Dr Minh Alexander retired consultant psychiatrist 22 September 2022
Summary: The Care Quality Commission has downgraded North Teed and Hartlepool NHS trust which was found by the Employment Tribunal to be responsible for severe whistleblower reprisal against two of its staff, with the Well Led domain now rated “Requires Improvement”. However, this does not change the fact that CQC failed to find any breach of CQC Regulation 5 Fit and Proper Persons (FPPR) in these cases. Nor does it seem likely that it will deter future whistleblower reprisal, as individual and not organisational sanctions are needed. Moreover, the CQC’s inspection report describes cultural issues which would make whistleblowing substantially more difficult at the trust, but CQC did not seem to weigh these factors when assessing the trust’s whistleblowing governance.
I have on several occasions criticised the CQC’s failure to hold any erring NHS senior managers to account under CQC Regulation 5 Fit and Proper Persons (FPPR), even for very serious breaches such as whistleblower reprisal. For example:
CQC has not found any breach of FPPR by North Tees and Hartlepool NHS Trust in response to my referrals on two trust directors criticised by the Employment Tribunal for their actions against trust whistleblowers Linda Fairhall senior nurse and Mr Manuf Kassem, surgeon. The trust managers whom I referred were Lynne Taylor Director of Planning and Performance, now retired, and Dr Deepak Dwarakanath the Medical Director who remains in post.
CQC unusually wrote to me, unprompted, to say that it was inspecting North Tees:
Also, and most unusually, CQC sent me the North Tees 16 September 2022 inspection report:
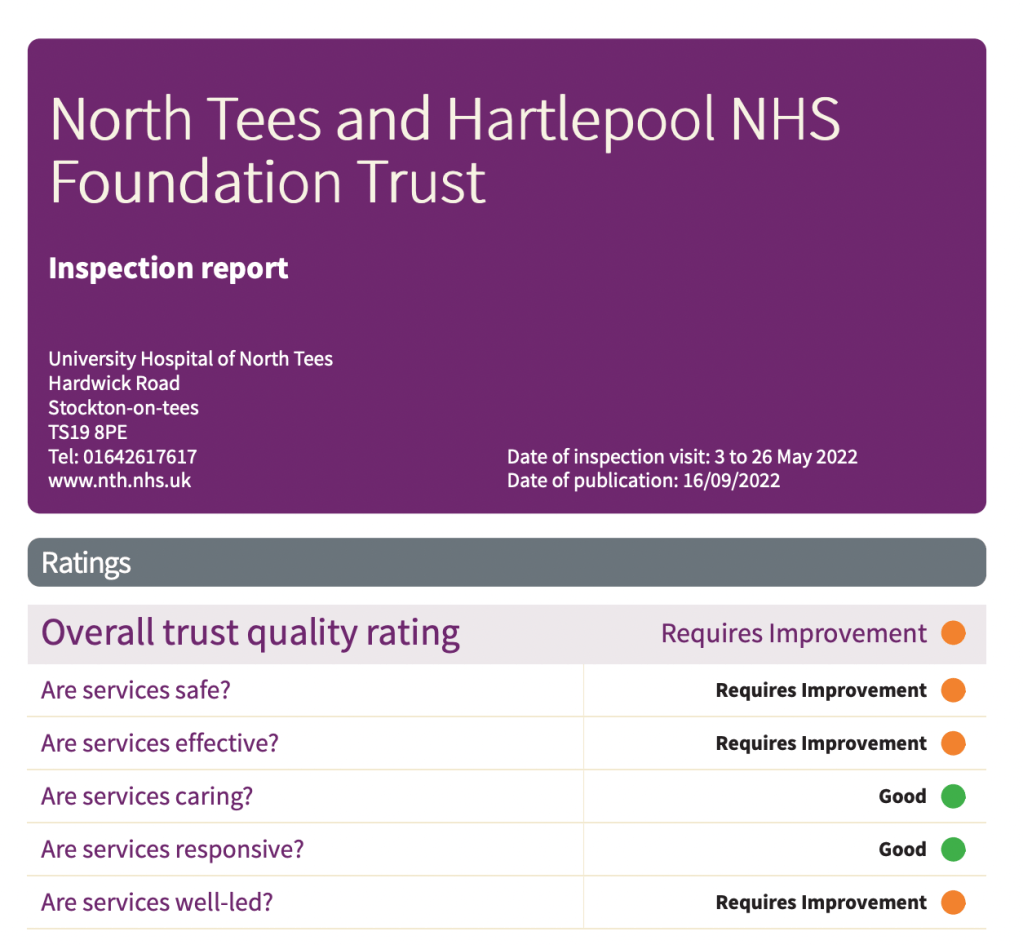
The inspection report makes some unfavourable observations about North Tees’ senior management; and downgrades the rating on the Well Led domain to “requires improvement”:
“Due to the ratings given at this inspection, the trust’s overall ratings of good across all domains changed to requires improvement in safe, effective and well-led. This meant that the trust’s overall rating changed from good to requires improvement.”
“Our rating of services went down. We rated them as requires improvement because:
• The trust had interim arrangements in place for several key roles, and there was a lack of united leadership and succession planning. Most strategies were in draft, incomplete and not complementary.
• Senior and executive leaders did not always operate effective governance systems to manage risks and issues within the service. Governance arrangements were complex and the board did not always have sufficient oversight and focus on operational risks.
• The trust did not have enough medical and midwifery staff in the areas we inspected to care for patients and keep them safe. Medical staff did not all have regular, up to date appraisals.
• The trust had not engaged with its local community to find out what people wanted and needed. Engagement strategies were not existent, or in development, and had not included consultation with the wider community, equality groups, the public or other local organisations.
• The trust did not always discharge its responsibilities fully under Duty of Candour regulations and did not audit compliance. Complaints were not being handled in line with the trust’s complaints policy”
However, despite two recent Employment Tribunal judgments against the trust for severe whistleblower detriment, the CQC gave only a bureaucratic account of the trust’s whistleblowing governance:
“Staff we spoke to said that they did feel able to speak up and raise concerns, and in midwifery, staff told us they had seen the Freedom to Speak Up Guardian (FTSUG) in their department. The FTSUG reported to the board yearly through an annual report and prepared a monthly report for the executive team. The FTSUG was appointed in August 2021, with an increase in hours to a full time role.
There were also 10 freedom to speak up champions across the trust and NTH Solutions. All could be contacted by email, and the FTSUG could also be contacted by telephone, however the trust’s speak up policy, associated flowchart and poster were confusing and did not clearly state that a member of staff with patient safety concerns could directly contact the FTSUG.
The FTSUG formed part of the formal induction process for new starters and had also attended some volunteer induction sessions. In 2021, the FTSUG had received no cases in quarter one, two in quarter two, 34 in quarter three, and 14 in quarter four. The main themes were around senior management and culture, staffing, patient safety and the working environment. No more detail was presented to board on these themes or any action taken as a result and there was no documentation of any discussion around the sudden increase in Q3.”
Remarkably, CQC sought to portray the trust as victims of publicity following the Employment Tribunal’s findings in favour of whistleblowers:
“The trust had experienced departures of some well-known staff, had been ruled against in two recent employment tribunals with some media interest in these. Leaders spoke about the challenges these had posed, the toll that they had taken on staff, and a wish to ‘move on’ with culture work.”
That is surely a very special way of looking at whistleblower reprisal and accountability.
Also, CQC’s anodyne account of North Tees’ whistleblowing governance seems to be contradicted by its acknowledgment of a “disconnect” between the frontline and the trust board:
“During our inspection front line staff did not describe leaders as visible and approachable and morale was not always positive in the two core services we visited.
There was a clear disconnect and difference in views around the board leadership, with the executive team talking incredibly positively about leadership and the changes they had made for the better. However, others we spoke with did not share this view and were less positive about the direction of leadership, describing challenges and differences of opinion.
Staff working ‘on the ground’ in frontline services did not describe any of these benefits and some told us they didn’t feel senior leaders were visible or approachable.”
How does CQC imagine whistleblowing works if the trust board signals that it does not like bad news, and the frontline don’t feel that the trust board are approachable?
Moreover, CQC ticked its boxes on its inspection of FPPR:
“We found that the Fit and Proper Person Procedure was fit for purpose and the files were predominantly in line with the requirements of the regulation.
There is a requirement for providers to ensure that directors are fit and proper to carry out their role. This included checks on their character, health, qualifications, skills, and experience. During the inspection we carried out checks to determine if the trust was compliant with the requirements of the Fit and Proper Persons Requirement (FPPR) (Regulation 5 of the Health and Social Care Act (Regulated Activities) Regulations 2014).
We reviewed four executive and non-executive director files in total. Our review included checks for the newest executive and non-executive appointments. All files included references and signatures saying copies of original documents such as degree certificates had been seen.
We also looked at the trust’s Fit and Proper Person Procedure and spoke to the company secretary who was responsible for oversight and compliance with the FPPR procedure. We reviewed the six-monthly self-declarations, made by the directors, to confirm that they remained fit and proper and saw that these were consistently completed.”
The issues of malice raised by the two whistleblowing Employment Tribunal judgments against the trust are minimised by CQC’s failure to acknowledge them.
Perhaps CQC believes it has discharged its duty by downgrading the trust’s rating.
But if the managers responsible for whistleblower reprisal experience no personal consequences, what is there to stop them from harming future whistleblowers?
Meanwhile, NHS England’s tortoise-like implementation on the Kark Review recommendations for Fit and Proper Persons in the NHS crawls on.
Please click and add your signature to this petition to reform UK whistleblowing law – whistleblowers protect us all but weak UK law leaves them wholly exposed, lets abusers off the hook and it is a threat to public safety.
Dr Minh Alexander retired consultant psychiatrist 5 September 2022
Summary: The Care Quality Commission’s poor whistleblowing governance has been exposed by the case of Dr Shyam Kumar who was found by an Employment Tribunal to have suffered detriment by the CQC, explicitly linked to Mr Kumar’s whistleblowing.
The case reveals that the CQC:
– Failed to protect a whistleblower – Failed to act on his concerns – Failed to accept that his whistleblowing was valid, minimised his concerns and saw the whistleblowing as a nuisance and a threat – Mistreated the whistleblower seriously and smeared him with a number of unjust and false claims – When challenged by the whistleblower about this poor treatment, the regulator sought to portray him as a difficult and “challenging”, and ridiculed his claim of whistleblower reprisal by the CQC – Tried to dig dirt about the whistleblower to retrospectively manufacture a case justifying its mistreatment, abusing regulatory power in the process – Suggested falsely to the Employment Tribunal that Mr Kumar was attacking non-consultant grade doctors at his trust for financial gain, because he did not want them to do work which reduced the waiting list – Fed false information to the Ombudsman to shut down a legitimate complaint by the whistleblower about his mistreatment by the CQC – Claimed reasons for its treatment of the whistleblower which were not believed and were rejected by the ET, calling into questions the truthfulness of the claims – Operated oppressive HR policy and practice, but foolishly and incompetently maintained up to the last minute that its processes were fine.
Introduction
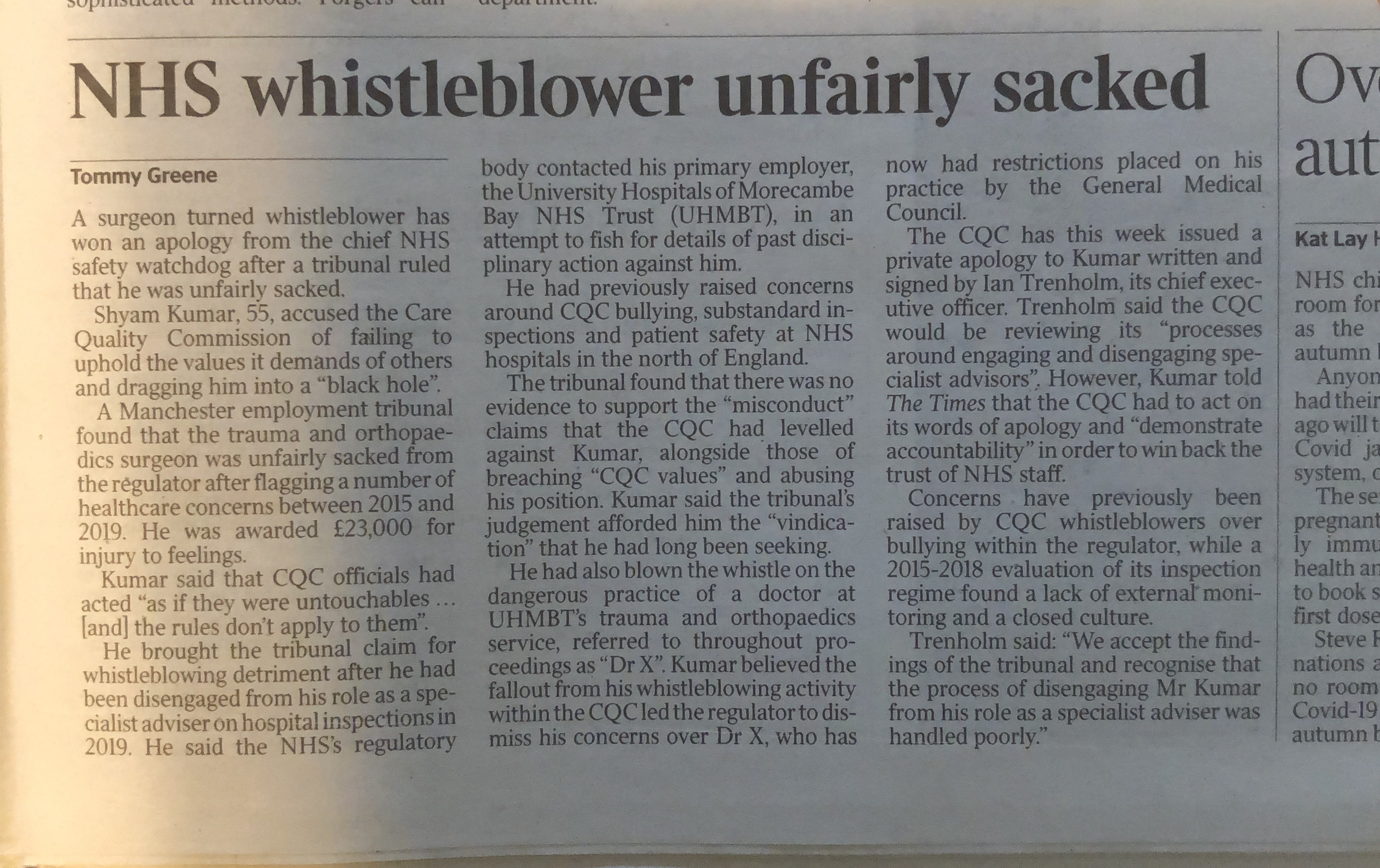
The Health and Social Care regulator the Care Quality Commission has lost an important whistleblowing Employment Tribunal case against surgeon and NHS whistleblower Mr Shyam Kumar.
This important case reveals failures by the regulator on several levels, some of which arguably amounts to serious misconduct by CQC personnel.
The regulator is supposed to protect whistleblowers and ensure good whistleblowing governance by regulated bodies.
Moreover, the CQC is legally a Prescribed Person, which means that it is supposed to be a safe haven body, to which Health and Social Care whistleblowers can make protected disclosures.
But CQC has been found by the ET to have unfairly dismissed and seriously harmed a whistleblower.
And the reason for this current failure is the same as the previous failure: CQC reacted badly to concerns about its poor regulatory performance.
CQC has clearly learnt little.
This matter raises serious questions about the honesty and probity of the regulator, which holds the welfare of so many patients and service users in its hands.
Mr Kumar’s role as a CQC Specialist Advisor
Mr Kumar is an experienced orthopaedic surgeon of unblemished record.
He has experience of assisting whistleblowers through a previous role as an active member of BAPIO. He has also has a legal qualification.
He was of good standing and hired by the Care Quality Commission as a Specialist Advisor in July 2014, on the basis of a secondment contract.
By 2015, he was in bad odour with the CQC’s senior managers, because he whistleblew to them about poor management of a CQC inspection and an experience of being bullied by the CQC inspection lead, who prevented him from talking to NHS trust whistleblowers during the inspection:
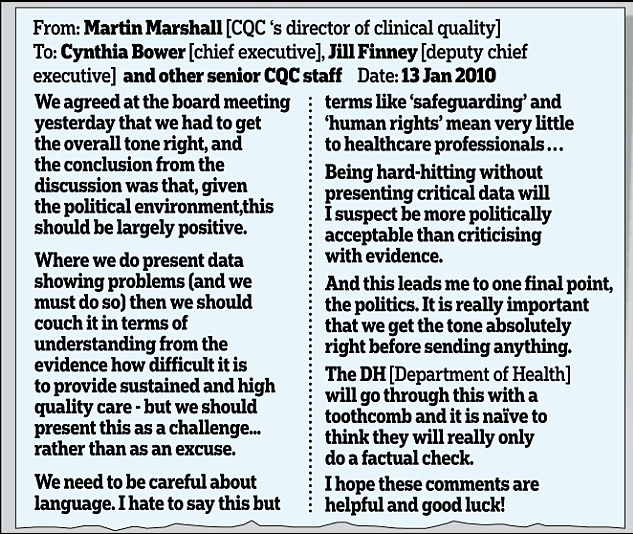
One of the concerns raised in this letter is of collusion by the CQC:
“There appears to remain a culture within the CQC, which results in some medical directors and chief executives being let off lightly when whistleblowers have raised concerns.
Mr Kumar is not aware that his concerns were ever investigated, despite a reminder. Neither has the CQC produced any records to prove that it investigated his concern.
Whistleblowing to the CQC in 2018
By June 2018 Mr Kumar had cause to whistleblow again to CQC managers, over two areas of concern:
1. CQC’s flawed inspection methodology which included using Specialist Advisors in inspections for which they were not expert. Mr Kumar’s concerns arose from a chaotic CQC inspection of East Lancashire Hospitals NHS Trust.
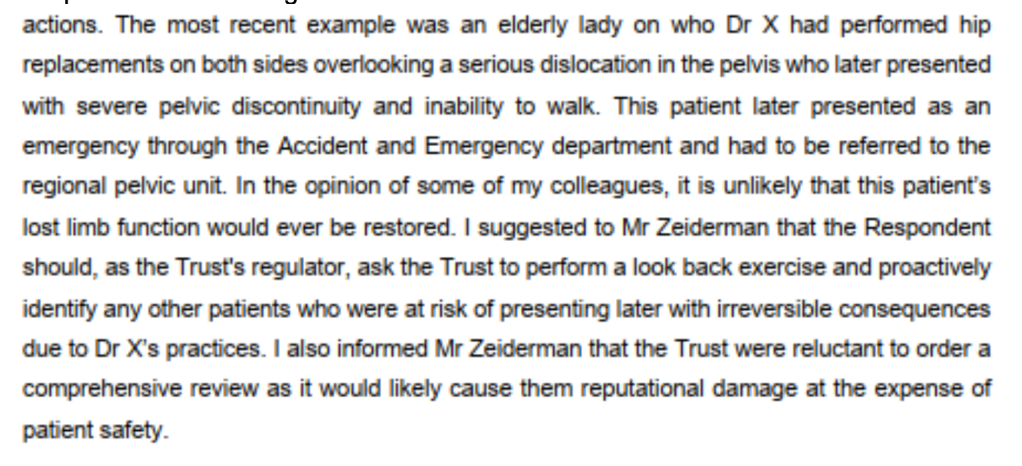
2. Issues about very serious patient safety at his own trust, University Hospitals Morecambe Bay NHS Foundation Trust.
These patient safety issues revolved around the poorly supervised orthopaedic practice of a Dr X, about which a number of consultants raised concerns. These safety concerns have been validated by two external investigations. The GMC imposed restrictions on dr X’s practice in 2018, as a result of whistleblowing by Mr Kumar and other colleagues.
As well as the patient safety concerns, Mr Kumar also raised concerns with the CQC about the governance at his trust, failure by the trust to act effectively on the patient safety issues and the fact that he had not been protected from severe whistleblowing reprisal.
The whistleblower reprisal included serious false allegations against him, including in group emails involving his peers. In one email Mr Kumar was dubbed a “traitor”.
“80. On 30 October 2018, Mr S [REDACTED], in an email to a broad recipient list, described individuals who were involved in activities against doctors of Indian origin as being ‘traitors of their community’ (p.393). Given that the claimant had raised complaints about the Dr X’s practice, and the close nexus in time that this comment is made to those complaints, on balance it is likely that this comment is about the claimant.”
Mr Kumar also raised concerns with the CQC about white consultants feeling intimidated to to raise patient safety concerns in case they would be subject to counter-allegations of racism
Mr Kumar’s concerns about the above governance failure at UHMBT have been vindicated by both external and internal investigations.
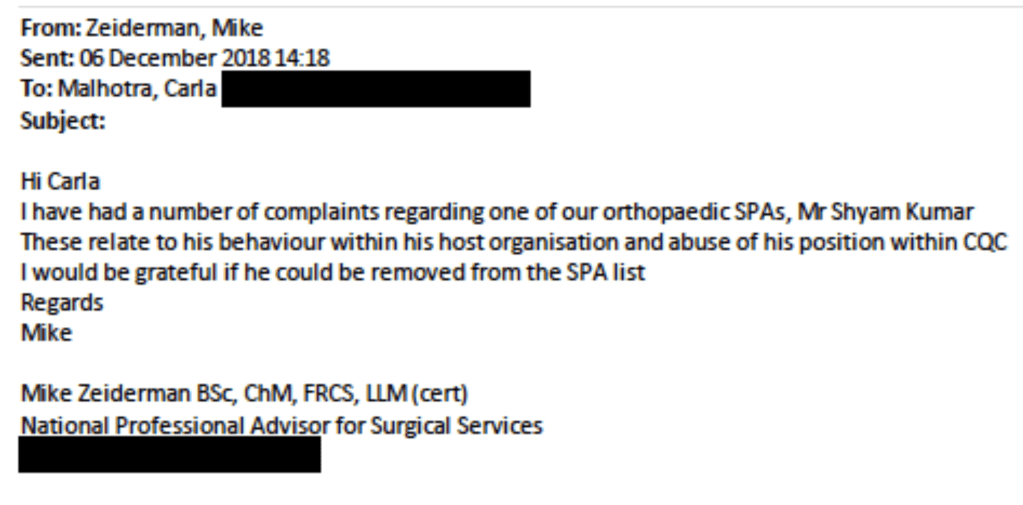
His disclosures to CQC were made primarily to the CQC National Professional Advisor, Mike Zeiderman, colorectal surgeon based at Southport and Ormskirk.
This is list of Mr Kumar’s disclosures that the ET ruled met the legal threshold of protected disclosures:
Instead of recognising the seriousness and validity of Mr Kumar’s concerns, it appears that the CQC regarded Mr Kumar’s disclosures as a nuisance and a threat.
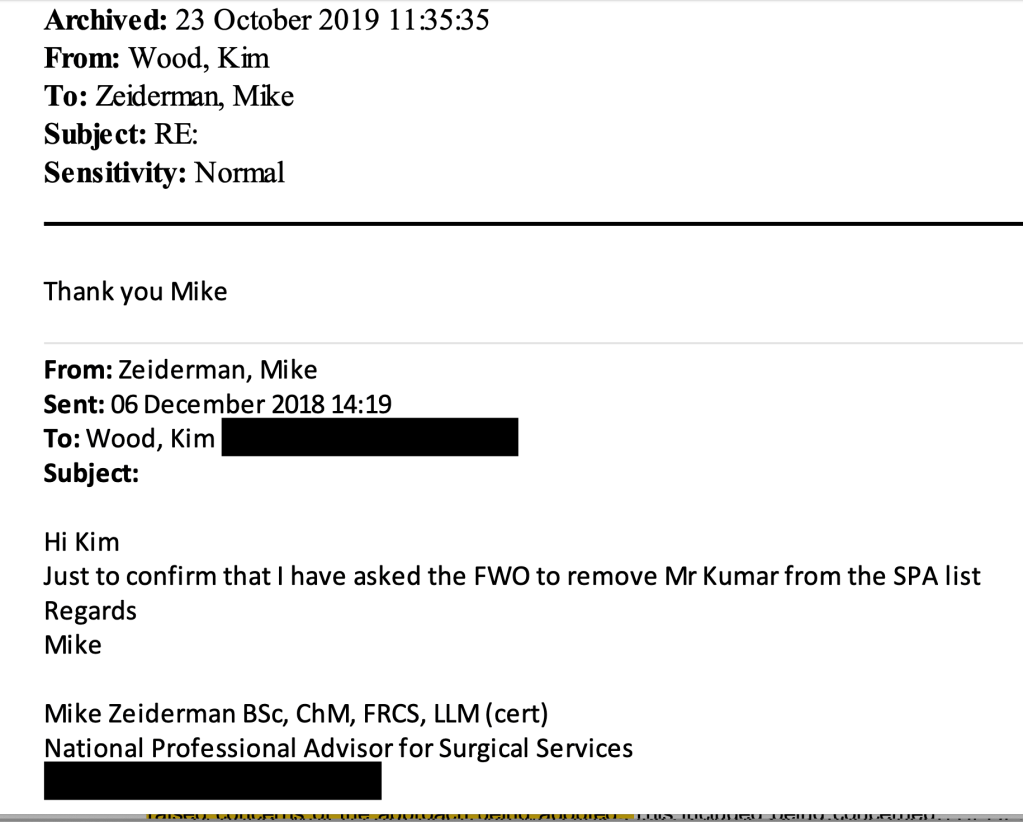
The ET considered that correspondence by Mike Zeiderman made it clear that a decision in December 2018 to sack Mr Kumar as a Specialist Advisor was explicitly linked to Mr Kumar’s disclosures to Mike Zeiderman.
These are examples of Mr Kumar’s disclosures:
The ET summarised another disclosure by Mr Kumar as follows:
“On 29 June 2018, following up his email of 16 June 2018, the claimant called Mr Zeiderman. During this phone call, the claimant reiterated concerns that matters had been raised with the Trust’s Medical Director, but that the Trust was refusing to look into those concerns but was wanting to cover up the issues. The claimant also raised specific examples of to suspicious deaths, after which the Trust had not taken steps to prevent further harm. The claimant provided specific details of the two cases to Mr Zeiderman in this phone call. The claimant was disclosing information of serious and/or potential harm to patients. Mr Zeiderman accepted the claimant’s paragraph 38 as being the content of that phone call.”
This is Mr Kumar’s account of another disclosure to Mike Zeiderman:
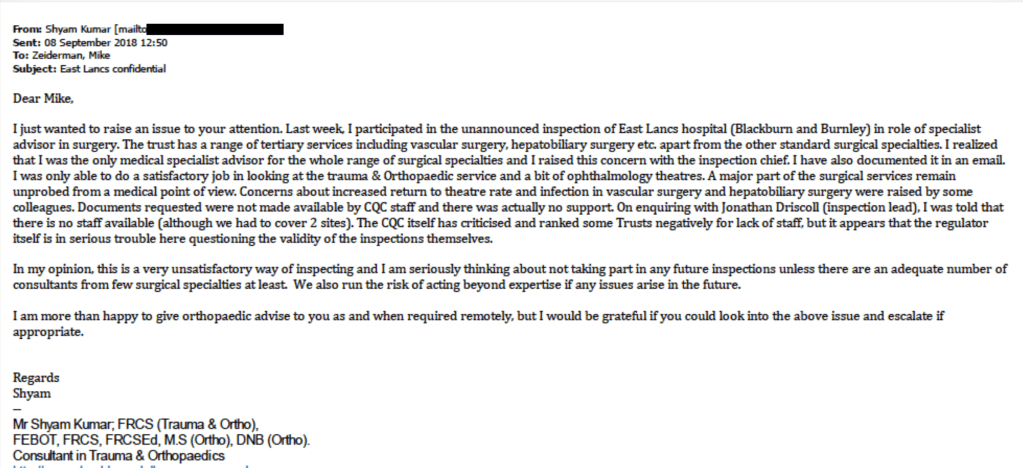
The most threatening of these disclosures from CQC’s point of view would have been the email of 8 September 2018, in which Mr Kumar made serious criticisms of CQC’s unsafe inspection methodology at East Lancashire.
The CQC later accepted that some of Mr Kumar’s communications were protected whistleblowing disclosures, but the regulator and Prescribed Person contested five significant disclosures (disclosures 2,3,4,8,10) right up to the point when the Employment Tribunal ruled that they were bona fide whistleblowing.
The ET judgment reveals that a witness statement by the local CQC inspector Kim Wood had a denigratory tone in that it referred to Mr Kumar’s valid disclosures as “persistent”:
“Ms Wood compounds this at paragraph 33 of her witness evidence, where she explains whilst discussing the decision to disengage and the letter to Mr S [REDACTED] that ‘This was particularly so against the background of the persistent emails to Mike about the use of SAS doctors and patients concerns…’ Ms Wood again refers to emails as part of the decision making process. These emails are protected disclosures 2-10.” [my emphasis]
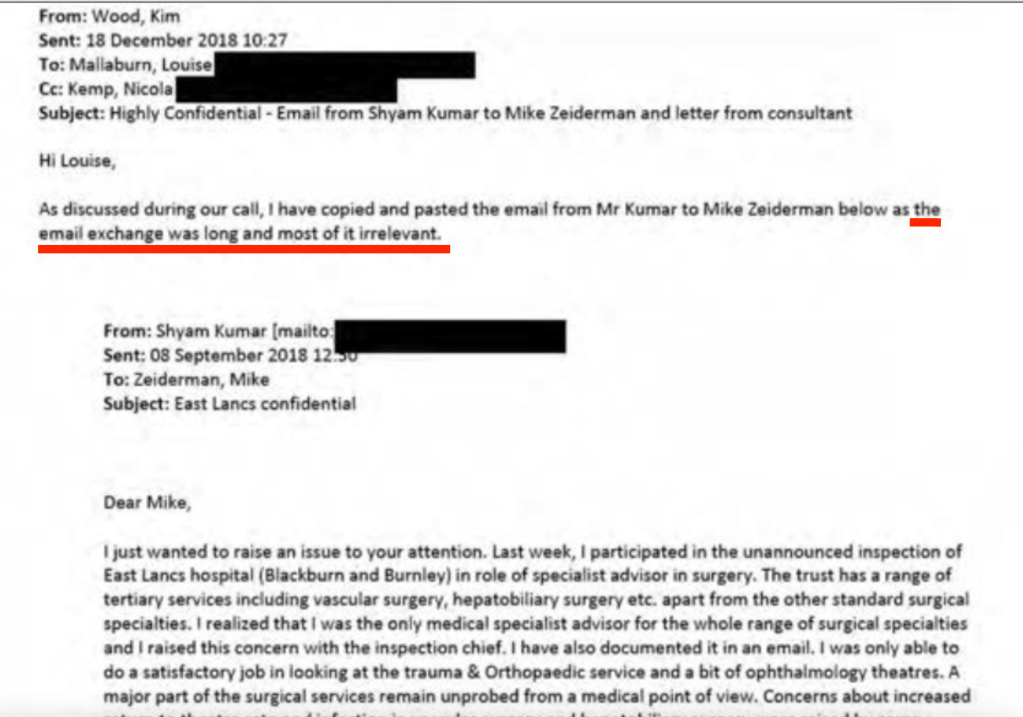
In one email thread, Kim Wood dismissed correspondence from Mr Kumar as “largely irrelevant”.
The ET later concluded that this correspondence by Mr Kumar, which Wood had so casually dismissed, was NOT irrelevant but were protected disclosures:
“The emails forwarded by Ms Wood were relevant and played a central role in this decision to disengage the claimant from his role with the respondent. The emails contained in this email were:
a. The 08 September 2018 email from the claimant to Mr Zeiderman (Protected Disclosure 7)
b. The 17 September 2018 email from the claimant to Mr Zeiderman (Protected Disclosure 8)
c. The letter of 29 November 2018 (wrongly dated as August) that Mr S [REDACTED] had sent to Ms Wood.”
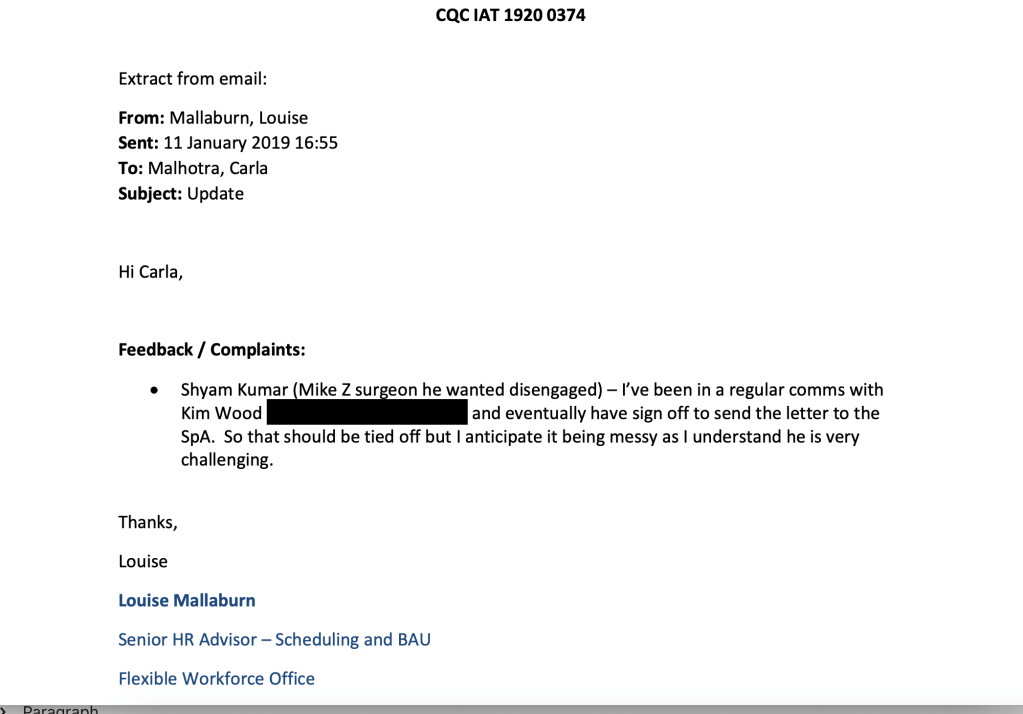
The dismissive and disrespectful attitude is echoed in later emails by Louise Mallaburn CQC Senior HR Advisor who wrote that Mr Kumar was “very challenging” and in another email made a sarcastic comment about him writing long emails.
The unfair dismissal by CQC
In November 2018 a CQC inspection took place at UHMBT, Mr Kumar’s trust.
Mr Kumar wrote to Kim Wood CQC inspector to express concerns that one of his persecutors at the trust, Dr S, might make inappropriate and damaging comments about him during the inspection.
This proved to be a realistic fear as Dr S did indeed make false and highly damaging claims about Mr Kumar during a CQC focus group.
The ET noted that Dr S’s remarks were inappropriate in that forum:
“In this meeting, Mr S [REDACTED] raised a number of issues which the Investigating Manager, Ms Helen Vine, considered were not appropriate for the Focus Group.”
The ET found that Mr Kumar was entitled to feel upset and injured by the serious attack on his character, probity and standing:
“The matters raised by the claimant, in his letter to Mr S [REDACTED], were serious issues. The claimant, if these matters were true, had the right to feel upset, in particular with the matters that were probity matters or race. All involved in this case accept that allegations concerning probity, bias and racism are serious matters and could have impacted on the claimant’s fitness to practise.”
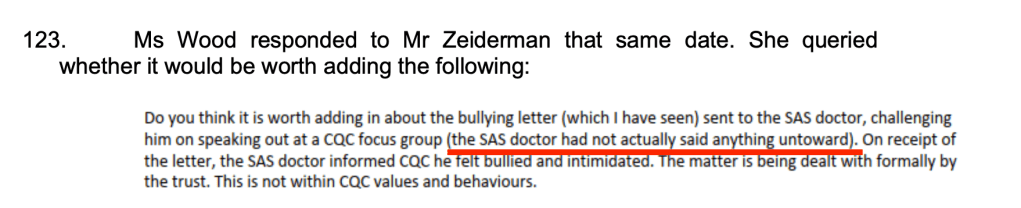
Extraordinarily though. Kim Wood later wrote to Mike Zeiderman on 6 May 2019, when they were deciding how to respond to a request for information by the CQC Chair’s office, that Dr S had not said “anything untoward”.
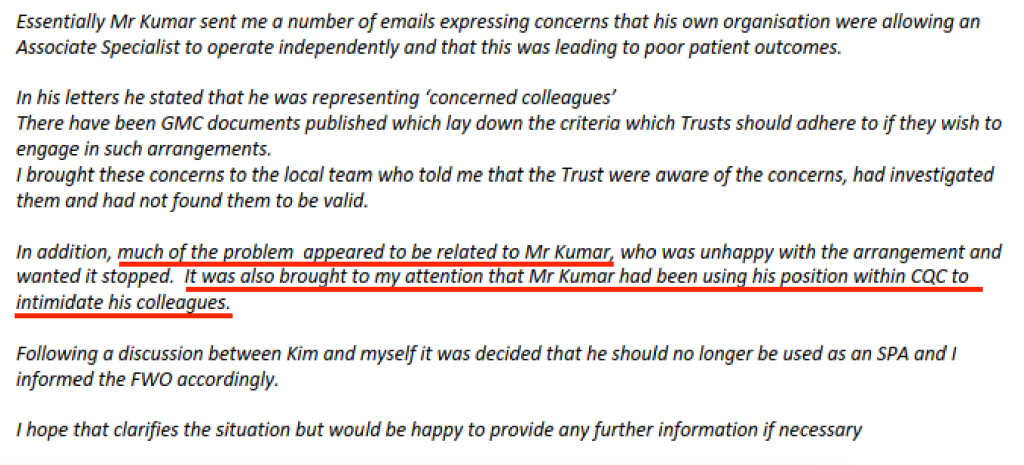
On the same day, Mike Zeiderman’s drafted a response to the CQC Chair, which cast Mr Kumar as the problem and undermined his credibility as a whistleblower:
This dismissal of Mr Kumar’s experience of whistleblowing reprisal contrasted with the CQC’s over reaction to counter-claims by Dr S.
After the above CQC focus group, Mr Kumar wrote a letter to Dr S with advice from the BMA, setting out his concerns about Dr S’s conduct. He proposed steps for resolution. The ET accepted that this was a good faith attempt to resolve the matter
“The letter sent by the claimant to Mr S [REDACTED] was an attempt to resolve matters informally, before making any decision as to whether to pursue a formal process. This is in line with the policies and procedures adopted by both the respondent and the employing Trust. We accept the claimant’s evidence on this, which is consistent with the wording in the letter that he sent to Mr S [REDACTED], in which he is seeking to resolve the situation. This is also consistent with the approach the claimant took after this letter was sent.”
However, the CQC seized on the fact that Mr Kumar had written a letter to Dr S as a means of dismissing him.
This is correspondence in which Mike Zeiderman instructed HR to sack Mr Kumar and informed Kim Wood of the sacking:
CQC’s line of attack thereafter focussed on a vague claim that Mr Kumar’s letter to Dr S proposing a resolution was in fact improper and a breach of CQC’s values.
CQC maintained this line of attack throughout the ET proceedings. During the June ET hearing, which I attended via web link, CQC’s witnesses made much of Dr S’ alleged response to Mr Kumar’s letter. The CQC contended that the definition of bullying includes the “victim’s” experience and it claimed that Dr S was so distressed by Dr K’s letter that the letter should be viewed as bullying.
The ET did not accept this.
In his evidence to the Employment Tribunal, Mike Zeiderman said that he had seen the letter from Mr Kumar to Dr S, before sacking him.
Damningly, the ET did not believe this:
“102. On balance we find that before 06 December 2018, Mr Zeiderman had not seen the letter that the claimant had sent to Mr S [REDACTED]. Although Mr Zeiderman in his oral evidence said he had seen the letter, the evidence before the tribunal suggests on balance that he did not see it by this date.“
That is, the central reason claimed by the CQC for dismissing Mr Kumar – his letter to Dr S – had not even been examined by Zeiderman at the point of the decision to dismiss Mr Kumar.
The ET determined that CQC’s dismissal of Mr Kumar was a “forgone conclusion” and therefore unfair.
“Disengaging the claimant was a foregone conclusion at the point the claimant was informed that he was placed on hold, and in those circumstances it is not plausible that it is a neutral act.”
The ET considered that Mr Kumar had been sacked by the CQC because he had whistleblown:
145. Given our findings above, it is very clear that the emails and concerns raised by the claimant in the form of protected disclosures had a material influence on the decision to disengage him. Amongst other reasons, this is particularly because of:
a. The reasons provided by Mr Zeiderman for disengaging the claimant appeared to develop throughout the period between the decision to disengage him on 06 December 2018 and his correspondence Mr Matt Wood from the Private Office Correspondence Unit, and into these proceedings. This and the lack of reference to the alleged offending letter to Mr S [REDACTED] a form the claimant, casts great doubt on that being the reason for disengagement and placing on hold of the claimant.
b. The correspondence with the claimant disengaging him provides little in terms of explaining in what way his behaviour fell below the expected behaviours or values of the respondent. And there was no detail as to what in the letter from the claimant to Mr S REDACTED] offended those principles. This again casts doubt on this being the sole reason, with other matters being trivial in the decision making process, for the decisions made.
c. During the phone call between Mr Zeiderman and Ms Wood in early December 2018, when Mr Zeiderman formed the view that the claimant could no longer be used as a special advisor, the claimant had at the forefront of his mind the emails which he had received from the claimant over the course of 2018. The emails that he is referring to include a number that are protected disclosures, or more specifically Protected Disclosures 2-10.”
The Tribunal determined that the CQC made no proper and reasonable investigation prior to dismissing Mr Kumar and that it failed to protect him as a whistleblower:
“Alongside this, this tribunal is mindful that this is a case where the claimant was being disengaged for having conducted himself in a manner not befitting of the respondent, without any proper and reasonable investigation. Where his professionalism was being questioned, and his action, which was later used as the reason for disengagement was in response to that. Where he had made the decision-makers aware of potential retaliatory action against him, and no safeguards were put in place. Against this backdrop, the decision to disengage him clearly reaches the level of detriment.”
CQC dismissed Mr Kumar without an appeal process, claiming that its policies allowed it to sack him without appeal, and that this was CQC’s normal practice.
The ET considered that this was unreasonable employer behaviour, and a detriment.
Thus it follows that the CQC is operating an oppressive employment practice, which takes no heed of natural justice.
CQC dug for dirt
One of the most extraordinary aspects of this case is that CQC sought to retrospectively justify its arbitrary and unfair treatment of Mr Kumar by placing pressure on his employer (University Hospitals Morecambe Bay NHS Foundation Trust, UHMBT) to give it dirt on Mr Kumar.
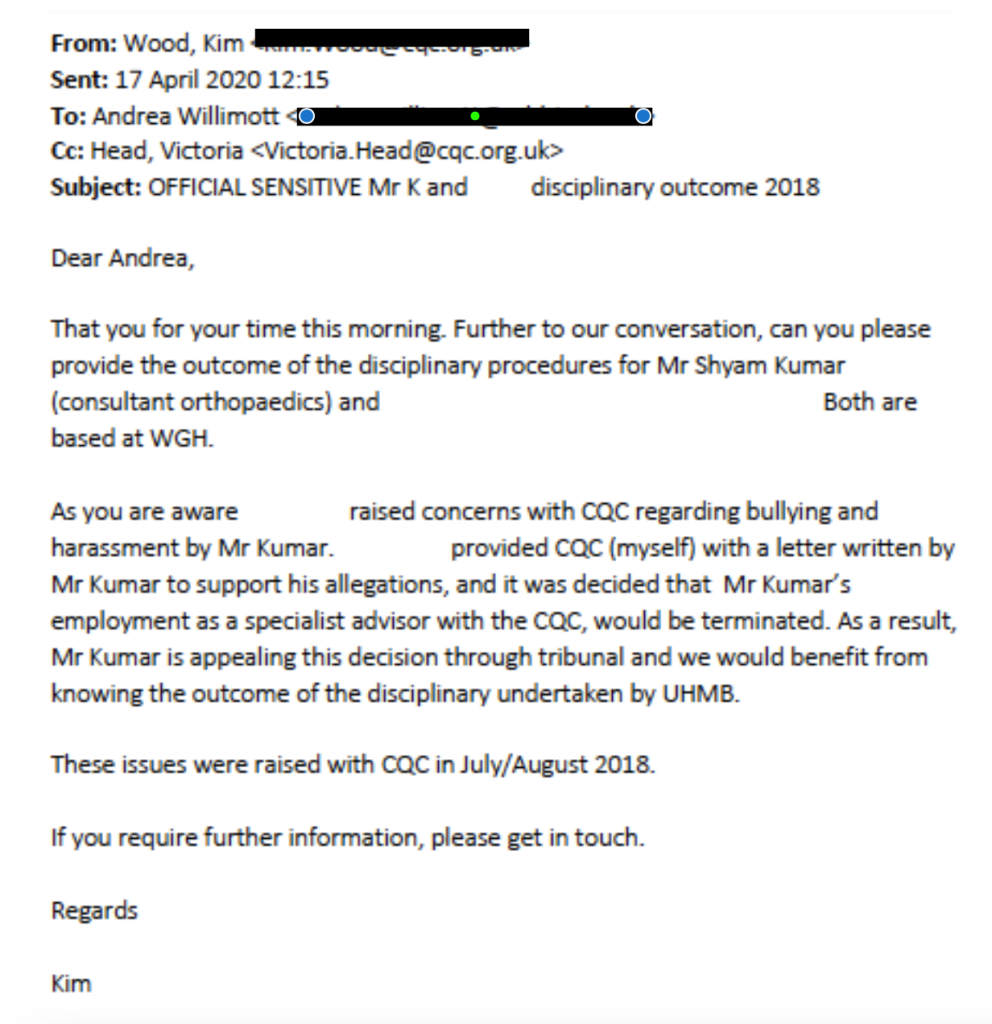
After Mr Kumar filed an ET claim against CQC for whistleblower detriment, the CQC asked UHMBT for information about UHMBT’s disciplinary action against Mr Kumar for his letter to Dr S, when no such disciplinary action ever took place.
The Victoria Head copied into this email is a CQC Inspection Manager, working on CQC’s Maternity Inspection Programme
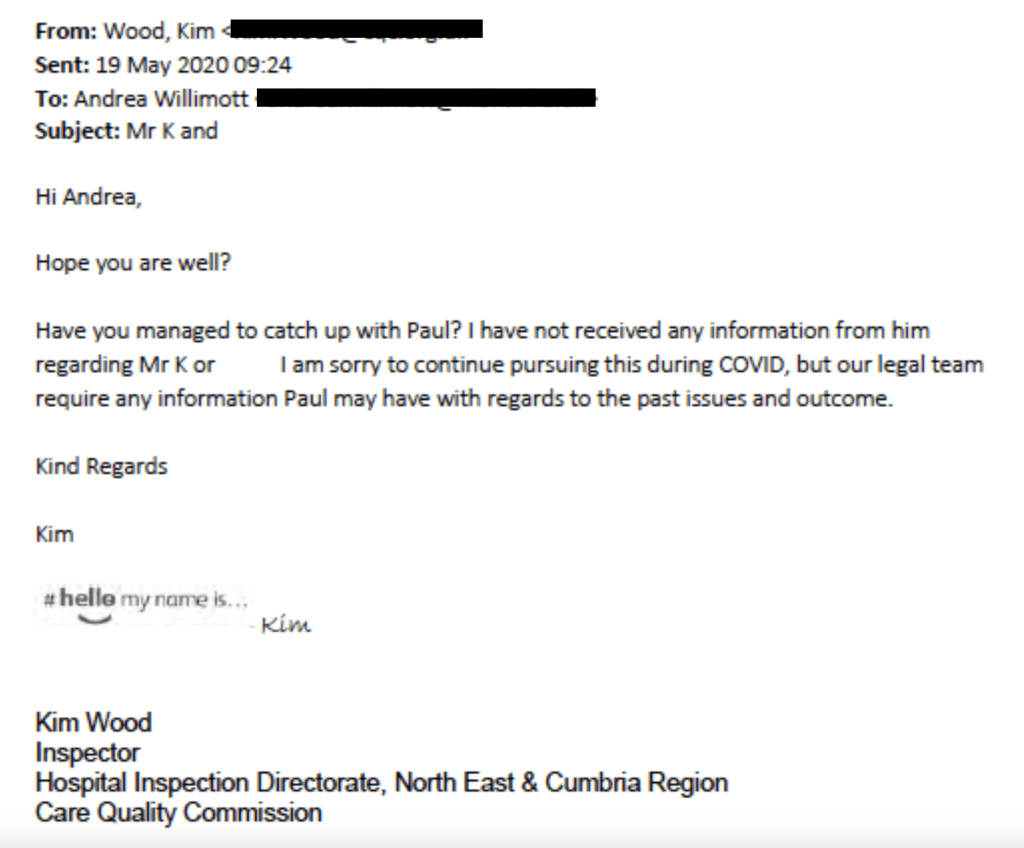
A month later, Kim Wood pursued UHMBT staff for “past issues” about Mr Kumar that could be useful to CQC’s lawyers:
In fact, the ET noted that Dr S, for all the CQC’s protestations of injury on his behalf, never even filed a grievance against Mr Kumar.
The fact that the regulator would ask a regulated body for information that was outwith the regulatory process, and was in fact requested for self-serving reasons, seems a most serious matter.
Especially when that purpose is to retrospectively justify the regulator’s poor treatment of a whistleblower.
This seems to me to be a gross abuse of power.
It would be for a lawyer to opine on whether it amounts to Misconduct In Public Office.
The CQC makes false counter-allegations against whistleblowers
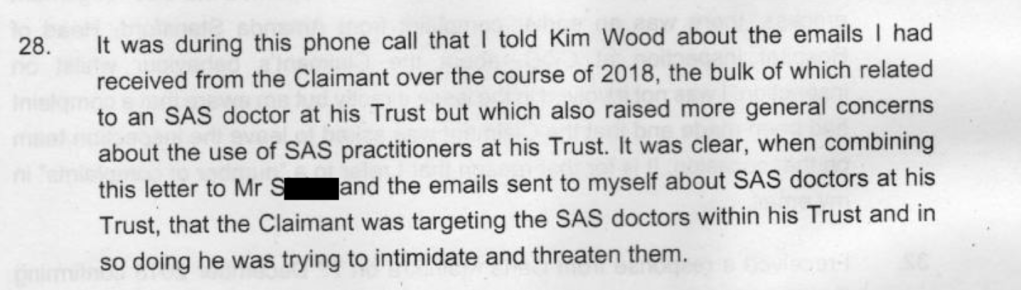
As part of its defence strategy against Mr Kumar’s claim to the Employment Tribunal, the CQC sought to portray his whistleblowing about the unsafe practice of a single doctor as an attack on all the SAS (non-consultant grade) doctors at his trust, for potential financial gain.
Mike Zeiderman’s witness statement to the Tribunal repeatedly claimed that Mr Kumar was “targeting” SAS doctors because some were allowed to work autonomously.
Zeiderman accused Mr Kumar of abusing his position as a CQC Specialist Advisor to intimidate others. Almost no particularisation was given of this alleged intimidation or the basis of the accusation.
Zeiderman’s witness statement claimed that a motive for attacking SAS doctors might be that their work to reduce waiting lists affected on the private income of consultant surgeons, as waiting lists encouraged patients to seek private treatment.
There was no basis for this suggestion that Mr Kumar might benefit financially. Dr X was helping to reduce trust waiting lists for LOWER limb cases such as hip and knee replacements. Mr Kumar is an UPPER limb surgeon.
But such a serious allegation about a doctor’s probity would normally require a fellow doctor to refer the individual to General Medical Council, as part of their professional obligations to safeguard patients. The CQC did NOT refer Mr Kumar to the GMC, despite Zeiderman stating clearly in his witness statement that CQC sacked Mr Kumar for reasons of probity:
Moreover, Louise Mallaburn repeated untrue claims about Mr Kumar in correspondence, which were very harmful to his reputation. The false claims are highlighted below:
This is correspondence from Mr Kumar’s trust, UHMBT, which confirmed that there had never been any such record of bullying and harassment on his file:
The false allegation by Louise Mallaburn in her email of 8 January 2019 that Mr Kumar was not often used by the CQC because he had previously been found to be “unsuitable”, was later echoed in Mike Zeiderman’s witness statement of 30 October 2020. In this statement, Zeiderman claims Mr Kumar was asked to leave a CQC inspection [in 2015]. This was false because it was Mr Kumar who made a complaint about Amanda Stanford’s conduct,, AFTER the end of the 2015 inspection.
The CQC doesn’t act on whistleblowers’ concerns
Mr Kumar has never received a satisfactory response from the CQC regarding the whistleblowing concerns that he raised with Mike Zeiderman and subsequently with other senior CQC managers.
This is an email of 16 May 2019 by Mr Kumar to the CQC noting this failure:
Months later a letter by the CQC Chief Executive to the Secretary of State in August 2019 conceded that the CQC had yet to address all of Mr Kumar’s concerns:
“I will ensure that where any of Mr Kumar’s concerns remain outstanding we address those as soon as possible.”
The CQC does not apologise or back down
More serious than an original failure are failures to learn and to take responsibility.
CQC directors rejected Mr Kumar’s complaint about his mistreatment. They stood by their man, Mike Zeiderman.
The final letter from CQC, sent by Ted Baker Chief Inspector of Hospitals, dismissing Mr Kumar’s complaint is painful to read:
By August 2019, CQC PR staff conferred on what “line” to take in explaining CQC’s conduct to Matt Hancock, then Health Secretary:
The CQC informed the Health Secretary that Mr Kumar had been dismissed because of poor behaviour. The regulator through its Chief Executive Ian Trenholm confirmed Mr Kumar had been expected to inspect areas where he was not expert, but it denied that there was anything wrong with its inspection methodology. This was despite CQC’s own National Professional Advisor Mike Zeiderman stating in his ET witness statement that he agreed with Mr Kumar that Specialist Advisors should not be asked to inspect areas in which they were not expert, and that this was an acknowledged problem nationally on which the CQC had been working.
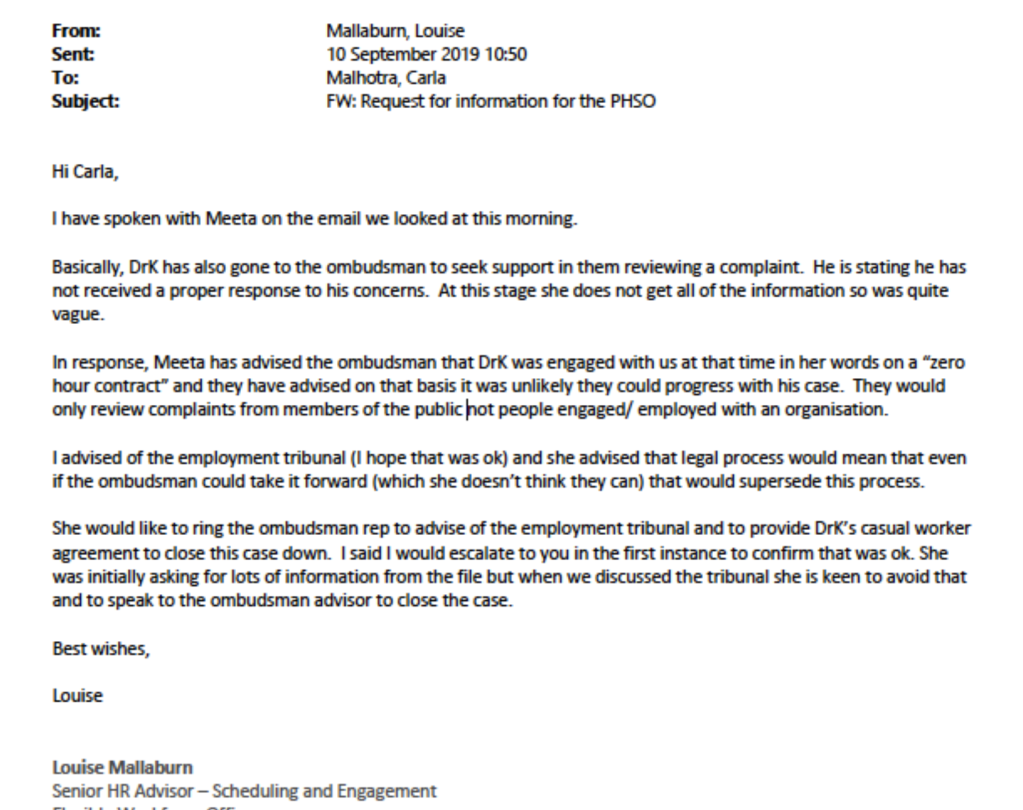
Mr Kumar complained to the PHSO about his treatment by the CQC: The CQC fed false information to the PHSO about Mr Kumar being on a zero hours contract.
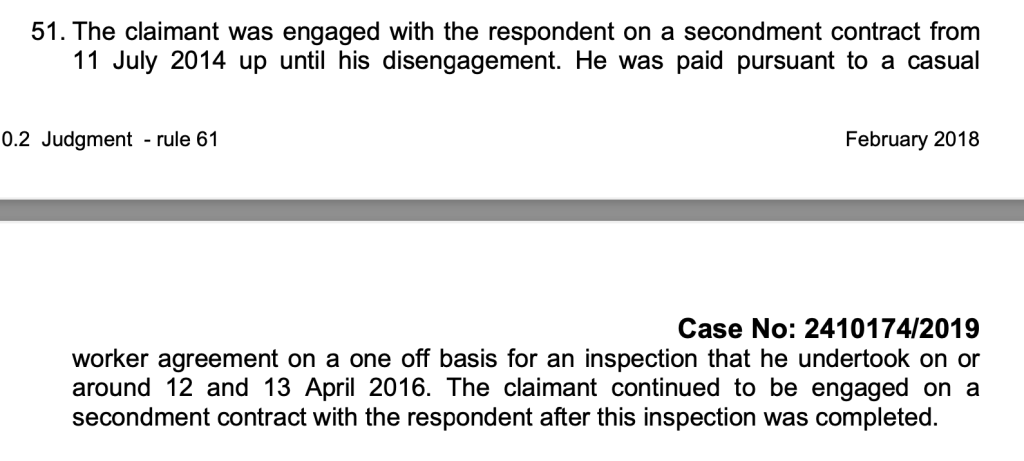
Mr Kumar was in fact on a secondment contract, as determined by the ET.
Failed to accept that his whistleblowing was valid, minimised his concerns and saw the whistleblowing as a nuisance and a threat
Mistreated the whistleblower seriously and smeared him
When challenged by the whistleblower sought to portray him as a difficult and “challenging”, and ridiculed his claim of whistleblower reprisal by the CQC
Tried to dig dirt about the whistleblower to retrospectively manufacture a case justifying its mistreatment, abusing regulatory power in the process
Fed false information to the Ombudsman to shut down a legitimate complaint by the whistleblower about his mistreatment by the CQC
Claimed reasons for its treatment of the whistleblower which were not believed and were rejected by the ET, calling into questions the truthfulness of the claims
Operated oppressive HR policy and practice, but foolishly and incompetently maintained up to the last minute that its processes were fine.
I asked the CQC press office to comment on whether it believes it has anything to learn from Mr Kumar’s case, and whether the CQC personnel involved in these serious governance failures should continue in CQC’s employ and hold responsibility for vulnerable patients and service users. I received no reply. I then asked the new CQC Chair Ian Dilks to comment, and have not so far received a reply.
One also has to wonder, if the CQC as an organisation would have been quite so blind to Mr Kumar’s professional credentials and standing, and his professionalism in standing up for patients, or treated him so contemptuously, had he been a Caucasian doctor.
Although the CQC vilified him and caused Mr Kumar and his family so much hurt, it seems clear that he has done all whistleblowers, especially Health and Social Care whistleblowers, and the public a great service.
Will anyone be disciplined or sacked for the harm to Mr Kumar as a whistleblower and the harm to the public interest?
Mr Kumar and his BMA representative asked the then NHS National Freedom To Speak Up Guardian Henrietta Hughes to review the issues raised by his case, but no case review has ever materialised.
But then, why would the National Guardian seek to challenge her employer, the CQC?
That would take the courage of a whistleblower.
I have asked Steve Barclay the Health Secretary to protect Mr Kumar and his family from further trauma and to prevent a wasteful appeal against the ET judgment by the Care Quality Commission, an arms length body of the Department of Health and Social Care.
Appendix: CQC dramatis personae
These are individuals at the CQC who either took an active part in handling Mr Kumar’s case or were party to the case from being copied into correspondence.
This is press coverage from July 2022 of Mr Kumar’s evidence to the ET about bullying culture at the CQC, and his complaint about Amanda Stanford’s conduct:
In keeping with the grand traditions of the NHS, Amanda Stanford’s Airedale NHS Foundation Trust biographical profile states:
“Amanda has an active interest in developing compassionate leadership, quality improvement and how education and training and creating a just and learning culture.”
I have written to Steve Barclay Health Secretary to ask that he ensures Mr Kumar’s concerns about the CQC are properly addressed, and that he ensures that the CQC will not appeal against the ET judgment and inflict further suffering on Mr Kumar and his family.
I have written to the BEIS Secretary about serious failure of the ramshackle system of “Prescribed Persons” under flawed UK whistleblowing law, arising from Mr Kumar’s case and others. Prescribed Persons such as the CQC have minimal legal duties and are too often complicit or directly responsible for harm to whistleblowers.
This means that large swathes of the NHS workforce will be apprised of the regulatory failure and forewarned about CQC’s unreliability as a Prescribed Person.
In the current political and regulatory landscape, I advise whistleblowers to consider whistleblowing directly to the media, either on an anonymous basis or with protection of identity. Take careful advise before doing so, as there are legal tests to fulfil if you wish to maintain protected status under current UK whistleblowing law.
UPDATE 9 SEPTEMBER 2022
CQC has responded briefly only to the media breaking the scandal of Mr Kumar’s case. It claimed in correspondence and through a media statement that it had already learned lessons and made improvements. However, it provided little evidence of these claimed improvements.
Today, it responded to an enquiry that I made about learning lessons and whether those implicated in Mr Kumar’s whistleblower victimisation should remain in the CQC’s employ, and in positions of public trust.
The CQC response today was brief and minimal but of note, referred in the future tense to learning lessons from Mr Kumar’s case:
“We accept the findings of the Employment Tribunal and will consider lessons to be learned from the judgement.” (my emphasis)
UPDATE 13 SEPTEMBER 2022
On 12 September 2022 the Health Service Journal provided further coverage of Mr Kumar’s case, in which it highlighted the Employment Tribunal’s findings on evidence by Mike Zeiderman, CQC National Professional Advisor:
“The unimpressed tribunal judge, meanwhile, said Mr Zeiderman’s explanation for terminating the contract “appeared to develop” in the months after his decision “and into these proceedings”.
HSJ also drew attention to the fact that the ET revealed Mr Kumar’s trust had “hidden” evidence of serious patient harm:
Ian Trenholm CQC CEO: “Thanks very much Ian, this I think Jade is referring to the recent case involving Mr Kumar. Just for clarity we’re not appealing that judgment and I have no intention of doing that. I think it is worth saying we have very few Employment Tribunal cases. In the round, we have a handful at any one time and very few of them actually proceed to a Tribunal. I think it would be difficult for us to make a blanket statement that we were never going to appeal an ET but but U think it is something that would be really very much by exception. So I think it is something we take very seriously. Thank you for the question Jade. Thank you.”
Ian Dilks CQC Chair: “[Inaudible first few words]….it links to the public purse that is something we have to take account of. That means we have to look into each case on its merits rather than making blanket statements about what we would do.”
PETITION
Please click and add your signature to this petition to reform UK whistleblowing law – whistleblowers protect us all but weak UK law leaves them wholly exposed, lets abusers off the hook and it is a threat to public safety.
This is not the first time by far that seconded CQC Specialist Advisors have criticised CQC’s poor inspection methodology and chaotic approach.
I know of doctors who tried the role but resigned due to the problems described by Mr Kumar in his disclosures to the CQC.
Hugh Cannell a former CQC specialist advisor committed his experiences and concerns to paper, in this article of 2019, thus contemporaneous with Mr Kumar’s struggles with the CQC:
Dr Minh Alexander retired consultant psychiatrist 2 September 2022
An Employment Tribunal found on 15 August 2022 that Dr Al-Jehani was unfairly dismissed and subject to a number of detriments by the Royal Free NHS Foundation Trust because she had made protected disclosures in the public interest:
The story is complex and I am unable to do it justice at present, but am briefly posting to share the ET outcome as it appears to be a very serious matter of NHS probity.
Dr Al-Jehani was employed as biomedical scientist by the Royal Free, with an honorary contract with University College London (UCL). She worked for the trust, but was based at UCL’s Institute for Liver and Digestive Health.
She became concerned that human tissue was being diverted into for-profit activities by fellow researchers at UCL, some of whom she alleged had conflicts of interest and held shares in the commercial venture which she believed were benefiting from this diversion of human tissue.
The company named in the ET judgment as the focus of Dr Al-Jehani’s concerns was Engitix, which is listed at Companies House:
Extraordinarily, UCL conducted three separate strands of investigation in response to her concerns – research misconduct, poor human resources practice and financial impropriety – but with a plan agreed with the Royal Free to withhold the fact that the UCL investigations were completed, and their findings, from Dr Al-Jehani.
In the meantime, the Royal Free moved to dismiss her through redundancy. The trust’s managers left a trail of correspondence which showed that they wished to remove her as soon as possible, as they considered her a “thorn in the side”.
The ET concluded that it had no jurisdiction over Dr Al-Jehani’s claims against UCL because the claims were made out of time.
But a very serious question mark clearly hangs over UCL’s part in the matter.
The ET determined that Dr Al-Jehani’s concern that a cover up had taken place was a protected disclosure and that her belief was reasonable in the circumstances.
It also concluded that the Royal Free NHS Foundation Trust’s detrimental actions against Dr Al-Jehani were motivated by self-interest. Namely, a desire to stay on good terms with UCL, and to protect the powerful:
“Furthermore, the fact that the Claimant was kept in the dark about the outcome of UCL’s investigations into her complaints, and that was on specific instructions of RK [Robert Kleta, Director of the Division of Medicine, UCL with clinical appointments as Honorary Consultant in Paediatric Nephrology (Great Ormond Street) and Renal Medicine (Royal Free)](who was meant to be acting as a complainant on behalf of the Claimant, and therefore in her interests), is another important piece in the jigsaw.”
“The picture that emerges shows that the Claimant’s protected disclosures ruffled a few important feathers at UCL, nobody at UCL wanted to deal with the Claimant and wanted her out of sight as soon as possible.”
“The Trust was not going to stick up for the Claimant. Instead, it wanted to solve the problem by finding a way of getting the Claimant out of ILHD [UCL’s Institute for Liver and Digestive Health ]as soon as possible. The paused redundancy process was the most convenient vehicle to achieve that”.
The ET agreed with Dr Al-Jehani’s contention that the redundancy exercise by the trust was a sham:
“The fact that Patricia Blake was first included in the pool, but then removed by DT [Douglas Thorburn] under the pretext that she was included in MP’s [ employment package, with rather dubious evidence in support of that (see pp 1776 and 238), gives us further grounds to infer that the main purpose of the resumed redundancy exercise was to remove the Claimant’s role from ILDH as soon as possible. rather than to achieve financial savings.”
The Employment Tribunal rejected the evidence of several trust managers, which it did not believe.
The Royal Free decided not to call a key witness, Douglas Thorburn (“DT”), Clinical Director for Hepatology and Liver Transplant. He had written an email of 24 July 2019 about dismissing Dr Al-Jehani as follows:
“Hi Robert& Massimo, I’m away at present. I spoke with our ops manager mon evening before I left. Because we had started looking at termination of her role (and one other RFH funded post in ILDH- Sheri-Ann) before she put in her initial complaint we are at liberty to progress the case for redundancy or relocation. (Indeed all her actions have likely been prompted by her recognising her position was at risk…….). The case is in hand and will be submitted for approval shortly (I understand this or next week). Given the problems created it is highly likely/certain it will be approved and the issues will cease. I’m sorry that in the meantime she remains a thorn in the side but I believe this is best just tolerated in the knowledge she will be gone soon. I’ll check in with Lee re anticipated time scales.”
The ET reasoned:
“375. DT writes in that email: “Because we had started looking at termination of her role (and one other RFH funded post in ILDH- Sheri-Ann) before she put in her initial complaint we are at liberty to progress the case for redundancy or relocation. [..] The case is in hand and will be submitted for approval shortly (I understand this or next week). Given the problems created it is highly likely/certain it will be approved and the issues will cease. I’m sorry that in the meantime she remains a thorn in the side but I believe this is best just tolerated in the knowledge she will be gone soon. I’ll check in with Lee re anticipated time scales.” DT could not be any clearer. He wants the Claimant out and because there is that paused redundancy process, which had started before the claimant blew the whistle, the matter can be progressed and the rest will be mere formality.
376. In our judgment, that was effectively the decision to dismiss the Claimant. It was taken by DT. The principal reason for which he took that decision was “the problems created” by the Claimant by making the protected disclosures. The rest was just a matter of executing on the decision. The HR Department was on board with the decision (NW writes in her reply – “We are following the process you have set out in your email.” – p.1877). LG, with assistance from SS, sets the wheels in motion.”
The ET concluded that Douglas Thorburn would have been a damaging witness for the Royal Free, on the following basis:
“Based on our findings of fact (see paragraphs 69-76) we find that the Claimant’s protected disclosures were the main factor in the Trust’s decision to resume the redundancy process. The email from DT [Douglas Thorburn] speaks volumes. The Trust decided not to call DT to give evidence to the Tribunal. NW confirmed in her evidence that DT was still an employee of the Trust. Therefore, the Tribunal draws an inference that DT’s evidence to the Tribunal would have been unhelpful to the Trust’s case, and DT would not have been able to give an alternative reasonable explanation to the apparent meaning of his email. On a fair reading, DT states that the problem of the Claimant being “a thorn in the side” will be solved through redundancy. The redundancy case will almost certainly be approved (given the problems the Claimant had created), and it is just a matter of time to let the process run its course while tolerating the Claimant “in the knowledge she will be gone soon”.
The ET noted that Patricia Rubin claimed that UCL’s investigations were sound, but when questioned by the ET about this, Rubin was unable to give reasons. She also admitted that the appeal panel did not look into a grievance by Dr Al-Jehani (which the ET reported had been sent to the Site Chief Executive Officer Kate Slemeck).
“The letter concluded by saying: “On the matters related to your speaking up concerns, your treatment as outlined in your grievance, the panel is confident that UCL have fulfilled its legal obligations to ensure speaking up concerns and grievances are appropriately investigated in accordance with their own regulatory requirements and internal procedures”.
116. I asked Ms Rubin what gave the panel that confidence. She was not able to provide any satisfactory answer. She was also not able to explain on what basis the panel “noted” that the Claimant did not appeal the speaking up/grievance outcome, when the former waskept secret from her for over a year and UCL’s grievance letter said that she had no right of appeal. It is even more surprising considering Ms Rubin’s admission in cross-examination that the panel did not look into the Claimant’s grievance.”
“…Ms Rubin’s evidence was highly unsatisfactory. While she maintained that the Claimant’s whistleblowing had nothing to do with the panel’s decision to refuse the Claimant’s appeal, she could not properly explain on what basis the panel made its decision (see the Tribunal’s findings of fact at paragraphs 113-116 above).
349. Furthermore, Ms Rubin accepted in her evidence that the panel did not consider any alternatives to the dismissal. She was not even certain whether the appeal had the power to reinstate the Claimant. She could not say what the Claimant could have said or done at the appeal meeting to avoid the dismissal. She later said that the Claimant could have presented new evidence.
350. However, the Claimant did present evidence (not least by telling the panel why she considered her complaints had not been properly dealt with), but the panel chose not to investigate them and instead roundly dismissed them on the basis of the panel being “confident that UCL have fulfilled its legal obligations to ensure speaking up concerns and grievances are appropriately investigated in accordance with their own regulatory requirements and internal procedures”. Ms Rubin was unable to explain on what basis the panel came to that decision”
“312. Looking at the subsequent steps in the process: – SS telling the Claimant that it would be better for her wellbeing to leave ILDH, failure to deal with the Claimant’s February 2020 grievance, and the haste with which the Claimant was eventually dismissed after UCL had sent its letter of 10 June 2020 (and that is despite the 3 months hold on redundancies), we are drawn to the conclusion that the real reason why the Trust had decided to resume the process was to eventually get rid of the Claimant because she had made herself a persona non-grata at ILDH and created unwelcome problems for UCL and the Trust by blowing the whistle on what the Claimant considered to be illegal practices at ILDH.”
The Actions and Omissions of the Royal Free Freedom to Speak Up system
The trust Freedom To Speak Up Guardian Jim Mansfield Unison Staff Side Chair was informed of Dr Al-Jehani’s whistleblowing disclosures in November 2017 and he and the Workforce Director met with her:
“The Claimant’s complaint contained, inter alia, allegations that: (i) tissues samples at TAPb were being used by those who controlled access to it for commercial profit in preference to scientific non-for-profit research, (ii) there was a conflict of interest because AG needed to raise at least £8,000 a month from tissue samples in TAPb to keep his job, (iii) to obtain patients’ consent to donate liver organs GM [Giuseppe Mazza] impersonated a medical doctor, (iv) AG [Amir Gander] attempted to get non-English speaking patients to sign consent forms in English, and (v) donors when signing the consent form did not know that their organs would be used for commercial profit and not for medical research.”
“On 19 January 2018, Natalie Ware (“NW”), Head of Workforce for the Trust’s Hospital Business Unit, and JM met the Claimant to discuss her complaints. NW and JM [Jim Mansfield Speak Up Guardian] asked the Claimant to gather further information on the matters she complained about.”
Dr Al-Jehani provided the Freedom To Speak Up Guardian and the Director of Workforce with information on several occasions.
Natalie Ware discussed Dr Jehani’s case with the trust Chief People Officer and the Chief Medical Officer:
According to the ET, the Freedom To Speak Up Guardian toed the trust management line of not telling Dr Al-Jehani that UCL’s investigations into her concerns had concluded and that her concerns were rejected by UCL.
The ET “preferred” Dr Al-Jehani’s evidence to that of the Freedom To Speak Up Guardian and the Director of Workforce. The ET expressed concern that neither the Freedom To Speak Up Guardian or the Director of Workforce took meeting notes, made records of meetings or sent a follow up email to Dr Al Jehani after meetings.
“On 17 December 2018, the Claimant had a meeting with NW [Natalie Ware] and JM [Jim Mansfield]. They did not tell the Claimant that the investigation had been concluded or what the outcome was. The Claimant remained unaware of that until her redundancy consultation meeting on 10 December 2019. On balance, the Tribunal prefers the Claimant’s evidence on this issue because it is supported by documentary evidence (see pp.1204, 1222 and 1225), which shows that as late as August 2019 the Claimant was operating under a misapprehension that the investigation into her complaints was still ongoing. It is also consistent with NW’s admission that she withheld the outcome report from the Claimant because RK had told her not to share it with the Claimant. It is striking that neither NW (being an HR professional) nor JM (being Speaking-up Guardian) took any notes at the various meetings they had with the Claimant, or made any file notes following the meetings, or sent any follow-up emails to the Claimant recording what had been discussed at the meetings.”
The Tribunal concluded that the Royal Free kept Dr Al-Jehani in ignorance, in concert with UCL, to disadvantage her and suppress her raising of concerns:
“The respondents did not call RK [Robert Kleta] to give evidence to the Tribunal to explain the reasons he told NW not to share the outcome of the investigation with the Claimant. Based on that and the evidence in front of us, the Tribunal draws an inference that RK wished the Claimant to remain unaware of the outcome of the investigation for as long as possible, so that steps could be taken to have the Claimant relocated away from ILDH (see p. 1878) without the Claimant first attempting to appeal the outcome of the investigation or otherwise escalating the matter, or making further complaints against UCL staff. This was discussed and agreed with the Trust (see pp.1877, 1878).”
The finding by the ET that the Royal Free’s Freedom To Speak Up Guardian “did not tell the Claimant that the investigation had been concluded or what the outcome was” illustrates yet again why the government’s Freedom To Speak Up project is fundamentally flawed.
It puts Freedom To Speak Up guardians who are subordinate employees in the impossible position of holding their bosses to account, when in reality this means that they must either risk victimisation for doing so, or they do what they are told, against the public interest.
It is a form of institutionalised bullying.
Dr Al-Jehani’s validated Protected Disclosures
The ET accepted the following as legally protected disclosures by Dr Al-Jehani.
Public Interest Disclosure 1
“209. She relies on various passages in her email in which she complains that her access to liver sample in the TAPb was being obstructed whereas GM [Giuseppe Mazza] and Prof Rombouts [Krista Rombouts Professorial Research Associate, Engitix shareholder] were able to obtain hundreds of whole livers from the TAPb, which then were being used for commercial purposes via Engitix.
210. The Trust does not accept that it was a protected disclosure. It states that the nature of the letter was the Claimant asking various questions (e.g. is it ethical?) rather than disclosing information alleging potential breach of the HTA. It also argues that it was the Claimant’s way of getting access to tissue samples, as the Claimant accepted in cross-examination.
211. We find that, read as a whole, the email does disclose information, as it contains sufficient factual information. The fact that the Claimant then poses various questions regarding the ethics and legality of the practices she complains about does not mean that the factual content of the email is not sufficient. It clearly identifies the facts, which the Claimant claims show inappropriate and potentially illegal behaviour.
212. We are also satisfied that the Claimant had a reasonable belief that the information she was disclosing tended to show a criminal offence, namely the use of human tissue contrary to the HTA and that she reasonably believed the disclosure was in the public interest. In concluding her email, she wrote: “I believe that it is in the interest of the NHS and the general public that the issues I have raised above are addressed immediately by the NHS or other appropriate body”.
213. Therefore, we find that PID 1 was a protected disclosure under s.43A ERA.”
Public Interest Disclosure 29
“222. Still in the same email of 22 November 2017 the Claimant stated that AG [Amir Gander] had tried to get non-English speaking patients to sign donor’s consent form in English and had asked the Claimant to translate it orally to the patients, which the Claimant had declined to do.
223. She claims that the information tended to show a criminal offence by reference to various sections in the HTA, and also a failure to comply with a legal obligation, namely various provisions in the Human Tissue Authority Code of Conduct E – Research (pp 217 – 218 of Appendices to PD table) – (“Code of Conduct E”).
224. The Trust does not admit that it amounted to a protected disclosure but does not make any further submissions.
225. We find that it was a protected disclosure. The relevant passage in the email contains sufficient factual information – GM [Giuseppe Mazza]approaching non-English speaking patients to sign consent forms in English and asking the Claimant to translate for him. The Claimant goes on to say that she told AG [Amir Gander] that to obtain a valid consent the form would need to be translated into Arabic, which AG said it was too complicated. However, the Claimant claims that subsequent to that conversation AG was caught approaching non-English speaking patients in the private wing of the hospital for consent. Therefore, we find that the Claimant reasonably believed that the information she was disclosing tended to show that AG was committing a criminal offence by attempting to obtain patients’ consent in contravention of the HTA. We also find that she reasonably believed the disclosure was in the public interest. Therefore, PID 29 was a protected disclosure.”
Public Interest Disclosure 49
231. The Claimant relies on her email of 12 February 2018 to JM [Jim Mansfield Speak Up Guardian] in which she states that she overheard a telephone conversation in which GM [Giuseppe Mazza] said to the person at the other end of the line (who the Claimant thought was a potential investor into Engitix) that he (GM) was able to source human tissue and that he had a team who were proficient in decellularizing all human tissue. GM also told the “investor” about his plants to travel to Japan and the USA to meet with other investors, and of GM’s plans to set up a human myofibroblast (a type of human cell) biobank.
232. The Claimant says that this communication contained information that tended to show “commercialisation of human tissue” which she says is a criminal offence under the HTA and also a failure to comply with a legal obligation under the Code of Conduct E.
233. The Trust does not admit that the email amounts to a protected disclosure and states that the nature of the content of the communication is the Claimant asking questions and it did not tend to show a criminal offence or a failure to comply with a legal obligation.
234. We find that it was a protected disclosure, when read in the context of the Claimant’s earlier 22 November disclosure. Essentially, the Claimant provides further information in support of her PID 1, which she reasonably believed tended to show that human tissue samples were being used for commercial purposes in breach of the HTA. We also find that she reasonably believed that the disclosure was in the public interest. Therefore, we find PID 49 was a protected disclosure.
Public Interest Disclosure 33
“227. Although listed under 22 November 2017, it appears the Claimant relies on her email of 13 April 2018 and the attachments, in which she alleged that MP [Massimo Pinzani] and GM [Giuseppe Mazza] had obtained ethical approval to use tissue from TAPb for domestic research only, however in their funding application they wrongly asserted that the approval covered commercial use, including abroad through Engitix.
228. She claims that information tended to show a criminal offence under the HTA, and also under s.2 of the FA, and that there was a failure to comply with a legal obligation under various paragraphs of the Code of Conduct E.
229. The Trust does not admit that the disclosure amounted to a protected disclosure and points out that if the alleged breach is of the Code of Conduct, that is insufficient.
230. We find that the communication was a protected disclosure. The Claimant includes the original application for human tissue by GM and MP for the organ regeneration project and the ethics approval letter and provides details, which she says, show that the ethics approval covered only domestic use, whereas the funding application represented that the ethics approval covered a wider use and that was a false representation contrary to the HTA. We also find that the Claimant reasonably believed that the disclosure was in the public interest. Therefore, PID 33 was a protected disclosure.”
Public Interest Disclosure 3
“273. The Claimant relies on her email of 31 May 2018 to JM [Jim Mansfield Speak Up Guardian] and NM [Natalie Ware], in which she wrote about a talk given at the Research and Development Open Day at the Royal Free Hospital. At that talk, AG [Amir Gander] and Dr Emma Lawrence, Engagement Director at UCL, talked about problems researchers face in accessing human tissue samples and how TAPb was facilitating access to samples. The Claimant asked a question about what percentage of donated organs were ended up being used by NHS. Dr Lawrence said that she did not have such information. The Claimant then asked whether they had information on recovery costs for procuring tissue samples. The answer was no. The Claimant then explained the difficulties she had with accessing sample at TAPb, and AG said that it was not the right forum to discuss these issues.
274. The Claimant claims that this email contained information, which in her reasonable belief tended to show that a criminal offence of using/storing donated materials for a non-qualified purpose, namely commercial profit contrary to s.8 HTA.
“281. The Claimant relies on the same email of 31 May 2018, in which she also wrote about her encounter with a PhD student, who she suspected was unwittingly exploited by GM [Giuseppe Mazza] and MP [Massimo Pinzani] for the benefit of Engitix and was not properly supervised. She wrote that she believed that the students were not being given correct guidance and training on ethical use of human tissue, HTA regulations, data protection and other governance and therefore “many of these regulations are being violated”.
282. She claims that in her reasonable belief the information tended to show criminal offences under the HTA and the FA, and a failure to comply with a legal obligation under Code of Conduct – E, the DPA and GDPR.
283. We find it was a protected disclosure. It contains factual information about the Claimant’s conversation with the student from which she discovered that the student was working on a project for Engitix. She makes assertions that the work was not properly supervised, and applicable regulations violated. Although those assertions are not supported by concrete evidence in that email, when read together with her earlier disclosures, in particular 1, 33, 39, 43, 49 and 75, we find that the Claimant did believe that the information provided tended to show likely violations of the relevant laws and regulations and in the circumstances that belief was reasonable. We also find that she reasonably believed that the information disclosed was the public interest. Therefore, it was a protected disclosure.”
Public Interest Disclosure 75
242. The Claimant relies on her email to JM [Jim Mansfield Speak Up Guardian] of 12 March 2018 in which she reported a serious breach of data protection. She wrote that she had discovered that GM [Giuseppe Mazza] had a folder labelled “human liver” which contained highly sensitive information related to NHS patients from whom human liver samples had been obtained and kept in TAPb and that folder was kept on a shelf in a shared office which many UCL staff and students had access to.
243. The Claimant claims that she reasonably believed the information tended to show that a criminal office had been committed under s.170 of the Data Protection Act 2018 (“the DPA”) (unlawful obtaining of personal data without consent) and a failure to comply with legal obligations under the DPA, the General Data Regulations 2016, Code of Conduct E and UCL-RFH BERC Guidelines.
244. The Trust does not admit that it was a protected disclosure but makes no further submissions.
245. We find that it was a protected disclosure. The email contained detailed factual information, the Claimant reported it as a serious data protection breach. We find that she reasonably believed that the information tended to show a failure to comply with a legal obligation under the data protection legislation and possibly a criminal offence. Given the likely number of patients (the data went back to 2014) whose highly sensitive personal data the Claimant thought was at risk, we find that she reasonably believed the disclosure was in the public interest. Therefore, we find PID 75 was a protected disclosure.”
Public Interest Disclosures 81/82
“287. The Claimant relies on paragraphs 282-305 in her 5 February 2020 grievance in which she complains that her complaints were not properly investigated, and the Screening Panel decision was a sham. The Claimant explained that she disagreed with the Panel’s conclusions because these were based on untrue submissions by the Individual Respondents, and because her complaints had been rejected without any proper investigation. She also complained that the Trust had failed to inform her of the outcome of the investigation despite knowing it from late 2018 or early 2019. She said it was a cover up.
288. The Claimant claims that these paragraphs in her grievance contained information, which in her reasonable belief tended to should concealment of criminal offences and failures to comply with legal obligations contained in her earlier disclosures.
289. The Trust does not admit it was a protected disclosure because it says it was “not disclosure of information tending to show…”
290. We find that it was a protected disclosure. The Claimant gives detailed factual information about what happened with her complaints and why she believes these have not been properly dealt with. She explains why she disagrees with the Screening Panel conclusions and why such conclusions could not have been reasonably made on the evidence presented if a due investigation process had been followed. She says that she believes it was a cover up. Her complaints that had been passed to the Screening Panel, as we found, contained protected disclosures falling within s.43B(1)(a) and (b). Therefore, we find that the Claimant did disclose information, which she believed tended to show that the matters she had complained about in protected disclosures had been deliberately concealed. In the circumstances we find that her belief was reasonable and that she reasonably believed that the disclosure of that information was in the public interest. Therefore, we find that PID81/82 was a protected disclosure.”
Some of Dr Dr Al-Jehani’s very serious concerns about wrongdoing did not meet the legal threshold of protected disclosures as they were suspicions which the ET considered did not constitute “reasonable beliefs”, but they are nevertheless sobering reading.
For example:
“On 22 May 2018, the Claimant sent further information to NW and JM, again raising the issues of GM keeping confidential patients’ data in the shared office and also making new allegations of inappropriate use of charity funds by a company called 3P, whose shareholders included GM and MP.”
The ET has taken the unusual step of attaching a list of the disclosures that Dr Al-Jehani relied upon, in Appendix 2 of the ET judgment.
This is the UK law which sets out the way in which use of human tissue is strictly controlled and creates criminal offences for breach of its requirements:
Amir Gander Tissue Access for Patient Benefit (“TAPb”) Manager
And of course, where would we be without the National Guardian’s cheery contributions.
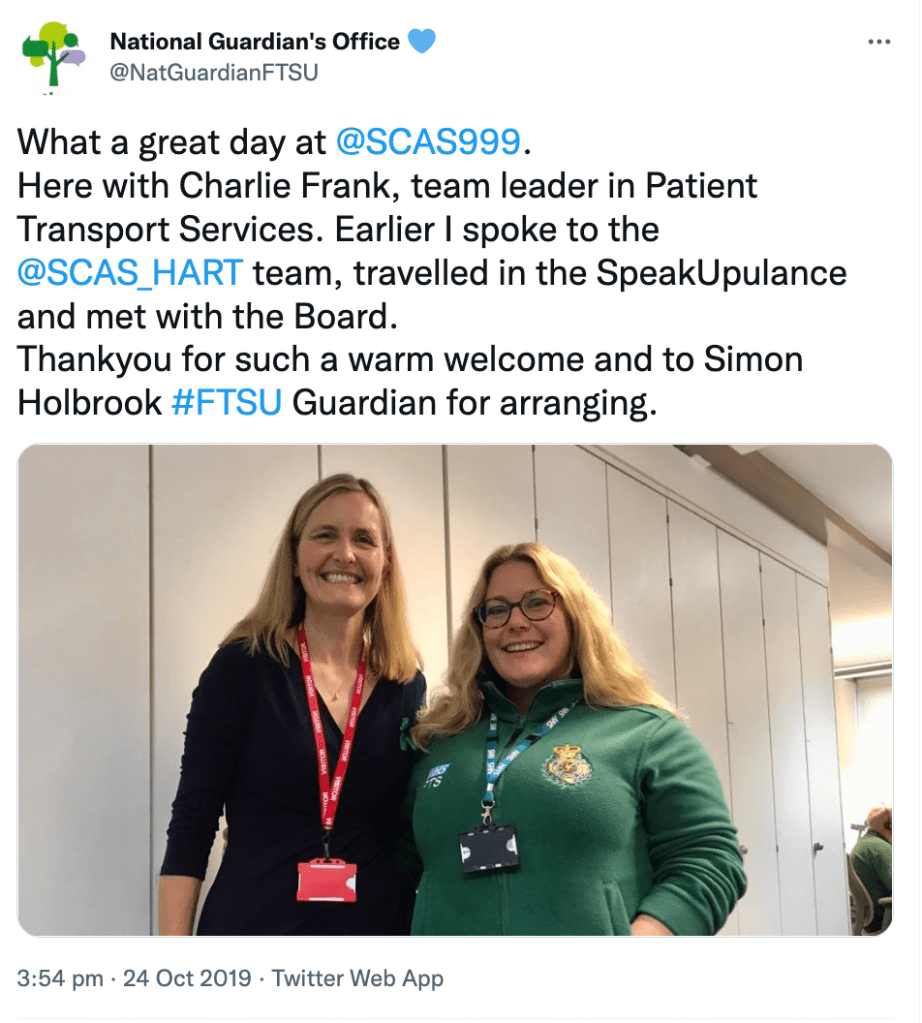
This is the former National Guardian Henrietta Hughes, featured in the Royal Free’s publicity material about Freedom To Speak Up in October 2019:“It’s your time to speak up”
UPDATE 3 SEPTEMBER 2022
I have written to the Health Secretary as follows about this matter and the general failure of the Freedom To Speak Up project:
BY EMAIL
Stephen Barclay
Secretary of State for Health and Social Care
3 September 2022
Dear Mr Barclay,
Serious failure of the NHS Freedom To Speak Up project, related waste and serious allegations about the Royal Free NHS Foundation Trust and the Human Tissue Act
The Freedom To Speak Up project, of installing employee “Guardians” at NHS trusts, with national leadership but not line management, by a National Freedom To Speak Up Guardian office without any powers, has failed.
The creation of this model of whistleblowing governance was expressly to
– prevent serious detriment to whistleblowers and destructive litigation
“Rare” was the goal defined by the report of the Freedom To Speak Up Review by Robert Francis:
“10.6 It will be important that progress is reviewed regularly. Culture change is not a one-off event,but requires constant attention and development. I believe that the widespread introduction ofFreedom to Speak Up Guardians, with a national point of reference created through the new postof the Independent National Officer, is a key component in keeping watch over the way concernsare handled, providing support to those who need it, and ensuring the patient safety issue is alwaysaddressed. The climate that can be generated by these measures will be one in which injustice to whistleblowers should become very rare indeed, but is redressed when it does occur.”
– protect patients from harm due to cover ups.
This has not been achieved. Seriously harmed whistleblowers, failed by the Freedom To Speak Up mechanism, continue to sue the NHS and their cases reveal gross patient safety/ abuse/ rights issues.
“Our analysis suggests that the role’s potential contribution might be understood less as supporting whistleblowers who bear witness to clear-cut wrongdoing, and more as helping those with lower-level worries to construct their concerns and what to do with them.”
In any case, all Freedom To Speak Up Guardians do in most cases is pass on concerns. They are not empowered to act as advocates, and any who do so are themselves harmed.
This is one of the latest examples of the model’s ineffectiveness:
Dr Al-Jehani’s proven case of unfair dismissal for whistleblowing is shocking in all respects, and it reveals that the Royal Free NHS Foundation Trust Freedom To Speak Up Guardian, along with senior trust manages, did not tell her investigations into her disclosures had been completed and had rejected her concerns. The Employment Tribunal concluded that the trust’s withholding of this information was done to disadvantage her, and suppress her raising of concerns.
Yet millions continue to be poured into the Freedom To Speak Up model.
But how can employee Freedom To Speak Up Guardians realistically hold senior trust managers to account or oppose their instructions?
Should the public purse really pay for an ineffective model that is so fundamentally flawed by conflicted interest at the heart of its design?
I would be grateful if you consider these matters and also if you could ensure a proper resolution of Dr Al-Jehani’s concerns about the Royal Free NHS Foundation Trust’s role in alleged breaches of the Human Tissue Act.
Dr Al-Jehani contended that there had been a cover up of her concerns and the Employment Tribunal determined that her belief about this was reasonable in the circumstances.
Yours sincerely,
Dr Minh Alexander
Cc Amanda Pritchard CEO NHS England
UPDATE 7 SEPTEMBER 2022
The Times legal editor picked up this story on 5 September 2022
Please click and add your signature to this petition to reform UK whistleblowing law – whistleblowers protect us all but weak UK law leaves them wholly exposed, lets abusers off the hook and it is a threat to public safety.
Recent examples of NHS whistleblowers who were unprotected and unfairly dismissed despite the introduction of the ineffective Freedom To Speak Up model include Nephrologist Dr Macanovic and Jane Archibald Senior Nurse. Both of these blameless professionals have had to suffer years long ordeals and legal battles that are still not concluded. Both were specifically failed by the Freedom To Speak Up system at their respective NHS trusts:
Dr Minh Alexander retired consultant psychiatrist 25 August 2022
Henrietta Hughes the former NHS National Freedom To Speak Up Guardian is a non executive director at South Central Ambulance Service NHS Foundation Trust. She took up this role in January 2022, after leaving the National Guardian’s Office at the end of 2021.
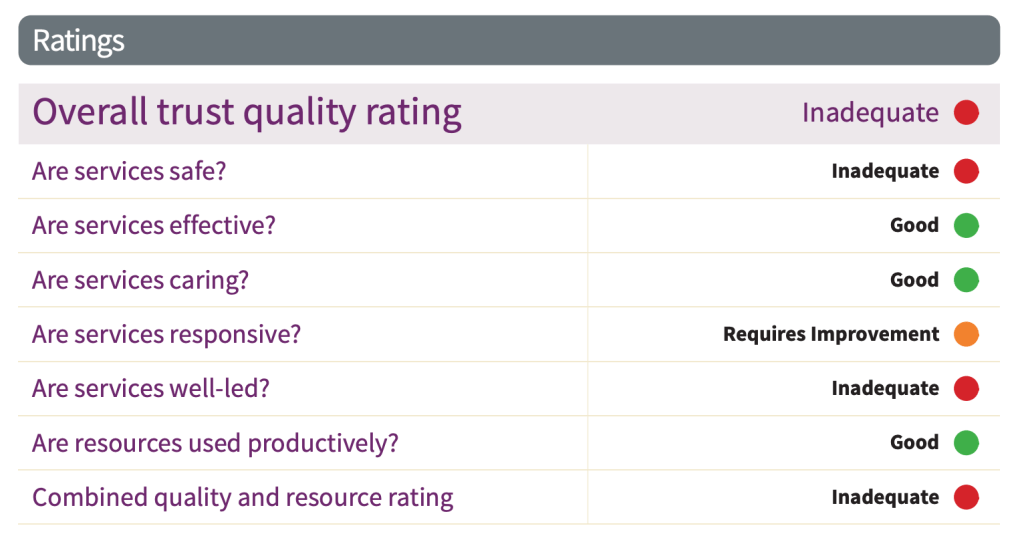
SCAS has been rated ‘Inadequate’ on Safety and the Well Led domain:
The trust board was criticised for insightlessnes, out of touch, “extreme positivity”:
“The board saw the culture as a strength of the organisation. It was sold with positivity, with many examples of forward thinking, innovation and high profile projects. There was undoubtedly much good work taking place and a genuine desire to be the very best. The risk of such extreme positivity was that this could feel dismissive of reality to the frontline staff and limit the feeling that raising or reporting concerns was a good thing to do.” [my emphasis]
A trademark of Hughes’ style is her “extreme positivity”. This was ridiculed from the outset of her tenure as National Guardian when she gave an interview to the Times in which she said the highly complex and engrained issues of poor NHS culture would be improved if only staff were more cheerful.
Most people with basic analytic capacity and emotional intelligence would more likely say that the NHS has a serious leadership problem, not that it was staff’s fault for being grumpy.
If that’s not overbearing intrusiveness and out of touch “positivity”, what is?
The CQC itself has form for over-rating trusts. It has fought a valiant battle against ambulance service reality for some years now. CQC insisted on rating West Midlands Ambulance Service as ‘Outstanding’ despite coroners’ warnings, other service failures and staff suicides.
Only in February this year CQC conducted an inspection triggered by whistleblowers and rated South Central Ambulance as ‘Good’ overall and ‘Good’ across all domains despite the whistleblowers’ concerns, although that rating seems to have now been removed from the CQC’s website. There are still some digital traces of the February ‘Good’ rating:
“We were contacted by a member of staff who had raised serious concerns during the inspection. They agreed for us to reveal their identity so that we could address the concerns.”
The CQC has also reportedly noted issues of very poor whistleblowing governance, with management smearing of the named whistleblower. Other SCAS whistleblowers who were not willing to be identified expressed understandable fears of retribution:
“It was suggested that the whistle blower had acted maliciously and was not behaving in line with their professional code of conduct. This was untrue and the whistle blower was able to produce documentary evidence that they had repeatedly raised concerns internally, although there was no requirement for them to do so. This aligns with information from others who shared concerns with the Commission but wanted their identities protected because they were afraid there would be retribution.”
CQC reported failure to act on concerns about the treatment of female staff, especially trainees:
“We received information from someone raising concerns about some women’s negative experiences at the trust; they said that this applied especially to student paramedics. The whistle blower said that concerns had been raised with senior leaders, the Freedom to Speak up Guardian and the organisational development team, but there was no evidence the concerns were being addressed. This correlates with reports from staff across the organisation who felt that the Freedom to Speak up Guardian was solely about patient safety issues and that other concerns were not recognised by leaders as being within the Freedom to Speak up Guardian’s remit, even though the role was created in line with national guidance. “
CQC reported that there were generally gross organisational culture issues.
This is especially embarrassing for the government given that one of its anointed figureheads for patient safety, Henrietta Hughes, was also SCAS’ Workforce Wellbeing Guardian.
“Henrietta Hughes acknowledged that staff were likely to be exhausted given the sustained pressures and highlighted how she would be delighted to support from the perspective of her new role as Workforce Well-Being Guardian.”
From SCAS board papers 26 May 2022
These are some of the adverse CQC findings about culture and staff experience at SC AS:
“Review of investigation reports and discussions with leaders and staff showed that organisational learning was not an embedded part of the culture. Incident investigations resulted in apportioning or suggesting where blame lay rather than focusing on the potential learning across the organisation. The actions tended to be around retraining for individuals rather than wider dissemination to mitigate future risks. Some reports blamed the patients for not providing accurate information to crews and many were judgmental about patients in their reporting.”
“Some staff felt the organisation’s leadership were visible, but others were concerned about the lack of recognition at senior level of the situation frontline staff were facing. Data provided by the trust showed two key executives, the CEO and the Director of Operations had visited sites and spoken with staff throughout the pandemic, but other executives and non-executive staff had not. Visible leadership is vital to support staff and could be achieved in a safe and pragmatic way either virtually or in person with appropriate PPE, meeting outside and other safety measures. Following receipt of the draft report, the trust shared details of additional visits by executives. It is acknowledged that face-to-face visits were reduced in line with national guidance to limit footfall and reduce the risk of viral transmission.”
“The trust had appointed a freedom to speak up guardian. However, several staff told us they could only access this service in their own time, which made this less accessible to those who had already worked a long day and needed a break. After the inspection the trust said that they freedom to speak up guardian worked flexibly to support staff, however this was not the experience of the staff which we spoke with. No impact on ratings.”
“The organisation employed in excess of 4,500 staff, but only had one Freedom to Speak up Guardian. They reported to the Interim Director of Patient Care and Service transformation; some staff said that they felt uncomfortable raising concerns that would be reported to someone in their own line management structure and worried that they could be identified.”
“Following the inspection, the provider said that there was a process in place for when the FtSUG felt there was a conflict of interest in the management structure; an alternative route for speaking up was in place. However, the staff we spoke with were not aware of this and said that they did not feel comfortable raising concerns because they felt there was a conflict of interest.”
“Our CQC survey had several comments made relating to harassment and bullying. One said, “When sexual harassment is reported it seems to be brushed under the carpet and the person is given a second chance. In the eyes of the law sexual harassment and abuse is never given a second chance and as a result people are reprimanded for their actions.”
Henrietta Hughes is not of course responsible for all the failures at SCAS.
However, in addition to sitting on its board for the last seven months, she was the National Guardian for over five years and shaped the insulting, happy clappy, PR approach to NHS whistleblowing.
As the good ship Freedom To Speak Up slowly sinks, and is exposed for the sad charade that it is, Henrietta Hughes has stepped into a air-sea rescue helicopter.
It is also fitting that ambulance trusts, which she neglected in her tenure as National Freedom To Speak Up Guardian, are helping to torpedo the government’s lies about progress in NHS whistleblowing.
But be positive.
Smile.
PETITION
Please click and add your signature to this petition to reform UK whistleblowing law – whistleblowers protect us all but weak UK law leaves them wholly exposed, lets abusers off the hook and it is a threat to public safety.
Dr Minh Alexander retired consultant psychiatrist 23 August 2022
This is a post to share data extracted from the. Chief Coroner’s website on coroners’ safety warnings related to NHS ambulance trusts in England.
Emergency services have recently collapsed due to a confluence of many disastrous factors.
Some have suggested that thousands are now dying because of NHS ambulance delays.
The Times reported on 21 August 2022 that there has been a spike in non COVID deaths and that the South West is most affected by excess deaths:
“Since the start of May, about 7,400 more people have died of non-Covid reasons than would be expected in the same period, an analysis of data from the government’s Office for Health Improvement and Disparities suggests.
The increase in deaths has been highest in southwest England, where about 8 per cent more people have died than expected. The region’s ambulance services are also suffering the worst handover delays of any region, with nearly a third of all patients in July being forced to wait more than an hour to get into A&E, a report by the Association of Ambulance Chief Executives (AACE) suggests.”
The Department of Health and Social Care is reportedly investigating:
“Early enquiries suggest most of the excess deaths in recent months have been in heart attack, stroke and diabetes patients, officials said.”
The database is not user friendly and there is no search function. This obscures patterns from public view, and therefore reduces accountability to the public.
Previously, it was necessary to laboriously search the whole database manually in order to extract data for analysis. In recent years, cases have been loosely grouped under a few categories, which allows greater public access. This is not fool proof as the indexing sometimes does not capture all cases that belong in a particular category. Nevertheless, it is now possible to manually sift each category.
The NHS ambulance trust related PFDS published since 2019 relate mostly to deaths which occurred in 2018 and 2019:
These PFD reports therefore give a snapshot of some of the problems that were building up in our emergency services in these years, before the final, current collapse.
This is a spreadsheet of the 59 ambulance trust related PFD reports that I found:
The coroners dealing with North West Ambulance Service seem most vocal in this regard.
When I previously looked at coroners’ PFDs, ambulance trusts were already noticeable for an escalating number of PFDs and findings of unsafe service pressure and problems with hospital handover.
A striking an example of a recent coroner’s PFD warning about unsafe pressures relates to the death of William Oliver on 1 November 2018, in which the coroner highlighted the severe problems for ambulance trusts facing long hospital handovers:
“An emergency call was placed to NWAS at 06.00…Mr Oliver thought he may have had two strokes in the night and he thought he had fractured his hip. In addition he was struggling to breathe and was sweating. The call was graded as requiring a Category 3 response. Subsequent calls at 06.26 between NWAS and Mr Oliver) and 06.44 (between Anchorcall and NWAS) were dealt with inappropriately and Mr Oliver’s deteriorating condition was not re-triaged. The Court found on the balance of probabilities that the response would have been increased to at least a Category 2 response…at 07.44 hrs a further call was received from Anchorcall who by this time could not make contact with Mr Oliver and the call was escalated at 07.50. At 07.51 an emergency ambulance was allocated and arrived on the scene at 08.05 when Mr Oliver was found deceased”.
“Another contributing factor to the unavailability of ambulances on the 31st October – 1st November 2018 was the turnaround times at Manchester Royal Infirmary, North Manchester General Hospital, Royal Oldham, Salford Royal and Stepping Hill were all particularly higher than anticipated with numerous ambulances delayed for over one hour. In total from the commencement of the nightshift on 31st October 2018 more than 273 hours of ambulance availability were spent at hospital sites handing over patients. The evidence from NWAS did not suggest this was significantly different to other nights or uncommon.” [my emphasis]
Concerns were also raised in the, death of Diane Gudgeon in May 2018, that the ambulance service protocol for mobilising extra resources in response to demand was set at too high a threshold and also was not always implemented when needed:
“Although EMAS was in a Capacity Management Plan (CMP) status (initially 2 and escalated to 3 at 10.35pm on 21st May 2018) this did not lead to the deployment of any additional vehicular resource. EMAS say that additional financial resources have now been made available”.
“The effectiveness of the EMAS Capacity Management & Escalation Plan (CMP) including, inter alia, the fact that:‐
a) CMP status 1 – 3 does not trigger the deployment of additional vehicular resources.
b) CMP 4 is only triggered when 200 calls are holding (this was previously 150) – this is a high threshold.
c) A Technical Commander can overrule a CMP status e.g. even if 200 calls are holding (CMP 4), this can simply be downgraded to CMP 3 by the Technical Commander.”
Generally, the PFD reports give a harrowing sense of routine, excessive pressure on the ambulance service. The delays are wasteful in that substantial resource is dedicated to precariously keeping all plates spinning – such as checks that have to be made on patients waiting for delayed ambulances. Inevitably, some of the deaths related to failures to keep all plates spinning.
“She called the emergency services on the 11th Nov 2018 to report she was feeling suicidal and threating to take an overdose. Reviews were supposedly undertaken at 22.39, 00.30 and 03.43 hours but these did not occur due to pressure at work. The paramedics eventually attended at 04.34 hours some 6 hours and 35 minutes after the initial call was made. The deceased was pronounced dead at her home on 12th November 2018 at 4 Bexon Court, Louth”
“Mr Jepson suffered stomach pain and called 999. The evidence was that the initial call was made at 15.32. That call was initially triaged as Category 5 but when the paramedic telephoned an hour later the matter was re classified at category 3. The ambulance arrived at 19.31….During the inquest, evidence showed:-
1. that the pressure on resources was high that day.
2. that a review at the two hour point should have taken place to ascertain if the matter needed re categorisation.
3. Such a review didn’t happen.
4. Whilst the evidence at inquest was that this is unlikely to have changed the outcome in this case, it was a concern to me that it could be in another case”.
Extreme service pressure may also lead to unprepared staff making mistakes. In the death of Sean Mansell, a paramedic who had not been trained was asked to assist with call handling due to severe service pressure, and made an error:
“Sean Mansell had a medical history of alcohol dependence syndrome. On the 5th July 2021, the West Midlands Ambulance Service received a 999 call at 19.23 hours from a neighbour of the deceased who reported that the deceased couldn’t walk. The call was allocated a category 3 disposition which had a target response time frame of 120 minutes. An ambulance arrived on scene at 03.38 on the 6th July which was 8 hours and 15 minutes later and not within the response time frame. This was due to the fact that demand outstripped available resources. A welfare call was undertaken at 21.28 hours by a paramedic who had been asked to go into the control room to assist with welfare calls due to the high volume of 999 calls outstanding. The paramedic had not received prior training on how to complete these calls.The welfare call was conducted with the neighbour. No contact was made directly with the deceased during the 8 hour delay which led to a missed opportunity to identify a change in his condition. When the ambulance arrived, the deceased had passed away on the sofa in his front room”
In addition to the handover at hospitals due to hospital bed shortages and delayed discharges due to social care shortages, there is also an example of another safety net that has been withdrawn by at least one local authority – the local Falls service, which might normally allow a welfare check and care whilst an ambulance was en route, had been axed. Death of 93 year old Douglas Minns:
“4 CIRCUMSTANCES OF THE DEATH
The deceased suffered a fall at home, [REDACTED] on 21st August 2018 at 8.30pm in the evening and he made an emergency call to the ambulance service. He was attended to by the ambulance service at 00.25 on 22nd August 2018 and he was eventually conveyed to Milton Keynes University Hospital arriving at 02.08. A CT scan revealed a large subarachnoid and subdural bleed caused by the fall. He died at the hospital at 15.50 on 22nd August 2018. The delay in the ambulance attending was due to high operational demand.
5 CORONER’S CONCERNS The MATTERS OF CONCERNS are as follows:
During the course of the evidence it was explained to me that the provision of a falls service was withdrawn some years ago, the service would provide for someone to attend the home of the person who had fallen, get them on their feet, assess their wellbeing, serve a cup of tea and get them back into bed if required. If they required more urgent treatment, they would report to the ambulance service. The withdrawal of the service puts patient’s lives at risk and, in view of the strains on the ambulance service, consideration should be given to reintroducing it. It is unacceptable for a 93 year old man to be left lying on the floor for four hours before someone responds.”
How many other cash strapped local authorities are in this position?
Indirectly related to resource levels, the PFDs also showed recurrent problems with ambulance service algorithms/ protocols for assessing need and priority. The fact that NHS ambulance call handlers are not clinically qualified means that if there is a flaw in an algorithm, or even if an appropriate algorithm has not been created, matters can very easily become unsafe for patients. The death of Christopher Williams in January 2019:
“His GP attended and requested an urgent ambulance since she was concerned about cauda equina. She also arranged for him to be admitted directly to the ward at the NNUH. She called the ambulance at 14.17 hrs, she was told it may take up to four hours, a pick up time of 15.17 was entered. At 15.20 the trust called the patient back his condition was worsening however the call handler did not escalate this information within the call centre and thus no one else was aware. It is understood the call handler used an incorrect algorithm (haemorrhage)….a further welfare call was made at 17.40 but no answer was received so this was escalated to the Duty Officer who subsequently upgraded the call to category 3. At 19.41 [redacted] made an 999 call describing Mr Williams as not being alert and having difficulty in breathing and the call was upgraded to a category 1. A RRV and DSA were dispatched at 19.45 hrs and arrived on the scene at 19.58. Mr Williams was conveyed to the NNUH arriving at 20.59 hrs. He was then kept in the ambulance until 23.56 hrs when he finally entered the Emergency Department….despite intensive treatment he died on 26 January 2019.”
“The trust’s Business Continuity Manager was unaware until the inquest that the call handler had erred in failing to escalate and in using the wrong algorithm….He gave evidence that the trust does not have an algorithm dealing with neurological deficits only.
This obviously costs more, but could it reduce waste and error? It is not only deaths that arise from the collapse of our emergency services, but also there will be increased morbidity and disability from failure to treat promptly, which all has a cost.
A number of coroners sent their PFDs to national ambulance organisations such as the Association of Ambulance Chief Executive (AACE) to raise concerns about flaws in algorithms or other systems issues.
One key concern was about the allocation of suspected heart attacks to Category 2 responses – within 18 to 40 minutes.
East Midlands Ambulance Service informed the coroner that they had an adjunct protocol, on top of the national protocol, for giving cases of chest pain and suspected heart attacks top priority in their call Category, but that this sometimes failed because of service pressure.
“The 999 call was triaged in line with national protocol for a primary complaint of chest pain and graded as a Category 2 response. Due to the overwhelming demand on the ambulance service that night, the ambulance did not attend Mrs Woods within the prescribed time of 18 to 40 minutes for a Category 2 call. At 01.26 hrs a further 999 call was made by the neighbour and Mrs Woods went into cardiac arrest during that call. Paramedics attended promptly but failed to administer Amiodarone contrary to National Rescuscitation guidance and without good reason. The delay in dispatching an ambulance and the failure to administer medication represent failings that prevented Mrs Wood from having the best possible chances of survival….Both EMAS witnesses agreed that 40 minutes appears too long to wait for an ambulance/ solo responder when the complaint is chest related and most likely a cardiac event….
The MATTERS OF CONCERN are as follows: 1) Patients requiring an emergency ambulance response reporting symptoms consistent with a cardiac event, but who are not yet in cardiac arrest, may wait for up to 40 minutes for a category 2 response in line with current national response times. 2) To combat this perceived inadequacy in nationally agreed response times, the East Midlands Ambulance Service NHS trust has developed an adjunct to the protocol by triaging all non Category 1 calls to upgrade calls such as Mrs Woods for a priority response. However, resources do not permit each and every call to be triaged, and Mrs Woods’ call was not triaged before she went into cardiac arrest.”
The coroner was concerned that ambulance standards were not necessarily based on clinical need:
“If the system for national response times is having to be supported by local adjuncts to the system, this rather suggests that the allocation of these calls in Category 2 lies outside clinical need.”
Some of the PFDs raised issues of leadership and organisational learning. After highlighting several concerns about East of England Ambulance Service’s handling of Christopher Williams’ case, the coroner remarked:
“This is not an isolated incident and it appears there are systemic failures in your organisation which should be addressed”.
It does appear that ambulance trusts and their staff have not been adequately supported and have been taken for granted for years, without adequate action by the government and without care for public safety. This is despite many warning signs, including the above explicit warnings by coroners.
It is not hard to see how covers up arise. Or that whistleblowers are suppressed. Or how staff welfare is impacted by the daily grind of juggling inadequate resources and knowing that patients have been avoidably harmed despite their best efforts.
NHS England too has been warned for years now by coroners of problems. The NEAS review is unlikely to be sufficiently rigorous in view of the conflicts of interest in the situation.
Given the gravity of the threat to public safety from the ambulance service collapse nationally, and how we arrived at this terrible mess, surely it should be a properly independent judge-led inquiry, with statutory force? And should its remit should be widened to include risks that are common to all NHS ambulance trusts?
Dr Minh Alexander retired consultant psychiatrist 20 August 2022
We have a perfect storm of collapsed emergency services. Years of under investment in the NHS and social care, loss of safe capacity, bed cutting, delayed discharges, loss of NHS staff from Brexit, a pandemic that has been allowed to run wild and wreak havoc, COVID related NHS staff sickness, and dangerous waiting lists. Not a storm, a tsunami.
Nevertheless, it is useful for context to this investigation to glance at relevant indicators that may shed light on NEAS’ workforce practices and governance.
Firstly, NEAS has been caught out trying to silence whistleblowers with highly inappropriate and unlawful secrecy clauses, to prevent them from pursuing public interest disclosures and requiring them to destroy evidence of wrongdoing.
NEAS’ past FOI disclosures and other information show following outlay on settlement agreements:
The settlement in 2021/22 is of special interest given what is known about the trust’s attempts to silence whistleblowers in the current deaths scandal, and the timeline of the scandal.
Based on NHS Digital data, NEAS has a trend towards increasing numbers of staff leaving in recent years. It shares this in common with other ambulance trusts.
Between 2011 and 2019, 1,395 NEAS staff resigned. The trust’s establishment is about 3,000 staff.
Between 2011 and 2019, a total of 42,350 NHS ambulance trust staff in England left:
Between 2011 and 2019 a total of 27,205 NHS ambulance trust staff in England resigned:
The NHS staff survey is another source of data on workforce relations. The overall response rate for the NHS is poor. Amongst ambulance trusts there is great variation in the response rate, raising some questions about the validity of the data and staff engagement in some of the trusts. Alternatively, it may also reflect the management approach to staff “compliance” with the survey:
From NHS Staff Survey 2021
The 2021 NHS staff survey confirmed that ambulance trust operational staff experience the highest levels of burnout:
The 2021 NHS staff survey revealed that ambulance staff are the group most likely to report detrimental understaffing:
From NHS Staff Survey 2021
This table shows how this metric on the NHS staff survey plummeted at ambulance trusts between 2020 and 2021. The most shockingly low score was at East of England Ambulance Service, where only 12.2% of staff thought there was sufficient staffing:
From NHS staff survey 2021
In recent years, roughly only a quarter of NEAS staff thought that there was safe staffing:
From NHS Staff Survey 2021
Ambulance trusts used to be gross outliers for bullying. This has improved in recent years, but most ambulance trusts still have levels of bullying above the national average. East of England Ambulance Service remains a gross outlier. This was the rate of reported bullying for each ambulance trust in 2021:
From NHS Staff Survey 2021
Ambulance trust staff gave mixed messages on the 2021 staff survey questions about whistleblowing, in common with the rest of the NHS. There is higher scoring on feeling able to report unsafe care, but a decrease in the perception that staff can speak out about anything. As has consistently been the case, staff are less likely to think that concerns will be addressed:
From NHS Staff Survey 2021From NHS Staff Survey 2021
The above are hypothetical questions about what might happen.
On a question about what actually happened, Ambulance trust staff said they under-reported bullying to the following degrees, which raises questions of engagement and trust. Ambulance trusts are all below the national NHS average for reporting bullying:
From NHS Staff Survey 2021
But that might not be so surprising given that the NHS staff survey composite scores on “compassionate leadership” is the lowest overall for ambulance trusts:
From NHS Staff Survey 2021
We shall see how the Dame handles the deaths scandal at NEAS.
It is worth bearing in mind that she had a whistleblowing scandal of her own, which the former National Freedom To Speak Up Guardian helped to suppress by breaching her own procedures in a most arbitrary and extraordinary way:
Please click and add your signature to this petition to reform UK whistleblowing law – whistleblowers protect us all but weak UK law leaves them wholly exposed, lets abusers off the hook and it is a threat to public safety.
Dr Minh Alexander retired consultant psychiatrist 19 August 2022
The Employment Tribunal was meant to provide accessible justice but in reality claimants who are unrepresented are much disadvantaged, as reported by this Cardiff University paper which looked at family courts and other civil cases::
“8. Unrepresented litigants participated at a lower intensity but made more mistakes. Problems faced by unrepresented litigants demonstrated struggles with substantive law and procedure. There was other evidence of prejudice to their interests.
9. There was at best only modest evidence that cases involving unrepresented litigants took longer, though cases with unrepresented parties were less likely to be settled.”
Employment Tribunal (ET) claimants, unfamiliar with the legal bear traps, tend to be over-optimistic about their chances of success:
“Claimants’ expectations about the outcome of the case at the point of initiating their claim were generally positive (Table 7.1). Nearly all claimants (92 per cent) thought that they had at least an even chance, and this included 53 per cent who thought that they were very likely to be successful. These positive views were widespread, even where the outcome turned out to be unsuccessful. For example, only 2 per cent of those whose claim turned out to be unsuccessful at tribunal, expected this to be the outcome at the start of the claim”
In the ET, only those who can match employer’s firepower with equal quality of legal representation have much chance of success and even then, many are only partly successful.
A guide written by a lawyer for lawyers facing unrepresented claimants or “litigants in person” in personal injury cases, , gives an example of how the other side might think:
In the ET, discrimination and whistleblowing cases have particularly poor outcomes for claimants, because the legal tests favour employers.
Many whistleblowers who go to Court are unrepresented.
A 2020 Greenwich University study found that half of whistleblowers are unrepresented in the Employment Tribunal:
A thorny issue is the price of justice.
Lay people may not understand how much justice costs.
The Courts have to manage this cost with fairness and the public purse in mind, and also the list of waiting cases. The Court backlog has grown as a result of the pandemic. Case management hearings are an opportunity for Tribunals to ensure the most efficient handling of cases.
But claimants who represent themselves, are at special risk of driving up the cost of cases and exposing themselves to a cost claim by the other side (the “Respondent”).
If Claimants are deemed to have caused unreasonable and unacceptable costs, possibly because of insufficient objectivity or perhaps because they do not fully understand the cost implications of the way in which they conduct their claim, they may have to pay the other side’s costs.
“Employers were more likely than claimants to be aware that costs could be awarded against a party if they unreasonably pursued and employment tribunal case. While 67 per cent of employers said they were aware of this, this applied to only 54 per cent of claimants”
“When a costs order or a preparation time order may or shall be made
76.—(1) A Tribunal may make a costs order or a preparation time order, and shall consider whether to do so, where it considers that—
(a)a party (or that party’s representative) has acted vexatiously, abusively, disruptively or otherwise unreasonably in either the bringing of the proceedings (or part) or the way that the proceedings (or part) have been conducted; or
(b)any claim or response had no reasonable prospect of success.
(2) A Tribunal may also make such an order where a party has been in breach of any order or practice direction or where a hearing has been postponed or adjourned on the application of a party.
(3) Where in proceedings for unfair dismissal a final hearing is postponed or adjourned, the Tribunal shall order the respondent to pay the costs incurred as a result of the postponement or adjournment if—
(a)the claimant has expressed a wish to be reinstated or re-engaged which has been communicated to the respondent not less than 7 days before the hearing; and
(b)the postponement or adjournment of that hearing has been caused by the respondent’s failure, without a special reason, to adduce reasonable evidence as to the availability of the job from which the claimant was dismissed or of comparable or suitable employment.
(4) A Tribunal may make a costs order of the kind described in rule 75(1)(b) where a party has paid a Tribunal fee in respect of a claim, employer’s contract claim or application and that claim, counterclaim or application is decided in whole, or in part, in favour of that party.
(5) A Tribunal may make a costs order of the kind described in rule 75(1)(c) on the application of a party or the witness in question, or on its own initiative, where a witness has attended or has been ordered to attend to give oral evidence at a hearing.”
“Ability to pay84. In deciding whether to make a costs, preparation time, or wasted costs order, and if so in what amount, the Tribunal may have regard to the paying party’s (or, where a wasted costs order is made, the representative’s) ability to pay.”
It is held that it is harder for employers to win costs against unrepresented claimants,
But most private individuals can ill afford costs of any sort.
Particularly sacked whistleblowers who face the prospect of blacklisting and loss of livelihood.
An interesting ET judgment has been published in which the Court ruled that a claimant conducted her case unreasonably, racking up costs with little understanding that she was doing so. BUT it has decided not to make her pay costs because her former employer, Kings, failed to give her a cost warning:
“Although the claim had no prospects of success and notwithstanding the Claimant was told this, she continued with it up to the hearing, she seemed genuinely perplexed by the legal complexities involved. The Tribunal considers that she would have had no understanding of the costs implications of what she was doing. The Tribunal considers that the Claimant ought to have received a costs warning to make her appreciate the implications of what she was doing. It was not enough to state the legal position to her on three occasions. In these circumstances, the application is refused.”
So it seems ignorance can be a defence sometimes.
Going to the other extreme, some employers make aggressive cost applications as a means of intimidating claimants, and if they are represented, running up the claimant’s legal bill.
A costs warning letter can in certain circumstances be a useful tool in persuading claimants to settle or drop a matter before a final hearing. The content of a good costs warning letter should include a detailed overview of why the claimant’s claim is legally flawed and, in no uncertain terms, set out the consequences of a claimant going on to pursue his or her claim to a final hearing. Careful thought does however need to be put into the content, timing and tone of a costs warning letter. Not every case is right for a costs warning letter, and Tribunals often take unkindly to overly aggressive costs letters against unrepresented claimants.” [my emphasis]
Regardless of any possible leniency and considerations by the Court for unrepresented claimants, do be very circumspect if as a whistleblower you are forced into the Courts. No matter how provoked you are, do your utmost to be reasonable and try to ensure that your conduct cannot be criticised. Otherwise it could be expensive.
Better still, try and avoid an employment dispute altogether, as few whistleblowers walk away from such disputes without emotional, professional and financial loss. There is also huge impact on families, especially where there are dependants.
In these days of great unreliability and corruption in government and captured regulators, it is worth considering whistleblowing directly to the press either anonymously or with agreed protection of your identity. Take careful advice before doing so.
Obviously there will be circumstances when some whistleblowers feel that such whistleblowing will not be sufficient to resolve their concerns, and they must go on the record.
In which case, prepare as much as you can for all eventualities, and again, take careful advice.
Dr Minh Alexander retired consultant psychiatrist 12 August 2022
Very important new evidence has arisen from hard-won FOI data that the US government bounty hunting programme has been tainted by cronyism and a revolving door between regulators and industry, and all facilitated by secrecy.
Alexander Platt an Associate Professor of Law at the University of Kansas has succeeded, after a two year battle, in uncovering the dominance of a small number of specialist law firms. Under cover of great secrecy, these “repeat players” have been hoovering up the bounty cash. It also seems that there is a revolving door and that law firms with ex-regulatory staff have been more favoured. Eye watering amounts of public cash have been involved, with law firms taking upwards of 30-40% contingency fees from hundreds of millions dollars of bounties.
Platt reported that one former senior Securities and Exchange Commission (SEC) lawyer, now a bounty hunter, was:
“…responsible for 10 awards in my [his] dataset, accounting for $152,575,000 – about 20% of all dollars awarded.”
The terrible mess described by this study is the very system that the lamentable Whistleblowing APPG and its troubling secretariat WhistleblowersUK want to introduce to the UK.
It is hardly surprising that monetising a core public function would lead to such a situation. This is a key reason why so many genuine whistleblowers oppose the appalling proposals.
I have been exchanging correspondence with the government department which currently controls UK whistleblowing law, BEIS, to raise concerns about the Whistleblowing APPG’s proposals.
As per usual, the government’s responses have been deflective and impenetrable. But I have now sent through the Platt paper as further evidence of concern. Given the high risk of misuse of public funds if the US bounty hunting model is replicated in the UK, I have copied my correspondence to the Public Accounts Committee, the Standards Committee and to Lord Evans, Chair of the Committee on Standards in Public Life.
Minister for Business, Energy and Corporate Responsibility
12 August 2022
Dear Lord Callanan,
University of Kansas: Evidence that the US bounty hunting model of whistleblowing sets up perverse incentives and wastes public funds on an industry that massively profits lawyers
Thank you for the letter from your department of 30 June 2022, attached, which is a reply to my letter to you of 30 May 2022, copied below.
In my letter I raised serious concerns about the nature of the Whistleblowing APPG, the APPG’s legislative ambitions, the PM’s Anti Corruption Champion John Penrose MP’s support of these ambitions and the conduct of its secretariat the private organisation WhistleblowersUK.
My reading of your department’s response to me is that it has not truly engaged with widespread whistleblowers’ concerns about those who would replace very weak existing UK law with something that is no better, and is in fact arguably worse in its exploitativeness.
I write now to pass on an item of academic research from Kansas University which has found cronyism and highly questionable practices at the heart of the US bounty hunting model, that some wish to import to the UK.
This is a link to the substantive report by Alexander Platt, Associate Professor of Law at Kansas:
It concludes that the US Securities and Exchange Commission and the US Commodity Futures Trading Commission have operated their whistleblower reward programmes in such a way that:
“…private whistleblower lawyers operate free from virtually all public accountability, transparency, or regulation”
A press report by Kansas University sums up the findings thus:
“the CFTC has awarded nearly two-thirds of all money to tipsters represented by a single law firm and the SEC had disproportionately favored tipsters represented by former SEC officials”
“About one-quarter of dollars awarded by the SEC have gone to clients of lawyers who formerly worked for the agency. Platt estimates that means as much as $70 million has been paid by the SEC to its own alumni.”
These revelations came only after a two year FOI battle by Professor Platt with the Securities and Exchange Commission and Commodity Futures Trading Commission, with improper secrecy being another criticised aspect of the matter.
The relevant tables from Professor Platt’s paper are copied below.
These tables show that a huge proportion of the monies paid out from the public purse go to the lawyers, and that a small number of law firms (“repeat players”) dominate the scene.
Astonishingly, Professor Platt also established from the FOI data that Jordan Thomas the former US official, who established SEC’s whistleblower programme but went into private practice, was:
“…responsible for 10 awards in my [his] dataset, accounting for $152,575,000 – about 20% of all dollars awarded.”
I hope all this illustrates graphically how ill-advised monetisation of whistleblowing will introduce all sorts of perverse incentives practices, that have nothing to do with the public interest whatsoever.
It would serve only to enrich a tiny few, whilst large tranches of socially important but unprofitable whistleblowing will be pushed aside by those who primarily seek to extract money from whistleblowing. The repeated scandals in the health and care sectors will not be improved by adopting this very flawed US model, as it rests only on financial recovery of looted money from scams in the financial sector.
I really do urge the government not to follow the US down this rabbit hole of injustice and highly questionable use of public money.
I should point out that the much-criticised Whistleblowing APPG and its even more troubling secretariat have received funds from the US bounty hunting law firm Constantine Cannon.
In December 2021, Constantine Cannon was open about its recruitment of a former SEC official:
I would be grateful to know where the government currently stands on adoption of the Whistleblowing APPG’s proposals for an Office of the Whistleblower as set out in the Robinson/Kramer Bills:
I copy this to Public Accounts Committee, the Standards Committee and Lord Evans of the Committee for Standards in Public Life with reference to the high risk of misuse of public funds if the Whistleblowing APPG’s proposals are adopted.
Yours sincerely,
Dr Minh Alexander
Public Accounts Committee
Standards Committee
Lord Evans, CSPL
From: “BEIS Correspondence” [address redacted]
Subject: A response to your recent enquiry – Ref: TOB2022/13299
Date: 30 June 2022 at 14:44:53 BST
To: Minh Alexander [address redacted]
Reply-To: BEIS Correspondence
Dear minh alexander,
Please find attached our response to your recent enquiry.
Subject: Concerns about lobbying by various parties to add flawed whistleblowing provisions to the Economic Crime Bill
BY EMAIL
Lord Callanan
Minister for Business, Energy and Corporate Responsibility
30 May 2022
Dear Lord Callanan,
Concerns about lobbying by various parties to add flawed whistleblowing provisions to the Economic Crime Bill
I write to raise a concern about the proposals by a number of parties to insert whistleblowing clauses into the Economic Crime Bill (ECB), which will not serve the public interest.
1) The organisation Protect has petitioned to piggyback the creation of its version of a Whistleblowing Commission onto the ECB.
Protect’s Whistleblowing Commission ultimately does not compel investigation of and follow up on whistleblowers’ concerns, thereby replicating the core weakness of existing UK whistleblowing legislation which has been failing whistleblowers for over twenty years.
2) The controversial Whistleblowing APPG, established with funding from US bounty hunting lawyers, has lobbied to piggyback the creation of an even worse US style “Office of the Whistleblower” onto the ECB.
Shockingly, WhistleblowersUK has approached bereaved people on social media to proffer legal services. I see this as part of a campaign to broaden the UK definition of whistleblower, to create the conditions for US style bounty hunting, where any informant can claim a bounty, even criminals.
Some members of the Whistleblowing APPG have also called for whistleblowers to be “rewarded” and “incentivised”.
The majority of genuine whistleblowers do not support such a US bounty model. Apart from conflicting with public sector Nolan principles, conflating genuine whistleblowing with the use of paid informants brings the good name of whistleblowers and whistleblowing into jeopardy. Whistleblowers already struggle to be heard and believed. They do not need to be further stigmatised.
Any Office set up primarily to retrieve money will also neglect whistleblowers from non-financial sectors and those whose disclosures are concerned with protecting people and not property.
If those lobbying in the interests of the bounty hunting industry succeed in massively widening the UK definition of a whistleblower, in order to recoup maximum profit for the industry, this dilutes the availability of finite protection resources for workers who are the real whistleblowers, and who need protection from severe detriment such as job loss.
The recent ten minute Bill put forward by the Whistleblowing APPG on 26 April 2022 has many worrying features. It can be understood as a bounty hunters’ Bill. The Bill proposes a scheme for whistleblower “recognition” which appears to mean financial recognition. The Bill also proposes massive fine of up to £18 million or more, which would cause great harm if levied against a public service. Whistleblower colleagues and I have prepared a formal critique to point out numerous areas of concern in the Whistleblowing APPG’s Bill, and the ways in which it gives comfort to bounty hunters:
I ask that if the government makes any whistleblowing provision within the Economic Crime Bill,
1) That it does not create any Whistleblowing Office or Commission under government control. Independence is key and the majority of whistleblowers see full independence of a whistleblowing agency as a key issue.
2) That the list of those protected is restricted to workers, close relatives who may be equally affected by detriment and a number of relevant non-workers such as listed by the EU Whistleblowing Directive (contractors etc…)
3) That it ensures that any whistleblowing body created has a remit and powers to investigate whistleblowers’ concerns if employers and regulators fail to investigate or fail to investigate appropriately
4) That financial rewards for whistleblowing are explicitly prohibited, and that fair compensation for loss and non-financial redress are the remedies
5) That any whistleblowing body created has powers to litigate to protect the interests of whistleblowers, for example by making relevant third party interventions
6) That any whistleblowing body created does NOT have the power to impose fines on public bodies, only against individuals, in recognition that public services should not suffer because of wrongdoing by senior managers.
7) That any whistleblowing body created is tasked with ensuring maximal early protection, conflict resolution and minimisation of wasteful litigation. The Whistleblowing APPG’s Bill fails to provide these elements, and perhaps unsurprisingly so, as it is not in the bounty hunting industry’s interest for conflict and litigation to be reduced.
8) That criminal offences are created in line with the full range of dissuasive penalties specified in the EU Whistleblowing Directive, and that any new whistleblowing body has powers of prosecution and to refer for prosecution.
9) That there are no legal barriers inserted which could be abused in order to persecute whistleblowers. For example, the Whistleblowing APPG Bill proposes, without definitions, that its Office of the Whistleblower may reject “frivolous, malicious or vexatious” whistleblower complaints. Given that the ‘good faith’ test of the Public Interest Disclosure Act was much abused before it was abolished, it would be seriously retrograde to re-introduce a means by which whistleblowers could be smeared as a legal technique for undermining their cases.
Lastly, please find below a link to an FOI disclosure by the Home Office which reveals email correspondence between the Whistleblowing APPG Chair and the Prime Minister’s Anti Corruption Champion. This confirms that the intention was to use a ten minute rule Bill by the APPG to target the Economic Crime Bill:
Former Health Secretary Sajid Javid announced that an independent investigation would take place into these matters, but not a public inquiry as requested by NEAS whistleblowers and bereaved families. The terms of reference are still awaited. The following written exchange took place in parliament on 1 August 2022:
To ask the Secretary of State for Health and Social Care, when he expects the independent review into the North East Ambulance Service (NEAS) to be completed; if he will publish the report of that review; and what steps he plans to take to help ensure that the standard of service provided by NEAS improves as quickly as possible.
NHS England is establishing governance arrangements for an independent review to formally commence as soon as is practicable. The families and staff affected will have an opportunity to contribute to the review’s Terms of Reference in due course. Once the review is completed, its report will be published independently of the National Health Service. Local commissioners and the NHS will support the implementation of any recommendations to improve the culture within and the quality of service provided by the North East Ambulance Service as soon as possible. Further details will be available shortly.
NHS England advises that the North East Ambulance Service NHS Foundation Trust has measures in place to improve the standards of service it provides. An investment of £38 million has been agreed for 2022/23 to improve clinical care, recover ambulance response times, increase the operational and Emergency Operations Centre (EOC) workforce and the establishment of an additional EOC in the south of the Trust’s area.
This revealed that trust managers failed to heed legal advice from the trust’s own solicitors about complying with coronial law.
The trust initially claimed in response to a recent FOI request, for an earlier and more clinically detailed interim AuditOne report of March 2020, that disclosure was exempt due to prejudice to the conduct of public affairs. It is currently responding to a request to internally review this refusal.
Alongside the 2020 AuditOne investigation of coronial process at NEAS, the trust also commissioned an external investigation into governance and workforce issues, including whistleblowing governance and bullying.
This was reportedly carried out by external investigators, Jennie Stanley (nee Fecitt) and Tracy Boylin.
NEAS was asked about the number of external whistleblowing and bullying and harassment investigations that it has commissioned in the last three years. It declined to answer on grounds that the numbers were too small and that disclosure might breach privacy through identifiability.
Asked why it opted to pay for private investigative services instead of seeking a review by the National Guardian’s Office, NEAS replied that it held no information about this.
NEAS refused to give even a summary of the recommendations arising from the Stanley report on whistleblowing and bullying.
It wriggled out of this with the implied claim that there are no existing summaries to disclose, and that it is not required under FOIA to generate new information:
“The Freedom of Information Act states that public authorities are not required to create new information to comply with a request for information under the act.”
Whilst this may be technically correct, assuming that NEAS is telling the truth that it has no existing summary of the recommendations to disclose, it seems a poor return for public expenditure.
Surely the public are entitled to at least a short explanation of why an investigation was needed, and what now needs to be done?
NEAS also contended that the information requested constituted personal data, and claimed this as a further exemption.
In the circumstances, given that bullying seems inked with poor whistleblowing governance, NEAS whistleblowers’ claims that the trust tried to apply unlawful gagging clauses to stop them raising public interest concerns and requiring whistleblowers to destroy evidence of wrongdoing, serious breaches of coronial law and apparent cover up of fatal care failures, the public interest arguably overrides the privacy exemption by NEAS.
NEAS has been asked to:
Clarify whether it has an existing summary of the Stanley report recommendations and to disclose if so;
The seniority of the individuals whose privacy NEAS claims would allegedly be breached – are of them any directors? This has a bearing on the public interest test in favour of disclosure.
Disclose the original recommendations of the Stanley report.
Local MPs have been informed of NEAS’ withholding of what appears to be significant data from public scrutiny.
Perhaps NEAS would be wise to think on this principle.
PETITION
Please click and add your signature to this petition to reform UK whistleblowing law – whistleblowers protect us all but weak UK law leaves them wholly exposed and it is a threat to public safety
Recent examples of NHS whistleblowers who were unprotected and unfairly dismissed despite the introduction of the ineffective Freedom To Speak Up model include Nephrologist Dr Macanovic and Jane Archibald Senior Nurse. Both of these blameless professionals have had to suffer years long ordeals and legal battles that are still not concluded:
Dr Minh Alexander retired consultant psychiatrist 1 August 2022
This is a brief post to share FOI data for anyone interested in events at BCUHB
Lack of NHS safe staffing and the linked issue of chronic NHS underfunding are unresolved issues that seem likely to remain with us for the foreseeable future, given our economic woes and troubled politics.
A cycle of politically driven suppression and bullying trail in their wake.
The same story plays out time and gain, and the same care scandals recur, despite investigations and inquiries such as the Mid Staffs public inquiry. The latter was politically awkward in that it advised that care should be driven by fundamental standards (ie. not resource driven). The inquiry laid a heavy emphasis on ensuring safe staffing levels, after cost-cutting, unsafe staffing levels were uncovered as a pivotal failure in the Mid Staffs disaster.
But then Robert Francis was knighted and appointed to the Care Quality Commission’s board and Jeremy Hunt the then Health Secretary scrapped NICE’s work on safe staffing standards and refused to introduce legislation on mandatory safe staffing.
On the frontline, a vicious cycle is set up of forced errors from thinly spread, stressed staff making inevitable errors and omissions and then being harshly scapegoated and punished for what are primarily system failings. Or they may not report incidents for fear of blame. Or if they raise concerns about system faults, they are bullied for that too.
Unsafe staffing is brutalising for both staff and patients. Burnt out staff cannot give of their best.
BCUHB consequently announced an investigation into these matters. The investigation should have concluded in July.
Via an FOI response of 19 July 2022, the health board has disclosed that staff raised a total of 3006 adverse events affecting staff levels over a three year period:
“From 1st April 2019 to 31st March 2022, there have been 3006 adverse events that affected staffing levels, please note this figure includes staff reporting positive COVID-19 statuses.”
The investigation was reportedly overseen by an external party, but my reading of the terms of reference is that an internal “review support team” assisted the external investigator:
Royal College of Nursing
This is a link to the RCN’s ongoing work on safe staffing: