Dr Minh Alexander retired consultant psychiatrist 21 April 2023
Care Quality Commission Regulation 12 provides a facility for unsafe provider organisations to be investigated for failures to provide safe care and ultimately to be prosecuted.
Like many others, I fail to see the utility of fining cash strapped public bodies, which only hurts patients as the end users.
However, the regulation exists and CQC is obliged to apply it where appropriate and importantly, to investigate where there is evidence of organisational failure.
University Hospitals Birmingham NHS Foundation Trust staff have been whistleblowing to UHB management and to the CQC about unsafe levels of staffing for a long time.
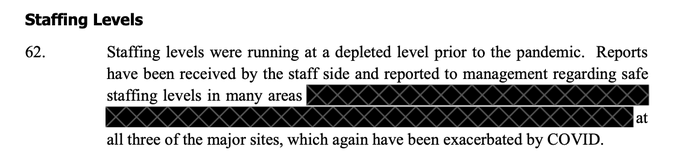
UNISON sent a dossier to CQC in July 2021which revealed that UHB staff across all three sites had been raising concerns with trust managers about “depleted” levels of staffing since before the pandemic.
CQC did not publicly acknowledge the existence of this dossier.
The BBC revealed its existence in recent months as part of the coverage of the UHB scandal.
CQC claimed that it undertook the inspection because:
“We conducted an urgent, unannounced inspection of the full medical care core service due to a number of concerns raised by patients and their families around the care and treatment they had received.”
The reports from this latest CQC inspection was published on 19 April 2023.
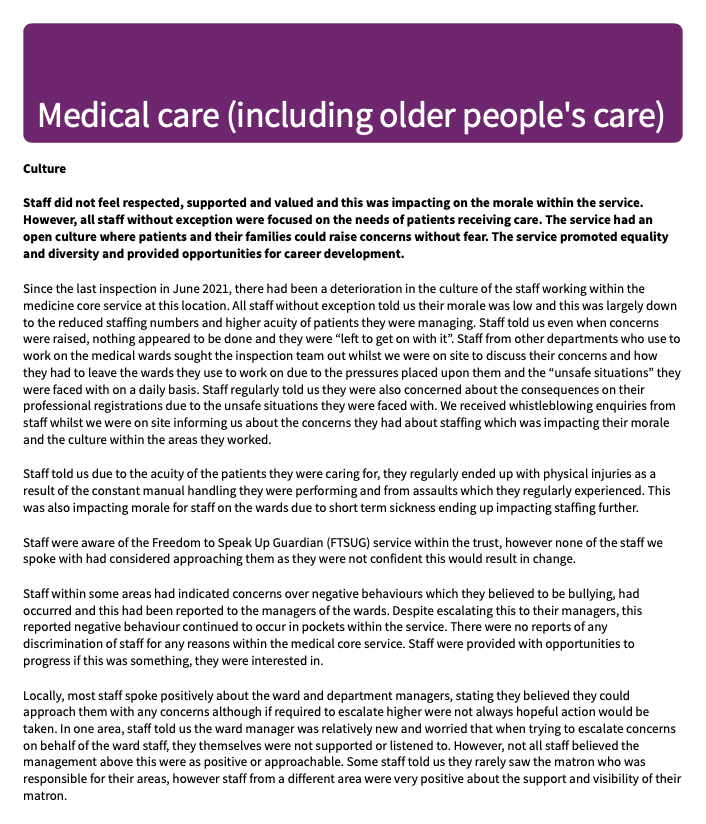
The report from the Good Hope Hospital inspection was damning on management failure to respond to concerns, in that staff had stopped using the internal route for raising concerns because of zero expectation that managers who act upon them:
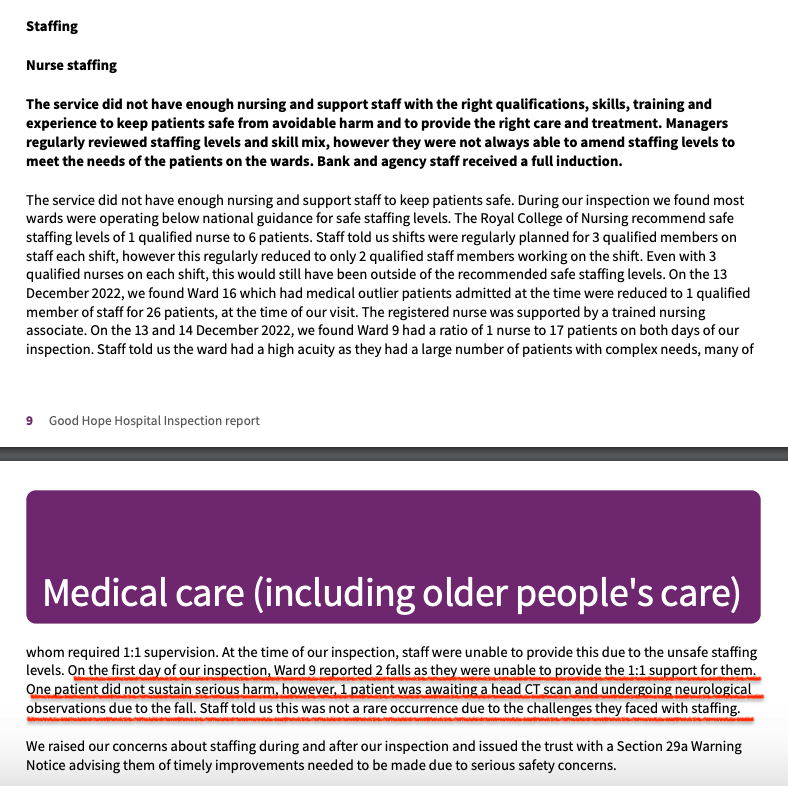
Deeply concerning was a CQC finding of very unsafe levels of staffing.
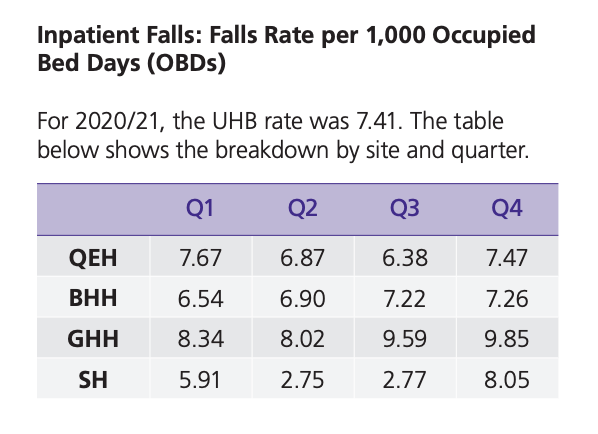
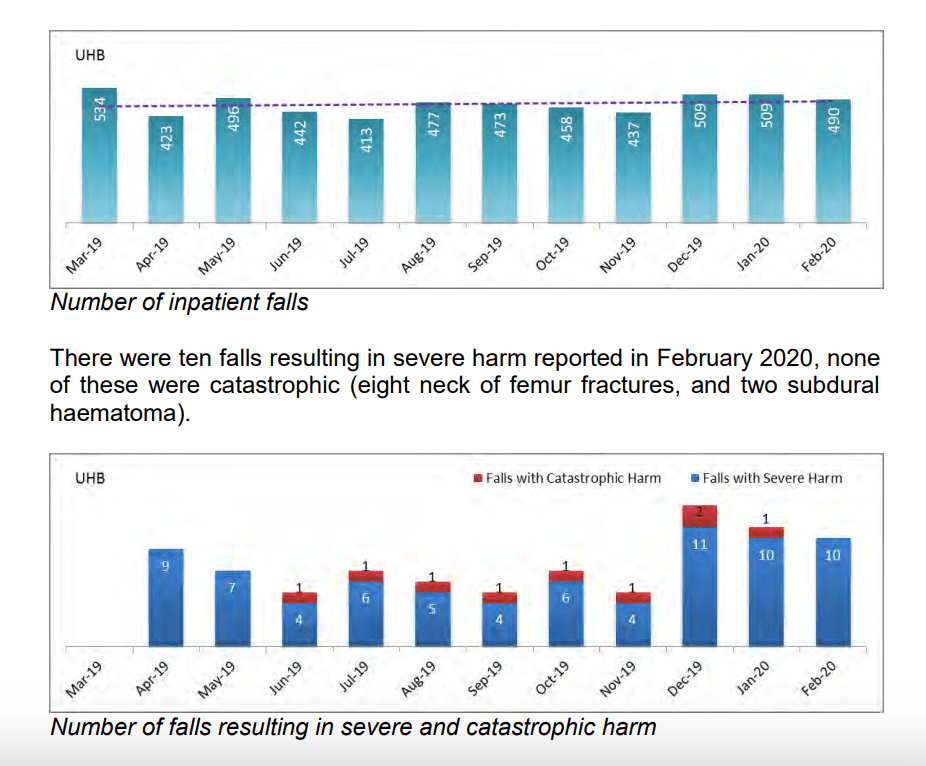
Related to this, patients suffered falls and suffered injuries DURING the CQC inspection:
The CQC issued a Section 29A improvement notice with respect to the unsafe levels of staffing:
The former NHS England Serious Incident Framework used this categorisation for degrees of harm:
Whilst neck of femur fractures may not result in immediate death, and may therefore sometimes receive a short term categorisation of “severe” rather than “catastrophic” harm, such fractures in older people may trigger a downwards spiral that eventually leads to death:
Given that there have been both longstanding understaffing at UHB AND evidence of regular, serious harm from falls, should the CQC be investigating UHB for Regulation 12 breaches, and not just issuing an improvement notice?
Indeed, the falls related injuries are not the only evidence of possible Regulation 12 breaches at UHB.
With the issue of the CQC warning notice, are we witness more to spectacle, than meaningful regulatory action?
Have harmed UHB patients and their families tried to raise concerns with CQC, but been fobbed off with the classic but misleading CQC refrain “We have no remit to investigate individual complaints”?
Reframing concerns as “complaints” blocks whistleblowers, patients and families, and CQC often does not disclose that it does have a remit to investigate incidents of avoidable harm under Regulation 12.
Dr Minh Alexander retired consultant psychiatrist 17 April 2023
A key matter which triggered BBC Newsnight reportage of the governance failings at University Hospitals Birmingham NHS Foundation Trust was the scandalous whistleblowing case of Tristan Reuser, ophthalmic surgeon.
Mr Reuser was seriously mistreated and unfairly dismissed.
One of the key issues was that he was unfairly suspended based on an unfounded allegation that the ET determined that Clive Ryder Deputy Medical Director and David Rosser Medical Director, later Chief Executive, knew or ought to have known was false.
A related, central issue was that the trust failed to show Tristan Reuser correspondence from an NHS agency called the National Clinical Assessment Service, NCAS (now called Practitioners Performance Advice, PPA), which has a statutory role in advising employers on the suspension of and disciplinary action against doctors.
The withheld correspondence would have revealed that his suspension was triggered on a false premise.
The MHPS rules of procedures require NHS employers to show referred doctors all correspondence relating to their case.
UHB not only failed to show Tristan Reuser the NCAS correspondence that he was entitled to see, but when Tristan Reuser asked for his personal data, UHB failed to disclose the NCAS correspondence.
The resistance to share the NCAS correspondence persisted into Employment Tribunal proceedings when UHB failed to disclose material documents even in the legal disclosure process, incurring the judge’s displeasure and a £20,000 costs award against the trust.
The effect of UHB’s secrecy was that misleading information supplied to NCAS by Clive Ryder UHB deputy medical director, to justify Tristan Reuser’s suspension, was hidden.
How could this have happened in a process that is supposedly safeguarded?
An MHPS “Designated Board Member” was allocated to Tristan Reuser’s case: Jon Glasby, non executive director, who was appointed as the UHB Independent Senior Director under Jacqui Smith’s tenure.
The Designated Board Member’s role in MHPS is to ensure fair play and that the accused doctor is not “incarcerated” by default through an excessively drawn out process.
“The Chairman of the Board must designate a non-executive member “the designated member” to oversee the case and ensure that momentum is maintained.”
“Role of designated Board member
13. Representations may be made to the designated Board member in regard to exclusion, or investigation of a case if these are not provided for by the NHS body’s grievance procedures. The designated Board member must also ensure, among other matters, that time frames for investigation or exclusion are consistent with the principles of Article 6 of the European Convention on Human Rights (which, broadly speaking, sets out the framework of the rights to a fair trial).”
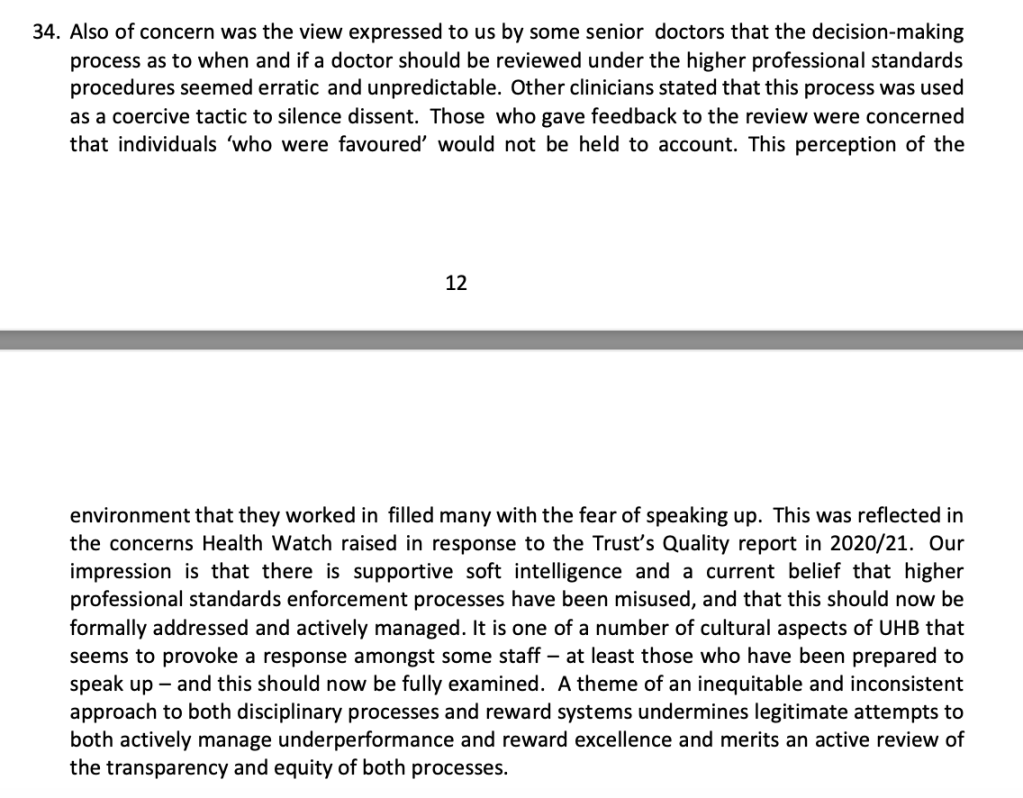
During his phase one investigation at UHB, Mike Bewick was told that the UHB consultant body had raised concerns with the UHB board about cronyism at all levels of medical management.
He was also told of staff perceptions of arbitrary discipline at the trust.
As a former Deputy Medical Director himself, he would surely understand the requirements of MHPS and the significance of any breaches of procedure.
In his report, Bewick stated that he considered that the findings of the Employment Tribunal in Reuser v UHB and the GMC’s warning to David Rosser called into question David Rosser’s fitness for a senior leadership role:
“31. In our opinion, statements made by the GMC and the Employment Tribunal were extremely serious and brought into question DR’s suitability for senior leadership roles.”
It follows that Rosser’s critical actions as a medical director, in suspending and disciplining doctors, should also be reviewed.
As part of Bewick’s investigation, could he not have called up data on UHB’s use of MHPS and adherence to the rules of procedure?
There was anecdote in Bewick’s report about this, but no hard data, making it inconclusive:
Dragging out the review process may benefit the UHB gravy train but not staff and patients.
In the meantime, I have asked the interim UHB Chair to consider some basic, urgent checks.
I have also suggested that when MHPS is applied at UHB, doctors should be clearly informed of their right to access case correspondence.
BY EMAIL
Yve Buckland
Interim Chair
University Hospitals Birmingham NHS Foundation Trust
17 April 2023
Dear Yve,
Failures of MHPS process
I do not know how familiar you are with the NHS conduct/capability process for disciplining doctors, Maintaining High Professional Standards in the Modern NHS (MHPS), but it has rules of procedure with supposed safeguards.
These failed entirely in the case of Tristan Reuser, UHB whistleblower.
One of the MHPS rules is that doctors who are subject to these procedures must be allowed to see all correspondence about their case, to fully enable them to reply to all allegations.
UHB not only failed to ensure this access to case correspondence, but persistently withheld crucial correspondence from Mr Reuser. This withheld correspondence showed that Clive Ryder Deputy Medical Director gave misleading information to an NHS body the National Clinical Assessment Service, as part of the procedure of triggering suspension under MHPS rules. This was later criticised by the Employment Tribunal as “beyond inaccurate”.
Was it really the case that the then deputy medical, the medical director, the director of human resources and the MHPS designated board member who should have ensured fair play (Jon Glasby), all experienced directors, were not aware that Mr Reuser should have been given sight of his MHPS case correspondence?
My concern now is how many other UHB doctors have been disadvantaged in this way?
How many staff are currently being disadvantaged in this way?
This document lists the many alleged failings that may land a doctor in hot water. But it does not say much about the organisation’s responsibilities to treat an accused doctor fairly.
Importantly, I cannot see that the policy says anything about an accused doctor’s rights to see all case correspondence.
The UHB policy cross references the national MHPS framework but gives no link.
It would empower staff if UHB actively gives access to the detailed rules of procedure. MHPS is arguably a contractual matter, and a matter of rights.
The national framework is a lengthy document and the information about the right to see case correspondence is brief and easily missed.
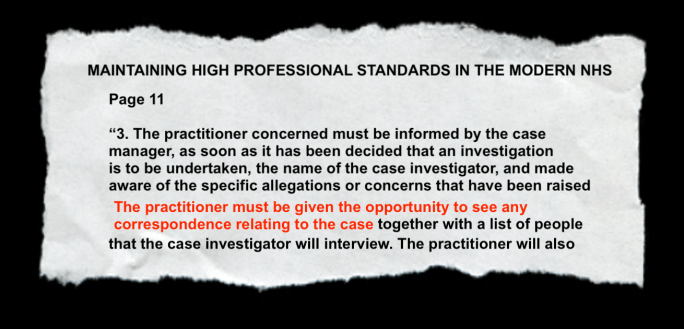
Page 11 of the national MHPS framework:
“3. The practitioner concerned must be informed in writing by the case manager, as soon as it has been decided, that an investigation is to be undertaken, the name of the case investigator and made aware of the specific allegations or concerns that have been raised. The practitioner must be given the opportunity to see any correspondence relating to the case together with a list of the people that the case investigator will interview. The practitioner must also be afforded the opportunity to put their view of events to the case investigator and given the opportunity to be accompanied.”
It would be helpful if the local UHB policy spells out clearly the right of access to case correspondence.
Does UHB need to rapidly audit adherence to basic MHPS standards, based on audit standards co-produced with staffside, to ensure that no further serious harm to individuals is currently unfolding, and that any other serious harm that has taken place besides Reuser v UHB is corrected?
There was a delay in UHB responding, despite my chasing. This was later explained as a switch between email accounts by the interim Chair which led to some email being unnoticed.
In the meantime, David Melbourne the CEO of Birmingham and Solihull ICB emphasised to local councillors at the Joint Health Overview and Scrutiny Committee that the media had got their figures wrong.
This was very distasteful given that the false information had been supplied by UHB.
Remarks on page 12 of Bewick’s report dovetail with the tone of Melbourne’s comments to JHOSC:
It is perplexing as to why Bewick focussed on the cases that DID result in GMC action, but omitted to discuss the cases which did NOT result in any GMC action.
One would have thought that all cases would have been counted in any check of accuracy.
And it is the cases that did not result in any GMC action that were of most concern in terms of UHB’s governance.
Yesterday, UHB finally responded through its Chief Legal Officer to my requests for the record to be corrected.
This is the response:
RESPONSE BY DAVID BURBRIDGE 13 APRIL 2023
Dear Dr Alexander
Please find below a response to your email to Dame Yve Buckland, dated 29 March.
For the period 1 April 2012 to 31 March 2022:
– How many doctors the trust referred to the GMC ?
At UHB (prior to and post the merger with Heart of England NHS Foundation Trust (“HEFT”)) there were 22 referrals At HEFT (prior to the merger with UHB) there were 16 (3 of these are dated just after the date of merger 1.4.2018, but are attributed to HEFT – we believe this may be because there was contact before the change of RO)
– How many of these referrals were signed off by the medical director?
At UHB 14/22, the remainder were signed off by Deputy Medical Director or acting Medical Director At HEFT 6/16 were signed off by the Medical Director and the remainder were by Deputy or Associate Medical Directors.
– How many of these referrals resulted in no further action by the GMC?
UHB – 4 were concluded at triage, 7 were investigated and concluded with no action, 11 were subject to advice, warning, undertakings, suspension or erasure HEFT – 3 were concluded at triage, 4 were investigated and concluded with no action, 9 were subject to advice, warning, undertakings, suspension or erasure
– How many doctors died whilst under GMC investigation or monitoring? None
– How many doctors died by suicide whilst under GMC investigation or monitoring? None Regards
David Burbridge Chief Legal Officer
That is to say, there were a total of 38 GMC referrals in the ten year period, 18 of which were either dropped (or “concluded” as UHB put it) at triage or which resulted in no further action by the GMC.
For all the protestations and smoke and mirrors, we still have best part of a score of doctors who were possibly referred to the GMC when this was apparently not essential.
GMC referrals are a serious business. Could alternatives have sufficed? Were any of these doctors referred out of careless misuse of power, or as a punishment or intimidation, to silence them?
Any further reviews of UHB should look carefully at these eighteen GMC referrals.
In the meantime, I have asked UHB to disclose how many of these eighteen GMC referrals which were dropped at triage, or which resulted in no further action by the GMC, were signed off by either David Rosser or Clive Ryder.
This is because both of these senior doctors were criticised by the Employment Tribunal for their actions in the whistleblowing case of surgeon Tristan Reuser, for acts which included supplying inaccurate information to NCAS (now PPA), suspending Mr Reuser on a basis which they knew or ought to have known was unfounded, and misleading the GMC in the course of referring Mr Reuser.
It is also because David Rosser made a GMC referral on a whistleblower, Mr Reuser, which ended in no further action being taken by the GMC.
It is also because of a concern raised by the consultant body about cronyism at all levels of medical management at UHB, and because of a reported staff perception of arbitrary application of discipline.
“It became clear that both Dr Ryder and Dr Rosser knew, or ought to have known, that it was unfounded before the exclusion was even put in place. That only came to light from documents which had not been disclosed but which were obtained by Mr Reuser through a subject access request (SAR).
No action was taken against Mr Negi in relation to what appeared to be a false allegation. This, coupled with my more detailed findings in relation to the exclusion earlier in this judgment, potentially suggests a level of bias and collusion at a senior management level against the claimant. Again, at the very least, it suggests a very serious lack of due care and attention to an important matter.”
“Dr Rosser was not sufficiently independent. There is a strong suspicion of bias given his approval of the exclusion on grounds he ought to have known were false. This appears further confirmed by the omissions and unjustifiably strong language of the GMC referral.”
UHB may object to my enquiry on grounds of personal data and confidentiality.
But the public interest and the seniority of the individuals in question are counter-arguments against such objection.
And for genuine culture change, as opposed to the PR and news management that NHS England and its hangers on will throw at this situation, truth and transparency are a pre-requisite.
Dr Minh Alexander retired consultant psychiatrist 11 April 2023
Mike Bewick’s rapid review of clinical safety at University Hospitals Birmingham NHS Foundation Trust was strangely silent on patient complaints, and so were the related statements by the external reference group and the Chair of Healthwatch Birmingham:
Consequently, I asked Healthwatch Birmingham if it collated and published data on concerns and complaints received from the public about UHB.
The response was a little reluctant, but Healthwatch Birmingham eventually revealed that it did, and that this data was sent to regulators and commissioners in a confidential, quarterly report.
I have now written to Healthwatch Birmingham’s Chair to ask that the data relating to UHB is transparently published in view of the great public interest.
Frankly, such data should be routinely published in view of Healthwatch’s purported role as champion of the public interest.
LETTER TO RICHARD BURDEN, CHAIR OF HEALTHWATCH BIMRINGHAM
BY EMAIL
Richard Burden
Chair of Healthwatch Birmingham
11 April 2023
Dear Richard,
Public access to complaints and concerns data about UHB that is held by Healthwatch Birmingham
I asked Healthwatch Birmingham via a Twitter conversation if it collated data on concerns and complaints from the public about local NHS services, with particular respect to UHB, for obvious reasons.
HW Birmingham initially directed me to the online feedback page of its website:
When I asked about correspondence received by HW Birmingham from the public regarding complaints and concerns, and whether this generated any summarised data and reports, HW Birmingham replied that correspondence would not be published because it was confidential.
After I pressed the point about summarised data, HW Birmingham indicated that anonymised data about concerns received is sent to regulators and commissioners in quarterly reports, which are confidential.
“Anonymised data is shared with regulators & commissioners in a confidential quarterly report. We also have avenues for directly raising concerns with services. Pls email info@healthwatchbirmingham.co.uk if you wish to discuss further. Thanks.”
I wonder if in view of the clear and current public interest in University Hospitals Birmingham NHS Foundation Trust, and the extraordinary omission of any patient complaints data from Mike Bewick’s phase one rapid review on clinical safety at UHB, whether Healthwatch Birmingham should now publish its anonymised data on all concerns and complaints received about UHB.
I can see no objection on grounds of confidentiality and privacy if the data is anonymised and aggregated.
A series of such data going back over years would be valuable in helping to set the current concerns about UHB’s culture, clinical performance and safety into context.
Furthermore, Healthwatch Birmingham’s dataset can be argued to be a more independent dataset that has not been controlled by the UHB board, and may have added value in this respect.
With best wishes,
Minh
Dr Minh Alexander
Cc
Birmingham and Solihull Joint Health Overview and Scrutiny Committee
The Parliamentary and Health Service Ombudsman triggered the multiagency Emerging Concerns Protocol in August 2022 because of concerns about poor culture, leadership and lack of learning from complaints and incidents at UHB.
PHSO expected to contribute to Bewick’s review but claimed it had been excluded, and this revelation was broadcast by BBC Newsnight. The transcript of Newsnight’s interview with Rob Behrens can found here:
Extraordinarily, Bewick’s rapid review of UHB safety indeed omitted any mention of evidence from PHSO or of the PHSO’s concerns.
Bewick and his small crew of fellow investigators, a paediatrician and a “chartered secretary and governance expert” also did not mention patient complaints in their report.
Is this because raising the spectre of patient complaints would inevitably remind the public and NHS staff of the missing PHSO data?
How can a report on clinical safety ignore patient complaints about clinical care?
Astonishingly, despite ignoring this core data on patient experience and outcomes, both from trust records and from the PHSO, Bewick and co concluded that UHB was “safe” overall.
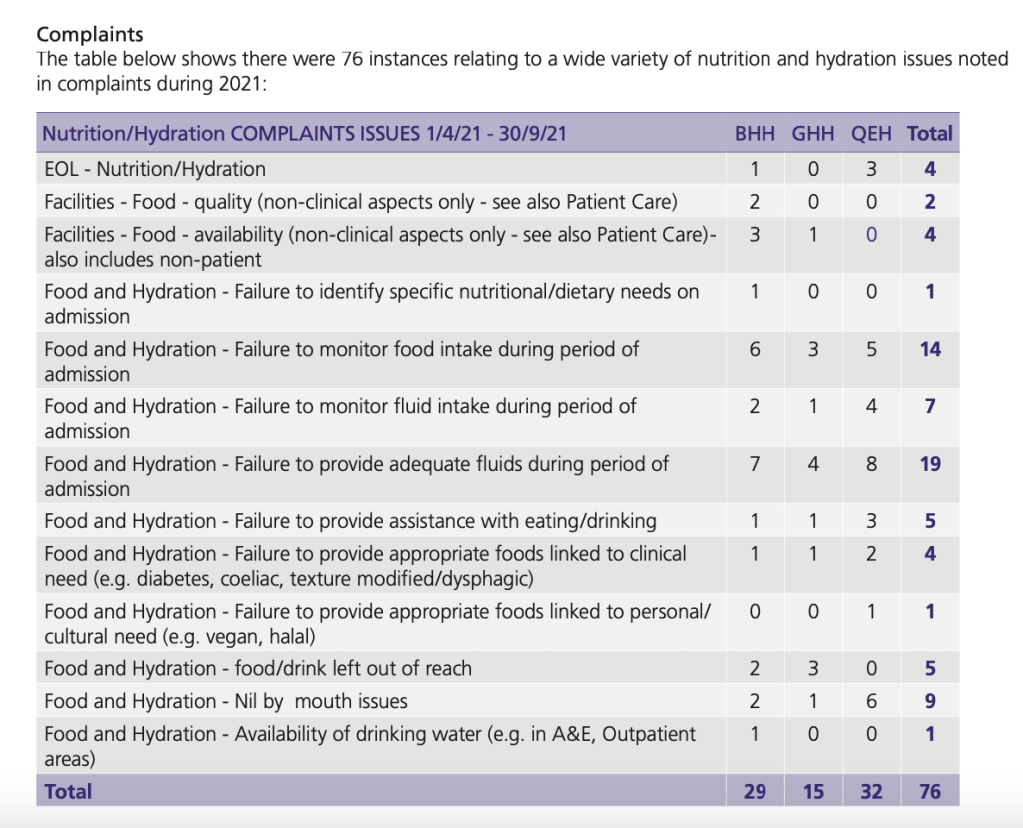
But under the subject of “Improving nutrition and hydration”, the trust did reveal more details of relevant complaints.
As you can see from the above table, these included failures of very basic care such as not monitoring food or fluid intake, not providing assistance with eating and drinking and leaving food and drink out of reach.
The UHB complaints about hydration and nutrition are consistent with this week’s news coverage. UHB families’ and patients’ reported food and drink being left out of reach and patients being left in their own waste:
With those caveats in mind, the data published suggested that complaints about clinical care comprised about half of the complaints.
YEAR
Total number of complaints from patients
% of complaints that related to clinical care
2013/14
956
52.3% (n = 500)
2014/15
1044
51% (n = 533)
2015/16
1075
48.5% (n = 522)
2016/17
949
41.5% (n = 394)
Looking at an overlapping and better-defined dataset from NHS Digital, data on written complaints in the English NHS, shows that complaints about clinical treatment accounted for less than a third of complaints:
YEAR
TOTAL NUMBER OF COMPLAINTS ABOUT CLINICAL TREATMENT
% OF ALL COMPLAINTS THAT WERE ABOUT CLINICAL TREATMENT
2015/16
59,678
32.0%
2016/17
51,145
26.7%
2017/18
48,904
26.2%
2018/19
53,084
27.5%
2019/20
53,018
27.1%
2020/21
40,854
26.9%
A proper interrogation of UHB’s complaints data and an examination of UHB’s response to complaints is needed.
Journalists might be interested to pursue the records relating to this event in 2021/22, as described in the foreword by David Rosser ex UHB CEO, in the trust’s quality account for that financial year:
“A wide range of omissions in care were reviewed in detail during 2021/22 at the Executive Care Omissions Root Cause Analysis (RCA) meetings chaired by the Chief Executive. Cases are selected for review from a range of sources including serious incidents, serious complaints, IT incidents, infection incidents and cross-divisional issues.”
Surely Bewick could hardly have been hampered by poor data systems as UHB’s former CEO and current CMO are ardent fans of digital health and data.
Rosser’s foreword in the 2021/22 proclaimed:
“Data quality and timeliness of data are fundamental aspects of UHB’s management of quality. Data is provided to clinical and managerial teams as close to real-time as possible through various means such as the Trust’s digital Clinical Dashboard. Information is subject to regular review and challenge at specialty, divisional and Trust levels by the Clinical Quality Monitoring Group, Care Quality Group and Board of Directors for example.”
The fact that Bewick was prepared to declare UHB safe without any evident discussion of UHB complaints data suggests two possibilities.
Either he decided it would be unfavourable to examine or report on complaints, or he did not consider patient experience or patient voice important when assessing patient safety.
Either option would suggest he should not be directing the UHB reviews.
And who directed Bewick?
It strikes me that the only NHS England or the Department of Health would have the power to ensure the exclusion of PHSO’s evidence from Bewick’s review.
Such high-level interference only additionally points to the need for a judge led inquiry with powers to compel evidence, as well as to protect witnesses and ungag silenced staff and former staff.
I think we should brace for more misdirection.
UPDATE 12 MAY 2023
I obtained data on the number of concerns raised by the public with Birmingham and Solihull Healthwatch. The data shows marked and continuing escalation beginning in 2021. Healthwatch disclosed under FOIA that it started meeting with the CQC on the basis of this sharp escalation in concerns and that these meetings continue:
I have sent the Healthwatch data to Bewick and suggested that he should examine and report on UHB’s patient complaint data, with both quantitative and qualitative analysis.
RELATED ITEMS
This is a statement of 4 April 2023 by the external reference group on Bewick’s reviews, which criticised some of the gaps in Bewick’s report:
However, this statement also did not mention the PHSO’s exclusion from Bewick’s review or the absence of any reference to patient complaints.
The latter is a little surprising given that Richard Burden former Labour MP is the current Chair of Healthwatch Birmingham and Solihull and a member of this external reference group.
A statement by Burden on 28 March mentioned the PHSO but not Bewick’s omission of patient complaints.
This post shares FOI data which showed that UHB and the ICB colluded to give a false impression that David Rosser had left UHB when he in fact remained an employee of the trust, and was just temporarily parked at the ICB, answering to the ICB’s CEO.
By Dr Minh Alexander retired consultant psychiatrist 6 April 2023
Summary: CQC has once more given scant regard to Employment Tribunal findings of gross whistleblower reprisal in the case of Dr Ambreen Malik and found a provider organisation, Cygnet Health Care, compliant under CQC Regulation 5 Fit and Proper Persons. CQC continues to make claims that it cannot make judgments about the fitness of individuals, and makes unsustainable regulatory judgments about process without taking into account the character of individuals of concern. CQC steadfastly and disingenuously claims that it has no remit to assess the fitness of individuals, despite Regulation 5 requiring that directors are of “good character”. It is also despite the fact that CQC’s own internal guidance states clearly that CQC has powers to take action against providers who have unfit directors, which of course is predicated on CQC making an assessment of individual fitness. CQC also provides almost no details about how it reaches its FPPR decisions, conveniently making them much harder to challenge.
Introduction and background
Two years ago I referred Cygnet directors who had been seriously criticised for harming a whistleblower to the Care Quality Commission under CQC Regulation 5 Fit and Proper Persons (FPPR).
Under this regulation, the CQC has powers to ensure that a provider has satisfactory processes for ensuring that its directors are Fit and Proper Persons.
The CQC has typically manipulated matters to allow board members of regulated bodies to evade accountability for serious wrongdoing.
It has done so by claiming that it has no remit to assess if individual directors are Fit and Proper Persons.
Instead, CQC claims it can only look at processes.
This is of course arrant nonsense. If for example, a regulated organisation appoints a freshly convicted serial killer to its board, even CQC might be forced to admit that based on an assessment of the individual, the provider was in breach of FPPR.
CQC Regulation 5 demands that directors must be of “good character”:
“The requirements referred to in paragraph (2) are that—
the individual is of good character,
the individual has the qualifications, competence, skills and experience which are necessary for the relevant office or position or the work for which they are employed,
the individual is able by reason of their health, after reasonable adjustments are made, of properly performing tasks which are intrinsic to the office or position for which they are appointed or to the work for which they are employed,
the individual has not been responsible for, been privy to, contributed to or facilitated any serious misconduct or mismanagement (whether unlawful or not) in the course of carrying on a regulated activity or providing a service elsewhere which, if provided in England, would be a regulated activity, and
none of the grounds of unfitness specified in Part 1 of Schedule 4 apply to the individual.”
Moreover, CQC’s own internal guidance shows that CQC is perfectly aware that it can use other regulations to force the removal of unsuitable provider directors, should it wish to.
“It is not the responsibility of CQC to ensure fitness although we can take action against the provider if we believe an unfit person to be in a directorship position.”
That is the key issue. Does CQC wish to?
Current media interest in CQC’s handling of FPPR and the UHB scandal
CQC’s disgraceful handling of FPPR is back in the full glare of publicity because the controversial investigator for the UHB scandal Mike Bewick has omitted to examine UHB’s much-criticised FPPR process in his phase one review of UHB.
“There are also several gaps in the report including the lack of recommendation resulting from the conflicting CQC reports. We must be granted access to previous documents such as the Fit and Proper Person Review (FPPR) which have not been shared. Releasing these reports and details of the process and people involved in commissioning and carrying them out is important to help ascertain any conflicts of interest, whether decisions made have contributed to the propagation of UHB’s toxic culture, and whether these amount to a ‘cover up’
Bewick’s omission of FPPR issues from his review relied on a false premise.
Bewick claimed that he did not request a copy of UHB’s still secret FPPR investigation or investigate UHB’s handling of FPPR because it was not within the scope he had been given:
Unsurprisingly, Bewick kicked that can down the road.
In this political backdrop, another astonishing but fully predictable CQC failure on FPPR has concluded in the whistleblowing case of Dr Ambreen Malik at Cygnet Health Care.
CQC’s contention that Cygnet is compliant with FPPR
After I referred the relevant Cygnet directors to CQC under FPPR in the light of the extremely critical judgment against Cygnet for whistleblower reprisal, the CQC delayed and justified the delay because Cygnet had appealed against the ET.
During this time, thousands of Cygnet patients remained potentially exposed.
Only after lengthy legal proceedings concluded did CQC wrap up the FPPR process.
If CQC was concerned about patients, it would have independently reviewed Cygnet’s compliance with Regulation 5 without delay, and taken the approach that it would update any assessment if new information emerged.
In the UHB matter, CQC found UHB compliant with Regulation 5 but added that it would “reserve the right to review the case if further information is presented to the CQC”.
When it suits, in the pursuit of protecting the powerful, the arbitrary CQC will do as it pleases.
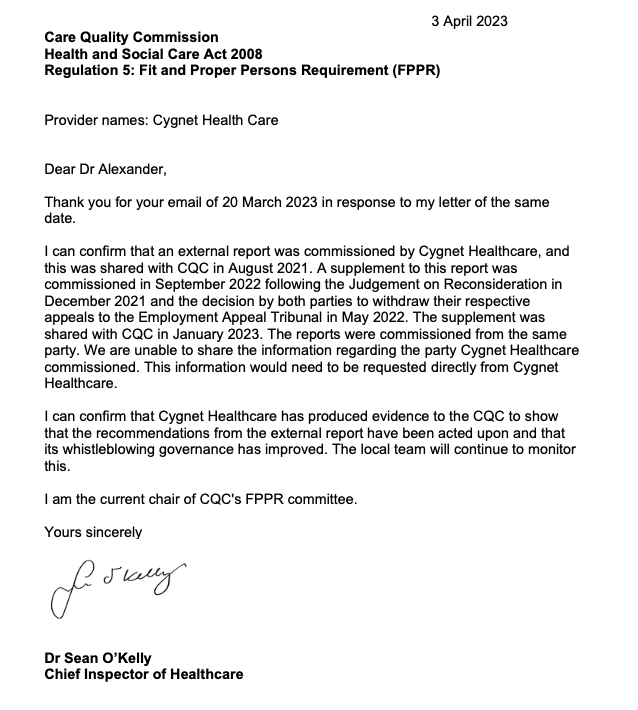
The letter came from CQC’s latest Chief Inspector of Hospitals, Sean O’Kelly, and ended with the signature CQC equivalent of shutting the door in a correspondent’s face:
“This concludes CQC’s review of Cygnet Health Care under this regulation, as well as our correspondence with you on the application of Regulation 5 to all information you supplied.”
For the sake of Dr Malik’s privacy I am not going into details, but the shocking disparity between CQC’s inaction and indifference, and everything that she has suffered is truly unforgivable.
Also, with impeccable timing CQC chose to shut down this Cygnet FPPR in the middle of the five week criminal trial of staff from Whorlton Hall (a Cygnet facility) , regarding abuse against highly vulnerable residents. This abuse was enabled by CQC’s failures to act upon the concerns of its own staff, including CQC whistleblower Barry Stanley Wilkinson.
The nine defendants in the Whorlton Hall abuse trial:
This was met with slightly more information on 3 April 2023, including a disclosure that O’Kelly is the current Chair of CQC’s FPPR committee, which makes the decisions on referrals:
O’Kelly’s role as chair of CQC’s FPPR committee introduces a potential conflict of interest. He may be faced with FPPR referrals which challenge the validity of previous, favourable CQC ratings for which he has ultimate responsibility as Chief Inspector.
Laughably and cynically, CQC suggested that I should contact Cygnet for a copy of the reports upon which CQC’s exoneration of Cygnet was based.
I doubt that Cygnet would be likely to willingly disclose their reports.
And of course, Cygnet Health Care is a private provider and beyond the reach of FOIA, so the reports cannot be obtained by this route either.
CQC’s ridiculous contention that Cygnet is compliant with FPPR because Cygnet’s whistleblowing processes have purportedly improved is predicated on an assumption that individuals change.
Some individuals are not capable of and may not wish to change. No amount of improved processes will protect patients or whistleblowers from such individuals.
That is why less compromised regulators actually ban failed/ rogue directors.
For example, Neil Cruickshank the former senior manager ultimately responsible for the Winterbourne View abuse scandal, who did not listen to whistleblowers’ disclosures, was banned for eight years by the Insolvency Service.
It is a pity that the same cannot be done to CQC, who failed to listen to the Winterbourne View whistleblowers and still fail horribly to listen to or protect whistleblowers by removing abusers.
I also asked NHS England on how it could exert its commissioning leverage to improve whistleblowing governance in the private sector. I have had no response despite numerous chasers.
It is also moot whether processes at Cygnet have genuinely improved. Scandals continue to emerge on a regular basis about Cygnet facilities, and most seriously of all, some of the scandals feature lack of learning and improvement after previous identification of failings.
Are some providers too big, wealthy and powerful to be allowed to fail?
And what of the revolving door between regulators and such powerful providers?
How many senior managers in our regulators have their eyes on the glittering prizes on the other side of the fence, and does that affect how they discharge their regulatory duties?
I have written as planned to asked Cygnet for a copy of their external FPPR reports:
BY EMAIL
Dr Tony Romero
CEO Cygnet Health Care Ltd
6 April 2023
Dear Dr Romero,
External FPPR reports
The Care Quality Commission has informed me that an Fit and Proper Person referral that I made on Cygnet directors under CQC Regulation 5 in 2021 has concluded, with the regulator concluding that whistleblowing processes at Cygnet have improved to the point where CQC considers that Cygnet is now meeting the requirements of Regulation 5.
I asked the CQC if there had been any transparency about the findings of external reports commissioned by Cygnet which the CQC relied upon to reach its conclusion of improvement.
The CQC did not reply directly to this question but suggested that I contacted Cygnet if I wanted copies of these external reports. They are:
– The external report shared with CQC in August 2021
– A supplement to this report in September 2022, which was shared with CQC in January 2023
In the NHS, the best practice guidance from NHS Providers is that there should be transparency about FPPR investigation findings, at least in summary form.
NHS Providers’ guidance also emphasises that visible rigour is important in contentious cases and where there have been failures of whistleblowing governance.
I would be grateful if Cygnet could accordingly disclose either copies of the external FPPR reports that it commissioned, or at least a summary of the main findings and recommendations.
I copy this to Sean O’Kelly CQC Chief Inspector of Hospitals, Amanda Pritchard CEO of NHS England in view of commissioning issues, and the relevant House of Commons committees.
Many thanks.
With best wishes,
Minh
Dr Minh Alexander
cc Sean O’Kelly CQC Chief Inspector of Hospitals
Amanda Pritchard CEO NHS England
Health and Social Care Committee
Joint Committee on Human Rights
I sent the above request to Cygnet on 6 April 2023 at 11.55 am.
I received the following reply from Cygnet’s General Counsel at 12.36 pm.
He has openly advocated that UK whistleblowers should be “incentivised”:
Other members of the Whistleblowing APPG have also spoken about whistleblower rewards and the APPG’s secretariat WhistleblowersUK has advocated for whistleblower rewards.
The offer of whistleblower rewards is against most ethical guidance on whistleblowing and against longstanding UK whistleblowing policy.
Kevin Hollingrake was appointed to the Department for Business, Energy and Trade as Parliamentary Under Secretary of State between 27 October 2022 and 7 February 2023.
Most recently Hollinrake was appointed Parliamentary Under Secretary of State at the Department for Business and Trade on 7 February 2023.
Will the review be conducted professionally, impartially and follow the evidence base?
Or will it be another Tory charade of thinly disguised cronyism, boot filling and back room deals?
Given all the evidence of government misconduct in recent years, one might reasonably think that the prospect of a bounty model, that siphons obscene amounts of cash into the hands of whistleblowing industry middlemen and bounty hunting lawyers, has just become more likely.
Especially if the increasing excitation of the assorted denizens of the Whistleblowing APPG’s murky waters is anything to go by.
Don’t be optimistic of any genuine governance.
Do expect the parade of dubious celebrities, useful idiots, fake talking heads, planted articles puffing the Office of the Whistleblower and social media sock puppeteers to get worse.
That is of course, only if some further terrible government scandal does not upend all plans by this time next week, and we get another clutch of heartsink ministers.
By Dr Minh Alexander retired consultant psychiatrist 29 March 2023
On 18 November 2022 it was announced by both University Hospitals Birmingham NHS Foundation Trust (UHB) and the commissioning body Birmingham and Solihull Integrated Care Board (ICB) that David Rosser CEO of UHB was moving on to a new role.
This role was regional “Strategic Director of Digital Health and Care”.
Curiously, there appeared to be no sign of an office, team, website locus, operating details or contact details. As the weeks and months passed, this did not change.
Eventually, repeated enquiries to Patrick Vernon the ICB Chair resulted in an admission, via the ICB FOI team, that Rosser had not left UHB at all.
He remained technically employed by UHB.
Jonathan Brotherton was carrying out his former duties as acting UHB CEO.
In Rosser’s new Digital role, he was reportedly “hosted” by the ICB and reported to the ICB’s chief executive David Melbourne.
Yes, that is the same David Melbourne who has been directly involved in the oversight of the ICB’s reviews on UHB’s failing governance and who has been responsible for briefing local councillors about the progress of the reviews via the Joint Health Overview and Scrutiny Committee.
All very intertwined and not very independent looking.
The ICB could not even produce a formal position specification/ job description, answering pitifully:
“Further specifics are being scoped with system partners”
And if it was all innocent, why was there a need for the carefully crafted, coordinated statements which omitted to mention that Rosser had not actually left UHB at all?
Why was the word “regional” tacked onto the role, giving the impression of distance from local arrangements?
Would the man on the Clapham Omnibus think that it all looked a bit furtive and collusive?
What were the ICB and NHS England trying to hide?
We will likely hear more as the threads continue to unravel.
Oh, and Bewick’s phase 1 report on UHB was published today, with a good many departures from his terms of reference, through substantial omissions.
We can at least thank Dr Bewick for helping to expose the situation further and for additionally making the case for a judge led inquiry with powers to protect vital witnesses who have had to remain silent so far.
UPDATE 3 April 2023
I asked the ICB if Mike Bewick had been in on the contrived fiction that Rosser had left UHB when he had in fact remained in UHB’s employ all along.
I have asked the ICB Chair Patrick Vernon to answer the questions clearly, as follows:
BY EMAIL
Patrick Vernon
Interim Chair
Birmingham and Solihull Integrated Care Board
3 April 2023
Dear Mr Vernon,
Circumstances of David Rosser’s employment and information disclosed to Mike Bewick
Thank you for the further FOI response from the ICB on this matter.
I feel the ICB has not responded to my FOI request. It has answered past the point and possibly disingenuously.
The ICB has stated in its response that Mike Bewick knew about the circumstances of David Rosser’s new role because they came into the public domain on 18 November 2022, when David Rosser’s appointment to the regional role of “Strategic Director of Regional Digital Health and Care” was announced, before Mike Bewick took on the UHB review.
Also, the ICB indicated that Mike Bewick was nonetheless informed of these details upon being appointed by the ICB, [to undertake the phase 1 rapid review of University Hospitals Birmingham NHS Foundation Trust].
However, in my FOI request I specifically asked the ICB if Mike Bewick has been informed of the fact that David Rosser had been “hosted” by the ICB and was reporting to the ICB chief executive.
These facts were disclosed to me only via an ICB FOI response in February 2023.
It was not public knowledge that David Rosser had in fact, as the ICB admitted in February, remained in UHB’s employment.
This was despite coordinated press releases by both UHB and ICB which gave the impression that he had left UHB.
These facts about his continuing employment by UHB and secondment to the ICB did not come into the public domain until late March when they were revealed by the BBC: first by Michele Paduano, and then Newsnight on 28 March 2023.
Accordingly, could the ICB provide a response to my specific questions as follows.
Did the ICB inform Mike Bewick upon appointing him, to undertake the phase 1 rapid review into UHB, that David Rosser:
a) Was still employed by UHB?
b) Was “hosted” by the ICB?
c) Was reporting to the ICB CEO?
Please also advise of an additional matter:
1) Upon being contracted to undertake the phase 1 rapid review of UHB, did Mike Bewick inform the ICB of the basis upon which he called himself “Professor”?
2) Did Mike Bewick provide the ICB with details of his qualifications and how he came by this title of “Professor”?
By Dr Minh Alexander retired consultant psychiatrist 26 March 2023
My apologies for a late post. This is due to a combination of illness and an excess of commitments.
As many whistleblowers, patients and bereaved families will know, the Care Quality Commission is fond of fending off concerns by labelling them as “complaints”. This is because CQC claims that it has no remit to investigate individual “complaints”.
CQC’s refusal to investigate countless serious matters, using this ploy, has caused endless frustration and distress. Importantly, it has wasted many opportunities for learning and public protection.
However, the regulator does have a duty under CQC Regulation 12, 2014, to investigate incidents that tend to show a failure by a regulated provider to provide “safe care and treatment”.
The CQC has powers to prosecute under this regulation. Clearly, in order to do so, it must first investigate.
Baby Harry Richford’s death and Regulation 12
An example of CQC’s unreliability arose in the case of baby Harry Richford’s death at East Kent.
CQC initially told his family in 2018 that it was unable to investigate their concerns and also that his death did not fall under Regulation 12.
The details of this matter were previously summarised here.
CQC came to an initial conclusion that no organisational failings contributed to Harry’s death. This was despite:
1. The trust’s own internal incident analysis concluding explicitly that there were systemic failures which contributed to Harry’s death:
“This leads us to conclude that this incident occurred due to system failures.”
Some of this was echoed in external reports at the time.
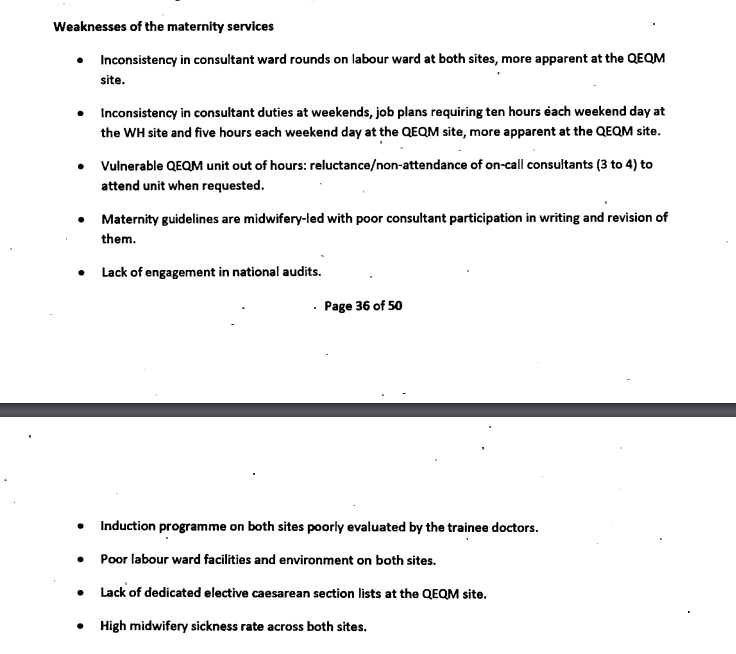
2. A 2015 Royal College review which had also previously identified systemic failings in the maternity service.
The systems failings identified by the Royal College included:
There had also been other signs of organisational failure by that point. Bill Kirkup’s October 2022 report on East Kent noted that the CCGs had raised concerns about maternity safety. CQC also received a whistleblowing disclosure from a consultant obstetrician in 2015 about poor leadership in East Kent’s maternity services. CQC received other disclosures about the culture of the maternity service. CQC itself found issues of culture in maternity services in 2014 inspection, when it rated the whole trust “inadequate”.
Despite the above evidence from multiple sources, the CQC claimed to Harry Richford’s family in 2018 there was only evidence of failings by individuals and not by the trust, and this meant that CQC Regulation 12 did not apply:
“After an extensive review, we do not believe there has been a breach in regulation. The concerns raised in this incident are centred on an individual’s decision or error. The criminal offences CQC can prosecute against only apply to registered person failures.”
However, the regulator later admitted that it had a remit under Regulation 12 to investigate Harry’s death.
The CQC replied defensively on 24 November 2022, acknowledging that it had erred only in respect of the fact that its local inspector had used “conclusive” language when informing Harry Richford’s family in 2018 that Regulation 12 had not been breached.
“When Emma Carroll drafted her email of 17 August 2018, the local team, based on the information they had available at that time could not establish all of these elements. However, in Emma’s email, she unfortunately used conclusive language. After the conclusion of our prosecution. we carried-out a learning review of the investigation and within that we highlighted Emma’s correspondence to the family in August 2018. The learning point was that, for any potential offence and after any initial assessment, further information can always come to light and therefore we should not use categorical language in our communication with victims and families which states a conclusive position.”
CQC focussed on the fact that she should have explained to the Richfords that new information might change CQC’s assessment.
The CQC contended that because it was tracking Harry’s inquest, it had not closed its file, and was still investigating.
There was nothing in this response about the quality of the 2018 CQC appraisal of Harry’s case, or any admission or explanation of why CQC had bizarrely overlooked ample evidence of organisational failure that existed by 2018, or why it had failed by that point to obtain a copy of the Royal College report.
But then, neither did Bill Kirkup fully acknowledge CQC’s failings in his recent report on East Kent. His main, repeated focus was on denial by East Kent managers.
Kirkup did make limited references in his report to missed opportunities by the CQC, but it would not do to direct too much fire at the powerful.
A bit like the strange silences about senior managers at Frimley, contrasted with the heavy focus on cover ups by frontline staff in his report about baby Elizabeth Dixon’s death.
But coming to the main point, CQC conceded in November 2022 correspondence that if it receives information about a possible breach of Regulation 12, such disclosures would be considered as part of CQC’s “assessment” about the purported breach:
So, don’t let CQC kick your concern into the long grass by framing it as a “complaint”.
Rather, insist – if it is so – that your concern engages Regulation 12.
UPDATE 9 April 2023
A coroner’s inquest has revealed that the CQC badly failed very vulnerable older patients at a HC-One home, by failing to act on numerous concerns.
Three residents died in February and March 2019.
One family member contacted the CQC NINE times to raise concerns.
The CQC did not inspect the home until August 2019.
By Minh Alexander NHS whistleblower and Martin Morton Social Work whistleblower 22 March 2023
The Care Quality Commission is the quality regulator for health and social care in England. It is supposed to be an impartial guardian of care standards and accountable to the public.
In reality, CQC was created in the aftermath of government embarrassment by a previous health regulator which uncovered the MidStaffs disaster.
The CQC was not intended to repeat such embarrassment and its first CEO was in fact the former CEO of the West Midlands SHA, a body that was central in the Mid Staffs disaster.
All told, the CQC has proven to be a politicised and suppressive organisation.
It has failed countless whistleblowers, including its own. This all the worse for the fact that CQC is a Prescribed Person under UK whistleblowing law and should at least not harm whistleblowers, whether by act or omission.
However, last year, the regulator was proven to have seriously harmed a CQC whistleblower in the ET case of Kumar v CQC.
The government has allowed the CQC to investigate and control investigations into itself regarding this spectacular failure.
At least one of these investigations, a barrister led review of the Kumar case and a mysterious, undisclosed sample of other whistleblower cases, should have reported by now, but nothing has been released into the public domain.
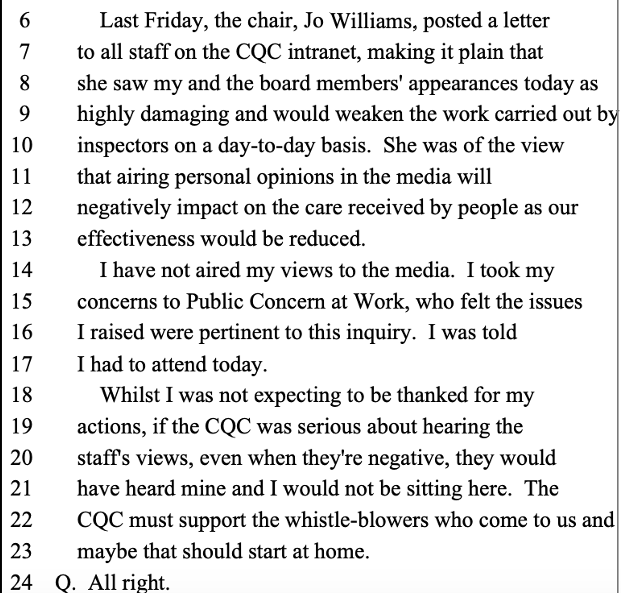
CQC’s whistleblowing governance reviews
Sparse terms of reference for the CQC reviews post Kumar v CQC were issued.
It was not disclosed how the additional whistleblower cases for review were chosen. CQC instructed a barrister from Matrix Chambers. FOI enquiries revealed that
In the meantime, the CQC has shown itself to be disingenuous despite its glib claims that it would learn from the Kumar case.
In an internal briefing to CQC staff in September 2022, disclosed via FOI, CQC’s CEO Ian Trenholm claimed shortly after the ET loss that both the CQC and the National Freedom To Speak Up Guardian had good track records on supporting whistleblowers.
Trenholm also decried CQC’s critics.
Is denial a novel technique for creating a safe environment that helps staff to raise concerns?
CQC’s failure under FOIA to produce all of its Freedom To Speak Up Guardian reports
When this obvious error was pointed out, CQC reverted to silence. It has still not properly responded to the FOI request.
Some of CQC’s internal Freedom To Speak Up Guardian reports were actually published via CQC board papers, but not all seem to have been released. There are gaps in the timeline of published reports, taken from archived CQC records.
The chief executive and CQC board will be given high level information about all concerns raised by our staff through this policy and what we are doing to address any problems. The CQC Guardian will produce a report twice a year to the board setting out the volume and type of concerns that have been raised, without identifying individuals. The board supports staff raising concerns and wants you to feel free to speak up.”
The CQC’s silence in response to the request for all its Freedom To Speak Up Guardian’s reports is troubling. Are important matters being concealed? Were some of these reports produced for internal consumption only, and have they been improperly withheld from FOIA disclosure?
Of the so far published CQC Freedom To Speak Up Guardian rreports, these present superficial data which raise more questions than they answer. Links to these uploaded CQC reports and some examples of how limited data is presented in these reports is summarised here.
CQC denial of detriment and dissembling about feedback about its Freedom To Speak Up process
In the course of the above FOI correspondence about CQC’s whistleblowing governance, CQC implausibly denied that there had been any detriment suffered by employees in 131 recorded speaking up cases over five years:
“…we can inform you that nobody raised that they feel they have suffered detriment as a result of speaking up.”
Curiously, despite being adamant that there was no detriment in any of these 131 case, CQC claims it is unable to answer a question about its employees’ satisfaction with the CQC speaking up process.
This allegedly because it would have to manually review files and this would take too long.
CQC has claimed a slew of other FOIA exemptions as well, indicating how reluctant it is to answer this very basic question about whether its staff are satisfied by their speaking up experiences.
Number of cases raised with a patient safety element
Number of cases raised with an element of bullying or harassment
Number of cases in which detriment occurred
Professional background
Feedback: “Given your experience, would you speak up again?”
There is a published national dataset based on this reporting system.
The so far published CQC Freedom To Speak Up Guardian reports do not reveal most of this required transparency data.
CQC’s internal whistleblowing policy gives cursory guidance on what records are made:
“What will we do? We are committed to the principles of the Freedom to Speak Up review and its vision for raising concerns, and will respond in line with them. We anticipate that some concerns may be capable of being dealt with informally to the satisfaction of all concerned, without contacting the ambassadors. If you choose to go through one of our FTSU ambassadors, your concern will be recorded and you will receive an acknowledgement within two working days. The central database will record the date the concern was received, whether you have requested confidentiality, a summary of the concerns and dates when we have given you updates or feedback, and any lessons learned.”
“To keep up to date records, recording contacts, concerns and outcomes in line with the CQC Freedom to Speak Up recording policy and process”
How did CQC know that no detriment has been reported via its Freedom To Speak Up arrangements? Was this a non-evidence based claim? Or is there collated data that is being withheld from the public, contrary to practice in the rest of the NHS?
If CQC is not collating data such as to whether its staff are satisfied with their experiences of the Freedom To Speak Up arrangements, through indicators such as whether they would speak up again, how can it claim to be learning?
CQC received the Kumar v CQC judgment in August 2022. The regulator has had over six months to reflect. The fact that it might be still failing to collect whistleblower feedback, ignoring the feedback or hiding the feedback is a very poor reflection on its intentions.
In fact, CQC’s Director of Engagement recently admitted in correspondence that CQC does NOT collect feedback from whistleblowers.
If so, why did CQC not simply admit this omission in its FOI response, instead of claiming that it would not produce the data due to an FOIA cost exemption?
“…there is only limited feedback available from those who have raised concerns with us about their experience of those processes and, therefore, how this might be improved.”
And yet CQC did not act on this. This is more evidence of CQC’s failure to take whistleblowing seriously.
Overall, it seems likely from the above inconsistent facts and CQC claims that there is dissembling in some manner, in addition to probable competence deficits.
Lastly, one of the authors has received information which contradicts CQC’s claim of zero detriment in 131 speak up cases.
This is hardly surprising, especially when CQC’s 2021 staff survey showed that only 49% of staff thought that it was safe to challenge the way things are done at the CQC, and that 10% of the staff who did not think it was safe reported that they had experienced repercussions as a result of speaking up previously.
So whatever is reported in CQC’s forthcoming reviews of its own whistleblowing governance, it would be safe to conclude that the reality is worse.
PETITION
Please click and add your signature to this petition to reform UK whistleblowing law – whistleblowers protect us all but weak UK law leaves them wholly exposed and it is a threat to public safety