He has openly advocated that UK whistleblowers should be “incentivised”:
Other members of the Whistleblowing APPG have also spoken about whistleblower rewards and the APPG’s secretariat WhistleblowersUK has advocated for whistleblower rewards.
The offer of whistleblower rewards is against most ethical guidance on whistleblowing and against longstanding UK whistleblowing policy.
Kevin Hollingrake was appointed to the Department for Business, Energy and Trade as Parliamentary Under Secretary of State between 27 October 2022 and 7 February 2023.
Most recently Hollinrake was appointed Parliamentary Under Secretary of State at the Department for Business and Trade on 7 February 2023.
Will the review be conducted professionally, impartially and follow the evidence base?
Or will it be another Tory charade of thinly disguised cronyism, boot filling and back room deals?
Given all the evidence of government misconduct in recent years, one might reasonably think that the prospect of a bounty model, that siphons obscene amounts of cash into the hands of whistleblowing industry middlemen and bounty hunting lawyers, has just become more likely.
Especially if the increasing excitation of the assorted denizens of the Whistleblowing APPG’s murky waters is anything to go by.
Don’t be optimistic of any genuine governance.
Do expect the parade of dubious celebrities, useful idiots, fake talking heads, planted articles puffing the Office of the Whistleblower and social media sock puppeteers to get worse.
That is of course, only if some further terrible government scandal does not upend all plans by this time next week, and we get another clutch of heartsink ministers.
By Dr Minh Alexander retired consultant psychiatrist 29 March 2023
On 18 November 2022 it was announced by both University Hospitals Birmingham NHS Foundation Trust (UHB) and the commissioning body Birmingham and Solihull Integrated Care Board (ICB) that David Rosser CEO of UHB was moving on to a new role.
This role was regional “Strategic Director of Digital Health and Care”.
Curiously, there appeared to be no sign of an office, team, website locus, operating details or contact details. As the weeks and months passed, this did not change.
Eventually, repeated enquiries to Patrick Vernon the ICB Chair resulted in an admission, via the ICB FOI team, that Rosser had not left UHB at all.
He remained technically employed by UHB.
Jonathan Brotherton was carrying out his former duties as acting UHB CEO.
In Rosser’s new Digital role, he was reportedly “hosted” by the ICB and reported to the ICB’s chief executive David Melbourne.
Yes, that is the same David Melbourne who has been directly involved in the oversight of the ICB’s reviews on UHB’s failing governance and who has been responsible for briefing local councillors about the progress of the reviews via the Joint Health Overview and Scrutiny Committee.
All very intertwined and not very independent looking.
The ICB could not even produce a formal position specification/ job description, answering pitifully:
“Further specifics are being scoped with system partners”
And if it was all innocent, why was there a need for the carefully crafted, coordinated statements which omitted to mention that Rosser had not actually left UHB at all?
Why was the word “regional” tacked onto the role, giving the impression of distance from local arrangements?
Would the man on the Clapham Omnibus think that it all looked a bit furtive and collusive?
What were the ICB and NHS England trying to hide?
We will likely hear more as the threads continue to unravel.
Oh, and Bewick’s phase 1 report on UHB was published today, with a good many departures from his terms of reference, through substantial omissions.
We can at least thank Dr Bewick for helping to expose the situation further and for additionally making the case for a judge led inquiry with powers to protect vital witnesses who have had to remain silent so far.
UPDATE 3 April 2023
I asked the ICB if Mike Bewick had been in on the contrived fiction that Rosser had left UHB when he had in fact remained in UHB’s employ all along.
I have asked the ICB Chair Patrick Vernon to answer the questions clearly, as follows:
BY EMAIL
Patrick Vernon
Interim Chair
Birmingham and Solihull Integrated Care Board
3 April 2023
Dear Mr Vernon,
Circumstances of David Rosser’s employment and information disclosed to Mike Bewick
Thank you for the further FOI response from the ICB on this matter.
I feel the ICB has not responded to my FOI request. It has answered past the point and possibly disingenuously.
The ICB has stated in its response that Mike Bewick knew about the circumstances of David Rosser’s new role because they came into the public domain on 18 November 2022, when David Rosser’s appointment to the regional role of “Strategic Director of Regional Digital Health and Care” was announced, before Mike Bewick took on the UHB review.
Also, the ICB indicated that Mike Bewick was nonetheless informed of these details upon being appointed by the ICB, [to undertake the phase 1 rapid review of University Hospitals Birmingham NHS Foundation Trust].
However, in my FOI request I specifically asked the ICB if Mike Bewick has been informed of the fact that David Rosser had been “hosted” by the ICB and was reporting to the ICB chief executive.
These facts were disclosed to me only via an ICB FOI response in February 2023.
It was not public knowledge that David Rosser had in fact, as the ICB admitted in February, remained in UHB’s employment.
This was despite coordinated press releases by both UHB and ICB which gave the impression that he had left UHB.
These facts about his continuing employment by UHB and secondment to the ICB did not come into the public domain until late March when they were revealed by the BBC: first by Michele Paduano, and then Newsnight on 28 March 2023.
Accordingly, could the ICB provide a response to my specific questions as follows.
Did the ICB inform Mike Bewick upon appointing him, to undertake the phase 1 rapid review into UHB, that David Rosser:
a) Was still employed by UHB?
b) Was “hosted” by the ICB?
c) Was reporting to the ICB CEO?
Please also advise of an additional matter:
1) Upon being contracted to undertake the phase 1 rapid review of UHB, did Mike Bewick inform the ICB of the basis upon which he called himself “Professor”?
2) Did Mike Bewick provide the ICB with details of his qualifications and how he came by this title of “Professor”?
By Dr Minh Alexander retired consultant psychiatrist 26 March 2023
My apologies for a late post. This is due to a combination of illness and an excess of commitments.
As many whistleblowers, patients and bereaved families will know, the Care Quality Commission is fond of fending off concerns by labelling them as “complaints”. This is because CQC claims that it has no remit to investigate individual “complaints”.
CQC’s refusal to investigate countless serious matters, using this ploy, has caused endless frustration and distress. Importantly, it has wasted many opportunities for learning and public protection.
However, the regulator does have a duty under CQC Regulation 12, 2014, to investigate incidents that tend to show a failure by a regulated provider to provide “safe care and treatment”.
The CQC has powers to prosecute under this regulation. Clearly, in order to do so, it must first investigate.
Baby Harry Richford’s death and Regulation 12
An example of CQC’s unreliability arose in the case of baby Harry Richford’s death at East Kent.
CQC initially told his family in 2018 that it was unable to investigate their concerns and also that his death did not fall under Regulation 12.
The details of this matter were previously summarised here.
CQC came to an initial conclusion that no organisational failings contributed to Harry’s death. This was despite:
1. The trust’s own internal incident analysis concluding explicitly that there were systemic failures which contributed to Harry’s death:
“This leads us to conclude that this incident occurred due to system failures.”
Some of this was echoed in external reports at the time.
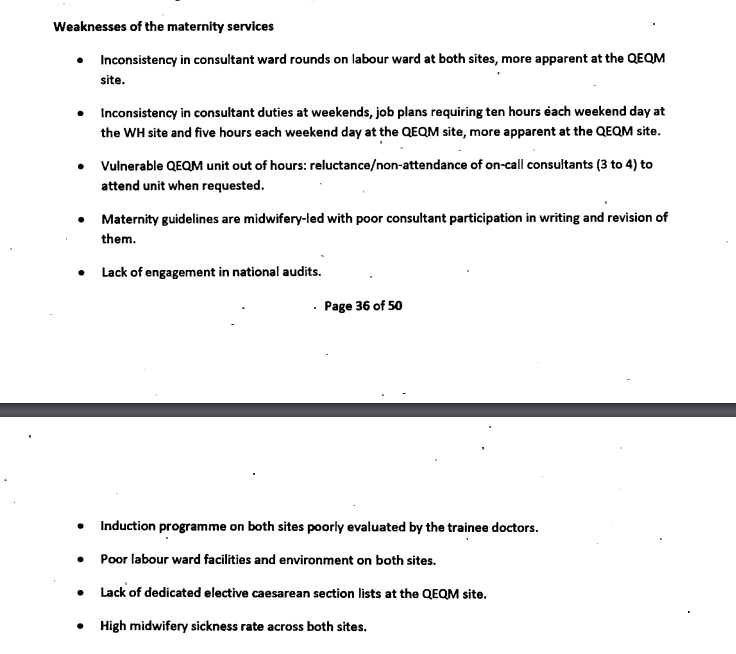
2. A 2015 Royal College review which had also previously identified systemic failings in the maternity service.
The systems failings identified by the Royal College included:
There had also been other signs of organisational failure by that point. Bill Kirkup’s October 2022 report on East Kent noted that the CCGs had raised concerns about maternity safety. CQC also received a whistleblowing disclosure from a consultant obstetrician in 2015 about poor leadership in East Kent’s maternity services. CQC received other disclosures about the culture of the maternity service. CQC itself found issues of culture in maternity services in 2014 inspection, when it rated the whole trust “inadequate”.
Despite the above evidence from multiple sources, the CQC claimed to Harry Richford’s family in 2018 there was only evidence of failings by individuals and not by the trust, and this meant that CQC Regulation 12 did not apply:
“After an extensive review, we do not believe there has been a breach in regulation. The concerns raised in this incident are centred on an individual’s decision or error. The criminal offences CQC can prosecute against only apply to registered person failures.”
However, the regulator later admitted that it had a remit under Regulation 12 to investigate Harry’s death.
The CQC replied defensively on 24 November 2022, acknowledging that it had erred only in respect of the fact that its local inspector had used “conclusive” language when informing Harry Richford’s family in 2018 that Regulation 12 had not been breached.
“When Emma Carroll drafted her email of 17 August 2018, the local team, based on the information they had available at that time could not establish all of these elements. However, in Emma’s email, she unfortunately used conclusive language. After the conclusion of our prosecution. we carried-out a learning review of the investigation and within that we highlighted Emma’s correspondence to the family in August 2018. The learning point was that, for any potential offence and after any initial assessment, further information can always come to light and therefore we should not use categorical language in our communication with victims and families which states a conclusive position.”
CQC focussed on the fact that she should have explained to the Richfords that new information might change CQC’s assessment.
The CQC contended that because it was tracking Harry’s inquest, it had not closed its file, and was still investigating.
There was nothing in this response about the quality of the 2018 CQC appraisal of Harry’s case, or any admission or explanation of why CQC had bizarrely overlooked ample evidence of organisational failure that existed by 2018, or why it had failed by that point to obtain a copy of the Royal College report.
But then, neither did Bill Kirkup fully acknowledge CQC’s failings in his recent report on East Kent. His main, repeated focus was on denial by East Kent managers.
Kirkup did make limited references in his report to missed opportunities by the CQC, but it would not do to direct too much fire at the powerful.
A bit like the strange silences about senior managers at Frimley, contrasted with the heavy focus on cover ups by frontline staff in his report about baby Elizabeth Dixon’s death.
But coming to the main point, CQC conceded in November 2022 correspondence that if it receives information about a possible breach of Regulation 12, such disclosures would be considered as part of CQC’s “assessment” about the purported breach:
So, don’t let CQC kick your concern into the long grass by framing it as a “complaint”.
Rather, insist – if it is so – that your concern engages Regulation 12.
UPDATE 9 April 2023
A coroner’s inquest has revealed that the CQC badly failed very vulnerable older patients at a HC-One home, by failing to act on numerous concerns.
Three residents died in February and March 2019.
One family member contacted the CQC NINE times to raise concerns.
The CQC did not inspect the home until August 2019.
By Minh Alexander NHS whistleblower and Martin Morton Social Work whistleblower 22 March 2023
The Care Quality Commission is the quality regulator for health and social care in England. It is supposed to be an impartial guardian of care standards and accountable to the public.
In reality, CQC was created in the aftermath of government embarrassment by a previous health regulator which uncovered the MidStaffs disaster.
The CQC was not intended to repeat such embarrassment and its first CEO was in fact the former CEO of the West Midlands SHA, a body that was central in the Mid Staffs disaster.
All told, the CQC has proven to be a politicised and suppressive organisation.
It has failed countless whistleblowers, including its own. This all the worse for the fact that CQC is a Prescribed Person under UK whistleblowing law and should at least not harm whistleblowers, whether by act or omission.
However, last year, the regulator was proven to have seriously harmed a CQC whistleblower in the ET case of Kumar v CQC.
The government has allowed the CQC to investigate and control investigations into itself regarding this spectacular failure.
At least one of these investigations, a barrister led review of the Kumar case and a mysterious, undisclosed sample of other whistleblower cases, should have reported by now, but nothing has been released into the public domain.
CQC’s whistleblowing governance reviews
Sparse terms of reference for the CQC reviews post Kumar v CQC were issued.
It was not disclosed how the additional whistleblower cases for review were chosen. CQC instructed a barrister from Matrix Chambers. FOI enquiries revealed that
In the meantime, the CQC has shown itself to be disingenuous despite its glib claims that it would learn from the Kumar case.
In an internal briefing to CQC staff in September 2022, disclosed via FOI, CQC’s CEO Ian Trenholm claimed shortly after the ET loss that both the CQC and the National Freedom To Speak Up Guardian had good track records on supporting whistleblowers.
Trenholm also decried CQC’s critics.
Is denial a novel technique for creating a safe environment that helps staff to raise concerns?
CQC’s failure under FOIA to produce all of its Freedom To Speak Up Guardian reports
When this obvious error was pointed out, CQC reverted to silence. It has still not properly responded to the FOI request.
Some of CQC’s internal Freedom To Speak Up Guardian reports were actually published via CQC board papers, but not all seem to have been released. There are gaps in the timeline of published reports, taken from archived CQC records.
The chief executive and CQC board will be given high level information about all concerns raised by our staff through this policy and what we are doing to address any problems. The CQC Guardian will produce a report twice a year to the board setting out the volume and type of concerns that have been raised, without identifying individuals. The board supports staff raising concerns and wants you to feel free to speak up.”
The CQC’s silence in response to the request for all its Freedom To Speak Up Guardian’s reports is troubling. Are important matters being concealed? Were some of these reports produced for internal consumption only, and have they been improperly withheld from FOIA disclosure?
Of the so far published CQC Freedom To Speak Up Guardian rreports, these present superficial data which raise more questions than they answer. Links to these uploaded CQC reports and some examples of how limited data is presented in these reports is summarised here.
CQC denial of detriment and dissembling about feedback about its Freedom To Speak Up process
In the course of the above FOI correspondence about CQC’s whistleblowing governance, CQC implausibly denied that there had been any detriment suffered by employees in 131 recorded speaking up cases over five years:
“…we can inform you that nobody raised that they feel they have suffered detriment as a result of speaking up.”
Curiously, despite being adamant that there was no detriment in any of these 131 case, CQC claims it is unable to answer a question about its employees’ satisfaction with the CQC speaking up process.
This allegedly because it would have to manually review files and this would take too long.
CQC has claimed a slew of other FOIA exemptions as well, indicating how reluctant it is to answer this very basic question about whether its staff are satisfied by their speaking up experiences.
Number of cases raised with a patient safety element
Number of cases raised with an element of bullying or harassment
Number of cases in which detriment occurred
Professional background
Feedback: “Given your experience, would you speak up again?”
There is a published national dataset based on this reporting system.
The so far published CQC Freedom To Speak Up Guardian reports do not reveal most of this required transparency data.
CQC’s internal whistleblowing policy gives cursory guidance on what records are made:
“What will we do? We are committed to the principles of the Freedom to Speak Up review and its vision for raising concerns, and will respond in line with them. We anticipate that some concerns may be capable of being dealt with informally to the satisfaction of all concerned, without contacting the ambassadors. If you choose to go through one of our FTSU ambassadors, your concern will be recorded and you will receive an acknowledgement within two working days. The central database will record the date the concern was received, whether you have requested confidentiality, a summary of the concerns and dates when we have given you updates or feedback, and any lessons learned.”
“To keep up to date records, recording contacts, concerns and outcomes in line with the CQC Freedom to Speak Up recording policy and process”
How did CQC know that no detriment has been reported via its Freedom To Speak Up arrangements? Was this a non-evidence based claim? Or is there collated data that is being withheld from the public, contrary to practice in the rest of the NHS?
If CQC is not collating data such as to whether its staff are satisfied with their experiences of the Freedom To Speak Up arrangements, through indicators such as whether they would speak up again, how can it claim to be learning?
CQC received the Kumar v CQC judgment in August 2022. The regulator has had over six months to reflect. The fact that it might be still failing to collect whistleblower feedback, ignoring the feedback or hiding the feedback is a very poor reflection on its intentions.
In fact, CQC’s Director of Engagement recently admitted in correspondence that CQC does NOT collect feedback from whistleblowers.
If so, why did CQC not simply admit this omission in its FOI response, instead of claiming that it would not produce the data due to an FOIA cost exemption?
“…there is only limited feedback available from those who have raised concerns with us about their experience of those processes and, therefore, how this might be improved.”
And yet CQC did not act on this. This is more evidence of CQC’s failure to take whistleblowing seriously.
Overall, it seems likely from the above inconsistent facts and CQC claims that there is dissembling in some manner, in addition to probable competence deficits.
Lastly, one of the authors has received information which contradicts CQC’s claim of zero detriment in 131 speak up cases.
This is hardly surprising, especially when CQC’s 2021 staff survey showed that only 49% of staff thought that it was safe to challenge the way things are done at the CQC, and that 10% of the staff who did not think it was safe reported that they had experienced repercussions as a result of speaking up previously.
So whatever is reported in CQC’s forthcoming reviews of its own whistleblowing governance, it would be safe to conclude that the reality is worse.
PETITION
Please click and add your signature to this petition to reform UK whistleblowing law – whistleblowers protect us all but weak UK law leaves them wholly exposed and it is a threat to public safety
Prior to this period, UHB’s predecessor body Heart of England NHS Trust published spending transparency data, but there appears to be no trail of UHB doing so.
In the last five years, UHB has resisted FOI requests for this data, and it has only released data when ordered to do so by the Information Commissioner.
Under a new Chair, UHB has now released all five years of hidden spending data in response to an FOI request. It has done so late, and only after an indication that a referral would be made to the ICO if there was any further delay.
The material was supplied in an unhelpful form, with entries mixed up in random date order, with some material from outside of the requested period mixed into the data.
In its FOI response letter, UHB claimed that the decision to stop publishing financial transparency data was made collectively at the executive director level.
Surprisingly, UHB claims that this important decision was not recorded.
“We do not hold this information, as the decision referred to above was not formally recorded”
The spending data is now being shared partly to ask for help from all to assess if there is any possible reason why UHB has been so secretive in hiding this financial data from public view.
If anyone thinks they understand why there has been such secrecy, please do send comments to BBC Newsnight or Michele Paduano BBC Midlands Health Correspondent, who are covering UHB.
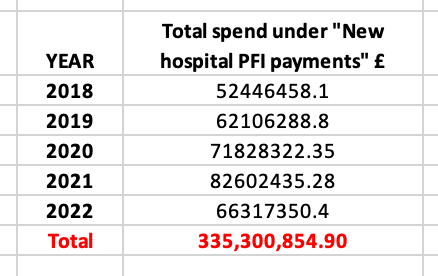
I have started organising the FOI data into years and under different areas of expenditure.
This is a spreadsheet of the data sorted into each of the five years, with extraneous years removed:
The data still contains items that were not asked for, in terms of spending amounts under £25K, but if desired, these can be excluded using the “filter” option on Excel.
There was no indication from UHB on whether all transactions under £25K had been included in the released data.
For the purposes of a quick and dirty look at the data, I am including all items of expenditure in the five year period, even in the knowledge that UHB may not have released all items of spending under £25K.
The data seems to be missing some items of expenditure currently under investigation by BBC Newsnight. It may well be incomplete in other respects.
We already know that UHB released inaccurate information about GMC referral outcomes, and has so far failed to correct this despite several approaches to the interim trust Chair Yve Buckland.
We have also seen UHB excoriated by the Employment Tribunal for withholding such a large number of significant documents in the Reuser whistleblowing case that the judge determined that he could not rule out deliberate dishonesty by UHB or similar future failures by trust management.
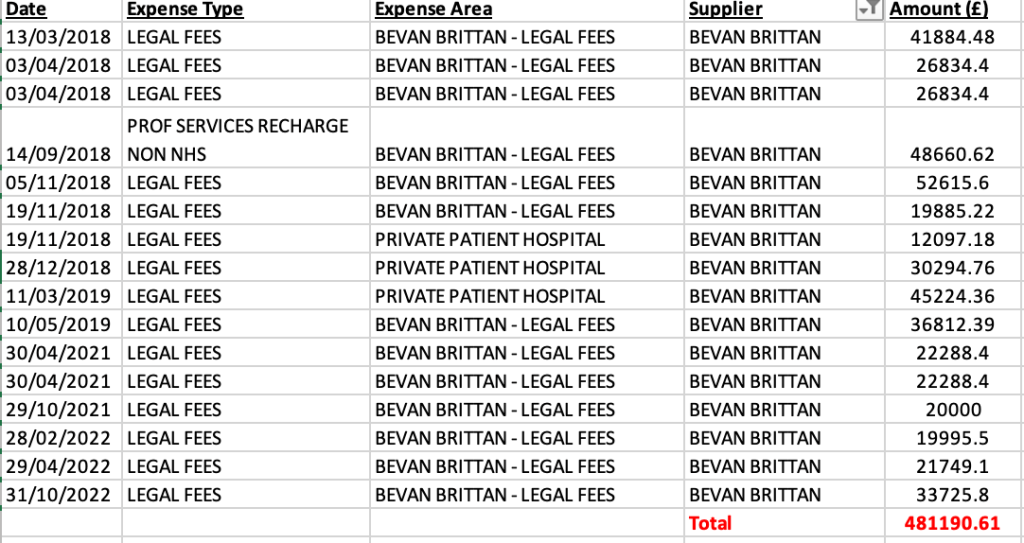
Bevan Brittan was the law firm which co-authored an FPPR investigation which reportedly cleared former UHB CEO David Rosser. I say “reportedly” because the report has never been published.
According to this disclosure: UHB spending on Bevan Brittan’s services in the five year period came to a total of £481,190.6 and broke down as follows:
Litigation continued after March 2020 as Tristan Reuser’s case in the EAT and ET rumbled on, there was an FPPR investigation involving a Bevan Brittan partner and David Rosser’s GMC defence was, according to an observer at a trust meeting, picked up by the trust. These alone would have incurred substantial costs.
University of Birmingham
As a teaching hospital trust, UHB is closely linked to the university.
According to the disclosed spending data, UHB spent a total of £50,286,941.81 on 247 transactions with UHB in the five year period.
A spreadsheet giving details of the transactions can be found here.
Alongside this financial relationship, the University was asked about whether it should now withdraw its award of an honorary professorship from David Rosser in the light of ET, GMC and other findings. It has not so far responded.
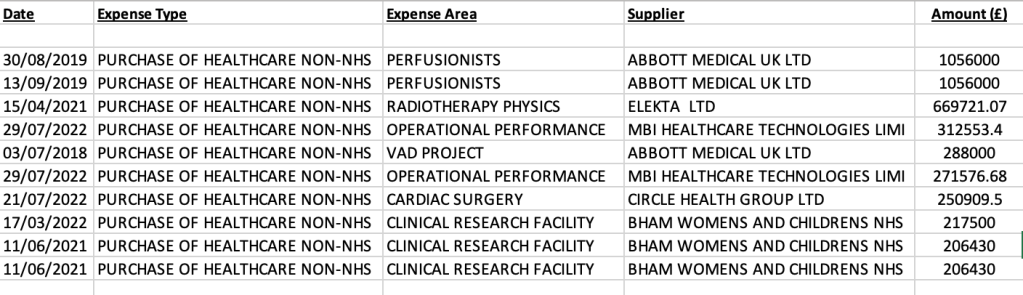
Purchase of “Healthcare Non NHS”
Under this category, UHB made a total purchase of £86,081,036.99 in the five years covered by the FOI.
The largest ten payments were as follows:
Cumulatively, UHB paid the most to Diaverum and Fresenius Medical Care.
There were 1396 payments to Diaverum UK ltd and Diaverum Facilities Management, totalling £33,938,705.2
There were 1383 payments to “FRESENIUS MEDICAL CARE RENAL”, totalling £22,743,634.4
A spreadsheet of all transactions listed under “Healthcare NON NHS” can be found here.
UHB Facilities Limited
In 2013 UHB set up a subsidiary company, UHB Facilities Ltd, reportedly for the purposes of VAT advantages.
The company’s current officers/directors include David Burbridge UHB Chief Legal Officer, Mike Sexton Chief Finance Officer, Peter Hirons UHB Facilities Manager,
UHB Facilities Ltd has a Financial Controller, Karen Cutler, and a commercial director Alan Ewan, for whom I cannot identify roles at UHB.
In the five years covered by the FOI, UHB paid UHB Facilities Limited a total of £14,067,213.71.
A spreadsheet with the details of the transactions can be found here.
Assure Dialysis Services Ltd
UHB set up another company in 2013, UHB Satellite Dialysis Limited.
“Assure Dialysis Services is a venture providing dialysis care for the patients of the Queen Elizabeth Hospital Birmingham (QEHB) and we therefore have an extensive partnership with University Hospitals Birmingham NHS Foundation Trust, which manages QEHB.”
Another part of the website stated:
“Smethwick Dialysis Centre (SDC) is a satellite dialysis unit of the Queen Elizabeth Hospital Birmingham. It functions like all other satellite units and a QEHB consultant manages patient care alongside the staff at Smethwick Dialysis Centre.”
The current company officers/ directors are David Burbridge UHB Chief Legal Officer, Dr Mike Hallissey, UHB Medical Director of Education, Robert Watkins Senior Finance Manager UHB.
David Rosser was previously a director of Assure Dialysis Services Ltd between 2014 and 2018.
Dr Clara Day was previously listed as one of the doctors who worked at Assure Dialysis Services Ltd.
Clara Day is now Chief Medical Officer of the ICB which is controlling the reviews of UHB.
In the five years covered by the FOI, UHB reportedly paid the company a total of £4,670,604.76.
A spreadsheet with details of all disclosed transactions can be found here.
Pharmacy@QEHB LTD
UHB set up this company in 2011.
Current company officers/directors include David Burbridge UHB Chief Legal Officer, Yma Choudhury UHB Managing Director Division 1, Mike Sexton UHB Chief Finance Officer and Inderjit Singh UHB Chief Pharmacist.
In the five years covered by the FOI, UHB reportedly paid Pharmacy@QEHB LTD a total of £265,122,325.5.
Details of the transactions can be found in a spreadsheet uploaded here.
Circle Health Group
Cardiology and cardiac surgery services have been controversial at UHB, with critics citing the trust’s scapegoating of cardiac surgeon Ian Wilson, whom they believe was unfairly vilified through the trust’s alleged manipulation of the media and irregular use of data.
Moreover, the BBC revealed in January that UHB has a cardiac surgeon – Neil Howell – who has been paid for five years but has not operated;
The BBC has learnt heart surgeon – Neil Howell – on the left – – hasn't operated for 5yrs – doesn’t appear on the trust web site – but has been paid throughout. UHB says it stands by its investigation, but cannot comment on a current employee @bbcmtdpic.twitter.com/A96ohoj4wk
Of the total paid of £2,858,365, £2,800,693 of this was accounted for by expenses areas “cardiac directorate” and “cardiac surgery”, including £1,359,461 expenses described as “management consultancy fees”.
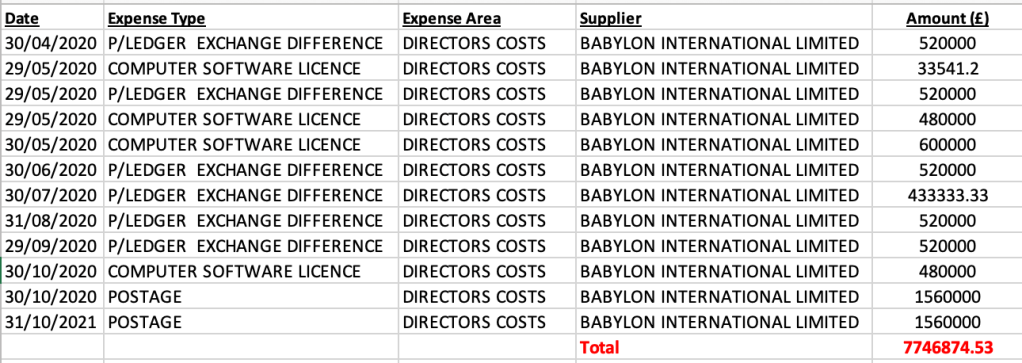
This is what UHB has disclosed about its spending on Babylon – a total spend of £7,746,874.53:
There are a multitude of other stories and information contained in this financial data. I hope it is of interest to some and helps to shed more light on UHB.
With best wishes.
Minh
RELATED ITEMS
Transcripts of BBC Newsnight broadcasts about UHB:
Dr Minh Alexander retired consultant psychiatrist 15 March 2023
The University Hospitals Birmingham scandal continues to unfold like a slow motion car crash.
Birmingham and Solihull Integrated Care Board currently nominally hold the poisoned chalice of managing the UHB reviews, but seem very much out of their depth.
Also, BBC Newsnight has revealed that the ICB CEO wrongly told the Joint Health Overview and Scrutiny Committee that Parliamentary and Health Service Ombudsman’s concerns about UHB had been resolved, when this was anything but the case.
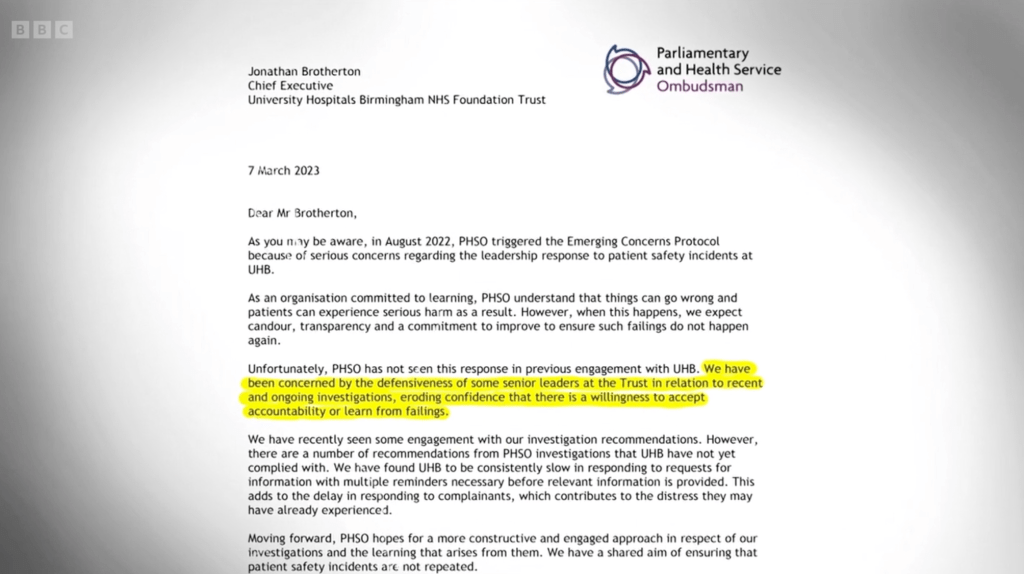
The PHSO continues to be vocally concerned about UHB. His public intervention amounts in my view to a thinly veiled accusation of a high-level cover up, and with some face validity.
Astonishingly, PHSO shared correspondence with Newsnight and gave an interview to Newsnight about his concerns, which featured in a broadcast of 14 March 2023.
Extraordinary times when agencies are “whistleblowing” about each other.
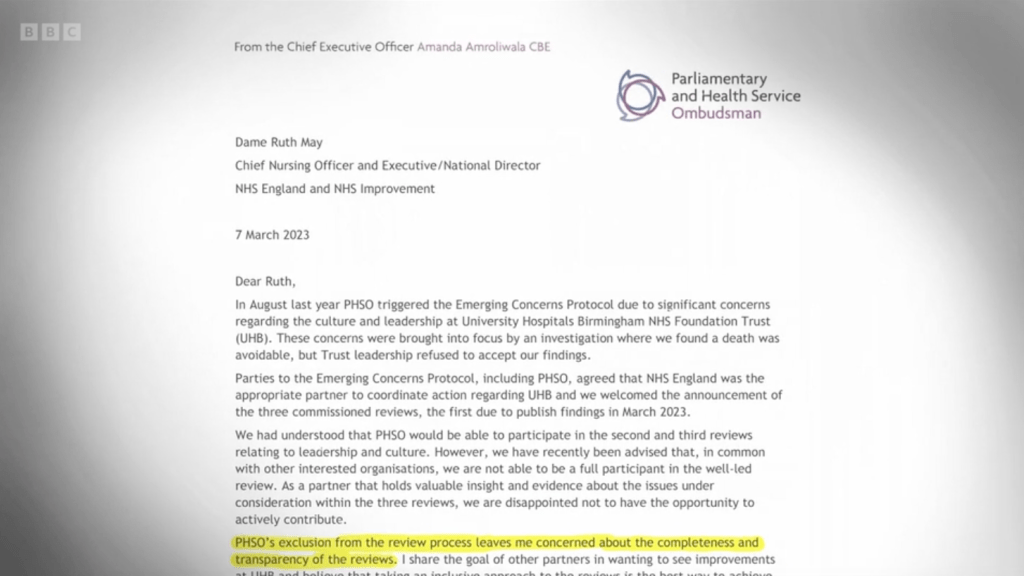
My transcript of the relevant sections of the programme and screenshots of disclosed correspondence to Ruth May NHS England CNO and the current UHB chief executive Jonathan Brotherton is provided below.
Scandalous though recent events have been, NHS England is by its opacity and incompetence actually helping to make the case for a properly independent judge led inquiry, with powers to protect witnesses.
EXCERPT FROM 14 MARCH 2023 BBC NEWSNIGHT BROADCAST
“Kirsty Wark BBC: In an exclusive interview safety investigator the Parliamentary and Health Service Ombudsman the last port of call for people who are unhappy with the NHS in England tells Newsnight of his serious concerns about the different roles and his difficulties investigating University Hospitals Birmingham. Here’s David.
David Grossman BBC: For the past six months Newsnight has been investigating one of England’s worst performing health trusts. We were repeatedly told it had a toxic culture. We heard from a governor of the trust who said he resigned after his warnings were ignored.
We heard allegations that patient safety warnings were ignored. And from doctors who feared that if they spoke up they’d be punished. Despite strenuous denials from UHB, NHS England took action. From the very moment that these reviews were announced, we were warned by insiders in the health service that they wouldn’t be rigourous or independent enough to get to the truth.
And now, in an unprecedented move, the most senior health service investigator in England the Parliamentary Health Service Ombudsman has complained to us that he has been excluded from giving evidence to the review.
He says he won’t be able to share the wealth of information that he’s gathered about repeated patient safety issues at UHB.
Rob Behrens Parliamentary and Health Service Ombudsman: By law and practice I’m the last resort for people who believe they’ve had either poor service or have been subject to some some clinical failure in the health service.
David Grossman BBC: Rob Behrens is the last chance investigator for health service complaints in England. If you’re unhappy with how your complaint has been treated, the Parliamentary Health Service Ombudsman and his team may look at it. He says they have to examine hundreds of complaints at UHB in the last three years, more than any other trust.
Rob Behrens Parliamentary and Health Service Ombudsman Some are about avoidable deaths, where unfortunately , sadly, tragically people have died on the balance of probability as a result of the failures of the clinicians to address the issues at the time.
David Grossman BBC: What’s been happening when you approach them?
Rob Behrens Parliamentary and Health Service Ombudsman A number of things. A lack of cooperation, a failure to engage with the Ombudsman in order to resolve cases and to learn from them.
The trust is continuously late or has been continuously late in providing us with the evidence which we’ve requested.
They have rejected our draft findings.
When we’ve had meetings to take the issues forward, under their previous leadership they were aggressive.
They failed to understand the seriousness of the issues and there was no learning culture in the organisation that we could see at all.
And that is very serious indeed because the issues are about patient safety.
David Grossman BBC: The Ombudsman was so worried about what was happening at UHB that last summer he took the extremely unusual step of issuing what’s called an Emerging Concerns Protocol to alert NHS England.
Rob Behrens Parliamentary and Health Service Ombudsman This is the first time that I have done it, so that represents the seriousness with which we regard these issues. So when the reviews into UHB triggered by Newsnight’s investigation were announced, Rob Behrens and his team fully expected to turn over their huge body of evidence of serious failings at UHB to those inquiries.
Rob Behrens Parliamentary and Health Service Ombudsman In those early days we figured our concerns we were told by NHS England that we would be invited to participate into the second of the reviews and subsequently that invitation was withdrawn.
And my concern, general concern that the NHS is not good about commissioning independent reviews to make sure there’s proper learning from what has happened. I need to be reassured that in this case, that is not also the case. But I’m sceptical.
David Grossman BBC: The Parliamentary Health Service Ombudsman and his team have written to NHS England have written to NHS England to protest about being excluded.
You’re sceptical about whether this is going to be the thorough job that you said needs to happen?
Rob Behrens Parliamentary and Health Service Ombudsman: Yes
David Grossman BBC: How serious is that?
Rob Behrens Parliamentary and Health Service Ombudsman: Well, it’s a serious issue for a patient safety organisation not to want to involve Ombudsmen, leaders and regulators in giving evidence to try and address the operational that have caused the inquiry to be commissioned.
To me, it doesn’t make sense.
David Grossman BBC: The reviews are being run by the Integrated Care Board in Birmingham and Solihull, part of NHS England. Even though the reviews haven’t been completed, the chief executive of the Integrated Care Board recently suggested to councillors that they wouldn’t find anything seriously wrong that would affect patient safety.
[At this point Newsnight showed footage of David Melbourne reporting to Birmingham and Solihull Joint Health Overview and Scrutiny Committee as follows:
“I did want to update you on where we were with the review commissioned following the allegations in Newsnight”
“All three of the reviewers were very clear that they would be happy for their families to be treated at University Hospitals Birmingham.”]
Rob Behrens Parliamentary and Health Service Ombudsman It does not chime with my experience. I’m surprised that at this stage someone would make a statement like that when the first review has taken place entirely in private. We don’t know what evidence has been taken.
I would need to see evidence documented before I accepted that view.
David Grossman BBC: The Ombudsman is so concerned about what’s happening at UHB that at the end of last week he wrote to trust management.
These concerns are entirely at odds with what the chief executive of the Integrated Care Board told local councillors.
He reassured them that any issues that the Ombudsman may have had, had quote “been resolved”.
[At this point Newsnight showed footage of David Melbourne ICB CEO telling the Joint Health and Overview Scrutiny Committee:
“What has happened is that has been… the issues Parliamentary Ombudsman raised have now been resolved through that process”]
David Grossman BBC: Is that your understanding?
Rob Behrens Parliamentary and Health Service Ombudsman It’s not my understanding. The issues in broad terms have not been resolved. A small number of issues have been addressed. But the reason I wrote to the new chief executive was to express my concerns that there was still a lot to do, and we needed convincing that change of culture was going to take place that was going to impact on operational practice.
David Grossman BBC: UHB told us that they’d responded to the Ombudsman’s letter to provide reassurances that his concerns were being taken seriously. They’d previously told us that patient safety is always their primary concern. The Integrated Care Board in Birmingham and Solihull they hadn’t heard from the Ombudsman, they would welcome the opportunity to provide assurances to the Ombudsman. A spokesman for NHS England Midlands told us that the three reviews have been commissioned to rigorously to scrutinise leadership and culture in the organisation to ensure they are providing safe care for patients, and that they welcome the offer of support from the Ombudsman’s Office.
The stated purpose of these reviews is to learn lessons and restore confidence in one of England’s biggest and most trouble health trusts.
But with such a significant voice as the Parliamentary Health Service Ombudsman questioning their rigour, that job looks harder than ever.”
UPDATE 8 APRIL 2023
The publication of Mike Bewick’s phase 1 report on UHB confirmed that he did indeed airbrush PHSO’s concerns and findings out of the picture.
Such an extraordinary omission could surely only have been carried out under instruction from NHS England or the Department of Health?
And yet the timeline of events suggests that PHSO’s interventions at UHB were significant in helping to set off the chain of events:
4 August 2022 PHSO triggered multi-agency Emerging Concerns Protocol about UHB
Further related meetings about UHB held on:
12 October 2022
10 January 2023
7 February 2023
18 November 2022 Rosser’s fictional “departure” from UHB announced
25 November 2022 New interim Chair for UHB announced
RELATED ITEMS
Regarding Mike Bewick’s and other’s honorary professorships:
By Dr Minh Alexander retired consultant psychiatrist 13 March 2023
There has been disquiet and rumbling controversy for some years about the fashion for those who do not have substantive chairs to style themselves as “professors” in everyday life.
Universities award the title of “Visiting professor” and “Honorary professor” to substantive professors from other universities as part of academic collaborations, as a legitimate convention.
However, “Visiting” and “honorary titles” may be bestowed on those who do not have substantive chairs, for a number of reasons. For example, some may be awarded honorary professorships in recognition of achievements in public life or more controversially, it has been suggested that such awards may be made to flatter or as a quid pro quo to the powerful or those who control the purchase of services from universities. Such as senior NHS managers.
“There is a real danger this could be seen as “grace and favor” or “quid pro quo” when an honorary award is made to someone in a senior position in an organisation that provides a service to, or is a “customer” of, the awarding university.”
Then there is the moot issue of whether such titles are misused by some, unwittingly or intentionally in some cases to polish their CV and personal presentation.
A number of compelling arguments against the practice of using honorary and visiting titles in everyday life are made in this paper, especially when the word “honorary” or “visiting” is omitted:
Perhaps it is time that medical institutions take a leaf out of this book.
Examples of honorary titles used in everyday life
There are many examples of individuals who style themselves as professors on the basis of apparently non-substantive posts. Here are three examples:
David Rosser former medical director and then CEO of University Hospitals Birmingham NHS Foundation Trust, now purportedly regional strategic director of digital health and care.
His trust University Hospitals Birmingham NHS Foundation Trust disclosed that this was based on an honorary professorship.
The awarding body was the University of Birmingham.
The University was asked if it condones his use of the title in day-to-day life. It has not yet replied.
2. Steve Field GP and former Chief Inspector of primary care Care Quality Commission, then Chair of Royal Wolverhampton NHS trust and later also Chair of Walsall Healthcare NHS Trust.
Field styles himself as “Professor”
A biog about Field, announcing his appointment to the organisation Policy Connect, stated that he held two honorary professorships at University of Warwick and University of Birmingham:
3. Mike Bewick GP and former Deputy Medical Director NHS England, who set up a private consultancy firm IQ4U Consultants Ltd after leaving NHS England, styles himself as “Professor” on his current LinkedIn profile.
Mike Bewick is of course currently in the public eye as he has been hired to conduct reviews on University Hospitals Birmingham NHS Foundation Trust after a scandal, exposed by BBC Newsnight.
He is represented on reports by his company IQ4U Consultants Ltd as “Professor Mike Bewick”.
I asked Mike Bewick about his use of the title “professor”.
He advised:
“I hold an honorary chair at UCLan only not a substantial professional one”.
I asked him why he used the title of “professor” in day-to-day life if it was an honorary title.
I have not yet received a response.
NHS England, the ICB, Preet Gill MP and Richard Burden Chair of Healthwatch (the latter two had agreed to chair and be part of external reference group on the conduct of Bewick’s reviews on UHB) all refer to Bewick as “professor”.
No doubt the title confers confidence in some people’s eyes.
But is it right that this title is used?
UCLAN, the body which awarded the honorary professorship to Bewick, says that it would not condone the day-to-day use of an honorary title.
See the UCLAN letter of 7 March 2023, copied below:
7 March 2023
Ref: FOI 2940
Dear REDACTED,
I am writing in response to your request for information regarding honorary titles (Ref FOI 2940).
No, the University does not condone this use of honorary titles.
If we became aware that the recipient of an honorary doctorate was styling themselves as “Doctor” inappropriately, we would inform them that this was not condoned.
If you are unhappy with the way we have handled your request for information, you are entitled to ask for an internal review; however, you must do so within 40 working days of the date of this response. Any internal review will be carried out by a senior member of staff who was not involved with your original request. To ask for an internal review, contact DPFOIA@uclan.ac.uk in the first instance.
If you are unhappy with the outcome of any internal review, you are entitled to complain to the Information Commissioner. To do so, contact:
There are many, many more examples of individuals who use honorary titles in the NHS.
I note that coinciding with enquiries to universities, two of the three examples given above have stopped styling themselves as professors in their twitter accounts.
Letter to the Secretary of State requesting policy review and better culture
I have written to the Secretary of State about regularising policy in the NHS on the use of honorific titles, for better culture.
BY EMAIL
Steve Barclay
Secretary of State for Health
13 March 2023
Dear Professor Doctor Barclay,
Use of honorary titles in everyday life in the NHS
Forgive my unconventional address but I write on the use of honorary titles in everyday life in the NHS, which in the main, universities do not condone.
Many senior NHS managers have been using honorary titles in a confusing and perhaps misleading way to represent themselves as professors and doctors etc when they hold only honorary titles.
“Dr” Paula Vasco-Knight the convicted fraudster was one of the most prominent examples.
Some have raised questions about whether or not academic institutions have made these awards to flatter the powerful who hold budgets that universities wish to access.
I would be very grateful if you address this policy issue and ensure that these matters are regularised, to set a better example on probity and moderation.
Many thanks and best wishes
Yours sincerely,
Dr Minh Alexander
Cc Amanda Pritchard CEO NHS England
Steve Brine Chair of Health and Social Care Committee
Mr Peter Seaby was a vulnerable resident, with a diagnosis of Down’s Syndrome, at the Oaks and Woodcroft care home in Norfolk. The care home is run by Conquest Care Homes (Norfolk) Limited, which is owned by the Priory Group.
Mr Seaby was at risk of choking and of aspirating food into his lungs (which causes serious infection). He required a special diet and supervision at mealtimes. These needs were reflected in his care plan.
However, according to a recent coroner’s inquest, the care plan was not reliably carried out.
Mr Seaby did not always receive his special diet and he was sometimes not supervised at mealtimes.
This did not accord with the provider’s published claims that the care home provides “person-centred” care:
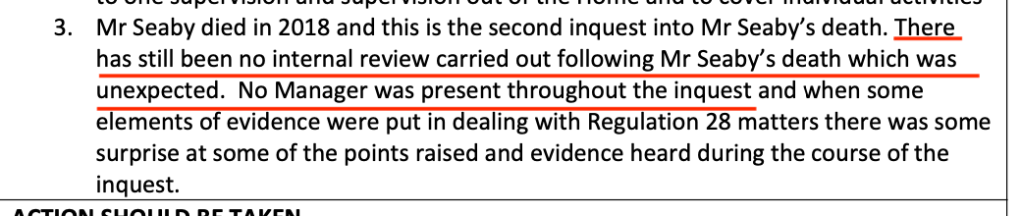
Peter Seaby sadly died of aspiration pneumonia. A piece of carrot was also found lodged in his throat after death, showing that his care plan had not been properly followed. He was aged 63.
The outcome of this inquest and how it was handled by the coroner Yvonne Blake was challenged by Mr Seaby’s family through judicial review, leading to the latest inquest:
After the second inquest, which commenced in July 2022, the coroner Jacqueline Lake determined that the primary cause of death was aspiration pneumonia, to which poor care possibly contributed:
“Mr Seaby died of aspiration pneumonia. Inadequate preparation of his lunchtime meal and inadequate supervision at his lunchtime meal possibly contributed to his death.”
She also issued a Prevention of Future deaths (PFD) report, addressed to the care provider in February 2023.
In her PFD, the coroner was concerned about under-staffing at the care home which meant that patients who needed one to one supervision did not always receive it, as in Peter Seaby’s case.
It was previously reported that on the day before his death, Peter Seaby served himself at a meal, whilst a carer was attending to another resident.
Of huge concern, there still appeared to be no internal review of Mr Seaby’s death by the Priory group.
No manager from the provider even attended the second inquest, a matter noted by the coroner as above.
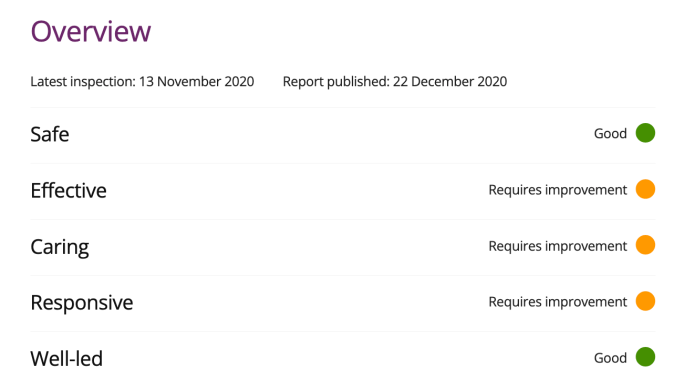
And yet the Care Quality Commission inspected the home in November 2020 and rated the home “Good” on the Well Led domain.
In December 2020 the CQC made the following observations about risk assessment and care plan management, which seemed to rely mostly on scanning documentation, as opposed to checking that care plans were actually delivered:
“There was good oversight and management of risk. We found however that at least one person had regularly refused blood tests due to high anxiety levels. This was now being addressed through a desensitization programme but previous barriers to accessing health care had not been addressed in a timely way.”
“Both care plans and risk assessments for people were clearly written and reviewed in line with changing need and risk. Although a key worker system meant all staff had responsibility to oversee people’s care, most of the documentation had been written by the deputy manager. Not all the documentation demonstrated a collaborative approach or showed who had been involved in collating information or who was involved in best interest decisions.”
The CQC inspection report did refer glancingly to audit, but again relied on audit data produced by the provider:
“Audits helped ensure policies were being followed and regular checks were carried out to ensure the environment remained safe and free from hazards. We sampled some health and safety records, and these were in order.”
The CQC was glowing about the unit’s good governance and learning from incidents:
“Since the last inspection a manager had been appointed to work solely at this location whereas previously one manager oversaw two separate locations. There were good overarching governance processes and the registered manager was well supported. Audits helped to identify any areas for development and there was a robust action and development plan in place. There was oversight of accidents, incidents, safeguarding and near misses. These were reported and analysed to help identify actions taken at the time and to ensure these were appropriate so lessons could be learnt. The outcome of which were shared with staff.”
It is hard to square this with the coroner’s discovery that the provider had not even internally reviewed Mr Seaby’s possibly avoidable death.
Alarmingly, it appears that CQC had been warned of problems at the care home prior to its November 2020 inspection:
“Concerns were received about this service which meant we brought the inspection forward and looked at three key questions where we had previously identified breaches of regulation.”
So in context, there should have been special diligence in carrying out the November 2020 inspection of The Oaks and Woodcroft, with proper verification of the provider’s claims.
“People had documented dietary needs, but some information was contradictory, and staff also gave us contradictory information which could increase the risk for people at the service not getting their dietary needs met or risks of choking fully mitigated. A recent incident had been referred to the safeguarding team and we are waiting for the outcome which is linked to people’s dietary needs and changing care needs.”
So if aware, the regulator should have been actively tracking the provider’s handling of the serious untoward incident, and it should have picked up any failures to carry out an internal review or to genuinely mitigate risks to other service users.
We are a decade on from the death of Connor Sparrowhawk and ensuing scandal over Southern Health.
CQC also failed badly on that previous occasion. CQC failed to either identify or report that hundreds of deaths of mental health and learning disabled people had not been investigated, as later revealed by the 2015 Mazars report.
How much longer should the public wait for a reliable regulator?
By Dr Minh Alexander retired Consultant Psychiatrist 7 March 2022
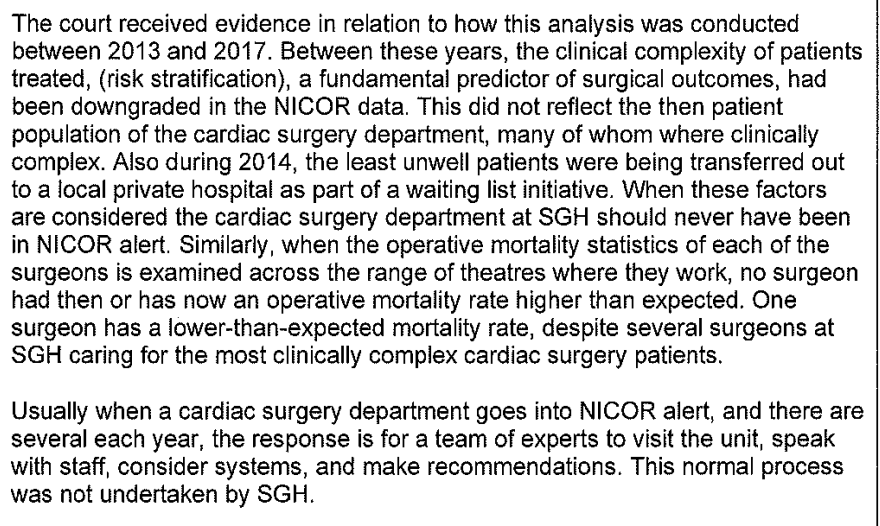
A controversy rumbles on about the cardiac surgery service at St Georges, where some allege that NHS England/ Improvement took a very heavy handed approach to mortality alerts. Mortality alerts do not prove that a service is unsafe, but they signal a need for review.
Several investigations took place of the St George’s cardiac surgery service, which was a specialist centre caring for patients with more complex needs, that sometimes presented greater surgical challenges.
This culminated in the so-called Lewis review by NHSE/I, which ended with 67 cases being referred to the coroner with allegations of poor care. The senior coroner dealing with these cases has so far rejected the vast majority of the Lewis review’s findings and criticised the review’s methodology. Some of the inquests remain to be heard.
These are some of the comments by the senior coroner on the St Georges affair:
However, a whole team of cardiac surgeons was also referred to the General Medical Council following NHS England’s “Lewis” review, but I understand all referrals ended with a “no case to answer” outcome.
“The surgeons and referring cardiologists had full visibility of the SJRs for cases where they were involved and were able to collate significant responses and material that was submitted to the panel. This was initially a 2 week period for response, but extensions were granted where requested. As mentioned above, full consideration of their opinions and additional information provided was given over a number of days across a 3 month period. This resulted in updates made to the SJRs, factual accuracy checks and reconsideration of opinion where appropriate. We do not agree with the suggestion in the PFD that this feedback “was mostly ignored”.
A recent “Lewis” inquest into the death of Mrs Maureen Brett, which I observed, gave rise to conflicting evidence. First hand evidence from clinicians and from Mr Mike Lewis himself (the chair of NHSE’s review) revealed that not all parties were given sight of the draft Lewis report or a right of reply.
Mike Lewis himself told the inquest that he asked for Salmon letters to be sent to relevant individuals, but he was not responsible for overseeing the process. If he received no responses, he assumed that the individuals had no comment to make.
I wrote to both Amanda Pritchard CEO of NHS England and to Stephen Powis about the concerns regarding NHSE’ Salmon process. Neither have replied.
I have also contacted a senior medical manager from NHS England, who was a contact point for St. Georges, to ask for information on who was responsible for NHS England’s Salmon process. He has not responded either.
The Bewick report on cardiac surgery at St Georges
The Lewis review was preceded by the briefer Bewick review on cardiac surgery at St. Georges.
Bewick’s 2018 report on cardiac surgery can be found here.
An FOI request has revealed that the review by Mike Bewick GP and former Deputy Medical Director of NHSE England, was commissioned by the trust with the “support and guidance” of NHS Improvement, a predecessor body of NHS England.
The FOI response from St Georges can be found here.
St. Georges stated in its FOI response:
“The Trust appointed Professor Bewick, a former Deputy Chief Medical Officer at NHS England, to lead the independent external review because he had specific experience of conducting similar reviews into cardiac surgery at NHS trusts in both Leeds and Bristol.”
“The Trust’s commissioning of the independent external review and the appointment of Professor Bewick was with the support and guidance of NHS Improvement.” [my emphasis]
In response to a question about the tendering process for this review, St Georges replied:
“Direct award, as provided for under the Trust’s Standing Financial Instructions.”
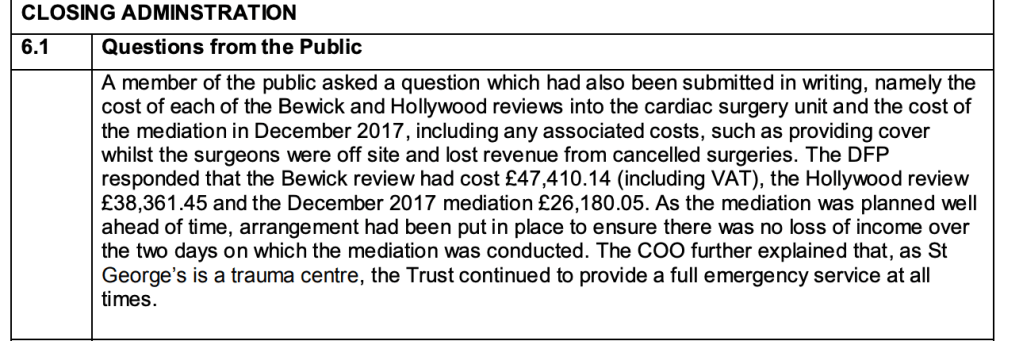
The Bewick review of cardiac surgery cost St Georges £47,410.14, as noted in trust board papers:
It is perhaps relevant to mention that St. Georges dragged its feet on the above FOI about NHSE’s involvement in the Bewick review, despite several reminders. The trust only issued a response after the matter was referred to the Information Commissioner.
All eyes are on Mike Bewick again, as he was recently commissioned by the Birmingham and Solihull ICB to carry out an urgent review, one of three, of University Hospitals Birmingham NHSFT (UHB) after revelations by BBC Newsnight of alleged bullying, safety concerns and governance failures by the trust.
This cannot be reassuring at all for the many staff who have been brave enough to come forward, and I repeat my general advice that it is probably safest to disclose directly to the media at present, either anonymously or with agreement that identity will be protected. But do take personalised advice first.
Was Bewick appointed to review UHB with “support and guidance” to the ICB from NHS England?
PETITION
Please click and add your signature to this petition to reform UK whistleblowing law – whistleblowers protect us all but weak UK law leaves them wholly exposed, lets abusers off the hook and it is a threat to public safety.
NHS England has to date failed to give a straight answer on whether it has checked that there are no ongoing matters at Sussex that might call into question Griffiths’ suitability to investigate the NEAS affair.
Her former trust University Hospitals Sussex NHS Foundation Trust has been resistive to recent FOIs about its recent whistleblowing and HR governance.
Sussex claimed that it was unable to give any details about Employment Tribunal claims filed against the trust, including those filed under the jurisdiction code of public interest disclosure (whistleblowing). This was on the unlikely basis that there was no central file and that it would cost too much to retrieve the data manually.
The trust also claimed that it had no central data on settlement agreements and could provide no data on confidentiality clauses used.
I wrote to Griffith’s successor George Findlay CEO (who like David Rosser ex CEO of UHB was the former medical director of the trust) to question the claim that the trust could not even tell me about current Employment Tribunal claims against the trust.
I also suggested that if Findlay was following the recommendations of the 2015 Freedom to Speak Up Review and personally taking responsibility as CEO for the contents of the trust’s settlement agreements, he should be able to give me some idea of the trust’s approach.
I did not receive a reply from Findlay, but a further FOI response was issued by the trust which reveals that there are currently FOURTEEN live employment tribunal claims against the trust. The trust refuses to say if any of these cases include whistleblowing claims:
“There are currently 14 employment tribunal cases in progress. We are unable to provide any further information relevant to these cases (e.g. those that include a PID as per your request) due to the small number of staff involved and the risk of identification.”
Moreover, the trust discloses that it has dismissed staff by professional group in the three years 1 April 2019 to 31 March 2022 as follows:
(The total here is different from that given in the previous trust FOI response)
The trust claims the total number of medical staff dismissed in this period is six. Also, that six doctors were referred to the General Medical Council in this period.
The trust claimed that this is its current template for confidentiality requirements in settlement agreements:
“1. Confidentiality
The Employee understands and accepts that she/he/they will remain bound by any pre- existing confidentiality obligations in her/his/their contract of employment, including the obligation to keep confidential any patient confidential information and all confidential information and know how that the Trust may have disclosed to the Employee, whether orally, in writing or digitally which includes but is not limited to data, financial information, financial projections, financial records, spreadsheets, computer software, patient information and any information which has been given to the Trust in confidence and any other information which the Employee is told is confidential which the Employee has obtained about the Trust or its patients or its employees and its officers during the currency of the Employee’s employment, however obtained, and whether held on document, computer disc, tape or otherwise and not to publish that information to any third party without the prior written consent of the Trust.”
Sussex’s above confidentiality requirement purportedly contains no restriction on disparagement or disclosing the existence of the agreement or its contents, but it is otherwise more exhaustively drafted than NHS Employer’s template for confidentiality about past employment.
Whether or not it has more force in law, Sussex’s longer list of “must nots” may certainly make former employers more anxious about what they can disclose.
Sussex provided the template purportedly used for the last settlement agreement that it reached:
So, is it a sustainable argument for George Findlay and University Hospitals of Sussex NHS Foundation Trust to claim that the trust cannot disclose if it is facing any whistleblower detriment claims on grounds of privacy?
I hope that journalists will be testing this and exploring further, for the sake of patients at both North East Ambulance Service and at Sussex, and any Sussex whistleblowers currently suffering in the obscurity imposed by the processes that are inflicted upon them.
It seems NHS England, which allegedly has a conflict of interest through mismanagement of the original NEAS whistleblower disclosures, seems disinclined to ask hard questions.
This previously unpublished inspection report by Health Education England of surgical training at the trust revealed the dire state of governance at Sussex which was suppressed by the trust, with help by CQC and the National Guardian’s Office:
Did Griffiths and Findlay, who took over after an organisational merger, follow up properly on the governance issues arising from the case?
Are there persisting unsafe systems and practices that allowed the unfair dismissal of a doctor who raised patient safety concerns?
Have other doctors since been sacked by the trust after raising concerns?
But facts may be immaterial to regulators.
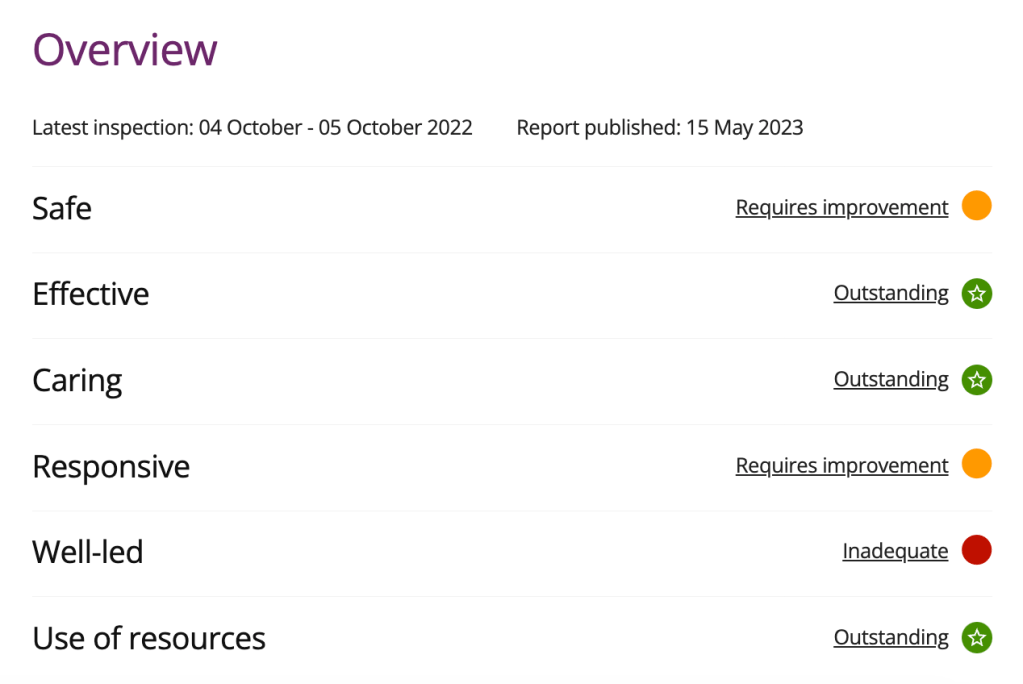
Sussex remains a favourite with the Care Quality Commission and retains its overall “Outstanding” rating from 2019 despite subsequent findings in 2021 of poor whistleblowing governance:
For all the trust’s pointless secrecy, one of the current whistleblowing cases will be heard next week at Croydon Employment Tribunal office. The case is scheduled to run from 5 to 16 June 2023.
This of course is deeply embarrassing for NHS England with regards to its investigation of North East Ambulance Service, led by Marianne Griffiths the former CEO of Sussex University Hospitals NHS Foundation Trust, under whose tenure several of the whistleblowing cases arose.