Dr Minh Alexander retired consultant psychiatrist 17 October 2022
| Summary: My condolences to all affected East Kent families. The Kirkup investigation into maternity failures at East Kent Hospitals University NHS Foundation Trust is due to report on Wednesday 19 October 2022. A Telegraph investigation has today added to the general concerns about NHS maternity care. It has revealed that some NHS trusts have been wrongly classifying neonatal deaths as stillbirths, with the alleged aim of covering up and avoiding an inquest. Mark Tattersall Consultant Obstetrician has whistleblown on this practice. He has made past disclosures about patient safety and his evidence on this is held by parliament. There have been concerns at East Kent maternity services for around a decade, in the context of generally poor trust governance and the CQC placing the trust into special measures in 2014. The trust came under increased scrutiny as a result of an avoidable death of baby Harry Richford on 9 November 2017. Harry’s mother was a healthy young woman, her pregnancy had been uneventful, and Harry’s death was shocking and unexpected. Harry died due to poor care, which centred around the poor supervision of a locum doctor whom the trust rostered for out of hours duties without checking his competence. The family’s search for the truth and media investigations led to increasing awareness that other families had been affected and that EKHUFT had repeatedly failed to refer cases to the coroner. Systemic failings were confirmed after the commencement of local Healthcare Safety Investigation Branch maternity investigations in 2018. The government ordered the Kirkup investigation as the scale of the failures emerged. In this post I share documents provided by Harry Richford’s family via @DerekRKENT to explain a key concern – regulatory failure to keep other babies and mothers safe. The documents give an audit trail of failures by EKHUFT to learn, and denial by the Care Quality Commission (CQC) of these systemic risks to the public. EKHUFT became an embarrassment to the authorities in 2014 when it had to be placed in special measures because of poor governance and unsafe care. Thereafter, CQC reported improvement. Despite evidence of continuing organisational failure and harm, CQC claimed to the Richfords in 2018 there was no breach of EKHUFT’s organisational legal duty under CQC Regulation 12 to provide safe care related to Harry’s death. Two years later, CQC reversed and prosecuted the trust, the first prosecution of its kind. CQC’s denial that Harry Richford’s death was linked to systemic failings was disproved by the trust’s internal investigation, five expert reports and the coroner’s findings, all of which identified organisational related failings by EKHUFT. CQC denied organisational failure even though EKHUFT failed to refer Harry’s death to the coroner. It was also despite the fact that the trust reported to external authorities that Harry’s death was “expected”, even though EKHUFT had identified that the death was linked to care failings. CQC also claimed it had never seen a highly critical Royal College of Obstetricians and Gynaecologists (RCOG) report on EKHUFT which was carried out before Harry’s death. The RCOG identified many examples of previous poor care, organisational failings and risks, including those which specifically led to Harry’s death. CQC claimed it had not reviewed the report until 2019, despite CQC being aware of a related action plan before that, and despite the fact that the RCOG report was commissioned with the involvement of the CCG and NHS England, who have joint working arrangements with the CQC. Most recently, it was found that the coroner’s Prevention of Future Deaths report on Harry Richford was not published as it should have been on the chief coroner’s website, and that NHS England’s and EKHUT’s responses to the coroner are missing. Will the pending Kirkup report reveal the whole truth about the failures at EKHUT and the failures of oversight bodies? Of relevance to EKHUFT’s future management, since April 2022 the CEO of EKHUFT has been the former CEO at Homerton, under whose tenure the ‘ Unhappy Midwives’ whistleblowing scandal arose. This related to multiple maternal deaths (usually very rare) and poor maternity care. Another Homerton maternity whistleblower, Pam Linton senior midwife, reported concerns to CQC but later discovered via a Subject Access Request that nothing appeared to have been done about her concerns. Harry’s family in their own words: Harry Richford’s family tenaciously investigated the factors contributing to Harry’s death and they have set out a summary of their experiences at this website: http://harrysstory.co.uk/ |
Systemic factors affecting maternity safety
Healthcare safety is an issue of resources, systems and leadership.
In all serious incidents, even if they involve errors or negligence by individuals, an organisation should take responsibility and reflect on whether it may have allowed a serious incident to occur.
For example, through poor staffing and skill mix, poor supervision, lack of drilling for emergencies, lack of quality monitoring, inadequate equipment, inadequate administrative support, poor team processes and dynamics or leadership unconducive to safety culture.
The Ockenden Review on maternity failures at Shrewsbury and Telford emphasised that dedicated focus is important to protecting service quality, and pointed out the importance of focused leadership on quality:
Ockenden page 54:
“PSIRF- Resources and expertise:
4.138 The review team discussed with NHS England that the National Maternity Assessment Tool recommends the following minimum staffing levels for governance teams:
• Maternity governance lead (who is a midwife registered with the NMC)
• Consultant obstetrician governance lead (Minimum 2 PAs90)
• Maternity safety manager (who is a midwife registered with the NMC or relevant transferable skills).
• Maternity clinical incident leads
• Audit midwife – a lead midwife for audit and effectiveness
- Practice development midwife
- Clinical educators, to include leading preceptorship programme
Appropriate governance facilitator and administrative support within the maternity department.”
In 2012, the NHS Litigation Authority (now rebranded as NHS Resolution) analysed ten years’ of maternity claims. NHSLA detected patterns in care failings and recommended systems solutions:
“The key risk management themes to emerge from the project are discussed. Namely, the need to: engage with the risk management process at all levels; provide suitable learning and training; ensure appropriate supervision and support; have in place up-to-date protocols and guidance with which staff are familiar; learn lessons from claims.
The report concludes that the most effective way to reduce the financial and human cost of maternity claims is to continue to improve the management of risks associated with maternity care, focusing on preventing incidents involving the management of women in labour, including the interpretation of CTG traces.”
Safe staffing
A critical organisational factor is safe staffing, in both numbers and skill mix.
Under conditions of inadequate staffing in healthcare, staff may make more mistakes and face disciplinary action for what are systems issues. They may report fewer incidents in consequence, fuelling a downwards safety spiral. Hansard recorded such an example at Mid Yorkshire Hospitals in 2016.
Jeremy Hunt former Health Secretary and self-styled ‘champion’ of maternity safety, who made political capital out of appearing to support the patient safety cause, decided not to introduce mandatory NHS safe staffing standards:
Why won’t the government implement safe staffing levels in the NHS?
We continue to see healthcare scandals, many of which are maternity scandals, across the NHS. As well as harm to the public, there is compensation and litigation cost for the public purse, particularly for maternity cases.
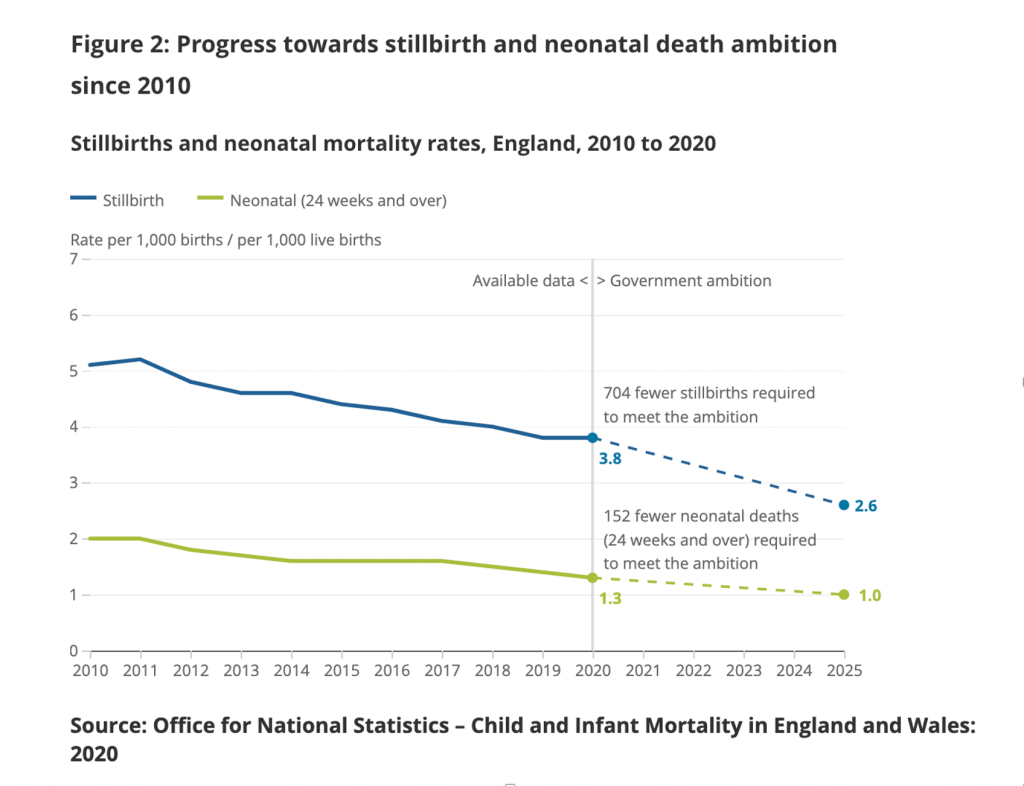
Nationally, some maternity outcomes had previously been on an improvement trajectory. Rates of neonatal deaths, infant deaths and stillbirths fell steadily in previous decades. The rate of safety improvement has slowed under recent Conservative governments. ONS data is available up to 2020 and shows the following trajectory, set against government targets for reduction by 2025:
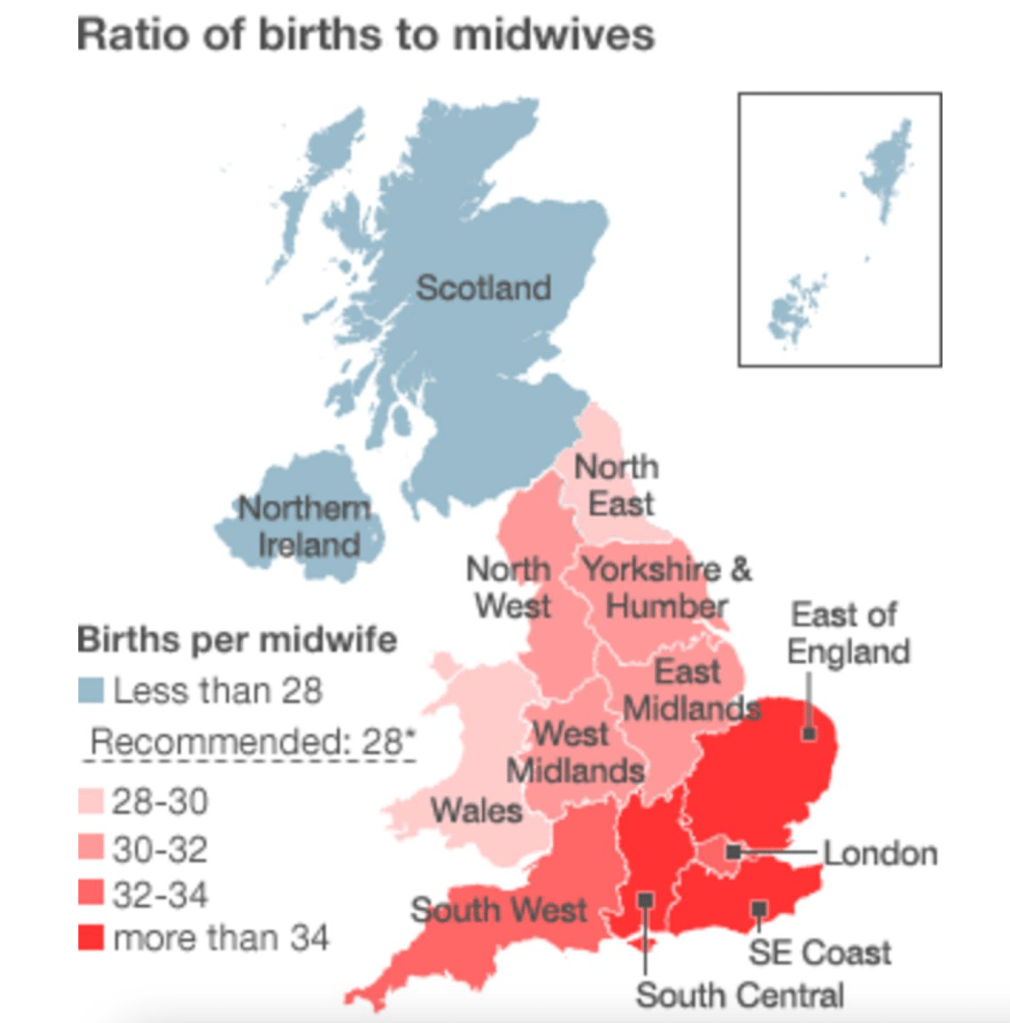
A BBC investigation in 2011 showed significant variation in midwife numbers across the NHS, with the lowest numbers found in the East and South East.
Staffing ratios should of course vary with the health of local populations, but the question is whether less than the minimum is sometimes provided.
In 2020, a survey by the Royal College of Midwives concluded that half of maternity units were understaffed.
The final Ockenden report on Shrewsbury and Telford Hospital NHS Trust, published this year, emphasised the importance of safe staffing:
“In the last year since our first report was published we have seen significant pressures in maternity services in the recruitment and retention of midwives and obstetricians.
“It is absolutely clear that there is an urgent need for a robust and funded maternity-wide workforce plan, starting right now, without delay and continuing over multiple years. This has already been highlighted on a number of occasions but is essential to address the present and future requirements for midwives, obstetricians, anaesthetists, neonatal teams and associated staff working in and around maternity services. Without this maternity services cannot provide safe and effective care for women and babies. In addition, this workforce plan must also focus on significantly reducing the attrition of midwives and doctors since increases in workforce numbers are of limited use if those already within the maternity workforce continue to leave. Only with a robustly funded, well-staffed and trained workforce will we be able to ensure delivery of safe, and compassionate, maternity care locally and across England. ”
Current official guidance on calculating required staffing seems elliptical and coy about setting a minimum standard, reflecting the government’s refusal to legislate for minimum staffing. Guidance refers the reader to other guidance, which leaves the ultimate decision with each local provider.
Midwifery staffing red flags
But NICE midwifery guidance from 2015 does recognise that clinical red flags should trigger a review of midwifery staffing:
“A midwifery red flag event is a warning sign that something may be wrong with midwifery staffing. If a midwifery red flag event occurs, the midwife in charge of the service should be notified. The midwife in charge should determine whether midwifery staffing is the cause, and the action that is needed.
• Delayed or cancelled time-critical activity.
• Missed or delayed care (for example, delay of 60 minutes or more in washing and suturing).
• Missed medication during an admission to hospital or midwifery-led unit (for example, diabetes medication).
• Delay of more than 30 minutes in providing pain relief.
• Delay of 30 minutes or more between presentation and triage.
• Full clinical examination not carried out when presenting in labour.
• Delay of 2 hours or more between admission for induction and beginning of process.
• Delayed recognition of and action on abnormal vital signs (for example, sepsis or urine output).
• Any occasion when 1 midwife is not able to provide continuous one-to-one care and support to a woman during established labour.
• Other midwifery red flags may be agreed locally.”
Based on the still steady stream of maternity care scandals, surely we are currently awash with such red flags?
Seriously unsafe midwifery staffing at East Kent Hospitals University NHS Foundation Trust?
In October 2021 the media reported that CQC had found severe staffing shortage in maternity services at East Kent, following unannounced inspections in July 2021.
Midwives were reportedly forced to work 20 hour days.
This are links to the reports from the July 2021 CQC site visits:
https://www.cqc.org.uk/location/RVV09
https://www.cqc.org.uk/location/RVV01
Was the CQC wilfully blind to organisational failings in maternity care at East Kent?
CQC appeared to ignore internal trust findings and external expert findings of organisational failure
At East Kent Hospital University NHS Foundation Trust, the Care Quality Commission bizarrely refused to acknowledge a link between a serious incident – the death of baby Harry Richford seven days after a catastrophic, avoidable birth injury – and evident systems issues.
This was despite the trust’s internal Root Cause Analysis (RCA) report concluding very clearly that there were multiple systems issues:
“This leads us to conclude that this incident occurred due to system failures.”
The trust RCA acknowledged that there was inadequate vetting of and supervisory support for the locum junior doctor involved in Harry’s death.
The RCA contained a hint that other staff were concerned about having a locum on call, as one midwife rolled her eyes in front of Harry’s mother upon being told which registrar was on call on the fateful night of Harry’s birth.
This raises many questions about organisational factors. It also linked to an earlier RCOG finding that maternity staff had stopped raising safety concerns because Leads did not act upon them.
Whistleblowing governance at East Kent Hospitals University NHS Foundation Trust The Royal College of Obstetricians and Gynaecologists (RCOG) was in 2015 commissioned to review governance failures and dysfunctional team relationships in East Kent maternity service. The College reported that there were issues of poor reporting culture, especially by doctors. Staff reporting was discouraged by the fact that past concerns were not acted upon. An FOI request that I submitted to EKHUFT in 2019 revealed that the so called ‘Freedom To Speak Up Guardians” – designated trust employees to whom other employees can whistleblow – had never escalated any whistleblowing matters to CQC or to the National Guardian. The BBC has reported that most East Kent staff were too frightened to speak to the media. This speaks loudly of organisational and senior leadership failure. |
The Richfords objected to the trust’s internal RCA investigation.
In response, EKHUFT commissioned two expert reports from a neighbouring NHS trust.These reports concluded that there were some failings. Overall, they were not as critical as later expert reports commissioned by the coroner but organisational failure is implied by:
– A concern that the trust may not have adhered to national guidelines on neonatal resuscitation. (This contradicted the trust internal RCA which concluded that resuscitation guidance was followed).
– A suggestion that EKHUFT should put in place a more robust system of training and drilling to ensure that staff were better equipped to deal with neonatal emergencies and resuscitation.
But CQC denied there was organisational failure by EKHUFT in Harry Richford’s case despite the trust’s RCA findings and these local external reports.
CQC appeared to ignore the probity implications of EKHUFT’s flawed reporting to external authorities about Harry’s death
CQC denied there was organisational failure despite the trust’s flawed decision not to refer Harry’s death to a coroner.
The trust justification for this was recorded in the RCA report. An argument was made that no referral was needed because the cause of death was known (and that it was hypoxia). This is a flawed argument. It failed to acknowledge other relevant criteria requiring a referral to the coroner, such as whether a death could be related to a clinical procedure.
The CQC should have seen the trust’s failure to refer Harry’s death to the coroner as a big red flag about organisational competence, probity and safety culture.
Instead, on 17 August 2018 Emma Carroll then a local CQC inspector (now Inspection Manager) wrote to Harry’s family that three management reviews by CQC had concluded that there had only been errors by individual staff, and that the trust itself was not in breach of regulations:
“We have held three management meetings to discuss the information shared by yourself and the trust, including the RCA, both independent reviews, the trust’s action plan and additional information requested from the trust. We have not received confirmation from the senior coroner as to whether they will be progressing with an investigation. However, I have requested CQC are made an interested party which means we will receive the final Coroner’s report.
After an extensive review, we do not believe there has been a breach in regulation. The concerns raised in this incident are centred on an individual’s decision or error. The criminal offences CQC can prosecute against only apply to registered person failures.”
Derek Richford, Harry’s grandfather, challenged this bizarre position.
The exchange of correspondence between Derek Richford and Emma Carroll on 17 August 2018 can be found here.
Instead of shutting down enquiries about organisational failure, the CQC should have been actively pursuing whether EKHUFT had failed to refer other deaths to the coroner, whether there were common themes between deaths and the level of risk posed to the public by EKHUFT’s systems failure.
The coroner later noted with concern the trust’s outrageous claim that Harry’s death was “expected” and its failure to inform the coroner of Harry’s death:
“Concern 17
The child death notification form was incorrectly completed in that Harry’s death was recorded as ‘expected’. No notification was made to the Coroner. No details were filled in on the notification form giving any detail of the problems leading to Harry’s death. As a result, the Child Death Overview Panel would have been unaware of the problems encountered and could not have shared learning to prevent other such deaths occurring. I make no recommendation in respect of the lack of notification to the Coroner as I am aware that the Senior Coroner has already dealt with this.”
Normally, arrangements for reviewing child deaths are very formal and involve substantial multiagency scrutiny.
On a related theme of reporting to external authorities, the coroner also found that EKHUFT’s report about Harry’s death to a national database was inaccurate:
“Concern 18
The MBRRACE form in respect of Harry Richford was inaccurate in a number of important areas. The form is important to provide robust national data to support the delivery of safe, high quality maternal and new born care as well as identifying errors and faults, if any, where there has been a maternal or infant death so that future deaths can be avoided.”
The CQC should have noted that EKHUFT’s MBRRACE submission was inaccurate and that this too was a warning sign.
The coroner noted another serious warning sign about EKHUFT managers’ accountability and transparency:
“Concern 19
Important independent reports do not appear to have been shared within the East Kent Trust’s staff, for instance the HSIB report into Harry’s death appeared during the inquest to be unknown to a number of the staff.”
Alongside the coroner’s above concerns about EKHUFT management’s reliability, it is relevant to note that EKHUFT was one of the trusts which had to repay an insurance discount to NHS Resolution, after it was found to have mis-declared its maternity services to be safer than they really were. The NHSLR spreadsheet which records these events can be foundhere. See Year 1 and Year 2.
CQC’s denial of organisational failings was discredited by the Coroner’s findings
Contrasting with CQC’s denial, the coroner later made in February 2020 a string of recommendations for avoiding future deaths. He made it abundantly clear that he thought there were avoidable organisational factors in Harry’s death, local and national.
The detailed coroner’s conclusions underlying the recommendations for preventing future deaths can be found here.
Three independent expert reports commissioned by the Coroner concluded that there were multiple care failings by EKHUFT and that some of these related to organisational factors.
Both the medical experts, an obstetrician and a paediatrician, concluded that Harry would have been born alive and in good condition if his care had been appropriate.
At inquest, the trust’s lawyers contended there was no neglect but the coroner rejected this and ruled that a contributory factor in Harry’s death was neglect:
“The cause of death was 1a Hypoxic Ischaemic Brain Encephalopathy. There was a narrative conclusion setting out some seven failures in the care of Harry Richford together with a conclusion that his death was contributed to by neglect.”
| Coroners’ findings of neglect A finding of neglect by a coroner is a very serious matter. Neglect was defined as follows in the case of R v HM Coroner of North Humberside and Scunthorpe Ex p Jamieson [1995] “Neglect in this context means a gross failure to provide adequate nourishment or liquid, or provide or procure basic medical attention or shelter or warmth for someone in a dependent position – because of youth, age, illness or incarceration – who cannot provide it for himself. Failure to provide medical attention for a dependent person whose physical condition is such as to show that he obviously needs it may amount to neglect. So it may be if it is the dependent person’s mental condition which obviously calls for medical attention (as it would, for example, if a mental nurse observed that a patient had a propensity to swallow razor blades and failed to report this propensity to a doctor, in a case where the patient had no intention to cause himself injury but did thereafter swallow razor blades with fatal results). In both the cases the crucial consideration will be what the dependent person’s condition whether physical or mental appeared to be”. |
Thus, Harry’s case also raised Safeguarding issues, which placed a particularly serious duty on CQC to protect other similarly vulnerable patients.
CQC’s denial of organisational failure was discredited by HSIB’s findings
The HSIB National Investigation team scoped Harry Richford’s case for potential national learning.
The exercise was reported in January 2019 and came to similar conclusions as the coroner’s experts.
The Healthcare Safety Investigation Branch (HSIB) also identified abundant evidence of organisational failures and lack of learning by EKHUFT.
Of note, HSIB identified that the trust had not followed its own policy (Engaging the Temporary Workforce, 2014) on checking the competence of locum staff. This policy recognised that the trust had a duty to proactively mitigate risk when locums are assessed as not being competent, for example by restricting practice or increasing supervision.
The trust had also not followed RCOG guidance on consultant attendance for certain procedures if a trainee has not been signed off as competent:
“The RCOG green-top guideline 2011 and Trust guideline 2015, recommends that a consultant obstetrician should attend in person for a trial of instrumental delivery if the trainee has not been assessed and signed off as competent. The Trust guideline also identifies caesarean section at full dilatation as a procedure the consultant should attend inperson if the trainee has not been signed off for independent practice for the procedure. The locum doctor’s competency was unknown.”
According to the Memorandum of Understanding between HSIB and CQC, it seems likely that HSIB sent CQC a copy of HSIB’s January 2019 scoping report:
“Sharing pre-published HSIB investigation reports and recommendations. To be open and transparent when in receipt of information regarding the safety of services that are registered with CQC and funded by the NHS in England. The information is shared with the CQC in a timely way through the named CQC contact or by a representative delegated by them.”
HSIB began its local maternity investigations in 2018. In February 2020, at the same time as the coroner’s PFD report was issued, HSIB produced a summary report on its local investigations at EKHUFT. In this report, HSIB observed that the same errors kept being made at EKHUFT:
“From December 2018, HSIB engaged frequently with the Trust to present evidence of recurrent patient safety concerns in its maternity services. Despite repeatedly raising these concerns with the Trust, HSIB investigators continued to see the same themes reoccurring and in August 2019, asked the Trust to self-refer themselves to their CCG and the CQC.”
HSIB also wrote to the CQC about the problems at EKHUFT in August 2019.
CQC knew without any doubt by August 2019 that there were organisational failings, linked to ongoing serious harm. By January 2020, a rare maternal death was amongst the EKHUFT incidents investigated by HSIB (page 3 HSIB summary report).
The CQC informed EKHUT on 1 October 2019 that it was commencing a criminal investigation into the circumstances of Harry’s death.
CQC did not announce that it would prosecute EKHUT under CQC Regulation 12 until October 2020.
The reported reason for delay was COVID operational pressures.
A question arises of CQC’s competence in identifying organisational failings and system risks, and or alternatively, its willingness to acknowledge them.
Another question is at what level of seniority in CQC was the original flawed conclusion reached about absence of organisational failings?
Harry’s grandfather Derek Richford objected to the CQC’s 17 August 2018 denial of organisational failure. He copied his objection to Ted Baker, then Deputy Chief Inspector of Hospitals.
Ted Baker responded more sympathetically to the Richfords in September 2018, but he maintained that the threshold for applying CQC regulation 12 was not met.
In December 2018,Ted Baker wrote again to offer the family a meeting in January 2019.
CQC claimed it had never seen the report of a 2015 RCOG review on EKHUFT maternity failings
The Richford’s meeting with CQC took place in early 2019, when the family made the CQC aware of a 2015 Royal College of Obstetricians and Gynaecologists (RCOG) report on EKHUFT maternity services. This report had been unearthed by Derek Richford via FOI, after the document had been mentioned in trust board papers.
Importantly, the RCOG report revealed that there had been previous concerns about the supervision of junior doctors, consultant availability and the general management of the labour ward at EKHUFT:
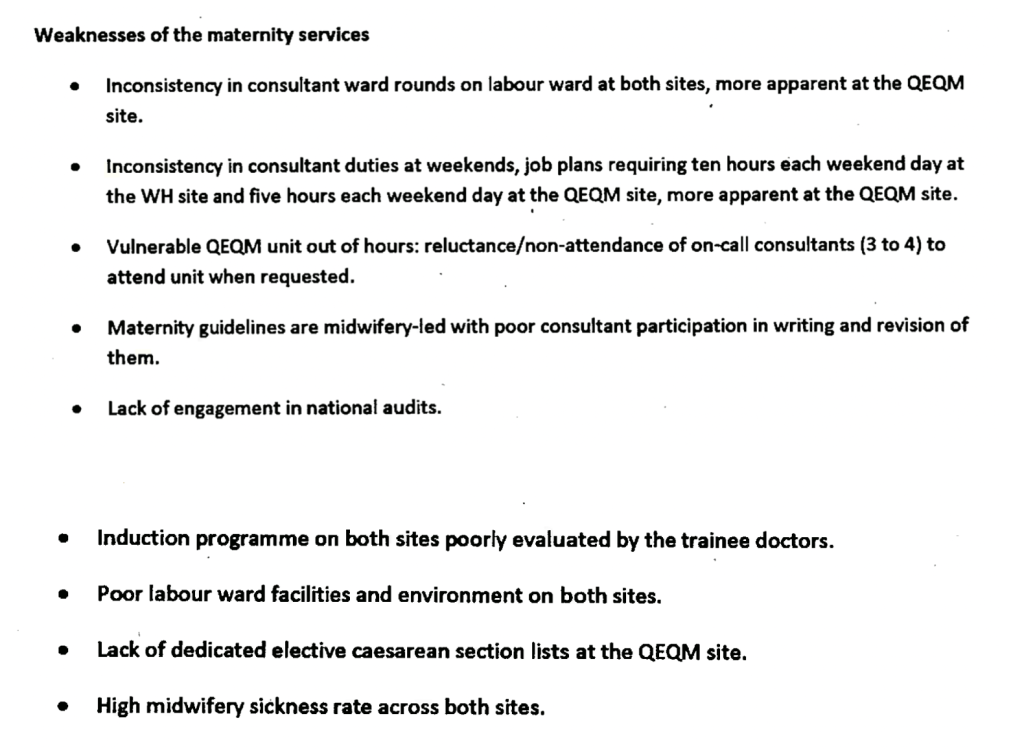
In other words, there were systems issues aplenty.
There were numerous examples of poor care and the RCOG described some clinical practices as “dangerous”, such as the poorly supervised use of Syntocinon.
The RCOG found evidence of poor whistleblowing and reporting practice. Consultants’ poor practice tended not to be challenged, or was omitted from incident action plans. Staff stopped raising concerns because they were not acted upon:
“Safety issues relating to practice were not reported as no action would be taken by the Leads.”
Indeed, the RCOG report was commissioned because of concerns about poor governance and team dysfunction in the EKHUFT maternity service:
In other words, organisational failures and systemic risks, as opposed to CQC’s narrative of isolated errors by individuals.
Specifically, the RCOG found evidence of patient harm related to locum doctors’ omissions, whilst working out of hours:
“The locum registrar did not review the patient overnight despite this woman’s details being on the handover sheet.” (Case 6 page 16)
The RCOG was concerned that safety could be affected by middle grade locum cover at night (page 34 and 35).
This proved to be an accurate concern in the light of the later harm to Harry Richford.
Even EKHUFT’s medical director observed, in terms, in a statement of 17 December 2019 to the coroner that Harry’s death was part of a chain of persistent failure and lack of organisational learning linking back to the RCOG report:
“The analysis of the root cause of Harry Richford’s death led to actions similar to some of those in the RCOG review, CQC reports of 2014-2016 and the HSIB recommendations, indicating a failure to sufficiently embed learning.”
Shockingly, it was reported that the CQC had never, until 2019, reviewed the 2015 RCOG report despite knowing of its existence.
A post by the Health Service Journal on 23 January 2020 reported:
“But what is perhaps even more shocking is that the Care Quality Commission did not see the report for nearly three years after it was written in February 2016. The CQC confirmed although it saw an action plan based on the report, its records indicate it did not see the report itself until January 2019.”
The RCOG report was mentioned in a trust board paper of April 2016, entitled “CQC IMPROVEMENT PLAN”.
Surprisingly, the trust stated in this document:
“Review report is clear – the Trust does not have an unsafe maternity service but there is improvement work to do around how the service is run in some areas.”
(Board papers indicated that in the corporate risk register later that year, maternity risk is rated as “extreme”).
It also stated:
“The MBRRACE-UK report has been published and shows the Trust to have a 10% lower average mortality rate for its comparator group. The RCOG report was received on the 18th February. Actions will need to be incorporated into the improvement plan. The deadline for embedding the new maternity dashboard has slipped and will be in place for the end of March 16.”
The comment about favourable MBRRACE-UK ranking is interesting in the light of the coroner’s finding that EKHUFT made an inaccurate submission to MBRRACE-UK about Harry’s death, and in light of today’s revelations in the Telegraph about possible manipulation of NHS deaths reporting.
Why did CQC claim that EKHUFT maternity services had improved and why did it deny that there were organisational failures?
EKHUFT’s response to the RCOG report is published via an undated entry on the trust’s website. It reads as a post hoc communication, drafted in the fallout from Harry Richford’s case.
EKHUFT’s response cites in its defence the praise that it received from CQC in 2018, at which time the Richfords were struggling to be heard by CQC:
“A further CQC inspection in August 2018 acknowledged that the East Kent maternity service had made great strides to drive learning, improve outcomes and improve innovation through a collaborative and multidisciplinary approach but there were continued concerns in several areas indicating that more improvement work remains to be done.”
One of the Richfords’ many concerns about the trust’s governance was the fact that years after the RCOG report, the trust admitted that it had only fully implemented two of the RCOG recommendations. The facts are revealed by this EKHUFT report of 16 July 2020:
“…it is not possible to evidence all actions from that report as having been completed. 23 recommendations were made by the RCOG. When the available evidence was reviewed the LRC concluded there was sufficient evidence that 2 recommendations had been met, that 11 had been partially met. For some of the recommendations where evidence weas [sic] insufficient…”
Why did CQC not identify this evidence of organisational failure sooner?
Was the imperative to create a positive narrative of improvement more important?
If so, from where did the imperative come?
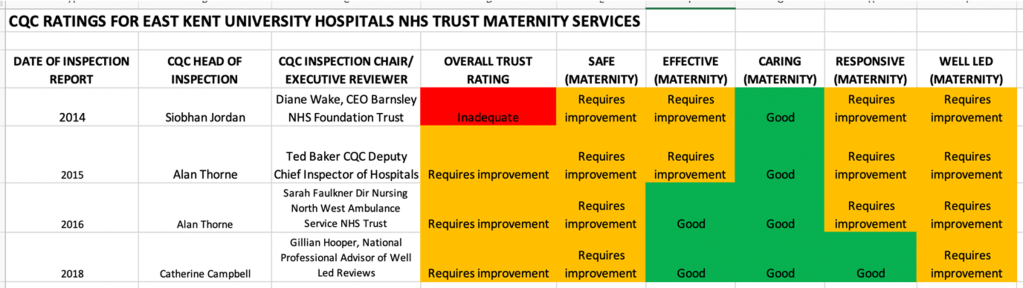
This is how CQC progressively rated EKHUFT’s maternity service, after putting the trust in special measures in 2014
Trust board papers of October 2016 noted that Philip Dunne Health Minister visited the trust and was pleased to see improvement:
“His visit gave him the opportunity to see for himself the progress that the Trust has made and he was quoted in the post-visit press release as saying:
“I saw first-hand the great strides in improving the quality of care that the Trust is making and the positive effect these changes are having on staff and patients.
“I enjoyed meeting and talking with a wide range of members of staff from across the hospital. It was very clear that everyone is passionate and united in their desire to continue to improve services.”

This brings to mind witness testimony from the Mid Staff Public Inquiry that officials were focused on an imperative of not embarrassing the Minister.
What was CQC and NHS England’s coordination on the critical RCOG report?
The RCOG report was received by the trust in 2016. This was AFTER publication of Bill Kirkup’s 2015 report on maternity care at Morecambe Bay.
A relevant recommendation from Morecambe Bay, which was accepted by the government, was that trusts should be under a duty to disclose external investigations.
The government claimed it would take steps to ensure this was embedded in regulations (page 74 and 75), but that as an interim measure, the CQC would use existing powers to compel disclosure by trusts:
“46. In the meantime, Monitor and the Care Quality Commission will continue to use their respective statutory information-gathering powers to require NHS Trusts and Foundation Trusts to notify them of both the commissioning and the conclusions of relevant external investigations.”
Did the CQC actually make any changes to its procedures, following the government’s promises in 2015 that CQC would compel disclosure of external investigations by NHS trusts?
Why did CQC reportedly not ask for a copy of the RCOG report when it first became aware of the report’s existence?
Why did CQC appear to accept the trust’s action plan as a reliable interpretation of the RCOG’s findings and recommendations, instead of insisting on seeing the report itself?
A CCG document of 8 December 2015 revealed that the RCOG report had been jointly arranged by the trust, CCGs and NHS England:
“Maternity services were reported as inadequate within the CQC report given the lack of progress…. The CCGs with NHSE and the trust have commissioned a Royal College review which is underway to support the service to make further improvements.”
What happened to CQC and NHS England’s joint working protocols?
For example:
“2.2 We commit to working together proactively to share information and intelligence about the quality of care in order to spot potential problems early, and manage risk. To do this we seek to explore ways of sharing data where there is a shared interest or common benefit.”
Did a risk summit of some sort take place about EKHUFT maternity services, as is common practice?
How could CQC plausibly claim that there were no systems issues if its fellow regulator, NHSE, had instigated an RCOG governance review based on CQC’s own inspection findings of systems failures?
Why did CQC change its mind about prosecution under Regulation 12 and why has CQC not applied Regulation 12 more consistently?
Eventually, under the glare of public scrutiny, and after the revelations by the Healthcare Safety Investigation Branch of other maternity deaths and serious management failures at EKHUFT, CQC announced two years later in July 2020, that it would prosecute EKHUFT under Regulation 12. This was for the harm caused to Harry and his mother, Sarah Richford.
What changed between 2018 and 2020? The facts of Harry’s case did not change. And CQC Regulation 12 did not change.
I asked CQC to comment on its various actions and omissions,. I also asked CQC about why it informs bereaved families such as the Richfords that it cannot investigate their concerns, when the discharge of CQC Regulation 12 appears to require investigation by the CQC.
CQC has to date only acknowledged my enquiry and indicated that it would respond.
It does seem very arbitrary as to how the CQC responds to harmed patients and families.
What happens to families who are no less seriously harmed than the Richfords, but who may be less articulate and cannot navigate CQC’s obstacle course?
Reservations about the usefulness of fining public bodies aside, why had CQC not taken a similar approach to other gross and proven NHS care failures?
Has CQC obscured the real levels of unmet need and harm, and how much will Kirkup’s report reveal?
A September 2022 BBC analysis of CQC reports shows that maternity service failings are widespread, with 7% of units rated by CQC as “posing a high risk of avoidable harm”.
Given what we know about CQC’s identification of systems risks, is the real figure higher?
Kirkup’s investigation of maternity services at EKHUFT is due to report on 19 October 2022.
Will he identify all relevant failings, regulatory, corporate and individual?
I was concerned that in a previous investigation, into the death of baby Elizabeth Dixon, Kirkup placed much emphasis on failings and dishonesty by individual practitioners.
His notable comment that there had been “a twenty year cover up” generated many headlines.
But did he do justice to Elizabeth’s parents through a thorough examination of controlling minds and corporate accountability? Should he have undertaken a more searching exploration of the powerful senior management of a favoured NHS trust, Frimley Health NHS Foundation Trust?
Frimley Health NHS Foundation Trust knew about the Dixons’ concerns for years before Kirkup investigated, and had plenty of chances to put the matter right.
Let us hope for better this time round, and that the CQC’s serious failure to help prevent deaths is fairly reflected in Kirkup report. And that the role of other oversight bodies is also fully explored.
It is relevant to note that Tracey Fletcher took up post as EKHUFT chief executive in April 2022. She was previously CEO at the Homerton, where a contentious maternity whistleblowing matter arose.
NHS England’s then medical director for London, Henrietta Hughes – later the National Guardian for whistleblowing – was a party in NHS England’s handling of the Homerton scandal.
And so the wheels turn.
| The curious non-publication of Harry Richford’s PFD report, and NHS England’s and EKHUFT’s missing responses to the coroner The public bodies which received a copy of Harry Richford’s PFD – the coroner’s report to Prevent Future Deaths on matters arising from Harry’s inquest – were legally obliged to respond to the coroner’s concerns about mitigating risk of future of deaths. A troubling discovery in the course of checking organisational responses to the coroner was that I found Harry Richford’s PFD was not published by the chief coroner, as it should have been. It is not known if the PFD was originally published, and then removed at some point. If anyone clearly recalls seeing it on the website, I would be grateful to know. A worker at the chief coroner’s office kindly checked and agreed with me that as of 11 October 2022, the Richford PFD was missing from the website, and so the organisational responses were also missing: “We have a system to allocate reference numbers to reports. I’ve checked the website and Harry Richford (2020-0117) report has not been published but 0116 and 0118 have been. I checked our system and found a response from DHSC, I will upload these shortly on our website.” The PFD and the government response have since been uploaded here. The ministerial response noted the trust’s unacceptable and misleading claim that Harry’s death was “expected” and its failure to refer his death to the coroner. The DHSC should hold progress reports by CQC and NHSE on improvement work at EKHUFT, if this ministerial commitment was honoured: “I expect to be regularly updated.” However, neither the chief coroner nor the local coroner have so far been able to locate NHS England’s response or the trust’s response. At this late stage, this seems an unusual anomaly. I will post the NHS England and trust responses below when I eventually obtain them. Or if it transpires that NHS England and or the trust failed to respond to the coroner, I will confirm this. |
RELATED ITEMS
The above failures are part of a familiar pattern of government failure.
Both the CQC and Jeremy Hunt as Health Secretary failed to act on whistleblowers concerns at Homerton:
Letter to Jeremy Hunt 16 October 2015 about his role regarding Homerton maternity whistleblowers
There was regulatory failure in the Morecambe Bay scandal, when oversight bodies accepted circular assurance from each other:
The Report of the Morecambe Bay Investigation by Bill Kirkup 2015
The CQC were also found wanting recently in the Shrewsbury and Telford Hospital NHS Trust maternity scandal:
Final Ockdenden review report 2022
This is the CQC’s letter to the Department of Health in response to criticism by the Ockenden review:
Letter from Ian Trenholm CQC CEO to Secretary of State 4 May 2022
These are some of the other East Kent families’ stories that have come into the public domain:
Rachel Higgs and Archie Batten
Shelley Russell, Nicholas Edwards and Tallulah-Rai Edwards
These are some related items about HSIB and its maternity investigations:
HSIB whistleblowers and the Secret King’s Fund Fact Lite report
More secret HSIB reports and failures of HSIB maternity investigations


Thank you, Dr A.
I must admit, I have not read your content-rich report as studiously as such a scholarly document deserves. However, it does appear to echo so many unbelievably scandalous headlines from the last few years that one assumed were being addressed – but apparently not.
How devastating for the families. Particularly when the initial tragedy is made worse by orders of magnitude by the attempts of cover-up.
I note the burying of evidence of negligence and worse by the institutions involved was treated with more care than the bodies of their victims.
I hear terrible things about the NHS but will not repeat them here as I don’t have first-hand evidence. Nevertheless, I think it is inevitable that the truth will come out eventually, notwithstanding the iron fist of NHS management and the impotence of the regulatory agencies and police.
I just hope we will be intact as a civilized society when that happens.
LikeLike