Summary: North East Ambulance Service (NEAS) has like other ambulance services been under chronic, major pressure. Like other ambulance trusts, it has poor workforce metrics. Like other ambulance trusts, it has had staff suicides. Of concern, NEAS tried to obfuscate about these suicides when asked about them via FOI. There are other questions about NEAS’ reliability in reporting. NEAS appears to have under-reported bullying in another FOI response, and there are questions about the fact that it appears to be an extreme outlier in reporting a lower number of serious incidents than other ambulance trusts. Moreover, NHS England is in control of the investigation into NEAS’s deaths scandal, but the terms of reference for the investigation reportedly ignore possible manipulation of coronial reporting processes. They have been described by a “source close to the investigation” as a “white wash”. A properly independent judge led inquiry is needed given the serious questions of probity and alleged criminal breaches of coronial law.
Background
North East Ambulance Service NHS Foundation Trust (NEAS) is, like other ambulance trusts, a highly stressed and neglected organisation.
NEAS is currently under the microscope after whistleblowers disclosed that it had been altering staff statements for coroners’ inquests and failing to report deaths to the coroner.
NHS England has been criticised for not acting upon the NEAS whistleblowers’ disclosures, yet NHSE has been left in charge of an investigation into these matters.
That serious conflict of interest was of itself appalling, but it has since emerged through a Health Service Journal report 0f 13 October 2022 that the terms of reference for NHS England’s investigation omit a vital area, and represent an attempt by NHS England to “whitewash” the matter.
“Mr Calvert said the AuditOne review was made aware of “numerous cases” and “not just the five” being examined by the new inquiry. Another source close to the investigation, who asked to remain anonymous, echoed the concerns about the limited number of cases being examined, and added: “What’s missing is an analysis of attempts to conceal facts from coroners, there’s nothing in the terms of reference about this.
The families want a full independent inquiry, this is going to be a whitewash.” [My emphasis]
Moreover, the person whom NHS England appointed to lead its investigation is an NHS insider, Marianne Griffiths former CEO of University Hospitals Sussex NHS Foundation Trust.
When a contentious whistleblowing matter arose at her trust, she and her board were improperly protected by the then National Guardian, Henrietta Hughes:
There is a serious question over whether this obfuscation of organisational failings and poor culture at Sussex contributed to later failures of whistleblowing governance, which affected maternity safety:
Information about staff suicides at NEAS from several sources led to the submission of an FOI request to NEAS about this.
NEAS responded on 12 October 2022, and initially tried to evade disclosure of this information. NEAS answered as follows:
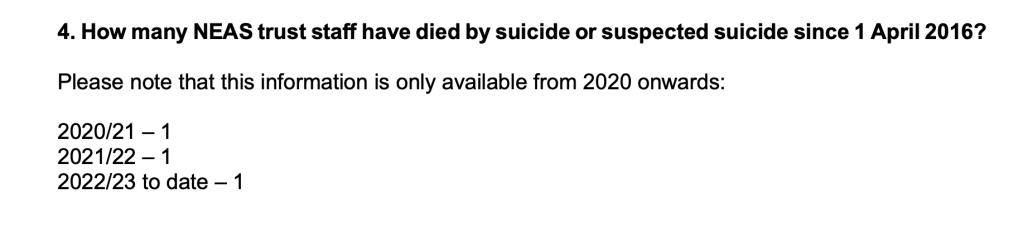
“How many NEAS trust staff have died by suicide or suspected suicide since 1 April 2016?
The Trust would confirm that it is the coroner who decides whether a death was suicide.”
(NEAS FOI disclosure ref. 22.271)
NEAS was challenged about the fact that its FOI response had not met the legal obligations under FOIA to:
Confirm whether or not it held the requested information
Indicate which legal exemption it relied on if it held the information, but did not want to disclose it.
On 18 October 2022 NEAS responded again, disclosing that there had been three staff suicides or suspected staff suicides since 2020:
NEAS denied that it held data before 2020.
In addition to the tragedy of ambulance trust staff’s working conditions, a very serious issue arising from this FOI matter is that NEAS initially attempted to evade the question about staff suicides.
This surely shows continuing organisational failure and secrecy?
For context this is an FOI disclosed by NEAS in 2018 about staff sickness related to mental health issues:
It has been reported that NEAS in fact established a mental health advisor post as part of Occupational Health services, following staff suicides. NEAS have been asked to confirm if this is correct, and to provide details about these issues.
Has NEAS issued a false FOI disclosure about levels of bullying?
In another area, NEAS’ reporting is also in doubt.
I have seen an FOI response by NEAS of 28 September 2022 which reports tiny numbers of reports of staff-staff bullying in recent years:
2019 < 5 cases
2020 6 cases
2021 < 5 cases
This is the relevant extract from NEAS’ FOI disclosure:
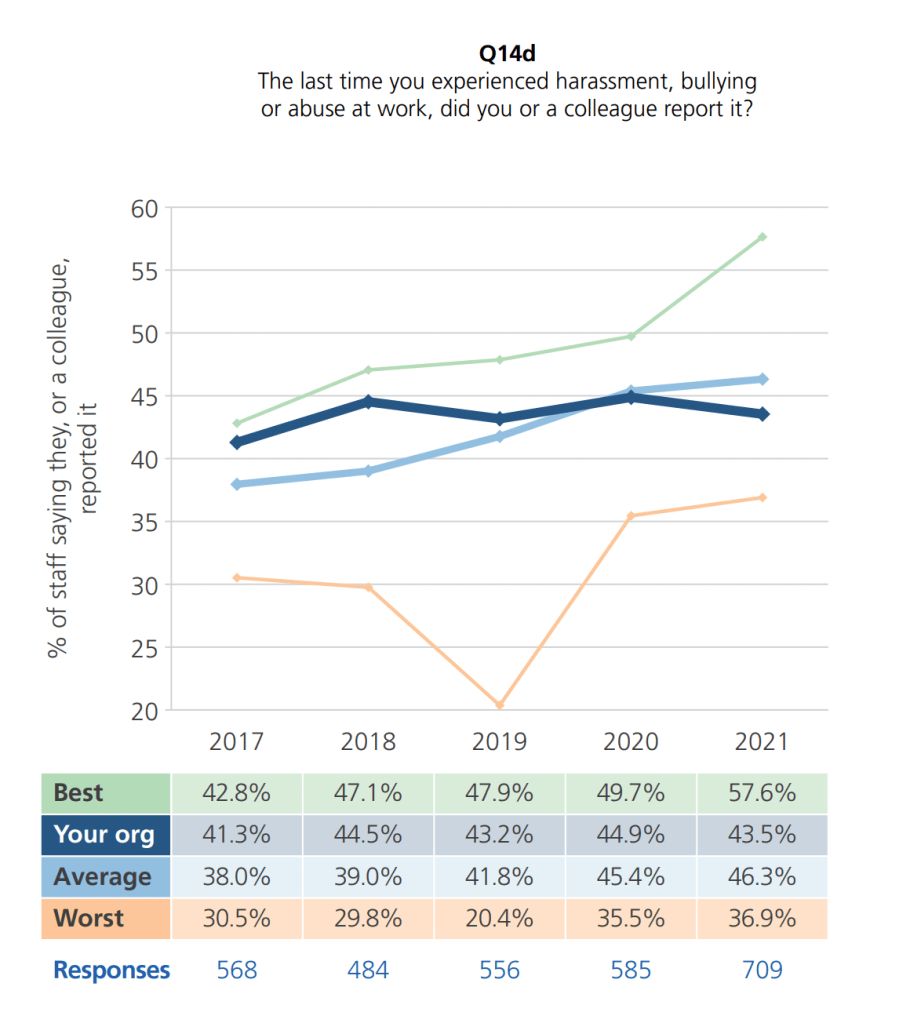
This data is strange because it does not match up with NHS Staff Survey data.
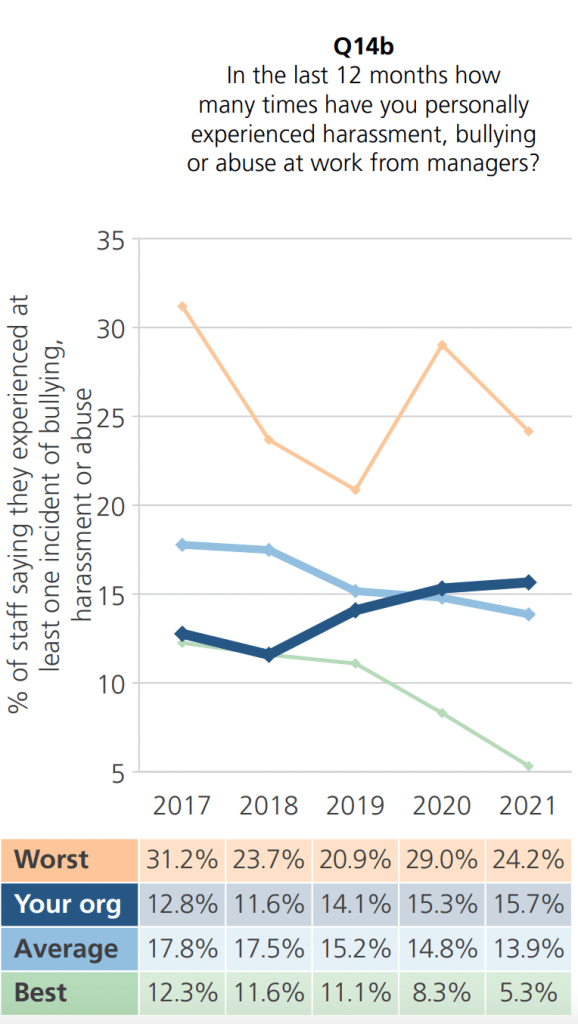
a) 15.7% of NEAS staff reported being bullied by a manager in the previous twelve months
Scaling this up, based on an NEAS workforce of approximately 2,700 staff gives an estimate of 424 staff who experienced bullying by a manager in the previous twelve months.
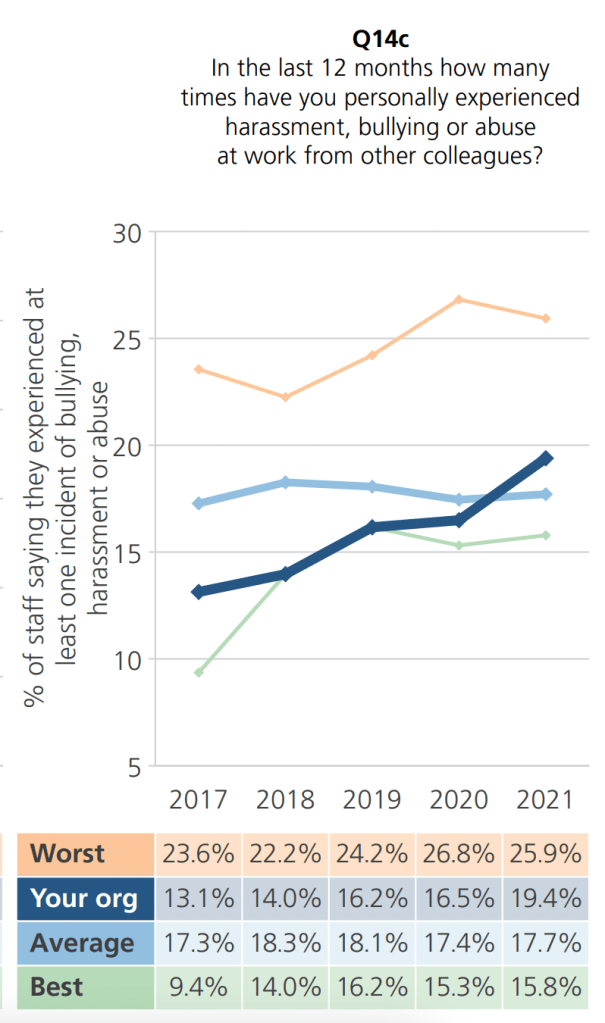
b) 19.4% of NEAS staff reported being bullied by a colleague in the previous twelve months:
Scaling this up, based on an NEAS workforce of approximately 2,700 staff gives an estimate of 524 staff who experienced bullying by a colleague in the previous twelve months.
c) 43.5% of NEAS staff reported the last incident of bullying and harassment that they experienced was reported:
Therefore, the total recorded incidents of reported bullying at NEAS that year should have been something like 43.5% of the hundreds staff who experienced bullying, and not the tiny single figures reported in NEAS’ FOI disclosure of 28 September 2022.
Questions arise of whether NEAS made a false statement under FOIA about its recorded incidents of bullying, or whether there is something terribly wrong with NEAS’ systems for recording and tracking the serious workforce issue of bullying.
Both options are disturbing.
NEAS claimed in its annual report of July 2022 that it planned to investigate the numbers of bullying incidents,
“In addition to the activities that have already commenced we have identified actions that will be progressed over the next 12 months, including….. Investigating the data around bullying and harassment in more detail and triangulate with free text comments, Freedom to Speak Up Guardian, grievances and exit interviews to get a more detailed picture.”
Is it really plausible that NEAS was unaware that its FOI release of 28 September was a gross misrepresentation of its levels of reported bullying?
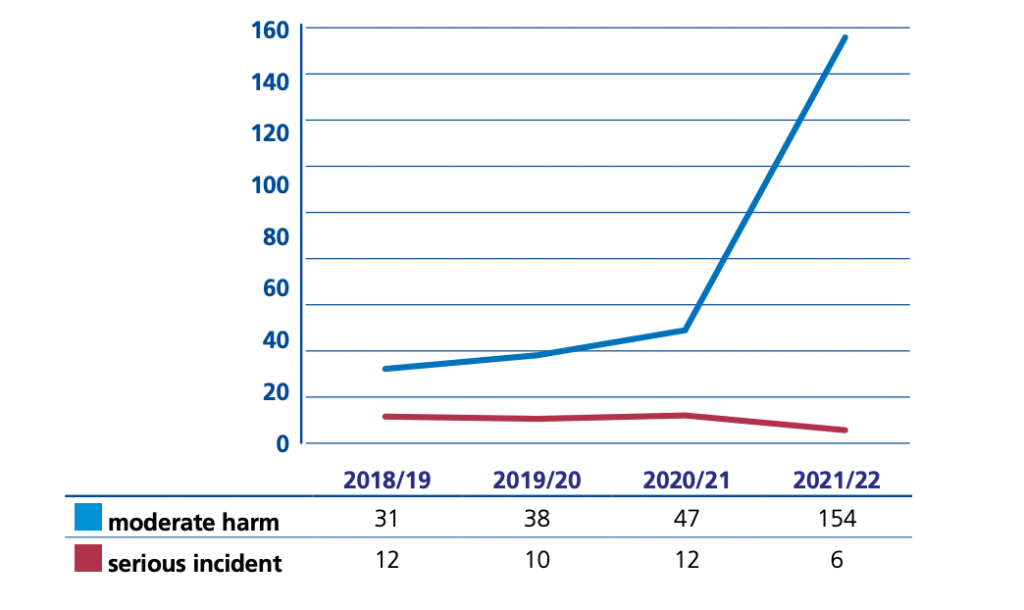
Is NEAS under-reporting serious incidents?
Someone has drawn my attention to a suspiciously low number of serious incidents reported by NEAS.
NEAS has been asked about its apparent outlier status on serious incident reporting.
Public inquiry in light of allegations of criminal breaches
The charade about NEAS’ governance will likely continue, given HSJ’s revelations about the deeply flawed terms of reference for Marianne Griffiths’ investigation of NEAS.
An NHS insider investigation seems a seriously inadequate response to matters which raise Article 2 and alleged criminal breachs of coronial law.
In light of ongoing evidence that NEAS may be obfuscating, given the Article 2 issues and given the extremely serious issues of alleged criminal breaches of coronial law, a fully independent judge led inquiry with statutory powers is needed.
PETITION
Please click and add your signature to this petition to reform UK whistleblowing law – whistleblowers protect us all but weak UK law leaves them wholly exposed, lets abusers off the hook and it is a threat to public safety.
Mark Tattersall Consultant Obstetrician has whistleblown on this practice. He has made past disclosures about patient safety and his evidence on this is held by parliament.
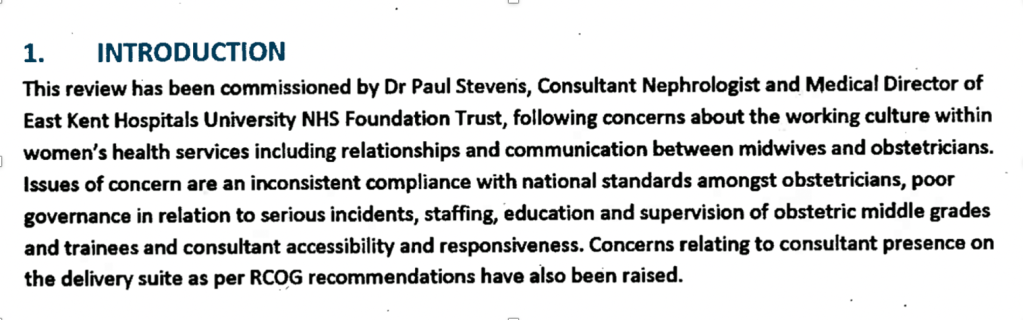
There have been concerns at East Kent maternity services for around a decade, in the context of generally poor trust governance and the CQC placing the trust into special measures in 2014.
The trust came under increased scrutiny as a result of an avoidable death of baby Harry Richford on 9 November 2017. Harry’s mother was a healthy young woman, her pregnancy had been uneventful, and Harry’s death was shocking and unexpected. Harry died due to poor care, which centred around the poor supervision of a locum doctor whom the trust rostered for out of hours duties without checking his competence. The family’s search for the truth and media investigations led to increasing awareness that other families had been affected and that EKHUFT had repeatedly failed to refer cases to the coroner. Systemic failings were confirmed after the commencement of local Healthcare Safety Investigation Branch maternity investigations in 2018. The government ordered the Kirkup investigation as the scale of the failures emerged.
In this post I share documents provided by Harry Richford’s family via @DerekRKENT to explain a key concern – regulatory failure to keep other babies and mothers safe. The documents give an audit trail of failures by EKHUFT to learn, and denial by the Care Quality Commission (CQC) of these systemic risks to the public.
EKHUFT became an embarrassment to the authorities in 2014 when it had to be placed in special measures because of poor governance and unsafe care. Thereafter, CQC reported improvement. Despite evidence of continuing organisational failure and harm, CQC claimed to the Richfords in 2018 there was no breach of EKHUFT’s organisational legal duty under CQC Regulation 12 to provide safe care related to Harry’s death. Two years later, CQC reversed and prosecuted the trust, the first prosecution of its kind.
CQC’s denial that Harry Richford’s death was linked to systemic failings was disproved by the trust’s internal investigation, five expert reports and the coroner’s findings, all of which identified organisational related failings by EKHUFT. CQC denied organisational failure even though EKHUFT failed to refer Harry’s death to the coroner. It was also despite the fact that the trust reported to external authorities that Harry’s death was “expected”, even though EKHUFT had identified that the death was linked to care failings. CQC also claimed it had never seen a highly critical Royal College of Obstetricians and Gynaecologists (RCOG) report on EKHUFT which was carried out before Harry’s death. The RCOG identified many examples of previous poor care, organisational failings and risks, including those which specifically led to Harry’s death. CQC claimed it had not reviewed the report until 2019, despite CQC being aware of a related action plan before that, and despite the fact that the RCOG report was commissioned with the involvement of the CCG and NHS England, who have joint working arrangements with the CQC.
Most recently, it was found that the coroner’s Prevention of Future Deaths report on Harry Richford was not published as it should have been on the chief coroner’s website, and that NHS England’s and EKHUT’s responses to the coroner are missing.
Will the pending Kirkup report reveal the whole truth about the failures at EKHUT and the failures of oversight bodies?
Of relevance to EKHUFT’s future management, since April 2022 the CEO of EKHUFT has been the former CEO at Homerton, under whose tenure the ‘ Unhappy Midwives’ whistleblowing scandal arose. This related to multiple maternal deaths (usually very rare) and poor maternity care. Another Homerton maternity whistleblower, Pam Linton senior midwife, reported concerns to CQC but later discovered via a Subject Access Request that nothing appeared to have been done about her concerns.
Harry’s family in their own words:
Harry Richford’s family tenaciously investigated the factors contributing to Harry’s death and they have set out a summary of their experiences at this website:
For example, through poor staffing and skill mix, poor supervision, lack of drilling for emergencies, lack of quality monitoring, inadequate equipment, inadequate administrative support, poor team processes and dynamics or leadership unconducive to safety culture.
4.138 The review team discussed with NHS England that the National Maternity Assessment Tool recommends the following minimum staffing levels for governance teams:
• Maternity governance lead (who is a midwife registered with the NMC)
• Consultant obstetrician governance lead (Minimum 2 PAs90)
• Maternity safety manager (who is a midwife registered with the NMC or relevant transferable skills).
• Maternity clinical incident leads
• Audit midwife – a lead midwife for audit and effectiveness
Practice development midwife
Clinical educators, to include leading preceptorship programme
Appropriate governance facilitator and administrative support within the maternity department.”
In 2012, the NHS Litigation Authority (now rebranded as NHS Resolution) analysed ten years’ of maternity claims. NHSLA detected patterns in care failings and recommended systems solutions:
“The key risk management themes to emerge from the project are discussed. Namely, the need to: engage with the risk management process at all levels; provide suitable learningand training; ensure appropriate supervision and support; have in place up-to-date protocols and guidance with which staff are familiar; learn lessons from claims.
The report concludes that the most effective way to reduce the financial and human cost of maternity claims is to continue to improve the management of risks associated with maternity care, focusing on preventing incidents involving the management of women in labour, including the interpretation of CTG traces.”
Safe staffing
A critical organisational factor is safe staffing, in both numbers and skill mix.
Under conditions of inadequate staffing in healthcare, staff may make more mistakes and face disciplinary action for what are systems issues. They may report fewer incidents in consequence, fuelling a downwards safety spiral. Hansard recorded such an example at Mid Yorkshire Hospitals in 2016.
Jeremy Hunt former Health Secretary and self-styled ‘champion’ of maternity safety, who made political capital out of appearing to support the patient safety cause, decided not to introduce mandatory NHS safe staffing standards:
We continue to see healthcare scandals, many of which are maternity scandals, across the NHS. As well as harm to the public, there is compensation and litigation cost for the public purse, particularly for maternity cases.
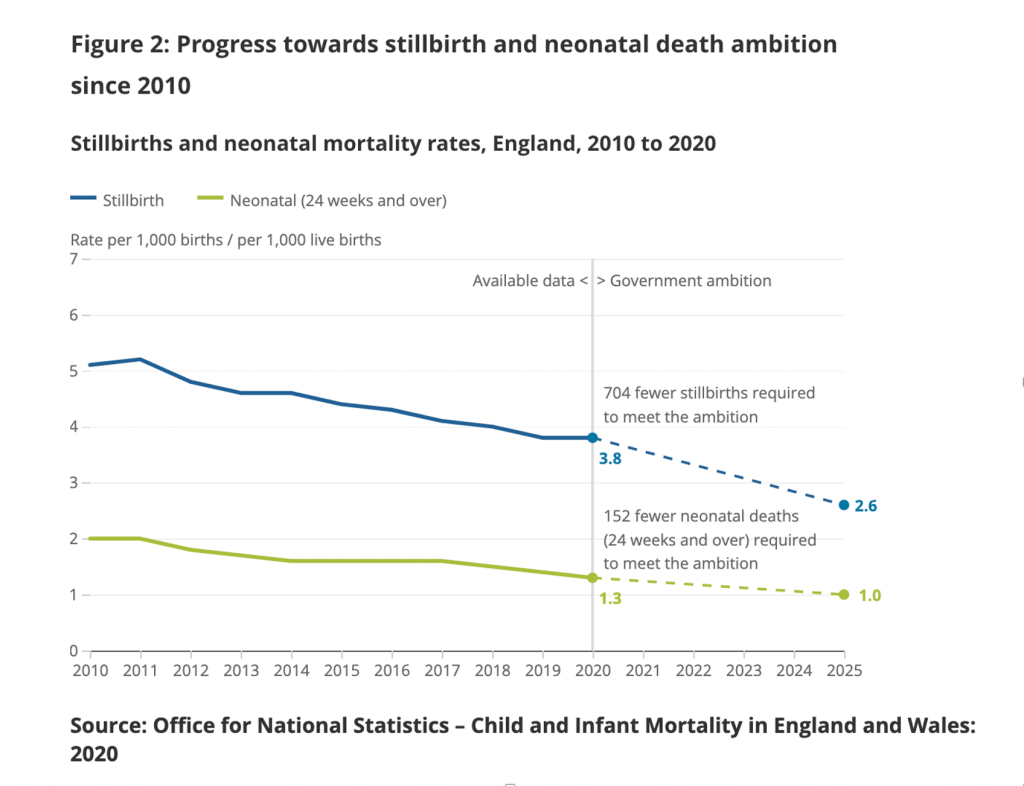
Nationally, some maternity outcomes had previously been on an improvement trajectory. Rates of neonatal deaths, infant deaths and stillbirths fell steadily in previous decades. The rate of safety improvement has slowed under recent Conservative governments. ONS data is available up to 2020 and shows the following trajectory, set against government targets for reduction by 2025:
The final Ockenden report on Shrewsbury and Telford Hospital NHS Trust, published this year, emphasised the importance of safe staffing:
“In the last year since our first report was published we have seen significant pressures in maternity services in the recruitment and retention of midwives and obstetricians.
“It is absolutely clear that there is an urgent need for a robust and funded maternity-wide workforce plan, starting right now, without delay and continuing over multiple years. This has already been highlighted on a number of occasions but is essential to address the present and future requirements for midwives, obstetricians, anaesthetists, neonatal teams and associated staff working in and around maternity services. Without this maternity services cannot provide safe and effective care for women and babies. In addition, this workforce plan must also focus on significantly reducing the attrition of midwives and doctors since increases in workforce numbers are of limited use if those already within the maternity workforce continue to leave. Only with a robustly funded, well-staffed and trained workforce will we be able to ensure delivery of safe, and compassionate, maternity care locally and across England. ”
Current official guidance on calculating required staffing seems elliptical and coy about setting a minimum standard, reflecting the government’s refusal to legislate for minimum staffing. Guidance refers the reader to other guidance, which leaves the ultimate decision with each local provider.
Midwifery staffing red flags
But NICE midwifery guidance from 2015 does recognise that clinical red flags should trigger a review of midwifery staffing:
“A midwifery red flag event is a warning sign that something may be wrong with midwifery staffing. If a midwifery red flag event occurs, the midwife in charge of the service should be notified. The midwife in charge should determine whether midwifery staffing is the cause, and the action that is needed.
• Delayed or cancelled time-critical activity.
• Missed or delayed care (for example, delay of 60 minutes or more in washing and suturing).
• Missed medication during an admission to hospital or midwifery-led unit (for example, diabetes medication).
• Delay of more than 30 minutes in providing pain relief.
• Delay of 30 minutes or more between presentation and triage.
• Full clinical examination not carried out when presenting in labour.
• Delay of 2 hours or more between admission for induction and beginning of process.
• Delayed recognition of and action on abnormal vital signs (for example, sepsis or urine output).
• Any occasion when 1 midwife is not able to provide continuous one-to-one care and support to a woman during established labour.
• Other midwifery red flags may be agreed locally.”
Based on the still steady stream of maternity care scandals, surely we are currently awash with such red flags?
Seriously unsafe midwifery staffing at East Kent Hospitals University NHS Foundation Trust?
In October 2021 the media reported that CQC had found severe staffing shortage in maternity services at East Kent, following unannounced inspections in July 2021.
Was the CQC wilfully blind to organisational failings in maternity care at East Kent?
CQC appeared to ignore internal trust findings and external expert findings of organisational failure
At East Kent Hospital University NHS Foundation Trust, the Care Quality Commission bizarrely refused to acknowledge a link between a serious incident – the death of baby Harry Richford seven days after a catastrophic, avoidable birth injury – and evident systems issues.
This was despite the trust’s internal Root Cause Analysis (RCA) report concluding very clearly that there were multiple systems issues:
“This leads us to conclude that this incident occurred due to system failures.”
The trust RCA acknowledged that there was inadequate vetting of and supervisory support for the locum junior doctor involved in Harry’s death.
The RCA contained a hint that other staff were concerned about having a locum on call, as one midwife rolled her eyes in front of Harry’s mother upon being told which registrar was on call on the fateful night of Harry’s birth.
This raises many questions about organisational factors. It also linked to an earlier RCOG finding that maternity staff had stopped raising safety concerns because Leads did not act upon them.
Whistleblowing governance at East KentHospitals University NHS Foundation Trust
The Royal College of Obstetricians and Gynaecologists (RCOG) was in 2015 commissioned to review governance failures and dysfunctional team relationships in East Kent maternity service.
The College reported that there were issues of poor reporting culture, especially by doctors.
Staff reporting was discouraged by the fact that past concerns were not acted upon.
This speaks loudly of organisational and senior leadership failure.
The Richfords objected to the trust’s internal RCA investigation.
In response, EKHUFT commissioned two expert reports from a neighbouring NHS trust.These reports concluded that there were some failings. Overall, they were not as critical as later expert reports commissioned by the coroner but organisational failure is implied by:
– A concern that the trust may not have adhered to national guidelines on neonatal resuscitation. (This contradicted the trust internal RCA which concluded that resuscitation guidance was followed).
– A suggestion that EKHUFT should put in place a more robust system of training and drilling to ensure that staff were better equipped to deal with neonatal emergencies and resuscitation.
But CQC denied there was organisational failure by EKHUFT in Harry Richford’s case despite the trust’s RCA findings and these local external reports.
CQC appeared to ignore the probity implications of EKHUFT’s flawed reporting to external authorities about Harry’s death
CQC denied there was organisational failure despite the trust’s flawed decision not to refer Harry’s death to a coroner.
The trust justification for this was recorded in the RCA report. An argument was made that no referral was needed because the cause of death was known (and that it was hypoxia). This is a flawed argument. It failed to acknowledge other relevant criteria requiring a referral to the coroner, such as whether a death could be related to a clinical procedure.
The CQC should have seen the trust’s failure to refer Harry’s death to the coroner as a big red flag about organisational competence, probity and safety culture.
Instead, on 17 August 2018 Emma Carroll then a local CQC inspector (now Inspection Manager) wrote to Harry’s family that three management reviews by CQC had concluded that there had only been errors by individual staff, and that the trust itself was not in breach of regulations:
“We have held three management meetings to discuss the information shared by yourself and the trust, including the RCA, both independent reviews, the trust’s action plan and additional information requested from the trust. We have not received confirmation from the senior coroner as to whether they will be progressing with an investigation. However, I have requested CQC are made an interested party which means we will receive the final Coroner’s report.
After an extensive review, we do not believe there has been a breach in regulation. The concerns raised in this incident are centred on an individual’s decision or error. The criminal offences CQC can prosecute against only apply to registered person failures.”
Derek Richford, Harry’s grandfather, challenged this bizarre position.
The exchange of correspondence between Derek Richford and Emma Carroll on 17 August 2018 can be found here.
Instead of shutting down enquiries about organisational failure, the CQC should have been actively pursuing whether EKHUFT had failed to refer other deaths to the coroner, whether there were common themes between deaths and the level of risk posed to the public by EKHUFT’s systems failure.
The coroner later noted with concern the trust’s outrageous claim that Harry’s death was “expected” and its failure to inform the coroner of Harry’s death:
“Concern 17
The child death notification form was incorrectly completed in that Harry’s death was recorded as ‘expected’. No notification was made to the Coroner. No details were filled in on the notification form giving any detail of the problems leading to Harry’s death. As a result, the Child Death Overview Panel would have been unaware of the problems encountered and could not have shared learning to prevent other such deaths occurring. I make no recommendation in respect of the lack of notification to the Coroner as I am aware that the Senior Coroner has already dealt with this.”
Normally, arrangements for reviewing child deaths are very formal and involve substantial multiagency scrutiny.
On a related theme of reporting to external authorities, the coroner also found that EKHUFT’s report about Harry’s death to a national database was inaccurate:
“Concern 18
The MBRRACE form in respect of Harry Richford was inaccurate in a number of important areas. The form is important to provide robust national data to support the delivery of safe, high quality maternal and new born care as well as identifying errors and faults, if any, where there has been a maternal or infant death so that future deaths can be avoided.”
The CQC should have noted that EKHUFT’s MBRRACE submission was inaccurate and that this too was a warning sign.
The coroner noted another serious warning sign about EKHUFT managers’ accountability and transparency:
“Concern 19
Important independent reports do not appear to have been shared within the East Kent Trust’s staff, for instance the HSIB report into Harry’s death appeared during the inquest to be unknown to a number of the staff.”
Both the medical experts, an obstetrician and a paediatrician, concluded that Harry would have been born alive and in good condition if his care had been appropriate.
At inquest, the trust’s lawyers contended there was no neglect but the coroner rejected this and ruled that a contributory factor in Harry’s death was neglect:
“The cause of death was 1a Hypoxic Ischaemic Brain Encephalopathy. There was a narrative conclusion setting out some seven failures in the care of Harry Richford together with a conclusion that his death was contributed to by neglect.”
Coroners’ findings of neglect
A finding of neglect by a coroner is a very serious matter.
“Neglect in this context means a gross failure to provide adequate nourishment or liquid, or provide or procure basic medical attention or shelter or warmth for someone in a dependent position – because of youth, age, illness or incarceration – who cannot provide it for himself. Failure to provide medical attention for a dependent person whose physical condition is such as to show that he obviously needs it may amount to neglect. So it may be if it is the dependent person’s mental condition which obviously calls for medical attention (as it would, for example, if a mental nurse observed that a patient had a propensity to swallow razor blades and failed to report this propensity to a doctor, in a case where the patient had no intention to cause himself injury but did thereafter swallow razor blades with fatal results). In both the cases the crucial consideration will be what the dependent person’s condition whether physical or mental appeared to be”.
Thus, Harry’s case also raised Safeguarding issues, which placed a particularly serious duty on CQC to protect other similarly vulnerable patients.
CQC’s denial of organisational failure was discredited by HSIB’s findings
The exercise was reported in January 2019 and came to similar conclusions as the coroner’s experts.
The Healthcare Safety Investigation Branch (HSIB) also identified abundant evidence of organisational failures and lack of learning by EKHUFT.
Of note, HSIB identified that the trust had not followed its own policy (Engaging the Temporary Workforce, 2014) on checking the competence of locum staff. This policy recognised that the trust had a duty to proactively mitigate risk when locums are assessed as not being competent, for example by restricting practice or increasing supervision.
The trust had also not followed RCOG guidance on consultant attendance for certain procedures if a trainee has not been signed off as competent:
“The RCOG green-top guideline 2011 and Trust guideline 2015, recommends that a consultant obstetrician should attend in person for a trial of instrumental delivery if the trainee has not been assessed and signed off as competent. The Trust guideline also identifies caesarean section at full dilatation as a procedure the consultant should attend inperson if the trainee has not been signed off for independent practice for the procedure. The locum doctor’s competency was unknown.”
“Sharing pre-published HSIB investigation reports and recommendations. To be open and transparent when in receipt of information regarding the safety of services that are registered with CQC and funded by the NHS in England. The information is shared with the CQC in a timely way through the named CQC contact or by a representative delegated by them.”
HSIB began its local maternity investigations in 2018. In February 2020, at the same time as the coroner’s PFD report was issued, HSIB produced a summary report on its local investigations at EKHUFT. In this report, HSIB observed that the same errors kept being made at EKHUFT:
“From December 2018, HSIB engaged frequently with the Trust to present evidence of recurrent patient safety concerns in its maternity services. Despite repeatedly raising these concerns with the Trust, HSIB investigators continued to see the same themes reoccurring and in August 2019, asked the Trust to self-refer themselves to their CCG and the CQC.”
HSIB also wrote to the CQC about the problems at EKHUFT in August 2019.
CQC knew without any doubt by August 2019 that there were organisational failings, linked to ongoing serious harm. By January 2020, a rare maternal death was amongst the EKHUFT incidents investigated by HSIB (page 3 HSIB summary report).
The reported reason for delay was COVID operational pressures.
A question arises of CQC’s competence in identifying organisational failings and system risks, and or alternatively, its willingness to acknowledge them.
Another question is at what level of seniority in CQC was the original flawed conclusion reached about absence of organisational failings?
Harry’s grandfather Derek Richford objected to the CQC’s 17 August 2018 denial of organisational failure. He copied his objection to Ted Baker, then Deputy Chief Inspector of Hospitals.
Importantly, the RCOG report revealed that there had been previous concerns about the supervision of junior doctors, consultant availability and the general management of the labour ward at EKHUFT:
In other words, there were systems issues aplenty.
There were numerous examples of poor care and the RCOG described some clinical practices as “dangerous”, such as the poorly supervised use of Syntocinon.
The RCOG found evidence of poor whistleblowing and reporting practice. Consultants’ poor practice tended not to be challenged, or was omitted from incident action plans. Staff stopped raising concerns because they were not acted upon:
“Safety issues relating to practice were not reported as no action would be taken by the Leads.”
Indeed, the RCOG report was commissioned because of concerns about poor governance and team dysfunction in the EKHUFT maternity service:
In other words, organisational failures and systemic risks, as opposed to CQC’s narrative of isolated errors by individuals.
Specifically, the RCOG found evidence of patient harm related to locum doctors’ omissions, whilst working out of hours:
“The locum registrar did not review the patient overnight despite this woman’s details being on the handover sheet.” (Case 6 page 16)
The RCOG was concerned that safety could be affected by middle grade locum cover at night (page 34 and 35).
This proved to be an accurate concern in the light of the later harm to Harry Richford.
Even EKHUFT’s medical director observed, in terms, in a statement of 17 December 2019 to the coroner that Harry’s death was part of a chain of persistent failure and lack of organisational learning linking back to the RCOG report:
“The analysis of the root cause of Harry Richford’s death led to actions similar to some of those in the RCOG review, CQC reports of 2014-2016 and the HSIB recommendations, indicating a failure to sufficiently embed learning.”
Shockingly, it was reported that the CQC had never, until 2019, reviewed the 2015 RCOG report despite knowing of its existence.
“But what is perhaps even more shocking is that the Care Quality Commission did not see the report for nearly three years after it was written in February 2016. The CQC confirmed although it saw an action plan based on the report, its records indicate it did not see the report itself until January 2019.”
“Review report is clear – the Trust does not have an unsafe maternity service but there isimprovement work to do around how the service is run in some areas.”
(Board papers indicated that in the corporate risk register later that year, maternity risk is rated as “extreme”).
It also stated:
“The MBRRACE-UK report has been published and shows the Trust to have a 10% lower average mortality rate for its comparator group. The RCOG report was received on the 18th February. Actions will need to be incorporated into the improvement plan. The deadline for embedding the new maternity dashboard has slipped and will be in place for the end of March 16.”
The comment about favourable MBRRACE-UK ranking is interesting in the light of the coroner’s finding that EKHUFT made an inaccurate submission to MBRRACE-UK about Harry’s death, and in light of today’s revelations in the Telegraph about possible manipulation of NHS deaths reporting.
Why did CQC claim that EKHUFT maternity services had improved and why did it deny that there were organisational failures?
EKHUFT’s response to the RCOG report is published via an undated entry on the trust’s website. It reads as a post hoc communication, drafted in the fallout from Harry Richford’s case.
EKHUFT’s response cites in its defence the praise that it received from CQC in 2018, at which time the Richfords were struggling to be heard by CQC:
“A further CQC inspection in August 2018 acknowledged that the East Kent maternity service had made great strides to drive learning, improve outcomes and improve innovation through a collaborative and multidisciplinary approach but there were continued concerns in several areas indicating that more improvement work remains to be done.”
“…it is not possible to evidence all actions from that report as having been completed. 23 recommendations were made by the RCOG. When the available evidence was reviewed the LRC concluded there was sufficient evidence that 2 recommendations had been met, that 11 had been partially met. For some of the recommendations where evidence weas [sic] insufficient…”
Why did CQC not identify this evidence of organisational failure sooner?
Was the imperative to create a positive narrative of improvement more important?
If so, from where did the imperative come?
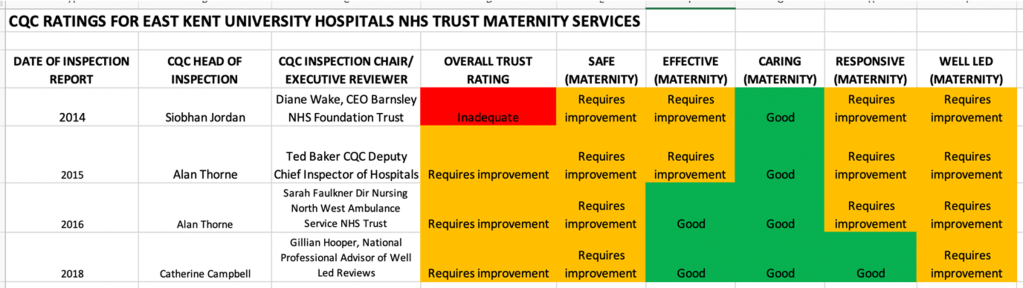
This is how CQC progressively rated EKHUFT’s maternity service, after putting the trust in special measures in 2014
“His visit gave him the opportunity to see for himself the progress that the Trust has made and he was quoted in the post-visit press release as saying:
“I saw first-hand the great strides in improving the quality of care that the Trust is making and the positive effect these changes are having on staff and patients.
“I enjoyed meeting and talking with a wide range of members of staff from across the hospital. It was very clear that everyone is passionate and united in their desire to continue to improve services.”
This brings to mind witness testimony from the Mid Staff Public Inquiry that officials were focused on an imperative of not embarrassing the Minister.
What was CQC and NHS England’s coordination on the critical RCOG report?
A relevant recommendation from Morecambe Bay, which was accepted by the government, was that trusts should be under a duty to disclose external investigations.
“46. In the meantime, Monitor and the Care Quality Commission will continue to use their respective statutory information-gathering powers to require NHS Trusts and Foundation Trusts to notify them of both the commissioning and the conclusions of relevant external investigations.”
Did the CQC actually make any changes to its procedures, following the government’s promises in 2015 that CQC would compel disclosure of external investigations by NHS trusts?
Why did CQC reportedly not ask for a copy of the RCOG report when it first became aware of the report’s existence?
Why did CQC appear to accept the trust’s action plan as a reliable interpretation of the RCOG’s findings and recommendations, instead of insisting on seeing the report itself?
“Maternity services were reported as inadequate within the CQC report given the lack of progress…. The CCGs with NHSE and the trust have commissioned a Royal College review which is underway to support the service to make further improvements.”
“2.2 We commit to working together proactively to share information and intelligence about the quality of care in order to spot potential problems early, and manage risk. To do this we seek to explore ways of sharing data where there is a shared interest or common benefit.”
Did a risk summit of some sort take place about EKHUFT maternity services, as is common practice?
How could CQC plausibly claim that there were no systems issues if its fellow regulator, NHSE, had instigated an RCOG governance review based on CQC’s own inspection findings of systems failures?
Why did CQC change its mind about prosecution under Regulation 12 and why has CQC not applied Regulation 12 more consistently?
What changed between 2018 and 2020? The facts of Harry’s case did not change. And CQC Regulation 12 did not change.
I asked CQC to comment on its various actions and omissions,. I also asked CQC about why it informs bereaved families such as the Richfords that it cannot investigate their concerns, when the discharge of CQC Regulation 12 appears to require investigation by the CQC.
CQC has to date only acknowledged my enquiry and indicated that it would respond.
It does seem very arbitrary as to how the CQC responds to harmed patients and families.
What happens to families who are no less seriously harmed than the Richfords, but who may be less articulate and cannot navigate CQC’s obstacle course?
Reservations about the usefulness of fining public bodies aside, why had CQC not taken a similar approach to other gross and proven NHS care failures?
Has CQC obscured the real levels of unmet need and harm, and how much will Kirkup’s report reveal?
A September 2022 BBC analysis of CQC reports shows that maternity service failings are widespread, with 7% of units rated by CQC as “posing a high risk of avoidable harm”.
Given what we know about CQC’s identification of systems risks, is the real figure higher?
Kirkup’s investigation of maternity services at EKHUFT is due to report on 19 October 2022.
Will he identify all relevant failings, regulatory, corporate and individual?
I was concerned that in a previous investigation, into the death of baby Elizabeth Dixon, Kirkup placed much emphasis on failings and dishonesty by individual practitioners.
His notable comment that there had been “a twenty year cover up” generated many headlines.
But did he do justice to Elizabeth’s parents through a thorough examination of controlling minds and corporate accountability? Should he have undertaken a more searching exploration of the powerful senior management of a favoured NHS trust, Frimley Health NHS Foundation Trust?
Frimley Health NHS Foundation Trust knew about the Dixons’ concerns for years before Kirkup investigated, and had plenty of chances to put the matter right.
Let us hope for better this time round, and that the CQC’s serious failure to help prevent deaths is fairly reflected in Kirkup report. And that the role of other oversight bodies is also fully explored.
The curious non-publication of Harry Richford’s PFD report, and NHS England’s and EKHUFT’s missing responses to the coroner
The public bodies which received a copy of Harry Richford’s PFD – the coroner’s report to Prevent Future Deaths on matters arising from Harry’s inquest – were legally obliged to respond to the coroner’s concerns about mitigating risk of future of deaths.
A troubling discovery in the course of checking organisational responses to the coroner was that I found Harry Richford’s PFD was not published by the chief coroner, as it should have been.
It is not known if the PFD was originally published, and then removed at some point. If anyone clearly recalls seeing it on the website, I would be grateful to know.
A worker at the chief coroner’s office kindly checked and agreed with me that as of 11 October 2022, the Richford PFD was missing from the website, and so the organisational responses were also missing:
“We have a system to allocate reference numbers to reports. I’ve checked the website and Harry Richford (2020-0117) report has not been published but 0116 and 0118 have been. I checked our system and found a response from DHSC, I will upload these shortly on our website.”
The PFD and the government response have since been uploaded here.
The ministerial response noted the trust’s unacceptable and misleading claim that Harry’s death was “expected” and its failure to refer his death to the coroner.
The DHSC should hold progress reports by CQC and NHSE on improvement work at EKHUFT, if this ministerial commitment was honoured:
“I expect to be regularly updated.”
However, neither the chief coroner nor the local coroner have so far been able to locate NHS England’s response or the trust’s response.
At this late stage, this seems an unusual anomaly.
I will post the NHS England and trust responses below when I eventually obtain them. Or if it transpires that NHS England and or the trust failed to respond to the coroner, I will confirm this.
RELATED ITEMS
The above failures are part of a familiar pattern of government failure.
Both the CQC and Jeremy Hunt as Health Secretary failed to act on whistleblowers concerns at Homerton:
Dr Minh Alexander retired consultant psychiatrist 15 October 2022
In 2018 the government commissioned a review of Fit and Proper Persons in the NHS after a number of scandals and also concerns about the Care Quality Commission’s application of CQC Regulation 5 Fit and Proper Persons:
NHS England, despite being one of the targets affected by Kark’s recommendations, was put in control of implementing the recommendations.
Unsurprisingly, NHSE has dragged its feet and been secretive about the work undertaken these past few years, albeit it has attributed some of the delay to lack of government permission. At the last update earlier this week, NHS England advised that the terms of reference for its NEW Kark Steering Group will be finalised at the start of next month.
The GGI states on its website that it employs as a senior consultant, Mason Fitzgerald a director sacked last year by the NHS after a furore about CV inaccuracy.
GGI previously failed to answer a question about this.
Material by the GGI that is in the public domain raises questions about whether the GGI – and indeed possibly Mason Fitzgerald – may be undertaking other work with NHSE and Integrated Care Systems.
I have asked NHS England to review it systems, approach to contracts and its relationship with the GGI.
This is the relevant letter to Ruth May, with the details, and is copied to Amanda Pritchard NHSE CEO, the NHSE director responsible for the Kark report implementation and Tom Kark QC:
BY EMAIL
Ruth May
Chief Nursing Officer
NHS England
15 October 2022
Dear Ruth,
NHSE, the Good Governance Institute’s governance and Mason Fitzgerald, sacked former NHS director
I write to follow up my response to your social media promotion of the GGI’s work on a staff survey conducted by the GGI, for your team:
I am really concerned that senior NHS managers appear either oblivious of, or unconcerned about, the GGI hiring Mason Fitzgerald, an NHS director sacked last year after false CV claims.
The current GGI website profile for Mason Fitzgerald, described as a GGI ‘senior consultant’, omits to mention anything about his sacking. See attached screenshot and link:
As you may recall, Mason Fitzgerald’s false CV claim was missed by ELFT and the CQC, but emerged after he was almost appointed as CEO of NSFT. Had that appointment process been completed, he would have had power over thousands of extremely vulnerable mental health patients:
The GGI appears to be unaccountable regarding its hiring of Mason Fitzgerald. When I wrote to the Institute in April this year about it hiring him, it failed to respond.
According to the GGI’s material, a number of NHS organisations continue to use its services.
In particular, the GGI published a blog by Mason Fitzgerald on 10 October 2022, in which he stated:
“GGI is currently working with ICSs to review their governance arrangements, and, through our networks and events, we are developing thinking on how ICSs should approach their first end of year review.”
The GGI tweeted this blog on 11 October 2022, tagging in NHS England (see screenshot), raising a question of whether NHS England is a partner in this work and has commissioned the GGI to undertake this project:
According to a response to this tweet by the GGI Chief Executive, the GGI is working with 13 Integrated Care Systems:
Does the NHS therefore still employ Mason Fitzgerald, as a senior consultant, through the GGI?
If so, is it appropriate for an individual sacked by the NHS after false CV claims, to be vetting governance by NHS organisations?
I am especially concerned if NHS England promotes the GGI or contracts with the GGI in the light of its hiring of Mason Fitzgerald, because NHS England is supposed to be implementing the Kark recommendations on tracking impaired or unsuitable NHS managers.
If NHS England had implemented the Kark recommendations in a timely and effective way, Mason Fitzgerald’s subsequent role at the GGI would have been flagged up if he undertook any work for the NHS through the GGI.
I ask that:
a. NHS England and its officers stop all promotion of the GGI until the issue of the GGI’s employment of Mason Fitzgerald, and the questions arising from this about the GGI’s governance, are further clarified and addressed,
b. NHS England reviews any existing contracts with the GGI based on the evidence, through the GGI’s hiring of Mason Fitzgerald, that the GGI’s choice and deployment of consultants and its governance are in question. Please also review whether Mason Fitzgerald is currently working for NHS England, any ICS or any other NHS body under NHSE’s control, as a GGI senior consultant.
c. NHS England considers in its Kark implementation the specific issue of whether NHS managers sacked by the NHS may resume employment through the back door as consultants, and that NHSE designs Fit and Proper Person systems that are strong enough to detect such a situation.
d. NHS England considers generally in its Kark implementation how it will ensure that consistent Fit and Proper Persons standards apply to contractors and contracted services, in the same way that it currently makes other quality requirements of contractors, through the way NHSE’s contracts are drafted.
I copy this to Amanda Pritchard, Jacqueline Davies NHSE lead director for the Kark implementation and to Tom.
With best wishes,
Minh
Dr Minh Alexander
Cc Amanda Pritchard NHS England CEO, Jacqueline Davies NHSE Director of Leadership, Lifelong learning and talent , Tom Kark KC
UPDATE 15 MARCH 2023
Unsurprisingly, Ruth May CNO NHS England ignored me entirely. I wrote to her boss Amanda Pritchard CEO NHSE England in December 2022, who also ignored me.
I reminded them both via social media, but they continued in their silence.
I have now filed a formal complaint with NHSE England’s National Head of Complaints, copied to the Secretary of State and House of Commons Health Committee.
The correspondence to Pritchard and the formal complaint can be found here.
In the meantime, the Good Governance has promoted Mason Fitzgerald from “senior consultant” to “Director of Consultancy and Principal Consultant”. How much of this rise has been based on NHS work?
UPDATE 4 JULY 2023
I heard that the Kark implementation work had been held up as part of the NHS Workforce plan delay. However, the NHS Workforce plan has now been published and there is little sign of Kark review implementation in the plan. I have written to Navina Evans, erstwhile consultant psychiatrist former medical director then CEO of East London NHS Foundation Trust and former colleague of Mason Fitzgerald, now NHS England’s Chief Workforce Officer, to seek clarification.
This is on the same day of news that the Insolvency Service has banned the former CFO of Carillion for eleven years, for making inaccurate and misleading financial statements.
In the NHS, it is said that CFOs are generally penalised by the centre for NOT making over optimistic financial statements.
RELATED ITEMS
NHS England and its predecessor bodies have plenty of form on erring senior NHS managers.
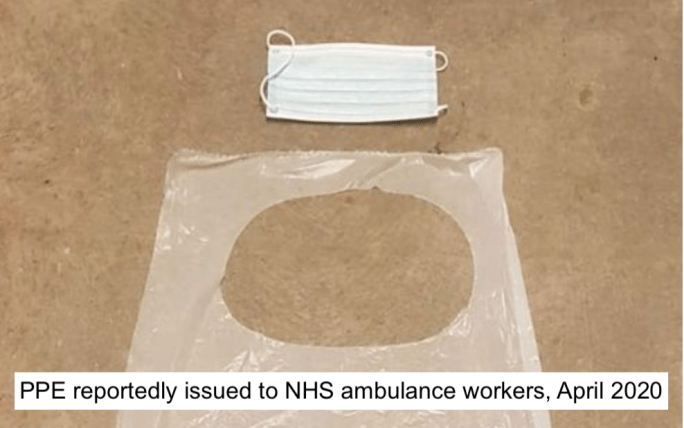
A particularly tragic aspect of the pandemic is that key workers, including NHS workers who continued to work to help keep us all safe, died and suffered some of the worst COVID injuries due to their greater exposure.
For a long time into the pandemic, key workers were not supplied with suitable personal protective equipment (PPE).
This was revealed by the Liverpool Echo, so the disclosure most likely related to North West Ambulance Service.
As well as the serious COVID injuries sustained by key workers such as NHS staff, due to the major mishandling of the pandemic, there was also a cost in added workforce shortage and pressure.
Grace Pritchard a member of the public did a great public service last year by making FOI requests to NHS trusts and universities, via the What Do They Know website. She asked about statistics on staff who developed long COVID.
Her requests and the responses to these requests, are collected at this page on the website:
Disturbingly, some NHS trusts failed to respond at all to Grace Pritchard, including powerful organisations such as Imperial Healthcare, Barts and University Hospitals Birmingham.
Some NHS trusts replied, equally disturbingly, that they did not hold the requested data, implying that no one was actively tracking harm suffered by their staff. For example, St Georges, East of England Ambulance, Sheffield Health and Social Care (the home of Tim Kendall, the NHS mental health Tsar).
Table 5 of the September 2022 ONS spreadsheet gives data on the percentage of people in the “health care sector” affected by long COVID as 3.76%. This figure is an estimate based on scaling up a sample.
But this is not the same as specific, precise data on how NHS staff have been affected by long COVID.
I therefore asked NHS Resolution, which handles staff personal injury claims in the NHS, if it held national data on long COVID personal injury claims by NHS personnel.
NHS Resolution advised that it could not answer without a manual search of case files, because it has no specific code for long COVID (which could be used to run a computer analysis).
“We are unable to answer this request, as we do not have an injury code for Long Covid.”
According to NHS Resolution, to answer my question based on a manual search would reportedly exceed the legal cost limits for FOIs:
“We are unable to provide this information without interrogating individual claims files. Although NHS Resolution may hold some information relating to claims such as what you have requested (England only claims), due to the way claims are recorded on our claims database, we will not be able to identify such specific cases. It might be helpful to explain that when claims are notified to NHS Resolution they are categorised against pre-defined cause, injury and speciality codes. Unfortunately, we do not have a code thatwould allow us to readily extract claims where the injury is due to long COVID. Therefore, while there may be information held in our records, we are not readily able to identify the relevant files by searching the database. To do so would involve a manual review of all cases to identify the claims where the injury is due to long COVID. We estimate we would need to spend approximately 10 minutes reviewing each claims file to identify and extract the relevant information. We would need to review hundreds of claims.”
I have accordingly asked NHS Resolution for more details on how cases of long COVID might be coded under its systems, and I have narrowed the original scope of my request for data on long COVID claims to just three NHS trusts.
It is a concern that there is apparently no central record, at least by NHS Resolution, of the number of NHS staff who are taking legal action for COVID injuries.
I have now asked the Department of Health and Social Care whether any public body holds central data on numbers of NHS staff long COVID cases and personal injury claims, and if the Department holds any of this data, for disclosure of the data itself.
UPDATE 12 November 2022
The DHSC has responded. It does not hold data on NHS staff affected by Long COVID. It has no intention of collating this data. I have sent the DHSC’s response to the UK COVID public inquiry:
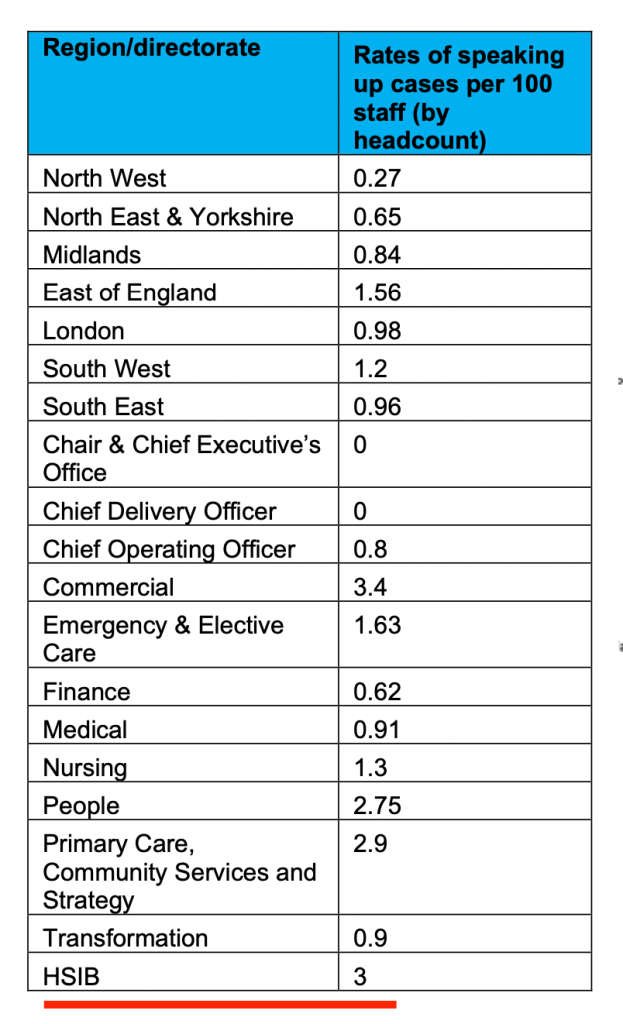
The report shows that out of all NHS England’s departments, the Healthcare Safety Investigation Branch (HSIB) has the second highest rate of whistleblowing complaints, at 3 cases per 100 staff:
Whatever NHS England has done following the much-publicised bullying and whistleblowing at HSIB in recent years, it does not seem to have reduced the need for staff to whistleblow.
The NHS England department with the highest rate of speaking up is the Commercial directorate, at 3.4 cases per 100 staff. One wonders what the disclosures concern.
The great variability in rates between NHS England departments is striking: from zero to 3.4 cases of speaking up per 100 staff.
The annual report contains the usual Freedom To Speak Up propaganda – that staff feel more able to speak up, that managers are taking it more seriously, etc…
This narrative is unconvincing though, when there is a current whistleblowing Employment Tribunal claim against NHS England.
The Freedom To Speak Up report in fact reveals that the majority of NHS England’s whistleblowers do not want their name revealed to the rest of the organisation:
“7. The number of cases received in 2021/22 (152) almost tripled in comparison to the previous year (56). The proportion of people speaking up anonymously fell from 59% to 35%. However, the proportion of people who wanted their name kept confidential rose 7% from 58% to 65%.”
Given the Machiavellian nature of the organisation, exactly how secure is its internal Freedom To Speak Up system and how confidential can any disclosures be?
We have recently seen a case emerge from the Royal Free NHS Foundation Trust of a Freedom To Speak Up Guardian cooperating with the employer’s detrimental withholding of information from whistleblower Dr Rajai Al-Jehani:
NHS England is the Great Keeper of NHS Secrets and Dirty Deeds by the Department of Health and Social Care. It has helped to suppress whistleblowers in NHS provider organisations, and it often enforces silence by these organisations, to oil the wheels of government. Silencing of its own whistleblowers is to be expected.
Moreover, NHSE’s annual Freedom To Speak Up report urges greater human resources influence over whistleblowing processes at NHSE, when in fact human resources are a weapon deployed against whistleblowers.
“Closer collaborative working between FTSU Guardians and HR BPs in relation to directorate/region wide people-related initiatives eg anti bullying; civility and respect and inclusion.”
This suggestion is contrary to the 2015 Freedom To Speak Up Review report, which was critical of NHS organisations turning whistleblowing into an employment issue.
I would advise NHS England whistleblowers to be extremely circumspect about using internal whistleblowing routes. If a better way is possible, and after taking careful advice, take it.
Lastly, let us not forget that NHS England and its predecessor bodies have provided what has been called a “donkey sanctuary” for disgraced NHS serious managers, who are removed from wreaking damage on the frontline but are allowed to keep fat salaries.
Or that NHS England has dragged its feet for years on implementing the recommendations of the Kark Review, to introduce a system for identifying, tracking and debarring unfit NHS managers.
NHS England has to date refused to do anything about Cubbon, now its Chief Delivery Officer.
And the reported rate of whistleblowing in his team? Zero
Dr Jasna Macanovic’s whistleblowing case
Dr Macanovic’s remedy hearing will be held shortly, but no compensation is enough for the years long ordeal that she suffered, with all the usual personal costs of a traumatic whistleblowing experience.
Both ET judgments issued to date in her Employment Tribunal claim contain valuable detail about the governance failures:
Please click and add your signature to this petition to reform UK whistleblowing law – whistleblowers protect us all but weak UK law leaves them wholly exposed, lets abusers off the hook and it is a threat to public safety.
Another recent example of an NHS whistleblower who was unprotected and unfairly dismissed despite the introduction of the ineffective Freedom To Speak Up model is Jane Archibald Senior Nurse. She was specifically failed by the Freedom To Speak Up system at her trust:
By Dr Minh Alexander retired consultant psychiatrist 8 October 2022
Summary: I write to share FOI data from the Care Quality Commission (CQC) which raises questions about CQC’s approach to its Specialist Advisors. According to the FOI response, the CQC excludes Specialist Advisors from its staff survey. A disclosed CQC document states that CQC regularly collates feedback from Specialist Advisors, and this is sent to Directorates for “continuous improvement”. However, the CQC claimed in its FOI response letter to me that it holds no analysed data from this feedback. CQC’s disclosed document shows that it collects data on whether Specialist Advisors decide to withdraw from its inspections. However, CQC claimed to me that it does not hold data on the number of Specialist Advisors who have resigned from their role. What are we to believe? That the CQC has not collated data despite its documented claims that it does? Or that CQC collated data but destroyed it? Or does CQC hold analysed data on Specialist Advisor feedback and resignations, despite its current denial? I have asked Ian Dilks CQC Chair to look into these anomalies.
Background:
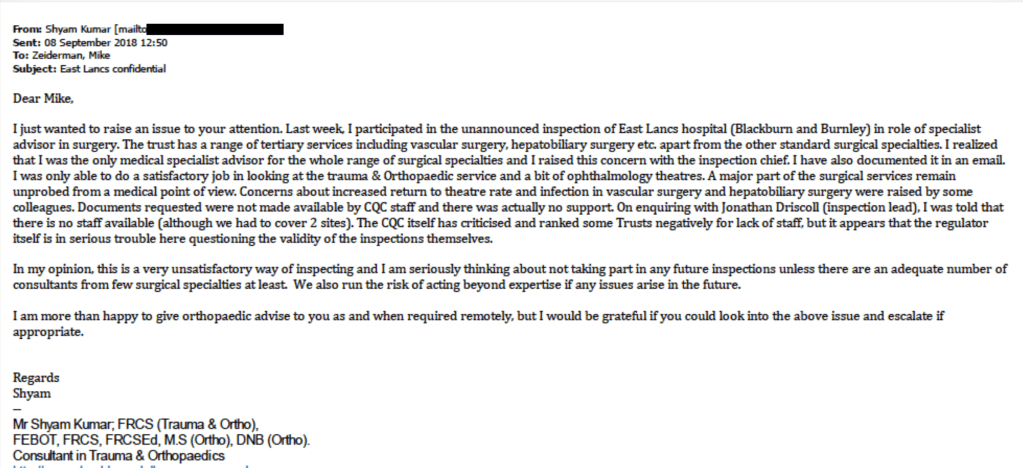
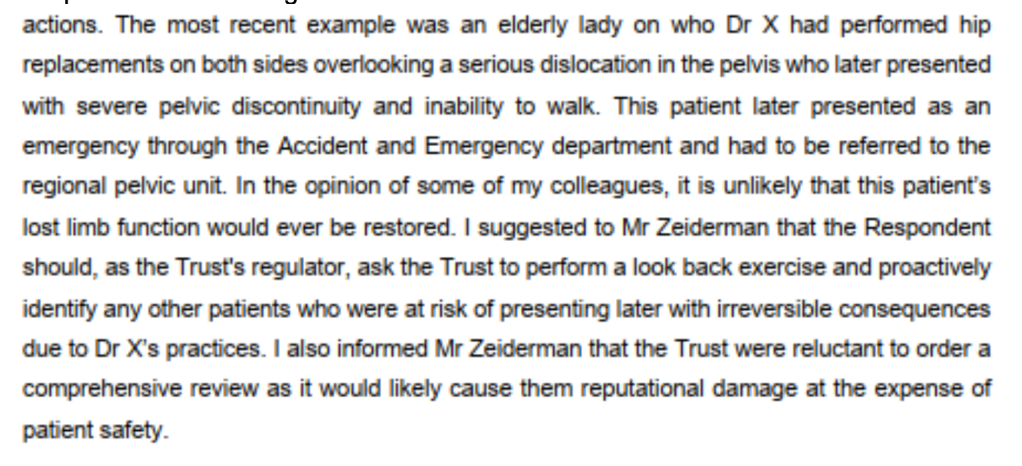
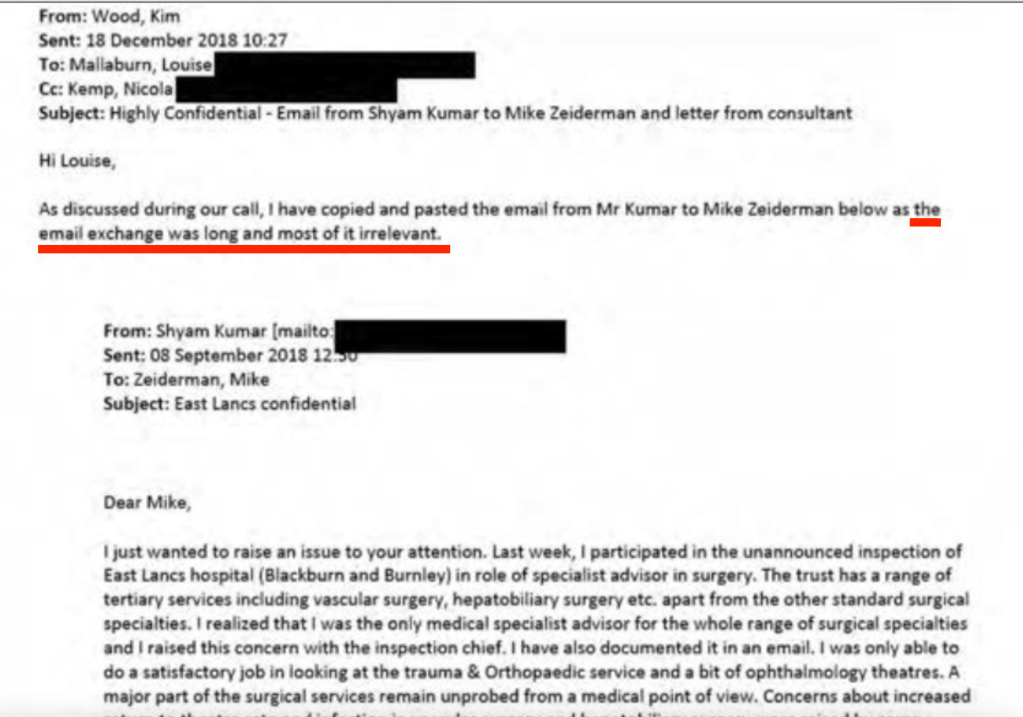
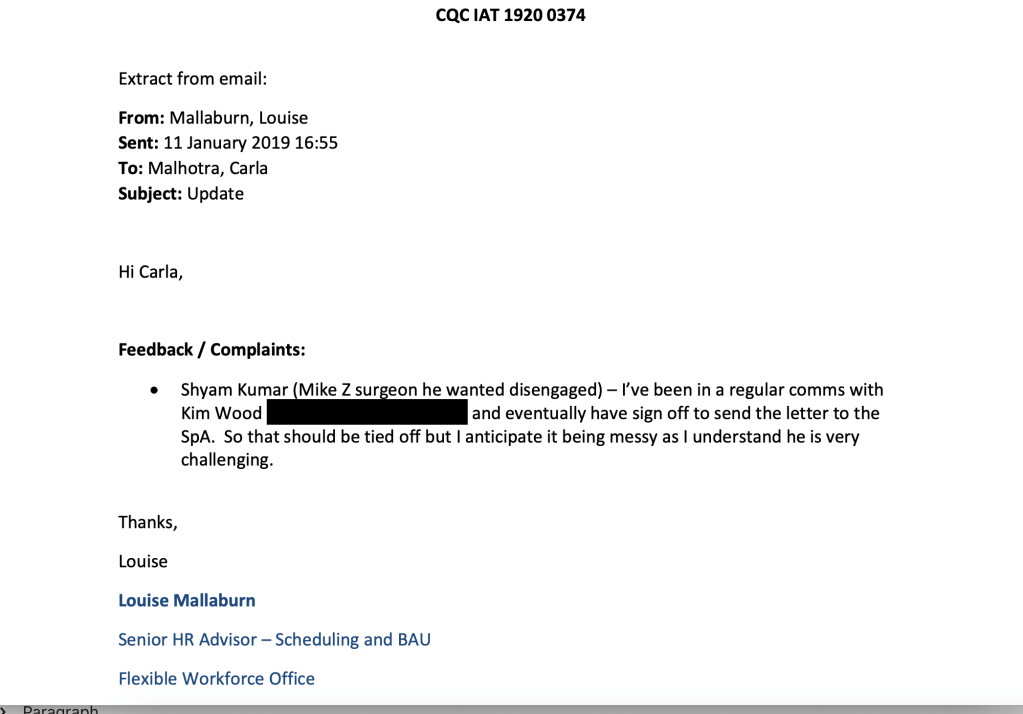
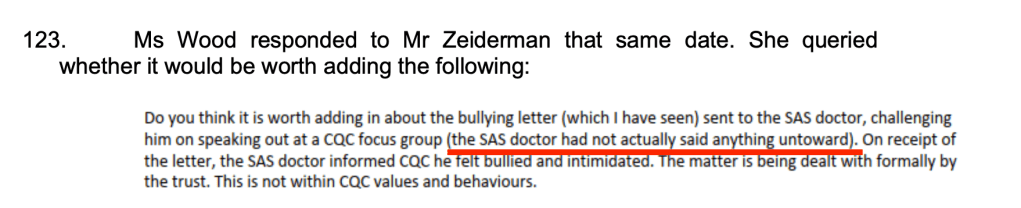
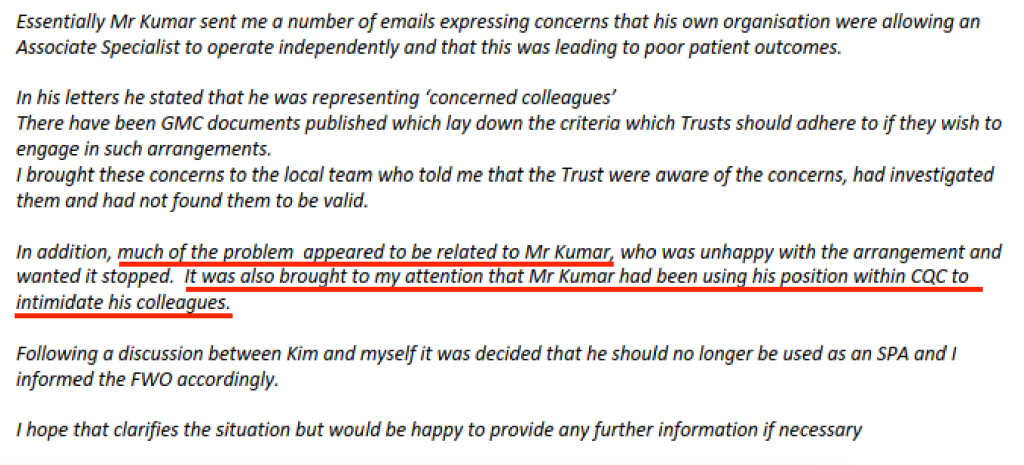
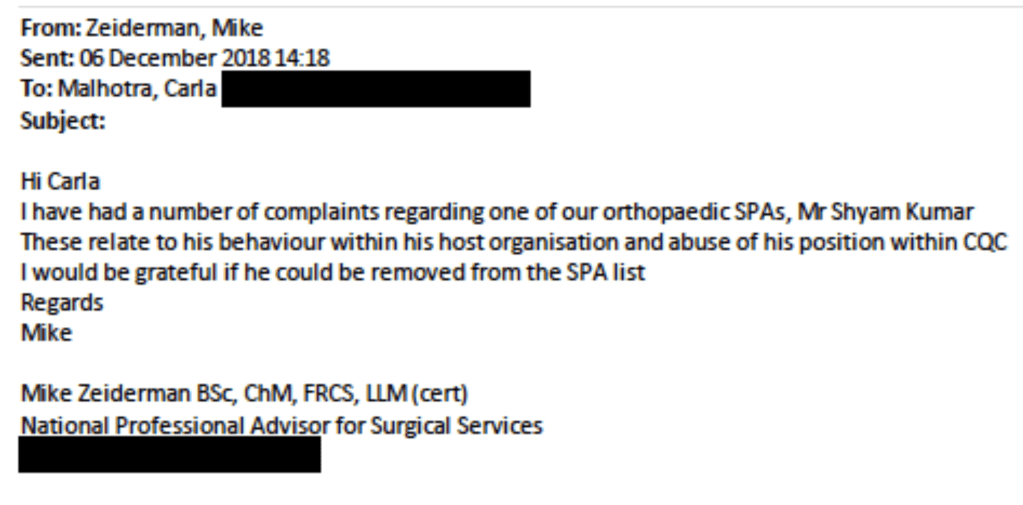
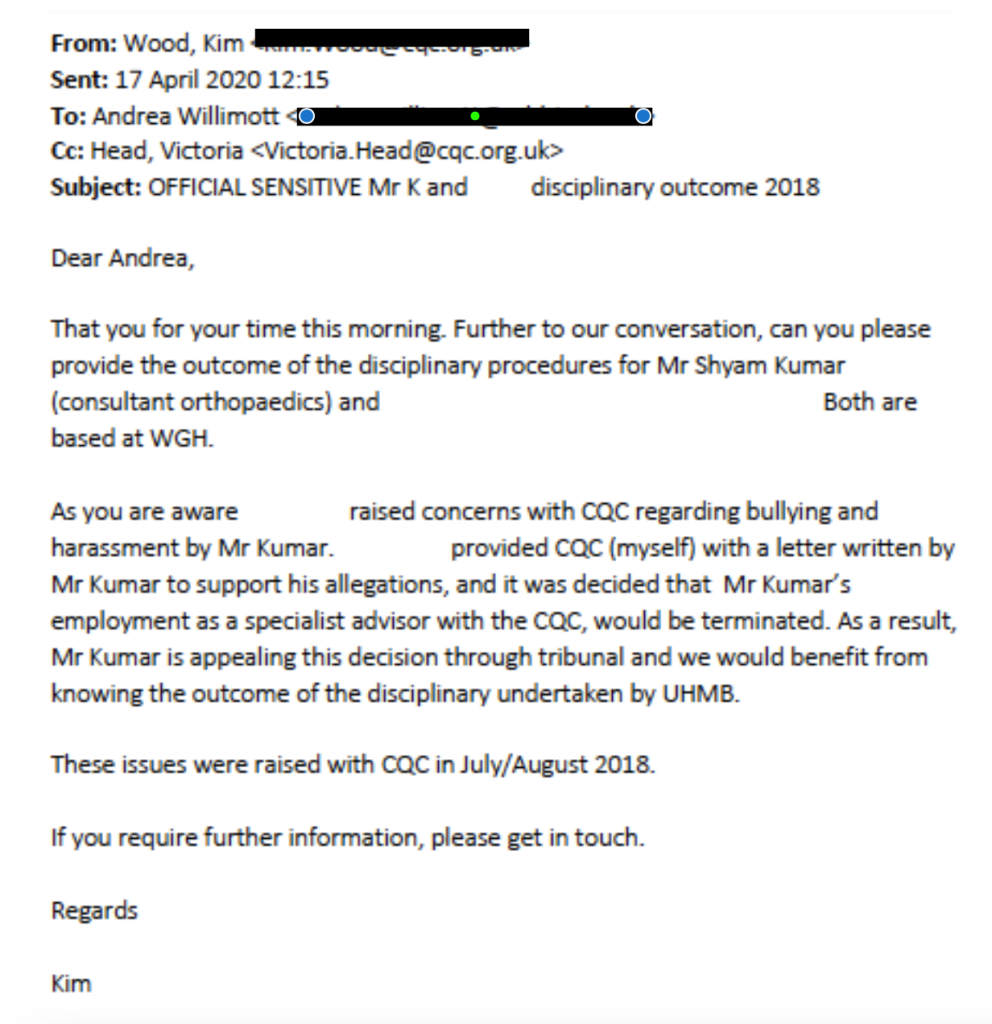
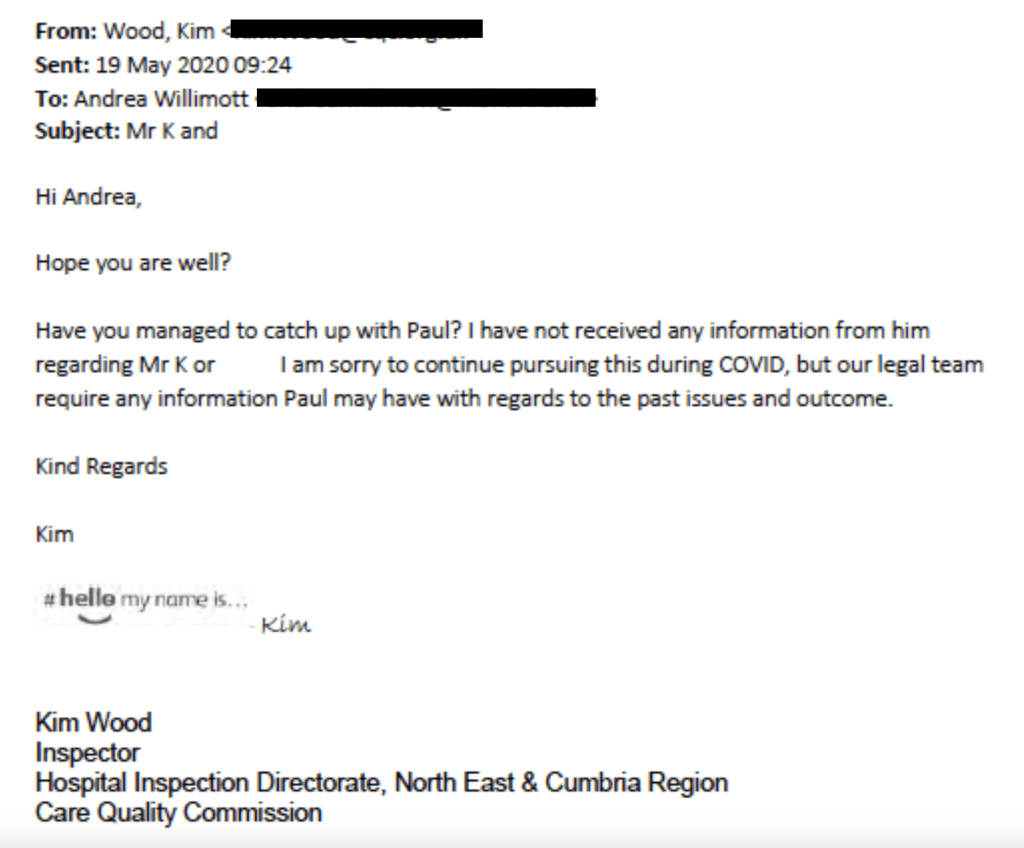
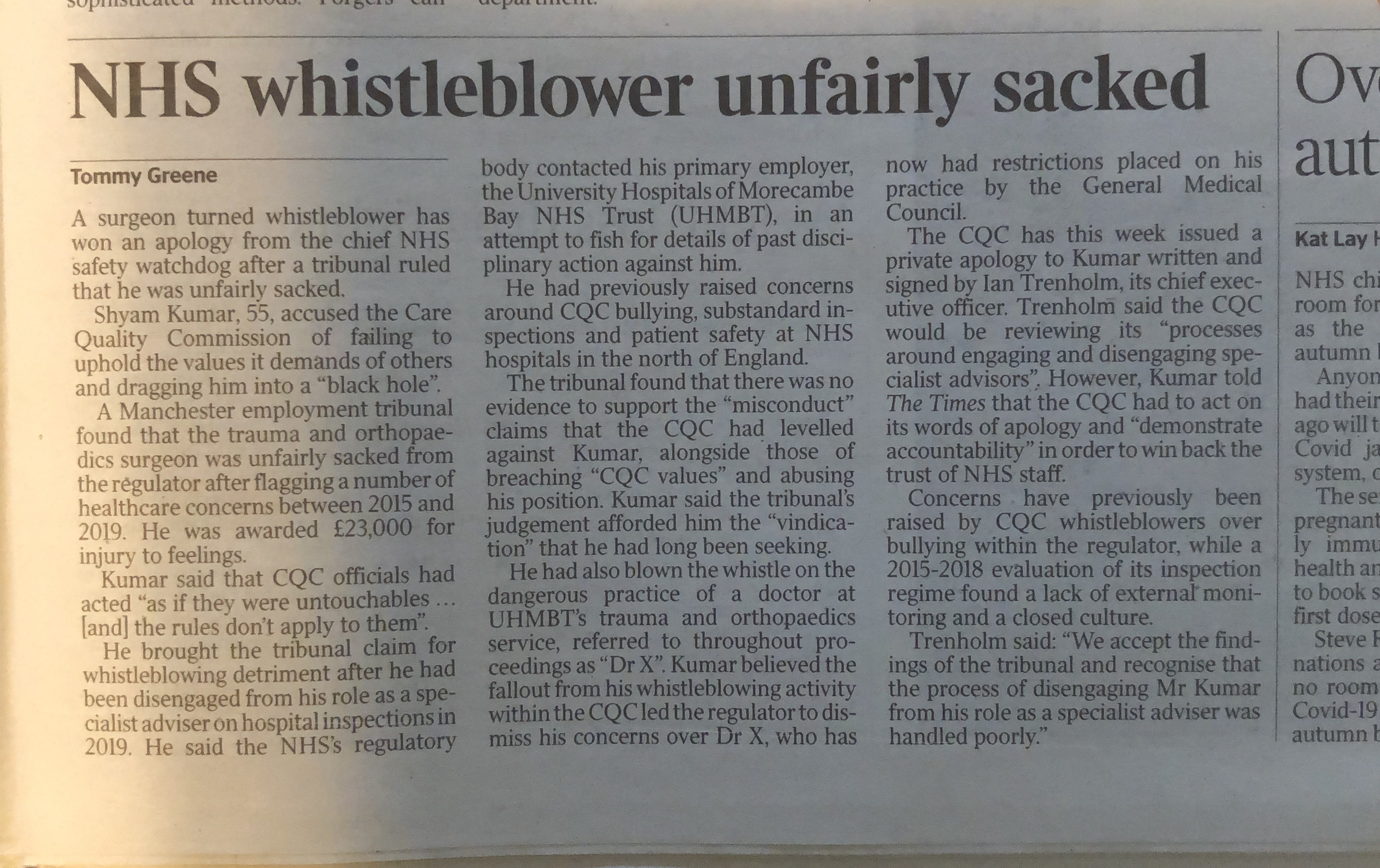
The Care Quality Commission (CQC) is currently under pressure because it has been found by an Employment Tribunal to have seriously victimised one of its own whistleblowers, Mr Shyam Kumar, senior surgeon.
CQC Specialist Advisors (SpAs) are a type of inspector. They are clinicians seconded from provider organisations for their specialist expertise in various areas.
Many clinicians are registered as SpAs.
They work on an ad hoc basis and are retained on a bank.
The CQC handbook for Specialist Advisors explains how CQC handles the SpA role:
Employing SpAs on this limited contract may save the CQC money, but it does add to the concerns about the closeness between CQC and regulated organisations.
Some SpAs maintain strict professionalism. A number of such individuals either leave CQC or whistleblow, or both.
Mr Kumar’s case is of serious political significance, because a regulator should be above reproach.
It is clearly intolerable for an organisation which has a duty to enforce standards to behave so badly, and it is particularly reprehensible that an organisation which judges others’ failures of organisational learning has itself refused to learn.
“CQC’s Executive Team has appointed Zoë Leventhal KC of Matrix Chambers to lead an independent review into our handling of protected disclosures shared by Mr Shyam Kumar alongside a sample of other information of concern shared with us by health and care staff.
The aim of the review will be to determine whether we took appropriate action in response to this information. It will include consideration of whether the ethnicity of the people raising concerns impacted on decision making or outcomes.
The full terms of reference for the review will be published shortly. The review is expected to conclude by the end of this year, with Zoë reporting her findings and recommendations publicly to CQC’s Board.
Alongside this barrister-led review we will conduct a wider review, led by our new Director of Integrated Care, Inequalities and Improvement, Scott Durairaj, which will seek input from people using and working in health and social care and from our colleagues.
This will explore whether there are issues of culture, process or both within the organisation which need to be addressed so we are better able to listen and to act on what we hear when information of concern is shared with us. The review will have a focus on inclusivity, including understanding whether race or any other protected characteristic has any impact on how we treat information of concern. Terms of reference will be developed in consultation with internal and external partners and will be published once agreed.”
Mr Kumar is in fact not alone in his experience as a Specialist Advisor of being marginalised. Other doctors have experienced difficulties in the Specialist Advisor role. An important paper by another surgeon who also worked as a CQC Specialist Advisor, Hugh Cannell, gave a useful insight into working for the CQC:
Mr Cannell set out concerns about whether the CQC values its SpAs, or whether CQC employs them to give surface legitimacy, but does not actually listen to what SpAs have to say:
“The CQC, however, is hardly encouraging or valuing the work of SpAs in the way it should. Ad hoc SpAs too often appear to be regarded by the CQC’s core staff as a distraction from the important work of box ticking. Sometimes SpAs are treated as little more than window dressing.”
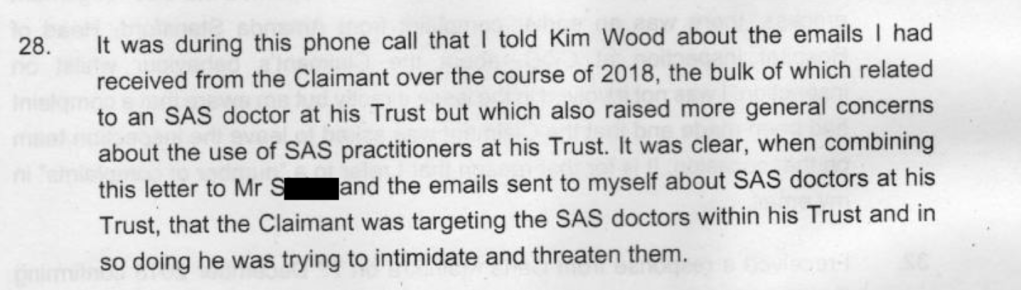
Importantly, Mr Cannell reported that instances of NHS trust staff whistleblowing were not always reflected in CQC inspection reports.
This chimes perfectly with Mr Kumar’s experience of being discouraged by a CQC manager from following up on NHS trust whistleblowers’ concerns, when he participated in a CQC inspection in 2015:
This CQC response contains extracts of a letter from CQC to Matt Hancock Health Secretary in 2019 about Shyam Kumar’s case. This includes an assertion that SpAs are meant to provide expert input “in a broad sense”:
“SpAs provide expert input on the quality of the service from a clinical perspective in a broad sense across the service, as well as on particularly [sic] specialties within the service. There are many different surgical and medical specialties, and it would not be possible or appropriate to bring SpAs to inspect every one of those specialities in detail on inspections.”
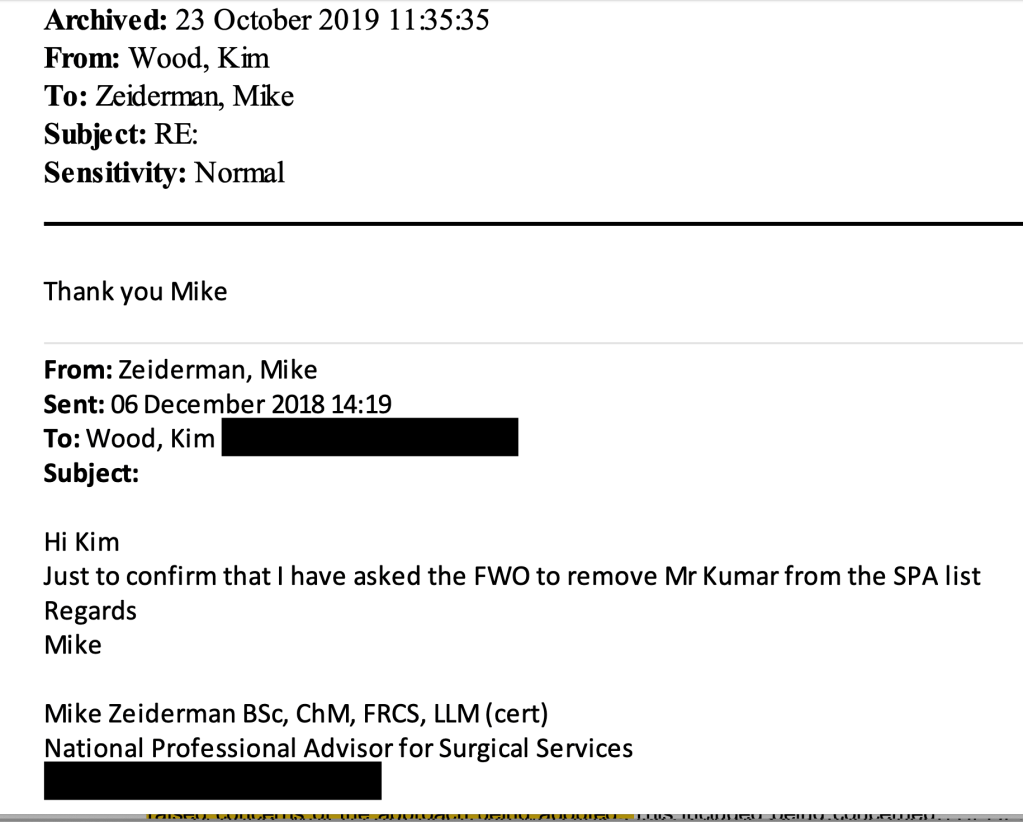
This is at variance to evidence by Mike Zeiderman CQC National Professional Advisor during Mr Kumar’s Employment Tribunal. Mike Zeiderman stated that he agreed with Mr Kumar’s concerns that CQC did not do enough to match Specialist Advisors to the Specialties inspected.
Surely the clue is in the name, “Specialist Advisor”?
As to inclusivity, the CQC has clarified that it does NOT include Specialist Advisors in its regular staff survey:
“Colleagues eligible to participate in our people surveys (also referred to as staff surveys) include permanent staff, fixed term and/or temporary staff, National Professional Advisors and Clinical Fellows. Contractors, bank staff, or SPAs are not eligible to participate.” [My emphasis]
This seems a questionable approach.
I asked CQC to disclose a copy of the feedback form that SpAs fill in after CQC inspections, and for analyses carried out by the CQC of the data gathered.
This is a copy of the online SpA feedback questionnaire:
This questionnaire asks important questions about how CQC inspections are conducted and whether CQC staff demonstrate CQC’s values of Excellence, Caring, Integrity and Teamwork during inspections:
The SpA feedback form implies that somebody in CQC actually reads these feedback forms, because it states:
“If concerns are raised by you the Flexible Workforce Team will contact you to discuss these”.
Even though CQC asks SpAs for this feedback, and it claims that it will respond, when Mr Kumar whistleblew in 2015 to CQC’s Chief Inspector of Hospitals about bullying and suppression during an inspection, he was repeatedly stonewalled by CQC.
Astonishingly, the CQC has claimed that it holds no analysed data from the SpA feedback questionnaires:
“We do not hold any analysis of this data.”
Has CQC never analysed this data?
Is public money spent gathering the data that is not then used?
It is hard to believe that CQC has never analysed the data.
Judging from the SpA feedback questionnaire form disclosed by the CQC, the questionnaire appears to be filled online.
How is it possible that large bank of highly accessible digital data has never been analysed by the CQC?
Or is that CQC has analysed this data, but decided that it was better to keep any analyses under wraps?
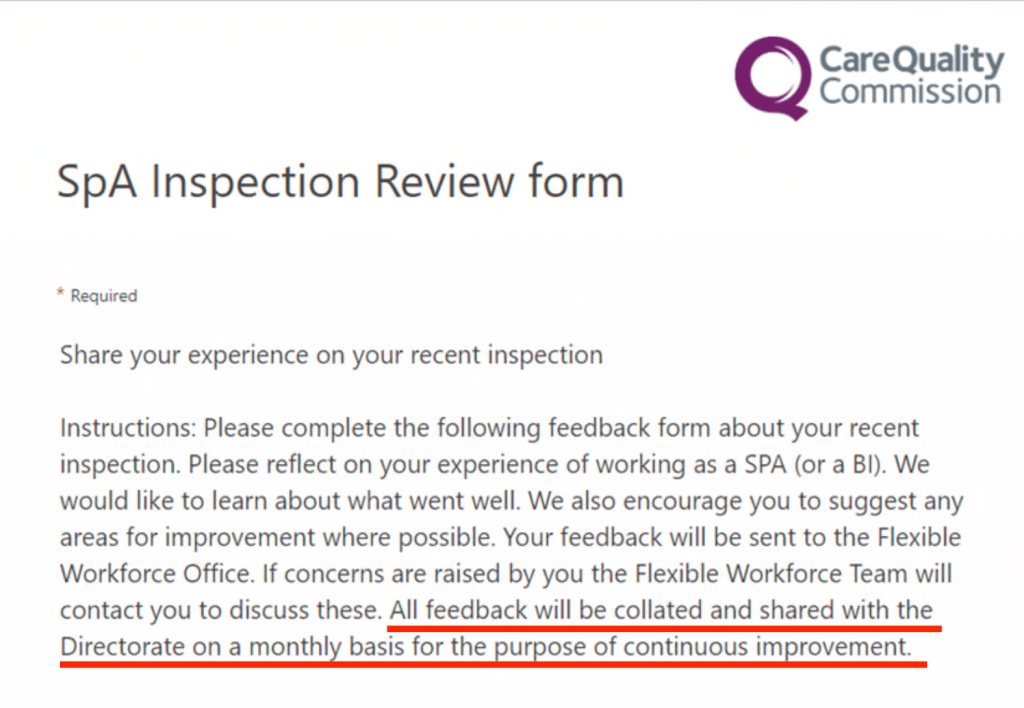
Within the SpA questionnaire form disclosed by the CQC, it actually says that the SpA feedback data is “collated and shared with the Directorate on a monthly basis”:
The options are:
– CQC did not collate data as promised
– CQC collated but shredded the analysed data
– CQC does hold the analysed data, despite its denial
Moreover, where is the employer’s duty of care to CQC’s Specialist Advisors?
CQC should transparently share analysed data with its workforce and provide proof that it is acting on concerns and difficulties.
I asked the CQC how many SpAs have resigned from CQC since 2018.
The regulator replied:
“We do not hold this information centrally and so a manual review of each personal record would be required to ascertain why they exited CQC. Therefore, we are unable to provide you with the requested information as we believe the cost of doing so would exceed the cost limit as defined by s12 of the FOIA.”
This is curious as during Mr Kumar’s Employment Tribunal it became clear that CQC has some form of database on SpAs.
How does CQC manage staffing demand if it holds no central data on leavers and resignations?
The SpA feedback questionnaire in fact includes the questions:
“Would you like to be involved in future inspections? [YES/NO]”
“Please explain why you would not like to be involved in future inspections? [FREE TEXT]
So again, a question arises of whether or not CQC has answered truthfully when it claims that it cannot say how many SpAs have resigned, and that it could only carry out a manual search which would breach FOI cost exemptions.
I have questioned, via Ian Dilks CQC Chair, CQC’s denial that it holds any analysed data on SpA feedback or data on the number of SpAs who have resigned.
LETTER TO IAN DILKS:
BY EMAIL
Ian Dilks, CQC Chair
7 October 2022
Dear Mr Dilks,
Analysis of CQC Specialist Advisor feedback and the number of Specialist Advisors who decide not to take part in further CQC inspections
Thank you for ensuring that there was no excessive further delay in the CQC answering my FOI request for information on CQC’s governance with respect to Specialist Advisors.
I received CQC’s response today – please see the attached.
I originally asked the CQC:
“4) Please disclose any analysis since 1 January 2018 of the routine feedback questionnaires completed by CQC Specialist Advisors after inspections Please disclose a copy of the questionnaire itself”
In its response, the CQC has claimed that it holds no analysed data from the Specialist Advisor feedback questionnaires:
“We do not hold any analysis of this data.”
I have to question whether this CQC claim is a factual inaccuracy.
This is because the feedback questionnaire is an online form and CQC should therefore hold a large amount of accessible digital data, no doubt with analysis in mind.
I also question CQC’s claim that it does not hold analysed data on Specialist Advisors’ feedback questionnaire because the form itself states the questionnaire data is: “collated and shared with the Directorate on a monthly basis”:
In light of this evidence that CQC does collate Specialist Advisors’ feedback data centrally and disseminate it to Directorates, please could CQC provide me with all the collated data reports that it has sent to Directorates on Specialist Advisor questionnaire feedback since 1 January 2018.
Also, I asked CQC:
5) How many Specialist Advisors have resigned from the CQC since 1 January 2018?”
CQC responded:
“We do not hold this information centrally and so a manual review of each personal record would be required to ascertain why they exited CQC. Therefore, we are unable to provide you with the requested information as we believe the cost of doing so would exceed the cost limit as defined by s12 of the FOIA.”
I struggle to see how this can be correct, because the CQC’s online Specialist Advisor feedback questionnaire gathers information about how many Specialist Advisors decide not to take part in future inspections. It asks the question:
“Would you like to be involved in future inspections? [YES/NO]”
To be more precise, can the CQC say on how many occasions have Specialist Advisors ticked the ‘NO’ box since 1 January 2018?
Many thanks,
Minh
Dr Minh Alexander
PETITION
Please click and add your signature to this petition to reform UK whistleblowing law – whistleblowers protect us all but weak UK law leaves them wholly exposed, lets abusers off the hook and it is a threat to public safety.
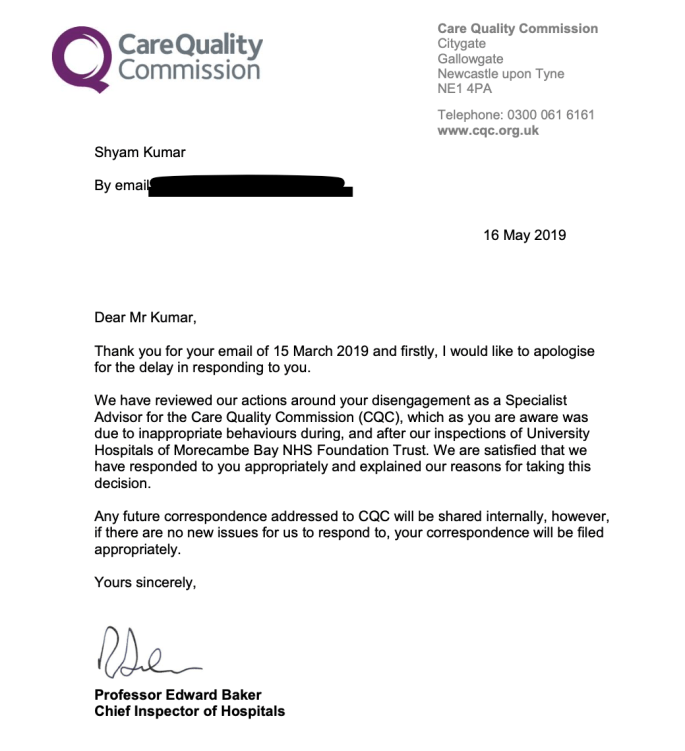
Ted Baker former CQC Chief Inspector of Hospitals failed to protect Mr Kumar as a whistleblower. When Mr Kumar sought help from him regarding his experience of reprisal, Ted Baker maintained the CQC line that Mr Kumar had been sacked for inappropriate behaviour, a position that was later comprehensively rejected by the Employment Tribunal.
Ted Baker retired from the CQC but has recently been appointed Chair of the Healthcare Safety Investigation Branch, a position which one presumes requires sharp analysis and sound judgment.
The CQC’s dreadful history of handling whistleblowing within both its own organisation and provider bodies speaks for itself.
By Dr Minh Alexander retired consultant psychiatrist 26 September 2022
Summary: The Scottish Independent National Whistleblowing Office (INWO) for the Scottish NHS, headed by Rosemary Agnew, has published a first report. The INWO is a better model than the English National Guardian for the English NHS, because it has the investigative powers of an Ombudsman and by policy it can investigate whistleblowers’ concerns and whether they are properly handled. The INWO can also address detriment suffered by individuals. In the English Freedom To Speak Up system, the National Guardian’s Office (NGO) conducts only superficial case reviews and by policy does NOT investigate whistleblowers’ concerns. The NGO has also flatly refused to address detriment to individuals (including legally proven cases) despite this being recommended by the original Freedom To Speak Up review. The Scottish INWO however has no enforcement powers to correct wrongdoing or order redress for whistleblowers. In the INWO’s first report on concerns raised about chaotic COVID contact tracing, she upholds concerns about insufficient training and poorly managed instructions to staff. The INWO concluded that the failings could have resulted in wrong information being given to the public on COVID isolation periods. Disappointingly. there was no finding on whether the contact tracing service did give incorrect advice to the public. Was this side step a political omission? The whistleblower’s concern about detriment was not upheld by the INWO. The justification for this finding was withheld in a private section of the INWO’s report. The reason given for withholding this information was to protect individuals’ privacy, but this has a cost in public confidence and accountability. The INWO should at least track whistleblowers’ satisfaction with its process and transparently publish that outcome. Ultimately, a central whistleblowing agency with protected independence and wider powers is required, along with reform of ineffective UK whistleblowing law.
Background
A key failure of UK whistleblowing law (the Public Interest Disclosure Act) and governance is that no one has the legal duty to actually investigate whistleblowers’ disclosures and correct proven wrongdoing.
The National Freedom To Speak Up Guardian’s Office in the English NHS was designed to be ineffective.
It has no powers, few duties and concentrates its efforts on propaganda. The duties that it does have, it conducts in the most half-hearted way possible. The NGO has carried out few case reviews since inception in 2016 – only nine reviews at the following NHS trusts:
Southport and Ormskirk 2017
Northern Lincolnshire and Goole NHS Foundation Trust 2017
Derbyshire Community Mental Health Services 2018
Nottinghamshire Healthcare NHS Foundation Trust 2018
Royal Cornwall Hospitals NHS Trust 2018
Brighton and Sussex University Hospitals NHS Trust 2019
North West Ambulance Service NHS Trust 2019
Whittington Health NHS Trust 2020
Blackpool Teaching Hospitals NHS Foundation Trust 2021
These reviews are very superficial and by policy they only glance at whistleblowing governance in general.
Most crucially, they NEVER investigate the original concerns raised by whistleblowers.
This is a cynical avoidance, the roots of which lay with the Department of Health (then headed by self-proclaimed patient safety fan Jeremy Hunt) and Robert Francis, in their conduct of the 2015 Freedom To Speak Up Review of whistleblowing in the NHS. The review was very carefully designed to avoid any investigation of whistleblowers’ concerns. And indeed, Francis later confirmed to me that the evidence submitted to his review by hundreds of NHS whistleblowers was destroyed after the conclusion of the review.
In the report of the Freedom To Speak Up Review, Francis left the investigation of NHS whistleblowers’ concerns wholly under the control of employers.
Francis weakly slipped in a rider that employers might wish to consider commissioning external investigations, but that was discretionary. We of course know that he who pays the piper calls the tune. Employers can afford to hire a whole orchestra whereas whistleblowers struggle to afford a tin whistle.
In fairness to Francis, he did stipulate in the report of the Review that the Independent National Officer (the National Guardian in other words) should address and help to ensure redress to whistleblowers and patients harmed by poor whistleblowing governance.
Disgracefully, successive National Guardians have steadfastly refused to do this. The NGO has also erected ridiculous and arbitrary barriers to its services. For example, it tells many whistleblowers that it will not accept their cases until Employment Tribunal processes have ended. This can take years.
In contrast, the Scottish government later created an Office which DID investigate whistleblowers’ concerns. This is the Independent National Whistleblowing Officer (INWO), which is hosted by the Scottish Public Services Ombudsman (SPSO).
The INWO has the statutory powers of the SPSO to investigate and direct disclosure of information. It also sets standards for whistleblowing governance in the Scottish NHS and it operates across the Scottish NHS, whereas the English National Guardian has confined her case review role to NHS provider trusts.
The INWO describes itself as the “final stage of the process for those raising whistleblowing concerns about the NHS in Scotland”.
“We follow up on any recommendations we make and we will require evidence to be provided that the organisation has taken action.”
I cannot see from the relevant legislation – The Public Services Reform (The Scottish Public Services Ombudsman) (Healthcare Whistleblowing) Order 2020 – that any such requirement by the INWO has force. This leaves a large loophole through which neither wrongdoing or harm to whistleblowers is reliably corrected.
And unfortunately, the INWO is only a facility for the NHS (and related contractors), leaving huge swathes of whistleblowing in other sectors unaddressed.
Whistleblower ‘C’ and COVID contact tracing failures
The INWO has recently published a report of its investigation into whistleblowing about a COVID contact tracing service overseen by National Services Scotland (NSS) the national NHS board in Scotland:
The whistleblowing concerns related chiefly to poor administration of the service, with inadequate staff training, poor recording of frequently changing instructions to staff and incorrect calculation of COVID exposure and isolation dates and therefore incorrect advice to the public on isolation.
In context, there were obvious operational pressures as the pandemic surged, which was later acknowledged by the INWO.
NSS initially conducted an investigation and concluded that none of the whistleblower’s concerns was upheld:
“NSS’s position was that none of the issues summarised in paragraph 2 above was substantiated by their own investigation of the concerns raised.”
This denial was contradicted by the fact that NSS still identified learning points and improvement action, implying that it HAD found failures.
The INWO commented:
“I see that, although NSS’s investigation did not uphold C’s concern, it identified learning and improvement actions and made recommendations in relation to training, staff rotation and gathering feedback from staff. This appears contradictory in the way presented and I can understand why C was dissatisfied with NSS’s stage 2 response.”
The INWO concluded after investigation that contact tracing staff training was insufficient and that incorrect advice could have been given to the public:
“My view is that it is more likely than not that these conditions resulted in an increased risk of incorrect information being given to members of the public.”
In my view, there is a pulled punch here – why is there no finding on whether wrong information on COVID isolation periods was actually given to members of the public?
Would that have been a step too far in terms of government liability for such failures?
The INWO’s public report lacks detailed substantiation for some of its conclusions, such as a conclusion that the employer mounted a suitably impartial investigation.
It is possible that private sections of the INWO’s report addressed this. The stated reason for withholding some of the report material was to protect the whistleblower’s identity.
However, there remains a question mark over the INWO’s conclusion that the employer’s investigation was impartial when it failed to uphold any of the whistleblower’s concerns, despite identifying learning points.
The INWO also concluded that there was a “misunderstanding”by the employer in that it wrongly and initially advised the whistleblower that an HR process was more appropriate than the whistleblowing process. Is a “misunderstanding” too kind an interpretation, and should the INWO have simply concluded that the wrong process was chosen, without imparting a mitigating theory for how it happened?
In terms of NSS’ treatment of the whistleblower, the INWO upheld concerns that there was not sufficient care taken to protect the whistleblower’s identity, and that the confidentiality of witnesses was also not protected.
The INWO concluded that there was no detriment beyond the confidentiality issues:
“84. Based on the evidence provided by NSS and interview with C, the head of complaint that NSS failed to protect the whistleblower from detriment associated with speaking up is not upheld.”
There is no public justification for this finding. The INWO’s rationale was withheld for reasons of individuals’ privacy:
“82. The evidence is summarised in private Appendix F. Due to the sensitive nature of the evidence, I have decided that all of the detail must remain confidential, as to disclose it risks identifying C and other staff.”
It may be that some whistleblowers will understandably prefer anonymity. But this approach by the INWO is different to the relative transparency of Employment Tribunal proceedings, where detailed justifications for findings are usually provided in fully published judgments. It is hard to see why the INWO could not at least give summary information on alleged detriments and her broad reasons for upholding them or not.
The cost of anonymity and completely withheld data is less public confidence that justice has been done and that organisations have been duly held accountable for failings.
The INWO could partly mitigate against this by tracking whistleblowers’ satisfaction with its investigations and transparently publishing the outcome.
Whilst the Scottish INWO is a better offering than the cynically pointless English National Guardian, there are still limitations.
In all though, piecemeal sticking plasters like the Scottish INWO and the English National Guardian are not a satisfactory substitute for a proper central whistleblowing agency with a more comprehensive range of powers. UK whistleblowing law needs reform and such an agency needs to created.
Any whistleblowing agency is prone to capture or other erosion, especially if modelled along the lines of US whistleblowing agencies which feature the payment of massive bounties, with lawyers profiting:
A better model is that of the US Office Special Counsel, which protects federal whistleblowers and is designed with greater public service ethos in mind. Its guiding principle is to fairly restore whistleblowers to the position they would have had but for the whistleblowing, and it also has powers to address wrongdoing uncovered by whistleblowers.
What is crucial is that the design of any central whistleblowing body comes with protection of its independence from the government of the day, along with direct reporting to parliament.
None of the Bills laid before parliament to date as alternatives to PIDA have featured this independence.
PETITION
Please click and add your signature to this petition to reform UK whistleblowing law – whistleblowers protect us all but weak UK law leaves them wholly exposed, lets abusers off the hook and it is a threat to public safety.
This is a recent and key case which has revealed both failure and possibly misrepresentation by the National Guardian’s Office, and orchestrated whistleblower reprisal by the National Guardian’s part funder and employer, the Care Quality Commission:
This is another key case, which revealed the fatal weakness of the Freedom To Speak Up project, in its preposterous assertion that employee Guardians can hold erring executives to account.
Other recent examples of NHS whistleblower cases which show serious failure of the Freedom To Speak Up project are those of Jasna Macanovic, renal physician and Jane Archibald, senior specialist nurse. Both these blameless whistleblowers have suffered a years long ordeal. Both suffered failure of the Freedom To Speak Up mechanism at their respective NHS trusts.
Dr Minh Alexander retired consultant psychiatrist 22 September 2022
Summary: The Care Quality Commission has downgraded North Teed and Hartlepool NHS trust which was found by the Employment Tribunal to be responsible for severe whistleblower reprisal against two of its staff, with the Well Led domain now rated “Requires Improvement”. However, this does not change the fact that CQC failed to find any breach of CQC Regulation 5 Fit and Proper Persons (FPPR) in these cases. Nor does it seem likely that it will deter future whistleblower reprisal, as individual and not organisational sanctions are needed. Moreover, the CQC’s inspection report describes cultural issues which would make whistleblowing substantially more difficult at the trust, but CQC did not seem to weigh these factors when assessing the trust’s whistleblowing governance.
I have on several occasions criticised the CQC’s failure to hold any erring NHS senior managers to account under CQC Regulation 5 Fit and Proper Persons (FPPR), even for very serious breaches such as whistleblower reprisal. For example:
CQC has not found any breach of FPPR by North Tees and Hartlepool NHS Trust in response to my referrals on two trust directors criticised by the Employment Tribunal for their actions against trust whistleblowers Linda Fairhall senior nurse and Mr Manuf Kassem, surgeon. The trust managers whom I referred were Lynne Taylor Director of Planning and Performance, now retired, and Dr Deepak Dwarakanath the Medical Director who remains in post.
CQC unusually wrote to me, unprompted, to say that it was inspecting North Tees:
Also, and most unusually, CQC sent me the North Tees 16 September 2022 inspection report:
The inspection report makes some unfavourable observations about North Tees’ senior management; and downgrades the rating on the Well Led domain to “requires improvement”:
“Due to the ratings given at this inspection, the trust’s overall ratings of good across all domains changed to requires improvement in safe, effective and well-led. This meant that the trust’s overall rating changed from good to requires improvement.”
“Our rating of services went down. We rated them as requires improvement because:
• The trust had interim arrangements in place for several key roles, and there was a lack of united leadership and succession planning. Most strategies were in draft, incomplete and not complementary.
• Senior and executive leaders did not always operate effective governance systems to manage risks and issues within the service. Governance arrangements were complex and the board did not always have sufficient oversight and focus on operational risks.
• The trust did not have enough medical and midwifery staff in the areas we inspected to care for patients and keep them safe. Medical staff did not all have regular, up to date appraisals.
• The trust had not engaged with its local community to find out what people wanted and needed. Engagement strategies were not existent, or in development, and had not included consultation with the wider community, equality groups, the public or other local organisations.
• The trust did not always discharge its responsibilities fully under Duty of Candour regulations and did not audit compliance. Complaints were not being handled in line with the trust’s complaints policy”
However, despite two recent Employment Tribunal judgments against the trust for severe whistleblower detriment, the CQC gave only a bureaucratic account of the trust’s whistleblowing governance:
“Staff we spoke to said that they did feel able to speak up and raise concerns, and in midwifery, staff told us they had seen the Freedom to Speak Up Guardian (FTSUG) in their department. The FTSUG reported to the board yearly through an annual report and prepared a monthly report for the executive team. The FTSUG was appointed in August 2021, with an increase in hours to a full time role.
There were also 10 freedom to speak up champions across the trust and NTH Solutions. All could be contacted by email, and the FTSUG could also be contacted by telephone, however the trust’s speak up policy, associated flowchart and poster were confusing and did not clearly state that a member of staff with patient safety concerns could directly contact the FTSUG.
The FTSUG formed part of the formal induction process for new starters and had also attended some volunteer induction sessions. In 2021, the FTSUG had received no cases in quarter one, two in quarter two, 34 in quarter three, and 14 in quarter four. The main themes were around senior management and culture, staffing, patient safety and the working environment. No more detail was presented to board on these themes or any action taken as a result and there was no documentation of any discussion around the sudden increase in Q3.”
Remarkably, CQC sought to portray the trust as victims of publicity following the Employment Tribunal’s findings in favour of whistleblowers:
“The trust had experienced departures of some well-known staff, had been ruled against in two recent employment tribunals with some media interest in these. Leaders spoke about the challenges these had posed, the toll that they had taken on staff, and a wish to ‘move on’ with culture work.”
That is surely a very special way of looking at whistleblower reprisal and accountability.
Also, CQC’s anodyne account of North Tees’ whistleblowing governance seems to be contradicted by its acknowledgment of a “disconnect” between the frontline and the trust board:
“During our inspection front line staff did not describe leaders as visible and approachable and morale was not always positive in the two core services we visited.
There was a clear disconnect and difference in views around the board leadership, with the executive team talking incredibly positively about leadership and the changes they had made for the better. However, others we spoke with did not share this view and were less positive about the direction of leadership, describing challenges and differences of opinion.
Staff working ‘on the ground’ in frontline services did not describe any of these benefits and some told us they didn’t feel senior leaders were visible or approachable.”
How does CQC imagine whistleblowing works if the trust board signals that it does not like bad news, and the frontline don’t feel that the trust board are approachable?
Moreover, CQC ticked its boxes on its inspection of FPPR:
“We found that the Fit and Proper Person Procedure was fit for purpose and the files were predominantly in line with the requirements of the regulation.
There is a requirement for providers to ensure that directors are fit and proper to carry out their role. This included checks on their character, health, qualifications, skills, and experience. During the inspection we carried out checks to determine if the trust was compliant with the requirements of the Fit and Proper Persons Requirement (FPPR) (Regulation 5 of the Health and Social Care Act (Regulated Activities) Regulations 2014).
We reviewed four executive and non-executive director files in total. Our review included checks for the newest executive and non-executive appointments. All files included references and signatures saying copies of original documents such as degree certificates had been seen.
We also looked at the trust’s Fit and Proper Person Procedure and spoke to the company secretary who was responsible for oversight and compliance with the FPPR procedure. We reviewed the six-monthly self-declarations, made by the directors, to confirm that they remained fit and proper and saw that these were consistently completed.”
The issues of malice raised by the two whistleblowing Employment Tribunal judgments against the trust are minimised by CQC’s failure to acknowledge them.
Perhaps CQC believes it has discharged its duty by downgrading the trust’s rating.
But if the managers responsible for whistleblower reprisal experience no personal consequences, what is there to stop them from harming future whistleblowers?
Meanwhile, NHS England’s tortoise-like implementation on the Kark Review recommendations for Fit and Proper Persons in the NHS crawls on.
Please click and add your signature to this petition to reform UK whistleblowing law – whistleblowers protect us all but weak UK law leaves them wholly exposed, lets abusers off the hook and it is a threat to public safety.
Dr Minh Alexander retired consultant psychiatrist 5 September 2022
Summary: The Care Quality Commission’s poor whistleblowing governance has been exposed by the case of Dr Shyam Kumar who was found by an Employment Tribunal to have suffered detriment by the CQC, explicitly linked to Mr Kumar’s whistleblowing.
The case reveals that the CQC:
– Failed to protect a whistleblower – Failed to act on his concerns – Failed to accept that his whistleblowing was valid, minimised his concerns and saw the whistleblowing as a nuisance and a threat – Mistreated the whistleblower seriously and smeared him with a number of unjust and false claims – When challenged by the whistleblower about this poor treatment, the regulator sought to portray him as a difficult and “challenging”, and ridiculed his claim of whistleblower reprisal by the CQC – Tried to dig dirt about the whistleblower to retrospectively manufacture a case justifying its mistreatment, abusing regulatory power in the process – Suggested falsely to the Employment Tribunal that Mr Kumar was attacking non-consultant grade doctors at his trust for financial gain, because he did not want them to do work which reduced the waiting list – Fed false information to the Ombudsman to shut down a legitimate complaint by the whistleblower about his mistreatment by the CQC – Claimed reasons for its treatment of the whistleblower which were not believed and were rejected by the ET, calling into questions the truthfulness of the claims – Operated oppressive HR policy and practice, but foolishly and incompetently maintained up to the last minute that its processes were fine.
Introduction
The Health and Social Care regulator the Care Quality Commission has lost an important whistleblowing Employment Tribunal case against surgeon and NHS whistleblower Mr Shyam Kumar.
This important case reveals failures by the regulator on several levels, some of which arguably amounts to serious misconduct by CQC personnel.
The regulator is supposed to protect whistleblowers and ensure good whistleblowing governance by regulated bodies.
Moreover, the CQC is legally a Prescribed Person, which means that it is supposed to be a safe haven body, to which Health and Social Care whistleblowers can make protected disclosures.
But CQC has been found by the ET to have unfairly dismissed and seriously harmed a whistleblower.
And the reason for this current failure is the same as the previous failure: CQC reacted badly to concerns about its poor regulatory performance.
CQC has clearly learnt little.
This matter raises serious questions about the honesty and probity of the regulator, which holds the welfare of so many patients and service users in its hands.
Mr Kumar’s role as a CQC Specialist Advisor
Mr Kumar is an experienced orthopaedic surgeon of unblemished record.
He has experience of assisting whistleblowers through a previous role as an active member of BAPIO. He has also has a legal qualification.
He was of good standing and hired by the Care Quality Commission as a Specialist Advisor in July 2014, on the basis of a secondment contract.
By 2015, he was in bad odour with the CQC’s senior managers, because he whistleblew to them about poor management of a CQC inspection and an experience of being bullied by the CQC inspection lead, who prevented him from talking to NHS trust whistleblowers during the inspection:
One of the concerns raised in this letter is of collusion by the CQC:
“There appears to remain a culture within the CQC, which results in some medical directors and chief executives being let off lightly when whistleblowers have raised concerns.
Mr Kumar is not aware that his concerns were ever investigated, despite a reminder. Neither has the CQC produced any records to prove that it investigated his concern.
Whistleblowing to the CQC in 2018
By June 2018 Mr Kumar had cause to whistleblow again to CQC managers, over two areas of concern:
1. CQC’s flawed inspection methodology which included using Specialist Advisors in inspections for which they were not expert. Mr Kumar’s concerns arose from a chaotic CQC inspection of East Lancashire Hospitals NHS Trust.
2. Issues about very serious patient safety at his own trust, University Hospitals Morecambe Bay NHS Foundation Trust.
These patient safety issues revolved around the poorly supervised orthopaedic practice of a Dr X, about which a number of consultants raised concerns. These safety concerns have been validated by two external investigations. The GMC imposed restrictions on dr X’s practice in 2018, as a result of whistleblowing by Mr Kumar and other colleagues.
As well as the patient safety concerns, Mr Kumar also raised concerns with the CQC about the governance at his trust, failure by the trust to act effectively on the patient safety issues and the fact that he had not been protected from severe whistleblowing reprisal.
The whistleblower reprisal included serious false allegations against him, including in group emails involving his peers. In one email Mr Kumar was dubbed a “traitor”.
“80. On 30 October 2018, Mr S [REDACTED], in an email to a broad recipient list, described individuals who were involved in activities against doctors of Indian origin as being ‘traitors of their community’ (p.393). Given that the claimant had raised complaints about the Dr X’s practice, and the close nexus in time that this comment is made to those complaints, on balance it is likely that this comment is about the claimant.”
Mr Kumar also raised concerns with the CQC about white consultants feeling intimidated to to raise patient safety concerns in case they would be subject to counter-allegations of racism
Mr Kumar’s concerns about the above governance failure at UHMBT have been vindicated by both external and internal investigations.
His disclosures to CQC were made primarily to the CQC National Professional Advisor, Mike Zeiderman, colorectal surgeon based at Southport and Ormskirk.
This is list of Mr Kumar’s disclosures that the ET ruled met the legal threshold of protected disclosures:
Instead of recognising the seriousness and validity of Mr Kumar’s concerns, it appears that the CQC regarded Mr Kumar’s disclosures as a nuisance and a threat.
The ET considered that correspondence by Mike Zeiderman made it clear that a decision in December 2018 to sack Mr Kumar as a Specialist Advisor was explicitly linked to Mr Kumar’s disclosures to Mike Zeiderman.
These are examples of Mr Kumar’s disclosures:
The ET summarised another disclosure by Mr Kumar as follows:
“On 29 June 2018, following up his email of 16 June 2018, the claimant called Mr Zeiderman. During this phone call, the claimant reiterated concerns that matters had been raised with the Trust’s Medical Director, but that the Trust was refusing to look into those concerns but was wanting to cover up the issues. The claimant also raised specific examples of to suspicious deaths, after which the Trust had not taken steps to prevent further harm. The claimant provided specific details of the two cases to Mr Zeiderman in this phone call. The claimant was disclosing information of serious and/or potential harm to patients. Mr Zeiderman accepted the claimant’s paragraph 38 as being the content of that phone call.”
This is Mr Kumar’s account of another disclosure to Mike Zeiderman:
The most threatening of these disclosures from CQC’s point of view would have been the email of 8 September 2018, in which Mr Kumar made serious criticisms of CQC’s unsafe inspection methodology at East Lancashire.
The CQC later accepted that some of Mr Kumar’s communications were protected whistleblowing disclosures, but the regulator and Prescribed Person contested five significant disclosures (disclosures 2,3,4,8,10) right up to the point when the Employment Tribunal ruled that they were bona fide whistleblowing.
The ET judgment reveals that a witness statement by the local CQC inspector Kim Wood had a denigratory tone in that it referred to Mr Kumar’s valid disclosures as “persistent”:
“Ms Wood compounds this at paragraph 33 of her witness evidence, where she explains whilst discussing the decision to disengage and the letter to Mr S [REDACTED] that ‘This was particularly so against the background of the persistent emails to Mike about the use of SAS doctors and patients concerns…’ Ms Wood again refers to emails as part of the decision making process. These emails are protected disclosures 2-10.” [my emphasis]
In one email thread, Kim Wood dismissed correspondence from Mr Kumar as “largely irrelevant”.
The ET later concluded that this correspondence by Mr Kumar, which Wood had so casually dismissed, was NOT irrelevant but were protected disclosures:
“The emails forwarded by Ms Wood were relevant and played a central role in this decision to disengage the claimant from his role with the respondent. The emails contained in this email were:
a. The 08 September 2018 email from the claimant to Mr Zeiderman (Protected Disclosure 7)
b. The 17 September 2018 email from the claimant to Mr Zeiderman (Protected Disclosure 8)
c. The letter of 29 November 2018 (wrongly dated as August) that Mr S [REDACTED] had sent to Ms Wood.”
The dismissive and disrespectful attitude is echoed in later emails by Louise Mallaburn CQC Senior HR Advisor who wrote that Mr Kumar was “very challenging” and in another email made a sarcastic comment about him writing long emails.
The unfair dismissal by CQC
In November 2018 a CQC inspection took place at UHMBT, Mr Kumar’s trust.
Mr Kumar wrote to Kim Wood CQC inspector to express concerns that one of his persecutors at the trust, Dr S, might make inappropriate and damaging comments about him during the inspection.
This proved to be a realistic fear as Dr S did indeed make false and highly damaging claims about Mr Kumar during a CQC focus group.
The ET noted that Dr S’s remarks were inappropriate in that forum:
“In this meeting, Mr S [REDACTED] raised a number of issues which the Investigating Manager, Ms Helen Vine, considered were not appropriate for the Focus Group.”
The ET found that Mr Kumar was entitled to feel upset and injured by the serious attack on his character, probity and standing:
“The matters raised by the claimant, in his letter to Mr S [REDACTED], were serious issues. The claimant, if these matters were true, had the right to feel upset, in particular with the matters that were probity matters or race. All involved in this case accept that allegations concerning probity, bias and racism are serious matters and could have impacted on the claimant’s fitness to practise.”
Extraordinarily though. Kim Wood later wrote to Mike Zeiderman on 6 May 2019, when they were deciding how to respond to a request for information by the CQC Chair’s office, that Dr S had not said “anything untoward”.
On the same day, Mike Zeiderman’s drafted a response to the CQC Chair, which cast Mr Kumar as the problem and undermined his credibility as a whistleblower:
This dismissal of Mr Kumar’s experience of whistleblowing reprisal contrasted with the CQC’s over reaction to counter-claims by Dr S.
After the above CQC focus group, Mr Kumar wrote a letter to Dr S with advice from the BMA, setting out his concerns about Dr S’s conduct. He proposed steps for resolution. The ET accepted that this was a good faith attempt to resolve the matter
“The letter sent by the claimant to Mr S [REDACTED] was an attempt to resolve matters informally, before making any decision as to whether to pursue a formal process. This is in line with the policies and procedures adopted by both the respondent and the employing Trust. We accept the claimant’s evidence on this, which is consistent with the wording in the letter that he sent to Mr S [REDACTED], in which he is seeking to resolve the situation. This is also consistent with the approach the claimant took after this letter was sent.”
However, the CQC seized on the fact that Mr Kumar had written a letter to Dr S as a means of dismissing him.
This is correspondence in which Mike Zeiderman instructed HR to sack Mr Kumar and informed Kim Wood of the sacking:
CQC’s line of attack thereafter focussed on a vague claim that Mr Kumar’s letter to Dr S proposing a resolution was in fact improper and a breach of CQC’s values.
CQC maintained this line of attack throughout the ET proceedings. During the June ET hearing, which I attended via web link, CQC’s witnesses made much of Dr S’ alleged response to Mr Kumar’s letter. The CQC contended that the definition of bullying includes the “victim’s” experience and it claimed that Dr S was so distressed by Dr K’s letter that the letter should be viewed as bullying.
The ET did not accept this.
In his evidence to the Employment Tribunal, Mike Zeiderman said that he had seen the letter from Mr Kumar to Dr S, before sacking him.
Damningly, the ET did not believe this:
“102. On balance we find that before 06 December 2018, Mr Zeiderman had not seen the letter that the claimant had sent to Mr S [REDACTED]. Although Mr Zeiderman in his oral evidence said he had seen the letter, the evidence before the tribunal suggests on balance that he did not see it by this date.“
That is, the central reason claimed by the CQC for dismissing Mr Kumar – his letter to Dr S – had not even been examined by Zeiderman at the point of the decision to dismiss Mr Kumar.
The ET determined that CQC’s dismissal of Mr Kumar was a “forgone conclusion” and therefore unfair.
“Disengaging the claimant was a foregone conclusion at the point the claimant was informed that he was placed on hold, and in those circumstances it is not plausible that it is a neutral act.”
The ET considered that Mr Kumar had been sacked by the CQC because he had whistleblown:
145. Given our findings above, it is very clear that the emails and concerns raised by the claimant in the form of protected disclosures had a material influence on the decision to disengage him. Amongst other reasons, this is particularly because of:
a. The reasons provided by Mr Zeiderman for disengaging the claimant appeared to develop throughout the period between the decision to disengage him on 06 December 2018 and his correspondence Mr Matt Wood from the Private Office Correspondence Unit, and into these proceedings. This and the lack of reference to the alleged offending letter to Mr S [REDACTED] a form the claimant, casts great doubt on that being the reason for disengagement and placing on hold of the claimant.
b. The correspondence with the claimant disengaging him provides little in terms of explaining in what way his behaviour fell below the expected behaviours or values of the respondent. And there was no detail as to what in the letter from the claimant to Mr S REDACTED] offended those principles. This again casts doubt on this being the sole reason, with other matters being trivial in the decision making process, for the decisions made.
c. During the phone call between Mr Zeiderman and Ms Wood in early December 2018, when Mr Zeiderman formed the view that the claimant could no longer be used as a special advisor, the claimant had at the forefront of his mind the emails which he had received from the claimant over the course of 2018. The emails that he is referring to include a number that are protected disclosures, or more specifically Protected Disclosures 2-10.”
The Tribunal determined that the CQC made no proper and reasonable investigation prior to dismissing Mr Kumar and that it failed to protect him as a whistleblower:
“Alongside this, this tribunal is mindful that this is a case where the claimant was being disengaged for having conducted himself in a manner not befitting of the respondent, without any proper and reasonable investigation. Where his professionalism was being questioned, and his action, which was later used as the reason for disengagement was in response to that. Where he had made the decision-makers aware of potential retaliatory action against him, and no safeguards were put in place. Against this backdrop, the decision to disengage him clearly reaches the level of detriment.”
CQC dismissed Mr Kumar without an appeal process, claiming that its policies allowed it to sack him without appeal, and that this was CQC’s normal practice.
The ET considered that this was unreasonable employer behaviour, and a detriment.
Thus it follows that the CQC is operating an oppressive employment practice, which takes no heed of natural justice.
CQC dug for dirt
One of the most extraordinary aspects of this case is that CQC sought to retrospectively justify its arbitrary and unfair treatment of Mr Kumar by placing pressure on his employer (University Hospitals Morecambe Bay NHS Foundation Trust, UHMBT) to give it dirt on Mr Kumar.
After Mr Kumar filed an ET claim against CQC for whistleblower detriment, the CQC asked UHMBT for information about UHMBT’s disciplinary action against Mr Kumar for his letter to Dr S, when no such disciplinary action ever took place.
The Victoria Head copied into this email is a CQC Inspection Manager, working on CQC’s Maternity Inspection Programme
A month later, Kim Wood pursued UHMBT staff for “past issues” about Mr Kumar that could be useful to CQC’s lawyers:
In fact, the ET noted that Dr S, for all the CQC’s protestations of injury on his behalf, never even filed a grievance against Mr Kumar.
The fact that the regulator would ask a regulated body for information that was outwith the regulatory process, and was in fact requested for self-serving reasons, seems a most serious matter.
Especially when that purpose is to retrospectively justify the regulator’s poor treatment of a whistleblower.
This seems to me to be a gross abuse of power.
It would be for a lawyer to opine on whether it amounts to Misconduct In Public Office.
The CQC makes false counter-allegations against whistleblowers
As part of its defence strategy against Mr Kumar’s claim to the Employment Tribunal, the CQC sought to portray his whistleblowing about the unsafe practice of a single doctor as an attack on all the SAS (non-consultant grade) doctors at his trust, for potential financial gain.
Mike Zeiderman’s witness statement to the Tribunal repeatedly claimed that Mr Kumar was “targeting” SAS doctors because some were allowed to work autonomously.
Zeiderman accused Mr Kumar of abusing his position as a CQC Specialist Advisor to intimidate others. Almost no particularisation was given of this alleged intimidation or the basis of the accusation.
Zeiderman’s witness statement claimed that a motive for attacking SAS doctors might be that their work to reduce waiting lists affected on the private income of consultant surgeons, as waiting lists encouraged patients to seek private treatment.
There was no basis for this suggestion that Mr Kumar might benefit financially. Dr X was helping to reduce trust waiting lists for LOWER limb cases such as hip and knee replacements. Mr Kumar is an UPPER limb surgeon.
But such a serious allegation about a doctor’s probity would normally require a fellow doctor to refer the individual to General Medical Council, as part of their professional obligations to safeguard patients. The CQC did NOT refer Mr Kumar to the GMC, despite Zeiderman stating clearly in his witness statement that CQC sacked Mr Kumar for reasons of probity:
Moreover, Louise Mallaburn repeated untrue claims about Mr Kumar in correspondence, which were very harmful to his reputation. The false claims are highlighted below:
This is correspondence from Mr Kumar’s trust, UHMBT, which confirmed that there had never been any such record of bullying and harassment on his file:
The false allegation by Louise Mallaburn in her email of 8 January 2019 that Mr Kumar was not often used by the CQC because he had previously been found to be “unsuitable”, was later echoed in Mike Zeiderman’s witness statement of 30 October 2020. In this statement, Zeiderman claims Mr Kumar was asked to leave a CQC inspection [in 2015]. This was false because it was Mr Kumar who made a complaint about Amanda Stanford’s conduct,, AFTER the end of the 2015 inspection.
The CQC doesn’t act on whistleblowers’ concerns
Mr Kumar has never received a satisfactory response from the CQC regarding the whistleblowing concerns that he raised with Mike Zeiderman and subsequently with other senior CQC managers.
This is an email of 16 May 2019 by Mr Kumar to the CQC noting this failure:
Months later a letter by the CQC Chief Executive to the Secretary of State in August 2019 conceded that the CQC had yet to address all of Mr Kumar’s concerns:
“I will ensure that where any of Mr Kumar’s concerns remain outstanding we address those as soon as possible.”
The CQC does not apologise or back down
More serious than an original failure are failures to learn and to take responsibility.
CQC directors rejected Mr Kumar’s complaint about his mistreatment. They stood by their man, Mike Zeiderman.
The final letter from CQC, sent by Ted Baker Chief Inspector of Hospitals, dismissing Mr Kumar’s complaint is painful to read:
By August 2019, CQC PR staff conferred on what “line” to take in explaining CQC’s conduct to Matt Hancock, then Health Secretary:
The CQC informed the Health Secretary that Mr Kumar had been dismissed because of poor behaviour. The regulator through its Chief Executive Ian Trenholm confirmed Mr Kumar had been expected to inspect areas where he was not expert, but it denied that there was anything wrong with its inspection methodology. This was despite CQC’s own National Professional Advisor Mike Zeiderman stating in his ET witness statement that he agreed with Mr Kumar that Specialist Advisors should not be asked to inspect areas in which they were not expert, and that this was an acknowledged problem nationally on which the CQC had been working.
Mr Kumar complained to the PHSO about his treatment by the CQC: The CQC fed false information to the PHSO about Mr Kumar being on a zero hours contract.
Mr Kumar was in fact on a secondment contract, as determined by the ET.
Failed to accept that his whistleblowing was valid, minimised his concerns and saw the whistleblowing as a nuisance and a threat
Mistreated the whistleblower seriously and smeared him
When challenged by the whistleblower sought to portray him as a difficult and “challenging”, and ridiculed his claim of whistleblower reprisal by the CQC
Tried to dig dirt about the whistleblower to retrospectively manufacture a case justifying its mistreatment, abusing regulatory power in the process
Fed false information to the Ombudsman to shut down a legitimate complaint by the whistleblower about his mistreatment by the CQC
Claimed reasons for its treatment of the whistleblower which were not believed and were rejected by the ET, calling into questions the truthfulness of the claims
Operated oppressive HR policy and practice, but foolishly and incompetently maintained up to the last minute that its processes were fine.
I asked the CQC press office to comment on whether it believes it has anything to learn from Mr Kumar’s case, and whether the CQC personnel involved in these serious governance failures should continue in CQC’s employ and hold responsibility for vulnerable patients and service users. I received no reply. I then asked the new CQC Chair Ian Dilks to comment, and have not so far received a reply.
One also has to wonder, if the CQC as an organisation would have been quite so blind to Mr Kumar’s professional credentials and standing, and his professionalism in standing up for patients, or treated him so contemptuously, had he been a Caucasian doctor.
Although the CQC vilified him and caused Mr Kumar and his family so much hurt, it seems clear that he has done all whistleblowers, especially Health and Social Care whistleblowers, and the public a great service.
Will anyone be disciplined or sacked for the harm to Mr Kumar as a whistleblower and the harm to the public interest?
Mr Kumar and his BMA representative asked the then NHS National Freedom To Speak Up Guardian Henrietta Hughes to review the issues raised by his case, but no case review has ever materialised.
But then, why would the National Guardian seek to challenge her employer, the CQC?
That would take the courage of a whistleblower.
I have asked Steve Barclay the Health Secretary to protect Mr Kumar and his family from further trauma and to prevent a wasteful appeal against the ET judgment by the Care Quality Commission, an arms length body of the Department of Health and Social Care.
Appendix: CQC dramatis personae
These are individuals at the CQC who either took an active part in handling Mr Kumar’s case or were party to the case from being copied into correspondence.
This is press coverage from July 2022 of Mr Kumar’s evidence to the ET about bullying culture at the CQC, and his complaint about Amanda Stanford’s conduct:
In keeping with the grand traditions of the NHS, Amanda Stanford’s Airedale NHS Foundation Trust biographical profile states:
“Amanda has an active interest in developing compassionate leadership, quality improvement and how education and training and creating a just and learning culture.”
I have written to Steve Barclay Health Secretary to ask that he ensures Mr Kumar’s concerns about the CQC are properly addressed, and that he ensures that the CQC will not appeal against the ET judgment and inflict further suffering on Mr Kumar and his family.
I have written to the BEIS Secretary about serious failure of the ramshackle system of “Prescribed Persons” under flawed UK whistleblowing law, arising from Mr Kumar’s case and others. Prescribed Persons such as the CQC have minimal legal duties and are too often complicit or directly responsible for harm to whistleblowers.
This means that large swathes of the NHS workforce will be apprised of the regulatory failure and forewarned about CQC’s unreliability as a Prescribed Person.
In the current political and regulatory landscape, I advise whistleblowers to consider whistleblowing directly to the media, either on an anonymous basis or with protection of identity. Take careful advise before doing so, as there are legal tests to fulfil if you wish to maintain protected status under current UK whistleblowing law.
UPDATE 9 SEPTEMBER 2022
CQC has responded briefly only to the media breaking the scandal of Mr Kumar’s case. It claimed in correspondence and through a media statement that it had already learned lessons and made improvements. However, it provided little evidence of these claimed improvements.
Today, it responded to an enquiry that I made about learning lessons and whether those implicated in Mr Kumar’s whistleblower victimisation should remain in the CQC’s employ, and in positions of public trust.
The CQC response today was brief and minimal but of note, referred in the future tense to learning lessons from Mr Kumar’s case:
“We accept the findings of the Employment Tribunal and will consider lessons to be learned from the judgement.” (my emphasis)
UPDATE 13 SEPTEMBER 2022
On 12 September 2022 the Health Service Journal provided further coverage of Mr Kumar’s case, in which it highlighted the Employment Tribunal’s findings on evidence by Mike Zeiderman, CQC National Professional Advisor:
“The unimpressed tribunal judge, meanwhile, said Mr Zeiderman’s explanation for terminating the contract “appeared to develop” in the months after his decision “and into these proceedings”.
HSJ also drew attention to the fact that the ET revealed Mr Kumar’s trust had “hidden” evidence of serious patient harm:
Ian Trenholm CQC CEO: “Thanks very much Ian, this I think Jade is referring to the recent case involving Mr Kumar. Just for clarity we’re not appealing that judgment and I have no intention of doing that. I think it is worth saying we have very few Employment Tribunal cases. In the round, we have a handful at any one time and very few of them actually proceed to a Tribunal. I think it would be difficult for us to make a blanket statement that we were never going to appeal an ET but but U think it is something that would be really very much by exception. So I think it is something we take very seriously. Thank you for the question Jade. Thank you.”
Ian Dilks CQC Chair: “[Inaudible first few words]….it links to the public purse that is something we have to take account of. That means we have to look into each case on its merits rather than making blanket statements about what we would do.”
PETITION
Please click and add your signature to this petition to reform UK whistleblowing law – whistleblowers protect us all but weak UK law leaves them wholly exposed, lets abusers off the hook and it is a threat to public safety.
This is not the first time by far that seconded CQC Specialist Advisors have criticised CQC’s poor inspection methodology and chaotic approach.
I know of doctors who tried the role but resigned due to the problems described by Mr Kumar in his disclosures to the CQC.
Hugh Cannell a former CQC specialist advisor committed his experiences and concerns to paper, in this article of 2019, thus contemporaneous with Mr Kumar’s struggles with the CQC:
Dr Minh Alexander retired consultant psychiatrist 2 September 2022
An Employment Tribunal found on 15 August 2022 that Dr Al-Jehani was unfairly dismissed and subject to a number of detriments by the Royal Free NHS Foundation Trust because she had made protected disclosures in the public interest:
The story is complex and I am unable to do it justice at present, but am briefly posting to share the ET outcome as it appears to be a very serious matter of NHS probity.
Dr Al-Jehani was employed as biomedical scientist by the Royal Free, with an honorary contract with University College London (UCL). She worked for the trust, but was based at UCL’s Institute for Liver and Digestive Health.
She became concerned that human tissue was being diverted into for-profit activities by fellow researchers at UCL, some of whom she alleged had conflicts of interest and held shares in the commercial venture which she believed were benefiting from this diversion of human tissue.
The company named in the ET judgment as the focus of Dr Al-Jehani’s concerns was Engitix, which is listed at Companies House:
Extraordinarily, UCL conducted three separate strands of investigation in response to her concerns – research misconduct, poor human resources practice and financial impropriety – but with a plan agreed with the Royal Free to withhold the fact that the UCL investigations were completed, and their findings, from Dr Al-Jehani.
In the meantime, the Royal Free moved to dismiss her through redundancy. The trust’s managers left a trail of correspondence which showed that they wished to remove her as soon as possible, as they considered her a “thorn in the side”.
The ET concluded that it had no jurisdiction over Dr Al-Jehani’s claims against UCL because the claims were made out of time.
But a very serious question mark clearly hangs over UCL’s part in the matter.
The ET determined that Dr Al-Jehani’s concern that a cover up had taken place was a protected disclosure and that her belief was reasonable in the circumstances.
It also concluded that the Royal Free NHS Foundation Trust’s detrimental actions against Dr Al-Jehani were motivated by self-interest. Namely, a desire to stay on good terms with UCL, and to protect the powerful:
“Furthermore, the fact that the Claimant was kept in the dark about the outcome of UCL’s investigations into her complaints, and that was on specific instructions of RK [Robert Kleta, Director of the Division of Medicine, UCL with clinical appointments as Honorary Consultant in Paediatric Nephrology (Great Ormond Street) and Renal Medicine (Royal Free)](who was meant to be acting as a complainant on behalf of the Claimant, and therefore in her interests), is another important piece in the jigsaw.”
“The picture that emerges shows that the Claimant’s protected disclosures ruffled a few important feathers at UCL, nobody at UCL wanted to deal with the Claimant and wanted her out of sight as soon as possible.”
“The Trust was not going to stick up for the Claimant. Instead, it wanted to solve the problem by finding a way of getting the Claimant out of ILHD [UCL’s Institute for Liver and Digestive Health ]as soon as possible. The paused redundancy process was the most convenient vehicle to achieve that”.
The ET agreed with Dr Al-Jehani’s contention that the redundancy exercise by the trust was a sham:
“The fact that Patricia Blake was first included in the pool, but then removed by DT [Douglas Thorburn] under the pretext that she was included in MP’s [ employment package, with rather dubious evidence in support of that (see pp 1776 and 238), gives us further grounds to infer that the main purpose of the resumed redundancy exercise was to remove the Claimant’s role from ILDH as soon as possible. rather than to achieve financial savings.”
The Employment Tribunal rejected the evidence of several trust managers, which it did not believe.
The Royal Free decided not to call a key witness, Douglas Thorburn (“DT”), Clinical Director for Hepatology and Liver Transplant. He had written an email of 24 July 2019 about dismissing Dr Al-Jehani as follows:
“Hi Robert& Massimo, I’m away at present. I spoke with our ops manager mon evening before I left. Because we had started looking at termination of her role (and one other RFH funded post in ILDH- Sheri-Ann) before she put in her initial complaint we are at liberty to progress the case for redundancy or relocation. (Indeed all her actions have likely been prompted by her recognising her position was at risk…….). The case is in hand and will be submitted for approval shortly (I understand this or next week). Given the problems created it is highly likely/certain it will be approved and the issues will cease. I’m sorry that in the meantime she remains a thorn in the side but I believe this is best just tolerated in the knowledge she will be gone soon. I’ll check in with Lee re anticipated time scales.”
The ET reasoned:
“375. DT writes in that email: “Because we had started looking at termination of her role (and one other RFH funded post in ILDH- Sheri-Ann) before she put in her initial complaint we are at liberty to progress the case for redundancy or relocation. [..] The case is in hand and will be submitted for approval shortly (I understand this or next week). Given the problems created it is highly likely/certain it will be approved and the issues will cease. I’m sorry that in the meantime she remains a thorn in the side but I believe this is best just tolerated in the knowledge she will be gone soon. I’ll check in with Lee re anticipated time scales.” DT could not be any clearer. He wants the Claimant out and because there is that paused redundancy process, which had started before the claimant blew the whistle, the matter can be progressed and the rest will be mere formality.
376. In our judgment, that was effectively the decision to dismiss the Claimant. It was taken by DT. The principal reason for which he took that decision was “the problems created” by the Claimant by making the protected disclosures. The rest was just a matter of executing on the decision. The HR Department was on board with the decision (NW writes in her reply – “We are following the process you have set out in your email.” – p.1877). LG, with assistance from SS, sets the wheels in motion.”
The ET concluded that Douglas Thorburn would have been a damaging witness for the Royal Free, on the following basis:
“Based on our findings of fact (see paragraphs 69-76) we find that the Claimant’s protected disclosures were the main factor in the Trust’s decision to resume the redundancy process. The email from DT [Douglas Thorburn] speaks volumes. The Trust decided not to call DT to give evidence to the Tribunal. NW confirmed in her evidence that DT was still an employee of the Trust. Therefore, the Tribunal draws an inference that DT’s evidence to the Tribunal would have been unhelpful to the Trust’s case, and DT would not have been able to give an alternative reasonable explanation to the apparent meaning of his email. On a fair reading, DT states that the problem of the Claimant being “a thorn in the side” will be solved through redundancy. The redundancy case will almost certainly be approved (given the problems the Claimant had created), and it is just a matter of time to let the process run its course while tolerating the Claimant “in the knowledge she will be gone soon”.
The ET noted that Patricia Rubin claimed that UCL’s investigations were sound, but when questioned by the ET about this, Rubin was unable to give reasons. She also admitted that the appeal panel did not look into a grievance by Dr Al-Jehani (which the ET reported had been sent to the Site Chief Executive Officer Kate Slemeck).
“The letter concluded by saying: “On the matters related to your speaking up concerns, your treatment as outlined in your grievance, the panel is confident that UCL have fulfilled its legal obligations to ensure speaking up concerns and grievances are appropriately investigated in accordance with their own regulatory requirements and internal procedures”.
116. I asked Ms Rubin what gave the panel that confidence. She was not able to provide any satisfactory answer. She was also not able to explain on what basis the panel “noted” that the Claimant did not appeal the speaking up/grievance outcome, when the former waskept secret from her for over a year and UCL’s grievance letter said that she had no right of appeal. It is even more surprising considering Ms Rubin’s admission in cross-examination that the panel did not look into the Claimant’s grievance.”
“…Ms Rubin’s evidence was highly unsatisfactory. While she maintained that the Claimant’s whistleblowing had nothing to do with the panel’s decision to refuse the Claimant’s appeal, she could not properly explain on what basis the panel made its decision (see the Tribunal’s findings of fact at paragraphs 113-116 above).
349. Furthermore, Ms Rubin accepted in her evidence that the panel did not consider any alternatives to the dismissal. She was not even certain whether the appeal had the power to reinstate the Claimant. She could not say what the Claimant could have said or done at the appeal meeting to avoid the dismissal. She later said that the Claimant could have presented new evidence.
350. However, the Claimant did present evidence (not least by telling the panel why she considered her complaints had not been properly dealt with), but the panel chose not to investigate them and instead roundly dismissed them on the basis of the panel being “confident that UCL have fulfilled its legal obligations to ensure speaking up concerns and grievances are appropriately investigated in accordance with their own regulatory requirements and internal procedures”. Ms Rubin was unable to explain on what basis the panel came to that decision”
“312. Looking at the subsequent steps in the process: – SS telling the Claimant that it would be better for her wellbeing to leave ILDH, failure to deal with the Claimant’s February 2020 grievance, and the haste with which the Claimant was eventually dismissed after UCL had sent its letter of 10 June 2020 (and that is despite the 3 months hold on redundancies), we are drawn to the conclusion that the real reason why the Trust had decided to resume the process was to eventually get rid of the Claimant because she had made herself a persona non-grata at ILDH and created unwelcome problems for UCL and the Trust by blowing the whistle on what the Claimant considered to be illegal practices at ILDH.”
The Actions and Omissions of the Royal Free Freedom to Speak Up system
The trust Freedom To Speak Up Guardian Jim Mansfield Unison Staff Side Chair was informed of Dr Al-Jehani’s whistleblowing disclosures in November 2017 and he and the Workforce Director met with her:
“The Claimant’s complaint contained, inter alia, allegations that: (i) tissues samples at TAPb were being used by those who controlled access to it for commercial profit in preference to scientific non-for-profit research, (ii) there was a conflict of interest because AG needed to raise at least £8,000 a month from tissue samples in TAPb to keep his job, (iii) to obtain patients’ consent to donate liver organs GM [Giuseppe Mazza] impersonated a medical doctor, (iv) AG [Amir Gander] attempted to get non-English speaking patients to sign consent forms in English, and (v) donors when signing the consent form did not know that their organs would be used for commercial profit and not for medical research.”
“On 19 January 2018, Natalie Ware (“NW”), Head of Workforce for the Trust’s Hospital Business Unit, and JM met the Claimant to discuss her complaints. NW and JM [Jim Mansfield Speak Up Guardian] asked the Claimant to gather further information on the matters she complained about.”
Dr Al-Jehani provided the Freedom To Speak Up Guardian and the Director of Workforce with information on several occasions.
Natalie Ware discussed Dr Jehani’s case with the trust Chief People Officer and the Chief Medical Officer:
According to the ET, the Freedom To Speak Up Guardian toed the trust management line of not telling Dr Al-Jehani that UCL’s investigations into her concerns had concluded and that her concerns were rejected by UCL.
The ET “preferred” Dr Al-Jehani’s evidence to that of the Freedom To Speak Up Guardian and the Director of Workforce. The ET expressed concern that neither the Freedom To Speak Up Guardian or the Director of Workforce took meeting notes, made records of meetings or sent a follow up email to Dr Al Jehani after meetings.
“On 17 December 2018, the Claimant had a meeting with NW [Natalie Ware] and JM [Jim Mansfield]. They did not tell the Claimant that the investigation had been concluded or what the outcome was. The Claimant remained unaware of that until her redundancy consultation meeting on 10 December 2019. On balance, the Tribunal prefers the Claimant’s evidence on this issue because it is supported by documentary evidence (see pp.1204, 1222 and 1225), which shows that as late as August 2019 the Claimant was operating under a misapprehension that the investigation into her complaints was still ongoing. It is also consistent with NW’s admission that she withheld the outcome report from the Claimant because RK had told her not to share it with the Claimant. It is striking that neither NW (being an HR professional) nor JM (being Speaking-up Guardian) took any notes at the various meetings they had with the Claimant, or made any file notes following the meetings, or sent any follow-up emails to the Claimant recording what had been discussed at the meetings.”
The Tribunal concluded that the Royal Free kept Dr Al-Jehani in ignorance, in concert with UCL, to disadvantage her and suppress her raising of concerns:
“The respondents did not call RK [Robert Kleta] to give evidence to the Tribunal to explain the reasons he told NW not to share the outcome of the investigation with the Claimant. Based on that and the evidence in front of us, the Tribunal draws an inference that RK wished the Claimant to remain unaware of the outcome of the investigation for as long as possible, so that steps could be taken to have the Claimant relocated away from ILDH (see p. 1878) without the Claimant first attempting to appeal the outcome of the investigation or otherwise escalating the matter, or making further complaints against UCL staff. This was discussed and agreed with the Trust (see pp.1877, 1878).”
The finding by the ET that the Royal Free’s Freedom To Speak Up Guardian “did not tell the Claimant that the investigation had been concluded or what the outcome was” illustrates yet again why the government’s Freedom To Speak Up project is fundamentally flawed.
It puts Freedom To Speak Up guardians who are subordinate employees in the impossible position of holding their bosses to account, when in reality this means that they must either risk victimisation for doing so, or they do what they are told, against the public interest.
It is a form of institutionalised bullying.
Dr Al-Jehani’s validated Protected Disclosures
The ET accepted the following as legally protected disclosures by Dr Al-Jehani.
Public Interest Disclosure 1
“209. She relies on various passages in her email in which she complains that her access to liver sample in the TAPb was being obstructed whereas GM [Giuseppe Mazza] and Prof Rombouts [Krista Rombouts Professorial Research Associate, Engitix shareholder] were able to obtain hundreds of whole livers from the TAPb, which then were being used for commercial purposes via Engitix.
210. The Trust does not accept that it was a protected disclosure. It states that the nature of the letter was the Claimant asking various questions (e.g. is it ethical?) rather than disclosing information alleging potential breach of the HTA. It also argues that it was the Claimant’s way of getting access to tissue samples, as the Claimant accepted in cross-examination.
211. We find that, read as a whole, the email does disclose information, as it contains sufficient factual information. The fact that the Claimant then poses various questions regarding the ethics and legality of the practices she complains about does not mean that the factual content of the email is not sufficient. It clearly identifies the facts, which the Claimant claims show inappropriate and potentially illegal behaviour.
212. We are also satisfied that the Claimant had a reasonable belief that the information she was disclosing tended to show a criminal offence, namely the use of human tissue contrary to the HTA and that she reasonably believed the disclosure was in the public interest. In concluding her email, she wrote: “I believe that it is in the interest of the NHS and the general public that the issues I have raised above are addressed immediately by the NHS or other appropriate body”.
213. Therefore, we find that PID 1 was a protected disclosure under s.43A ERA.”
Public Interest Disclosure 29
“222. Still in the same email of 22 November 2017 the Claimant stated that AG [Amir Gander] had tried to get non-English speaking patients to sign donor’s consent form in English and had asked the Claimant to translate it orally to the patients, which the Claimant had declined to do.
223. She claims that the information tended to show a criminal offence by reference to various sections in the HTA, and also a failure to comply with a legal obligation, namely various provisions in the Human Tissue Authority Code of Conduct E – Research (pp 217 – 218 of Appendices to PD table) – (“Code of Conduct E”).
224. The Trust does not admit that it amounted to a protected disclosure but does not make any further submissions.
225. We find that it was a protected disclosure. The relevant passage in the email contains sufficient factual information – GM [Giuseppe Mazza]approaching non-English speaking patients to sign consent forms in English and asking the Claimant to translate for him. The Claimant goes on to say that she told AG [Amir Gander] that to obtain a valid consent the form would need to be translated into Arabic, which AG said it was too complicated. However, the Claimant claims that subsequent to that conversation AG was caught approaching non-English speaking patients in the private wing of the hospital for consent. Therefore, we find that the Claimant reasonably believed that the information she was disclosing tended to show that AG was committing a criminal offence by attempting to obtain patients’ consent in contravention of the HTA. We also find that she reasonably believed the disclosure was in the public interest. Therefore, PID 29 was a protected disclosure.”
Public Interest Disclosure 49
231. The Claimant relies on her email of 12 February 2018 to JM [Jim Mansfield Speak Up Guardian] in which she states that she overheard a telephone conversation in which GM [Giuseppe Mazza] said to the person at the other end of the line (who the Claimant thought was a potential investor into Engitix) that he (GM) was able to source human tissue and that he had a team who were proficient in decellularizing all human tissue. GM also told the “investor” about his plants to travel to Japan and the USA to meet with other investors, and of GM’s plans to set up a human myofibroblast (a type of human cell) biobank.
232. The Claimant says that this communication contained information that tended to show “commercialisation of human tissue” which she says is a criminal offence under the HTA and also a failure to comply with a legal obligation under the Code of Conduct E.
233. The Trust does not admit that the email amounts to a protected disclosure and states that the nature of the content of the communication is the Claimant asking questions and it did not tend to show a criminal offence or a failure to comply with a legal obligation.
234. We find that it was a protected disclosure, when read in the context of the Claimant’s earlier 22 November disclosure. Essentially, the Claimant provides further information in support of her PID 1, which she reasonably believed tended to show that human tissue samples were being used for commercial purposes in breach of the HTA. We also find that she reasonably believed that the disclosure was in the public interest. Therefore, we find PID 49 was a protected disclosure.
Public Interest Disclosure 33
“227. Although listed under 22 November 2017, it appears the Claimant relies on her email of 13 April 2018 and the attachments, in which she alleged that MP [Massimo Pinzani] and GM [Giuseppe Mazza] had obtained ethical approval to use tissue from TAPb for domestic research only, however in their funding application they wrongly asserted that the approval covered commercial use, including abroad through Engitix.
228. She claims that information tended to show a criminal offence under the HTA, and also under s.2 of the FA, and that there was a failure to comply with a legal obligation under various paragraphs of the Code of Conduct E.
229. The Trust does not admit that the disclosure amounted to a protected disclosure and points out that if the alleged breach is of the Code of Conduct, that is insufficient.
230. We find that the communication was a protected disclosure. The Claimant includes the original application for human tissue by GM and MP for the organ regeneration project and the ethics approval letter and provides details, which she says, show that the ethics approval covered only domestic use, whereas the funding application represented that the ethics approval covered a wider use and that was a false representation contrary to the HTA. We also find that the Claimant reasonably believed that the disclosure was in the public interest. Therefore, PID 33 was a protected disclosure.”
Public Interest Disclosure 3
“273. The Claimant relies on her email of 31 May 2018 to JM [Jim Mansfield Speak Up Guardian] and NM [Natalie Ware], in which she wrote about a talk given at the Research and Development Open Day at the Royal Free Hospital. At that talk, AG [Amir Gander] and Dr Emma Lawrence, Engagement Director at UCL, talked about problems researchers face in accessing human tissue samples and how TAPb was facilitating access to samples. The Claimant asked a question about what percentage of donated organs were ended up being used by NHS. Dr Lawrence said that she did not have such information. The Claimant then asked whether they had information on recovery costs for procuring tissue samples. The answer was no. The Claimant then explained the difficulties she had with accessing sample at TAPb, and AG said that it was not the right forum to discuss these issues.
274. The Claimant claims that this email contained information, which in her reasonable belief tended to show that a criminal offence of using/storing donated materials for a non-qualified purpose, namely commercial profit contrary to s.8 HTA.
“281. The Claimant relies on the same email of 31 May 2018, in which she also wrote about her encounter with a PhD student, who she suspected was unwittingly exploited by GM [Giuseppe Mazza] and MP [Massimo Pinzani] for the benefit of Engitix and was not properly supervised. She wrote that she believed that the students were not being given correct guidance and training on ethical use of human tissue, HTA regulations, data protection and other governance and therefore “many of these regulations are being violated”.
282. She claims that in her reasonable belief the information tended to show criminal offences under the HTA and the FA, and a failure to comply with a legal obligation under Code of Conduct – E, the DPA and GDPR.
283. We find it was a protected disclosure. It contains factual information about the Claimant’s conversation with the student from which she discovered that the student was working on a project for Engitix. She makes assertions that the work was not properly supervised, and applicable regulations violated. Although those assertions are not supported by concrete evidence in that email, when read together with her earlier disclosures, in particular 1, 33, 39, 43, 49 and 75, we find that the Claimant did believe that the information provided tended to show likely violations of the relevant laws and regulations and in the circumstances that belief was reasonable. We also find that she reasonably believed that the information disclosed was the public interest. Therefore, it was a protected disclosure.”
Public Interest Disclosure 75
242. The Claimant relies on her email to JM [Jim Mansfield Speak Up Guardian] of 12 March 2018 in which she reported a serious breach of data protection. She wrote that she had discovered that GM [Giuseppe Mazza] had a folder labelled “human liver” which contained highly sensitive information related to NHS patients from whom human liver samples had been obtained and kept in TAPb and that folder was kept on a shelf in a shared office which many UCL staff and students had access to.
243. The Claimant claims that she reasonably believed the information tended to show that a criminal office had been committed under s.170 of the Data Protection Act 2018 (“the DPA”) (unlawful obtaining of personal data without consent) and a failure to comply with legal obligations under the DPA, the General Data Regulations 2016, Code of Conduct E and UCL-RFH BERC Guidelines.
244. The Trust does not admit that it was a protected disclosure but makes no further submissions.
245. We find that it was a protected disclosure. The email contained detailed factual information, the Claimant reported it as a serious data protection breach. We find that she reasonably believed that the information tended to show a failure to comply with a legal obligation under the data protection legislation and possibly a criminal offence. Given the likely number of patients (the data went back to 2014) whose highly sensitive personal data the Claimant thought was at risk, we find that she reasonably believed the disclosure was in the public interest. Therefore, we find PID 75 was a protected disclosure.”
Public Interest Disclosures 81/82
“287. The Claimant relies on paragraphs 282-305 in her 5 February 2020 grievance in which she complains that her complaints were not properly investigated, and the Screening Panel decision was a sham. The Claimant explained that she disagreed with the Panel’s conclusions because these were based on untrue submissions by the Individual Respondents, and because her complaints had been rejected without any proper investigation. She also complained that the Trust had failed to inform her of the outcome of the investigation despite knowing it from late 2018 or early 2019. She said it was a cover up.
288. The Claimant claims that these paragraphs in her grievance contained information, which in her reasonable belief tended to should concealment of criminal offences and failures to comply with legal obligations contained in her earlier disclosures.
289. The Trust does not admit it was a protected disclosure because it says it was “not disclosure of information tending to show…”
290. We find that it was a protected disclosure. The Claimant gives detailed factual information about what happened with her complaints and why she believes these have not been properly dealt with. She explains why she disagrees with the Screening Panel conclusions and why such conclusions could not have been reasonably made on the evidence presented if a due investigation process had been followed. She says that she believes it was a cover up. Her complaints that had been passed to the Screening Panel, as we found, contained protected disclosures falling within s.43B(1)(a) and (b). Therefore, we find that the Claimant did disclose information, which she believed tended to show that the matters she had complained about in protected disclosures had been deliberately concealed. In the circumstances we find that her belief was reasonable and that she reasonably believed that the disclosure of that information was in the public interest. Therefore, we find that PID81/82 was a protected disclosure.”
Some of Dr Dr Al-Jehani’s very serious concerns about wrongdoing did not meet the legal threshold of protected disclosures as they were suspicions which the ET considered did not constitute “reasonable beliefs”, but they are nevertheless sobering reading.
For example:
“On 22 May 2018, the Claimant sent further information to NW and JM, again raising the issues of GM keeping confidential patients’ data in the shared office and also making new allegations of inappropriate use of charity funds by a company called 3P, whose shareholders included GM and MP.”
The ET has taken the unusual step of attaching a list of the disclosures that Dr Al-Jehani relied upon, in Appendix 2 of the ET judgment.
This is the UK law which sets out the way in which use of human tissue is strictly controlled and creates criminal offences for breach of its requirements:
Amir Gander Tissue Access for Patient Benefit (“TAPb”) Manager
And of course, where would we be without the National Guardian’s cheery contributions.
This is the former National Guardian Henrietta Hughes, featured in the Royal Free’s publicity material about Freedom To Speak Up in October 2019:“It’s your time to speak up”
UPDATE 3 SEPTEMBER 2022
I have written to the Health Secretary as follows about this matter and the general failure of the Freedom To Speak Up project:
BY EMAIL
Stephen Barclay
Secretary of State for Health and Social Care
3 September 2022
Dear Mr Barclay,
Serious failure of the NHS Freedom To Speak Up project, related waste and serious allegations about the Royal Free NHS Foundation Trust and the Human Tissue Act
The Freedom To Speak Up project, of installing employee “Guardians” at NHS trusts, with national leadership but not line management, by a National Freedom To Speak Up Guardian office without any powers, has failed.
The creation of this model of whistleblowing governance was expressly to
– prevent serious detriment to whistleblowers and destructive litigation
“Rare” was the goal defined by the report of the Freedom To Speak Up Review by Robert Francis:
“10.6 It will be important that progress is reviewed regularly. Culture change is not a one-off event,but requires constant attention and development. I believe that the widespread introduction ofFreedom to Speak Up Guardians, with a national point of reference created through the new postof the Independent National Officer, is a key component in keeping watch over the way concernsare handled, providing support to those who need it, and ensuring the patient safety issue is alwaysaddressed. The climate that can be generated by these measures will be one in which injustice to whistleblowers should become very rare indeed, but is redressed when it does occur.”
– protect patients from harm due to cover ups.
This has not been achieved. Seriously harmed whistleblowers, failed by the Freedom To Speak Up mechanism, continue to sue the NHS and their cases reveal gross patient safety/ abuse/ rights issues.
“Our analysis suggests that the role’s potential contribution might be understood less as supporting whistleblowers who bear witness to clear-cut wrongdoing, and more as helping those with lower-level worries to construct their concerns and what to do with them.”
In any case, all Freedom To Speak Up Guardians do in most cases is pass on concerns. They are not empowered to act as advocates, and any who do so are themselves harmed.
This is one of the latest examples of the model’s ineffectiveness:
Dr Al-Jehani’s proven case of unfair dismissal for whistleblowing is shocking in all respects, and it reveals that the Royal Free NHS Foundation Trust Freedom To Speak Up Guardian, along with senior trust manages, did not tell her investigations into her disclosures had been completed and had rejected her concerns. The Employment Tribunal concluded that the trust’s withholding of this information was done to disadvantage her, and suppress her raising of concerns.
Yet millions continue to be poured into the Freedom To Speak Up model.
But how can employee Freedom To Speak Up Guardians realistically hold senior trust managers to account or oppose their instructions?
Should the public purse really pay for an ineffective model that is so fundamentally flawed by conflicted interest at the heart of its design?
I would be grateful if you consider these matters and also if you could ensure a proper resolution of Dr Al-Jehani’s concerns about the Royal Free NHS Foundation Trust’s role in alleged breaches of the Human Tissue Act.
Dr Al-Jehani contended that there had been a cover up of her concerns and the Employment Tribunal determined that her belief about this was reasonable in the circumstances.
Yours sincerely,
Dr Minh Alexander
Cc Amanda Pritchard CEO NHS England
UPDATE 7 SEPTEMBER 2022
The Times legal editor picked up this story on 5 September 2022
Please click and add your signature to this petition to reform UK whistleblowing law – whistleblowers protect us all but weak UK law leaves them wholly exposed, lets abusers off the hook and it is a threat to public safety.
Recent examples of NHS whistleblowers who were unprotected and unfairly dismissed despite the introduction of the ineffective Freedom To Speak Up model include Nephrologist Dr Macanovic and Jane Archibald Senior Nurse. Both of these blameless professionals have had to suffer years long ordeals and legal battles that are still not concluded. Both were specifically failed by the Freedom To Speak Up system at their respective NHS trusts: