By Dr Minh Alexander retired consultant psychiatrist 2 February 2023
Dame Marianne Griffiths is the former trust CEO and NHS insider picked by NHS England to conduct the investigation into the North East Ambulance service (NEAS) deaths scandal. It has been alleged that there have been breaches of coronial law, an extremely serious matter. It has also been alleged that NHS England has a conflict of interest because it did not respond appropriately to the whistleblowers who raised the concerns about NEAS.
A just published report by the Care Quality Commission from a recent inspection has acknowledged that NEAS crews were so pressurised they did not have time to restock between calls. This meant that they were attending some emergencies without all necessary life-saving drugs. BBC Newsnight has reported on this further scandal:
Of note, the CQC has downgraded the NEAS Well led domain to “Inadequate”

CQC stated in its report:
“Although staff were focused on the needs of patients receiving care, they did not always feel respected, supported and valued. Some staff told us they did not feel they could raise concerns without fear of blame or reprisal and the trust did not have effective systems to seek and act upon feedback from staff and other relevant persons.”
“Following this inspection, we served the trust with a notice under Section 29A of the Health and Social Care Act 2008. We told the trust it needed to make the following significant improvements: (1) to ensure governance systems operated effectively; (2) in listening, responding, and acting upon feedback from staff and other relevant persons”
Do CQC’s latest findings restrict NHS England’s and Griffiths’ room for manouevre?
There have been questions about Griffiths’ suitability.
Griffiths’ former trust at Sussex (an organisation arising from the merger of her trust Western Sussex Hospitals NHS Foundation Trust and Brighton and Sussex University Hospitals NHS Trust) was previously protected by the National Freedom To Speak Up Guardian who bizarrely and extraordinarily gave the trust board a free pass when trust whistleblowers asked for the National Guardian’s help. The then National Guardian Henrietta Hughes made up new rules by allowing Griffiths and her board a grace period to improve before conducting a review, and unsurprisingly later concluded that improvements had been made.
The dubious nature of this free pass was exposed when further signs of poor whistleblowing culture and patient risk and harm later arose at the trust, which even the CQC was forced to acknowledge.
Recent requests for information to University Hospitals Sussex NHS Foundation Trust have been met with resistance as to the number of recent whistleblowing cases at the trust.
Sussex claimed that it was unable to give any details about Employment Tribunal claims filed against the trust, including those filed under the jurisdiction code of public interest disclosure (whistleblowing). This was on the unlikely basis that there was no central file and that it would cost too much to retrieve the data manually.
“3-4. The specific information you are seeking relevant to qualifying public interest disclosures and employment tribunal claims is not held on a central administration system. Information related to this activity is recorded in a number of spreadsheet registers, but not to the level of detail that is required to answer these questions. Any effort to compile this information would require the manual audit of all individual claim files relevant to the periods outlined in your request.”
FOI response from University Hospitals Sussex 28 November 2022
The trust even claimed that it could not tell me how many of the ongoing ET cases were whistleblowing cases. I have written to the current trust CEO, formerly the Medical Director, to request at least this information.
A possible corollary of all this is that the trust has poor whistleblowing governance, by not troubling to learn from sentinel events such as being sued in the Employment Tribunal for whistleblowing detriment.
More likely in my view, University Hospitals Sussex NHS Foundation Trust is trying to draw a veil over sensitive and embarrassing matters whilst it gambles on settling and gagging its way out of current trouble.
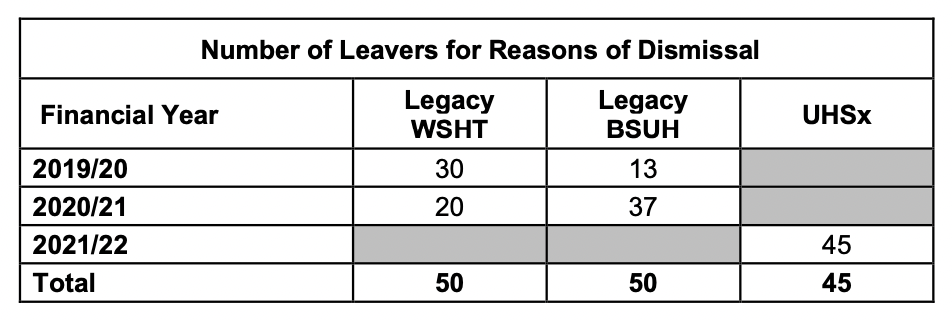
But the trust did admit to dismissing 145 staff over financial years 2019/20 to 2021/22.
I have asked for a breakdown of dismissals by staff group and of doctors in particular. I have also asked for the number of GMC referrals by the trust in the same period to see if there is internal consistency between decisions to dismiss and to refer.
University Hospitals Sussex NHS Foundation Trust uses the specialist employment law firm, Cater Leydon Millard, who are also used by Oxford University Hospitals.
Sussex has now admitted to spending at least £1,354500.13 on their services relating to 36 ET cases in the last five years:
“As at 04/01/2023, the Trust processed invoices dated between the following periods from Cater Leydon Millard:
- For the period between 2017/18 – 2020/21 for legacy Brighton and Sussex University Hospitals NHS Trust = £825,293.63
- For the period from 01/04/2021 to 30/11/2022 for University Hospitals Sussex NHS Foundation Trust = £529,206.50”
The trust refused to say how many settlement agreements Cater Leydon and Millard have handled for the trust and how many of the settlements contained gags, super-gags and non-disparagement clauses because – you’ve guessed it – there is no central record and it would cost too much to collate.
University Hospitals Sussex FOI response 30 January 2023 spend on Cater Leydon Millard solicitors
The trust CEO is supposed as a matter of good practice, under the terms of the Freedom To Speak Up Review, to take personal responsibility for reviewing and ensuring that settlement agreements are not excessively restrictive. I have asked him about the trust’s use of agreements.
I hope that journalists will keep a close eye on comings and goings at Sussex and ET listings.
And perhaps join the dots up, as appropriate, with proceedings at North East Ambulance Service.
I previously asked NHS England if it had carried out due diligence in appointing Griffiths to investigate the NEAS affair, including by checking that there were no ongoing whistleblowing matters spilling over from her time as CEO of Sussex. I asked:
“May I ask if NHS England has undertaken full due diligence into Marianne Griffiths’ past record on whistleblowing governance before appointing her to lead the NEAS investigation?
Has it satisfied itself that she is a Fit and Proper Person to adjudicate on matters of whistleblowing governance, and that there are no outstanding serious matters of alleged whistleblower suppression, failure to protect whistleblowers or harm to whistleblowers, that relate to her role as CEO of University Hospitals Sussex NHS Foundation Trust and its predecessor organisations?
For example, has NHSE satisfied itself that there are no formal, current internal trust processes such as grievances by whistleblowers or current litigation against the trust for whistleblower detriment, which relate to her tenure as trust CEO?
I ask as this seems a critical issue given that NEAS is accused of harming and trying to silence whistleblowers, and is proven to have attempted to gag them with unlawful NDAs.”
I received a non-reply on 8 December 2022:
“Dame Marianne is a retired NHS Chief Executive. Having never worked in the region, but with extensive knowledge of the NHS, Dame Marianne has the relevant experience to Chair this independent investigation.”
What might this tell us?
LETTER 2 FEBRUARY 2023 TO GEORGE FINDLAY CEO OF UNIVERSITY HOSPITALS SUSSEX NHSFT AND FORMER MEDICAL DIRECTOR
BY EMAIL
George Findlay
CEO University Hospitals Sussex NHS Foundation Trust
2 February 2023
Dear Dr Findlay,
FOI request – whistleblowing governance at University Hospitals Sussex NHS Foundation Trust
- I write to ask how many active Employment Tribunal cases are in progress against the trust, and how many of these include a claim filed under the jurisdiction code of Public Interest Disclosure (whistleblowing). I asked this previously as part of a wider FOI request, but the trust advised that checking files for details of ET claims would be too time consuming.
I am sure that checking files on just a few active cases would be a much quicker task.
- I would also be grateful if the trust could also disclose, drawing from the digital data submitted to NHS Digital:
- The number of dismissals for any reason by staff group for each of the financial years
2019/20
2020/21
2021/22
- The total number of medical staff dismissed in the period 1 April 2019 to 31 March 2022.
- The total number of doctors referred to the GMC by the trust in the period 1 April 2019 to 31 March 2022.
- I understand that the trust does not keep a central record of its settlement agreements and cannot give an exact overview of how many non-disclosure agreements and non-disparagement clauses that it has applied.
One of the recommendations of the report of the NHS Freedom To Speak Up Review was that NHS Trust Chief Executives should take personal responsibility for reviewing all settlement agreements made by their trusts. This is to ensure that they are not excessively restrictive.
If you are personally overseeing settlement agreements, could you possibly give a brief overview as CEO of the settlement agreements used by your trust and whether they typically contain:
- Clauses which require signatories to keep the existence of settlements agreements secret
- Clauses which require signatories to keep the contents of settlement agreements secret
- Clauses which require signatories not to disparage each other
And could you kindly supply a template of the settlement agreement commonly used by your trust, or better still, a redacted copy of the most recently applied settlement agreement which shows the restrictive clauses used?
Many thanks and best wishes,
Cc
Tom Grimes NHS England Lead for Whistleblowing
| Past lack of transparency by University Hospitals Sussex NHS Foundation Trust University Hospitals Sussex NHS Foundation Trust was previously criticised for not releasing the unredacted version of a 2019 Royal College of Surgeon’s report, which was conducted during Marianne Griffith’s tenure as Chief Executive. Hospitals Sussex urged to release review findings It was only released under FOI in heavily redacted form. Reportedly, “All issues and recommendations were obscured, with only positive feedback disclosed.” “The trust chose to reveal the number of incidents resulting in “no harm” and “low” harm, but redacted the number of incidents resulting in “moderate” and “severe” harm.” Let us hope that this will not be the approach taken to NEAS. But journalists may wish to further probe the trust’s denial: “The trust said the review of its neurosurgery department “did not highlight any safety concerns”, given the above propensity to selective comms. |
RELATED MATTERS
Staff suicides at West Midlands Ambulance Service NHS Foundation Trust
The National Guardian’s Office does not put a blue light on for ambulance staff
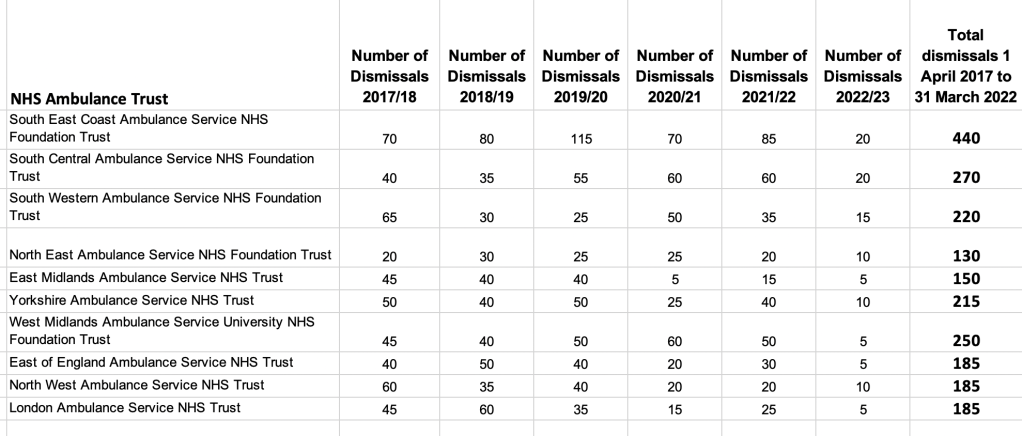
Dismissals by NHS trusts: Ambulance trusts dismiss disproportionately more staff