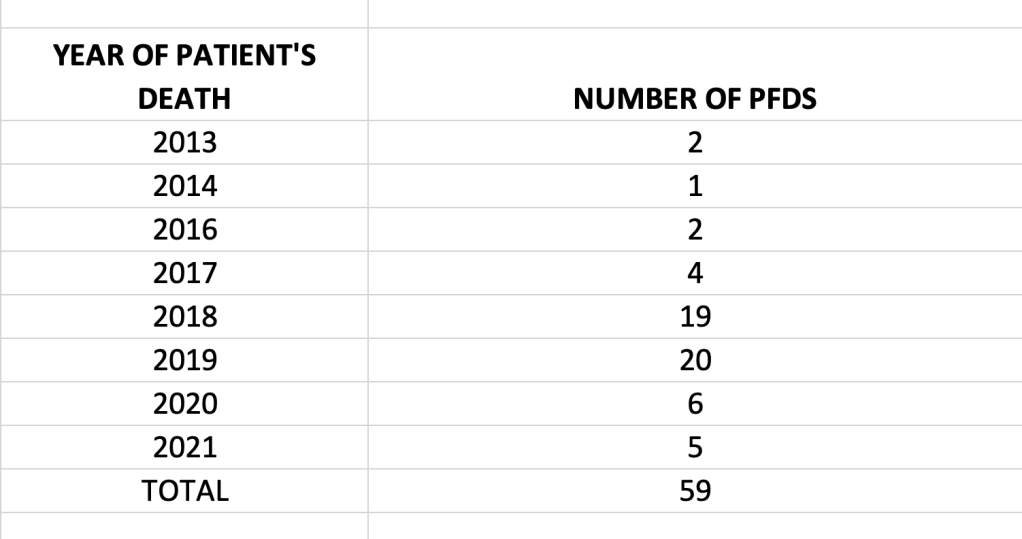
These PFD reports therefore give a snapshot of some of the problems that were building up in our emergency services in these years, before the final, current collapse.
This is a spreadsheet of the 59 ambulance trust related PFD reports that I found:
Spreadsheet of coroners’ PFDs related to NHS English ambulance trusts, 2019 to August 2022
Warnings about recurring resource issues and unsafe ambulance service pressure have been sent to directly to Health Secretaries since 2019:
Death of Gladys Furnival July 2018
Death of William Oliver November 2018
Death of John Murphy July 2021
The coroners dealing with North West Ambulance Service seem most vocal in this regard.
When I previously looked at coroners’ PFDs, ambulance trusts were already noticeable for an escalating number of PFDs and findings of unsafe service pressure and problems with hospital handover.
A striking an example of a recent coroner’s PFD warning about unsafe pressures relates to the death of William Oliver on 1 November 2018, in which the coroner highlighted the severe problems for ambulance trusts facing long hospital handovers:
“An emergency call was placed to NWAS at 06.00…Mr Oliver thought he may have had two strokes in the night and he thought he had fractured his hip. In addition he was struggling to breathe and was sweating. The call was graded as requiring a Category 3 response. Subsequent calls at 06.26 between NWAS and Mr Oliver) and 06.44 (between Anchorcall and NWAS) were dealt with inappropriately and Mr Oliver’s deteriorating condition was not re-triaged. The Court found on the balance of probabilities that the response would have been increased to at least a Category 2 response…at 07.44 hrs a further call was received from Anchorcall who by this time could not make contact with Mr Oliver and the call was escalated at 07.50. At 07.51 an emergency ambulance was allocated and arrived on the scene at 08.05 when Mr Oliver was found deceased”.
“Another contributing factor to the unavailability of ambulances on the 31st October – 1st November 2018 was the turnaround times at Manchester Royal Infirmary, North Manchester General Hospital, Royal Oldham, Salford Royal and Stepping Hill were all particularly higher than anticipated with numerous ambulances delayed for over one hour. In total from the commencement of the nightshift on 31st October 2018 more than 273 hours of ambulance availability were spent at hospital sites handing over patients. The evidence from NWAS did not suggest this was significantly different to other nights or uncommon.” [my emphasis]
Concerns were also raised in the, death of Diane Gudgeon in May 2018, that the ambulance service protocol for mobilising extra resources in response to demand was set at too high a threshold and also was not always implemented when needed:
“Although EMAS was in a Capacity Management Plan (CMP) status (initially 2 and escalated to 3 at 10.35pm on 21st May 2018) this did not lead to the deployment of any additional vehicular resource. EMAS say that additional financial resources have now been made available”.
“The effectiveness of the EMAS Capacity Management & Escalation Plan (CMP) including, inter alia, the fact that:‐
a) CMP status 1 – 3 does not trigger the deployment of additional vehicular resources.
b) CMP 4 is only triggered when 200 calls are holding (this was previously 150) – this is a high threshold.
c) A Technical Commander can overrule a CMP status e.g. even if 200 calls are holding (CMP 4), this can simply be downgraded to CMP 3 by the Technical Commander.”
Generally, the PFD reports give a harrowing sense of routine, excessive pressure on the ambulance service. The delays are wasteful in that substantial resource is dedicated to precariously keeping all plates spinning – such as checks that have to be made on patients waiting for delayed ambulances. Inevitably, some of the deaths related to failures to keep all plates spinning.
For example, in the death of Helen Barker in November 2018:
“She called the emergency services on the 11th Nov 2018 to report she was feeling suicidal and threating to take an overdose. Reviews were supposedly undertaken at 22.39, 00.30 and 03.43 hours but these did not occur due to pressure at work. The paramedics eventually attended at 04.34 hours some 6 hours and 35 minutes after the initial call was made. The deceased was pronounced dead at her home on 12th November 2018 at 4 Bexon Court, Louth”
Similar issues arose in the death of Arthur Jepson in October 2018:
“Mr Jepson suffered stomach pain and called 999. The evidence was that the initial call was made at 15.32. That call was initially triaged as Category 5 but when the paramedic telephoned an hour later the matter was re classified at category 3. The ambulance arrived at 19.31….During the inquest, evidence showed:-
1. that the pressure on resources was high that day.
2. that a review at the two hour point should have taken place to ascertain if the matter needed re categorisation.
3. Such a review didn’t happen.
4. Whilst the evidence at inquest was that this is unlikely to have changed the outcome in this case, it was a concern to me that it could be in another case”.
Extreme service pressure may also lead to unprepared staff making mistakes. In the death of Sean Mansell, a paramedic who had not been trained was asked to assist with call handling due to severe service pressure, and made an error:
“Sean Mansell had a medical history of alcohol dependence syndrome. On the 5th July 2021, the West Midlands Ambulance Service received a 999 call at 19.23 hours from a neighbour of the deceased who reported that the deceased couldn’t walk. The call was allocated a category 3 disposition which had a target response time frame of 120 minutes. An ambulance arrived on scene at 03.38 on the 6th July which was 8 hours and 15 minutes later and not within the response time frame. This was due to the fact that demand outstripped available resources. A welfare call was undertaken at 21.28 hours by a paramedic who had been asked to go into the control room to assist with welfare calls due to the high volume of 999 calls outstanding. The paramedic had not received prior training on how to complete these calls. The welfare call was conducted with the neighbour. No contact was made directly with the deceased during the 8 hour delay which led to a missed opportunity to identify a change in his condition. When the ambulance arrived, the deceased had passed away on the sofa in his front room”
In addition to the handover at hospitals due to hospital bed shortages and delayed discharges due to social care shortages, there is also an example of another safety net that has been withdrawn by at least one local authority – the local Falls service, which might normally allow a welfare check and care whilst an ambulance was en route, had been axed. Death of 93 year old Douglas Minns:
“4 CIRCUMSTANCES OF THE DEATH
The deceased suffered a fall at home, [REDACTED] on 21st August 2018 at 8.30pm in the evening and he made an emergency call to the ambulance service. He was attended to by the ambulance service at 00.25 on 22nd August 2018 and he was eventually conveyed to Milton Keynes University Hospital arriving at 02.08. A CT scan revealed a large subarachnoid and subdural bleed caused by the fall. He died at the hospital at 15.50 on 22nd August 2018. The delay in the ambulance attending was due to high operational demand.
5 CORONER’S CONCERNS The MATTERS OF CONCERNS are as follows:
During the course of the evidence it was explained to me that the provision of a falls service was withdrawn some years ago, the service would provide for someone to attend the home of the person who had fallen, get them on their feet, assess their wellbeing, serve a cup of tea and get them back into bed if required. If they required more urgent treatment, they would report to the ambulance service. The withdrawal of the service puts patient’s lives at risk and, in view of the strains on the ambulance service, consideration should be given to reintroducing it. It is unacceptable for a 93 year old man to be left lying on the floor for four hours before someone responds.”
How many other cash strapped local authorities are in this position?
Indirectly related to resource levels, the PFDs also showed recurrent problems with ambulance service algorithms/ protocols for assessing need and priority. The fact that NHS ambulance call handlers are not clinically qualified means that if there is a flaw in an algorithm, or even if an appropriate algorithm has not been created, matters can very easily become unsafe for patients. The death of Christopher Williams in January 2019:
“His GP attended and requested an urgent ambulance since she was concerned about cauda equina. She also arranged for him to be admitted directly to the ward at the NNUH. She called the ambulance at 14.17 hrs, she was told it may take up to four hours, a pick up time of 15.17 was entered. At 15.20 the trust called the patient back his condition was worsening however the call handler did not escalate this information within the call centre and thus no one else was aware. It is understood the call handler used an incorrect algorithm (haemorrhage)….a further welfare call was made at 17.40 but no answer was received so this was escalated to the Duty Officer who subsequently upgraded the call to category 3. At 19.41 [redacted] made an 999 call describing Mr Williams as not being alert and having difficulty in breathing and the call was upgraded to a category 1. A RRV and DSA were dispatched at 19.45 hrs and arrived on the scene at 19.58. Mr Williams was conveyed to the NNUH arriving at 20.59 hrs. He was then kept in the ambulance until 23.56 hrs when he finally entered the Emergency Department….despite intensive treatment he died on 26 January 2019.”
“The trust’s Business Continuity Manager was unaware until the inquest that the call handler had erred in failing to escalate and in using the wrong algorithm….He gave evidence that the trust does not have an algorithm dealing with neurological deficits only.
In some countries, for example in Germany, ambulance service dispatchers are paramedics.
This obviously costs more, but could it reduce waste and error? It is not only deaths that arise from the collapse of our emergency services, but also there will be increased morbidity and disability from failure to treat promptly, which all has a cost.
A number of coroners sent their PFDs to national ambulance organisations such as the Association of Ambulance Chief Executive (AACE) to raise concerns about flaws in algorithms or other systems issues.
One key concern was about the allocation of suspected heart attacks to Category 2 responses – within 18 to 40 minutes.
East Midlands Ambulance Service informed the coroner that they had an adjunct protocol, on top of the national protocol, for giving cases of chest pain and suspected heart attacks top priority in their call Category, but that this sometimes failed because of service pressure.
Death of Maureen Woods in January 2019:
“The 999 call was triaged in line with national protocol for a primary complaint of chest pain and graded as a Category 2 response. Due to the overwhelming demand on the ambulance service that night, the ambulance did not attend Mrs Woods within the prescribed time of 18 to 40 minutes for a Category 2 call. At 01.26 hrs a further 999 call was made by the neighbour and Mrs Woods went into cardiac arrest during that call. Paramedics attended promptly but failed to administer Amiodarone contrary to National Rescuscitation guidance and without good reason. The delay in dispatching an ambulance and the failure to administer medication represent failings that prevented Mrs Wood from having the best possible chances of survival….Both EMAS witnesses agreed that 40 minutes appears too long to wait for an ambulance/ solo responder when the complaint is chest related and most likely a cardiac event….
The MATTERS OF CONCERN are as follows: 1) Patients requiring an emergency ambulance response reporting symptoms consistent with a cardiac event, but who are not yet in cardiac arrest, may wait for up to 40 minutes for a category 2 response in line with current national response times. 2) To combat this perceived inadequacy in nationally agreed response times, the East Midlands Ambulance Service NHS trust has developed an adjunct to the protocol by triaging all non Category 1 calls to upgrade calls such as Mrs Woods for a priority response. However, resources do not permit each and every call to be triaged, and Mrs Woods’ call was not triaged before she went into cardiac arrest.”
The coroner was concerned that ambulance standards were not necessarily based on clinical need:
“If the system for national response times is having to be supported by local adjuncts to the system, this rather suggests that the allocation of these calls in Category 2 lies outside clinical need.”
Some of the PFDs raised issues of leadership and organisational learning. After highlighting several concerns about East of England Ambulance Service’s handling of Christopher Williams’ case, the coroner remarked:
“This is not an isolated incident and it appears there are systemic failures in your organisation which should be addressed”.
It does appear that ambulance trusts and their staff have not been adequately supported and have been taken for granted for years, without adequate action by the government and without care for public safety. This is despite many warning signs, including the above explicit warnings by coroners.
It is not hard to see how covers up arise. Or that whistleblowers are suppressed. Or how staff welfare is impacted by the daily grind of juggling inadequate resources and knowing that patients have been avoidably harmed despite their best efforts.
However, the government has put NHS England in control of the “independent” review on the NEAS deaths cover up scandal.
NHS England too has been warned for years now by coroners of problems. The NEAS review is unlikely to be sufficiently rigorous in view of the conflicts of interest in the situation.
Given the gravity of the threat to public safety from the ambulance service collapse nationally, and how we arrived at this terrible mess, surely it should be a properly independent judge-led inquiry, with statutory force? And should its remit should be widened to include risks that are common to all NHS ambulance trusts?
RELATED ITEMS
Staff suicides at West Midlands Ambulance Service NHS Foundation Trust
The National Guardian’s Office does not put a blue light on for ambulance staff


Thank you for all of your efforts, Dr A.
The length of time the ambulance delay scandal has been allowed to endure – many years – and with all of the suffering that involves – leaves me to conclude that there is a deliberate agenda at play dedicated to disconcerting, disempowering and harming both public and those NHS personnel who are devoted to their duties as opposed to being superfluous.
On paper at least, we are blessed with a wealth of expertise and management specialists in medical and non-medical roles within the NHS and its associates. And yet, no one can address such logistical problems or rather, provide a viable plan to integrate disparate disciplines and provide a way forward.
Instead, we are content to allow the innocent to suffer.
This country is circling the drain – and, it would seem, with no motivation to do otherwise.
I’m very sorry.
LikeLike