By Dr Minh Alexander, NHS whistleblower and former consultant psychiatrist, 16 December 2017
The Care Quality Commission the health and social watchdog should carefully examine care given at night, but its own data shows that it fails to do so.
Background
In 2012 the Royal College of Nursing surveyed its members about what they would hope for from the regulator, and submitted this evidence to the parliamentary Health Committee. A most interesting finding was that nurses wanted the CQC to inspect at night:

RCN 2012 Putting_Quality_into_the_Care_Quality_Commission_England
A perceptive reader might understand this to be a plea for help from a concerned workforce, that was not confident in speaking out. Any regulator worth its salt should have taken this seriously.
When there are severe pressures on services, a temptation for hard pressed managers is to make savings on staffing levels. Night shifts can be disproportionately cut by non-clinical managers who may assume reduced demand, and do not fully appreciate the clinical consequences or turn a blind eye.
Combined with staffing shortages, a controversial junior doctors’ contract and rota gaps, some very serious situations can arise.
In September, it was reported that two junior doctors at Plymouth were left looking after 436 patients.

Indeed, the well known and ongoing case of NHS whistleblower Dr Chris Day originated from a phone call that he made one night about an under-staffed shift.
|
“The dedicated NHS doctor they tried to gag then destroy: “So when, during yet another night shift, Chris made a telephone call to report to the duty manager that he believed overnight staffing levels were unsafe, and that patients with life-threatening conditions may be left ‘dangerously’ at risk, he simply believed he had discharged his duty as a responsible doctor. During his time on the unit, two ICU patients had died at night, in circumstances formally recorded by Lewisham and Greenwich NHS Trust as serious untoward incidents – meaning the deaths were unexpected or preventable. Yet unbelievably, that polite phone call left his career in tatters and sparked a two-year legal battle which is estimated to have cost the NHS hundreds of thousands of pounds in public funds. Rather than support his claim, NHS agencies accused him of having ‘personal and professional conduct issues’, removed his right to continue training and used the full weight of the law against him – destroying his promising career.” http://www.dailymail.co.uk/news/article-4503734/The-dedicated-NHS-doctor-tried-gag-destroy.html Dr Day’s campaign website: https://www.crowdjustice.com/case/junior-doctors-round-3/
|
A subsequent critical care peer review of the hospital in question flagged multiple areas of concern, including:
“The consultant to patient ratio was significantly low, presenting an area of serious concern…High number of peri-arrest calls and inadequate escalation pathway for deteriorating patients on the ward….Wards will tolerate a high NEWS scores and sometimes not report until score reaches 9”
Lewisham and Greenwich FOI-053581-Peer-Review-Report_Redacted
Understaffing at night can coincide with a vulnerable time for some patients. Older, confused patients may wander more and be at risk of falls and injury, particularly if they have received sedative medication.
Line of sight care is preferable for the most vulnerable but becomes impossible when nurse : patient ratios are insufficient to support suitably safe and intensive care.
There have been repeated coroners’ reports on deaths in which there was a failure to provide planned care – including 1-1 care – for confused patients who suffered falls and sustained major injury. For example:
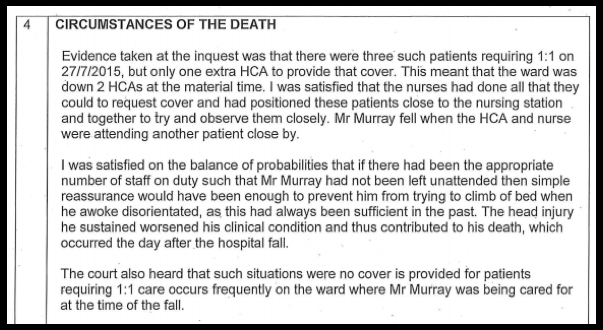
https://www.judiciary.gov.uk/publications/leslie-murray/
Unsafe nursing ratios also intermittently hit the headlines:

http://www.mirror.co.uk/news/uk-news/nhs-patients-suffering-falls-night-7826584
However, the government dismantled the Safe Staffing work by NICE and it stubbornly resists mandating safe staffing levels, in contrast to the Welsh government which passed legislation that will come into force in April 2018.
Under the new Welsh law, there is a requirement to calculate and deliver a safe level of staffing:
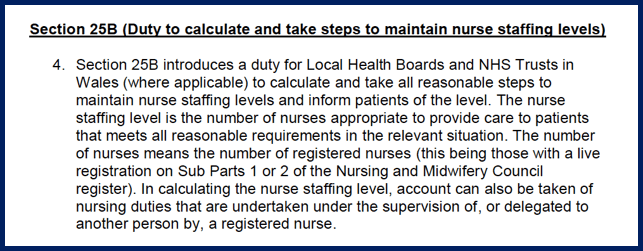
http://gov.wales/topics/health/publications/health/guidance/staffing-levels/?lang=en
Night staff in health and care settings can also be neglected and marginalised. Weak management can lead to silos and pockets of troubled culture. Unsupported staff may also sometimes escape from day time work to night work as a way of coping with unaddressed issues. I have worked in poorly led services where there was a very uncomfortable and noticeable Race divide, with some wholly BME staffed night shifts.
In the private care home sector, there are repeated reports of institutional abuse arising from chasing profit, mitigating against local authority cuts and skimping on staffing levels. A notorious practice is to drag residents out of their beds very early in the morning, for institutional convenience and to squeeze the most value out of night staff.
Publicly, CQC disapproves of this practice:
|
“Staff got some residents out of bed to be washed and changed as early as 5.15am, so that it was “easier” for staff to look after them. Some were then put back to bed. One nurse told Dispatches how she had to get people up at 3.30am to give them bed baths.” “Andrea Sutcliffe, the CQC chief inspector of adult social care, was appalled at “shocking evidence” of understaffing, bad practice and poor care. “The examples of poor care and a culture of inappropriate, institutionalised practice highlighted by this programme are wholly unacceptable,” she said. “Bupa has betrayed the very people it is paid to look after.”
|
The real CQC
But CQC did shockingly little when Helen Rochester a care home whistleblower reported a prime example of such practice.
CQC did not inspect for three months after Rochester’s disclosures. It only grudgingly pitched up at the care home after Rochester embarrassed the CQC board by attending its video recorded public meeting in June this year.
In April 2017 Rochester reported to CQC:
“I am also aware of institutional abuse happening on nights with the blessing of management. There is a list of 11 residents that have to be got up for the day staff and on Monday – Thursday carers start at around 04.15 to do this. I refused to do this at the weekend and when I questioned this I was told “they can sleep in their chairs”. I was also told all 11 have “other needs” that make them eligible for this treatment by the deputy. If that is the case then the home needs to be staffed accordingly so they can be got up unrushed at a sensible time.
On one night I saw this man being got up at 05.20 against his wishes to accommodate the day staff. His name is on the list of 11”
Despite being given this information, when CQC eventually sauntered along to the care home three months later, it did so at 06.00 am:
“The inspection took place on the 13 July 2017. This visit was unannounced and started at 06.00 in the morning in order to review what care was being provided by night staff to people early in the morning. It was completed by two inspectors”
And despite the serious Safeguarding concern raised by Rochester, the dilatory CQC only spoke to three residents:
“During the inspection we talked with three people who use the service and five relatives”
and cheerily reported:
“When the inspectors arrived six people were in the lounge. Although they were alone in a lounge area, the homes’ chef was nearby and provided early morning drinks. People were comfortable and chatting with each other. One told us they were very happy to be up and about early. “I am an early bird.””
To add insult to injury, and despite Rochester (an experienced former nurse and a previously vindicated whistleblower in another serious care home scandal) reporting a catalogue of other serious care failures, CQC rated the care home ‘Good’, safe and well-led.
Rochester complained about CQC’s conduct, but the CQC investigated and exonerated itself as usual. CQC informed Rochester that both the CQC Chair and Chief Executive had sight CQC’s dismissive complaint response before it was sent to her.
Undeterred, Rochester filed a Freedom of Information request about CQC’s out of hour inspection activity:
Helen Rochester FOI CQC out of hour inspections 14.11.2017
CQC’s response reveals unimpressive performance:
Out of hours response 201712012 Final FOI Response CQC IAT 1718 0550
Out of hours inspections 20171208 Data for disclosure CQC IAT 1718 0550
CQC disclosed that it has no definition of what constitutes an ‘out of hour inspection’.
CQC also failed to answer whether it has guidance for its staff on when an out of hours inspection should be conducted.
In its usual self-justifying style, CQC maintained that it did not respond to the RCN’s 2012 recommendations for more night time inspections because the Health Committee did not ask it to do so:
“There were no specific questions put to CQC by the Committee and therefore no response to those comments was required.”
Importantly, CQC revealed that a mere 1.5% (836 out of 55, 331) of its inspections take place out of hours:

This is perhaps understandable – so much nicer to arrive announced, when the reception committee has been fully prepared and the hospitality budget has been apportioned:

https://www.whatdotheyknow.com/request/cqc_spend?unfold=1
Extrapolating from CQC’s figures, these are the specific rates of out hour inspections for different sectors:
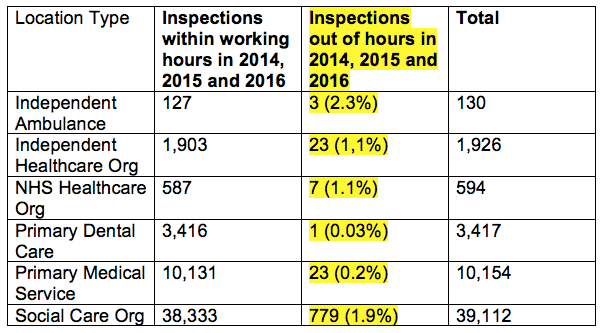
Specifically for care homes, CQC’s data shows that it conducts only 0.4% (123 out of 26,642) of its inspections out of hours:

CQC’s reluctance to grapple with the issues facing care and health staff at night is clear.
Whistleblowers like Rochester who knock on CQC’s door in good faith unwittingly disturb a hostile force, that sometimes unscrupulously wreaks serious damage on those who trespass on no-go areas.
In Rochester’s case, CQC breached her confidentiality as a whistleblower in an earlier case. It then advised her most recent employer to refer her to the Disclosure and Barring Service on spurious grounds, that were later dismissed by the DBS.
All whilst the CQC Chief Inspector for Adult Social Care is frequently seen in the limelight and writes articles extolling compassionate care and progressive workforce practices.

A very important coroner’s Section 28 warning report was issued to CQC in 2013. This considered that there should be clear standards on safe night time staffing levels in care homes and hospitals:
|
“I know that many hospitals are looking carefully at their staffing levels at night particularly in the wards where patients suffer from dementia and may be at a risk of falls through wandering and I am drawing this case to your attention so that you and your inspectors can look carefully at whether staffing levels for night time are adequate to meet the various needs of all the residents/patients in residential, nursing and hospital environments. It seems to me that only two members of staff caring for over twenty four residents, some of whom suffer from dementia and are restless, is not enough to meet all the complex needs, especially with their other duties over a long shift of almost twelve hours.” https://www.judiciary.gov.uk/publications/morris-2013-0295/
|
When I reviewed the Chief Coroner’s database of Section 28 reports earlier this year, I noticed that CQC’s response to this key Section 28 report had not been published by the Chief Coroner.
In September, I asked David Behan CQC Chief Executive to publish this missing response amongst others. After a reminder, CQC replied thus:
“CQC will keep the suggestions you make under consideration. We do not intend to engage in further correspondence with you on this matter.”
However, CQC’s response of April 2014 has now been quietly published on the Chief Coroner’s website:
https://www.judiciary.gov.uk/wp-content/uploads/2013/12/2013-0295R.pdf
In its response, CQC dodged the issue of safe staffing standards.
CQC also reassured the coroner:
Sleep tight.
RELATED ITEMS:
CQC, Coroner’s warnings and the neglect of older people in hospital
CQC, coroners’ warnings & the neglect of older people in hospital
Care home deaths and more broken CQC promises
Breach of confidentiality by CQC and complicity in referring a whistleblower to the Disclosure and Barring Service
Helen Rochester v CQC Act II: Wherein a Whistleblower Sueth a Prescribed Person
Helen Rochester v CQC, Act II: Wherein a Whistleblower Sueth a Prescribed Person



So typical and their own data says it far better than I ever could re their non actions on night concerns. They are a reactive not a pro active regulator.
They only react when they are criticised for not acting and issue bland reassurances of lessons learned going forwards. Winterbourne View is just one example. They never learn.
In the later Morris case referred to in this blog they eventually pitched up in the home some 2 years after this man tragically died in 2012. It was also 6 months after the inquest in 2013, where they are issued with a section 28, warning. They eventually do a reactive out of hours inspection in 2014 as a result of that warning.
Most whistle blowers will contact them before someone dies, as did I , and expect them to act. That was also the case when Ivy Aitkin died.
The CQC simply file these concerns until something happens and instead concentrate any contemporaneous actions on discussing the WB with employers.
Not fit for purpose as a regulator or the prescribed authority IMHO.
LikeLiked by 1 person
Thank you, Dr A.
I see that the CQC arrange to collect the data that they wish to collect in order to record the result that they wish to record. By coincidence, that result will invariably be nothing that is too disturbing because that might distress the CQC’s bosses.
Btw, I have a friend who now lives in Mexico. He explained that their Government (and therefore institutions) are as self-serving (i.e. corrupt) as ours. The only difference is that the Mexican people know and accept this. So, they are still robbed and abused but at least are not surprised. We, in the UK (and USA) allow ourselves to become mortally distressed when we compare what should, and could, be with what actually is.
Heaven help the innocent and the vulnerable.
LikeLiked by 1 person