Dr Minh Alexander retired consultant psychiatrist 8 March 2023
This is a brief post to share a Prevention of Future Deaths report which was kindly brought to my attention, with concerns raised about CQC’s role.
The PFD details have been reported by the Eastern Daily Press and the BBC:
Peter Seaby inquest: Care home slammed over resident’s death
Peter Seaby: Poor supervision could have led to care home death
Mr Peter Seaby was a vulnerable resident, with a diagnosis of Down’s Syndrome, at the Oaks and Woodcroft care home in Norfolk. The care home is run by Conquest Care Homes (Norfolk) Limited, which is owned by the Priory Group.
Priory’s website describes the unit as follows:
Mr Seaby was at risk of choking and of aspirating food into his lungs (which causes serious infection). He required a special diet and supervision at mealtimes. These needs were reflected in his care plan.
However, according to a recent coroner’s inquest, the care plan was not reliably carried out.
Coroner’s Prevention of Future Deaths report on Peter Seaby 27 February 2023
Mr Seaby did not always receive his special diet and he was sometimes not supervised at mealtimes.
This did not accord with the provider’s published claims that the care home provides “person-centred” care:
Peter Seaby sadly died of aspiration pneumonia. A piece of carrot was also found lodged in his throat after death, showing that his care plan had not been properly followed. He was aged 63.
A multi-agency review concluded in November 2019 that “Peter’s death was, on balance, potentially avoidable.”
A jury inquest in 2021 concluded death was by natural causes of aspiration pneumonia.
The outcome of this inquest and how it was handled by the coroner Yvonne Blake was challenged by Mr Seaby’s family through judicial review, leading to the latest inquest:
Successful judicial review quashing the first inquest into the death of vulnerable man Peter Seaby
After the second inquest, which commenced in July 2022, the coroner Jacqueline Lake determined that the primary cause of death was aspiration pneumonia, to which poor care possibly contributed:
“Mr Seaby died of aspiration pneumonia. Inadequate preparation of his lunchtime meal and inadequate supervision at his lunchtime meal possibly contributed to his death.”
She also issued a Prevention of Future deaths (PFD) report, addressed to the care provider in February 2023.
In her PFD, the coroner was concerned about under-staffing at the care home which meant that patients who needed one to one supervision did not always receive it, as in Peter Seaby’s case.
It was previously reported that on the day before his death, Peter Seaby served himself at a meal, whilst a carer was attending to another resident.
Of huge concern, there still appeared to be no internal review of Mr Seaby’s death by the Priory group.
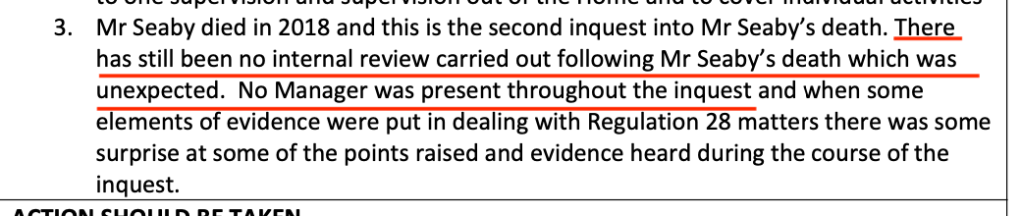
No manager from the provider even attended the second inquest, a matter noted by the coroner as above.
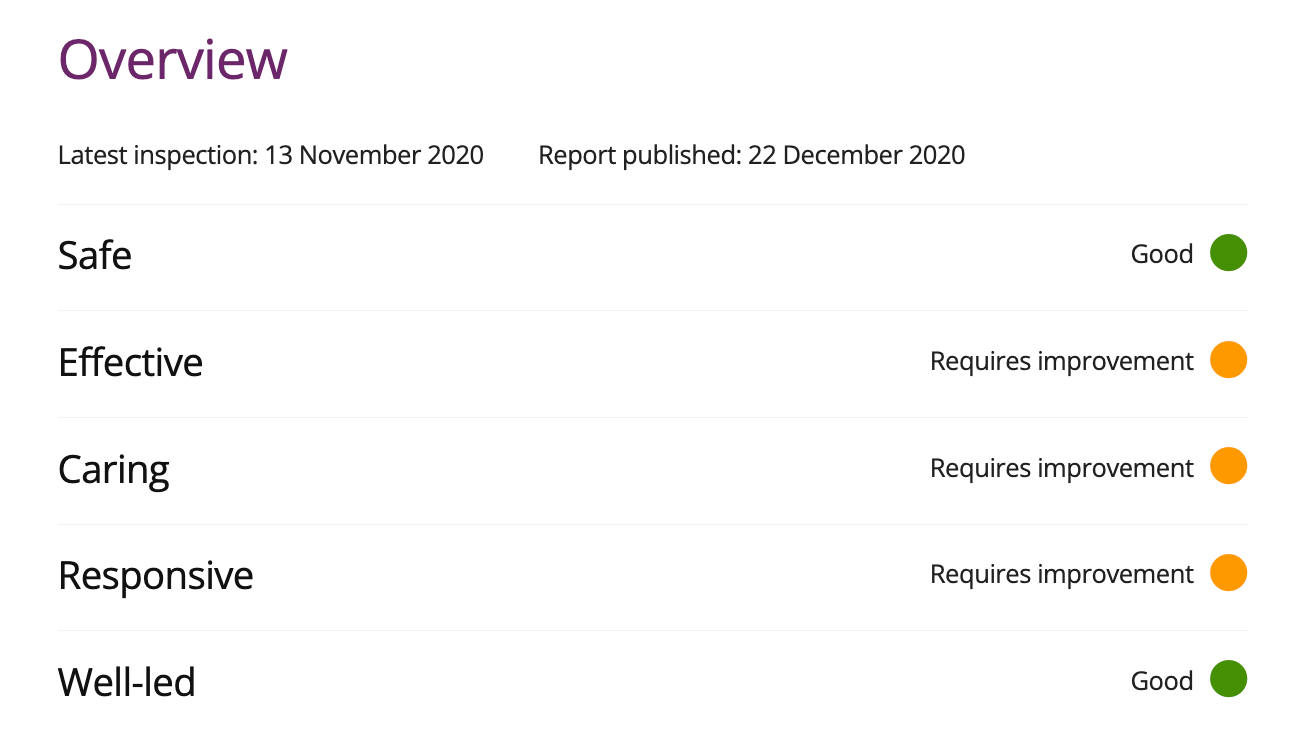
And yet the Care Quality Commission inspected the home in November 2020 and rated the home “Good” on the Well Led domain.
CQC inspection report 22 December 2020 on The Oaks and Woodcroft care home, Dereham, Priory Group
In December 2020 the CQC made the following observations about risk assessment and care plan management, which seemed to rely mostly on scanning documentation, as opposed to checking that care plans were actually delivered:
“There was good oversight and management of risk. We found however that at least one person had regularly refused blood tests due to high anxiety levels. This was now being addressed through a desensitization programme but previous barriers to accessing health care had not been addressed in a timely way.”
“Both care plans and risk assessments for people were clearly written and reviewed in line with changing need and risk. Although a key worker system meant all staff had responsibility to oversee people’s care, most of the documentation had been written by the deputy manager. Not all the documentation demonstrated a collaborative approach or showed who had been involved in collating information or who was involved in best interest decisions.”
The CQC inspection report did refer glancingly to audit, but again relied on audit data produced by the provider:
“Audits helped ensure policies were being followed and regular checks were carried out to ensure the environment remained safe and free from hazards. We sampled some health and safety records, and these were in order.”
The CQC was glowing about the unit’s good governance and learning from incidents:
“Since the last inspection a manager had been appointed to work solely at this location whereas previously one manager oversaw two separate locations. There were good overarching governance processes and the registered manager was well supported. Audits helped to identify any areas for development and there was a robust action and development plan in place. There was oversight of accidents, incidents, safeguarding and near misses. These were reported and analysed to help identify actions taken at the time and to ensure these were appropriate so lessons could be learnt. The outcome of which were shared with staff.”
It is hard to square this with the coroner’s discovery that the provider had not even internally reviewed Mr Seaby’s possibly avoidable death.
Alarmingly, it appears that CQC had been warned of problems at the care home prior to its November 2020 inspection:
“Concerns were received about this service which meant we brought the inspection forward and looked at three key questions where we had previously identified breaches of regulation.”
So in context, there should have been special diligence in carrying out the November 2020 inspection of The Oaks and Woodcroft, with proper verification of the provider’s claims.
Importantly, a preceding CQC inspection report of February 2020 suggested that CQC were aware of Peter Seaby’s death:
“People had documented dietary needs, but some information was contradictory, and staff also gave us contradictory information which could increase the risk for people at the service not getting their dietary needs met or risks of choking fully mitigated. A recent incident had been referred to the safeguarding team and we are waiting for the outcome which is linked to people’s dietary needs and changing care needs.”
So if aware, the regulator should have been actively tracking the provider’s handling of the serious untoward incident, and it should have picked up any failures to carry out an internal review or to genuinely mitigate risks to other service users.
We are a decade on from the death of Connor Sparrowhawk and ensuing scandal over Southern Health.
CQC also failed badly on that previous occasion. CQC failed to either identify or report that hundreds of deaths of mental health and learning disabled people had not been investigated, as later revealed by the 2015 Mazars report.
How much longer should the public wait for a reliable regulator?



What an incredibly sad episode.
Thank you so much for recording this man’s story and thus honouring a frail life not apparently considered important enough to care for.
Unfortunately, I can’t see evidence that the familiar circumstances that allowed such a scandal to occur will not happen again.
LikeLike