By Dr Minh Alexander, NHS whistleblower and former consultant psychiatrist
In August 2017 I reported on four years of data published on the Chief Coroner’s website, which revealed that over 1700 coroners’ reports on action to prevent future deaths had been issued between July 2013 and July 2017, 57% of which related to NHS organisations.
Worryingly, there were no published responses from the parties who had been sent coroners’ warning reports in 62% of these cases.
I made some further enquiries, focussing on the Chief Coroner’s office and central NHS bodies, from the Department of Health and Social Care downwards. This has uncovered further anomalies and concerns.
My full update findings, with all supporting responses from the Chief Coroner Department of Health and Social Care and arms length bodies and disclosed documents, are reported here
This is the summary of the update report:
“Summary
How diligently does the government protect the public from risks?
This is a follow up paper about the system response to coroners’ Section 28 warning reports on Action to Prevent Future Deaths, and how the NHS in particular responds risks to public safety.
The overall picture at the top of the NHS is one of defensiveness, half-answered questions and some conflicting accounts from different bodies, or even from the same body. It is very unclear to what extent the audit cycle is safely closed after coroners raise a concern.
If that is the example set at the top, this raises concerns about governance through the system.
Since 2013, coroners in England and Wales have been under a duty to issue a Section 28 report on action to prevent future deaths (also known as PFD reports) if they find risk factors that pose a threat to life.
Parties who receive a Section 28 report must provide a written response within 56 days.
By law, Coroners are required to send their report and any responses to the Chief Coroner.
Coroners and Justice Act 2009
“Schedule 5 Powers of Coroners
Action to prevent other deaths 7 (1) Where— (a) a senior coroner has been conducting an investigation under this Part into a person’s death, (b) anything revealed by the investigation gives rise to a concern that circumstances creating a risk of other deaths will occur, or will continue to exist, in the future, and (c) in the coroner’s opinion, action should be taken to prevent the occurrence or continuation of such circumstances, or to eliminate or reduce the risk of death created by such circumstances, the coroner must report the matter to a person who the coroner believes may have power to take such action. (2) A person to whom a senior coroner makes a report under this paragraph must give the senior coroner a written response to it. (3) A copy of a report under this paragraph, and of the response to it, must be sent to the Chief Coroner.”
http://www.legislation.gov.uk/ukpga/2009/25/pdfs/ukpga_20090025_en.pdf
The Chief Coroner has discretion to publish the reports and corresponding responses, or not:
The Coroners (Investigations) Regulations 2013
“PART
28. (5) On receipt of a report the Chief Coroner may—
(a)publish a copy of the report, or a summary of it, in such manner as the Chief Coroner thinks fit; and
(b)send a copy of the report to any person who the Chief Coroner believes may find it useful or of interest.”
http://www.legislation.gov.uk/uksi/2013/1629/part/7/made
The Chief Coroner has advised in his 2016/17 annual report that in 2016, 46% (241,211 of 524, 723) of registered deaths were referred to coroners. 40,504 of these cases that were reported to coroners were deemed to need investigation and inquest.
Section 28 reports are exceptionally issued and represent very significant concern by coroners. The Chief Coroner advised that between June 2016 and July 2017, 375 Section 28 reports were issued. My enquiries and other data have shown that whilst an NHS trust may have hundreds of inquests, they may typically be issued only a handful of Section 28 reports.
The coronial system relies on reporting but is hampered by failures of reporting. This context increases the significance of Section 28 reports.
Earlier this year, I analysed four years of data published by the Chief Coroner and found that there were no published responses to 62% of the Section 28 reports on the Chief Coroner’s website.
Four years of published coroners’ Section 28 reports in England and Wales, 24 August 2017
In some cases, this has since proved to be because respondents had failed to comply with Section 28 notices. For example, the government failed to respond to a coroner’s 2015, pre-Grenfell warning about the need for sprinklers in housing stock, especially for vulnerable residents. It only replied to the coroner in December 2017, after an enquiry about its missing response:
https://www.judiciary.gov.uk/publications/emma-waring/
https://minhalexander.com/wp-content/uploads/2018/01/171214-dclg-response-to-coroner-waring175602.pdf
My search of the Chief Coroner’s website was laborious as the website has minimal search capability, and Section 28 data has to be manually sifted.
I also found no published evidence of corresponding central analysis by the NHS of Section 28, from the Department of Health and Social Care downwards.
Subsequent enquiries to the Chief Coroner’s office and the Department of Health and Social Care and other central NHS bodies revealed some conflicting statements about whether responses to Section 28 reports had been withheld from publication by the Chief Coroner.
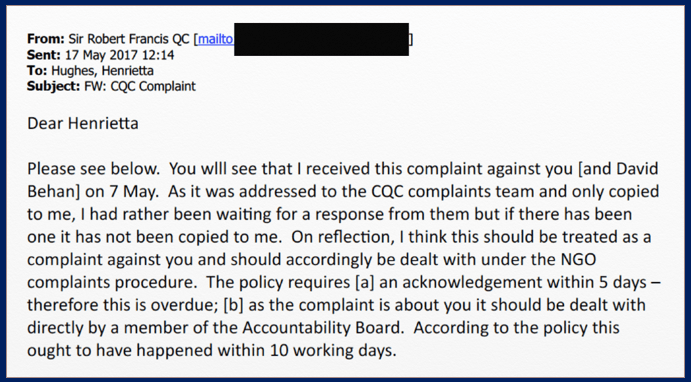
CQC claimed that it had asked for some its responses to Section 28 reports to be withheld from publication by the Chief Coroner. The Chief Coroner advised that his office had not received any such requests. In the face of this information from the Chief Coroner, the CQC indicated that it did not contest the Chief Coroner’s account of events.
There also appeared to be variance between some coroners and the Chief Coroner’s office. The Chief Coroner advised that he published all or most of the material received from coroners.
A sample of 21 coroners reported that they had submitted all Section 28 reports and related responses to the Chief Coroner. However, the Chief Coroner’s website showed a total of 342 Section 28 reports from these 21 coroners over a four year period, for which there were published responses in only 128 (37%) cases.
Similarly, information from some test enquiries to trusts also suggested not all Section 28 reports that are issued to trusts reach the Chief Coroner’s website. The Chief Coroner was alerted to this.
Nonetheless, the Chief Coroner has now committed in principle to full publication of all Section 28 reports and related responses.
There is no apparent system for ensuring compliance by coroners and the Chief Coroner has stated that he merely encourages coroners to write and submit reports when appropriate.
With regards to government learning from the Section 28 data, there appears to have been a change of policy in that the Chief Coroner’s office stopped producing regular trends analysis of Section 28 reports after September 2013. The office also advised that it was not sufficiently resourced to make improvements to its public facing database, to give the public greater access.
With regards to the NHS, there was limited evidence of systematic analysis and learning, with only relatively recent attempts to track and analyse trends shown by Section 28 reports. Moreover, the learning from thematic analyses has not been shared with service providers or the public.
There was reluctance by CQC to disclose analyses that it had undertaken, with initial claims that these were exempt from disclosure that were eventually waived.
The Department of Health and Social Care (DHSC) showed the greatest resistance to learning. It essentially claimed that analyses of Section 28 data were not worthwhile because the data is insufficiently standardised. This is difficult to square with its arms length bodies’ differing approaches and commitment to better future analysis of this data. Indeed, NHS England considered coroners’ Section 28 reports to be a ‘reliable’ source of data.
There was also no evidence that the arms length bodies are working together to reliably share information on Section 28 reports. NHS Improvement advised that it relies on trusts to notify it of Section 28 reports, when it could in fact make use of routine notifications by coroners to the CQC.
The DHSC, NHS England, the CQC and NHS Improvement all refused to disclose copies of their responses to particularly significant Section 28 reports that had been missing from the Chief Coroner’s website. NHS England, CQC and NHS Improvement relied on a past ICO decision that responses to coroners’ Section 28 reports are court documents and exempt under Section 32 FOIA. This is despite the fact that the ICO has confirmed to me that there is nothing to stop these bodies from voluntarily disclosing their responses to coroners if they chose to do so:
“An organisation can choose to proactively publish information even if that information is exempt from disclosure under the Freedom of Information Act, or if the organisation is not subject to the Act.”
ICO Group Manager of FOI Appeals and Complaints Department 6 December 2017
The DHSC tried to washed its hands of responsibility by claiming that it was the Chief Coroner’s responsibility to publish the documents, and stated that FOI exemptions would likely apply in any case.
This concerted opacity is a failure of leadership and accountability. It leaves major questions about under-resourcing of the NHS and systemic governance flaws unanswered. For example, whether national failings in managing ligature point risk have been addressed.
That said, although the CQC and NHS England refused to disclose key missing responses to some key Section 28 reports, some of the missing responses have now quietly appeared on the Chief Coroner’s website.
For example, the CQC’s previously missing 2014 response to a 2013 Section 29 report about national guidelines on night time staffing levels, which shows that CQC side-stepped the issue of committing to firm standards.
Another previously withheld but recently published CQC response to a high profile avoidable death at the private facility the London Bridge Hospital, rated ‘Outstanding’ by the CQC, reveals that the hospital initially informed the CQC that the death was ‘expected’.
Overall, there needs to be a more proactive, joined up and transparent system response to coroners’ Section 28 reports.
The government should ensure that all Section 28 reports and responses are published, and the NHS should adopt a policy of open reporting on Section 28 reports, responses and related analyses, subject to redaction of third party personal data where required.
The NHS should not be hiding behind FOI exemption, especially when the Chief Coroner has agreed that all Section 28 reports and responses should be published.
The Chief Coroner’s office should also be adequately resourced so that it can once again report on a regular basis on national trends in Section 28 reports and maintain a database with sufficient functionality to allow meaningful, open access by the public.”
I provide below a vignette to illustrate some of the manoeuvring by central NHS bodies:
How the Care Quality Commission dodged the coroner’s warning about John Gwynfryn Morris’s (‘Gwyn’s’) death and safe staffing standards

Gwyn suffered from dementia and died of hypothermia after going missing from a care home one night in December 2012.
The staff on duty were very stretched. There were two staff caring for 24 residents and Gwyn slipped out of the care home whilst staff were attending to an incident.
The coroner issued a warning report to the CQC on 11 November 2013, stating:
“I am drawing this case to your attention so that you and your inspectors can look carefully at whether staffing levels for night time are adequate to meet the various needs of all the residents/patients in residential, nursing and hospital environments. It seems to me that only two members of staff caring for over twenty four residents, some of whom suffer from dementia and are restless, is not enough to meet all the complex needs, especially with their other duties over a long shift of almost twelve hours.”
In retrospect, this was a significant and politically sensitive coroner’s letter in the context of the subsequent, hugely controversial decision in June 2015 to suspend the National Institute for Health and Social Care Excellence’s (NICE) work on safe staffing.
The CQC should have provided a written response to the coroner’s warning within 56 days. The coroner indicated that he expected a response by the week ending 10 January 2014.
However, I found that CQC’s response was missing from the Chief Coroner’s website as of July 2017.
Accordingly, I asked CQC for a copy but CQC refused to disclose its response, claiming an FOI exemption that according to advice from the ICO was entirely discretionary.
I subsequently noticed that CQC’s response to the coroner had been quietly published on the Chief Coroner’s website.
This showed that CQC did not reply to the coroner’s warning until 16 April 2014.
CQC’s response to the coroner of April 2014 skirted around the issue of safe staffing standards. CQC refused to commit to a clear opinion about whether the home had been under-staffed.
However, CQC assured the coroner:
“The care that is given to people who live with dementia is taken extremely seriously by the Commission.
…In terms of night time inspections, the Commission does currently carry out inspections at night if we have a concern about the care being provided at night, and we will be undertaking more out-of-hours inspections in the future.”
The CQC also informed the coroner that it had undertaken a ‘themed inspection’ on the care of people with dementia between December 2013 and February 2014.
CQC promised it would address safe staffing issues in a national report in May or June 2014, based on its themed inspection.
A national CQC report on the care of people with dementia was eventually published in October 2014.
This was what the report said about levels of staffing:
“4.4 Staffing
Staff have an important role in supporting people living with dementia to have a good quality of life. Having the right knowledge, skills and time is essential to good care. Key to achieving this is ensuring that there is the right number of staff, with the right values, who are supported through training, supervision and access to resources.”
“4.4.3 Numbers of staff
The time staff had to spend with people, over and above providing the required aspects of personal and clinical care, varied across the care homes and hospitals visited. However, it was often a significant factor in caring for people living with dementia. We spoke to several managers and staff who expressed frustration that, due to a lack of resources, they were not able to provide the care needed.
We saw how people living with dementia were affected when there was not enough staff, including changes to their behaviour that caused distress to them and others around them.”
So, no clear commitment to rigorous inspection, and no measurable, enforceable standards.
In fact, just empty platitudes and nothing to embarrass any Minister.
And despite the CQC’s above emollient assurances to the coroner that it would conduct more out of hours inspections, whistleblowers and FOI data show that CQC’s efforts remain very poor.
The Secretary of State for Health and Social Care promised over two years ago that there would be ‘Learning Not Blaming’. This needs to start at the top.
RELATED ITEMS
Care home deaths and more broken CQC promises
CQC, coroners’ warnings and the neglect of older people in hospital
Who Speaks for the Dead? Ivy Atkin and the Unaccountable CQC
The above update report on the government’s handling of coroners’ warnings has also been summarised in a blog for the Centre for Health and the Public Interest. The Centre’s website features many items on health and the public interest, such as the implications of PFI and the safety of private health services.











 `Letter from David Behan 20 April 2017
`Letter from David Behan 20 April 2017
















 Source: Public Concern at Work
Source: Public Concern at Work






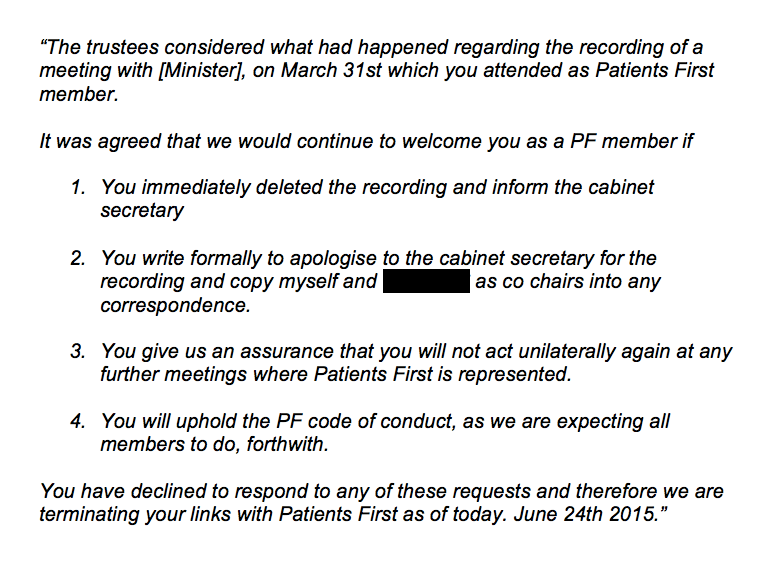 I asked Patients First why it was expelling X but not another member, who had made frequent reference on social media to making covert recordings of her employer.
I asked Patients First why it was expelling X but not another member, who had made frequent reference on social media to making covert recordings of her employer.