By Dr Minh Alexander NHS whistleblower and former consultant psychiatrist, 9 September 2017

Helen Rochester a care home whistleblower has made a claim in the Employment Tribunal against the Care Quality Commission (CQC).
Background
On 20 June 2017 Helen Rochester confronted the CQC board about CQC’s behaviour towards her as a whistleblower on two separate occasions in 2013 and 2017. CQC first breached her confidentiality. It was then later complicit in reprisal, being party to Rochester’s inappropriate referral to the Disclosure and Barring Service by her employer.
These matters were summarised previously:
Rochester’s 2013 whistleblowing was previously reported by Private Eye in March 2015, which was not complimentary about the CQC:
Private Eye Go Whistle Article on Helen Rochester March 2015
In a letter of 30 June, after an internal investigation, CQC still maintained to Rochester that it had acted appropriately in suggesting that her former employer should consider referring her to the Disclosure and Barring Service. CQC said that its Chair and Chief Executive both saw this letter before it was sent to Rochester.
On 24 June I informed the National Freedom to Speak Up Guardian of Rochester’s case. I asked her to hold the CQC to account and to establish how many other cases had been mishandled, as this could have not only life changing implications for whistleblowers, but potentially posed serious risk to patients.
The National Guardian, who has an annual budget of £1 million, took over two months to respond and did not actually indicate whether she had established if CQC had breached other whistleblowers’ confidentiality.
https://minhalexander.com/2017/09/03/national-guardian-expects/
Whistleblowers – with zero budget – have in fact established that CQC has conducted no audit of its performance on whistleblower confidentiality since David Behan its CEO promised categorically in 2013 that CQC would not breach whistleblowers’ confidentiality:
CQC FOI disclosure 3 August 2017
At the very least, this shows complacency by the regulator.
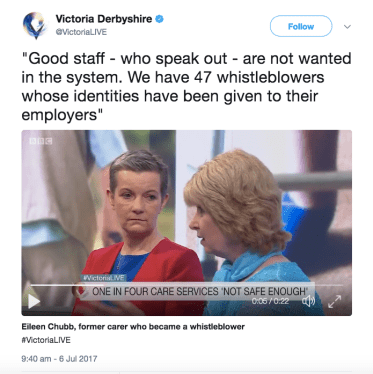
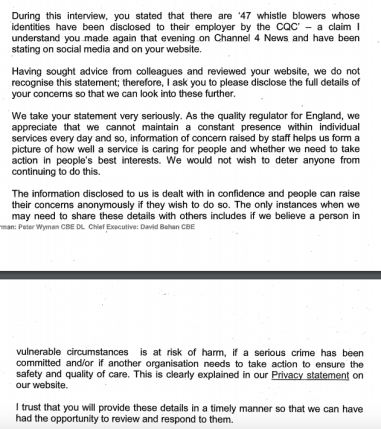
The CQC has refuted recent allegations by the campaigning charity Compassion in Care that the CQC has breached the confidentiality of 47 whistleblowers to their employers. 1
On 14 July 2017 Andrea Sutcliffe the CQC’s chief inspector of Adult Social Care wrote “we do not recognise this statement” and insisted on proof before CQC could act. 2
One wonders upon what evidence this denial was founded, if CQC has never actually audited its performance.
On 11 August 2017 Sutcliffe repeated a claim that the CQC could not look into the alleged breaches of whistleblower confidentiality unless it was first provided with proof. 3 This seems a questionable position for the CQC to take when it has obvious recourse to audit as a means of proactively answering the question for itself.
Rochester’s claim against the CQC
Rochester has now made a claim against the CQC in the Employment Tribunal.
The claim has been made on the basis that Rochester alleges CQC is jointly liable for detriment in respect of its actions in causing her unwarranted referral to the Disclosure and Barring service (DBS), and contends there is an indirect employment relationship. Rochester argues that CQC acted detrimentally and unreasonably upon information from her former employer without verifying it, despite being aware that she was a whistleblower.
Whether or not the Public Interest Disclosure Act (PIDA) 4 and Employment Rights Act 5 are the correct legal tools for dealing with CQC’s behaviour is for the Court to decide. The man on the Clapham Omnibus will very likely see CQC as being at fault, and think that a challenge in law is reasonable.
However, Rochester is an unrepresented, unemployed care worker. CQC is resisting the claim. It is a multimillion pound corporation. Its annual income regularly exceeds £200 million. 6
An FOI enquiry by NHS whistleblower Clare Sardari @SardariClare last year revealed that CQC spends millions annually on legal services:
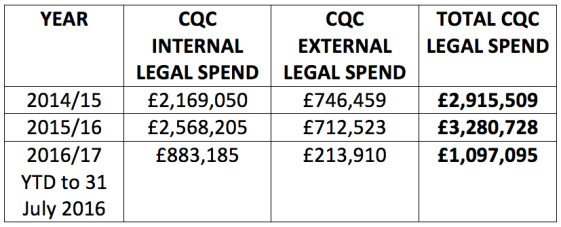
This stark inequality of arms speaks for itself.
Whatever the legal merits of Rochester’s ET claim, it is most unusual for a whistleblower to sue a PIDA Prescribed Person 7. A search has not so far revealed any precedents.
Rochester’s claim follows NHS whistleblower Dr Chris Day’s legal action against Health Education England 8 and Dr Eva Michalak’s action against the General Medical Council 9. These cases posed interesting questions about the definition of the employment relationship under the Public Interest Disclosure Act and or what cases may be heard in the Employment Tribunal.
CQC’s mishandling of Rochester’s safety concerns
It is worth giving this some attention as the case is very typical of how CQC treats whistleblowers from all sectors.
As Private Eye noted of Rochester’s previous whistleblowing experience:
“Ms Rochester complained to the health and social care watchdog immediately after leaving Manor Gardens in April 2013 but it was nine months before inspectors arrived.”
This time, CQC excelled itself by suggesting that Rochester – the whistleblower – should be referred to the DBS before it acted upon her disclosures by making a Safeguarding referral. Within 24 hours of learning of her whistleblower case on 20 April, the CQC advised her employer of its duty to refer Rochester to the DBS. Yet CQC took until 24 April to make a Safeguarding referral to the local authority: “…the first safeguarding referral we made on 24 April 2017”.
Morevover, CQC has now given Rochester’s former employer a clean bill of health despite her serious patient safety disclosures.
The CQC’s re-inspection report dated 30 August 2017 rates the care home a ‘Good’ overall, and ‘Good’ on the ‘Safe’ and ‘Well Led’ domains.
This is despite Rochester raising serious safety concerns with CQC in April, that threw doubts on the leadership of the care home.
The CQC report shows that CQC did not re-inspect the home until 13 July 2017, but claims that it acted in response to concerns:
“We carried out a comprehensive inspection of ********************** on 7 and 8 February 2017. After that inspection we received new information of concerns in relation to people’s safety and the leadership of the service. As a result we undertook a focused inspection on 13 July 2017 to look at these concerns.”
Rochester is concerned that CQC did not act upon her concerns when she first raised them, but re-inspected only after she attended the public CQC board on 20 June 2017 and because she caused the regulator severe embarrassment by exposing its inaction and its dereliction of duty both to her and service users.
Rochester raised concerns with CQC in April about numerous safety issues. Key details from her meticulous disclosure correspondence are provided below in the reference section. This audit trail puts a very human face on the dangers faced by helpless elderly people in care and the serious dilemmas that whistleblowers face everyday.
The broad areas of Rochester’s disclosure to CQC were as follows:
Unsafe staffing, especially at night 10
This is in fact an important national care home quality issue, about which the CQC has been issued with a coroners’s Section 28 warning.
The coroner considered that there should be clear standards set for night time staffing levels:
| “I know that many hospitals are looking carefully at their staffing levels at night particularly in the wards where patients suffer from dementia and may be at a risk of falls through wandering and I am drawing this case to your attention so that you and your inspectors can look carefully at whether staffing levels for night time are adequate to meet the various needs of all the residents/patients in residential, nursing and hospital environments. It seems to me that only two members of staff caring for over twenty four residents, some of whom suffer from dementia and are restless, is not enough to meet all the complex needs, especially with their other duties over a long shift of almost twelve hours.”
Coroner’s Section 28 warning report about death of John Gwyfryn Morris |
This coroner’s challenge not only posed a potential threat to the care industry’s profits but to government austerity plans for health and social care. There is currently no published CQC response to this key coroner’s Section 28 report. David Behan has been asked to disclose CQC’s response to this Section 28 report.
CQC’s latest inspection report on Rochester’s former employer determined that staffing levels were safe, despite the CQC raising and not answering its own question about emergency response:
“However it was not clear how two care staff working at night would ensure emergency situations would be responded to quickly and effectively”
This inconclusiveness by CQC is especially poor given that Rochester had told CQC in an email of 20 April 2017 that the care home falsified records to hide understaffing:
“I also worked with two people who will falsify documentation to say care given when it is not.”
A call bell system which was not fit for purpose and unsafe 11
CQC previously inspected the care home in February and did not detect this problem. It was not mentioned at all in the related CQC inspection report of 25 April 2017.
CQC’s latest report of 30 August 2017 mentions the problem only to say that the care home has promised to address the issue. Rochester is concerned that CQC glosses over the fact that her employer failed to act promptly upon her concerns about this issue.
Poor infection control and lack of staff training 12
In April Rochester told her former employer and the CQC of several examples of serious infection control risks:
| “*********’s infection control procedures are appalling. I have never seen her wash her hands and she does not change her gloves between patients. She will throw or drop soiled pads onto the floor and pile dirty linen outside of doors until she picks it all up and carries it against her uniform to the laundry. When ********* had diarrhoea she did not have a clue re universal precautions..” 12 |
CQC’s previous inspection of the care home in February did not detect this serious problem, and CQC’s related inspection report of 25 April 2017 does not mention infection control. Rochester has concerns about the rigour of CQC’s latest claims that the care home is compliant.
Unsafe manual handling, including pulling drag lifting and pulling patients by the neck, staff not properly trained 13
This is one of the relevant excerpts from Helen Rochester’s resignation letter of 17 April 2017 to her former employer, which she submitted to the CQC as evidence when raising her concerns about the care home’s safety:
| “*********‘s moving and handling is dangerous both to the residents and her. Until told by me she was not using slide sheets when indicated and was not raising beds when the facility was available to her. I have caught her pulling residents by the wrists and neck when moving them on her own and she will do it in front of me so clearly thinks this is acceptable practice. She has never been corrected.” 13 |
Rochester informed the CQC that the care home had residents who were unable to weight bear even though it had no hoist equipment to safely move them.
Even though Rochester told CQC the care home had no hoists, CQC seemed to uncritically accept the care home’s practice of locating immobile residents on the first floor:
“…immobile people were cared for on the first floor”
despite clear recognition in its inspection report that this presented an additional challenge in the event of a fire.
Rochester also informed the CQC that care home staff were falsifying records to pretend that patients were being moved with two staff, when they were being unsafely moved with just one member of staff. 14
However, CQC’s latest report is blandly positive about manual handling at the home and relies in part on what the care home reported, despite Rochester’s warning that the care home falsified evidence:
“Due to the facilities and lay out of the service the mobility of people was reviewed regularly and taken into account within the care provision to ensure people’s safety. We were told that those people who needed assistance in moving used a stand aid as they could hold their weight when standing. Staff received training on moving and handling people safely and we observed them using the stand aid appropriately and safely.”
Poor care of patients with pressure sores and poor related Safeguarding practice 15
CQC’s latest inspection report gives a superficially positive account of the care home’s handling of skin care with focus on documentation, but does not address Rochester’s concerns that the care home did not purchase the appropriate – if costly – alternating air mattress equipment for nursing patients with open pressure sores.
Institutional abuse because patients were taken out of their beds very early in the morning to suit the care home’s regime and staff convenience 16
Rochester told CQC that the care home got residents out of their beds in the small hours of the morning for its own convenience, a very bad practice that marks out the worst homes. The CQC did not re-inspect early enough in the morning to detect this practice.
Despite Rochester’s serious disclosures of numerous examples of poor standards amounting to institutional abuse and the specific example of getting people out of their beds in the small hours, CQC inexplicably only spoke to three residents during its latest re-inspection:
“At the time of the inspection there were 33 people living at ****************. During the inspection we talked with three people who use the service and five relatives.”
Unsafe lack of training for staff and unsafe staff clearance 17
Rochester told the CQC that she was particularly concerned that staff lacked training in safety practices around medicines management, infection control and manual handling.
According to Rochester, staff training at the care home consists of filling in questionnaires whilst provided with the answers. CQC’s inspection regime ticked off the paperwork generated from this ‘training’.
Rochester told the CQC that the care home put her to work unsupervised before her DBS clearance came through.
“There is no issue with my DBS check but that is hardly the point. I could have been anyone with a criminal record and I was left unsupervised in charge of 34 vulnerable adults many of which have dementia purely for the sake of convenience and to avoid them having to employ expensive agency staff over the Easter weekend.”
The latest CQC inspection found no fault with the care home’s clearance procedures.
Nationally, it has emerged that the CQC has resisted the coroner’s criticism and recommendations following the unlawful killing of Ivy Atkin, in which CQC failings regarding DBS scrutiny were considered to present a risk to the public.
| The neglect of Ivy Atkin a care home resident was so gross that an inquest made a finding of unlawful killing. She reportedly lost almost half her body weight in 48 days and was discovered close to death with an infected pressure sore. There was an accompanying criminal conviction of manslaughter against the care home owner. regulator, CQC was criticised for not checking DBS compliance itself and allowing smaller homes to effectively mark their own homework, because of a purported loophole in regulations. The coroner issued a Section 28 warning report on 25 October 2016 and asked CQC to rectify this. CQC did not respond until 21 March 2017. CQC’s response was not published until last month by the Chief Coroner after the lack of a published response was questioned. The response revealed that CQC had resisted the coroner’s recommendation that it should change its practices on DBS:
|

Poor whistleblowing governance 18
Rochester told CQC in April that staff with whom she worked were too frightened to raise concerns. 18
On the ‘Well-Led’ domain, CQC’s latest inspection report has not mentioned that Rochester’s former employer has made factually inaccurate claims about a whistleblower, falsified a dismissal that has been rejected by the Tribunal and made a referral to the Disclosure and Barring Scheme that has also been rejected.
Instead, CQC provides this alternative vision of reality:
“Staff told us they had the opportunity to raise any concern internally and knew there were other agencies to contact if concerns were not addressed. Staff were confident any concern would be dealt with effectively and quickly by the registered manager. Staff told us they felt they were listened to and their views were taken into account. For example, one staff member told us “If anything is needed like any equipment all you have to do is ask and it is provided.”
One effect of regulators giving poor employers good reports is that they can help to undermine a whistleblower’s position.
Quis custodiet ipsos custodies?
I asked the CQC to comment on Rochester’s legal action and it said:
| “The individual who has submitted an employment tribunal claim against CQC, is not and has never been an employee of CQC. The individual has raised a complaint with the CQC and this was not upheld. However, as this is subject to ongoing tribunal proceedings, we will not comment further until these proceedings have been completed.” |
CALL FOR HELP
If there are any lawyers interested in the matters raised by the Rochester case who would like to get in touch or may be able to contribute any information or help of any sort, please get in touch via the contact page of this site.
UPDATE 11 SEPTEMBER 2017
Letter to Public Accounts Committee submitting evidence about Helen Rochester’s case and requesting re-review of whistleblowing:
Letter to Public Accounts Committee 11 Sep 2017 Re-Review of whistleblowing
RELATED ITEMS
Watch Helen Rochester at the CQC public board meeting on June 20 2017 (1.15):
https://cqc.public-i.tv/core/portal/webcast_interactive/291254
FPPR: CQC has lost all moral authority but what will the National Guardian do?
The CQC denies…
https://minhalexander.com/2017/01/08/the-cqc-denies/
Letter to the Health Service Journal’s Patient Safety Correspondent
Ian Paterson and failure by oversight bodies
https://minhalexander.com/2017/06/01/ian-paterson-and-failure-by-oversight-bodies/
NHS gagging: How the CQC sits on its hands
https://minhalexander.com/2016/09/23/nhs-gagging-how-cqc-sits-on-its-hands-2/
Homerton maternity whistleblowers: FOI disclosure of the London Clinical Senate on four maternal deaths and the National Guardian
Care home deaths and more broken CQC promises
https://minhalexander.com/2016/10/08/care-home-deaths-and-more-broken-cqc-promised/
REFERENCES
1 Several networks reported Compassion in Care’s concern’s disclosure about CQC breaches of whistleblowers’ confidentiality
2 From letter 14 July 2017 by Andrea Sutcliffe CQC Chief Inspector Adult Social Care to Compassion In Care
3 From letter 11 August 2017 by Andrea Sutcliffe CQC Chief Inspector Adult Social Care to Compassion In Care:

4 Public Interest Disclosure Act 1998
http://www.legislation.gov.uk/ukpga/1998/23/contents
5 Employment Rights Act 1996 Section 47B
https://www.legislation.gov.uk/ukpga/1996/18/section/47B
6 CQC annual report 2016/17
Click to access CQC_annual_report_accounts_2016_17_web_version.pdf
7 Under PIDA, Prescribed Persons should in theory provide a safe haven where whistleblowers can make confidential, legally ‘protected’ disclosures, but in reality they have poorly defined roles and powers, and a poor reputation.
https://www.gov.uk/government/publications/whistleblowing-guidance-for-prescribed-persons
8 Dr Chris Day’s website:
http://www.54000doctors.org/thecase/1-intro-and-how-this-case-affects-you.html
The Court of Appeal judgment in Dr Chris Day’s case:
http://www.54000doctors.org/judgments/court-of-appeal-judgment.html
9 The Supreme Court judgment in Dr Eva Michalak’s case:
http://www.bailii.org/ew/cases/EWCA/Civ/2016/172.html
10 Examples from Helen Rochester’s resignation letter to her employer, which was sent to CQC on 17 April 2017 as part of raising concerns about the care home’s safety:
“I also suggested if you want real quality care on nights you need an extra member of staff particularly at times when the dependency levels are high.”
“I have come away on all four of my shifts feeling that I have given care that is rushed and barely adequate within the resources I have which have been to the poor standard contained in this letter”
“Over the course of the night I observed both ********** and ********* adapting documentation timings to show things happening when they were not.”
Email 20 April from Rochester to CQC:
“I also worked with two people who will falsify documentation to say care given when it is not.”
11 Email 22 April 2017 by Helen Rochester to CQC:
“Furthermore unless you are by the office or the kitchen you cannot hear any call bells or sensor mats activating so he could have been left unattended for some time.”
12 An example from Helen Rochester’s resignation letter to her employer, which was sent to CQC on 17 April 2017 as part of raising concerns about the care home’s safety:
“********* infection control procedures are appalling. I have never seen her wash her hands and she does not change her gloves between patients. She will throw or drop soiled pads onto the floor and pile dirty linen outside of doors until she picks it all up and carries it against her uniform to the laundry. When ********* had diarrhoea she did not have a clue re universal precautions and I discussed this with ********** on Sunday.”
Rochester reports that there were no liquid handwash dispensers or paper towels in most of the residents’ rooms in April, which meant that staff had to wash and dry their hands using a used bar of soap and a used towel, or leave residents’ rooms to wash their hands.
13 An example from Helen Rochester’s resignation letter to her employer, which was sent to CQC on 17 April 2017 as part of raising concerns about the care home’s safety:
“********‘s moving and handling is dangerous both to the residents and her. Until told by me she was not using slide sheets when indicated and was not raising beds when the facility was available to her. I have caught her pulling residents by the wrists and neck when moving them on her own and she will do it in front of me so clearly thinks this is acceptable practice. She has never been corrected.”
“On the Friday night I worked with her I caught her handling ******* by the ankles in an effort to drag him towards the end of the bed so he could get round the cot side. When I challenged her as to why she was doing this and put the side down she told me she had never been shown this. She also was quick to point out she had asked ********** for advice on this and said he did not know either.”
“I asked ******** what practical moving and handling training she has had. She says nothing but has apparently asked for some and it has not been given. She is reliant on other people supervising her and she is not getting this.”
14 Examples from email 22 April 2017 by Helen Rochester to CQC:
“********* needs hoist to transfer and is/was being drag lifted out of bed by night staff. Multiple skin tears due to poor handing”
“….violent and aggressive and lashes out at staff. Handed over to me needs two to put to bed. Has stand aid to transfer and also has a paralysed left arm. Agency carer (under other team leader instructions) had put her to bed on her own putting both at risk of injury and then team leader falsifies documentation to show two people. At night when there are only two on duty the rest of the home is then left unattended whilst dealing with this challenging lady”
15 An example from an email by Helen Rochester to CQC on 20 April 2017:
“There are serious issues in this home on night duty which i have outlined below. I cannot speak for what happens on days but in the case of resident ********** (cannot recall surname but in room 45) she has pressure sores and it would appear, to the best of my knowledge, nobody (days or nights) has raised this as a safeguarding issue or have they dealt with her inadequate bed. This lady needs an air mattress that alternates pressure before her hips break down as well. At present she is on a foam mattress with some other aids put in. they are not working on her hips or are they designed to.”
16 An example from an email by Helen Rochester to CQC on 20 April 2017:
“I am also aware of institutional abuse happening on nights with the blessing of management. There is a list of 11 residents that have to be got up for the day staff and on Monday – Thursday carer’s start at around 04.15 to do this. I refused to do this at the weekend and when I questioned this I was told “they can sleep in their chairs”. I was also told all 11 have “other needs” that make them eligible for this treatment by the deputy. If that is the case then the home needs to be staffed accordingly so they can be got up unrushed at a sensible time.”
17 Email from Helen Rochester to CQC 22 April 2017:
“I walked out of this home on the morning of the 16th April 2017 I was so disgusted at what I was seeing and being expected to manage. I lasted four nights.
During those four nights I worked unsupervised without a valid DBS check. At the time of writing this email it is still not through. I brought this to the attention of the registered manager on Wednesday 19th April who then lied to me saying it was. As I had not received it I phoned the DBS to check. It was still at stage 4 and not complete.
There is no issue with my DBS check but that is hardly the point. I could have been anyone with a criminal record and I was left unsupervised in charge of 34 vulnerable adults many of which have dementia purely for the sake of convenience and to avoid them having to employ expensive agency staff over the Easter weekend.”
18 An example from Helen Rochester’s resignation letter to her employer, which was sent to CQC on 17 April 2017 as part of raising concerns about the care home’s safety:
“I cannot work like this and I am very uncomfortable with some of the things I have witnessed in only four nights. The problems you have on nights are overwhelming for one person to deal with when they are new. Furthermore ***********’s approach seems to be tackling this through having people into the office for a telling off whereas mine would have been through training and support .
It would then be known it was me who reported all this given I have spoken out at the time of seeing things happening and I will not be able to build working relationships with the people I have to work with for twelve hours.
I also suggested if you want real quality care on nights you need an extra member of staff particularly at times when the dependency levels are high. According to *********** you are legal on paper and “nobody else has had a problem” indicating that I am a problem for raising this. If this is the reaction that is standard then it’s not surprising people do not say anything.”
“However because of ***********’s reaction to me I would feel uncomfortable ever raising a concern again.”


Thanks for publishing this Minh.
I feel very let down by the CQC. I will not comment further at this time, because of the ongoing case.
Their actions towards a whistleblower are bad enough but it’s their failures when they inspected this home almost immediately (for them) after I attended their board meeting that beggar belief.
They found on their re-inspection commencing at 6am:
1) Only 2 members of staff on duty for a home that is laid out over two Victorian buildings with no service lift and a third newer extension block that does have a small lift. There were 33 residents in situ of varying needs according to their report. That is one carer per 16.5 residents. Safe? Apparently so to the regulator who is ignoring section 28 warnings re this.
2) Six residents already in the lounge. Only one of those was apparently able to tell them it was their choice to be there at that time so they went and checked the documentation which apparently said the other five also wanted to be. This is in a home where I had already warned them of false documentation.
Obviously I cannot speak re the residents in the home at this time. When I worked there we had a list of 11 residents to be got up. From recollection the vast majority had a deprivation of liberty safeguarding (DOLS) in place. They cannot make decisions but were documented as doing so. I wonder if the CQC checked this on their most recent inspection. The home is well led apparently.
3) A call bell system still in place 5 months after I raised it as not fit for purpose. Safe? Apparently so according to the regulator who now does not have to pitch up anytime soon to check an alternative it is purchased and working.
4) Residents left in the lounge from before or at 6am with no call bell facility and only the chef “nearby” in her locked kitchen for supervision. Safe? Yes according to the CQC.
On my last working night the emergency call system was activated by a resident in her room. I only heard it as I happened to be near the central display and attended. It was nothing but could have been a real emergency. My agency colleague did not hear it at all due to being in another building so did not attend. Safe?
5) Only two members of staff to respond to any emergency including fire. Safe? Apparently so according to the CQC. I wonder if the man on the Clapham omnibus would agree?
6) The CQC found “adequate” hand washing facilities (one of the most basic safety issues) but do not elaborate. When I worked there none of these frail vulnerable elderly people had a liquid soap dispenser and paper towels in their rooms for staff to wash their hands before going onto another resident. Safe?
I could go on but the question has to be asked if the CQC rate all of this as safe, what would they class as inadequate?
LikeLike