This was helpful reportage, apart from a bum note of someone slipping in a misleading and inaccurate claim of Jeremy Hunt being an anti-gagging NHS hero, when he was no such thing.
Paul Calvert, a former police officer, latterly a coroner’s officer and one of the whistleblowers who revealed the failings at NEAS, has continued to talk to the media.
He has now revealed more details of a typical NHS whistleblower’s journey, and the often futile attempts to escalate through successive layers of indifferent, incompetent and or malign management.
Calvert, like so many other NHS whistleblowers who have been failed, attests to the ineffectiveness and in his case the harmfulness, of NHS whistleblowing arrangements.
This is a model where a trust employee is appointed by senior trust managers to act as a purported reporting point for whistleblowers. This individual is supposed to challenge senior trust managers if necessary, and to make referrals outside of their organisations to regulators. In good trusts it is unnecessary, in corrupt trusts it is a conflicted, compromised non-starter.
“In his first approach to a “Freedom to Speak Up” casework manager at NHS England, Mr Calvert wrote: “I have a reasonably held belief that the North East Ambulance Service have caused harm, to members of the general public, by concealing, altering and destroying relevant information that should have been supplied to HM Coroner.
“The trust’s patient safety department does not have the necessary policies and processes in place, in order to ensure the trust meets its statutory obligations as prescribed by law.
“For the past year, myself and colleagues have continued to raise our concerns, with the relevant individuals.
“We are aware that these concerns not only failed to be addressed, but are constantly ‘pushed under the carpet’.”
Mr Calvert, who is from Peterlee, told the case worker he had already raised his concerns with his MP, Grahame Morris, who represents Easington and subsequently discussed the matter in Parliament.
Mr Calvert has said is he aware of 90 cases where changes have been made to medical reports at inquests to hide mistakes by ambulance crews where someone has died.
They include the case of 17-year-old Quinn Beadle, from Shildon, who died by suicide in 2018.
Key details omitted from the report to coroner in the hearing the establish the circumstances surrounding her death.
In his email last July, Mr Calvert said: “The North East Ambulance Service are continuing to fail members of the public and putting lives at risk by failing to address these very issues.
“I am of the opinion that these matters require urgent attention to prevent the public suffering any further harm.”
Mr Calvert, who claims he has been the victim of bullying and is unable to work due to ill health, said NHS England did “little to nothing” regarding his concerns and merely passed his information to the Care Quality Commission.
He said: “The trust continues to ignore that there is a problem and is unwilling to listen or consider the concerns being raised or acknowledge the supporting evidence regarding this.
“The trust also continues to bully and harass the members of staff who are attempting to raise the concerns, taking punitive action against the people speaking up, whilst the parties responsible for the failings are afforded complete impunity.
“However, the mechanisms for raising concerns within the trust are entirely ineffective, being used to cover up and delay matters, rather than investigate and address the concerns raised.” [My emphasis]
It seems unclear from the Northern Echo report whether NHS England did anything about this extremely serious allegation, even though it would have been well within its power to take action. I have sought clarification from the NHSE/I Head of whistleblowing.
Corporate Freedom To Speak Up Guardians at North East Ambulance Service
According to trust board papers Jennifer Boyle former Trust Secretary was previously trust Freedom To Speak Up Guardian.
Her LinkedIn entry shows she was NEAS trust secretary between May 2015 to June 2021.
She has since moved to Gateshead Health NHS Foundation Trust where she is also Trust Secretary, working under Yvonne Ormston CEO, who was NEAS CEO until 2019.
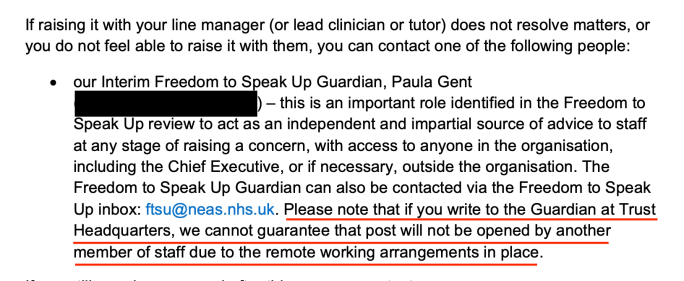
According to NEAS trust board papers, the role of NEAS Freedom To Speak Up Guardian has since been taken over by another person from trust corporate services, Paula Gent, whose LinkedIn entry describes her as “Executive Personal Assistant to Director of Strategy, Transformation and Workforce at North East Ambulance Service”, but makes no reference to the Freedom To Speak Up role.
Hard to see how corporate appointments would make whistleblowing frontline staff feel very comfortable, or understood.
Shockingly, NEAS’ whistleblowing policy tells trust staff that there is no guarantee that their highly sensitive disclosure emails will only be opened by the Freedom To Speak Up Guardian. It does NOT say who else might open their emails:
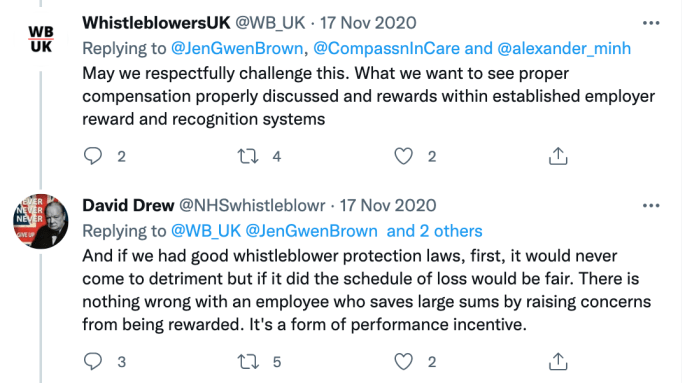
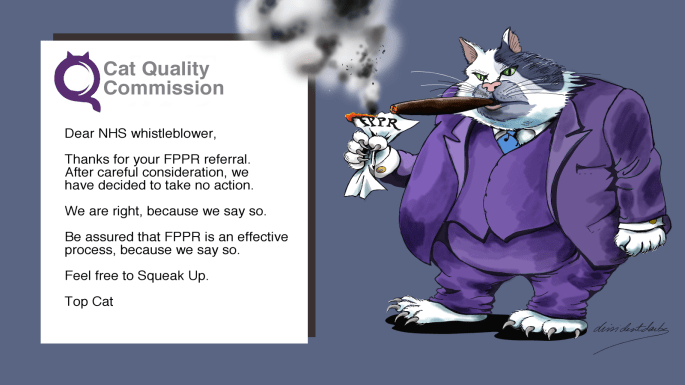
So does life imitate caricature?
The NHS National Freedom To Speak Up Guardian
Sitting at the head of the failed NHS Freedom To Speak Up project is a propaganda outpost of the Department of Health and Social Care, known as the Office of the National Freedom To Speak Up Guardian. It came embedded with DHSC personnel from the outset.
In a totally conflicted and compromised arrangement, the National Guardian is funded and overseen by NHS England/ Improvement and the Care Quality Commission (CQC), but is also supposed to hold these bodies to account.
The National Guardian is appointed by the CQC, with participation from NHSE/I. She reports to the CQC chief executive. She also reports to the government via the Department of Health and Social Care.
Her funding comes from CQC and NHSE/I. She produces annual reports for CQC and NHSE/I boards.
CQC and NHSE/I oversee her work through a board which consists of a representative from CQC, NHSE/I and the National Guardian.
This committee used to be called the “Accountability and Liaison Board”. Latterly the name has been softened by the NGO to the “Advisory and Liaison Board”.
Farcically, despite all the above, we are expected to believe that the National Guardian is “independent”:
“the role is independent”
“The NGO will set its own priorities, have its own budget and identity and speak independently of its sponsor bodies.”
AND that the NGO will hold the whole system including CQC, NHSE/I and DHSC to account:
“Make recommendations to individual and national organisations (NHS trusts and foundation trusts, NHS England, NHS improvement, CQC and the Secretary of State for Health) on trends, common issues and interventions to drive and support culture change across the NHS”
Yes, and pigs can fly.
And where are the National Guardian’s reviews on NHS England/Improvement, CQC and DHSC’s whistleblowing failures?
Oh yes, of course, there aren’t any.
The National Guardian is not in the business of giving NHS staff truthful information about the real risks of whistleblowing. She and her Office pump out rose-tinted claims about how staff will be supported by Freedom To Speak Up Guardians, when the evidence shows that this does not reliably happen.
I have challenged misinformation by the National Guardian’s Office on several occasions. There is a current complaint about the latest National Guardian lodged with the Chair of the CQC about such a matter.
The latest concerns by Paul Calvert represent another hole in the jerry-built Freedom To Speak Up wall.
National Guardian’s planned review of speaking up in ambulance services
The National Guardian’s Office started THINKING about a thematic review of speaking up culture of ambulance trusts in June 2020, after the staff suicides at East of England Ambulance Service NHS Trust made national headlines.
The NGO continued thinking about it until this spring, when I started asking about progress.
The NGO FOI response to my enquiry stated that the work was “in the early stages”:
“We are in the early stages of this review process, and therefore have not agreed final parameters yet”.
The NGO refused to disclose relevant correspondence, claiming exemption on grounds of Section 22 FOIA documents intended for publication. Nonsense of course, as such documents would not be published. Importantly however, they would show the dates on which work had actually commenced.
Overall, the NGO has displayed little sense of urgency, despite the obvious distress and strain on ambulance services:
Even the Director of Nursing at WMAS has repeatedly been in recent news, making dire predictions of unsustainable service pressure, inevitable patient deaths and looming service collapse:
It is unsurprising that the National Guardian’s Office is so little trusted by frontline NHS staff that it receives very few whistleblowing disclosures. This includes NHS ambulance staff.
The April FOI response revealed that the National Guardian had received a mere twelve whistleblowing disclosures from NHS ambulance staff in the period 1st April 2017 to 31st March 2021
This week, the National Guardian finally published terms of reference for her thematic review:
Only five of the 10 ambulance trusts will receive in depth scrutiny. It is not revealed which five trusts have been selected. I have asked the NGO to specify which trusts have been chosen and why.
Former ambulance staff can contribute to the thematic review.
BUT individual whistleblowers’ cases will NOT be investigated.
No embarrassing details wanted, just a demonstration that “something” has been done.
This perfectly complements Sajid Javid’s announced review of NEAS, which has not satisfied relatives or whistleblowers, who want a public inquiry:
Please click and add your signature to this petition to reform UK whistleblowing law – whistleblowers protect us all but weak UK law leaves them wholly exposed, lets abusers off the hook and it is a threat to public safety.
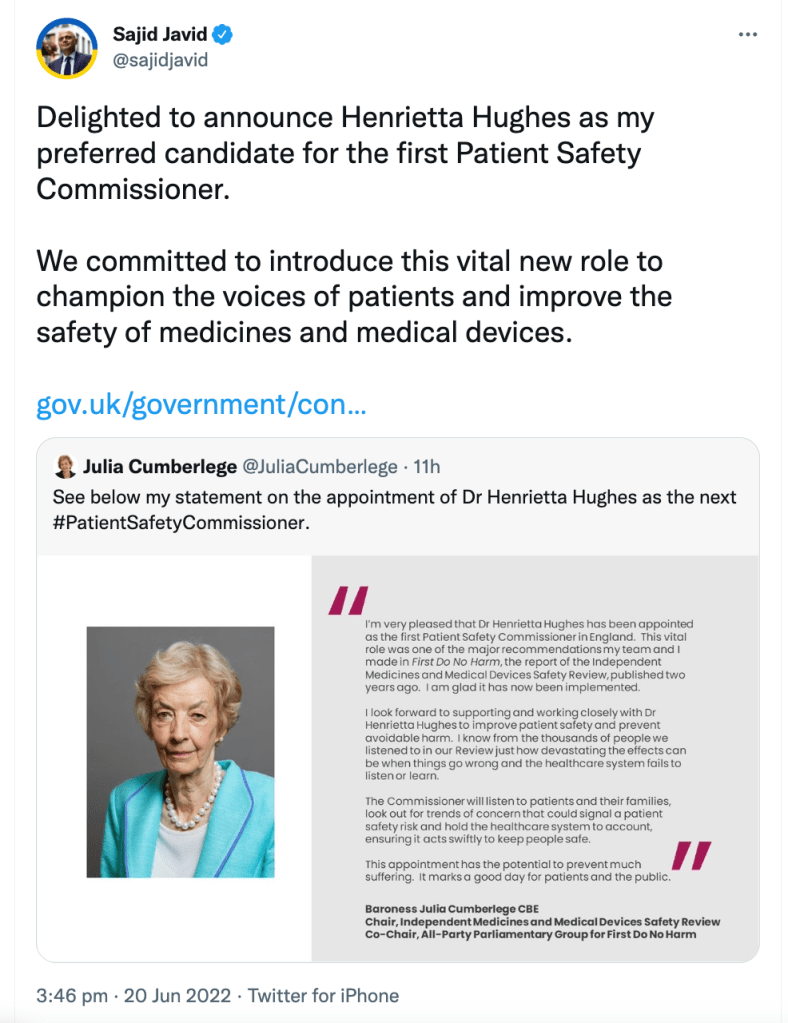
Many harmed NHS whistleblowers, who know her from her last government job as National Freedom To Speak Up Guardian, will likely groan inwardly at this news.
The Patient Safety Commissioner is a new role, which is as yet ill-defined. Perhaps predictably so.
It is limited in scope to the safety of medicines and medical devices:
“The core role of the Commissioner will be to promote the safety of patients in the context of the use of medicines and medical devices and to promote the importance of the views of patients and other members of the public in relation to the safety of medicines and medical devices.”
It was proposed in a 2020 review led by Julia Cumberlege which had been tasked with making “recommendations for improving the healthcare system’s ability to respond where concerns have been raised about the safety of particular clinical interventions, be they medicines or medical devices.” The review examined the care failures over pelvic mesh surgery, valproate and primidos.
The review proposed the creation of a Patient Safety Commissioner, which in its general description sounded very similar to the slippery job description of the NHS National Freedom To Speak Up Guardian.
A loose, vague remit to do what it pleases, with limited accountability attached to this freedom. The Cumberlege review states:
“The Commissioner would be free to look at whatever they wish to within her/his remit of patient safety, open to requests for areas to consider and free to publish their findings. The Commissioner would be accountable to the Parliamentary Health and Social Care Select Committee. Alongside annual hearings and using the power to bring matters to the attention of the Committee, the Commissioner could receive and act on information and requests from the Committee, and from the Secretary of State for Health.”
“…the Commissioner would have a general statutory power ‘to do anything which appears to it to be necessary or expedient for the purpose of, or in connection with, the performance of its functions. This would give the Commissioner the power to take a permissive and flexible approach to gathering information necessary for specific issues and to issue advice to those who are engaged in activities relating to improving patient safety. Giving the Commissioner the power to bring matters to the attention of both Houses of Parliament and the Secretary of State for Health and Social Care would provide a proportionate and focused means of highlighting where improvements are needed.”
Something that could have been written by Sir Humphrey.
Or perhaps the long-served William Vineall, Director of NHS Quality, Safety and Investigationsof the Department of Health and Social Care since 2016, who appears to be the appointing officer judging from the DHSC job advert.
The person specification is tragi-comic:
“Set an example of integrity and ethical leadership, reinforcing the position’s reputation as an open and independent role, which puts the needs and interests of the public, patients and service users first.”
“The PSC will be under an obligation to publish a set of principles to govern the way in which they carry out their core duties. The PSC must take steps to consult patients and to ensure that patients are aware of their role.
The everyday workings of the PSC are to be finalised. Regulations will be made setting out further details about the appointment and operation of the commissioner, for example the terms of office.”
There is no guarantee therefore, that the final Office will reflect the recommendations of the Cumberlege review.
It seems more likely that the Patient Safety Commissioner will be another political tool for the DHSC, and more waste of public money on window dressing.
The Department doth protest too much about independence:
“How independence will be safeguarded
We expect the Secretary of State to work with the PSC to agree how their independence will be safeguarded.
It is common for commissioners to be sponsored by the government departments with relevant policy responsibility while maintaining their independence.”
So good they had to say it twice:
“Independence
To be effective, it is fundamental that the commissioner has the freedom to act independently.
It is common practice for commissioners to be sponsored by the government department with relevant policy responsibility. The Children’s Commissioner does an exemplary job whilst being sponsored by the Department for Education. The Victims’ Commissioner does the same and is sponsored by the Ministry of Justice.
A relationship with DHSC would allow the commissioner a powerful place within the system. A commissioner which is entirely removed from the policy department can be more easily overlooked by government. It is crucial that the right person is appointed into the role, someone who is confident and knowledgeable of the sector to bring weight and intelligence to the commissioner position.
Independence will necessarily be exercised in the carrying out of the commissioner’s functions. For example, the commissioner will have the power to make recommendations or reports to the Secretary of State, who will then be under a duty to consider and respond, ensuring that the department is kept accountable. We will expect that the commissioner makes any such reports or recommendations independently, without recourse to or clearance from the Secretary of State or DHSC.”
I complained yesterday to the new Chair of the CQC about the National Guardian’s Office ongoing public communications, which mislead NHS staff about the real risk of whistleblowing.
“I contacted the national office myself and was told that they do not get involved in individual cases or disciplinary processes and that I will be free to submit a case review form if/ and when I win a case for unfair dismissal in court.”
“This approach is appalling. I was lucky enough as I had a cast-iron case, and was resilient and financially capable of taking the case to the court. I do not know anyone else around me who would have survived this process. The ferocity and avalanche of unwarranted insults would have destroyed anyone.”
It is preposterous to tell whistleblowers to come back years later after they have been mauled by the litigation process. It is not only a great injustice to the whistleblower, but an incomprehensible reaction to the patient safety issues that have been buried along with the whistleblower. What happened on Hughes’ watch was the equivalent of more soil being shovelled on top.
This was a far cry from the role described in the Freedom To Speak Up Review on NHS whistleblowing which proposed the role of the National Guardian. It was supposed to be a “nimble” office that sought redress for both harmed whistleblowers and patients who were harmed by failures to handle whistleblowing properly:
“…to recommend to the relevant systems regulator or oversight body that it make a direction requiring such action.
This may include:
– addressing any remaining risk to the safety of patients or staff
– offering redress to any patients or staff harmed by any failure to address the safety risk
– correction of any failure to investigate the concerns adequately”
Conveniently for the government and many senior NHS managers, Hughes never accepted responsibility for helping to ensure such redress.
She also refused to support the one thing that would make a real difference to whistleblowers and therefore patients – legislative reform and replacement of useless UK whistleblowing law. Even though her role included identifying and acting on barriers to speaking up.
If Hughes is confirmed as Patient Safety Commissioner, it would be surprising to see any real change of direction.
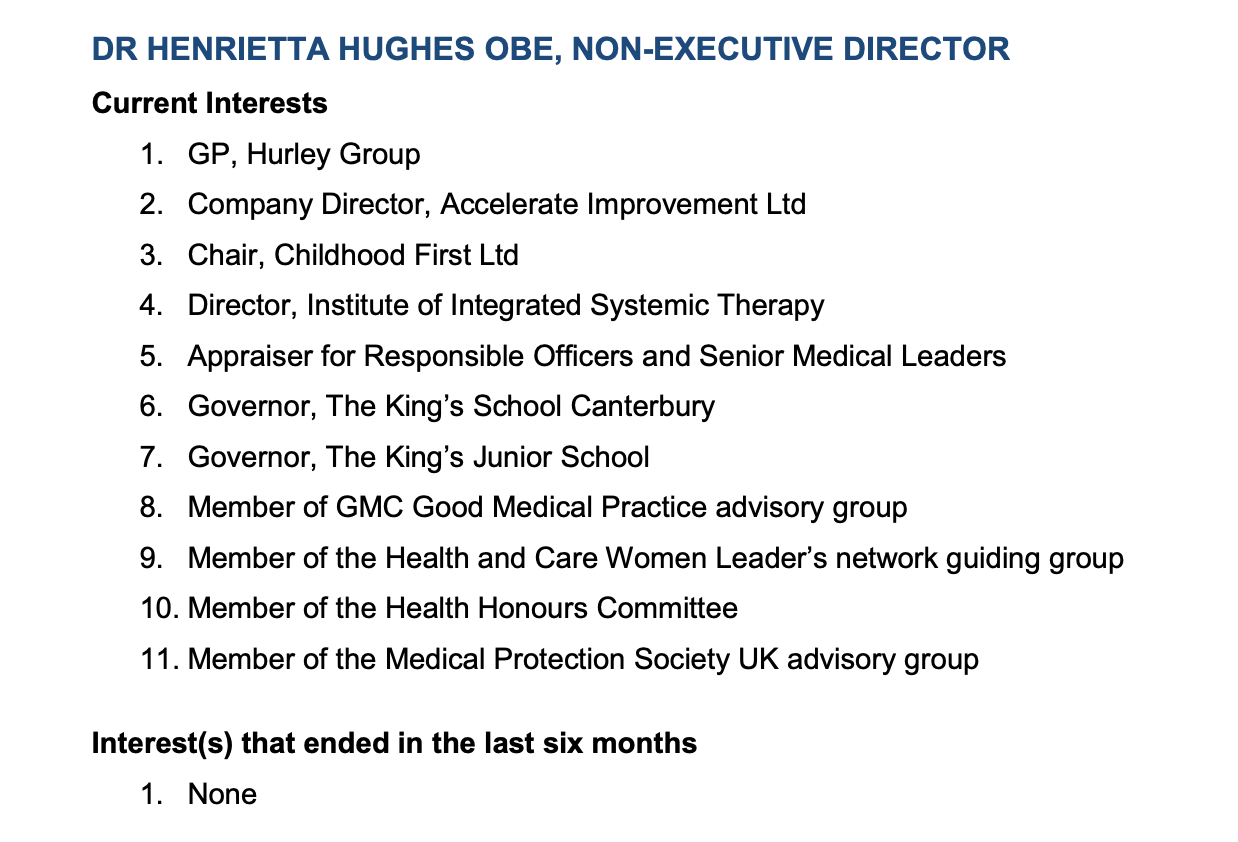
Henrietta Hughes’ declaration of interests
Since leaving her post as National Guardian in September 2021, Hughes has been busy.
In December 2021, she set up a company, Accelerate Improvement Ltd Company number 13784948. This is categorised under “Other human health activities”. The firm has not yet filed accounts according to Companies House. I have been unable to find any digital footprint for the firm beyond basic company details.
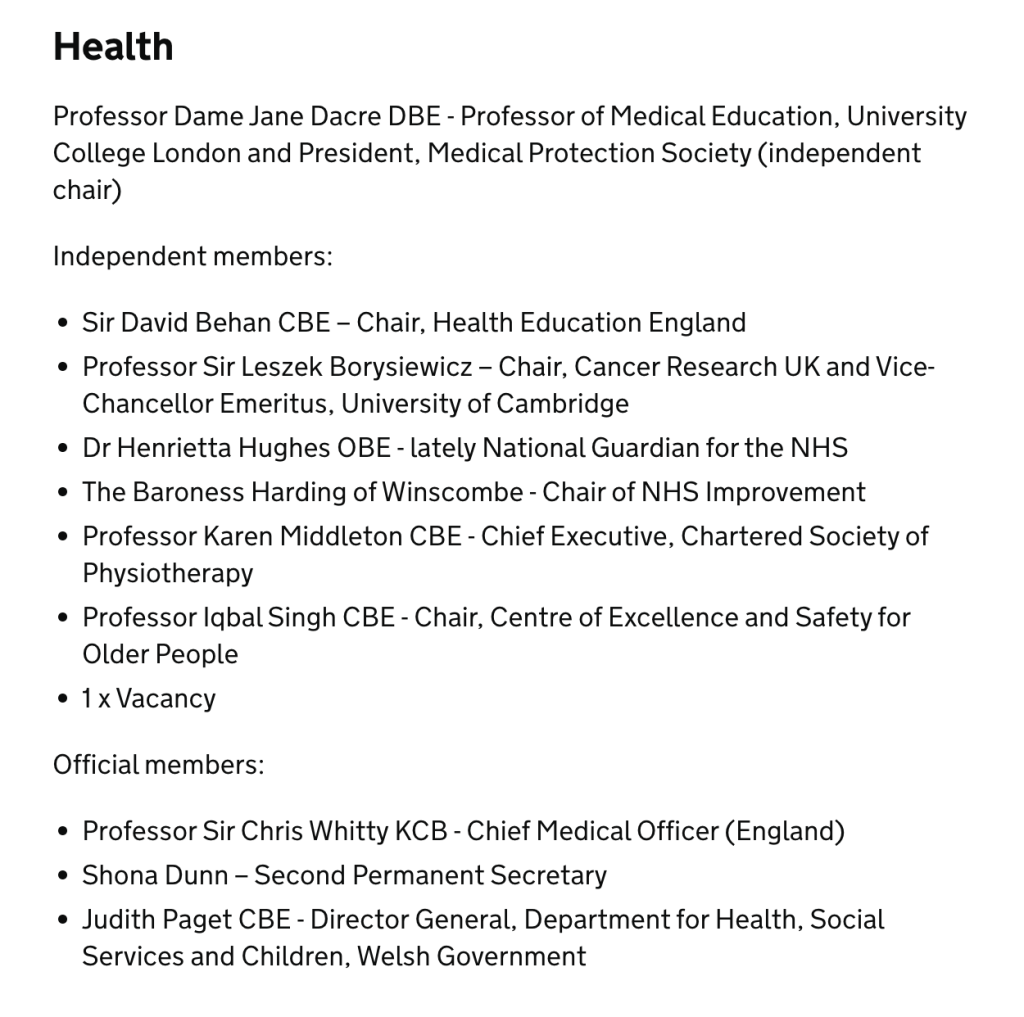
The declaration revealed interests at the heart of government with a seat on the Health honours committee – a useful lever on power, in company with David Behan and Dido Harding amongst others.
There is also a seat at the General Medical Council and at the Medical Protection Society – a medical defence union, defending doctors against negligence claims.
The latter is an awkward fit with her putative role as the Patient Safety Commissioner.
Hughes is also Chair of Childhood First South, Childhood First East Anglia and Childhood First Midlands three businesses categorised as “Other residential care activities not elsewhere classified”, for children. They have charitable status. According to Companies House, she became a person of significant control of these companies on 10 November 2021.
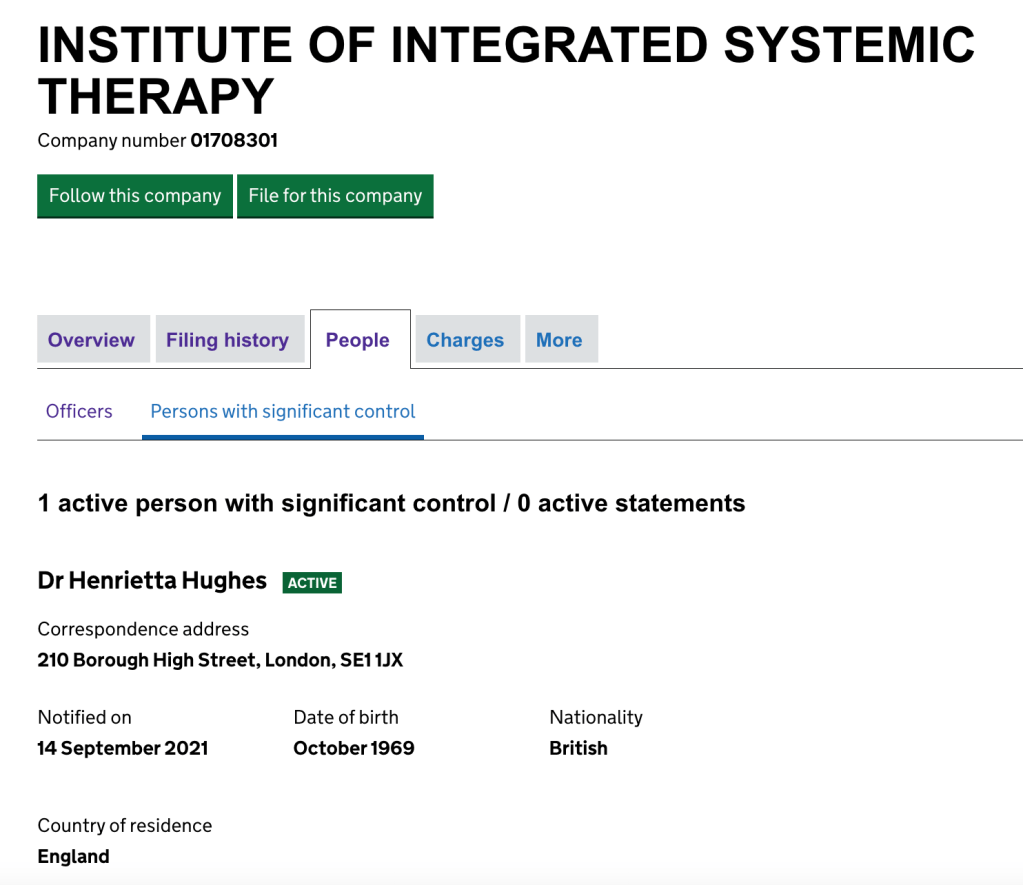
It was also announced that she would take up the Chair of the Institute of Integrated Systemic Therapy in September 2021, of which she is listed as the person in significant control.
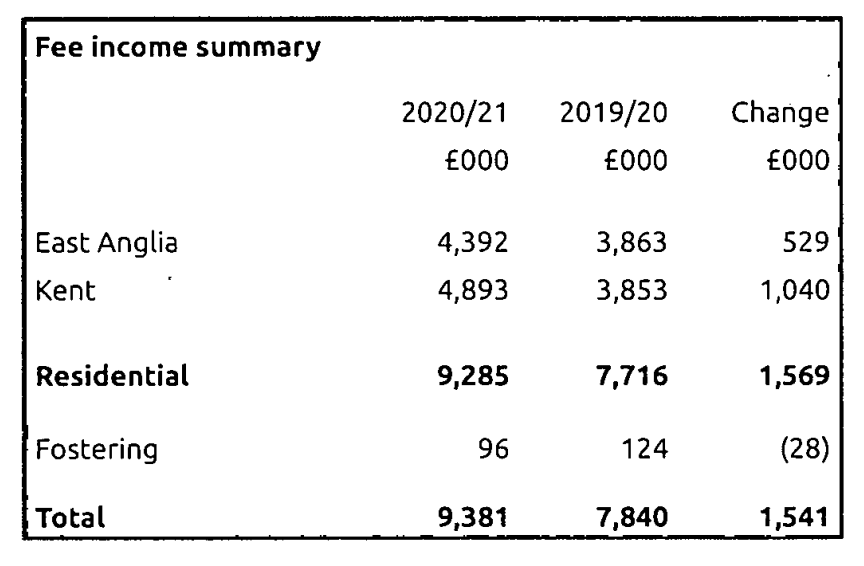
The Institute of Integrated Systemic Therapy was formerly a company named “Childhood First” until 2015, and appears to be the parent company for the regional Childhood First branches. It has charitable status. According to the company’s reports, it runs children’s homes, as therapeutic communities, and fostering services. Fee income in 2020/21 was almost ten million pounds:
Which of these many jobs will Hughes give up to become the Patient Safety Commissioner?
Whatever, the trajectory is clearly one of an insider, not a challenger.
Here is Henrietta Hughes and her former Office, independently and rigorously challenging NHS England – her former employer and one of the key sources of suppression and top-down bullying in the NHS:
Oh how they trembled.
One can see why the Minister is delighted too:
As one commentator from Left Foot Forward quipped after Hughes’ supremely embarrassing oxytocin/Love Actually gaffe,
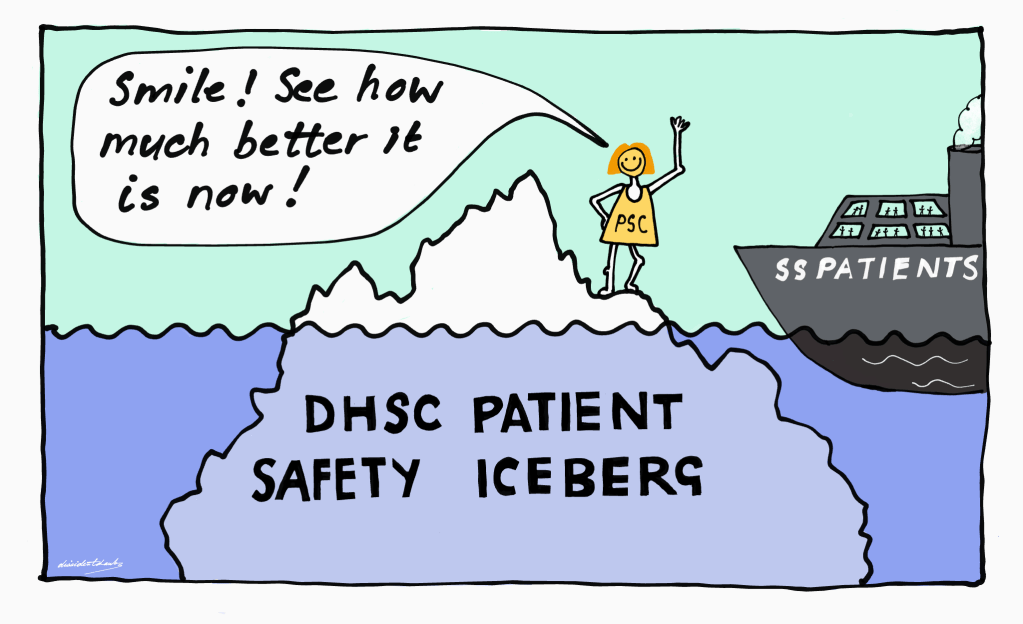
Patients and families similarly need to brace for problems with the Patient Safety Commissioner. The likely scenario will be that a few cases/ issues will be paraded, but under the iceberg’s waterline, more people will be failed.
And expect propaganda. Lots and lots of it.
PETITION
Please click and add your signature to this petition to reform UK whistleblowing law – whistleblowers protect us all but weak UK law leaves them wholly exposed, lets abusers off the hook and it is a threat to public safety.
Here are just some cases of NHS whistleblowers who continued to be severely harmed during the years in which Henrietta Hughes was the NHS National Freedom To Speak Up Guardian:
This case of ‘Paul’ (a pseudonym for the story) reported by Byline Times documents how an NHS whistleblower was failed by Henrietta Hughes’ Office, in a repetition of behaviour very similar to her strategic inaction at Brighton:
“But Paul did not have much luck with the National Guardian’s Office. It turned out that it had previously given the trust in question three months to improve its treatment of whistleblowers – in a case review which the NGO confirmed to Byline Times was published in 2018 – and this deadline had been far exceeded. Instead of recognising this as a systemic issue, the NGO decided not to do anything in order to give the new trust chief executive time to deal with these issues. This appears to be the complete opposite of being a ‘guardian’ of helping people to speak up.”
Henrietta Hughes’ Office breached a whistleblower’s confidentiality at Harrogate. The trust chief executive told the whistleblower that it was Hughes herself who breached confidentiality. An NHS Improvement investigation concluded that it was an underling who breached confidentiality. But Hughes failed to ensure that the whistleblower received a timely apology from her Office or that there was proactive learning:
By Dr Minh Alexander retired consultant psychiatrist 16 June 2022
Summary: The Employment Tribunal (ET) has been very critical of governance by University Hospitals Birmingham NHS Foundation Trust (UHB) in the whistleblowing case of Mr Tristan Reuser, surgeon. Misleading, inaccurate information was given to an advisory body to justify Mr Reuser’s suspension. David Rosser the medical director, now CEO, made a misleading declaration in referring Mr Reuser to General Medical Council. Other concerns have added to governance failings identified by the ET. There are questions about whether the General Medical Council and Care Quality Commission have taken robust enough action against those who treated Mr Reuser unfairly. The GMC at least issued Dr David Rosser with a warning for making a misleading declaration to the GMC. Twenty five of twenty six GMC referrals by the trust since 2012 had medical director sign off. It is therefore important to ensure that doctors are fairly treated. The CQC is especially open to criticism because it has deemed UHB is compliant with CQC Regulation 5 Fit and Proper Persons despite the ET’s criticism of David Rosser. FOI material from the trust has revealed an apparent conflict of interest in the trust’s Fit and Proper Person process (FPPR). A non executive director who worked with David Rosser as MHPS Designated Board member, overseeing the trust’s suspension and disciplinary action against Mr Reuser, later helped to oversee the trust’s FPPR review on David Rosser’ detrimental actions against Mr Reuser. CQC also misleadingly claimed to have received an “independent” Fit and Proper Person (FPPR) review report on Rosser. However, the report was in fact jointly written by a UHB trust employee and a solicitor from a law firm that had a prior commercial relationship with the trust. When CQC was challenged, the chair of the CQC FPPR panel Rosie Benneyworth Chief Inspector of Primary Care tried to brazen it out. She has so far not accepted that CQC has done anything wrong. In response to an FOI request, CQC admitted to accepting at least three FPPR investigation reports that were written partly or entirely by NHS trust staff. CQC has also admitted that it in fact asked UHB to carry out an external FPPR review. Through hindsight goggles, CQC excused its failure to enforce acceptable practice by UHB by denying it has powers to insist that providers follow better FPPR process. This is despite numerous references in CQC’s published and internal guidance to its intention to ensure “robust” FPPR process by providers. As a small concession, CQC apologised in its FOI response for its previous misleading claim that the Rosser FPPR review was “independent”. But CQC still insisted that support to the FPPR review from a law firm which was an existing UHB supplier was “independent”. Shockingly, there is evidence that CQC was informed of the above conflicts of interest which compromised the Rosser FPPR process before the CQC decided to rubber stamp the trust’s governance. I will be making a fresh FPPR referral to CQC on the board of University Hospitals Birmingham NHS Foundation Trust and the trust’s former chair Jacqui Smith based on several matters, including the abuse of process by the trust board in asking a subordinate to determine a senior’s fitness. Natural justice and common decency would tell anyone – except it seems the CQC – that the latter is very, very wrong. Evidence of CQC’s further failures on FPPR will also be submitted to parliament.
Backgroundand the GMC’s findings
Mr Tristan Reuser was an experienced senior surgeon at University Hospitals Birmingham NHS Foundation Trust who the Employment Tribunal determined was unfairly dismissed after he whistleblew about patient safety issues of safe staffing and theatre cover.
The ET also found that his then medical director Dr David Rosser, now the trust CEO, made a misleading referral to the General Medical Council omitting the fact that Mr Reuser was a whistleblower. This was in contravention of GMC’s procedures to protect whistleblowers. Under guidelines produced for the GMC by former Court of Appeal judge Sir Anthony Hooper, an incorrect declaration of this sort should trigger a review of the referring senior doctor’s Fitness to Practice.
The ET’s criticism was serious and raised doubts about whether Dr Rosser made an inadvertent mistake.
These are the relevant passages from the Employment Tribunal judgment of 8 October 2018 which raised doubt about whether Dr Rosser’s failure to inform the GMC that Mr Reuser was a whistleblower was a matter of simple oversight.
“Misleading the GMC
23.1 The GMC were given inaccurate and misleading information and those failings were serious.
23.2 The respondent suggested that these failings were both inadvertent and after the decision to dismiss and hence irrelevant. However, it seems to me that I am entitled, and required, to consider all the circumstances when, for example, considering whether to draw adverse inferences in the whistle-blowing claim. It is also potentially relevant in the context of assessing the independence and neutrality of Dr Rosser.
23.3 In his referral to the GMC Dr Rosser’s failure was far more than the omission of a piece of insignificant information. He was required to address whether the claimant had raised protected disclosures and asserted positively that, “To my knowledge Mr Reuser has not been involved in any whistleblowing episode or other attempt to raise concerns within the organization.”
23.4 It may well be that Dr Rosser was unaware of the full details of the Hooper Review on the handling by the GMC of cases involving whistle blowers but, as the responsible officer, he was required to be aware of the main principles and purpose. For example: “If a doctor being referred to the GMC has raised concerns about patient safety or the integrity of the system with the organization making the referral, then the necessary steps should be taken to obtain from the organization material which is relevant to an understanding of the context in which the referral is made.” “Investigators assessing the credibility of an allegation made by an organization against a doctor who has raised a concern should take into account, in assessing the merits of the allegation, any failure on the part of an organization to investigate the concern raised and/or have proper procedures in place to encourage and handle the raising of concerns.”
23.5 In relation to that latter quote, it was not in dispute that the respondent had failed to properly investigate and respond to the claimant’s concerns. It is possible that, irrespective of any link to the reasons for the claimant’s dismissal, Dr Rosser wanted to conceal this failure.
23.6 The Hooper review continues: “Failure to answer the question truthfully would no doubt lead to the signing doctor’s fitness to practise being investigated and, if discovered during the course of the investigation, would be an important factor in assessing the credibility of the allegation.”
23.7 Dr Rosser was taken in re-examination to the GMC response to Hooper and confirmed that he believed all documents from the GMC were given to him by the GMC liaison officer.
23.8 Dr Rosser initially suggested that he must have overlooked the claimant’s whistleblowing letter when writing to the regulator. That appears surprising given that the letter was included with, and referred to in, the Claimant’s Statement of Case and emailed separately to the disciplinary panel before the hearing. It was also referred to at the hearing just 4 days before Dr Rosser wrote to the GMC.
23.9. Dr Rosser accepted that he was required to consider the documents on both sides before reaching a decision. The decision was reached and written on the same day as the GMC referral was made. Dr Rosser wrote both letters. It is unlikely, therefore, that he had forgotten the protected disclosure.
23.10. In response to this challenge, Dr Rosser’s second, somewhat contradictory, explanation was that he misunderstood the legal terminology and did not consider that the letter should be treated as a protected disclosure.
23.11 It seems to me surprising that the Respondent’s Responsible Officer would not understand what amounted to a whistle blowing episode, not least because he asserted that he had focussed on encouraging reporting of concerns. He certainly ought to have enquired about any whistle blowing episodes before making an express representation about them to the regulator.
23.12 In any event his assertion was that there had been no “other attempt to raise concerns within the organisation.” If Dr Rosser had not identified the claimant’s letter as containing protected disclosures it remains difficult to understand how he did not view them as “concerns”.
23.13 Dr Rosser has not written to the GMC to inform them that he misled them. He asserts that he told the liaison officer but there is no record of that discussion. If Dr Rosser did inform the GMC it is, at best, surprising that they did not write to Mr Reuser to inform him of the new information received, nor was there any mention of it in their findings”
David Rosser’s referral did not result in any GMC action against Mr Reuser.
Instead, I and others referred David Rosser to the GMC for his misleading GMC referral and he subsequently received a warning on 22 July 2021 for his misleading referral.
An FOI request by fellow NHS whistleblower Maha Yassaie @Lady_yassaie has revealed that 25 of 26 of GMC referrals by UHB since 2012 were signed off by the medical director:
It is important therefore that doctors are treated fairly by the medical director.
Shortly after the GMC warning, Rosser relinquished his GMC registration. This coincided with challenges to the GMC from some referrers about the veracity of the regulator’s claims that Rosser’s error in misleading the GMC was an isolated incident.
I have seen correspondence from a year prior to the July 2021 GMC warning, about an earlier concern raised with the GMC about incorrect evidence by Dr Rosser on another occasion. The individual who raised this concern with the GMC also wrote to the then UHB chair Jacqui Smith in October 2019 raising this issue and they questioned Rosser’s fitness. Smith reportedly never replied.
Another referrer had raised concern with the GMC about David Rosser signing off a incorrect declaration on maternity safety at his trust, which had to be retracted. His personal sign off was revealed by an FOI request to NHS Resolution. The incorrect declaration was amongst several made by a number of trusts, which resulted in wrongly paid discounts on insurance having to be repaid to NHS Resolution, as reported in an Independent story of 7 March 2021.
According to the GMC’s record of the investigation hearing on 22 July 2021, David Rosser’s barrister Fiona Horlick QC argued that his incorrect declaration to the GMC:
“was clearly an isolated incident in a previous unblemished career”
The GMC record indicated that David Rosser was in attendance when this submission was made on his behalf. Did he at this point recall that he had also made a mis-declaration to NHS Resolution, a mis-declaration publicised by the press four months before the GMC investigation committee hearing? If he did, should he have disclosed this to the GMC?
Although the GMC claimed in its warning of July 2021 that David Rosser was “developing” insight, he later gave an interview to the Health Service Journal which seemed to minimise his actions in misleading the GMC. He stated in the interview:
“At the end of the day, after two and a half years of intensive investigation, the accusation was that I made a mistake on the GMC referral. I can live with that frankly, that I made an administrative error,” he added.”
University Hospitals Birmingham NHS Foundation Trust withheld damaging documents from the Employment Tribunal
UHB withheld documents which revealed that it had suspended Mr Reuser based on false information. It should in fact have given Mr Reuser the documents at the time of his suspension as a matter of policy.
The trust later failed to produce the documents during the legal disclosure process for the Employment Tribunal and it also failed to disclose the documents in response to a subject access request by Mr Reuser.
Mr Reuser only managed to obtain the revealing documents through a subject access request to the National Clinical Assessment Service (NCAS), to whom UHB had provided the false information which had led to NCAS agreeing his suspension.
The ET judge noted:
“25.1 The Respondent disclosed no documents at all from NCAS, either in the litigation or via the SAR. Mr Reuser obtained them direct from NCAS. I was invited to draw the inference that they were withheld intentionally.”
In the ET judge’s view, the information given to NCAS by the trust was seriously misleading:
“25.2 It appears that Dr Ryder gave NCAS seriously misleading and inaccurate information as identified earlier in my findings. This further supports my view on apparent bias and/or incompetence at a senior management level.”
Cost orders against NHS trusts are very rare. Tribunals do not like to impose costs on cash strapped public bodies.
The fact that a cost order was made represented a significant criticism of UHB.
Does the CQC which need a dictionary to understand the word ‘independent’?
Despite the specific criticisms by the original ET judgment against David Rosser regarding his reliability as a witness;
Despite his misleading GMC referral on Mr Reuser;
Despite his ultimate responsibility as medical director for the unjustified suspension and unfair dismissal of a medical whistleblower;
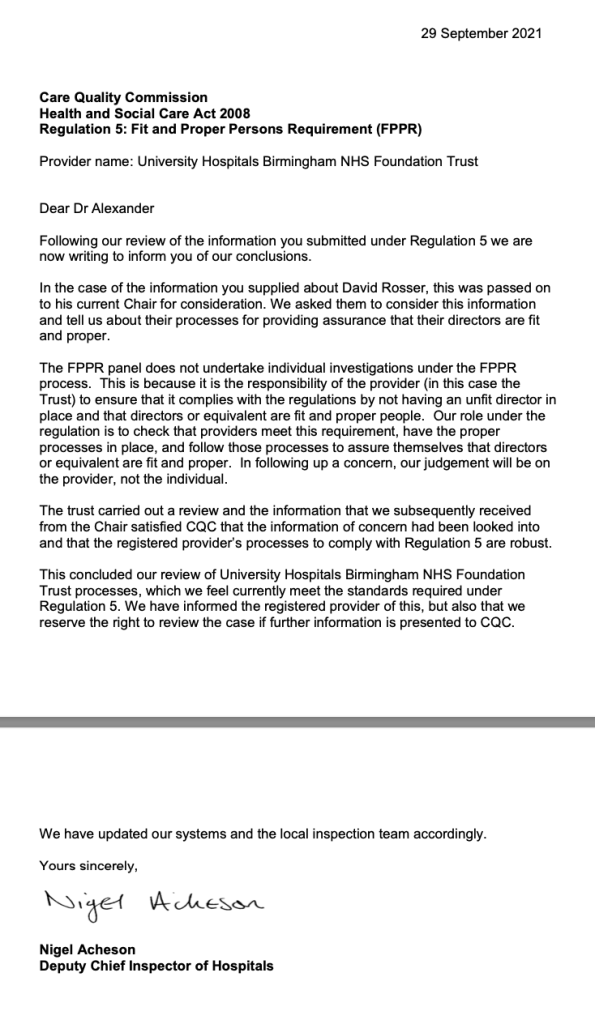
CQC last year typically concluded that David Rosser was a Fit and Proper Person under Regulation 5 (FPPR).
CQC accepted assurance by UHB that Rosser had been thoroughly investigated in this respect and had passed.
Because of concerns about the independence of the FPPR process undertaken by the trust, I asked CQC to confirm that it had reviewed primary documents itself and that it had satisfied itself that there was no conflict of interest in the trust’s process.
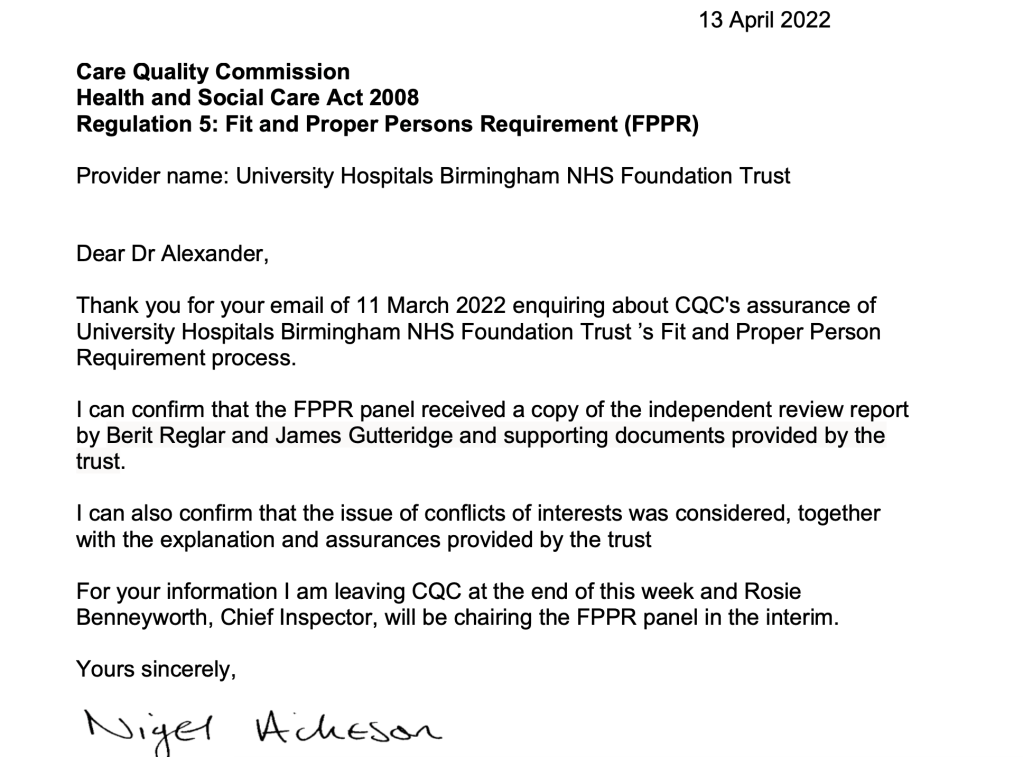
The CQC replied that it had satisfied itself that UHB’s process was sound and that its FPPR panel had received a copy of an “independent” FPPR report by two individuals, Berit Reglar and James Gutteridge.
The problem with this is that, astonishingly, cursory checking revealed that Berit Reglar is a longstanding trust employee, and that James Gutteridge is a partner at Bevan Brittan LLP, a law firm that had done recent work for UHB and which in some of its promotional material had listed UHB as a “key client”.
Furthermore, I have now seen correspondence in which Berit Reglar stated that she was in joint charge of the Rosser FPPR investigation process.
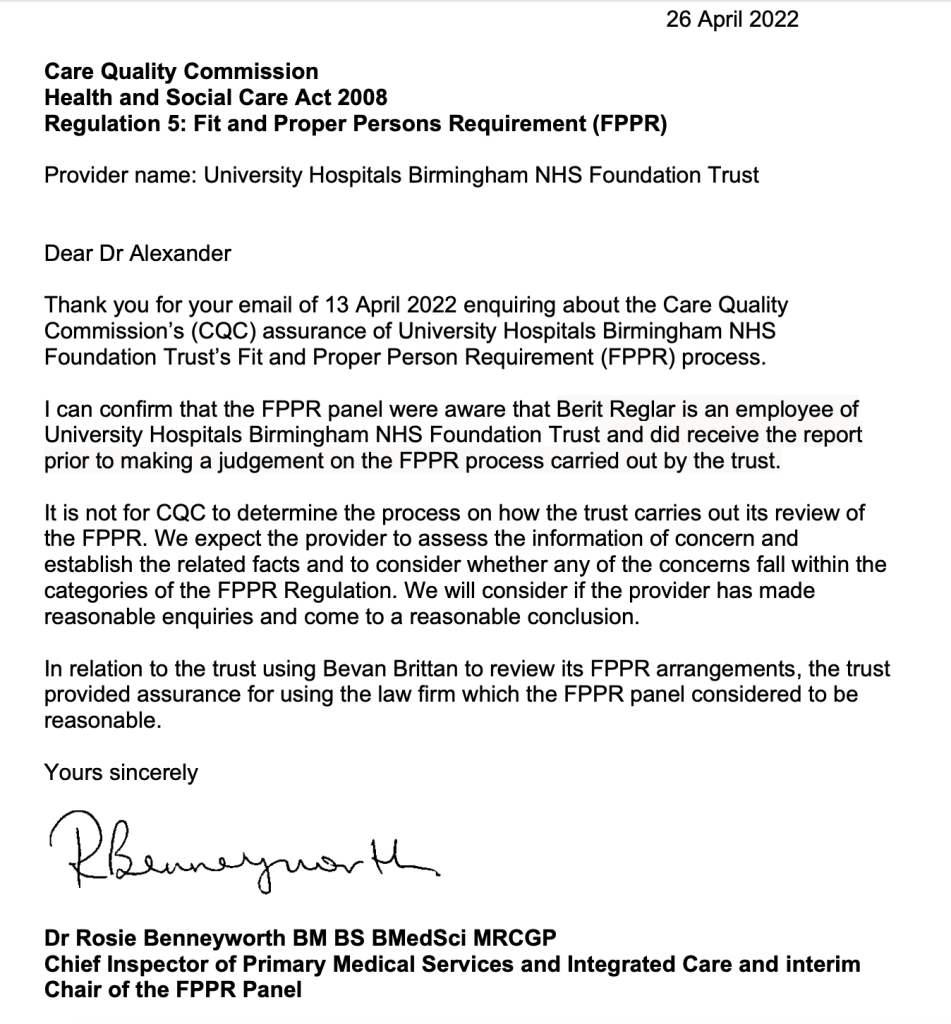
When I confronted CQC about its false claim that UHB’s report was “independent”, the regulator through Rosie Benneyworth Chief Inspector of Primary Care and current Chair of CQC’s FPPR panel, firmly stuck its chin out. Benneyworth insisted that CQC had done nothing wrong. In doing so, Benneyworth appeared to tear up the CQC FPPR rule book to justify what her panel had done, claiming that CQC had no say over a trust’s FPPR process:
Based on past experience I imagine her letter could well have emanated from CQC’s regrettable legal department. CQC has not yet responded to my challenge.
It transpired on further checking that the CQC had been warned of the conflict of interest regarding Bevan Brittan, an existing supplier, acting as an “independent” FPPR investigator. This was before CQC shut down the FPPR.
University Hospitals Birmingham NHS Foundation Trust spending on Bevan Brittan
The ICO’s records show that UHB unlawfully tried to resist an FOI request for details of spending over £25K in 2018, citing a “prevention of crime” and a “commercial interests” exemption. This is the ICO decision notice overruling UHB’s refusal:
Why did UHB stop routine publication of this financial information? Why would it not wish to be held accountable or to allow the public to scrutinise the record for any matters of possible concern?
Most recently, UHB was asked by NHS whistleblower Clare Sardari @SardariClare for information on its spending on Bevan Brittan’s services, but has failed to supply this so far, resulting in an ICO order to disclose.
Strikingly, it has been alleged that UHB met David Rosser’s full legal expenses, and that a statement to this effect was made by trust officers at a governors’ meeting in July 2021. The trust has been asked to clarify if there is any basis to this allegation, and has not yet responded.
Additionally CQC had been sent evidence that the trust, through Berit Reglar the internal FPPR investigator, gave Mr Reuser false information that Bevan Brittan had no prior connection with the trust:
From email by Berit Reglar of 3.11.2020, answering questions by Mr Reuser about the trust’s proposed FPPR process
The loss of trust arising from this and other matters was such that Tristan Reuser decided not to take part in the trust FPPR process.
Moreover, Mr Reuser became concerned about an issue of impartiality because Berit Reglar made an incorrect assumption about him in the course of correspondence. She admitted that she wrongly assumed he had made a GMC referral:
From email by Berit Reglar 3.11.2020, answering questions by Mr Reuser about the trust’s proposed FPPR process
[NB It is relevant to note here that the GMC decided to only pass a single anonymous referral to its investigators, but withheld my earlier referral on identical grounds. One possible explanation is that this circumvented the requirement to provide feedback to a named referrer.]
FOI data on CQC’s handling of FPPR
I requested update data on whether CQC had ever made a finding of breach of regulation 5 Fit and Proper Persons and to see how many of the “independent” FPPR reports CQC has accepted had in fact been written by NHS trust personnel from the very trusts under investigation.
Shocking, but no surprise to many NHS whistleblowers who are familiar with the whiff of collusion between CQC and abusive employers.
According to the FOI disclosure, CQC’s FPPR panel has accepted 95 FPPR referrals for consideration since 2014 but only 29 formal FPPR investigation reports were produced arising from this, raising questions about the rigour of CQC’s regulatory process.
The CQC claimed that three of the 29 formal FPPR investigation reports produced were authored partly or wholly by NHS trust staff, one of which would have been the Rosser FPPR investigation.
Significantly, CQC claimed that that it originally advised University Hospitals Birmingham NHS Foundation Trust to commission an external FPPR report:
“In the case of the review for the FPPR referral made for University Hospitals Birmingham (UHB) we suggested to the trust that they may benefit from an external independent review.”
CQC made post hoc excuses for not ensuring that UHB followed a suitably “robust process”, despite all its guidance, internal and published, indicating that CQC expects providers’ FPPR process to be “robust”. CQC gave these mealy mouthed excuses for letting UHB get away with a flawed and conflicted FPPR process:
“CQC are not in a position to insist on how the trust carries out their review of the fitness of an individual when an FPPR referral has been made.”
“there is scope for the trust to do a proper review without going out to someone independent.”
In UHB’s case, CQC tried to whitewash UHB’s flawed process thus:
“The trust gave their reasons for carrying out the review lead by a member of UHB staff (who is a qualified and practising solicitor) supported by an independent HR lawyer. The panel accepted that their decision was reasonable.”
CQC did at least apologise for misleading me by initially claiming that the UHB FPPR investigation into Rosser was “independent”:
“You asked if CQC reviewed any primary sources of information such as independent review reports on Dr Rosser’s fitness as a trust director (as opposed to any summarised information provided by the trust Chair) and in response to your question we referred to the Berit Reglar and James Gutteridge review as the independent review. We should have stated this was an internal review with independent support. Please accept our apologies for the error in our reference.”
Note that CQC still maintains that support to UHB’s FPPR review from the law firm Bevan Brittan, which was an existing trust supplier, was “independent”.
So conflict of interest would seem to be a highly plastic concept in the CQC-verse.
FOI data from University Hospitals Birmingham NHS Foundation Trust on the FPPR process on David Rosser
The trust did not respond to an FOI on this issue despite several reminders, including to its Chair, until ordered to do so by the Information Commissioner.
In this letter Harry Reilly responded to my concern that the trust had not recognised what a grave step a GMC referral was, in relation to ET criticisms of trust process. Reilly maintained that referral to the GMC “should not be seen as a punitive measure”.
This is so devoid of empathy that it is hard to comment on. There is no acknowledgment here of the damage done to doctors, regardless of intent.
Doctors have died of suicide and suffered acute illness such as heart attacks and strokes whilst under GMC investigation. After the GMC’s recent bizarre pursuit of Dr Arora over trivia, Chaand Nagpaul the BMA Chair went to war on the dysfunctional GMC process, calling for radical reform with the comment:
“Being notified and being investigated by the GMC can be one of the most traumatic experiences in a doctor’s life”.
But the rigid, stonewall attitude by UHB perhaps explains why it has kept digging itself into HR holes and does not seem to learn.
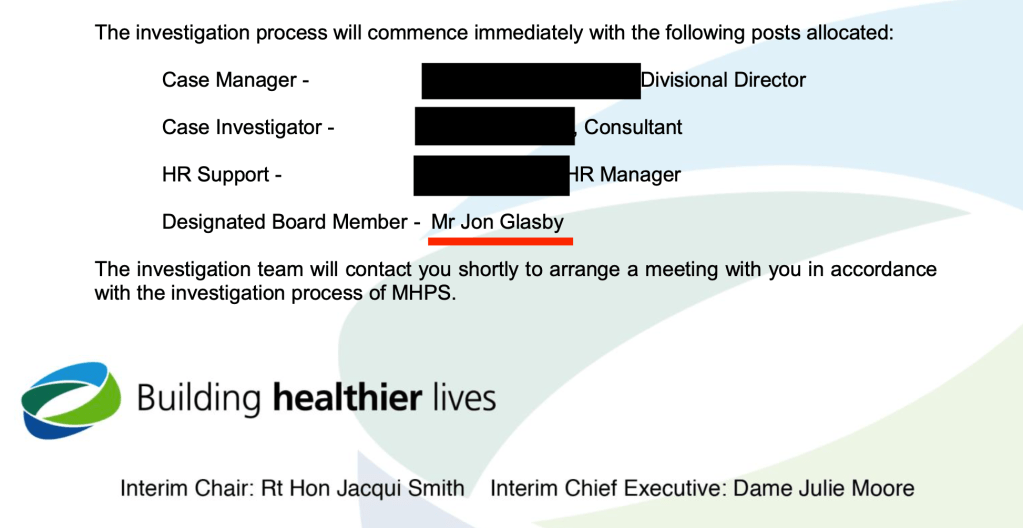
In addition, the trust claimed to me in its FOI response that there was no known conflict of interest in its FPPR process on David Rosser. However, the FOI response revealed that one of the trust’s non executive directors, Jon Glasby a social worker by background, acted as a support to the former trust Chair Jacqui Smith in the Rosser FPPR process:
This raised an additional issue of conflict of interest because Glasby had previously worked with David Rosser (then as Medical Director) to oversee the trust’s suspension of and disciplinary action against Tristan Reuser, in Glasby’s capacity as MHPS Designated Board Member:
MHPS (Maintaining High Professional Standards) is the disciplinary/incapability process for doctors
The apparently incorrect denial of conflict of interest in a statutory disclosure under FOIA has to be noted as another example of the trust providing unreliable information.
I have written to Harry Reilly trust chair to ask for the trust’s response to the apparent conflict of interest concerning Jon Glasby. There has been no response so far.
And should the CQC have detected this clash when it assessed the soundness of the trust FPPR process?
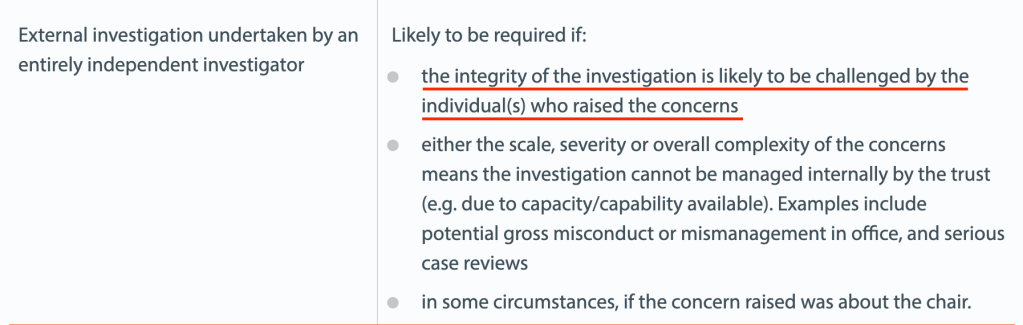
The trust maintained in its letter of 6 June 2022 that it adhered to NHS Providers’ guidance on FPPR. This is debatable given that NHS Providers’ criteria for triggering a fully external FPPR review is contentiousness. In the context of the Reuser litigation, that would seem to be fulfilled. Also, if the whistleblower at the centre of the matter did not have confidence in the process and had already withdrawn, the process had de facto been disputed.
Shockingly, I have now seen correspondence which shows that the CQC was informed that Jon Glasby was inappropriately involved in the Rosser FPPR review, BEFORE CQC decided to accept the trust’s FPPR evidence as satisfactory.
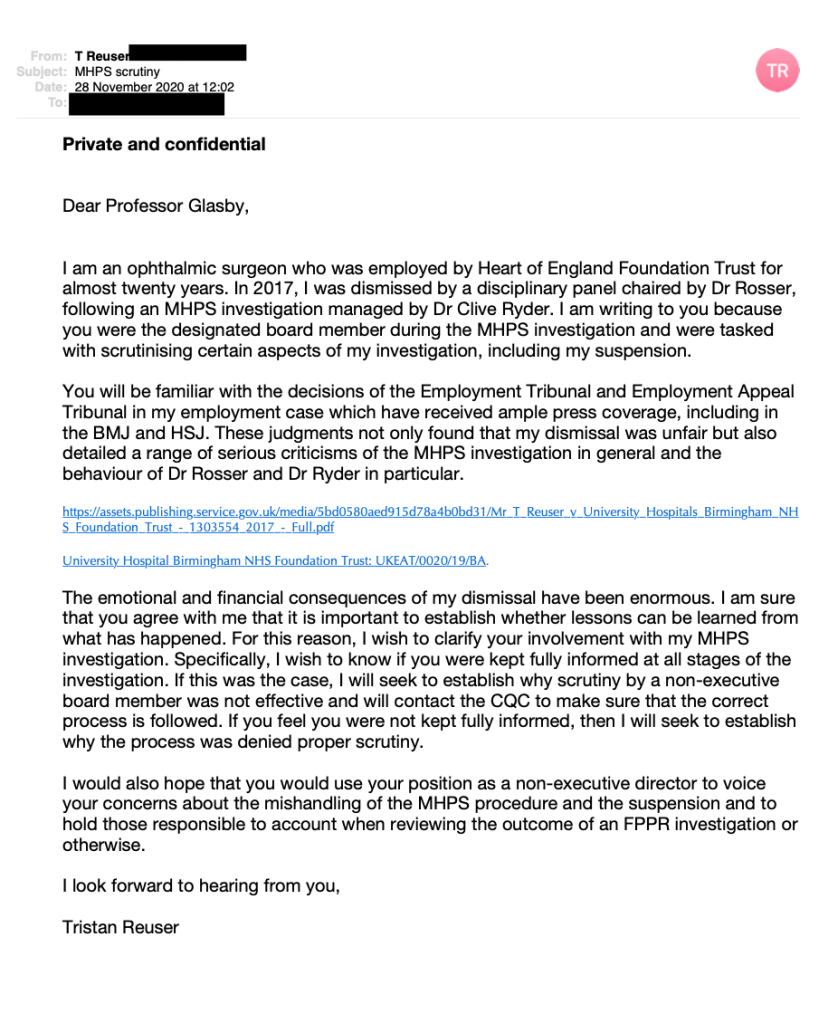
Separate to this, Mr Reuser wrote to Jon Glasby himself in November 2020, after the conclusion of his case in both the ET and the EAT. He asked if Jon Glasby had been kept properly informed of trust actions under MHPS, in the light of the ET and EAT’s serious criticisms of his suspension by the trust.
Glasby reportedly never responded to this letter. But by this point, the trust had drafted the terms of reference for the Rosser FPPR review. Did Glasby fail to respond to Tristan Reuser’s letter because he had already been appointed to the Rosser FPPR process and was conscious of the tension arising?
Trust learning from the Reuser case
UHB seem to have taken a cherry picker’s approach to the NHS Providers’ guidance on FPPR. This guidance emphasised the importance of retaining public confidence and it recommended publication of the outcome of FPPR investigations. It is unclear whether UHB has ever done so. I have asked Harry Reilly UHB chair to clarify if a summary outcome was ever published, and it not, whether the trust intends to publish a summary.
A previous enquiry that I made to the former trust chair Jacqui Smith about trust learning was repeatedly ignored. The trust eventually cursorily admitted in a seven month overdue FOI disclosure of 30 March 2022 that some level of wrongdoing was acknowledged, as board training was undertaken:
“The Trust has reflected upon the errors made in relation to the disciplinary process concerning Mr Reuser and the subsequent Employment Tribunal and has undertaken related training with all Board members, including the Trust’s current Responsible Officer (RO). This includes consideration of all relevant factors and advice when making a referral to the GMC.”
The reluctance to admit even this is not reassuring evidence of genuine learning or a change in attitude by the trust board. And there is no note of empathy.
I will be re-referring the UHB trust board and its former chair Jacqui Smith, now chair of Barts Health NHS Trust and Barking, Havering and Redbridge University Hospitals NHS Trust to the CQC under FPPR. This will include grounds of what I believe is the serious abuse of process in instructing a subordinate to determine the fitness of a senior. Although CQC is hardly fit to adjudicate given its part in rubber stamping UHB’s impropriety in its FPPR process.
Overall, the whole matter may look to some like CQC collusion with the trust.
How many other FPPR referrals have been processed in this shady way by the CQC, behind closed doors?
Ultimately, the ongoing evidence of CQC failure on FPPR will be submitted to the relevant parliamentary committees.
The regulation of NHS managers
If we revisit the original reasons for FPPR – the horrors of MidStaffs – and we contrast this against CQC’s obvious inaction, the question arises of what patient harm has CQC enabled in the last eight years of FPPR non-enforcement, in concert with cover ups and poor quality management of the NHS?
It has been a decade since the MidStaffs public inquiry, and the senior ranks of the NHS have continued to fiercely resist accountability, let alone regulation. The senior NHS ranks have been increasingly stuffed with government cronies, many of whom are financiers with little obvious connection to healthcare.
Instead of accountability, we see endless, incestuous recycling of the same individuals, revolving between provider and regulatory bodies, and sometimes the Department of Health. Shaking hands with a knowing wink as they keep swapping seats.
An example of CQC’s troubling proximity to the providers that it is supposed to regulate, and the fast-spinning CQC revolving door
Ellen Armistead was CQC Deputy Chief Inspector of Hospitals
CQC disclosed that she chaired the CQC’s FPPR panel between February 2016 and June 2019
Ellen Armistead’s bio from the Calderdale and Huddersfield NHS Foundation Trust website
The Kark review report on managing NHS managers’ fitness was carried out four years ago but remains unimplemented. Kark stopped short of full regulation but did recommend a central database and a barring mechanism, with full future regulation if these initial partial measures were not enough.
When I enquired again for the umpteenth time recently, I was told that there were still no implementation terms of reference to share with me because the work on the Kark report was still at an early stage – after four years!
A telephone meeting was held with NHS England/Improvement on 18 May 2022 and brief meeting minutes have now been agreed. It was revealed that there had not been Ministerial authorisation to go ahead with Kark implementation, but that was anticipated. A question about whether the Kark register will be retroactive has not so far been answered. If not, some will doubtless be pleased to delay the register’s establishment for as long as possible. It is anticipated that it will be at least a year before any Kark database is operational.
If patients are to be effectively protected, and frontline clinicians given the proper professional independence to care for them, the senior NHS management cabal must be tackled.
So of course must be the malign political influence of the Department of Health which sits at the apex of the pyramid of bullying and suppression.
Another example of the CQC revolving door
Mike Richards was a former CQC Chief Inspector of Hospitals who chaired CQC’s FPPR panel between December 2014 to February 2016.
Since the above was published, UHB’s performance continued to give cause for concern.
UHB’s CEO and Chair resigned.
BBC Newsnight has commenced an investigation into the trust.
Dozens of UHB staff have also contacted Preet Gill MP Birmingham, Edgbaston with concerns about poor culture.
I have made transcripts of two Newsnight interviews with proponents of the awful Freedom To Speak Up project, and of a revealing BBC interview with the UHB Freedom To Speak Up Guardian:
I have also written to the new interim Trust Chair to challenge leaked internal trust communications which implicitly denigrated current and former staff who have spoken to the BBC:
Please click and add your signature to this petition to reform UK whistleblowing law – whistleblowers protect us all but weak UK law leaves them wholly exposed and it is a threat to public safety
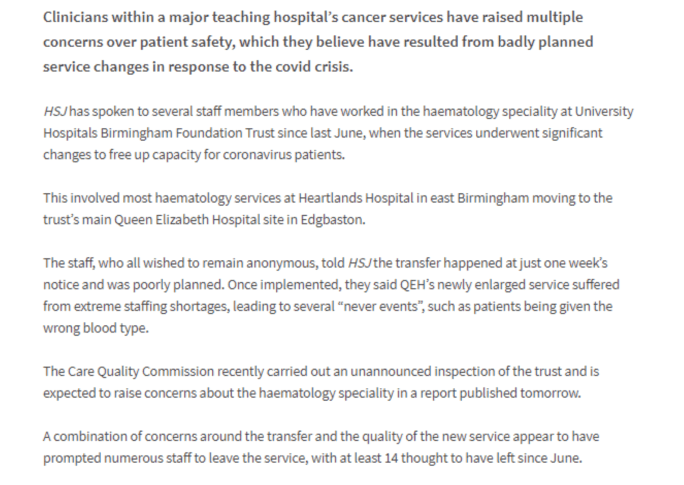
University Hospitals Birmingham NHS Foundation Trust also made the headlines on 5 June 2022 because of reportedly poor treatment of doctors in training in obstetrics and gynaecology, requiring regulatory intervention:
Based on Tristan Reuser’s case and others, NHS Resolution agreed that NCAS’ successor body will consider safeguards against being fed false information by unscrupulous employers:
“We know that most people get good care in the NHS, but sometimes they don’t get the outcomes they need or things go wrong. In these circumstances, it is vital that as a system we reflect and learn from these events to improve the safety of care”
“Rosie takes up her post with HSIB on 1 August 2022.”
Let us hope that Benneyworth does not take to tearing up any rule books at HSIB.
A particularly gross example of CQC conflict of interest and failure on FPPR was when it passed its notorious former Chair Jo Williams as a Fit and Proper Person, removing obstacles to her recycling back into the NHS fold:
Jane Archibald’s shocking whistleblowing case about a cover up of an unqualified assistant being allowed to run epilepsy clinics and vary complex epilepsy medication featured a failure by her former CEO Stephen Eames to respond to her disclosures. He simply did not respond to her correspondence. NHSE/I has been asked to review his suitability for his current post as CEO of the Humber region ICS.
Dr Jasna Macanovic’s recent NHS whistleblowing case adds to the pile of managerial recycling scandals. John Knighton the medical director found by the ET to be centrally involved in her premeditated unfair dismissal has been protected by the trust and Mark Cubbon the trust CEO who failed to ensure her protection as a whistleblower has been promoted to a senior post at NHS England.
An FPPR referral has now been made arising from the executive failures in this matter.
Information was requested from HSIB about “letters of concern” sent by HSIB to NHS trusts with particularly serious maternity safety failings and related poor governance.
Information was also requested on any evidence of conflicts of interest in HSIB’s own maternity operations, particularly in the light of the King’s Funds findings of HSIB staff perception of “unfairness” and “favouritism”.
HSIB’s maternity investigation function and conflicts of interest
The maternity programme became operational in 2018.
The central HSIB team investigated cases of national relevance under ‘safe space’ provisions.
In contrast, there were fourteen regional maternity HSIB teams with links to each trust providing maternity services, which investigated individual cases but not under ‘safe space’ provisions.
Concerns had been raised that applying ‘safe space’ to the local HSIB maternity investigations would obstruct duty of candour.
A less discussed issue is that of conflicts of interest arising from the local connections of HSIB maternity investigators.
After the Midstaffs scandal, the Healthcare Commission – the regulator which exposed the scandal was scrapped and replaced with the much criticised Care Quality Commission.
One of the first acts of the CQC was to disband a central investigation team and replace it with dispersed local teams and “relationship owners” assigned to individual provider organisations.
“…regional officers are at risk of what she calls “regulatory capture”. They can become too close to the trust managers they are supposed to monitor – and too keen to see them succeed”
It seems to me that the dispersed model of the HSIB maternity programme risks exactly the same type of capture.
It also embeds conflicts of interest due to recruitment of maternity staff from the regions.
The latter were attributed to the rapid expansion of the maternity programme, and could perhaps also be considered an artefact of the regionalisation of the service.
NEW INFORMATION FROM HSIB
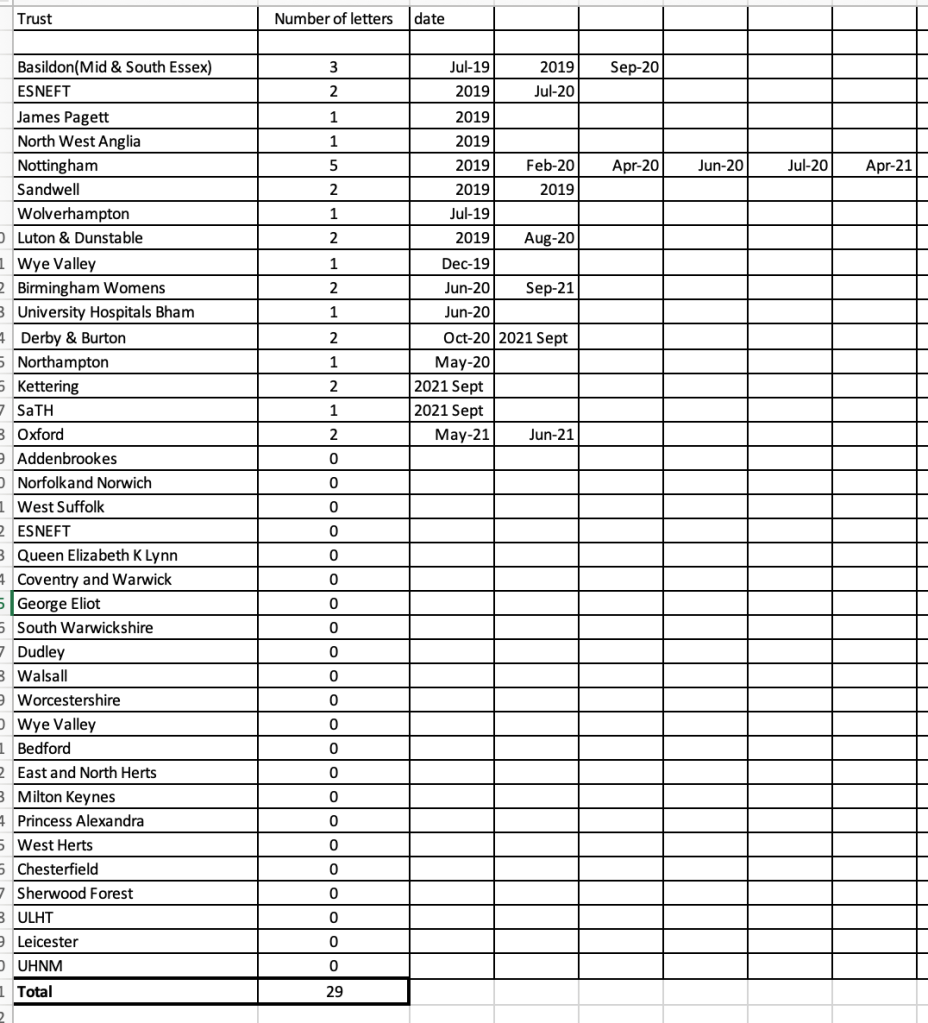
The latest data from HSIB has revealed that between 1st April 2018 and 31st March 2022, HSIB sent a total of 152 “letters of concern” to NHS trusts involved in the national maternity investigation programme.
These letters are sent when there is serious and urgent concern about patient safety:
“The urgent/emerging concerns panel will consider the significance and seriousness of the concerns raised and the urgency with which escalation should occur.
If outcome of urgent/emerging concerns panel is to proceed with escalation, then a letter detailing concerns is sent via email to the head of midwifery (HoM) or director of midwifery (DoM) and relevant clinical director (CD), and/or head of patient safety at the NHS trust.
The urgent/emerging concerns panel will decide if anyone else from the NHS trust should be copied into the escalation letter. Trust executives (medical director and chief nurse/DoM) copied into all escalation letters. Initial letters of escalation will be sent by RL [Regional Lead]/PNI [Principal National Investigator] unless panel consider otherwise.”
Depending on a trust’s response, HSIB has further stages of escalation, ending ultimately in onwards referral by HSIB’s Chief Investigator:
“HSIB chief investigator makes formal referral of concerns to CQC chief inspector of hospitals or referral to relevant professional regulator.”
The corollary of this seems to be that a dishonest but skilful trust could manipulate this escalation scheme by genuflecting and getting HSIB off its back with the right response, sincere or not.
Interestingly, HSIB has disclosed that it has no interagency protocols:
“We do not have any interagency protocols.”
This is HSIB’s escalation policy which determines the process for sending letters of concern to trusts:
Some trusts have received no HSIB letters of concern, and one trust received 15 letters of concern, which was the highest number.
There are concerns from some bereaved families that some trusts which have so far escaped significant criticism and scrutiny in fact also have elevated levels of maternity serious incidents. This raises a question of whether some trusts have had an easier ride than is warranted.
HSIB volunteered undated spreadsheet data which goes up to 2021, which at that point showed a total of 29 letters of concern, sent to sixteen trusts.
Nottingham had been sent the most letters (five) at that point:
An up-to-date version of this spreadsheet has been requested, with breakdown of the number of letters of concern by trust.
So it would seem that there has been a huge acceleration in the number of HSIB escalation letters sent over the last year or so, jumping from a total of 29 to 152.
As regards conflicts of interests in its regional maternity teams, HSIB maintains that it has these provisions in place to manage conflicts:
6. Please advise what due diligence NHSI undertook to ensure that appointments to regional HSIB maternity investigation teams were not compromised by conflicts of interest.
“NHS England and Improvement have not been involved, at any stage, in appointments or organising maternity teams. All maternity employees of HSIB are required to and have completed an annual declaration of interest form, highlighting trusts they have previously worked in or other known associated conflicts of interest. Maternity investigators do not carry out investigations in trusts they have previously worked in. Individuals are required to flag any conflicts of interest that may present during an investigation to enable them to be removed from the case, these may not relate to the trust.”
7. Please advise of HSIB’s approach to eliminating conflicts of interest in individual maternity investigations, by regional teams. Please disclose any relevant written guidance, policy or protocol.
“All maternity programme employees complete a declaration of interest form. Maternity investigators do not investigate in trusts they have previously worked in. Additionally, clinical advisors do not review or offer clinical advice in trusts they work in or have any associated conflicts of interest.”
But are these arrangements robust enough? It is not just individual HSIB investigators who matter, but their managers also impact on how investigations are handled and reported.
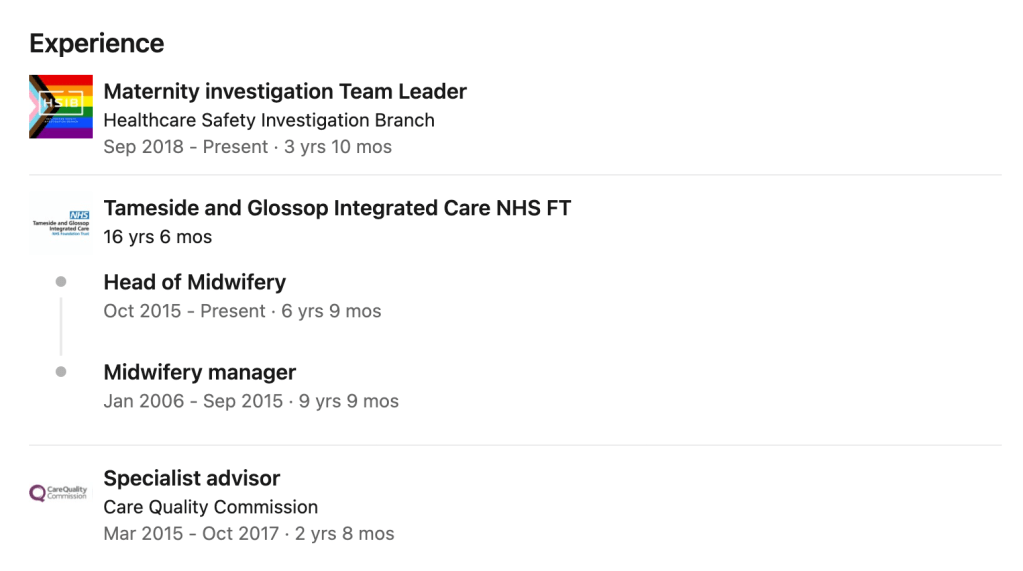
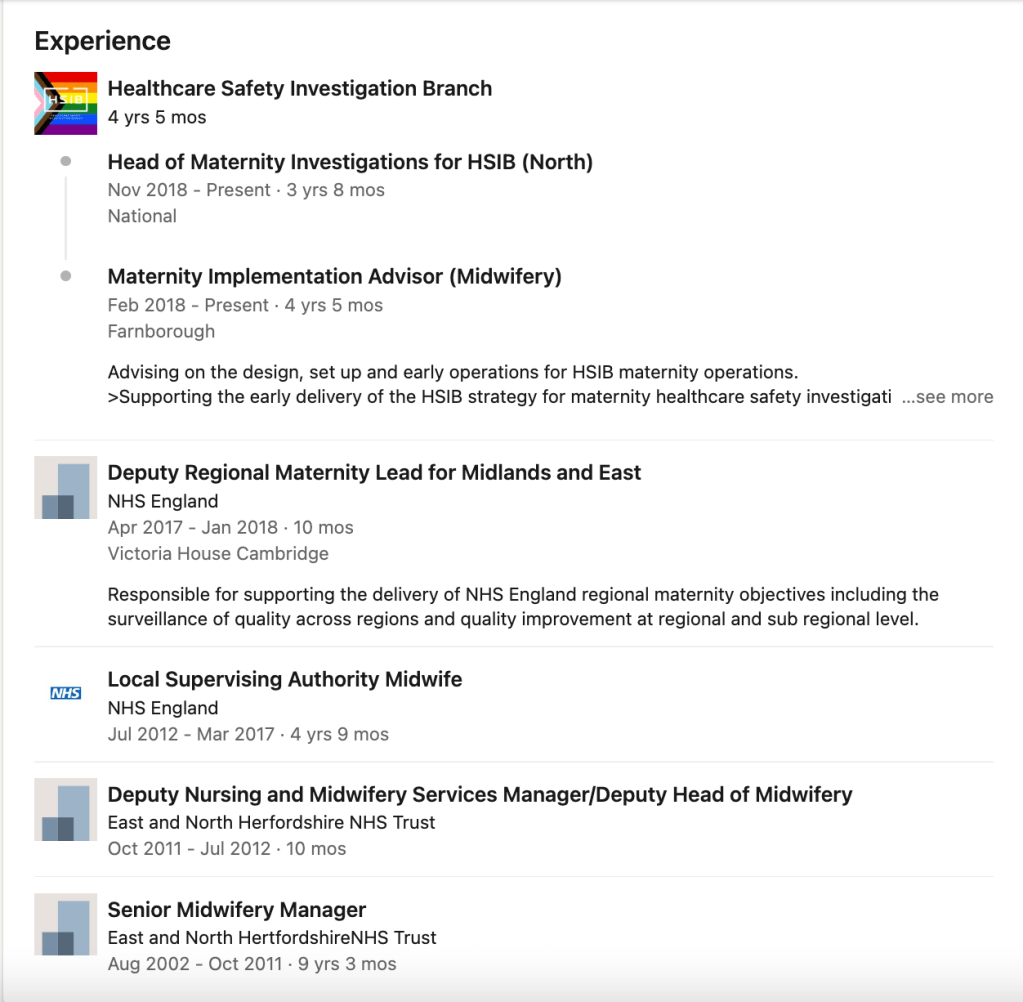
As an example, this is the CV of an HSIB Maternity investigation Team Leader according to her LinkedIn entry:
How do HSIB conflict of interest procedures apply to its regional maternity managers, especially those who have had past oversight of trusts in the same area/region?
Obviously, such individuals may potentially be conflicted in revealing evidence of past governance failure in their area/region.
When asked if there have been complaints or concerns about conflicts of interest, HSIB replied that there had been no complaints. It is less clear if there have been concerns eg. whistleblowing:
8. How many complaints and concerns has HSIB received about actual, potential or perceived conflicts of interest in maternity investigations by regional teams?”
“HSIB have received no complaints, that relate to actual, potential or perceived conflicts of interest relating to any part of the HSIB organisation.”
PETITION
Please click and add your signature to this petition to reform UK whistleblowing law – whistleblowers protect us all but weak UK law ignores their concerns, leaves them wholly exposed, lets abusers off the hook and it is a threat to public safety.
This is a special edition of our Parish newsletter.
Parishioners raised concerns that some Parish council officers might not have been behaving as they should.
It was rumoured that even when caught out, some of these officers were moved behind the scenes to new jobs, at a little office at the District Council known as the the “Donkey Sanctuary”.
The County Council eventually asked a nice gentleman to write a report in 2018, who suggested a “naughty list” be kept so that no one forgot any misbehaviours:
Unfortunately, it seems the District Council misfiled the report under “hedgerow maintenance schedules” and no action was taken.
Parishioners recently enquired about progress, and a meeting was held from the phone box by the FPPR Arms.
The WI would like to point out that they take great pride in keeping the phone box spick and span, and could the person who leaves crisp packets please be more considerate.
The District Council said that they had not actually received authorisation yet from the County Council to implement the report recommendations, but it is anticipated that the County Council may give the green light soon. The District Council were ready to make a plan. They did not know if old concerns could be added to the “naughty list”. They did not think they could show the draft template of the “naughty list” to all parishioners.
Mr A. Noyd, retired town clerk, from 12 Skittle Lane said it wasn’t run like that in his day. Not at all.
When Mrs Brown from the chip shop asked them how it was that crimes had taken place, but everyone was innocent, the constables were a little bit stumped.
In other news, a parishioner Ms Jane Archibald was promised some follow up action by her former MP at the end of her dreadful legal case. Ms Archibald wrote to remind the MP of their earlier discussions and an offer that he had made to speak to the Health Secretary.
However, her former MP did not seem interested to follow up an irregularity at his local hospital, and his team told her that this was because she had moved out of area.
“From: Dr Neil Hudson MP [REDACTED] Sent: Monday, May 23, 2022 3:49:54 PM To: Jane Archibald [REDACTED] Subject: Re: employment tribunal outcome – Archibald Case Ref: NH52) (Case Ref: NH54)
Dear Miss Archibald,
Thank you for your email. As MPs are only allowed by Parliamentary protocol to assist their own constituents, I suggest you contact the MP for your local area.
speaking to the Westmorland and Cumberland Herald last month, Mr Hudson said of his visit to the sanctuary: “Seeing her work in person really warmed my heart. While she told me some truly harrowing details of the neglect many of her donkeys faced prior to their rescue, it was heartening to know that now with Linda, these gentle animals are receiving such love and good care.”
Let us hope Mr Hudson will make some room in his warm heart for vulnerable patients at his local trust.
The Enquirer tried to reach the top man at the County Council for comment on the “naughty list”, but his staff said he unfortunately had to attend an urgent hospital appointment. We can see why judging from this photo. Get well soon Mr J!
By Dr Minh Alexander retired consultant psychiatrist 31 May 2022
Under FOIA, NHS England/Improvement reluctantly disclosed in April 2022 a suppressed and lack lustre King’s Fund report into poor culture and leadership at the Healthcare Safety Investigation Branch:
There was a reference in the King’s Fund report to HSIB staff dissatisfaction with previous reviews into cultural issues:
“…At the beginning of the work, staff had been clear that they would not trust the report outcomes if they were first shared with the executive team, owing to a perception that the findings of previous reviews had been changed before publication, or not shared at all.”
At the conclusion of the King’s Fund review, the level of staff distrust was such that it was recommended there should be external oversight of follow up actions and clear timescales for action:
“Given the level of mistrust expressed by staff that senior leaders had failed to act on previous review recommendations, it is important that the HSIB executive team, supported by NHS England and NHS Improvement and with oversight from the Department of Health and Social Care, commit to responding to this report with HSIB staff and confirm the timescale for implementation of these recommendations.”
Following the trail, I asked NHSE/I to disclose copies of the earlier reviews cited by the King’s Fund.
Today NHSE/I disclosed only a single internal review by HSIB senior staff, the Benson review, carried out in 2020, as follows:
“An internal review of our maternity team was undertaken in 2020. This was led by Dr Nick Woodier, Dr Dawn Benson and David Landreth at HSIB. From this review, a slide deck report was produced and delivered in June 2020.”
David Landreth is according to his Linkedin entry HSIB Associate Director of Information Management & Technology
“The review…was commissioned by and for the review of the Exec. Team at HSIB. They wanted to understand stakeholder’s opinion of the maternity services. There were responses back from 54 trusts and a total of 247 staff, mainly midwifery but also other clinical and medical leads including ambulance staff. The idea was to use that feedback, in confidence, to understand what themes HSIB should address to improve our practices within the maternity team when undertaking an investigation.”
The context of this is that the maternity investigation section of HSIB was established as an addition in 2018 and is based in the regions.
NHSE/I redacted information from the Benson review report claiming Section 41 FOIA exemption:
“The info was shared in confidence to HSIB by its staff to improve how its maternity functions operates. The information that has been shared is not trivial and has not been published elsewhere. Given the circumstances in which this information was provided, we consider it was imparted in circumstances giving rise to an obligation of confidence.
Furthermore, we consider that disclosing this information would cause detriment to the confiders and there is an expectation that this type of information should not be disclosed under the FOI Act.”
The reflex secrecy by NHSE/I was such that even though the regulator had disclosed the report authors’ names to me, it still redacted their names from the body of the report:
Child psychologists probably call that self-soothing behaviour.
The version of the Benson report disclosed by NHSE/I is similar to the previously disclosed King’s Fund report. It is very light on facts and full of opinions and summary conclusions that are not grounded in data.
It may be that a separate and very different version was produced for senior management consumption, but withheld from the troops.
Nevertheless, there are indications of serious cause for concern.
For a national body which sits in judgment of others, the Benson review made alarming findings of lack of basic structure and standards or common understanding of operating procedure in the maternity section of HSIB.
For example:
“10.3. Define the methodological approach taken to investigate events
Reports demonstrate a fundamental confusion between a method and methodology.
Reports do not clearly define the methodological approach to the investigation, which is strongly rooted in clinically reviewing the event. Rather they list the methods used to collect evidence.
Reports suggest a human factors approach is taken, but that in itself is not a methodology.
There is an opportunity to define the methodology and distinguish between methods and methodological approaches”
“IO 11. Focus on quality
Quality was explored recurrently through the evaluation with questions around quality of reports, analysis and recommendations.
There is a need to balance quality with efficiency, with early learning shared with trusts to help bring about changes.
There is no defined standard of ‘[Redacted]’ resulting in poorly written reports and recommendations that might not offer more than a standard, local, serious incident investigation. ‘[Redacted]’
Quality should include listening and responding appropriately to Trust challenges to findings and factual accuracy.
There is an opportunity for the maternity programme to define standards for quality throughout their investigations, including report writing, report content and recommendation writing.”
“10.2. Design and implement an investigation framework
There is little evidence in either the investigation process or reports, of the appreciation of systems factors which may have contributed to events.
The programme does not have the methodological framework to enable delivery against the directions to ‘identify all contributory factors that led to the outcome’. The investigation process lacks a basic methodological structure which means there is no analytical framework to guide investigations.
Findings are reached by clinicians who, where possible, evaluate what was done against what national and local guidance suggests should have been done. Where there is no such guidance, they review evidence, and influence and shape the recommendations, through their own clinical, and in some cases medico-legal experience. This often leads to reports which suggest responsibility for outcomes lie with the clinical practice of individuals and teams and fail to consider the systems of work which contribute to the outcome.
There is an opportunity to develop and introduce a framework for investigation planning, evidence collection and analysis, which supports investigators to identify all the contributory factors that led to outcomes.”
The Benson review acknowledged that many of the shortcomings arose from the fact that HSIB was forced to expand rapidly when it had to take on national maternity investigations, far outstripping its original capacity.
The review of course did not say so, but the origin of that malaise was political, with Jeremy Hunt’s maternity safety crusader agenda driving the expansion.
“When it comes to maternity safety, we are going to try a completely different approach. From next year, every case of a stillbirth, neonatal death, suspected brain injury or maternal death that is notified to the Royal College of Obstetricians and Gynaecologists’ “Each Baby Counts” programme—that is about 1,000 incidents annually—will be investigated not by the trust at which the incident happened, but independently, with a thorough, learning-focused investigation conducted by the healthcare safety investigation branch. That new body started up this year, drawing on the approach taken to investigations in the airline industry, and it has successfully reduced fatalities with thorough, independent investigations, the lessons of which are rapidly disseminated around the whole system.
The new independent maternity safety investigations will involve families from the outset, and they will have an explicit remit not just to get to the bottom of what happened in an individual instance, but to spread knowledge around the system so that mistakes are not repeated. The first investigations will happen in April next year and they will be rolled out nationally throughout the year, meaning that we will have complied with recommendation 23 of the Kirkup report into Morecambe Bay.”
The Benson review gathered the following concerns about the quality of maternity reports as follows:
Feelings that quality is driven by ensuring that the investigations have input and direction from clinical professionals.
A limited quality assurance review process against standards for reports before they are released. There is evidence of poor formatting, grammar and spelling in reports.
Evidence that the process does not fully take account of factual accuracy challenges with inclusion of changes or clarification to those challenging the report as to why changes have not been made.
Recommendations are generally lower in the hierarchy of effectiveness of recommendations and do not commonly focus on system improvements, rather guidance and policy. Trusts reported concerns that some recommendations were not linked to evidence or causality.
A repeated concern was the delay to receipt of actions from reports. This meant that trusts were not able to put in place early learning to help prevent similar invents and instead had to wait till the final report which may be a year later.
The review team also heard of individual cases that undermined the intention for HSIB to provide no-blame investigations via the way local staff have been interviewed.”
The Benson review listed areas for improvement as follows:
“Improvement Opportunities
IO 1. Define roles so that individuals are responsible for functions within their expertise. IO 2. Design and implement an investigation framework. IO 3. Define the methodological approach taken, and methods to be used to investigate events. IO 4. Empower maternity investigators to lead their investigations. IO 5. Review the expertise of the investigation team and consider introducing investigation scientists. IO 6. Review the process of obtaining clinical opinion in the programme. IO 7. Reassure the workforce. IO 8. Explore leadership development and coaching to foster a culture of support and where staff feel safe to challenge. IO 9. Evaluate and reflect upon the training programme. IO 10. Explore ways the senior team can develop their own understanding of safety/ investigation/ human factors science. IO 11. Focus on quality. IO 12. Taking the opportunity to learn.”
Alongside the operational disruption, the Benson report also noted cultural problems.
NHSE/I has drawn a ludicrous veil over these, as if people cannot deduce what happened from everything else that has come into the public domain since.
Here is a particularly absurd passage, which nevertheless flags bullying and intimidation:
“Culture
The structure, purpose and challenges of the maternity programme have driven a cultural identity which fosters pride in the combined aim to improve maternity services in England. The 14 regional teams provide individual investigators with a secure base from which they derive operational and emotional support and resilience.
Investigators reported:
• The programme structure and a ‘[Redacted]’ attitude cultivates a sense of oppression and control. • Significant numbers (>20) of investigators openly reported either feeling bullied themselves or having knowledge of other people who had been bullied by staff more senior to themselves. • Others (>30) recognised pressure which at times resembled bullying. • They largely attributed this to the pressure being placed upon their direct line managers to, ‘[Redacted]’ of reports. • Many investigators (>30) talked about feeling they could not challenge what was described as ‘Redacted’, which encouraged ‘Redacted’ attitudes towards investigations contrasting with the just culture they had been trained (at Cranfield) to adopt. • Job satisfaction is significantly affected by this and recent messages from the senior team that unless the backlog is cleared by November 2020 ‘[Redacted]’. • HSIB staff from across the whole organisations raised concerns that the ‘’[Redacted]’.
Matters were clearly serious as the review report noted:
“10.7. Reassure the workforce
Investigators feel insecure in their jobs and a significant number report they are considering or actively looking to leave HSIB because they feel their job is not secure.
This is something which has intensified over the period of the evaluation largely because of the pressure to reduce the backlog of reports.
[Redacted]
There is an opportunity to improve the wellbeing of the workforce and retention by offering reassurance about the methods being taken to reduce the backlog of reports.”
It appears that there were difficulties with whistleblowing, but as NHS Improvement have placed a strategic fig leaf over the relevant passage, it is difficult to be sure:
“8. Explore leadership development and coaching to foster a culture of support where staff feel safe to challenge.
• [Redacted]
• [Redacted]
There is an opportunity for improving the culture within the programme and the retention of the workforce. Exploring leadership coaching.”
Freedom To Speak Up at NHS England/ Improvement and whistleblowing by HSIB staff to Speak Up Guardians
NHSE/I have an extraordinary internal whistleblowing policy, where “triage” of whistleblowing matters, that are not immediately resolved by Freedom To Speak Up Guardians, is handled by a steering committee which includes the NHSE/I General Counsel.
Is it me or does that scream “containment”?
NHSE/I has disclosed that there are “55 NHSE / I Freedom to Speak Up Guardians across almost all regions and directorates. These Guardians are made up of staff from various roles and various levels of seniority.”
NHSE/I has also indicated that since HSIB became operational, 15 cases have been opened with Freedom To Speak Up Guardians on HSIB staff.
It would appear that the HSIB executive team were given ample warning in 2020, through the findings of the Benson report, of serious cultural problems in at least some parts of the organisation.
But for whatever reason, HSIB’s leaders failed to effectively address these problems, necessitating the further King’s Fund review in 2021, by which time staff trust had been further eroded.
A sad and telling entry in the review action log of December 2020 is the section that declares action on culture change “complete”:
There are serious questions arising about the consistency and quality of HSIB’s maternity investigations. Have some HSIB maternity investigations failed to identify all contributory factors? It sounds from the disclosed Benson report, for all its avoidance of hard data and detailed facts, that some investigation reports were defective and did not reveal the whole truth.
It is a pity that there is not a legal Duty of Candour for regulators, or that NHSE/I is compelled to own up to any families affected by any of these failures of HSIB maternity investigations. It is too awful to contemplate the abuse of trust. That harmed families put their trust in an independent investigation process which in some cases was not actually sound, and they may not have been told yet that this was so. And all the while, a former Secretary of State posed as a maternity safety champion, whilst strong arming a small safety agency to expand unsafely, for political gain and soundbites. And all the while he failed to implement the MidStaffs core recommendation on ensuring safe staffing for the NHS.
And we have yet to see if there are any other HSIB reviews that NHS Improvement has failed to disclose.
PETITION
Please click and add your signature to this petition to reform UK whistleblowing law – whistleblowers protect us all but weak UK law leaves them wholly exposed, lets abusers off the hook and it is a threat to public safety.
Jeremy Hunt’s patient safety reform/ maternity safety crusader narrative included selling a myth that Morecambe Bay trust had been turned around. It in fact continued to suppress several whistleblowers.
Jackie Daniel former CEO of University Hospitals of Morecambe Bay NHS Foundation Trust receiving a gong
By Dr Minh Alexander retired consultant psychiatrist 31 May 2022
There has been great concern that the controversial Whistleblowing All Party Parliamentary Group (a collection of parliamentarians with no formal status) has been trying to shape UK whistleblowing law in the interests of the US bounty hunting lawyers whose money helped to establish the APPG.
A now defunct Bill introduced by the APPG Chair Mary Robinson Tory MP for Cheadle could be understood as a bounty hunters’ Bill. It contained a number of disturbing features and omissions:
Alarmingly, John Penrose Tory MP for Weston and the Prime Minister’s Anti Corruption Champion expressed public support for the Whistleblowing APPG’s Bill in April. Penrose gave an interview to GB News just before Mary Robinson made a speech about the Bill on 26 April 2022. In this interview, Penrose alluded to insertion of whistleblowing clauses into the Economic Crime Bill as a back up option, if the APPG’s Bill did not pass.
Penrose batted off correspondence from me, on the pretext that I was not a local constituent, even though I had explicitly written to him in his capacity as the national Anti Corruption Champion.
I complained to the Home Office Permanent Secretary about this specious rebuff. Penrose wrote to me again, this time on Home Office stationery and signed in his proper capacity as Anti Corruption Champion. He justified his support for the Whistleblowing APPG Bill as democracy in action. A bit thin really, given that he had just undemocratically tried to ignore dissenting voices.
APPGs are notorious for exerting influence on behalf of private interests, particularly when well funded and amply resourced to drive an aggressive lobbying/ media campaign. The Whistleblowing APPG is notably glossy in its presentation, with very active media liaison and a steady stream of coverage.
Longstanding concerns about hidden interests and unethical conduct by APPGs
“37. Lobbying is an important part of a healthy democracy. It is crucial that the interests of different sectors, organisations, and communities can be brought to the attention of Members and Ministers. All-Party Parliamentary Groups provide a significant benefit to the House by providing a forum where matters of policy can be discussed and a vehicle for making representations to Ministers and the wider House.
38. It should not be the case, however, that those with greater financial means should enjoy a greater advantage in lobbying Members and Ministers, or that those without financial means should be excluded. All-Party Parliamentary Groups must not be a vehicle by which paid external interests can achieve a level of access and influence not available to others. There are few, if any, safeguards in place to ensure that APPGs are genuinely Member-led and are not simply used by external bodies as way to amplify their own message with the added advantage of an informal parliamentary imprimatur. The danger is that an APPG could all too easily become a parliamentary front for an external commercial entity. That would be wholly inappropriate. We therefore believe some limits must now be placed on secretariat services to APPGs.
39. We also advise that Members who set up, chair or play a role in an APPG should be extremely vigilant that the APPG’s agenda, funding and activities do not bring the House into disrepute; are genuinely led by Members rather than any external organisation or individual; and do not provide an inappropriate or unequal degree of influence to any one organisation, individual or set of organisations.”
I had also made a formal request for information about Penrose’s contact with the Whistleblowing APPG and requested disclosure of correspondence between him and the APPG.
This is the resultant FOI response from the Home Office on 30 May 2022:
The Home Office disclosed that there was a meeting between Penrose, the APPG and others on 1 December 2021:
The Home Office also disclosed a friendly email chain between Penrose and Mary Robinson the Whistleblowing APPG Chair, in which he agreed to support her ten minute rule Bill.
Most significantly of all, Penrose forwarded their correspondence to the Home Office on 21 April 2022 with these comments:
“Hi All FYI I have just agreed to be a co-signatory to this 10-minute rule Bill next week, as a way of getting it onto the Government agenda in advance of ECB2. No need for any of you to do anything in particular, but wanted you to know so you aren’t blindsided or surprised!
Best wishes
John Penrose”
So there we have it. The target was indeed the Economic Crime Bill, and the big bucks from bounties in the financial sector.
Bounty hunting is a billion dollar industry in the States, and US lawyers have been trying to break into the UK market for years now.
And all a million miles away from whistleblowers who report poor care and bring in no money at all. A million miles away from public sector Nolan principles of selflessness.
The US style Office of the Whistleblower, if created, will likely be stuffed with cronies, backscratching and promoting private industry interests. It won’t be about justice or real public protection, but milking as much profit as possible.
Nolan Principles of selflessness in public life make rewards for whistleblowing anathema in the public sector. In the NHS, workers are contractually obliged to whistleblow through the duties conferred by the NHS constitution, and registered professionals are additionally required by their professional codes of conduct to whistleblow. Any suggestion of rewards for whistleblowing in the NHS are particularly and deeply problematic.
The Whistleblowing APPG’s secretariat, the private organisation WhistleblowersUK and an associate, making clear public statements in support of whistleblower rewardsA post from the WhistleblowersUK website, now deleted, promoting the use of whistleblower rewards
The trust suspended her on trumped up charges. The Employment Tribunal determined that there were no factual grounds for disciplinary action or dismissal, and that those who dismissed Linda Fairhall did not genuinely believe they had a case against her.
“23. In terms of the unfair dismissal claim, the tribunal was not satisfied that the respondent had established that its reason or its principal reason for dismissing the claimant was a reason related to her conduct. Those responsible for the claimant’s dismissal and the dismissal of her appeal did not “genuinely believe” that the claimant had committed any acts of misconduct which are now alleged. There could be no such genuine belief because there were no reasonable grounds for that belief. There could be no reasonable grounds because there had not been a reasonable investigation. The respondent’s decision to dismiss the claimant fell outside the range of reasonable responses open to an employer in all the circumstances of this case. This was an employee of thirty-eight years unblemished service who was suspended from her role in circumstances where that suspension was unjustified and unreasonable. The investigation which followed that suspension was inadequate and unreasonable. The investigation did not produce any qualitative evidence which could have led a reasonable employer to decide to dismiss the claimant in those circumstances, for reasons related to her conduct. The procedure followed by the respondent was unreasonable and unfair. For those reasons the claimant’s complaint of unfair dismissal is well-founded and succeeds.”
Linda Fairhall’s partner died of a heart attack whilst she was unjustly suspended.
She herself was unwell and also a cancer survivor.
She won her Employment Tribunal in January 2020, but appallingly, the trust decided to make her suffer even more by appealing against the finding that her unfair dismissal related to whistleblowing.
What sort of an organisation does that to a bereaved woman, whose partner died whilst it unjustly suspended her? Words are not enough for this additional injury by North Tees.
The Employment Appeal Tribunal noted caustically in its judgment that it was not surprised that the trust had not appealed against a finding of unfair and wrongful dismissal, so “excruciating” were the ET’s detailed findings and laying out of the evidence against the trust.
“In its detailed findings of fact, the Tribunal described in excruciating detail the manifest failings and fundamental unfairness of the respondent in dealing with the claimant’s suspension, the investigation into her conduct, her grievance, her eventual dismissal and the rejection of her appeal.”
Moreover the EAT considered that the ET’s substantive finding of whistleblowing detriment was correct in law. It merely found that the ET could have given fuller reasons for some of its findings of whistleblowing detriment but advised the trust to consider whether it was proportionate to pursue this.
North Tees also persecuted whistleblower Dr Manuf Kassem, who remarkably won an Employment Tribunal in January 2021 for whistleblowing detriment after representing himself.
Mr Kassem raised patient safety concerns and suffered retaliatory disciplinary action. The Employment Tribunal severely criticised the medical director’s detrimental actions against Mr Kassem, which it linked to Mr Kassem’s whistleblowing. Other senior medical staff were also criticised. The ET also determined there was an element of Race discrimination in the trust’s mistreatment of Mr Kassem, and that the trust’s actions amounted to harassment.
As an example of the trust’s egregious mistreatment of Mr Kassem, it launched a fraud investigation into him, but eventually withdrew the allegations. A witness gave this evidence in support of Mr Kassem:
“Mr Tabaqchali concluded his evidence in this respect that he was aware that the claimant “did numerous additional sessions without claiming payments. I therefore think it is a great pity that the directorate has taken this approach rather than thanking him for his hard work and dedication. I would suggest that the directorate overall owe him more pay, not less pay.”
I referred Lynne Taylor, North Tees Director of Planning and Performance, named in the Linda Fairhall ET judgment to the Care Quality Commission under CQC Regulation 5 Fit and Proper Persons, on grounds of whistleblower reprisal.
As usual, CQC shut down the FPPR referral and gave the trust a pass. This was in November 2021, well after the ET judgment was issued in Mr Kassem’s case. At that point, the CQC should have been aware that North Tees was a recidivist whistleblower victimising organisation.
Lynne Taylor retired from the trust with accolades and flowers, a month before I received the CQC FPPR decision, in contrast to the abusive exit meted out to Linda Fairhall:
FOI requests to the trust revealed that the ‘independent’ FPPR process which satisfied the CQC consisted of a panel of three trust directors and two other trust managers reviewing the case.
A pall is cast over this by the trust’s admission under FOI that it was a collective trust board decision to appeal against the ET judgment in Linda Fairhall’s favour.
In other words, a bunch of executives who reportedly did not have the collective common decency to leave a grieving woman alone, and who made her suffer yet another traumatic legal process whilst unwell, were allowed to judge the fitness of a colleague found to have victimised her.
What a perfect picture of rigour and objectivity.
These are the two relevant FOI disclosures from North Tees:
I would have made an FPPR referral last year on North Tees with respect to Mr Kassem’s case but I took a break from campaigning work due to personal commitments.
I have now made a second FPPR referral to CQC on North Tees. I have pointed out to the CQC that North Tees is a recidivist employer, and that the original FPPR process in Linda Fairhall’s case was compromised because it was undertaken by trust directors who were reportedly party to the very poor decision to appeal the ET judgment.
I also recently asked CQC for update FOI information on its regulation of the Fit and Proper Persons provisions.
In response, CQC admitted on 25 May 2022 that since Regulation 5 Fit and Proper Persons came into force in 2014, it has received 147 referrals related to NHS trusts and which included 212 referrals on NHS trust directors.
95 of the 147 referrals on NHS trusts (featuring 108 NHS trust directors) were accepted for consideration by CQC’s FPPR panel, which CQC now admits has never made a single finding of NHS trust non-compliance in the eight years that Regulation 5 has been in force.
CQC has squirmed and tried to soften this stark fact by implying that it would have made findings of non-compliance if some of the individuals had not resigned or been sacked before the completion of its FPPR process.
And as CQC has been so fond of fobbing off whistleblowers with the mantra that it only regulates the soundness of trusts’ FPPR processes and not the fitness of individuals, it is very unconvincing of CQC to claim that its regulation of FPPR ends when suspect directors depart.
These are the relevant passages from CQC’s FOI response of 25 May 2022:
“Since Regulation 5 of the Health and Social Care Act 2008 (Regulated Activities) Regulations 2014 came into force, a total of 147 of the referrals made to the panel have related to NHS trusts. Some trusts have been referred more than once.
In total, these included 212 referrals of NHS trust directors. In some cases, this includes more than one referral of the same person.
Of the 147 total referrals relating to NHS Trusts, 95 were considered by the panel and these related to 108 directors (including some cases where the same director was referred more than once).
There are a number of reasons why a referral may not have been considered by the panel, for example where the person referred was no longer working in a role within the scope of the regulation or the information shared was not a matter that fell within the scope of regulation 5.”
“It is for the provider to discharge its legal duties under the regulation. FPPR referrals can conclude in a number of ways. For example, an FPPR referral may end where the director resigns from their post before the process has concluded or the director is dismissed through the disciplinary process. For this reason, no FPPR referrals relating to NHS trusts have reached an outcome that the provider is non-compliant with the regulation at the conclusion of the panel process.”
CQC has had the muscle all along to remove unfit directors if it wishes to do so. It told whistleblowers this at a meeting in 2014. This was confirmed by recently disclosed internal CQC audit material:
There is more to come about yet another CQC FPPR failure.
PETITION
Accountability is a key plank to preventing future cover ups and whistleblower reprisal.
Please click and add your signature to this petition to reform UK whistleblowing law – whistleblowers protect us all but weak UK law leaves them wholly exposed, lets abusers off the hook and it is a threat to public safety.
Partly because of CQC’s dismal handling of the Fit and Proper Person regulation, and following Jeremy Hunt’s own version of Mid Staffs disaster at Liverpool Community Health NHS Trust, the Department of Health in 2018 commissioned a report into the Fit and Proper Test in the NHS. This was done by barristers Tom Kark and Jane Russell. NHS Improvement was tasked with implementation but has done little since then. A recent meeting took place which revealed that ultimate approval was still awaited from the DHSC.
Dr Jasna Macanovic’s recent NHS whistleblowing case adds to the pile of managerial recycling scandals. John Knighton the medical director found by the ET to be centrally involved in her premeditated unfair dismissal has been protected by the trust and Mark Cubbon the trust CEO who failed to ensure her protection as a whistleblower has been promoted to a senior post at NHS England.
An FPPR referral has now been made regarding the executive failures in her case.
CQC also uses “specialist advisors” in its inspections who are current NHS staff, including managers who review the Well Led domain of inspections.
There has been an extraordinary local media report – by Leicestershire Live on 21 May 2022. This was about a former CQC specialist advisor, Shaun Chadwick. Colleagues and ex colleagues have accused Chadwick of abusive comments and social media posts.
Despite Leicestershire Live obtaining apparent evidence of the social media posts, which it has shared, Chadwick has reportedly denied the allegations:
“A manager working for the NHS has been accused of telling a former colleague Karma is a b****’ after she was diagnosed with multiple sclerosis – before calling her a “pathetic woman” and a “fat cow”.
Shaun Chadwick, senior executive partner at Spectrum Health in Oadby, has also been accused of regularly ‘fat shaming’ another former colleague. It has also been alleged he shared confidential questions with practice staff that CQC inspectors planned to ask during a visit – and telling them to be ready with the right answers.
Mr Chadwick has robustly denied the allegations in a statement issued by his current employers Spectrum Health. It says: “We can all confirm that such allegations are grossly inaccurate and insulting.”
Readers can take a look at the Leicestershire Live original article and related images of the social media posts to make up their own minds:
A comment on this article alleged that concerns had been raised with the CCG and NHS England, who failed to act:
“The repeat theme on these posts is that the Leicester/Leicestershire CCG, LMC and NHSE are continually failing in their duty to act despite suggestions of patients and staff raising concerns and it being their position to bring all those responsible to account.”
Chadwick is a GP practice manager.
According to Leicestershire Live, he is also accused of abusing his position as a CQC specialist advisor by sharing questions that CQC inspectors were due to ask with one of his own practices, whilst he was employed as a CQC specialist advisor:
“Mr Chadwick has also been accused of sharing questions that Care Quality Commission inspectors were due to ask staff at one of his practices during a forthcoming inspection, which is a breach of the CQC rules on confidentiality.
He was a specialist advisor for the CQC at the time, while he was also executive manager at nine practices across Leicestershire. But he told LeicestershireLivein 2020 that he was stepping down from his role due to his concerns within the CQC.
The email sharing the questions asks colleagues to treat the documents “in the strictest of confidence” and instructs them not to have them on the day of the inspection. He goes on to tell staff to familiarise themselves with the questions the inspectors will be asking and to approach him if anyone was “unsure of the answers.”
“…A CQC spokesperson said they would not be investigating the allegations because Mr Chadwick is no longer a specialist advisor.
The spokesperson added: “Shaun Chadwick used to work at the CQC as a specialist advisor in primary medical services, however he is no longer employed by the CQC. We are not aware that he sent an email to a GP practice including details about the CQC inspection framework.”
All of the above accusations have also been put to Mr Chadwick, Spectrum Health, NHS England and Leicestershire and Rutland CCG. Mr Chadwick has denied the allegations to LeicestershireLive.
A Spectrum Health spokesman said: “Mr Chadwick denies allegations made and legal proceedings via our solicitor and Leicestershire Police have commenced. Mr Chadwick takes such allegations extremely seriously and therefore ordered an external facilitator to investigate working culture at Spectrum Health.
“We can confirm that such allegations are grossly inaccurate and insulting.”
A joint statement from NHS England and LLR CCGs said: “We cannot comment on ongoing individual cases, but we are aware of concerns which have been raised and we are working to investigate following the appropriate NHS complaint processes.”
I can understand that CQC would not investigate Chadwick as an employee, now that his employment with his CQC has ended.
But surely CQC has grounds to investigate his service as a provider that allegedly abused the inspection process?
How many CQC specialist advisors use their insider inspector knowledge to benefit their own provider services? How does CQC manage the risk of such breaches?
“CQC recognises that in the course of your regular work outside of CQC, you may be asked to speak at conferences or make presentations to various groups. In these presentations you may wish to use your experiences of participating in CQC inspections to illustrate your talk. In such circumstances you must:
• notify the conference organisers that you are not speaking on behalf of CQC
• not imply that you are appearing and/or speaking for or on behalf of CQC;
• anonymise any data from which an individual could be identified; and
• not breach the confidentiality provisions as set out in this Agreement or any relevant CQC policy on confidentiality.
We advise you to seek guidance from CQC if you are unsure about your obligations around this and how they apply to a given set of circumstances. “
Some CQC specialist advisors have been known to sell regulatory compliance services to provider organisations.
The current National Freedom To Speak Up Guardian was a CQC specialist advisor and she also advertised consultancy services including CQC inspection advice:
Introduction: Mary Robinson Tory MP for Cheadle and Chair of the controversial Whistleblowing APPG introduced a new Bill in parliament on 26 April under the ten minute rule. A second reading was oddly scheduled on 6 May 2022 when parliament was prorogued, so the Bill fell. The Bill itself was not published until 3 May 2022, on the APPG’s website. It transpired that the real target might not actually be to pass this legislation but to secure related insertions into the Economic Crime Bill. The Whistleblowing APPG’s campaign to change UK whistleblowing law has caused concerns since its inception in 2018 with funding from US bounty hunting lawyers. The US bounty hunting model benefits only a handful of whistleblowers and is only interested in whistleblowing which recovers very large sums of money. It seems likely that the APPG will continue pushing. We have therefore examined and provided a critique of the recent, fallen Bill in anticipation of future attempts to introduce similar legislation.
A Critique of the Whistleblowing APPG’s April 2022 Whistleblowing Bill
By Minh Alexander NHS whistleblower, Martin Morton Social Care whistleblower, Clare Sardari NHS whistleblower 24 May 2022
Summary: The Whistleblowing APPG’s now fallen draft legislation could be understood as a bounty hunter’s Bill. The Bill is poorly written, mis-numbered and in parts frankly unintelligible. Although the APPG claims its Bill champions whistleblowers, it does not focus much on protection. It does not invest enough in ensuring a safe and appropriate response to whistleblowers’ concerns, nor in criminal sanctions which cover the full range of serious breaches against the public interest. Instead, the Bill focuses on:
Massively widening the definition of ‘whistleblower’, which would increase the bounty hunting market
Building in a gatekeeping mechanism to reject some whistleblowers if necessary – perhaps the less profitable?
Extracting information
Sharing information with foreign regulators
Making referrals to foreign regulators
Making provision for ‘recognition’ of whistleblowers which in other published material has been equated to financial payment
The uncapped financial aspects of redress orders
Making provision for massive financial fines, which at a later point could be made subject to bounties
Points 3 and 4 are particularly relevant to lucrative law suits under US bounty hunting law, which can be filed from overseas. The US bounty hunting business is a billion dollar industry for lawyers.
The APPG Bill borrows heavily from Dr Philippa Whitford MP’s Public Interest Disclosure Protection Bill but tellingly, it dropped the clause which expressly sought to minimise conflict and litigation. The APPG Bill also dropped a clause which prohibited financial rewards for making protected disclosures.
The APPG Bill does not particularise key areas, such as intended standards to be applied by its proposed Office of the Whistleblower. As the Bill places the Office of the Whistleblower firmly under government control, future policy and future whistleblowers will be at the government’s mercy. The poor drafting of the Bill and its failures of particularisation will also provide more employment for lawyers. The Bill does not appear to be so much a real challenge to power, but a knowing handshake. It is in short, a most dubious pig in a poke.
Some summarised comments follow on key areas
Please follow the links for more detailed discussion and references, if required.
The APPG Bill claims to:
“Establish an independent Office of the Whistleblower to protect whistleblowers and whistleblowing and uphold the Public Interest; to create offences relating to the treatment of whistleblowers and the handling of whistleblowing cases; to make provision for that body to set, monitor and enforce standards for the management of whistleblowing cases, to provide disclosure and advice services, to direct whistleblowing investigations, to order redress of detriment suffered by whistleblowers; to repeal the Public Interest Disclosure Act 1998; and for connected purposes.”
Mary Robinson MP and Whistleblowing APPG Chair claimed in her ten minute speech on 26 April 2022:
“The Whistleblowing Bill will set up an independent office of the whistleblower to make whistleblowing work properly and safely for everyone. It will champion whistleblowers and whistleblowing. It will be a central point where the would-be whistleblower could come for information and support. It will have support and advice services for regulators, organisations and the public. It will set standards and report back to the Government. It will ensure that those who inflict or suffer detriment will be properly compensated or properly held to account. It will have real teeth with the ability to issue redress orders, fines and penalties. For the worst offenders, there will be prison sentences.
The Bill will make whistleblowing work by ensuring that concerns are investigated and acted on. It will transform our culture, normalise speaking up and put an end to the discrimination against whistleblowers.”
There is no proactive legal duty to protect or to prevent detriment. The Bill makes no link to Human Rights.
The Whistleblowing APPG’s Bill provides no mechanism by which early protection, early resolution, prevention of escalation and litigation can be achieved. There are no protective provisions such as pre-approval mechanisms before dismissal. There is not even parity with current discrimination law in terms of a proactive public sector duty to promote Equality for whistleblowers.
For comparison, EU law gives whistleblowers access to legal aid.
The APPG Bill gives no clear provision for stays and injunctions against harm.
It does not encourage the use of internal channels, which can be seen as favouring the bounty hunting industry by maximising the number of potential clients who may go straight to lawyers.
The Whistleblowing APPG harvested whistleblower data and feedback, with this note in its report of April 2022:
“All of those interviewed or who participated in the call to evidence were asked what changes they would like to see introduced. We received 100% agreement for the importance of creating a truly independent Office of the Whistleblower”
It is remarkable then that the APPG has put forward its Bill for an Office which is NOT independent but under full government control.
The Whistleblowing APPG has lifted the core passage from Dr Philippa’s Bill to introduce a Whistleblowing Commissioner, but with highly significant changes and omissions which likely signal intent.
Dr Whitford’s Bill provides for a Commission as follows:
“(4) The objectives of the Commission are—
(a) to ensure that concerns raised by whistleblowers are acted upon;
(b) to promote good corporate governance and discourage misconduct and malfeasance;
(c) to protect the public purse and ensure that wrongdoers bear the cost of wrongdoing revealed by whistleblowing;
(d) to promote the normalisation of whistleblowing as part of ethical governance, operating with a presumption in favour of transparency; and
(e) to reduce conflict and litigation relating to whistleblowing.”
The APPG provides for an Office of the Whistleblower as follows:
“(4) The objectives of the Office are—
(a) to encourage and support whistleblowers to refer concerns to the appropriate authorities;
(b) to support an effective and fair whistleblowing process;
(c) to protect the public purse and ensure that wrongdoers bear the cost of wrongdoing revealed by whistleblowing;
(d) to promote good governance through the normalisation of whistleblowing:
(e) to ensure that concerns raised by whistleblowers are acted upon;
(f) to monitor and review the operation of this Act.
That is to say, the Whistleblowing APPG has actively removed the clause:
“to reduce conflict and litigation relating to whistleblowing”
These elements are of course necessary to the income of the bounty hunting industry.
The APPG Bill also gives the Office of the Whistleblower “powers to establish schemes for the recognition of whistleblowers”.
That looks like “rewards” by any other name. Indeed, some members of the Whistleblowing APPG have spoken in favour of whistleblower rewards and incentives.
The APPG Bill plants a dangerous barrier to whistleblowers who seek help from the Office of the Whistleblower by allowing it to reject complaints “determined to be frivolous, malicious or vexatious”. After so many years dispensing with the much abused “good faith” test in the Public Interest Disclosure Act (PIDA), this is a seriously retrograde step.
But the APPG’s proposed barrier could be useful to a bounty hunting organ that wanted to let through lucrative cases whilst blocking those that are unprofitable.
The APPG gives no standards of whistleblowing governance in statute. They are all left to the Office of the Whistleblower to define and by implication therefore at the government’s mercy.
An enquiry to Mary Robinson MP about her vision for the putative regulations to be applied by the Office of the Whistleblower has not been answered.
A particularly important sleight of hand to note is that the Bill seeks to control how whistleblowers’ concerns are investigated – albeit without saying how it will do so – but critically, the Bill omits enforcement of investigation and action upon whistleblower’s concerns.
The Bill borrows from Dr Whitford’s Bill in providing redress orders, but it again makes telling changes focussed on maximising financial payouts.
Dr Whitford’s Bill stated:
“A redress order may order financial redress but must not order financial reward for making a protected disclosure”
The Whistleblowing APPG has changed this to:
“A redress order shall include an order for financial redress where loss or damage has been incurred. No such order shall be subject to any cap.”
The APPG’s Bill proposes massive fines for organisations up to £18 million (or more if the government pleases). This would have a devastating effect on public services if levied against public bodies. Such fines are also self-defeating because it is often under-funding that contributes to public sector service failures, cover ups and whistleblower reprisal.
The proposed massive fines could be made subject to bounties with further legislation at a later date.
The APPG’s Bill restricts new criminal offences to only:
The EU requirements include dissuasive penalties against:
Hindering reporting
Vexatious proceedings against a whistleblower
Breaches of confidentiality of whistleblower identity
Lastly, for some light relief, we gave up at this word hurdle:
“…and, in the absence of evidence establishing the contrary, a relevant person shall be taken to decide on a failure to act when that person does an act inconsistent with doing the failed act or, if that person has done no such inconsistent act, when the period expires within which that person might reasonably have been expected to do the failed act if it were to be done.”
A prize for any soul who can unravel this contorted mystery. (Capped, and non-financial, of course).
Petition
If you would like to see effective reform of UK whistleblowing law that is genuinely in the public interest, and that is not about promoting any private interest and does not risk the good name of whistleblowers by confusing genuine public interest disclosures with bounty hunting or the use of paid criminal informants, please support this petition: