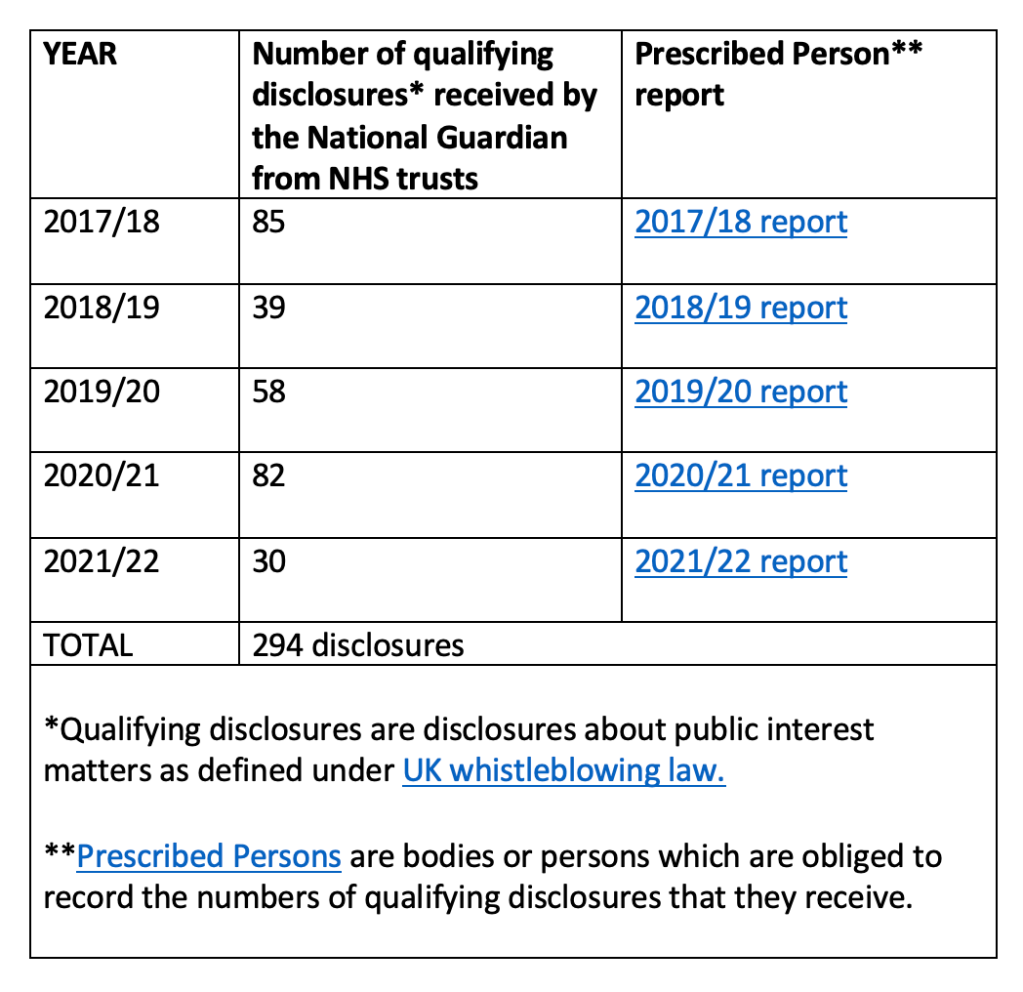
The NGO is not trusted by NHS staff. Few of them whistleblow to the NGO, as evident in the annual statistics of qualifying disclosures received by the NGO from NHS staff.
The National Guardian often tells NHS trust staff to go back to their organisations, which causes great distress to fearful staff, who may already have been victimised:
YEAR
Proportion of staff who made qualifying disclosures whom the NGO signposted to Trust Freedom To Speak Up Guardians
2017/18
No data given
2018/19
43.5 % (17 of 39)
2019/20
39.6 % (23 of 58)
2020/21
34.1 % (28 of 82)
2021/22
43.3 % (13 of 30)
It is unclear how many of the qualifying disclosures that NHS trust staff made to the National Guardian resulted in case reviews by the National Guardian, because the reports are worded in a way that does not clearly give this figure.
But extraordinarily, there is an admission that in 2021/22 the National Guardian stopped even giving advice to NHS staff on how to apply for a National Guardian case review:
YEAR
Number of cases in which the National Guardian’s Office “Initiated a case review, providing information on how a referral for a case review could be made, or explaining the case review process”
[following disclosure by NHS trust staff to the National Guardian]
2017/18
No data given
2018/19
12 (out of 39)
2019/20
24 (out of 58)
2020/21
19 (out of 82)
2021/22
0
What happened in 2021/22?
Was the purportedly independent National Guardian told to resist all requests for case review? If so, why?
Of 85 qualifying disclosures received by the National Guardian in 2017/18, only 17 came from NHS Freedom To Speak Up Guardians.
The fact that so few NHS Trust Freedom to Speak Up Guardians whistleblow to the National Guardian exposes the lie that Guardians employed by NHS trusts are independent.
Also of concern, the FOI response showed that even whistleblowing by NHS trust Freedom To Speak Up Guardians did not result in case reviews:
“The actions taken in response to the 17 qualifying disclosures from Freedom to Speak Up Guardians or their equivalents are detailed further below:
* 14 disclosures led to the office providing information, advice or guidance to a Freedom to Speak up Guardian or equivalent to help them support workers to speak up.
* 3 disclosures led to the office signposting the worker to other sources of advice or guidance, or to an appropriate regulator, authority or body.”
Whistleblowers keep reporting that they are fobbed off by the NGO. Recent examples of this are the cases of Dr Jasna Macanovic and Mr Shyam Kumar, both vindicated whistleblowers.
It is wilfully blind to whistleblowers’ concerns both by design and choice.
Robert Francis recommended that the NGO should have no responsibility for investigating whistleblowers’ concerns, and as a matter of policy, he left control of such investigations to employing NHS trusts.
The NGO collates data from NHS trust Freedom To Speak Up Guardians, but this expressly does NOT include whether whistleblowers’ concerns are safely resolved, despite a past challenge about this omission.
Further evidence has now arisen which again shows that the NGO does not take its responsibilities to whistleblowers seriously.
An FOI request has revealed that the NGO does not apply the same standards to itself as those that it expects of NHS trust Freedom To Speak Up Guardians:
The NGO asks NHS trust Freedom To Speak Up Guardians to submit quarterly data on:
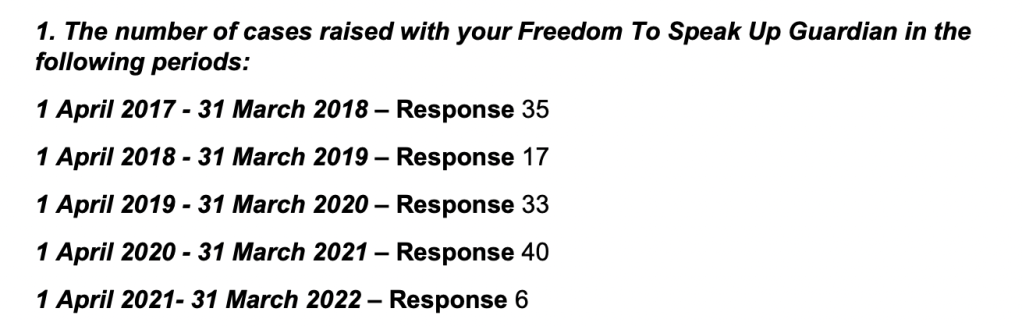
The number of cases raised
Whether the cases are raised anonymously
Whether cases feature an element of patient safety/quality
Number of cases with an element of bullying or harassment
Number of cases with an element of inappropriate attitudes and behaviours
Number of cases in which people report experiencing detriment after speaking up.
The NGO also expects NHS Trust Freedom To Speak Up Guardians to track patterns in cases for learning and to identify systemic issues.
The FOI has revealed that with regard to cases of NHS staff who contact the National Guardian, the National Guardian does NOT collate data on:
Whether the cases feature an element of patient safety
Whether individuals report any detriment after speaking up
This failure to collate crucial information suggests that the National Guardian is not tracking important safety patterns, and that she is not fully sighted on important variations in detriment between NHS trust.
Is that because it would be inconvenient to know which NHS trusts are the most abusive?
The FOI shows that the National Guardian’s central database about NHS staff who contact her Office focusses on administrative process and it features the following items:
Name of person Organisation Position/Type of contact (FTSUG, worker etc) Date in 20 working day response date Date responded Responsibility Same day 2-5 days 6-10 days 11-20 days Overdue Action taken
In my opinion, this suggests a tick box attitude.
The FOI shows that since 2016 when the National Guardian’s Office was established, it has received only 223 contacts from NHS staff.
It also shows that the number of NHS trust staff contacts to the National Guardian has ranged between zero to 5 for each of the NHS trusts in question.
In 20 instances, the worker did not even disclose the identity of their trust.
The FOI showed that the National Guardian has received disclosures from all NHS ambulance trusts as follows:
NHS AMBULANCE TRUST
Number of workers who have spoken up to the National Guardian since 2016
North East Ambulance Service
0-5
North West Ambulance Service
0-5
East Midlands Ambulance Service
0-5
West Midlands Ambulance Service
0-5
East of England Ambulance Service
0-5
Yorkshire Ambulance Service
0-5
London Ambulance Service
0-5
South Central Ambulance Service
0-5
South East Coast Ambulance Service
0-5
South Western Ambulance Service
0-5
NB The NGO has not given the exact numbers on grounds of possible identifiability
The National Guardian has also received disclosures from a sample of NHS trusts which have been troubled.
Number of workers who have spoken up to the National Guardian since 2016
University Hospitals Sussex NHS Foundation Trust (and predecessor bodies)
0-5
Greater Manchester Mental Health NHS Foundation Trust
0-5
West Suffolk NHS Foundation Trust
0-5
South Tees NHS Foundation Trust
0-5
Royal Free London NHS Foundation Trust
0-5
Portsmouth University Hospitals NHS Trust
0-5
NB The NGO has not given the exact numbers on grounds of possible identifiability
When did Greater Manchester Mental Health NHS Trust staff whistleblow to the National Guardian?
Did the National Guardian respond supportively to the worker(s) at Greater Manchester Mental Health NHS Foundation Trust?
Did the National Guardian take adequate action in response to these disclosures?
Could the National Guardian have helped to end the abuse?
Or was it the usual story of whistleblowers being fobbed off by her Office?
Did Greater Manchester Mental Health NHS trust staff whistleblow to BBC Panorama because they received no meaningful help from the National Guardian?
These questions need answers and I will ask NHS England to ensure that the independent investigation that it has commissioned considers these questions.
It is time for the government to stop wasting public money on window dressing and to give us fit for purpose UK whistleblowing law and infrastructure.
PETITION
Please click and add your signature to this petition to reform UK whistleblowing law – whistleblowers protect us all but weak UK law leaves them wholly exposed, lets abusers off the hook and it is a threat to public safety.
As part of the current discussions arising from the concerns about University Hospitals Birmingham, I have taken a quick and dirty look at the National Guardian’s most recent Speaking Up data, with a focus on reported detriment.
This is data supplied by NHS trust Freedom to Speak Up Guardians, who work for NHS trusts (whether substantively or sub contracted), which is sent to the National Guardian who publishes it.
The data is controlled and potentially filtered by employers, and potentially filtered again when it is processed by the National Guardian, so interpretation should circumspect.
I have looked at years:
2020/21
2021/22
2022/23 Quarter 1
(The National Guardian’s Office seems to have removed data from before 2020 from its website. I have some of the old datasets but not all, if anyone needs these.)
In my view, the data has become more incomplete and now resembles the levels of non-compliance seen when the NHS Trust Freedom To Speak Up Guardian posts were still new.
This means that unsavoury secrets can be hidden.
Unexplained failures to submit defeat the purpose of publication.
21 NHS trusts failed to return any speaking up data for Q1 2022/23, including UHB:
Birmingham Community Healthcare NHS Foundation Trust
Cambridgeshire and Peterborough NHS Foundation Trust
Dartford and Gravesham NHS Trust
East Kent Hospitals University NHS Foundation Trust
Great Western Hospitals NHS Foundation Trust
Imperial College Healthcare NHS Trust
Kingston Hospital NHS Foundation Trust
Leeds Teaching Hospitals NHS Trust
Maidstone and Tunbridge Wells NHS Trust
Northern Care Alliance NHS Foundation Trust
Royal National Orthopaedic Hospital NHS Trust
Sandwell and West Birmingham Hospitals NHS Trust
Shropshire Community Health NHS Trust
South Central Ambulance Service NHS Foundation Trust
South East Coast Ambulance Service NHS Foundation Trust
St Helens and Knowsley Teaching Hospitals NHS Trust
Sussex Partnership NHS Foundation Trust
Tavistock and Portman NHS Foundation Trust
The Clatterbridge Cancer Centre NHS Foundation Trust
University Hospitals Birmingham NHS Foundation Trust
University Hospitals Sussex NHS Foundation Trust
The data on detriment for UHB since 1 April 2020 is as follows:
YEAR
Number of reported cases of detriment after speaking up at University Hospitals Birmingham NHSFT
2020/21
7 cases (but there is also missing data from quarter 3, which was not submitted)
2021/22
18 cases (but there is also missing data from quarter 2, which was not submitted)
2022/23 Quarter 1
UHB submitted no Speaking Up data at all in Q1, including data on detriment
This data is insufficient to support meaningful discussion of UHB’s whistleblowing governance. An explanation is needed for the patchy data. The full dataset should be disclosed, or at least an explanation should be given on why data is missing.
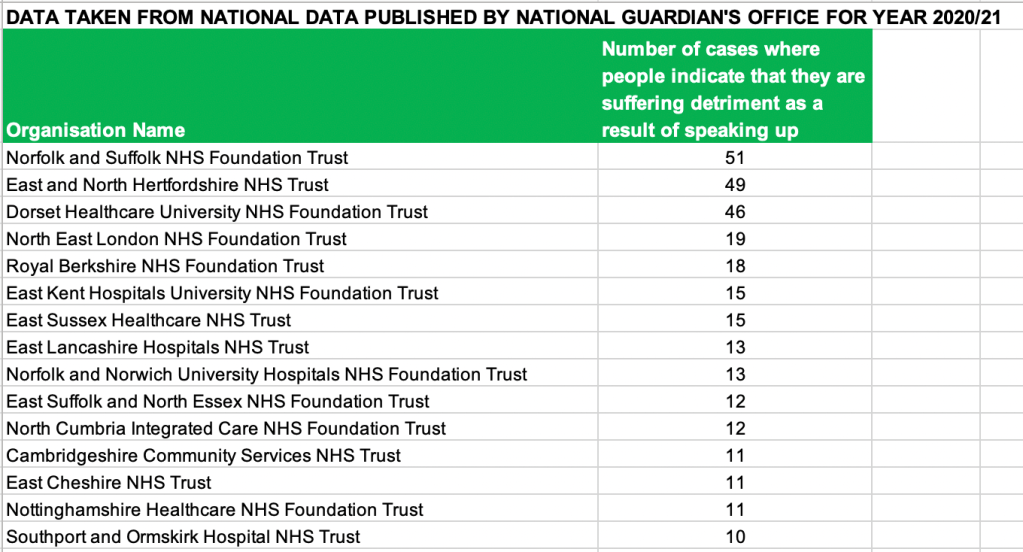
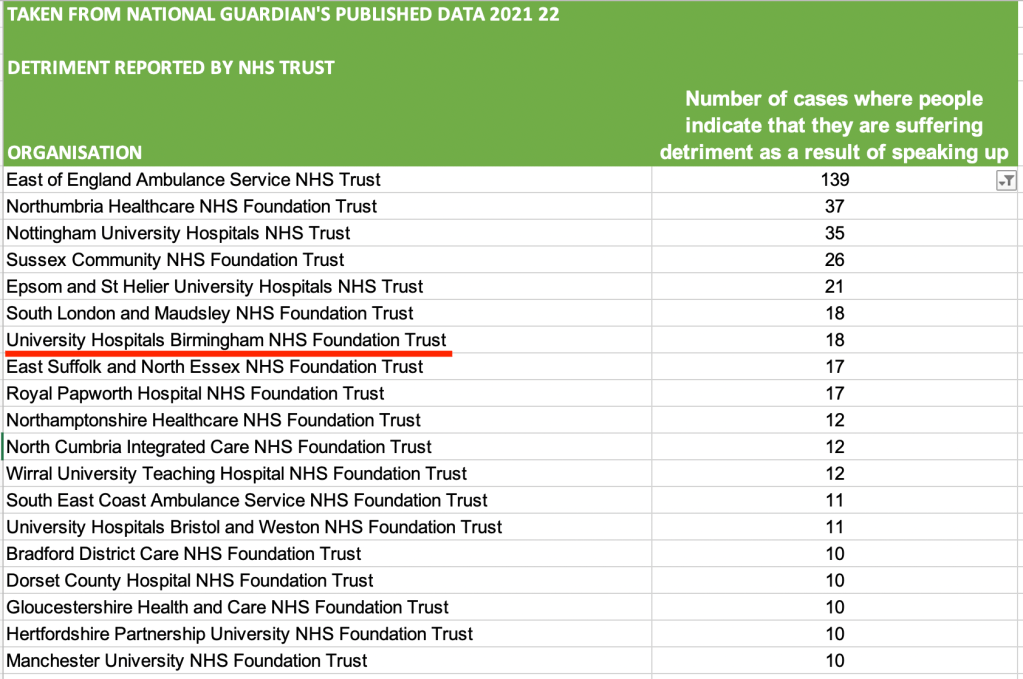
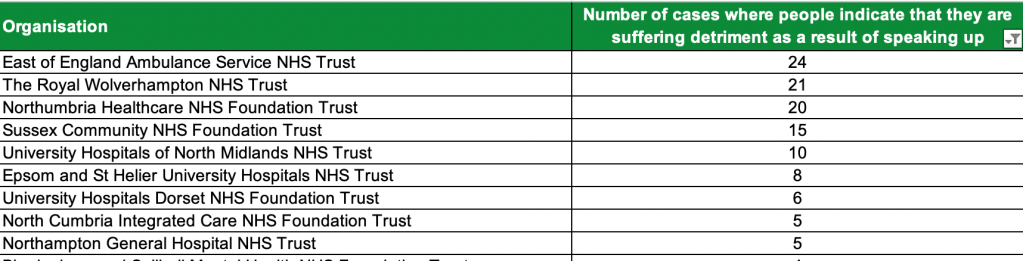
In general, the levels of detriment vary hugely between trusts:
YEAR
RANGE IN NUMBER OF CASES WHERE DETRIMENT WAS REPORTED AFTER SPEAKING UP
2020/21
Zero to 51
2021/22
Zero to 139
2022/ 23 Quarter 1
Zero to 24
The overall numbers of cases featuring detriment are as follows:
YEAR
TOTAL NUMBER OF CASES WHERE DETRIMENT WAS REPORTED AFTER SPEAKING UP
2020/21
666
2021/22
784
2022/ 23 Quarter 1
182 (If scaled up to a full year, assuming the current trajectory continues, the 2022/23 total would be 728)
The total number of cases of detriment for 2021/22 is especially high partly because East of England Ambulance service recorded a massive spike in detriment – 139 cases.
The NHS trusts reporting Speaking Up data are different in size and function, and it is not possible to interpret the data on numbers of cases of detriment as a league table.
That caveat apart, these are the trusts which reported the highest numbers of cases of detriment in 2020/21, 2021/22 and 2022/23 YTD:
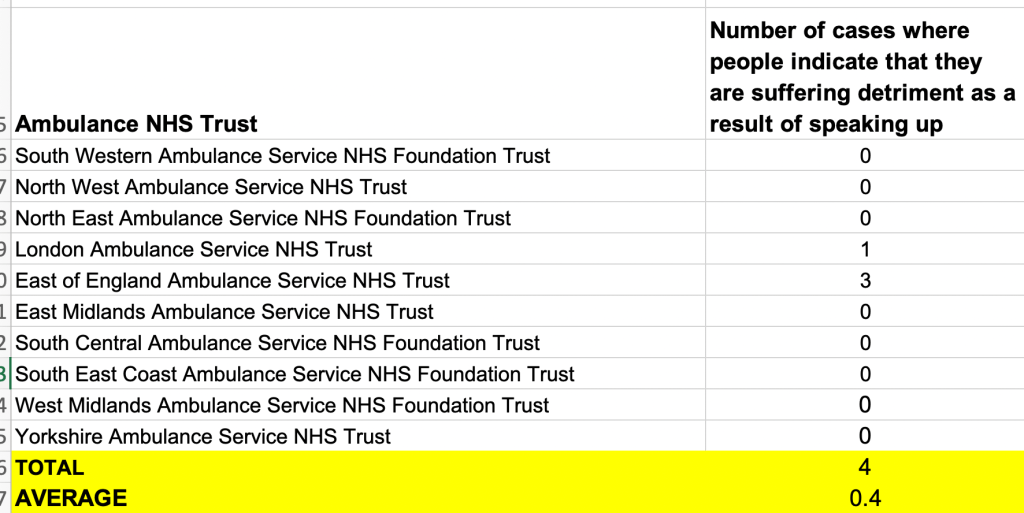
Importantly, low reported numbers of cases with detriment are not necessarily a good sign. It may reflect staff fearfulness to the point of not engaging at all, or it may reflect on the integrity of the data.
As an example, these are detriment statistics for ambulance trusts from 2020/21, which look implausibly low to me:
I scrubbed the National Guardian’s spreadsheets of non-NHS trust organisations in order to make the handling and analysis of Speak Up statistics on NHS trusts easier.
Here are uploaded spreadsheets, with Speaking Up data on just NHS trusts, for anyone who might have a use for them
For completeness, this is an FOI response from UHB in 2018, which revealed that the feedback from staff who had used the Freedom To Speak Up service was not collected in a structured format.
By Dr Minh Alexander retired consultant psychiatrist 3 December 2022
For decades the UK Government has resisted good whistleblowing governance across all sectors. It has refused to meaningfully reform very weak UK whistleblowing law.
It hired lawyer Robert Francis to review whistleblowing in the NHS after the Mid Staffs scandal.
Despite recognising that UK whistleblowing law is weak, Francis declined to support legislative reform. He claimed in his 2015 review report that it would take too long, and that his go-faster model, the Freedom To Speak Up model, would be more expedient.
Later however, Francis claimed in 2020 correspondence that his model required time to work. A third party sent me correspondence from Francis, which stated:
14 January 2020:
“I fear we are not going to agree about the value of the Freedom to Speak Up National Guardian. Her office and the network she leads is making a great deal of progress on promoting the freedom to speak up without legislative or regulatory powers. The concept of guardians in this context is a new one and needs time to develop.”
Francis also claimed expansively in his 2015 review report that his model would make serious reprisal in the NHS “very rare”. Possibly a claim that he now rues, given the steady stream of suspensions, unfair sackings and employment tribunal claims by harmed whistleblowers.
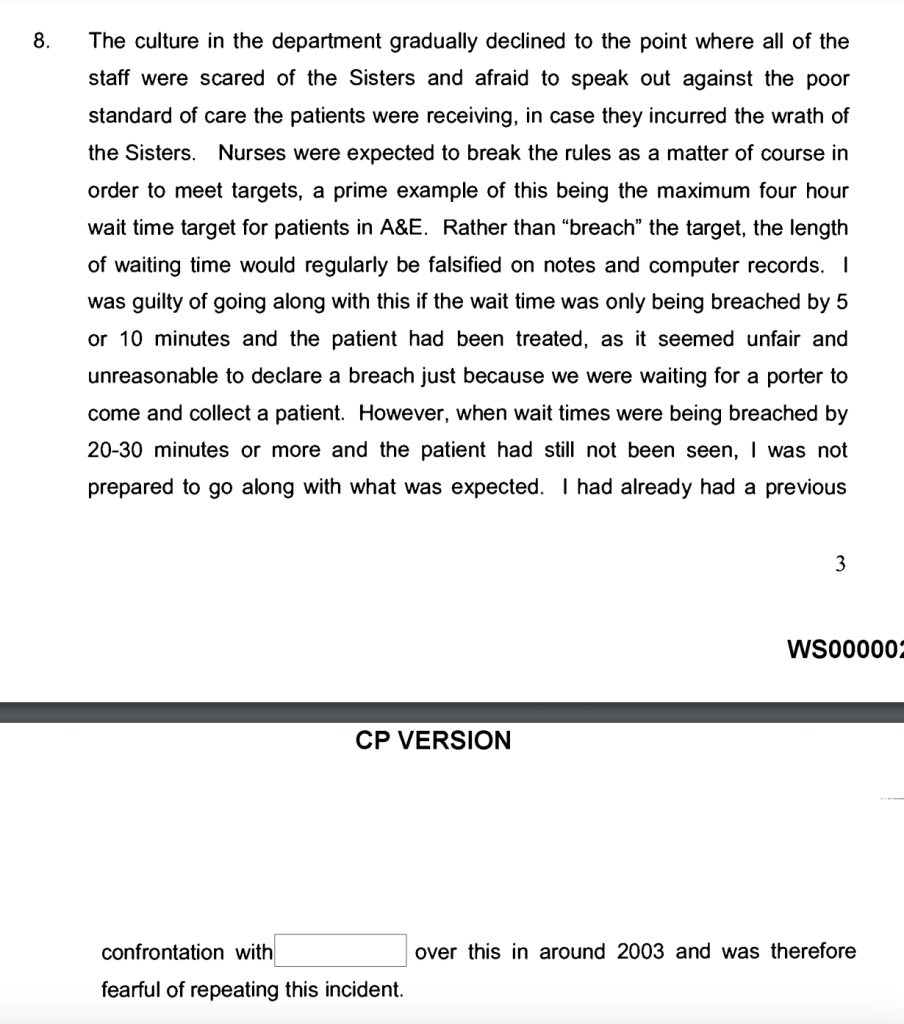
Seven years on from Francis’ review, we see yet another scandal about poor care and whistleblower reprisal making its way into the mainstream media – the situation at University Hospitals Birmingham Trust, which has been the subject of two lengthy articles on BBC Newsnight.
Francis was not interviewed by Newsnight, but two individuals who have been party to his project were interviewed last night:
A nurse who worked at Mid Staffs, reported that she was bullied for raising concerns and gave a statement to the related public inquiry about poor care. She described how records were falsified about A&E target times, including an admission that she went along with some of this, for in her opinion, justifiable reasons:
There is a possibility that the model was in fact based on earlier arrangements in the civil service.
Donnelly has worked with the National Guardian to produce publicity material for Health Education England on Freedom To Speak Up and has blogged for the National Guardian:
Donnelly has most recently left the NHS and is now reportedly Head of Safety Culture at the Nuffield Trust. I could find no details about this on the Trust’s website.
The BBC Newsnight interview2 December 2022
I could not clearly hear the whole interview but neither Dunne nor Donnelly seemed willing to acknowledge the flaws of the Freedom To Speak Up model.
When Donnelly was asked about issues of independence, and whether Guardians should be people who have worked for an NHS trust, she stated in response that the responsibility for resolving issues lay with senior managers and not Guardians.
Hardly any Guardians do so of course, because they are trust employees and subordinates of the trust directors who they are implausibly supposed to hold to account. And people have families and mortgages.
Therein lies the core unworkability of the Freedom To Speak Up model.
Donnelly spoke about the “right” people being appointed as Freedom To Speak Up Guardians. The flaw of this narrative is that in a bad organisation, directors will appoint either bad apples like themselves, or they will ignore or even harm Guardians. The latter has happened on occasion.
Selecting the “right” people to be Guardians is immaterial in the worst organisations. In a bad organisation, the Freedom To Speak Up model is a recipe for either creating more victims of reprisal – the Guardians – or producing PR material to hide executive misconduct.
Dunne stated that the model works in “the best” NHS trusts. In the process he accidentally indicted his government’s handiwork. He implicitly acknowledged that Freedom To Speak Up does not work in bad trusts and that it is therefore ineffective. Moreover, as the model is unnecessary in trusts with good culture, it is a humongous waste.
Dunne muddied the waters by claiming that Freedom To Speak Up Guardians had not been in place for long in all places. This is strictly true of NHS quangos but the core objective of appointing Guardians in all NHS trusts was achieved about five years ago. So there is no excuse for the model’s failures on grounds that it is recent.
When Dunne was asked if performance targets could be counterproductive, he replied that targets were necessary so that staff could plan their rotas. Hmm.
Donnelly was critical of targets and argued that there should be more realism about what could be achieved.
Neither spoke about the underfunding of the NHS, which is at the heart of so many cover ups, although Donnelly in fairness did touch on understaffing.
I have transcribed the interview and reproduce it below.
One hopes that Newsnight will look further into these matters.
We are almost a decade on from the publication of the Mid Staffs public inquiry, which recommended that criminal penalties should be introduced for whistleblower suppression.
The government rejected this recommendation, and Francis did not later fight for it in his report of the Freedom To Speak Up review.
In fact, Francis seemed faintly derisive in his report of contributors to his 2015 review who asked for criminal penalties to be introduced.
If the media does not explore and report in sufficient depth the legal and political factors that drive continuing whistleblower reprisal and cover ups, we will likely be no further forward in ten years’ time.
The GMC advised the BBC that in contrast, nationally, 33% of referrals result in action.
I sent the FOI data about UHB’s zero rate to UHB’s Freedom to Speak Up Guardian in June this year. I wonder what trust changes, if any, resulted from that.
From: Minh Alexander <REDACTED > Subject: Outcome of GMC referrals by UHB Date: 18 June 2022 at 15:55:22 BST To: Julian Bion <REDACTED>
Dear Professor Bion
I write to pass on information that may be of interest to you in your role as UHB Freedom To Speak Up Guardian:
This shows that 26 GMC referrals by the trust, 25 of which had medical director sign off, resulted in no further action by the GMC.
I wonder if this makes UHB an outlier, as employer referrals to the GMC usually have a much higher likelihood of resulting in GMC investigation.
I have also seen it said that employer referrals are more likely to result in GMC sanction, but I cannot find a supporting reference for this.
Best wishes,
Dr Minh Alexander
MY TRANSCRIPT OF THE BBC NEWSNIGHT INTERVIEW 2 DECEMBER 2022 WITH DUNN AND DONNELLY
Kirsty Wark: So when a trust is deemed one step away from Inadequate as is the case for the Birmingham University Trust, facing so many allegations, how do you turn it round and change the culture?
We can speak now to Conservative MP and former Health Minister Philip Dunne and also to Helene Donnelly registered nurse and key witness in the Mid Staffordshire NHS Foundation Inquiry. More recently she’s been an ambassador for cultural change in an NHS trust. She’s now Head of Safety Culture at Nuffield Health.
Good evening both of you. This is really a question for both of you. There was a system established As we’ve just been hearing that was meant to improve culture after 2016, after the Mid Staffs inquiry.
Tell me first of all Philip Dunne why hasn’t that worked out the best it could?
Philip Dunne: So good evening Kirsty So I was in post following Sir Robert Francis’ report in 2015 and we introduced when I was a minister in the Department of Health the National Guardian system.
Which began in 2016 by the appointment of Dr Henrietta Hughes who stepped down only last year and she’d gone on to become the patient safety commissioner.
That has recruited a network of Freedom To Speak Up Guardians right across the NHS. I believe there are now 800 Guardians who are there to act as a first point of referral when people have got a concern or a complaint and last year there were over 20,000 cases reported through to these Guardians. They haven’t been in post in all settings for that long. I understand that from the last Freedom To Speak Up Index, taking a look at the questions asked in the annual NHS staff survey, that something approaching two thirds – I think it’s 65.6% of staff said in answer to the question they felt safe to report concerns. Now, I think that is good but clearly it means that there are another one third of trusts where they, staff don’t feel that. And that’s where the focus needs to be.
Kirsty Wark: Well Helene I wonder because you know all about the Guardians obviously. So is there an issue with who appoints the Guardians. Are they truly independent. And also do people know how to find Guardians? Do they even know that system existed?
Helene Donnelly: Yes there’s a huge amount of advice and guidance that comes through from the National Guardian’s Office. However they are limited because they are under resourced themselves and they don’t have any actual statutory powers [inaudible] ….trusts themselves really….[inaudible] who they’re appointing and how they’re appopinting them and ensuring they have the right people. There are requirements for them to be trained by the National Guardian’s Office and also should be registered with the National Guardian’s Office….[inaudible] but there are here some in posts associated with that. I think there does need to be more on national scale, a national conversation about what why these failings keep happening. Why there’s no accountability? And every time where there isn’t accountability it leads to further corrosion of trust for the public, for the workforce and we’re already seeing workers leaving the NHS.
Kirsty Wark: Just hearing Sharan talking about the fact that as she was raising concerns, as somebody that was nothing to do with the medical profession, the nurse was keying [?] into a computer what was going on but the nurse felt she couldn’t raise concerns. Clearly her father didn’t have cancer, he’d been treated for cancer and he knew his gallbladder had to come out [?]. That’s so incredibly shocking isn’t it? And it must give pause to people who think I’m not sure things are going right in my own case. People have to have trust in the system, and I wonder in some instances, do you think it should ever be the case that a Guardian should ever have worked at that hospital?
Helene Donnelly: I think erm that there are Guardians that have worked at the hospital but they are limited… [inaudible] ….they have to escalate the concerns to the senior leadership and the responsibility is on the senior leadership, not the Guardians to resolve the concerns.
Kirsty Wark: Let me ask Philip Dunne that. Because the trust has told us that they take patient safety very seriously, high reporting culture, rigorous investigation of patient complaint., But of course the Guardians can only as Helene was saying can only go so far They’ve taken to senior management but and of course senior management are under pressure with the targets and so forth, and clearly something is going wrong at the Birmingham Trust and indeed probably at other hospitals [inaudible] Birmingham trust.
Philip Dunne: So when I was in post, when I visited trusts that were in special measures I always insisted on meeting the senior Guardian within the trust and would ask them whether they had direct access to the chief executive or one of the non executive directors of the trust appointed to have that relationship. And I think that’s what’s essential – for the Guardian to be taken seriously they have to be able to escalate issues right to the top of the organisation. And then the chief executive or the non executive, they’re charged to do it, need to have the confidence of the Guardians when they’re taking cases to them that they will get investigated. That happens in the best trusts and should happen…
Kirsty Wark: Sorry to interrupt. What I was going to say was in our investigations in this hospital, there are allegations that there is mafia style management, and that the mafia style management is allegedly using the threat of the GMC and other threats to silence doctors who want to speak out. How concerned are you about that Philip Dunne?
Philip Dunne: Well I can’t talk about those allegations….
Kirsty Wark: No, not about those specific allegations
Philip Dunne: Well what I do say is absolutely right is that that the culture within the organisation needs to be one where we learn from mistakes. Mistakes happen. There are 1.5, one and half million patient interactions every day in the NHS. That’s 550 million in a year so things can go wrong. And when they do go wrong, we have to have a culture where we learn from our mistakes. That’s what the whole patient safety culture we’re trying to instil across the NHS is all about.
Kirsty Wark: Helene do you think excessive targets and different indices for outcome are actually counterproductive at the moment?
Helene Donnelly: Yes I do. And we saw this ten years ago at Mid Staffs. Even worse now given the current pressures and the knock on effects of that. The fact that I’ve got so many healthcare professionals striking, so many healthcare professionals leaving, it’s just adding more and more pressure and it’s not actually protecting patients more. We need to be more realistic about what can be achieved. We need to listen to our staff, to value the staff. If we keep losing valued and talented, experienced [inaudible] professionals throughout the health and social care system then we will not be able to care fpr patients. We need to value the workforce and listen to them when they speak up to raise concerns.
Kirsty Wark: The phrase that was used earlier was a phrase that the staff, the nursing staff, are sometimes just too tired to have time to care.
Helene Donnelly: Yeah I absolutely recognise that. I think there’s a huge degree of apathy that’s creeping in as well. I believe it’s worse than when I was experiencing the issues at Mid Staffs. I think staff are being actively discouraged from speaking up because of the pressures across the country. This isn’t obviously just about Birmingham. There are widespread issues. Of course we understand that, but we are seeing a workforce which is on its knees and it is undervalued and under supported and that leaves the staff not being able to care for patients as they should and it leads to absolute corrosion of trust from the public and from the workforce itself.
Kirsty Wark: So Philip Dunne, I wonder if you concur that targets and the pressures that they’re bringing on at the moment, are not fit for purpose?
Philip Dunne: Well I think targets to recruit more people into the clinical workforce are absolutely right and the government is on its way to meeting the targets that have been set for this parliament. I think since 2010 there are thirty four thousand more doctors working in the NHS and forty four thousand more nurses. So the workforce is growing. I think the fact that there are over twenty thousand cases reported last year of this issue, to the Guardians, suggests that something is going better than it was when there were none before this system existed. But I absolutely recognise there are very significant pressures on everybody working in the NHS at the moment. If we…
Kirsty Wark: But on that question….
Philip Dunne: Going on strike is not going to help
Kirsty Wark: On that question of the pressure I’m seeing, it’s not the targets for recruitment I’m talking about. It’s targets about getting a certain amount of care done by a certain day, a certain degree to day a certain amount of operations through the system. Sometimes that’s actually probably counterproductive and leads to more pressure. I wonder if you recognise that?
Philip Dunne: Well there’s an enormous backlog of cases that have got to be treated so I think trying to set some kind of guidelines about how many cases should be dealt with and by particular specialties, it helps people to plan their rotas. Surgeons have to have rotas.
Kirsty Wark: Let me ask you about that Helene. You think surgeons can organise their rotas and nurses will be able to work as hard as they could without targets to drive them on.
Helene Donnelly: Absolutely and the bottom line is that there isn’t enough. I can see there have been improvements in the last year, last few years but equally in that time, the population rises, the pressures on the workforce [inaudible] …lots of medics, lots of nurses and other professionals are retiring early. We’re recruiting more, so perhaps you know they’re lacking in expertise and clinical experience. We’re lacking that.
Kirsty Wark: Thank you both very much indeed.
A National Guardian newsletter featured this:
UPDATE 12 DECEMBER 2022
A BBC Newsnight interview with the UHB Freedom To Speak Up Guardian on 9 December 2022 raised further concerns:
Please click and add your signature to this petition to reform UK whistleblowing law – whistleblowers protect us all but weak UK law leaves them wholly exposed, lets abusers off the hook and it is a threat to public safety.
Dr Minh Alexander retired consultant psychiatrist 1 December 2022
This is a post to share engineers’ reports and related documents on NHS buildings that are at risk due to unsafe roofs.
It also feedbacks about NHS trusts which have failed or refused to disclose such information, in a context of minimisation by NHS England.
The NHS has always been underfunded, and building hospitals is a complicated business, with a history of good intentions followed by misfires.
Decades ago, some NHS hospitals were built quickly on the cheap, with central government oversight – the “Best Buy” hospitals, which were offered with the slogan “Two for the price of one!”.
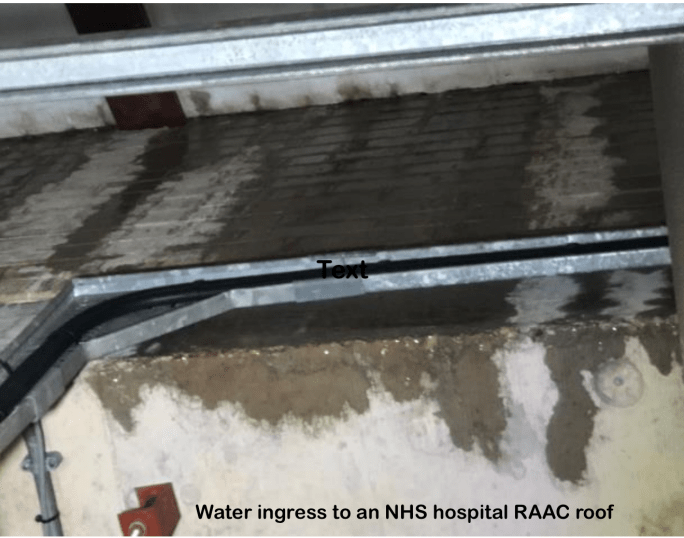
Simple construction techniques included the use of limited-life Reinforced Autoclaved Aerated Concrete (RAAC) beams in roofs.
RAAC roofs were often flat, resulting in later problems with water ingress.
Reinforced Autoclaved Aerated Concrete
RAAC was developed in Sweden a century ago.
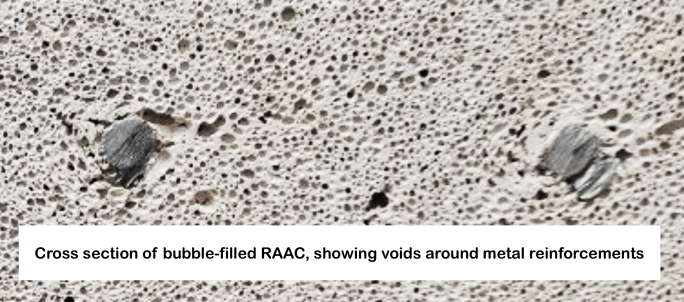
It is composed of bubble-filled concrete, without coarse aggregate, which is usually embedded with metal reinforcements.
The material is lighter, and insulates better, but it is less strong.
“Compressive strength is significantly lower than traditional concrete at 2-5N/mm², as are related flexural, shear, and tensile strengths. Elasticity and creep are substantially inferior to traditional concrete due to the aerated nature and lack of coarse aggregate, which are reflected in large observed long-term deflections. [Bending]”
RAAC also does not prevent corrosion of the embedded metal components as effectively as normal concrete.
Surveys of failing RAAC roofs on school buildings have shown that a lot of the damage has related to water ingress, resulting in corrosion of metal reinforcements, and loosening of the metal reinforcements from surrounding concrete.
“Not all defects are visible … panels which appear to be in a good condition may conceal hidden defects which could present a risk to the integrity of the panels,” it said. “The corrosion of reinforcement could lead to large pieces of RAAC falling which presents a risk to occupants.”
It has also been reported that there are variations in RAAC material, which may create additional unpredictability.
“By the 1980s, RAAC roof planks installed in the 1960s had begun to fail. Subsequent case studies revealed significant underlying issues with the RAAC roof planks. The steel reinforcement was often insufficiently covered, allowing corrosion to occur. Many roof planks had a high span to depth ratio, meaning that they did not have the suitable capacity to span between bearing points. Often, the steel reinforcement did not extend throughout the complete length of the product and contained an inadequate number of welded crossbars.”
RAAC beams bend and may disrupt water proofing materials as they warp. Water ingress by this route, or other routes, may pose an added threat to the beams. Some beams were cut to fit particular sites, which would have removed important, extra metal reinforcements located at the ends of the beams and compromised their load bearing capacity. Harsh weather can also pose a threat to RAAC roofs. For example, snowfall can push RAAC roofs to their limit and this has to be factored into the risk management.
“RAAC is a lightweight, ‘bubbly’ form of concrete that was commonly used in school and other buildings from the mid-1960s to the mid-1980s.”[my emphasis]
It is thought that the safe life span for RAAC structures is about thirty years.
Some NHS hospitals have RAAC roofs which are known to exceed this 30 year timescale.
Trust board papers by an affected NHS trusts, Queen Elizabeth Hospital King’s Lynn NHSFT (QEHKL), asserted in February 2020 that the life span was even shorter – 25 years.
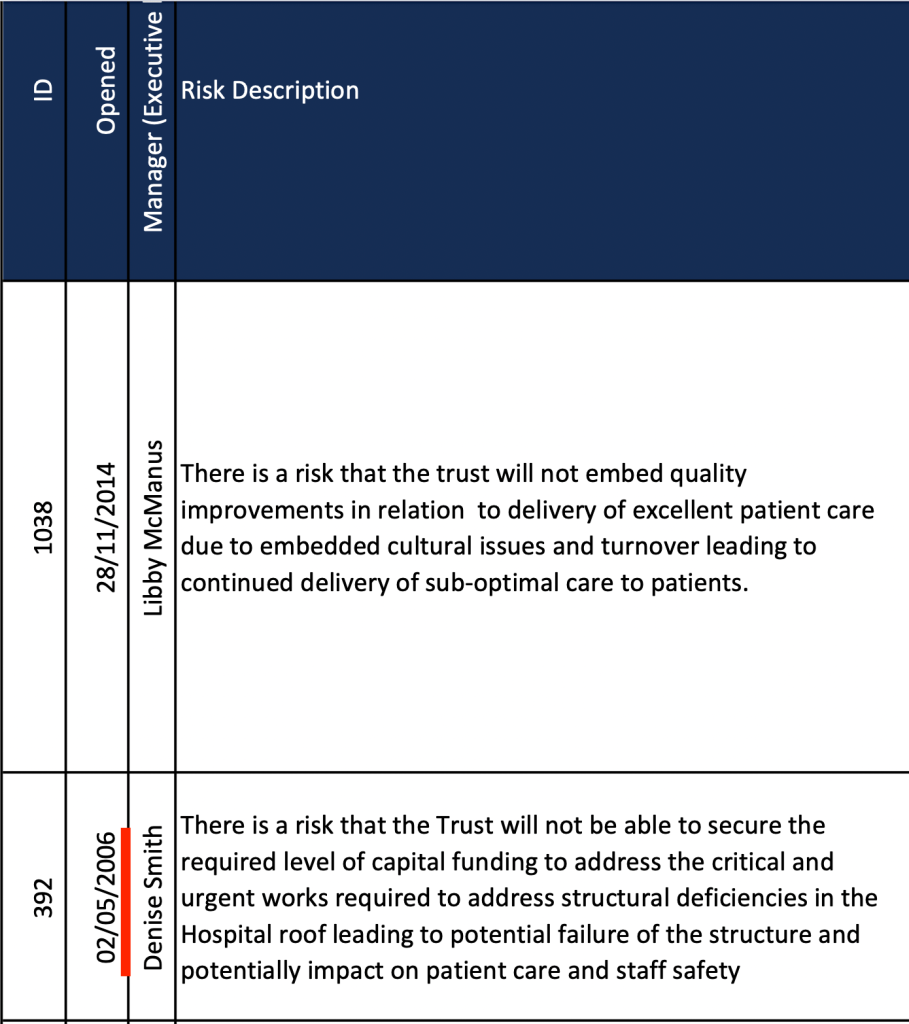
Consistent with this, QEHKL trust board papers indicate that the problem of the RAAC roofs has been on QEHKL’s risk register since May 2006 – twenty five years after the hospital was built.
To help prolong the life of RAAC panels, the following rules should be adopted generally. A structural engineer should be consulted if the following cannot be complied with:
No additional loads to be applied to any RAAC panels.
No new fixings should be installed to the panels
No additional penetrations should be formed through the RAAC panels without a review from a structural engineer
RULES FOR GENERAL OPERATION
The following should be put in place as operational procedures:
Where standing water is present on the roof, introduce robust pumping arrangements to discharge excessive quantities of water.
Snow build up on the roof should not be allowed to generally exceed 200mm. When removing snow, snow should not be piled in any location to height of greater than 300mm.
If snow does build up greater than 300mm, all accommodation below should be closed to access until the snow has been clear and panels re-assessed by a structural engineer.
Maintain robust roof permit system to control access to the roof and to inform personnel of restrictions
No roof maintenance should exceed the design loadings of 0.6kN/m2.”
Not all RAAC beams in NHS buildings have been surveyed due to problems of access, which makes risk assessment and management more difficult.
Some trusts have been forced into elaborate risk management arrangements, with frequent checks, physical propping of the roofs and full or partial decanting of some buildings.
Queen Elizabeth Hospital King’s Lynn NHSFT had to evacuate a theatre complex on an emergency basis this July, because of ceiling movement.
Local MP Liz Truss spoke about the problems at King’s Lynn during the recent Tory leadership race, but had reportedly ignored concerns for years.
In September the Lib Dems shared an FOI request to NHS England which revealed that there were 32 NHS buildings which had RAAC roofs:
Number of buildings with RAAC roofs
NHS TRUSTS
Queen Elizabeth NHS FT
4 (Kings Lynn)
West Suffolk NHS Foundation Trust
2
James Paget University Hospitals NHS Foundation Trust
1
North West Anglia NHS Foundation Trust
2 (Hinchingbrooke Hospital) 1 (Stamford Hospital)
Mid and South Essex NHS FT
1 (Broomfield)
Airedale NHS Foundation Trust
1
Liverpool University NHS FT
1 (Aintree)
Mid Cheshire Hospitals NHS FT
4 (Leighton)
Blackpool Teaching Hospitals NHS FT
2
Countess of Chester NHS FT
1
University Hospital Southampton NHS FT
1
Frimley Health NHS FT
1 (Frimley Park)
Midlands Partnership NHS FT
1 (Haywood)
Doncaster and Bassetlaw NHS FT
2 (Bassetlaw)
Worcestershire Acute Hospitals NHS Trust
1 (Kidderminster)
York Teaching Hospital NHS FT
1 (Scarborough)
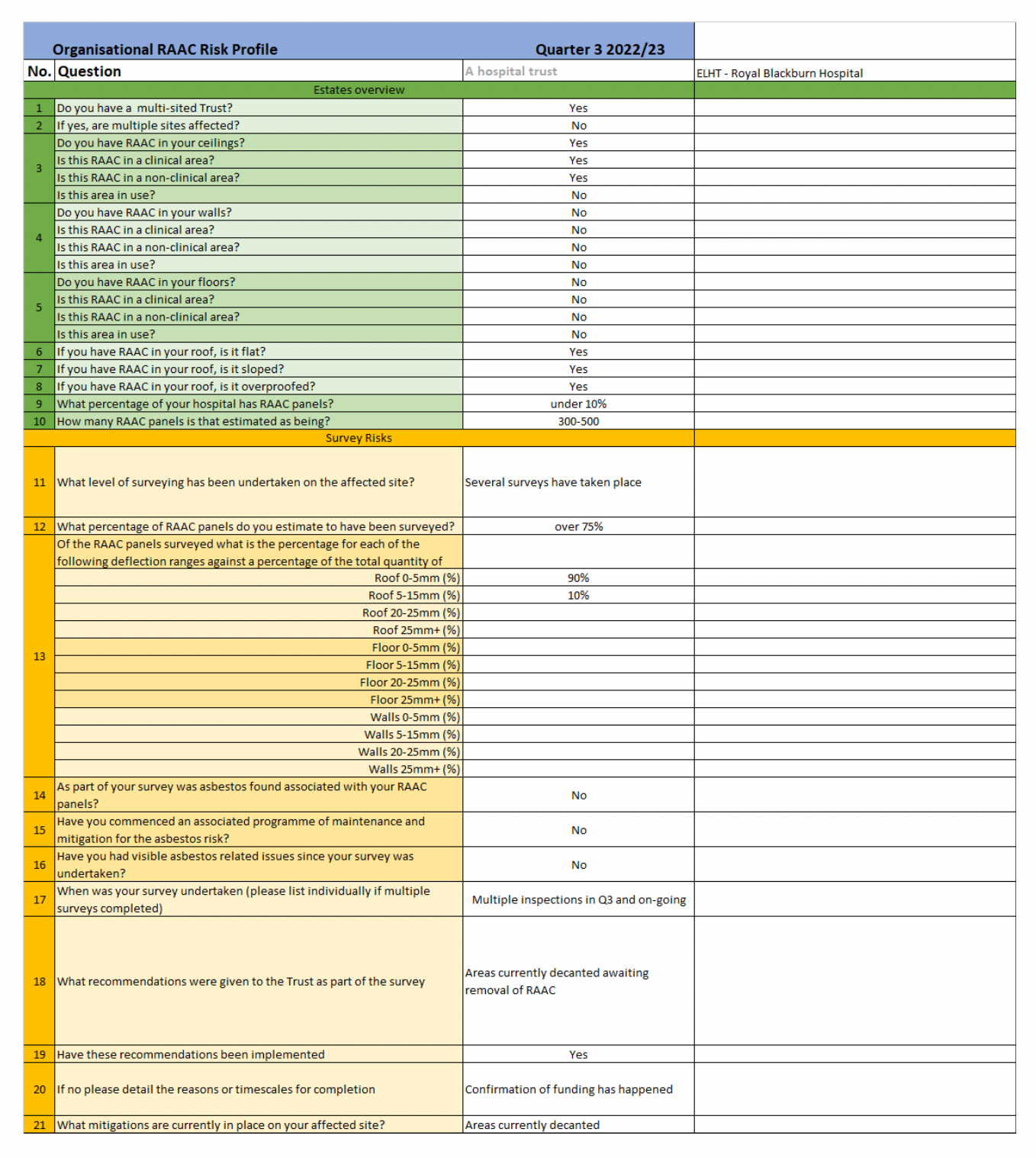
East Lancashire Hospitals NHS Trust
1 (Royal Blackburn)
Northern Care Alliance
1 (Royal Oldham) 1 (Salford)
NHS Trust total
30
NHS Property Services
1 Haverhill
1 Warren Farm
NHS Property Services total
2
NHS England advised on 28 October 2022 that this may not represent the full extent of NHS buildings affected by RAAC issues, and that effectively, no one knows how many more buildings need remediation.
“The safety of our people within our hospitals is of paramount importance to the NHS. On learning of the issues surrounding reinforced autoclaved aerated concrete (RAAC) beams, NHS England wrote out to all organisations in 2019-20, asking them to assess their buildings for RAAC. The result of this was the instigation of the national RAAC programme.
Proactive steps are being taken to ensure that all RAAC in the NHS is identified and subsequently eradicated; the list above represents our current understanding of RAAC across the NHS.
At this time, we cannot state that this is the final list of all instances of the material across the NHS however we have a clear process for tracking and mitigating RAAC if/as/when it occurs.” [my emphasis]
To obtain more detailed information on the risks, I asked affected NHS trusts and NHS Property Services for engineers’ reports and risk management documents.
Several trusts did not respond at all, or gave limited responses, which may reflect discouraging attitudes by NHS England and the Department of Health.
Others have upheld the public interest and shared information more transparently.
The data reveals a story of chronic anxiety, disruption and sometimes desperate making do.
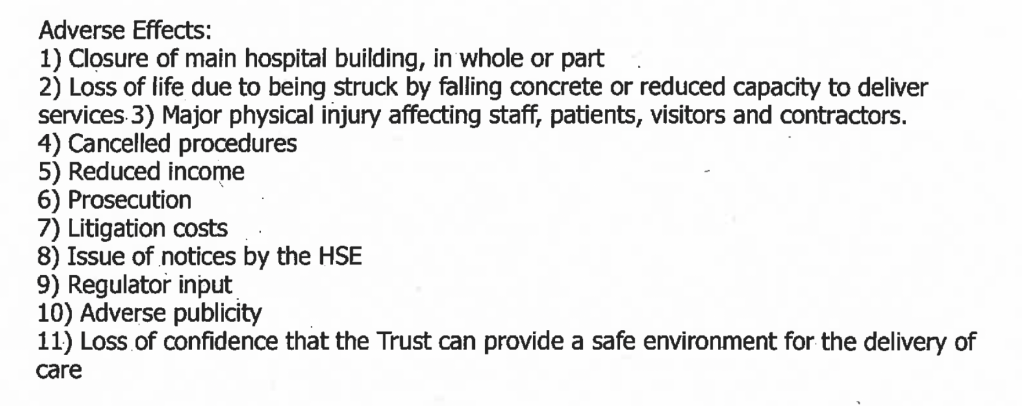
It also shows that affected NHS trusts are painfully aware of not just the risks to people, but the likely legal, regulatory and health and safety blowback if the roofs collapse.
The data shared, whether in full or only partially, puts to shame NHS England’s unsupportive comments last year about the QEHKL then chief executive’s advocacy for her service.
The trust gave the following account of its risk management:
“The Trust has made safe the RAAC units in the laundry by providing a fail safe supporting structure. In line with guidance and initial evaluation by the approved structural engineers these are now inspected on an annual basis, The planks are not above patient or public areas, and as they are independently supported no progressive deterioration can be expected. Consequently, no special evacuation plans over and above a standard space evacuation for fire is envisaged, and the area would be re-inspected by engineers in the event of any detectable failure or deterioration of a unit.
The Units on Phase 4 roof are immediately above medical records storage. Each unit is secured between steel supports; therefore no progressive collapse is anticipated. As with the laundry the units are inspected annually, and currently all are in good condition. Additional investigation and evaluation is being undertaken in November. The roof therefore has a low risk score of 2 and consequently no special evacuation plans over and above a standard space evacuation for fire is envisaged, and the area would be re-inspected by engineers in the event of any detectable.”
Queen Elizabeth Kings Lynn NHS Foundation Trust
The trust has had the highest profile with regards to RAAC roof problems.
It was opened in 1980. The site weas mostly constructed with RAAC roofs.
NHS England’s above disparaging comments about the trust’s external comms seems, unsurprisingly, to have dampened the trust’s willingness to reveal details.
The trust has not provided engineers’ reports as requested, with no explanation, and has disclosed only this summary:
“Rolling programme of maintenance and failsafe installation
79% of the hospital buildings have RAAC planks that need monitoring and emergency repairs carried out on a rolling basis. We have a dedicated team of surveyors and technicians who survey the buildings and identify where support props and failsafes are needed to reduce the risk of plank failures in the roof and maximise safety.
In 2021/22, with £20.6m national capital funding we opened new Endoscopy and Outpatient Units to create the necessary theatre and ward decant space for a three-year rolling failsafe programme.
The first year of an £80m three-year programme is currently underway to install failsafes across the first floor of the hospital. The investment maximises safety and does not create additional ward space or capacity.
Evacuation plan in the event of RAAC failure
We have robust plans in place in the event of RAAC failure and these are tested regularly. This includes the East of England RAAC response plan and a smart evacuation system (which is recommended by NHS England in the East of England for implementation across all acute and community providers in the region). There is also an overarching Trust-wide evacuation plan which covers all eventualities.
Appropriate training has taken place and several exercises have been undertaken to test our response to a RAAC emergency. Learnings from these exercises have been used to further strengthen our plans.”
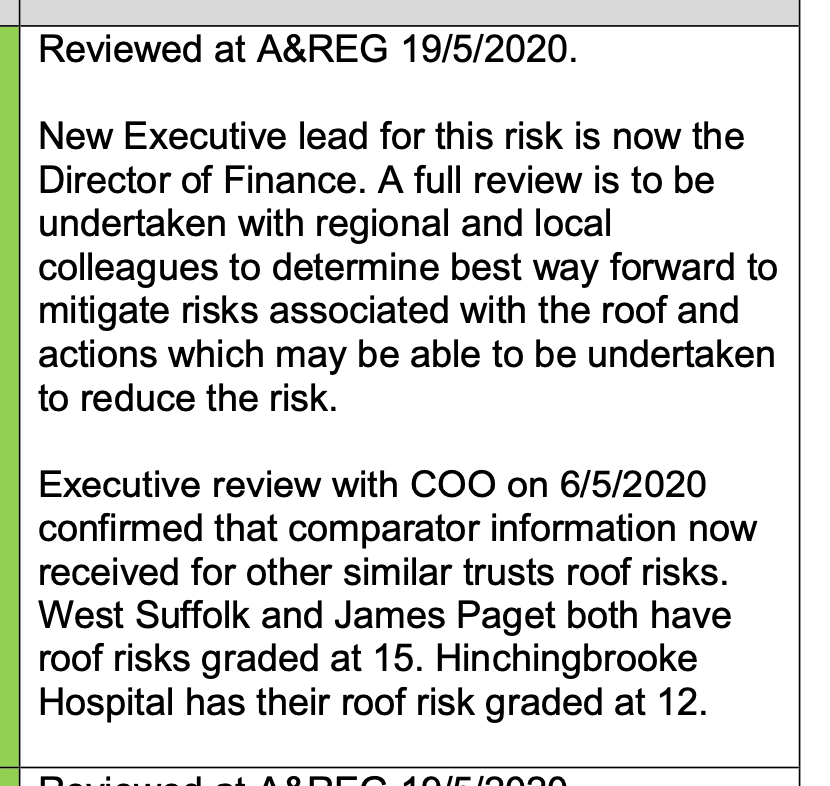
Although the trust has withheld engineers’ reports, there is a continuous summarised narrative in “Significant Risk” reports in the trust board papers.
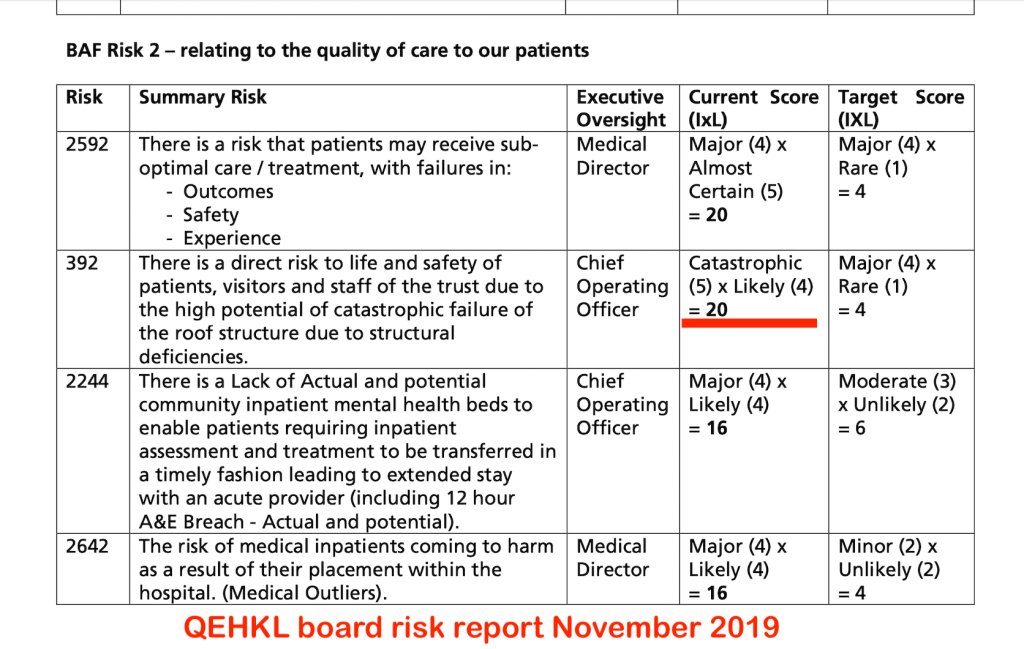
Risk has been graded at 20 since 2019 (Likely catastrophic harm).
The Board papers also show that the RAAC roofs have been an open item on the trust risk register since May 2006:
The trust has benchmarked with other affected trusts and concluded that it was more badly affected than comparators such as Hinchingbrooke Hospital and James Paget Hospital:
A hospital spokesperson, understandably, commented:
“This demonstrates once again that our hospital is unfit for purpose and the need for an urgent announcement about the desperately needed funding for a new QEH, recognising the impact on patient and staff experience and the operational running of our hospital.”
It beggars belief that a hospital that is incredibly stressed by COVID19 and all the other ills that beset the NHS, has to also juggle emergency evacuations of critical areas because of unpredictably failing infrastructure.
Frimley Health NHS Foundation Trust
Frimley claimed that it could not disclose the requested material because it is intended for future publication.
It has not answered questions about the purported future publication.
“We can confirm that in line with the following report points, we undertook the following actions:
6.2- the first floor of A block was cordoned off 6.3- immediate mitigation of temporary steel props to underside of ceiling 6.5- we are currently undertaking a programme of works to replace the roof
This work has been funded by the National RAAC Replacement scheme and is regularly monitored by them.”
North West Anglia NHS Foundation Trust
The roof at Hinchingbrooke Hospital, run by the trust, is a well known example of the RAAC roof problems.
The trust has issued a blanket refusal to disclose any engineers’ reports on spurious grounds of “commercial interest”:
“Following a detailed review of both your initial and subsequent request, North West Anglia NHS Foundation Trust (the Trust) is withholding the engineers’ reports. It is the Trust’s view that this information is exempt under Section 43 (Trade secrets and prejudice to commercial interests).”
The trust reported on 22 November 2022 that the affected areas have decanted and mothballed:
“The affected areas have been decanted and it has now become a restricted access construction site. Programme of works to remove the roof panels has commenced. There is no risk to patients, staff or the general public.”
Southampton University Hospital NHS Trust
The trust has not provided a response despite being reminded.
It advised on 27 October 2022 that props had been required and that the affected area had been decanted:
“Following a survey in February issues in three locations resulted in acro props being installed. Due to this the services were unable to safely access the day case unit, orthotics and out of hours nursing. Services were temporarily stood down and have now been fully decanted. The section of the Hospital with RAAC planks is now locked off and access managed and restricted to facilities and estates for the purposes of surveying and monitoring whilst the Trust works through the business case process for the replacement of the building.”
West Suffolk NHS Foundation Trust
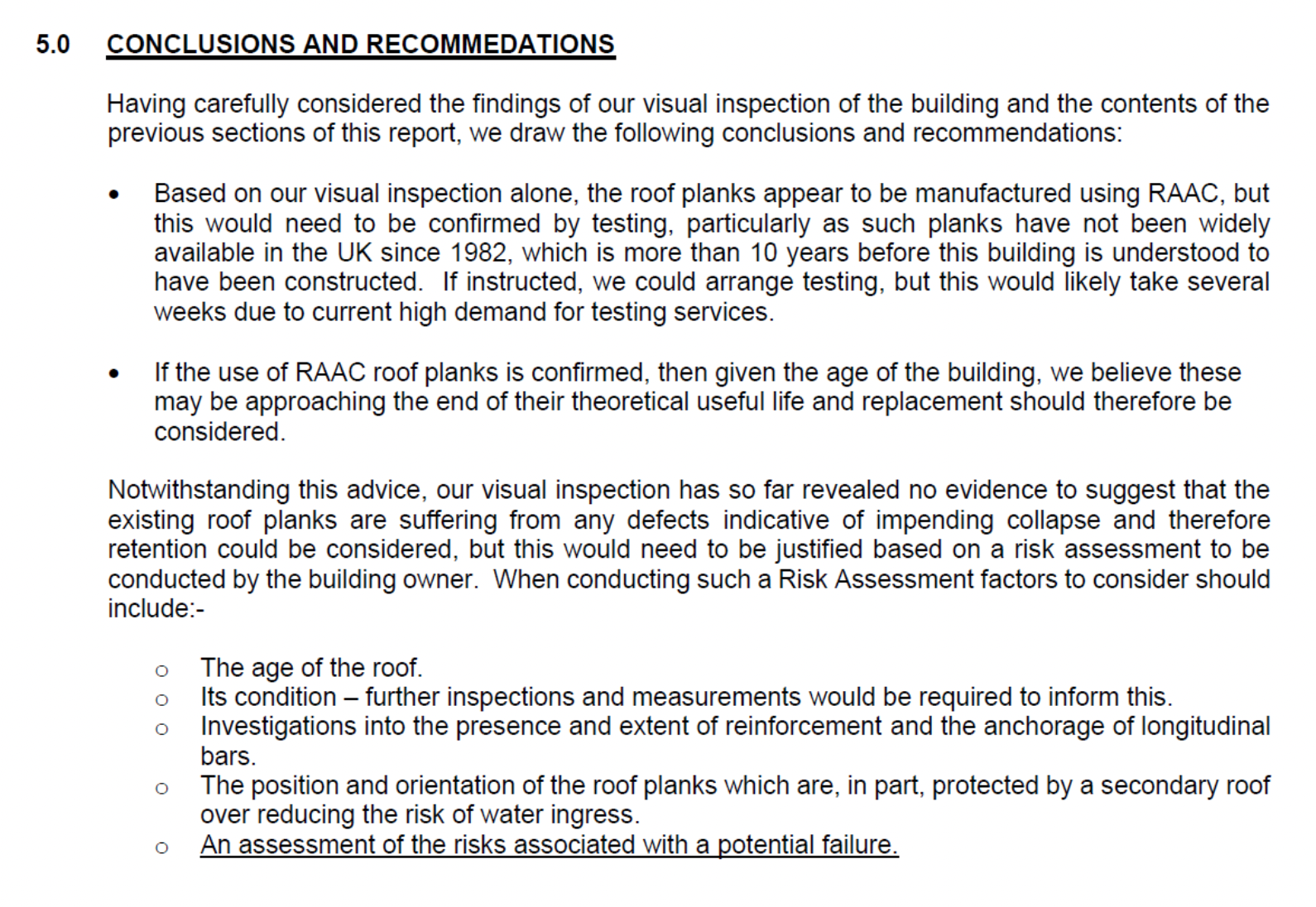
The trust has disclosed an engineer’s report and details of risk mitigation:
The trust gave this strange response to the request for details of risk management:
“In accordance with Regulation 12(4)(a) of the EIR, we can confirm that the Trust does not record/collate the above information.”
James Paget University Hospital NHS Foundation Trust
The trust has not responded at all despite being reminded.
Mid Cheshire Hospitals NHS Foundation Trust
The trust refused to disclose any information at all, pleading that it would require too much work to collate the documents:
“In order to comply with your request it would require an extensive manual review and cross reference of a vast number of reports, plans and protocols. In addition, some of this information is not held in a document format and would require additional work to collate it.”
If true, this is not reassuring evidence that it is on top of matters.
Mid Cheshire has now delayed its response to a request for internal review until 5 January 2023.
Could that be political water treading, pending an NHS England communication of some sort?
NHS Property Services
NHS Property Services did not answer at all despite being reminded.
However, a report on a property that it manages, Warren Farm Health Centre, which has an RAAC roof is in the public domain:
Dr Minh Alexander retired consultant psychiatrist 29 November 2022
The National Freedom To Speak Guardian’s Office (NGO) was not designed to help whistleblowers and patients but to help the government control the narrative about quality issues in the NHS.
It has no powers and what narrow remit it has, has been implemented in a mean and cynical way to deprive whistleblowers of any real support.
For example, its exclusion criteria are designed to abandon whistleblowers at the height of their conflict with employers – it tells whistleblowers who are in a legal dispute with their employers to come back when it is all over. This often takes years.
This is extraordinary cruelty and irresponsibility by the Office, which has been repeatedly meted out to highly distressed whistleblowers.
Through this withholding of help from NHS whistleblowers, the NGO has kicked many patients’ interests into the long grass
Patient safety matters should not wait for years at the National Guardian’s convenience.
For over two years now there have been incidents which call into question the National Guardian’s Office’s respect for whistleblower confidentiality and its diligence in keeping proper whistleblower cases files.
I had cause to challenge the Office twice this year.
Because of the NGO’s evasive and minimal answers, and failure to follow up on anomalies brought to its attention, I made an FOI request in September about its quality assurance processes.
In its responses, the NGO appears to have misled me about the existence of quality assurance processes for its whistleblower case records and protection of whistleblower confidentiality.
Bear in mind that failure to protect a whistleblower’s identity and confidentiality is now a criminal matter in some jurisdictions (for example, some EU countries, Australia, Ireland).
The National Guardian has personally also tried to prevent disclosure of accountability data by her Office through an implausible attempt to apply an exemption under FOIA that relates to prejudice to law enforcement.
The reasoning given is laughable. It claims that internal audits should not be published in case it puts people off audit.
This is also at complete variance to the National Guardian’s written guidance to NHS trusts, which advises regular audit of Freedom To Speak Up arrangements, and that audits should be“shared externally to support improvement elsewhere” !!!
The correspondence below gives the broad details of the National Guardian’s obfuscations.
BY EMAIL
Jayne Chidgey-Clarke
National Freedom To Speak Up Guardian
Care Quality Commission
28 November 2022
Dear Dr Chidgey-Clarke
Apparently misleading information provided by your Office and apparent lack of audit of case record keeping and confidentiality by your Office
I have received a response from your Office which suggests that it previously misled me by claiming that there had been two audits of the National Guardian’s case record handling and protection of whistleblowers’ confidentiality. It now appear these audits may not have taken place.
Time line of relevant events
On 13 September 2022, because of a number of events of concern, I asked you if your Office held data on audits undertaken about case record handling by your Office.
On 4 October your Office replied:
“Our office has had two audits since its inception in 2016, one in 2017/18 and one in 2020/21. We are due to undertake a further audit in the next financial year. Parts of these audits looked at risk management, including secure record management and confidentiality.”
On 7 October 2022 I asked you for copies of these two audits.
On 7 November your Office said it might not disclose the audit reports, and it was considering whether to apply Section 31 FOIA exemption (prejudice to law enforcement processes) on these grounds:
I was puzzled as your Office has no powers and only one statutory function as far as I am aware. I asked you to clarify which Section 31 categories of law enforcement you claimed applied.
On 15 November 2022 your Office wrote to:
1. Disclose what it claimed was the 2017/18 audit which included case records and confidentiality
What it disclosed was in fact a fragment from a document. The fragment contained no information about case record handling or confidentiality.
Your Office claimed that this was because Section 31 FOIA law enforcement, category “Health and Safety” applied:
“Internal audits are a way for organisations to test and improve their processes and improve their effectiveness and efficiency in performing their roles. A disclosure that would prejudice the effectiveness of future internal audits would therefore prejudice the future effectiveness and efficiency of the NGO in delivering on its purposes.
These prejudices would be likely to arise where disclosure of internal audit reports resulted in concern about the likely impact of disclosure of similar reports in the future. This would be likely to have the effect of prejudicing the candid and open approach of colleagues in their future interactions with auditors, and prejudicing the candid and open reporting of auditors findings in future reports. These prejudices to the effectiveness of the internal audit process would therefore be likely to prejudice the overall effectiveness and efficiency of the NGO in supporting Guardians in their work for the ultimate purpose of protecting the health and safety of people who speak up and patients.”
Your Office indicated that it had been your decision to apply Section 31 FOIA.
My reading of this is that your Office is implausibly claiming that the publication of audits will lead to your staff not contributing candidly to future audits, and you claim that this will threaten the health and safety of staff who speak up, and of patients.
I rejected this argument in my response to you of 17 November 2022:
Not least because your Office has issued written advice to NHS trusts, which urges them to regularly audit their Freedom To Speak Up arrangements, and that their audits should be “shared externally to support improvement elsewhere.”
I did not accept therefore that you genuinely believed there would be prejudice under Section 31 FOAI, as had been claimed.
On 25 November 2022 your Office wrote to say that the 2020/21 audit of record keeping and confidentiality practices which it claimed took place, did NOT take place.
It stated that the 2020/21 audit was about something else:
“However, please note that the 2021 audit was not around case handling and the handling of whistleblower confidentiality. The title of the audit is ‘Freedom to Speak Up Guardian role in arms-length bodies and regulators’.
It would therefore appear that your Office made an incorrect claim in its response of 4 October 2022, stating that there had been two audits of its case record keeping and handling of confidentiality, in 2017/18 and 2020/21.
1. I would very much appreciate an explanation of why I have been given conflicting information about whether your Office’s core processes, of case record keeping and handling of whistleblower confidentiality, have been audited. Please clarify if any such audits have ever been undertaken.
Please disclose the NGO risk register that was audited in 2017/18 as part of your reply, given your Office’s contention that the risk areas managed included record keeping and confidentiality.
I copy this correspondence to Ian Trenholm with respect to the regular accountability meetings that I believe he holds with you, and to Andrew Morris and Robert Francis as members of the National Guardian’s Accountability and Liaison Board.
You will be aware that as result of the recent responses by your Office, I wrote to Andrew asking if the Accountability and Liaison Board should review the National Guardian’s published values and mission, and its operations, to ensure better adherence to Nolan Principles of Accountability and Transparency.
I understand that Andrew gave you a copy of my letter and has forwarded it to Ian Trenholm for investigation of the specific issues.
2. I ask that the apparent inaccuracy of the 4 October 2022 response by your Office, claiming audits of case records and confidentiality had been undertaken – where none now appear to exist – be added as a matter for investigation.
3. If it is the case that your Office has NEVER undertaken any audit of its case record keeping and protection of whistleblowers’ confidentiality, despite Dr Campbell’s case and despite the other concerns raised, please advise if you will put this right and put in place an ongoing audit cycle.
Yours sincerely,
Dr Minh Alexander
Cc
Ian Trenholm CEO CQC
Andrew Morris Deputy Chair NHS England and Chair of National Guardian’s Accountability and Liaison Board
Robert Francis CQC NED and member of National Guardian’s Accountability and Liaison Board
UPDATE 9 DECEMBER 2022
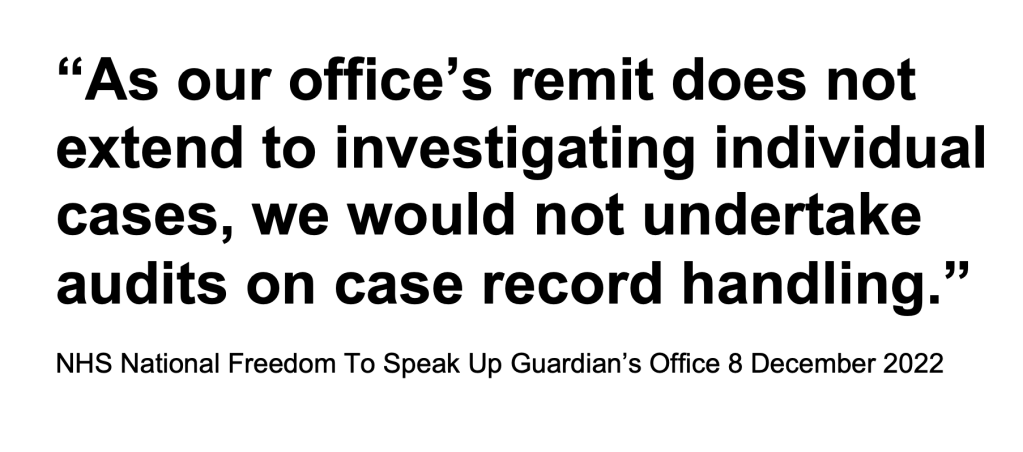
An exchange of correspondence with the National Guardian and her office has revealed that the claim that whistleblower case files had been audited on two occasions was not true.
The Office has now changed tack and ludicrously claims that it does not need to audit its whistleblower case files.
I have also repeated my request to Ian Trenholm CQC CEO for investigation of why the NGO gave me misleading and conflicting information.
PETITION
Please click and add your signature to this petition to reform UK whistleblowing law – whistleblowers protect us all but weak UK law leaves them wholly exposed, lets abusers off the hook and it is a threat to public safety.
By Dr Minh Alexander retired consultant psychiatrist 27 November 2022
Summary
CQC has a history of poor transparency about its staff surveys. In 2015, I asked for sight of CQC’s staff surveys. CQC subsequently announced that it would routinely publish future staff surveys. However, the data is not presented in a complete and accessible way. A current CQC staffing transparency page displays only results for 2018 and 2019. Results for 2020 appear to be missing from CQC’s website. It is possible that a survey was not even carried out in 2020. Results for the 2021 survey and surveys before 2018 could only be found only by a manual search of archived CQC board papers.
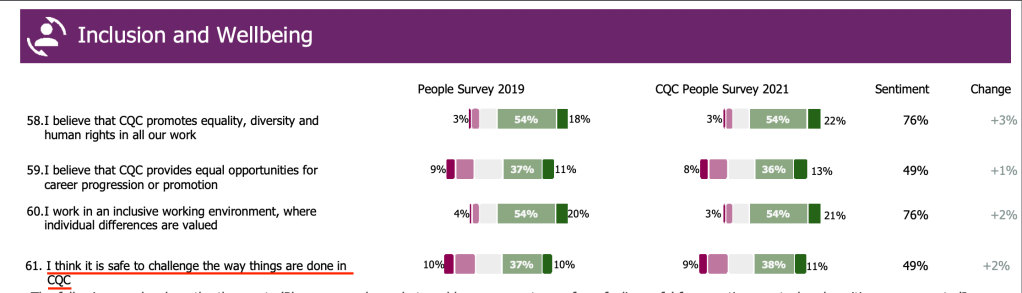
The 2021 CQC people survey shows:
Only 49% of CQC staff think it is safe to challenge the way CQC does things.
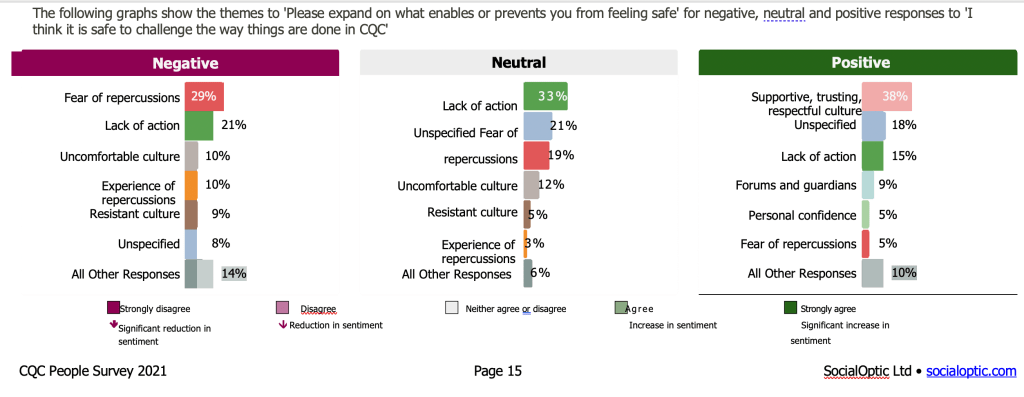
Of those who think it is not safe,
– 29% of these staff fear repercussions if they speak up
– 10% of these staff have actually experienced repercussions
The Care Quality Commission demands accountability from others, but CQC itself is often not accountable.
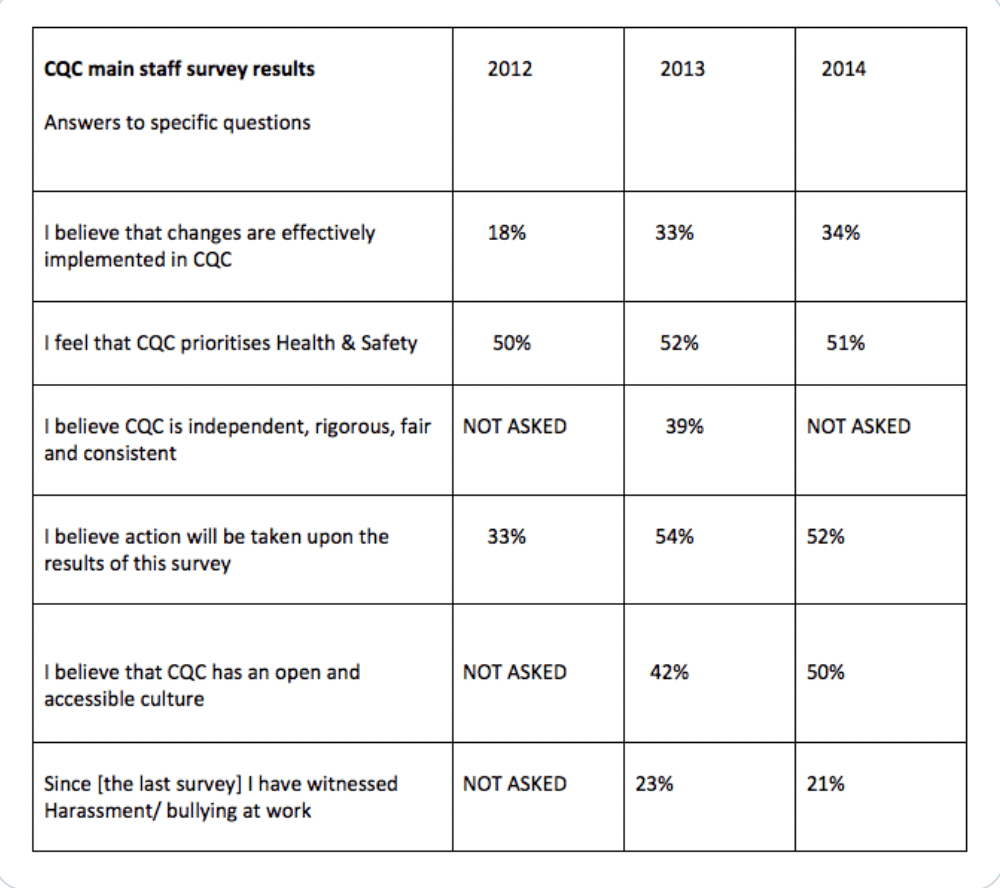
CQC employs over three thousand staff (FTE). The CQC staff surveys are of interest in that they have showed poor speaking up culture.
Some CQC “pulse” staff surveys, which are undertaken more frequently, are published but it seems the public dataset is not complete.
I could find no single place on the CQC website where all of CQC’s people survey reports are transparently gathered in one place.
I asked Ian Trenholm CQC CEO on 11 September 2022 if the missing CQC people survey reports from 2020 and 2021 would be published on the relevant CQC transparency web page.
He has still not answered, despite a reminder.
I have asked the Department of Health Permanent Secretary about his expectations of CQC transparency as an arms length body of the Department.
I have also trawled back through CQC’s archived board papers.
But I could find no 2020 CQC people survey report attached to CQC board papers.
It is possible that no survey was even carried out in 2020, as a survey in 2021 references 2019 results as a comparator, and not 2020.
The 2021 CQC people survey showed that less than half (49%) of CQC staff believe “it is safe to challenge the way things are done at CQC”:
Earlier CQC staff surveys, before 2018, also had to be located by a manual search of archived CQC board papers.
The scores on speaking up culture at CQC across the last six years have been poor overall, with less than half of staff feeling safe to challenge the status quo, but with a recent trend of improvement.
YEAR OF SURVEY
Percentage of staff replying affirmatively to CQC people survey question “I think it is safe to challenge the way things are done at CQC”
Please click and add your signature to this petition to reform UK whistleblowing law – whistleblowers protect us all but weak UK law leaves them wholly exposed, lets abusers off the hook and it is a threat to public safety.
Shockingly, this revealed that some NHS trusts were not bothering to collate data about long COVID in their staff.
A number of NHS trusts did not even bother to respond to the FOI request.
NHS Resolution holds some of the relevant data because NHS staff are starting to sue employers for COVID injuries.
But NHS Resolution said that it could not run a computer search for this data because long COVID is not assigned a specific injury code in its systems:
The Department of Health and Social Care callously said that it held no central data on NHS staff affected by long COVID, and crucially, that it had no intentions to collate this data:
The DHSC could not say authoritatively if the data was held elsewhere.
To fill in the gaps from Grace Pritchard’s FOI request last year, I have sent a similar request to all the trusts that did not bother to answer Grace’s questions.
I will post the replies below as they come in.
The first reply received has come from West London NHS Trust, which runs Broadmoor hospital:
The trust has disclosed 71 cases of long COVID in staff so far.
Of great concern, the trust has indicated that it has NOT been asked by NHS England for information on long COVID in its staff:
“5. Has NHS England asked the trust to specifically report data on how Long COVID has affected trust staff?
Response: No”
The concerted wilful blindness by oversight bodies is a great betrayal of the duty of care to frontline keyworkers.
I have written to Amanda Pritchard NHS England CEO, copied to the parliamentary Health and Social Care Committee, the Office of National Statistics, Health and Safety Executive and the Secretary of State.
BY EMAIL
Amanda Pritchard
CEO NHS England
24 November 2022
Dear Ms Pritchard,
Collation of data on long COVID injuries in NHS staff
I am writing to raise a concern that NHS England does not appear to be collating data on long COVID injuries suffered by NHS staff.
Please see below an FOI response from West London NHS Trust which records 71 staff affected by long COVID, and which indicates that the trust has not been asked by NHS England to report specific data on long COVID injuries amongst staff.
No central public body seems to be tracking the level of COVID injury amongst NHS staff.
ONS collates long COVID data by occupation, which allows a rough estimate, but it does not publish data by employer.
Some NHS Trusts are collecting data about long COVID in their staff.
NHS Resolution holds data on personal injury claims by NHS staff affected by long COVID, but says it has no specific code for long COVID and therefore cannot run a computer analysis.
This is a brief post to raise awareness that an interview of Mr Shyam Kumar about his whistleblowing experience at the Care Quality Commission will take place on 24 November 2022 and will be streamed:
Mr Shyam Kumar was appallingly treated by the CQC. An Employment Tribunal made decisive findings that he suffered detriment and was unfairly dismissed explicitly because he made public interest disclosures.
The ET rejected the CQC’s unpleasant dissembling during the ET process, which shockingly and falsely tried to cast him as a troublemaker and bully all through proceedings.
The details of the case and key documents can be found here:
On 11 September 2022 I asked Ian Trenholm, CQC’s CEO several questions about CQC’s and his own actions with regard to Mr Kumar’s case, and CQC’s whistleblowing governance.
Despite an indication from Trenholm’s Office that there would be a response, none has been issued, This is despite reminders.
These are just a few of the unanswered questions that I put to Ian Trenholm:
“8. Would you like to comment on the fact that only 47% of CQC staff replied affirmatively in the 2019 CQC staff survey to survey question number 62: “62. I think it is safe to challenge the way things are done in CQC”
In 2019, the NHS staff survey revealed that 71.7% of staff who participated stated that they would feel secure to raise a concern about unsafe clinical care.
Would you also like to comment on why only CQC staff surveys for 2018 and 2019 are published on this CQC webpage:
Were there no CQC staff surveys in 2020 and 2021, or is it that the survey was done in those years but the results were not published?
If CQC did carry out staff surveys in 2020 and 2021, will it now publish the results on this webpage?
Thank you.
Yours sincerely,
Minh
Dr Minh Alexander
Cc Ian Dilks CQC Chair, CQC press office”
Of concern, the CQC has been allowed to control an investigation into its own behaviour in Shyam Kumar’s case and a “selected” number of other cases of NHS trust whistleblowers.
There is no transparency about how the NHS trust cases have been selected – which gives rise to a concern that the selection is in CQC’s favour.
Of immense concern, the investigation terms of reference did NOT include any examination of CQC’s general whistleblowing governance. This is incomprehensible given:
CQC’s recurrent history of victimising its own whistleblowers
CQC’s appalling behaviour in Mr Kumar’s case
Surely when something so serious has happened, such as a regulatory cover up, it should be automatic to review the whole system which gave rise to it?
The exclusion of any examination of CQC’s general whistleblowing governance from the investigation is a slap in the face for CQC staff. Indeed, it is intimidatory, and possibly intended to be so.
But it is not so surprising given that CQC seems not to have accounted for its workforce relations in recent years.
Also, CQC recently unlawfully evaded an FOI request about its whistleblowing governance and failed to disclose internal reports by its own Freedom To Speak Up Guardian:
What is going on at CQC that requires such obfuscation?
No matter how much CQC tries to spin and manipulate its investigation to its advantage, a strong stink is still present.
PETITION
Please click and add your signature to this petition to reform UK whistleblowing law – whistleblowers protect us all but weak UK law leaves them wholly exposed, lets abusers off the hook and it is a threat to public safety.
Ian Trenholm CQC CEO was previously CEO of NHS Blood and Transplant 2014-2018. There have been several recent media revelations of bullying and Race discrimination at NHS Blood and Transplant, some of which reportedly took place when Trenholm was CEO.
Dr Minh Alexander retired consultant psychiatrist 12 November 2022
The UK is not good to its public servants.
ONS has just compiled basic data on armed forces veterans for the first time. It was astonishing that there were previously no such no official figures.
Frontline NHS staff injured by COVID19 whilst trying to keep services afloat despite government mismanagement of the pandemic, have been treated with disdain by the government..
NHS Resolution holds some of the central data on NHS staff long COVID cases, but says the data is not specifically coded to allow a computer search and analysis. See:
I asked the Department of Health and Social Care if it knew of any central data, and whether it held central data on long COVID-affected NHS staff.
The answer was ‘No’ and ‘No’.
Asked whether it intended to collate this data in future, the answer was also ‘No’.
The DHSC suggested I try ONS, but ONS only holds long COVID data by occupational group, and not by employer.
In the midst of an epic NHS workforce shortage, the DHSC knows of no central data about staff who have left the NHS due to long COVID:
“The numbers of NHS staff to date who have left their employment due to long covid
DHSC does not hold this information. Standard publications of information by NHS Digital does not record this level of detail and we are not aware of any specific NHS collections known to DHSC.”
The government’s treatment of key workers on the COVID frontlines is beyond words.
Will the unions campaign hard enough to ensure that COVID injured NHS staff are better treated and NHS staff are better protected from transmissible diseases?
It is not only a matter of justice but of public health. Unprotected workers are part of the engine of transmission and infection.
I have sent the DHSC’s FOI response to the COVID public inquiry.
By Dr Minh Alexander retired consultant psychiatrist 8 November 2022
The Care Quality Commission has a long history of politicisation, arbitrary regulatory behaviour and poor conduct towards whistleblowers, both its own and those from regulated bodies.
These extraordinarily omitted to explore CQC’s general handling of internal whistleblowing matters.
The ToR only focussed on a single internal CQC whistleblowing case and and examination of CQC’s conduct towards whistleblowers from regulated bodies:
“In relation to
(1) the protected disclosures made to the CQC by Mr Kumar; and
(2) a sample of whistleblowing concerns received by the CQC related to NHS Trusts, the size and date range of which is to be agreed:
The Review will:
(3) consider how CQC used these disclosures in its regulation of the relevant NHS Trusts and whether appropriate action was taken, taking account of all relevant factors including whether ethnicity played any part in the management of those disclosures; and
(4) make recommendations for improvement.
(5) Should the reviewer consider, during the course of the review, that these Terms of Reference require amendment, they will make a written proposal to that effect to the CQC Board for their consideration.”
This represents a defiant lack of apology to CQC’s workforce about its poor behaviour and it fails to ensure psychological safety for any current or future CQC whistleblowers.
It is possible of course that the above omission contains an implied threat to CQC’s workforce, and is a message that silence is preferred.
On 7 September 2022 Martin Morton social care whistleblower and former Social Services manager asked the CQC about its whistleblowing governance, via the What Do They Know website.
Included in his FOI request was a request for disclosure of the CQC’s own Freedom To Speak Up Guardian’s reports.
It was poor that CQC had not already published these reports. NHS trusts routinely publish these types of reports by their Freedom To Speak Up Guardians. That is to say, instead of being an exemplar as a regulator should, CQC is a governance laggard.
The CQC acknowledged the Morton FOI request and initially indicated that it would provide a response by 5 October 2022, the statutory deadline.
But CQC then changed course and stated to Martin Morton, on 6 October 2022, that it had encountered unspecified difficulties:
“Unfortunately, we are not currently able to respond to your request due to an unforeseen delay in processing your request.”
This was not a lawful response.
By 4 November 2022, as he had still not heard, Martin Morton prompted the CQC with the admonition that he would refer the matter to the ICO if necessary.
Faced with this, on 7 November 2022, the power-abusing CQC finally responded. This is the CQC’s response:
The response shows that in the course of five years, only 131 speaking up cases were raised with CQC’s own Freedom To Speak Up Guardian.
This is a small number of Speaking Up cases for a large organisation (over three thousand FTE workers), if compared to the reporting rate at NHS trusts.
Moreover in 2021/22, there was a sharp fall in CQC’s speaking up cases.
Is this because CQC’s victimisation of yet another of its own whistleblowers became public?
The CQC denies that any of the 131 speaking up cases featured detriment.
Most remarkably, in its FOI response of 7 November 2022, CQC continued to evade the request for copies of reports by its own, internal Freedom To Speak Up Guardian.
Instead of disclosing its own Freedom To Speak Up Guardian’s reports, CQC bizarrely pointed Martin Morton to published reports by the National Guardian.
What could CQC be hiding?
What content in the internal Freedom To Speak Up Guardian reports is CQC so reluctant to disclose?
This shabby organisational behaviour, whilst a review into CQC’s whistleblowing governance is underway, is hardly reassuring evidence of genuine remorse and learning.
Martin Morton continues to pursue the disclosure of the CQC Freedom To Speak Up Guardian reports.
In other news, CQC has tried to apply a patently invalid FOIA exemption to an FOI request by another whistleblower, but it retreated when challenged.
More coming soon about that misdemeanour.
PETITION
Please click and add your signature to this petition to reform UK whistleblowing law – whistleblowers protect us all but weak UK law leaves them wholly exposed, lets abusers off the hook and it is a threat to public safety.













{kind=link}
{kind=link}