
By Dr Minh Alexander NHS whistleblower and former consultant psychiatrist, 20 February 2021
On 19 February 2021 the Care Quality Commission published a local inspection report about Worcestershire Royal Hospital, which is run by Worcestershire Acute Hospitals NHS Trust.
Maternity service safety was criticised, as was poor culture and the trust’s response to maternity whistleblowers.
In consequence, CQC issued improvement notices to the trust on grounds of unsafe staffing and poor governance:
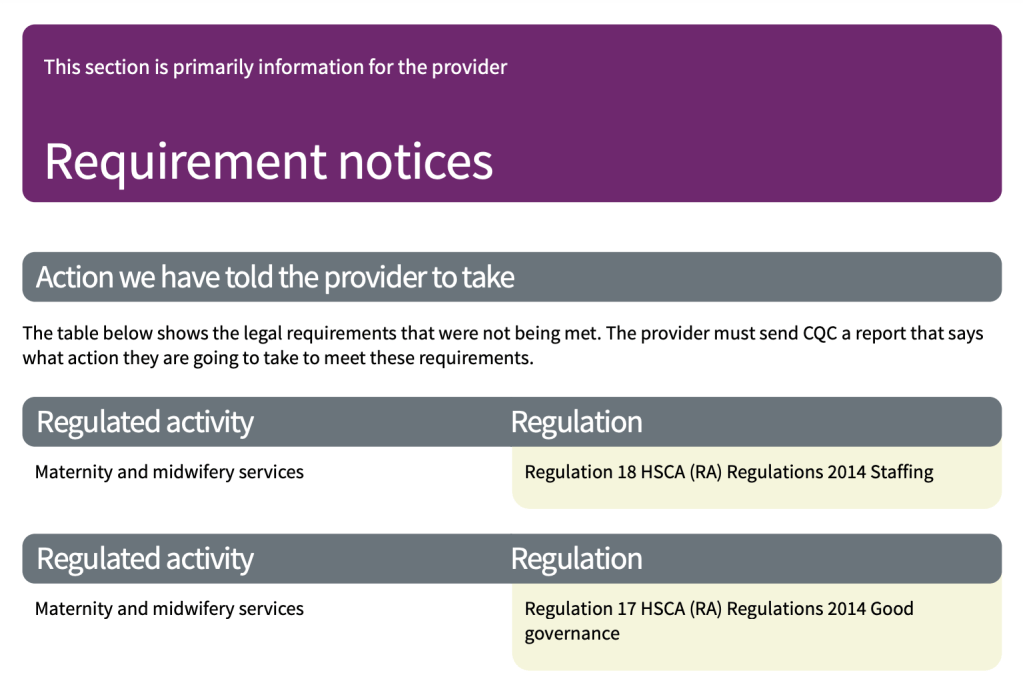
CQC Chief Inspector of Hospitals Ted Baker set the tone with the comment:
“Staff should never feel that their concerns are not listened to…”
Background
The trust has long been troubled. It has struggled for years with massive PFI debt, which was written off by the government only last year because of the pandemic. Alongside scraping around to make ends meet, the trust had problems with poor care quality and governance scandals such as several cases of whistleblower suppression and reprisal.
Worcestershire Acute Hospitals NHS Trust was placed into special measures for five years, finally exiting in 2020.
Very controversially, David Nicholson – of MidStaffs Public Inquiry notoriety – was appointed as Chair in 2018:
NHS Improvement also allocated as Improvement Director to the trust an NHS manager who had been criticised by an Employment Tribunal for whistleblower reprisal, in the unfair sacking of Andrew Smith a trade union rep at Mid Essex Hospital Services NHS Trust.
Andrew Smith was awarded £127K compensation by the Employment Tribunal.
Maternity safety at Worcestershire Acute NHS Trust and the CQC’s criticisms
On 8 October 2020 local media reported concerns by a maternity whistleblower who asked to be anonymous, about unsafe staffing:
“Whistleblower midwife says staff are exhausted and ‘working like dogs'”
Trust board papers claimed that maternity staffing in September 2020 was safe:
Trust board papers later referred to challenges in October and November 2020, but the trust claimed that safe staffing incidents had not caused patient harm:
“Achievement of safe staffing in maternity has been challenging. Whilst minimum safe staffing levels have been maintained in October and November there has been a reliance on the support of the escalation policy when acuity is high”.
“The main areas that were challenged were maternity services and speciality medicine wards at Alexandra Hospital and Avon 2 on the Worcester Royal site due to vacancies. There has been no harm to patients reported from staffing incidents.”
However, an internal trust report of 26 January 2021 admitted that there had been two fatal serious incidents in maternity services during Quarter 3:
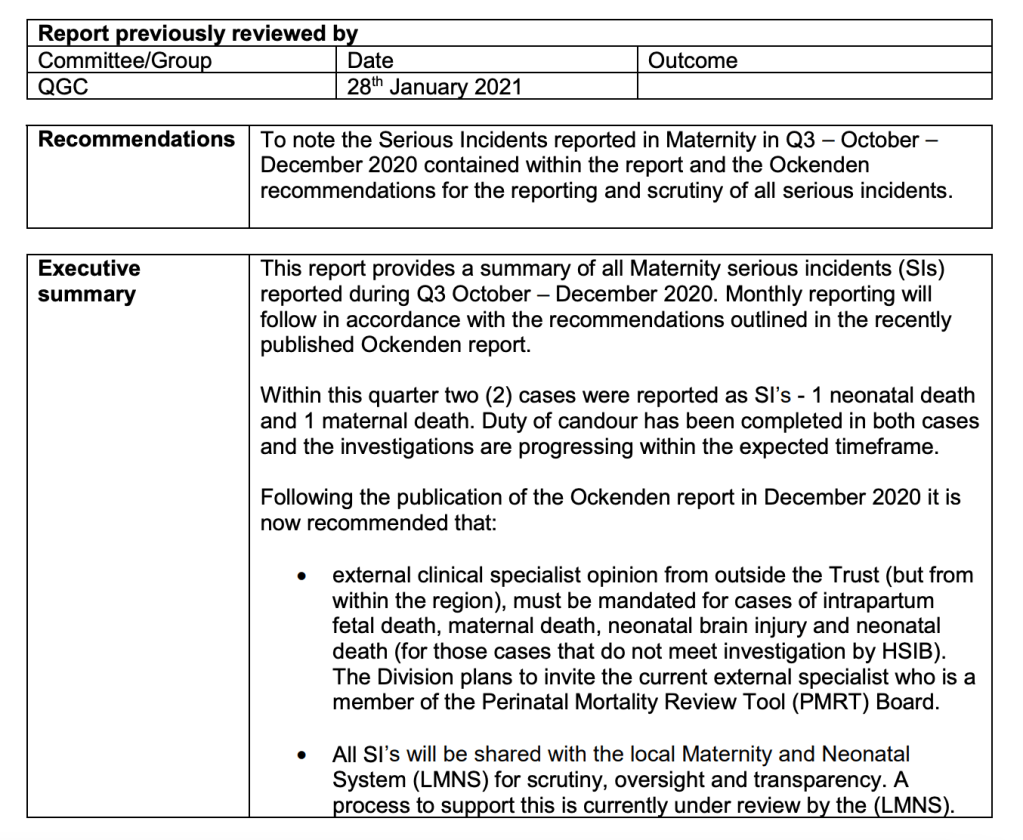
The two deaths were reported as follows in the trust’s document:
“Case 1
Incident category – Neonatal Death
Woman in her 1st pregnancy booked late at 25 weeks gestation and appropriately booked for consultant led care. Antenatal care – no concerns identified. At term, the mother called triage , reporting bleeding with spontaneous rupture of membranes. Immediately seen on arrival and a fetal bradycardia was noted, a category 1 lower segment caesarean section (LSCS) was called and a baby girl was born within 30 minutes. Birthweight 3232grams on the 30th centile, requiring extensive resuscitation – which was unsuccessful and therefore a neonatal death was confirmed. The Immediate Case Review was discussed at the Divisional Quality and Safety Review Meeting (QSRM ) on 09.12.20 further information requested before a decision on how the case should proceed. Presented again at QSRM on 16.12. 20 agreed to escalate as an SI – escalated to corporate team & reported via S tEIS on 21.12.20
Terms of reference agreed:
Investigate all aspects of maternity care in the antepartum, intrapartum and postpartum period, with specific focus on:
– The review at 38 weeks in triage and decision making in the intrapartum period.
– The process around the decision for induction
– The resuscitation and care of the baby up to the point of CPR being stopped.
– Ensure that the perception of events is captured from the family, the Trust and staff directly involved in the care of the mother and the baby
Immediate learning & review of guidance
· If the woman presents at or after 37+0 weeks of gestation, it is important to establish if the bleeding is an Antepartum Haemorrhage (APH ) or blood stained ‘show’. In the event of a minor or major APH, national guidance recommends induction of labour with the aim of achieving a vaginal birth to avoid adverse consequences potentially associated with a placental abruption. (R oyal College of Obstetricians & Gynaecologists Green Top Guideline, No 63, page 12, Nov 2011)
· In cases of recurrent unclassified APH , induction of labour should be considered at or near term even if fetal growth is satisfactory. (WHAT -TP -094, 15/11/19). Duty of Candour was completed by the Consultant Obstetrician . Case was immediately referred to:
– Coroners
– HSIB; however this case did not meet the criteria (as the woman not in labour ) .
Case 2
Incident Category – Maternal Death
A woman in her 3rd pregnancy attended maternity triage at Worcestershire Royal Hospital with a history of left sided lower abdominal pain. After assessment and treatment she was discharged with a plan for follow up in the Maternity Day Assessment Unit (DAU ) . She was reviewed the following day at maternity DAU complaining of frontal headache, screening for pre -eclampsia test undertaken and test result suggested that woman was low risk for developing pre -eclampsia. A plan was made for further follow up in 1 week. She attended as per plan and was complained of worsening symptoms. Admission was recommended to enable further investigations to be completed and she then had regular reviews, further blood tests and chest x -rays. During her inpatient stay the woman was reviewed by the consultant and noted to have a mild headache, visual disturbances and epigastric pain. The woman was found collapsed and unresponsive at her bedside. Cardiopulmonary Resuscitation (CPR) was commenced and a peri -mortem caesarean section was undertaken within the recommended 5 -7 minutes. A live baby was born and transferred to the neonatal unit for CPAP. Ongoing maternal resuscitation continue however following an extensive period of resuscitation and further surgical intervention resuscitation ceased following agreement with the attending team. Immediate learning & review of guidance
· VTE assessment was completed; however there has been discussion about whether the most appropriate dose of LMWH was prescribed.
· Duty of Candour completed with partner by Matron and letter provided. Family supported by bereavement specialist midwives.
· Staff supported by Trust Clinical Psychologist, OH advice provided and support from clinical leads, Matrons and wider DMT.
· Referred to HSIB – Investigation ongoing. Investigation within reporting deadlines (6 months HSIB)
· Referred to MBRRACE and Coroner
· Escalated to corporate patient safety team and reported via S tEIS. Initial postmortem – no cause of death identified.”
Maternal deaths are very rare and may indicate poor care quality.
The MBRRACE study reported there were 217 maternal death in the UK 2016-18:
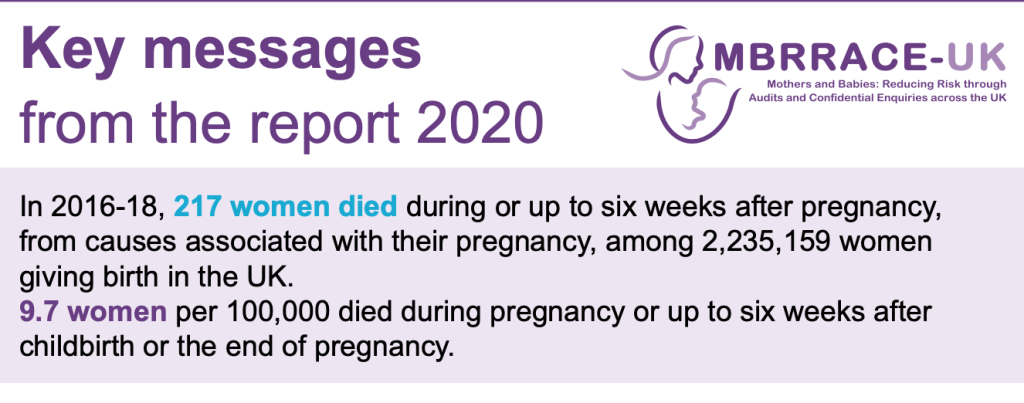
According to the CQC, Worcestershire Acute NHS Trust has reported four maternal deaths over a two year period:
CQC’s inspection report of 19 February 2021 on Worcester Royal Hospital severely criticised the management of the maternity service. This comes on top of previous criticism from an inspection in 2018.
CQC’s recent inspection was unannounced, reflecting the level of concern about intelligence received.
CQC concluded that:
- The maternity service was not sufficiently safe
- Not all maternity patients were adequately risk assessed
- Managers did not audit swab counts
- Safety incidents were not well managed and downgraded with suspected failures of Duty of Candour
- There was risk of baby abduction and other suboptimal safeguarding practice.
Echoing themes from the MidStaffs Public Inquiry, CQC noted:
“Staff did not always contribute to decision-making to help avoid potential financial pressures compromising the quality of care”
Most strikingly, the CQC stated:
“The service did not have an open culture staff felt they could raise concerns without fear”.
Whistleblowers told the CQC of delays in induction:
“Whistle-blowers reported that there were delays in induction of labour with some women waiting up to a week instead of one to two days. Managers told us that there had been delayed inductions of up to six women.”
Whistleblowers also complained to the CQC that managers ignored their concerns about safe staffing, and CQC was concerned about the trust’s inadequate levels of planned staffing:
“Between July and September 2020, we received four whistleblowing enquiries relating to maternity services. Staffing levels were the main area of concern reported. The whistle-blowers reported the introduction of the CoC model had negatively impacted on staffing levels,yet was a management priority. We spoke to staff of all disciplines throughout the unit who unanimously raised concerns about safe midwifery staffing levels and reported they did not feel their concerns were always considered by managers. Midwives told us that the service was always short staffed and that they were moved frequently within the department. We had concerns about planned staffing levels throughout the unit. Following the four whistleblowing concerns, managers had instigated meetings to listen to staff concerns and take actions to address them. A further planned introduction of another CoC team in December 2020 had been deferred until 2021 as new staff were expected to start in December and were delayed until January 2021.”
This is a list of key concerns about maternity services that were flagged by CQC’s report:
“Our rating of safe went down. We rated it as requires improvement because:
• Not all staff were up to date with their training.
• We were not assured that all medical staff had current knowledge relating to Mental Capacity Act 2005 and Deprivation of Liberty Safeguards due to poor training compliance.
• Risk to women was not always identified appropriately. Staff did not always complete and update risk assessments for each woman or act to remove or minimise risks. Staff did not always identify and act quickly when women were at risk of deterioration.
• Whilst staffing levels were often lower than planned, managers regularly reviewed and adjusted staffing levels and skill mix. Actions were taken to meet patient acuity, however, these were not robustly documented. Staff were redeployed within the unit when needed, to keep patients safe from avoidable harm and to provide the right care and treatment but records of this were weak.
• The service did not always manage safety incidents well. Staff recognised but did not report all incidents and near misses. Managers investigated incidents and shared lessons learned with the whole team and the wider service. However, staff did not always have time to check emails to find updated incident information. When things went wrong, staff apologised and gave patients honest information and suitable support.
• Staff did not always monitor the effectiveness of care and treatment. When care and treatment was monitored, they used the findings to make improvements and achieved good outcomes for women.
• Training compliance had fallen during the COVID-19 pandemic but a plan was in place to improve this. However, the service generally made sure staff were competent for their roles.
• Although leaders mostly had the skills and abilities to run the service and understood the priorities and issues the service faced, they did not always take timely action to address the concerns identified. They were visible in the service for women and staff.
• Staff did not always feel respected, supported and valued by all managers. They were focused on the needs of women receiving care. The service did not have an open culture staff felt they could raise concerns without fear.
• Although leaders and teams used systems to manage performance they did not always identify and escalate relevant risks and issues or identify actions to reduce their impact. They did not have plans to cope with unexpected events. Staff did not always contribute to decision-making to help avoid potential financial pressures compromising the quality of care.
• Whilst governance processes were in place leaders did not always operate these effectively throughout the service. Leaders liaised with partner organisations. Staff at all levels were not always clear about their roles and accountabilities and did not all have regular opportunities to meet, discuss and learn from the performance of the service.
• The service did not always collect reliable data and analyse it. Staff could not always find the data they needed, in easily accessible formats, to understand performance, make decisions and improvements. The information systems were integrated and secure. Data or notifications were consistently submitted to external organisations as required.
• Leaders did not always engage with staff effectively. However, staff actively and openly engaged with women, equality groups, the public and local organisations to plan and manage services. They collaborated with partner organisations to help improve services for women.
• Although all staff were committed to providing good quality care timely action was not always taken to improve.
“The labour ward and delivery suite posed a risk for baby abduction. Most staff were aware of the baby abduction policy but there were no baby abduction drills included in maternity specific training. This meant some staff may not know what to do in such circumstances. Managers told us that abducted baby procedures would be included in the next skills and drills courses.”
“The service did not always adequately risk assess all women in the ante-natal unit.”
“Managers were not auditing swab counts following vaginal or instrumental births.”
“We reviewed incidents reported on the National Reporting and Learning System by the trust from July to September 2020 which identified that term babies admitted to the neonatal unit were graded as no or low harm. This meant that incorrectly graded incidents may not be investigated and there was a risk that women were not informed of the significance of harm caused to them or their baby, or that appropriate action was taken to prevent further occurrences. We were not assured that incidents that were moderate, in line with definitions in Regulation 20 Duty of Candour guidance 2015, were always graded correctly according to the level of harm. We also saw that there were 11 incidents reported where safeguarding information was not transferred to all medical records. This meant that babies and young children may be at significant risk of harm if information was not shared appropriately.”
Worcestershire Acute Hospitals NHS Trust’s Freedom To Speak Up Guardian
The poor whistleblowing governance found by the CQC represents a serious embarrassment for the government’s woeful Freedom To Speak Up project, six years on from commencement of the project.
This is particularly because an examination of publicly available records shows that Worcestershire Acute Hospitals NHS Trust’s Lead Freedom To Speak Up Guardian is the Maternity Matron:
The small print of the CQC report noted that maternity staff had “concerns” with speaking with the trust Freedom To Speak Up Guardian:
“We met with members of the senior leadership team who demonstrated an awareness of the service’s performance and the challenges they faced, including staffing issues and the concerns staff had with speaking with the freedom to speak up guardian.”
The events at the trust lead to questions about whether the Guardian was part of the culture failure, or was unable to discharge her duty effectively due to the weakness of the Freedom To Speak Up model.
It was certainly awkward for maternity staff to be faced with whistleblowing to a senior member of the department, who potentially had conflicts of interest.
Whatever, the usual puffery has abounded.
The trust made the most of a small blessing – a finding that it had improved from an abysmal level on the national NHS staff survey questions about raising concerns:
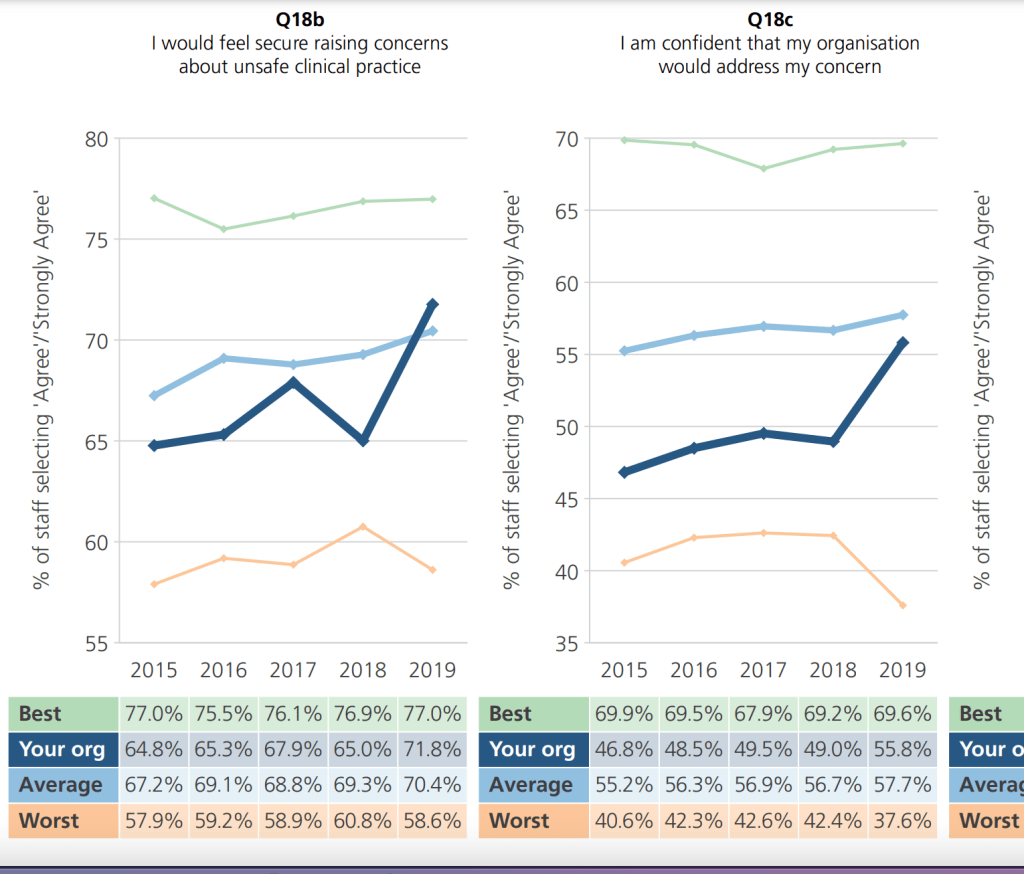
– with a local media splash:

And Henrietta Hughes the National Guardian has continued to aid and abet smiley government propapanda on the illusory success of the Freedom To Speak Up project.
With an unerring instinct to laud failure, she and her Office produced this happy image of whistleblowing at Worcester just weeks before the publication of CQC’s damning report:
We are literally going round in circles when a centrally criticised figure from the Midstaffs scandal involving unsafe staffing and suppression, returns to a chair a trust which is then criticised for unsafe staffing and ignoring whistleblowers.
We badly need reform of very weak UK whistleblowing law to sweep away pretences such the Freedom To Speak Up Potemkin village, and to genuinely protect UK whistleblowers and the public.
If you have not already done so, please sign and share this petition for whistleblowing law reform amongst your circle and across social media:
Petition: Replace weak UK whistleblowing law, and protect whistleblowers and the public
Many thanks
RELATED ITEMS
NHS Improvement was previously warned about its assignment of an Improvement Director to Worcestershire Acute Hospitals NHS Trust who had been criticised by an Employment Tribunal for whistleblower reprisal. As the recent CQC report indicated that trust managers were aware that staff had concerns about speaking with the Freedom To Speak Up Guardian, I have asked NHS Improvement to review its oversight of the trust and to establish whether managers acted appropriately on this staff concern.
Letter 20 February 2021 to Tom Grimes NHS Improvement head of whistleblowing, cc Dido Harding
Freedom to Speak Up Guardian jailed
The Disinterested National Guardian & Robert Francis’ Unworkable Freedom To Speak Up Project
Replacing the Public Interest Disclosure Act (PIDA)
The government’s Freedom To Speak Up project in an image:


