
By Dr Minh Alexander retired consultant psychiatrist 15 June 2026
This is a brief post to raise awareness of a second inquest which opens tomorrow into the death of 32 year old Andrew Edward Watson
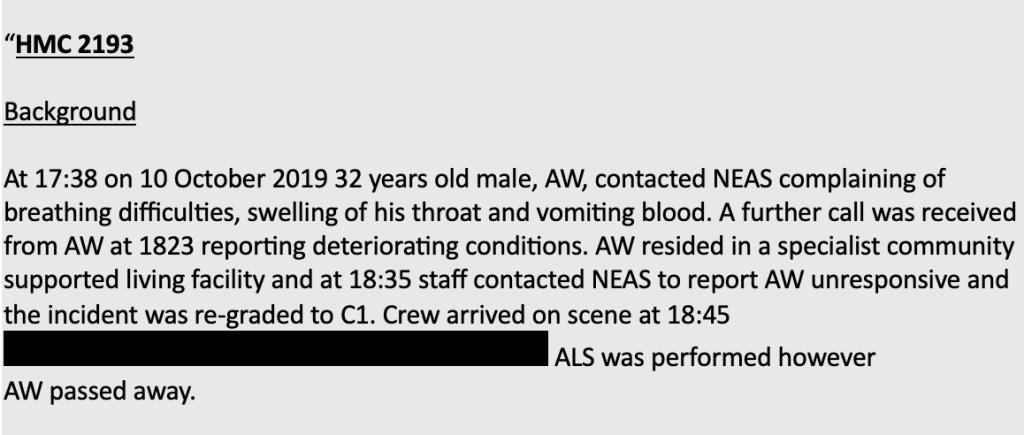
Andrew died on 10 October 2019 after being unable to breath due to a quinsy, which was an abscess in his throat related to severe tonsillitis.
The condition is a recognised emergency when signs of sepsis or airways obstruction, such as difficulty breathing, are present. It is in theory fully treatable.
An ambulance was called to Andrew’s home, but the response was delayed. He had become unresponsive by the time an ambulance arrived. He could not be revived despite attempts to resuscitate him.
North East Ambulance Service (NEAS) is accused of covering up its failings by withholding relevant information about the ambulance delay from the coroner:
Inquest to be held into NEAS County Durham ‘cover-up’ death
As a result of the information about the circumstances of Andrew’s death being withheld, a previous inquest held in 2019 concluded that Andrew’s death was due to natural causes.
However, a second inquest was scheduled after whistleblowing disclosures by Paul Calvert, a coroner’s officer employed by NEAS, revealed that information had been withheld from the coroner:
NHS ambulance service doctored documents to cover up truth about deaths
The second inquest highlights that matters regarding NEAS’ governance are far from resolved.
Both NEAS and NHS England (NHSE) were implicated in the failures, as NHSE failed to respond adequately to whistleblower concerns. However, NHSE was allowed to oversee the investigation into NEAS’ failings, which was controversially contracted to Marianne Griffiths.
Griffiths was the former CEO of University Hospitals Sussex NHS Foundation Trust which had recurrent whistleblower scandals including maternity care whistleblowing, an ongoing police investigation into surgical harm and most recently a maternity care scandal necessitating inclusion in the national investigation programme.
Griffiths’ investigation into NEAS commanded little credibility, not least because NHS England’s highly restrictive terms of reference for the investigation excluded many relevant cases, focusing only on four cases when trust whistleblowers flagged more than ninety:
Deaths inquiry will exclude dozens of concerning cases, says whistleblower
The Griffiths investigation was boycotted by whistleblowers and some families.
This is her final report, which was published in July 2023:
Griffiths failed to review Andrew Watson’s case despite it being one of the cases flagged by a previous report commissioned by NEAS, the so-called “Interim Audit One report”.
NEAS attempted to suppress the Audit One report for a long time, and it was only released into the public domain in 2025 in a very heavily redacted form after a prolonged FOI battle, involving an appeal to the Information Commissioner.
Both the Sunday Times and local media have confirmed that the Interim Audit One report covered Andrew’s case.
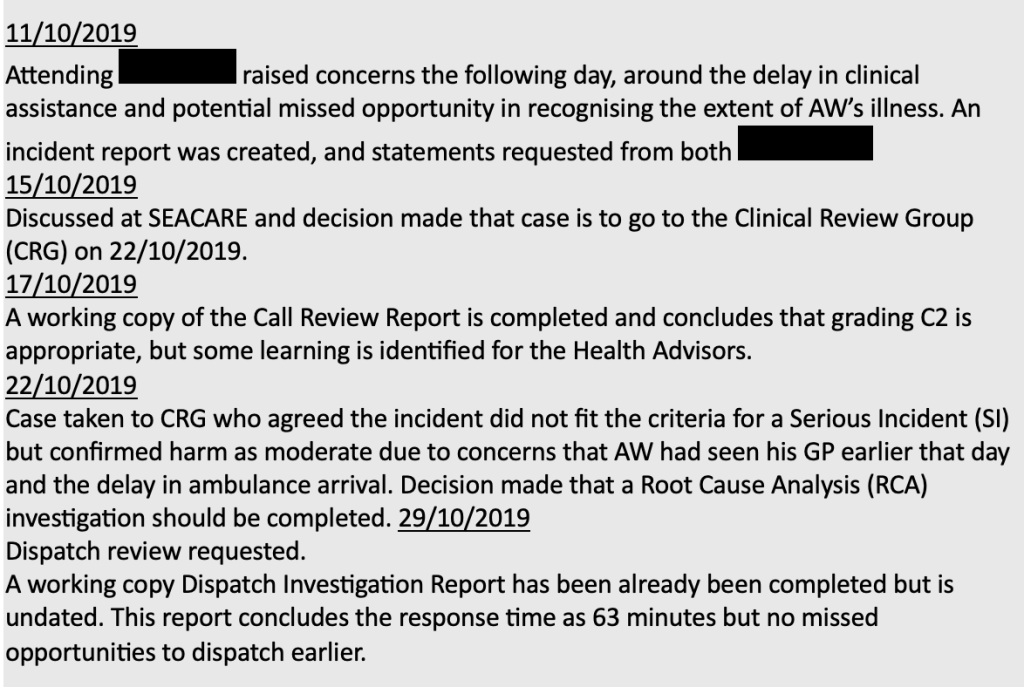
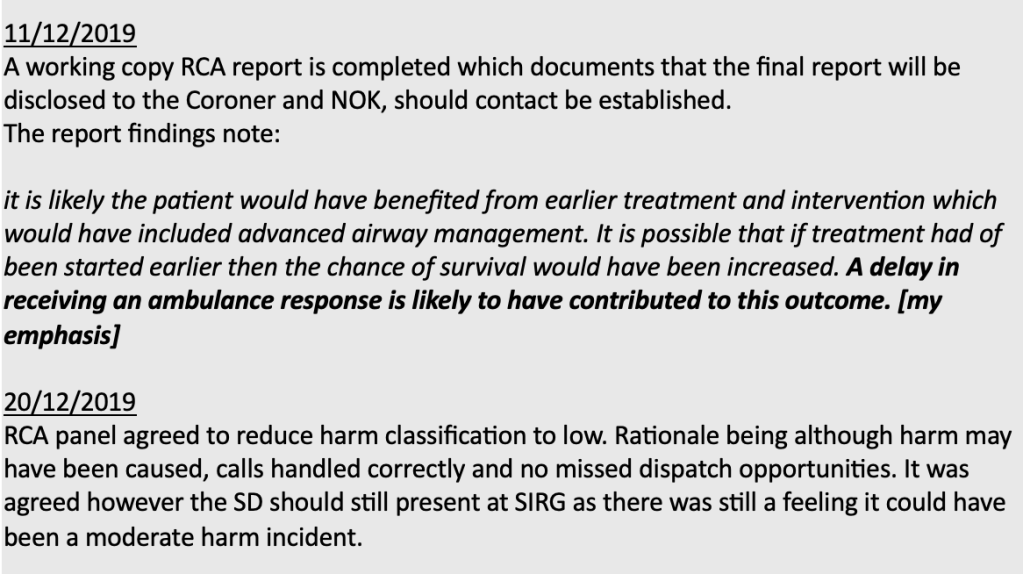
The relevant passage from the report crucially noted that an internal trust root cause analysis concluded ambulance delay contributed to Andrew’s death.
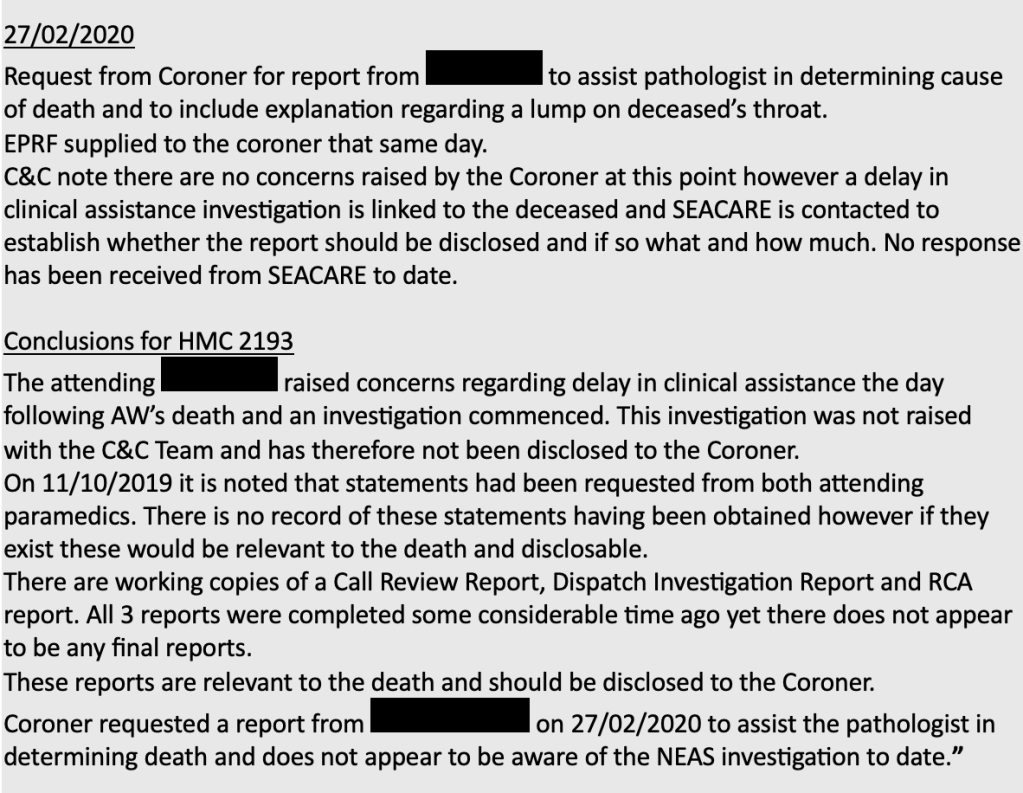
It also noted that this internal RCA report and other relevant documents were not disclosed to the coroner.
This is the crucial, relevant section from the Interim Audit One report on Andrew’s case:
Extraordinarily, the family reported that in June 2024 they nevertheless received correspondence from Trust lawyers which claimed that Andrew’s case had NOT featured in the Interim Audit One report.
Moreover, the Trust was unaccountable and refused to comment when asked by the Chronicle about its false claim.
Entwined with this poor governance and gaslighting, there is an ongoing NMC fitness to practice process on two former senior NEAS nurses.
They are accused of playing a key part in the minimisation of trust operational failures and subsequent failures to inform the coroner about these in relation to deaths. One of the accused registrants, SD, was reportedly party to the above decision on 20 December 2019 to downgrade Andrew’s death to a “low” harm classification.
Reclassification to “low harm” meant that the trust did not have to disclose these matters to Andrew’s family under the statutory Duty of Candour.
This is Care Quality Commission regulatory guidance which stipulates that provider organisations should disclose harm where the harm is classed as “moderate” or “severe”, and does NOT require disclosure when harm is classed as “low”:
CQC guidance on Regulation 20 Duty of Candour
The fitness to practice hearing was scheduled earlier this year but ended only part heard, and will resume next year.
The government has so far resisted calls for a public inquiry, which is an injustice in the face of the questions left unanswered and the serious failures of the Griffiths report and its commissioning.
Related items
Death of Mr Peter Coates – an example of manipulation of evidence by NEAS
On 23 March 2026 Paul Appleton the coroner for Teesside and Hartlepool issued a Prevention of Future Deaths report on the death of one of the victims of the NEAS scandal, Peter Coates.
Prevention of Future Deaths report Peter Coates 2026-0154
Mr Coates died of asphyxiation due to a combination of severe respiratory disease and a power cut at his home which meant that he was unable to access his usual oxygen treatment. He called 999 but there was a delay in an ambulance reaching Mr Coates because a nearby vehicle could not get through electrically controlled gates because of the power outage (and because the crew did not know of a manual override), and because another vehicle stopped to refuel despite having sufficient fuel in the tank.
The coroner concluded this year that the ambulance delay may have been a contributory factor in Mr Coates’ death:
“Peter’s death was possibly contributed to by delays in the arrival of the ambulance crew to him.”
In 2023 the Griffiths report acknowledged the family’s concern that the delayed ambulance response was a contributory factor in Mr Coates death, but in my view Griffiths’ report did not make it sufficiently clear that an inquest was yet to make a finding on this issue.
Originally, when the coroner first opened an investigation into Mr Coates’ death, NEAS did not fully disclose the circumstances of the death, downgraded the level of harm to “low” and excised facts from evidential documents, as reported by the Sunday Times:
“Although an investigation began the same day, the coroner was not made aware of this at the time, or of the fact that there had been any delay in getting help. Despite the mistakes and delays, a decision was made by bosses to downgrade the incident to “low harm”, on the basis that the primary reason for Coates’s death had been the oxygen equipment malfunction. The coroner, in fact, “should have been notified” straight away about the death and about the delays, the AuditOne investigation found. The NEAS internal investigation soon found that the second ambulance had in fact had sufficient fuel to complete the journey. This raised questions as to why the stop occurred. A statement made by one of the paramedics involved, explaining the decision to refuel, was never disclosed to the coroner. Instead, the paramedic was asked by bosses to produce a new statement, which made no reference to the decision to refuel. The coroner was “only supplied with the [later] statement, which does not include any reference to the refuelling”, AuditOne found.”
Unless a statutory public inquiry is held, we will never know how many other cases were subject to such manipulation of evidence and self-interested under-estimation of harm.

