Dr Minh Alexander retired consultant psychiatrist 26 September 2023
Because of concerns, I asked Gateshead Health NHS Foundation Trust about past failures of Disclosure and Barring Service (DBS) checks on its staff via a Freedom of Information request, which was refused by the trust on grounds that it would be making the information public at a forthcoming board meeting.
The FOI request to Gateshead:
These were the FOI questions, asked on 4 August 2023:
Please advise if since 1 April 2019 any failures of disclosure and barring procedure at Gateshead Health NHS Foundation Trust have been identified.
Please provide details of the nature and scale of any breaches (eg. how many staff were not subject to DBS checks or alternatively, how many staff records contained no evidence of DBS checks).
If known, when did any breaches commence?
If known, when were the breaches discovered?
What action did the trust take to address any breaches?
Did the trust inform NHS England and the Care Quality Commission of any DBS breaches, and if so, when did it inform them?
What reviews and or investigations have been conducted into any DBS breaches or potential breaches?
Please provide a broad account of any internal reviews and a summary of their outcome.
If external review has taken place, please disclose who undertook the review, the terms of reference given to them, a summary of the outcome and the report of any review.
This was Gateshead’s response of 5 September 2023 Ref FoI 2023-24.3185:
“We can confirm that the Trust holds the information requested in questions 4-13 inclusive, but considers it exempt from disclosure in accordance with s.22(1) of FOIA which covers information which is intended for future publication. The Trust intends to publicly disclose the information sought in relation to questions 4-13 at its Trust Board meeting on 28th September 2023.”
The checks are important in health and care services to ensure that trustworthy staff are employed to provide care, especially to the most vulnerable. DBS checks are an essential component of Safeguarding patients. Failures to carry DBS checks are a failure of Safeguarding, and are a serious matter.
Importantly, Gateshead was until March 2023 led by Yvonne Ormston, who was the former CEO of North East Ambulance Service NHS Foundation Trust, which has more recently been the subject of very serious concerns about whistleblower suppression, deaths and alleged manipulation of information supplied to the coroner.
Interestingly, at NEAS, there was an earlier reported failure of DBS checks over FOUR years, leading to the CQC issuing a Section 29A warning notice in February 2014 (Ormston became NEAS CEO in October 2014).
A recent FOI request was made about this to the CQC by David Change on 7 August 2023, on the What Do They Know website:
“The section 29A warning notice was issued at that time due to concerns that staff with positive DBS disclosures were not managed in line with trust policy. In addition, individuals employed by NEAS who had significant safeguarding concerns raised about them in respect of concerns raised outside of the workplace were not being managed appropriately or in a timely manner.”
Gateshead Health NHS Foundation Trust has now published a report on its past DBS failures, amongst its papers for a trust board meeting tomorrow. See page 104, report on Disclosure and Barring Service Checks by Amanda Venner, Interim Executive Director of People & OD.
Venner’s report admits:
“Following an internal review, some gaps were Identified in historical DBS records (either no record or record at lower level than required for job role).”
Venner fails to give the date of the “internal review” but she states:
“An internal audit in May 2023 identified that some staff did not have a DBS check recorded on their records or that their DBS check was not at the correct level of assurance.”
“After initial audit 977 staff and volunteer records had DBS either missing or incomplete.
Current position is:
• 863 checks complete.
• 1 check outstanding (Trust volunteer).
• 59 staff have left the organisation
• 10 found to be not required.
• 20 long term sick/maternity.
• 24 in progress (with the DBS or for internal checking).
There is 1 check outstanding for a Trust volunteer who is aware that they will not be able to undertake volunteering duties for the Trust until this check is complete.”
“15 individuals either self-declared or were found to have cautions/convictions on their DBS check. Any convictions declared by colleagues during the process or notified by the DBS service were risked assessed locally and signed off as low risk by the Deputy Chief Executive/Chief Nurse and Professional Lead for Midwifery and AHPs and Interim Executive Director of People and OD. There have been no formal procedures necessary as a result of information received from the DBS.”
Would the trust ever have publicly admitted to these failures if it had not been asked about them? And how long has the problem actually existed?
The trust would like us to focus on the period from May 2023, but it has not actually answered all the relevant questions.
Venner claims in her report:
“As soon as the situation became apparent to the Trust on 19th May 2023, the Care Quality Commission, the Integrated Care Board and NHS England were notified of the position and the plan to address it.”
Since 2020, up to June 2023, the Executive Director of People and OD at Gateshead was Lisa Critchton-Jones. These are details from her LinkedIn entry:
Since July 2023, she has been the Assistant Director of Engagement (North),at NHS Employers:
And we should of course remember that Ormston was named by the Health Service Journal as one of the top 50 NHS CEOs:
And HSJ has never, ever, ever been known to be wrong…..
RELATED ITEMS
The NEAS families and whistleblowers want a public inquiry into failures and cover ups.
Their case is strengthened by the growing deaths scandal at University Hospitals Sussex NHS Foundation, currently being investigated by the police, because the flawed NHS England on NEAS was conducted by Marianne Griffiths the former CEO at Sussex.
Dr Minh Alexander retired consultant psychiatrist 21 September 2023
This is a short post to document another example of NHS managerial recycling, in the context of debate about regulating NHS managers after the Letby killings.
A former employee of Medway NHS Foundation Trust Rosemary Bonney,service manager in acute medicine, successfully sued the trust for unfair constructive dismissal.
The relevant events took place at a time of turmoil in the trust:
“7. The First Respondent is an NHS Trust (hereafter ‘the Respondent’). It operates Medway Maritime Hospital in Gillingham. At the relevant times it was struggling:
7.1. the Respondent was in special measures between 2013 and 2017;
7.2. even after leaving special measures the respondent was in ‘SOF4’, Single Oversight Framework, grade 4. That is the highest form of external scrutiny”
Mrs Bonney’s appointment to the trust as a service manager in acute medicine was chaotic, with muddle by the trust as to which role she had actually been appointed.
“18. The confusing and chaotic approach to the Claimant’s role reflected wider chaos within the Respondent at that time:
18.1. The Respondent was operating in an at least partly dysfunctional state and was in various respects in some disarray;
18.2. There was no General Manager in post for Acute Medicine. The General Manager would normally be the line manager of the Service Manager;
18.3. Ms Spence herself was under great pressure in her role and was picking up the line management of the Service Manager in addition a very wide range of other duties.”
In short, the ET determined that Mrs Bonney, a Black worker, began working for Medway in April 2019 as a service manager and was later offered a new role in Transformation by Medway’s Chief Operating Officer, Harvey McEnroe, which she accepted.
However, the offer had been made without Human Resources input, and was withdrawn after HR discovered the offer. Mrs Bonney was eventually advised that the offered role did not exist:
“55. On 27 September 2019, the Claimant spoke to Ms Nyawade who told her that the role in Transformation did not exist and that there were no recruitment plans for the Transformation Team.”
Mrs Bonney was shortly after signed off sick with stress and remained on sick leave until her resignation. She also raised a grievance about these events. The grievance was investigated by the Head of Corporate and Legal, Paul Mullane.
During the course of the grievance investigation, Paul Mullane withdrew and the investigation was completed by John Sheath, trust solicitor.
During the grievance investigation, Harvey McEnroe denied offering Mrs Bonney the Transformation job. The ET rejected McEnroe’s evidence and cited various contemporaneous correspondence which supported Ms Bonney’s contention that this post had been offered.
For example, emails that had been exchanged with various managers and the fact that Jack Tabner Executive Director of Transformation and Digital had given Mrs Bonney a reading list to prepare for her new role in his department. Tabner had also sent Mrs Bonney an email welcoming her to his team and discussing practical details such as computer access:
Based on the job offer, Mrs Bonney said goodbye to her existing team, in correspondence.
Her post in acute medicine was filled by someone else.
Jack Tabner also denied during the grievance investigation that Mrs Bonney had been offered the Transformation post, despite the mass of evidence to the contrary.
The ET criticised the fact that Mc Enroe and Tabner gave “simply factually untrue” evidence during the grievance investigation:
“177. In their evidence to the grievance investigator, Mr Tabner and Mr McEnroe gave evidence which was of great importance but that was simply factually untrue:
177.1. Mr Tabner said that “No formal offer was made and this was an early conversation. I then had no further contact with Rosemary.” Mr Tabner also said: “What arrangements did you make to receive Rosemary in the team?” he answered “none at this early stage.” This evidence was simply untrue and there is documented correspondence in which makes plain that it was agreed the Claimant would be working in the Delivery Unit and steps were taken to on board her. But for HR intervention she would indeed have commenced working in the Delivery Unit very shortly.
177.2. Mr McEnroe said: “I did not offer a formal role change but did offer to discuss RB as a possible candidate for the Delivery Unit….Possible future roles were discussed at this meeting, in response to RB asking about possible alternative roles. Transformation roles were discussed at this time.”
This account is not right. Mr McEnroe offered the Claimant a role in the Delivery Unit in the meeting of 12 September 2019. He then confirmed this when he spoke with Mr Cairney as Mr Cairney’s contemporaneous email indicates.
178. There was no reasonable and proper cause for giving the above version of events. It is not what happened and the events in question were at that point in time relatively temporally proximate – they dated back around 6 months. There was also a paper trail that could have assisted Mr Tabner/Mr McEnroe to refresh their memories had they chosen to look into the emails they themselves had sent and/or received in respect of the matters the grievance investigator was asking them about.”
Kevin Cairney, formerly Medway’s Director of Operations for Unplanned and Integrated, gave oral evidence to the ET that McEnroe and Tabner worked in the “grey”:
“56. Mr Cairney’s oral evidence was that Mr McEnroe and Mr Tabner worked “off policy” with “grey” transactions to get things done. We find that essentially something like that happened here. An offer of a role was made and it was accepted. This done in the informal way described above. However, when it came to HR’s attention the plug was pulled.”
Mrs Bonney resigned from Medway in December 2020 shortly after receiving the outcome of her grievance appeal.
The ET concluded that the trust’s actions in withdrawing the Transformation post and the handling of Mrs Bonney’s grievance amounted to repudiatory breaches and that she was unfairly constructively dismissed.
The ET also criticised adverse line management feedback to Mrs Bonney about her performance and the repetition of these sentiments in the grievance report:
“81. The report’s conclusions, fairly read, find or assume that there was indeed significant under-performance on the Claimant’s part and/or that she had a lack of suitability for her role. There was no proper basis for that finding/assumption based on the evidence gathered in the investigation.”
The grievance appeal outcome, from Gurjit Mahil deputy Chief Executive framed the offer and withdrawal of the Transformation post as a matter of ineffective communication by the trust. It was ambiguous as to Mrs Bonney’s performance. The ET considered that it was a better quality piece of work than the grievance report, but accepted that the grievance appeal outcome was the “final straw”.
According to KentOnLine, Medway NHS Foundation Trust accepted the ET’s findings.
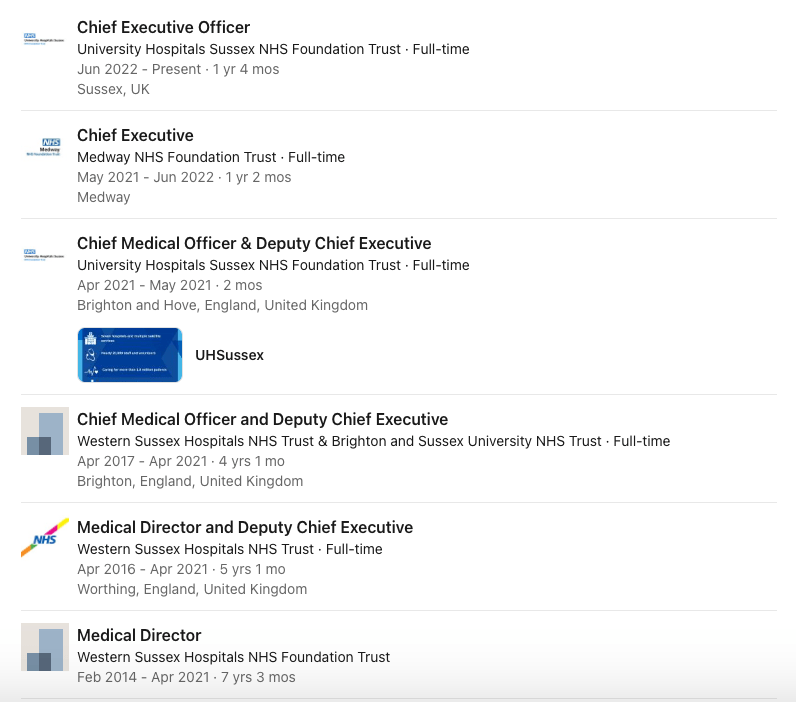
Harvey McEnroe’s linkedIn entry indicates that he moved to more senior management posts at NHS England in July 2021, rising to become Regional Head of Performance and Delivery and ICC Director – NHS South East England.
The Sussex connection is interesting as Medway’s CEO Jayne Black was formerly the Chief Operating Officer at Sussex, spanning some of the years relevant to current police investigation of deaths at Sussex.
Sussex’s former medical director now CEO George Findlay also spent a year at Medway as its CEO, preceding Black’s appointment as CEO.
The declaration that NHS directors must make annually is as follows:
“I declare that I am a fit and proper person to carry out my role. I: • am of good character • have the qualifications, competence, skills and experience which are necessary for me to carry out my duties • where applicable, have not been erased, removed or struck-off a register of professionals maintained by a regulator of healthcare or social work professionals • am capable by reason of health of properly performing tasks which are intrinsic to the position • am not prohibited from holding office (eg directors disqualification order) • within the last five years: ‒ I have not been convicted of a criminal offence and sentenced to imprisonment of three months or more ‒ been un-discharged bankrupt nor have been subject to bankruptcy restrictions, or have made arrangement/compositions with creditors and has not discharged ‒ nor is on any ‘barred’ list. • have not been responsible for, contributed to or facilitated any serious misconduct or mismanagement (whether unlawful or not) in the course of carrying on a regulated activity or providing a service elsewhere which, if provided in England, would be a regulated activity.“
I leave readers to consider the effectiveness of this arrangement.
In another employment dispute, Medway lost an ET case by default because the trust simply failed to respond to a claim:
I asked Jayne Black Medway’s CEO why the trust did not respond to the claim. She has provided no explanation so far. Her office only responded to say that “To confirm, this decision has been revoked and the Trust has submitted a defend [sic] to the claim.”
Robert Francis appeared on BBC Newsnight on 11 September 2023 and supported NHS England’s claims that full regulation is not needed for NHS managers:
Francis suggested on Newsnight that NHS employers are unaware of errant managers’ histories. By doing so, he drew a veil over what is an organised system of mutual protection and recycling, which has NHS regulators at its heart. The system even has a nickname, “The Donkey Sanctuary”.
The case of Paula Vasco-Knight exemplifies the collusion running throughout the system:
Dr Minh Alexander retired consultant psychiatrist 15 September 2015
Labour were responsible for installing Cynthia Bower, the former Chief Executive of the West Midlands Strategic Health Authority, which failed to prevent the disaster at Mid Staffs, as Care Quality Commission Chief Executive in 2009. She went on to fail and resigned.
Labour appointed Bower as CQC CEO in 2009 in spite of Alan Johnson, Labour Health Secretary, telling parliament in 2007 after an earlier NHS disaster that incompetent NHS managers should be removed.
The CQC further weakened itself and disbanded its central investigation team, leading to the compromised, cosy relationships between local CQC inspection teams and providers, that have often featured in subsequent, serious failings. Indeed, the CQC rated the Countess of Chester Hospital NHS Foundation Trust favourably whilst the trust was ignoring whistleblowers who tried to raise concerns about Letby’s killings. The CQC claimed at that point: “There was a very positive culture throughout the trust. Staff felt well supported, able to raise concerns and develop professionally”
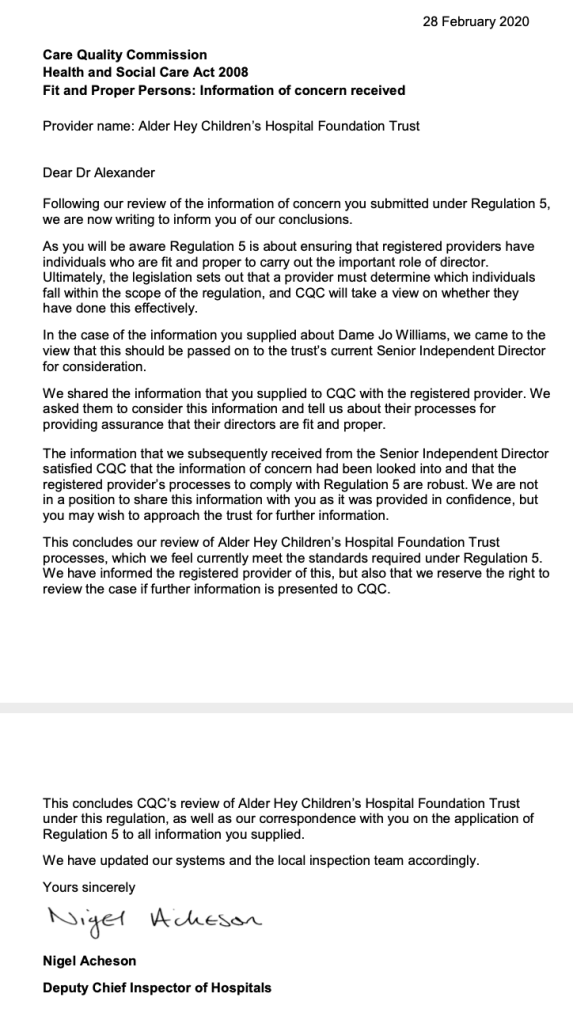
Indeed, CQC and the NHS jointly acted to recycle Jo Williams, the CQC Chair installed by Labour in 2009. This recycling was despite the fact that she had been criticised for harming CQC whistleblowers.
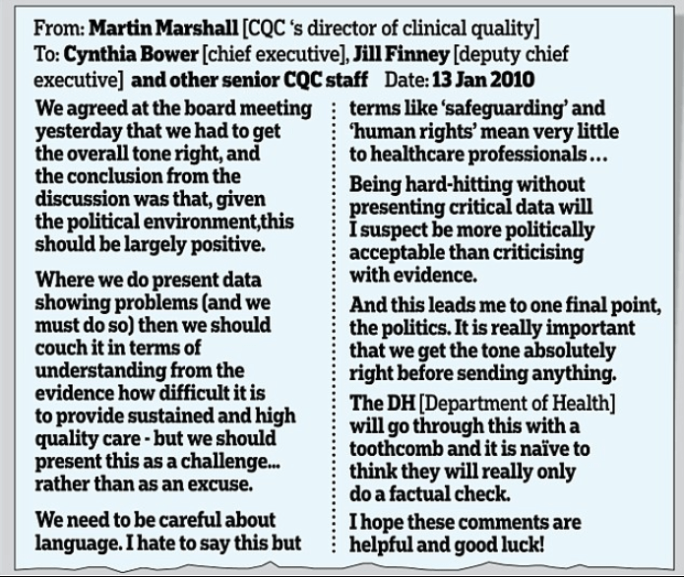
The CQC was shown to be politically subservient in internal correspondence which showed its senior leaders discussing how to appear tough, without actually sharing key details of service failure with the public.
Post Letby Wes Streeting, Labour Shadow Health Secretary, has intervened in the current debate about NHS management failure by promising to regulate NHS managers.
He has not clearly defined what he means by regulation, and in fact spoke on BBC Newsnight on 13 September 2023 about implementing existing recommendations.
There is currently no recommendation on the table for full managerial regulation that would bring NHS managers to the same level of accreditation and accountability as doctors, nurses and other registered healthcare professionals.
The Kark review recommended only a disbarment mechanism, with a view to full regulation in the future if this proved insufficient:
“On the evidence currently available to us, we have not at this stage recommended that the HDSC [Health Directors’ Standards Council] becomes a full ‘regulator of directors’, accrediting training, registering and regulating directors, and operating a form of revalidation process. But we do recommend that the design of the HDSC allows for a more extensive remit should that prove necessary.” [my emphasis]
Moreover, there is no proposal on the table to regulate ALL NHS managers. Only directors are covered by the Kark proposals, with the risk that more abuses will be simply commissioned further down the chain of command. Many whistleblower cases show that abuses start at middle management level. Should such power abusers be allowed to progress in their careers without any controls? As things stand, partaking in abuse often results in reward and promotion. I have only today received an anguished message from a victim about such a promotion.
Kirsty Wark: I’m joined now by the Shadow Health Secretary Wes Streeting, thank you very much for joining us, Wes Streeting. First of all, amongst the series of films that we’ve made over the last eighteen months, we’ve demonstrated a failure of NHS England to hold management to account for their failings. We just heard that line there, managers have no one to answer to. Why has it taken till the Lucy Letby conviction for politicians across the board to really focus on the problems of management?
Wes Streeting: Good question because there’s been a series of reviews. We’ve had Sir Robert Francis with his review, we’ve had the Kark review, we’ve had the Messenger review.
Kirsty Wark: You backed Sir Robert Francis didn’t you, on the Fit and Proper Person to be…
Wes Streeting: Of course we’ll back the recommendations but not all of the recommendations in all of those reviews have been followed. And in particular when it comes to the regulation of senior managers in the NHS, the government hasn’t gone as far as they really ought to. And one of the things I’ve said to the Health Secretary Steve Barclay because on patient safety issues, and particularly in the light of the most grotesque tragedy of what happened in the case of Lucy Letby and her heinous, undescribable crimes, don’t want to use this as a political football. I have said to the Health Secretary if he goes ahead with the recommendations of the Kark review, and the full implementation of all the other recommendations that have been made, he will have our whole hearted and full throated support.
If the government doesn’t act before the general election, if there’s a Labour government after the general election, we will act because one of the things that I find infuriating is this merry go round of failure and incompetence, which has led to the most appalling crimes going undiscovered. And that can’t be allowed to continue.
Kirsty Wark: So if those recommendations are published in full you’ll go along with that as far as the Conservatives are concerned. If a Labour government gets in, how quickly will you institute every single recommendation?
Wes Streeting: Well I think this has got to be a first order priority which is why….
Kirsty Wark: Immediately?
Wes Streeting: ….which is why I’ve given the government our support. To say if you bring forward the measures before an election, we’ll work with you. Because one thing I will say Kirsty, recommendations and regulation is one thing, the caveat I would add is that in relation to regulation of senior managers and the disbarring of senior managers, in the cases of professional negligence and misconduct which I think is essential, that is part of the answer.
There is a deeper challenge on culture. And that’s a much harder nut to crack. And it’s partly about penalties but it’s also about inculcating good culture through training, support and making this agenda a priority.
Kirsty Wark: Let’s just look at [inaudible] very quickly. As you say the regulation is there to be enacted in full. If you win the election and come in, will you enact that immediately and I really do mean within the first six months.
Wes Streeting: I’d hope so. Got to negotiate on the legislation programme but that would be my undertaking, because I think this is such a crucial priority. And actually Kirsty it’s one of the reasons why we started now to consult with NHS leaders and the wider workforce about getting the regulation right. Because I want to be ready to hit the ground running.
Kirsty Wark: One of the problems with this is that whistleblowers, people don’t feel safe still to come forward. There isn’t an atmosphere and there aren’t rules where people can speak out. Will you make sure that policy is cast iron?
Wes Streeting: Yes and in fact one of the things we are asking hard questions on is why is that the Duty of Candour which has already been established isn’t working. And this is why I come back to this point about culture, because as it stands there’s meant to be a Duty of Candour, one of the reactions…
Kirsty Wark: The programme on Monday night made it clear…
Wes Streeting: And by the way, I take my hat off to Newsnight’s investigative journalism. Thank goodness you have shone the light that you have, but this is why I have come back to this point about culture. When I spoke to someone senior in the NHS just last week about the Letby case and the merry go round of senior managers,I was told, but look, we’ve got the Fit and Proper Person’s test, and we now got a standardised form for references. My…This is why culture is crucial because my challenge back was “You think the answer is a form, I’m telling you the problem is culture, where poor performance is tolerated, where safety isn’t a genuine priority.
The Health Service Journal has meanwhile published on 12 September 2023 a letter by Streeting to NHS Confederation and NHS Providers, broaching the matter of managerial regulation:
Wes Streeting letter to NHS Confederation chief Matthew Taylor and NHS Providers chief Sir Julian Hartley
Dear Mr Taylor and Mr Hartley
I am writing following the murders of at least seven babies by Lucy Letby, and the failings in the management at the Countess of Chester Hospital uncovered by the subsequent trial.
These were acts of unspeakable evil which are impossible to fathom. However, it appears certain that the lives of newborn babies could have been saved, had hospital leaders acted when concerns were first raised by staff working on the ward. Instead, the brave doctors who sounded the alarm were met with hard-headed, stubborn refusal.
This is not the first time whistle-blowers in the NHS have been ignored at a cost to patient safety. Yet, despite the case for regulation being made pointedly and repeatedly in the past decade, little action has been taken. That is not good enough. The system must change.
I am writing to give the health service notice now that Labour is committing to act, and to state my intention that we work collaboratively towards delivering a regulatory framework that strengthens the accountability of managers and enhances patient safety.
I want to see supportive regulation that promotes excellent leadership and protects patients when things go wrong. Good management is vital for staff wellbeing, clinical outcomes, efficient services and, most of all, patient safety. Strong professional standards and training for managers can help to foster first-rate leadership throughout the health service. Likewise, I am clear that those found guilty of serious misconduct should be disbarred from the NHS.
I recognise the shortcomings of clinical regulation. It can be bureaucratic and misguided, and does not always lead to the best outcome, but this cannot be an excuse for inaction. We will learn from systems that are already in place, listening to experts and harnessing the learnings of multiple national reviews into the accountability of NHS managers.
I am keen to receive representations from NHS Confederation and NHS Providers so that I can take into account the views of your members and senior leaders in the NHS, alongside patient representatives, on four aspects:
How we subject managers to regulation and measure competency
How a professional register might work and how we avoid unnecessary bureaucracy, minimise overlap and streamline existing regulation
How we ensure whistle-blowers are listened to and empower staff to raise concerns.
How we deliver the best training to develop and support managers and how we adopt and spread good practice
We must get this right, for the sake of both patients and staff. We owe it to the victims of Lucy Letby and to the whistleblowers whose warnings were ignored.
I look forward to hearing from you.
Between now and final implementation of any controls on serious NHS leadership failures, there will no doubt be further lobbying and attempts to neuter any managerial regulation.
Those who are intimately acquainted with NHS leadership failures need to push back equally hard against the specious anti regulation arguments that are flying about.
PETITION FOR REGULATION OF NHS MANAGERS
This is a Westminster petition calling for regulation of NHS managers:
Francis suggested on Newsnight that NHS employers are unaware of errant managers’ histories. By doing so, he drew a veil over what is an organised system of mutual protection and recycling, which has NHS regulators at its heart. The system even has a nickname, “The Donkey Sanctuary”.
The case of Paula Vasco-Knight exemplifies the collusion running throughout the system:
Dr Minh Alexander retired consultant psychiatrist 14 September 2023
This is a short post to note that Medway NHS Foundation Trust, which has links with Brighton and Sussex University Hospitals NHS Trust (later University Hospitals Sussex NHS Foundation Trust), extraordinarily simply did not respond to an Employment Tribunal claim, and lost the case by default under Rule 21.
If the trust considered the claim meritorious, why did it not seek to resolve it at an earlier stage, instead of making the former member of staff suffer for even longer through a legal process?
Was the trust avoiding the public airing of damning information by not responding to the claim and was it suppressing evidence of serious managerial misconduct?
How much public money will have been wasted by the mishandling of this case?
Who are the directors of Medway NHS Foundation Trust?
The Medway Chair is a former Lloyds banker with expertise in offshoring, who was appointed as NED on 1 September 2015 on Hunt’s watch.
Medway’s chief executive since August 2022, Jayne Black a nurse, has sparse biographical details published on the trust’s website:
According to her LinkedIn entry, Black was formerly the Chief Operating Officer at Brighton and Sussex Hospitals University NHS Trust:
The Board of Western Sussex Hospitals NHS Foundation Trust, of which Black was a member, took over the running of Brighton and Sussex Hospitals University NHS Trust in 2017. The two trusts formally merged to become University Hospitals Sussex NHS Foundation on 1 April 2021.
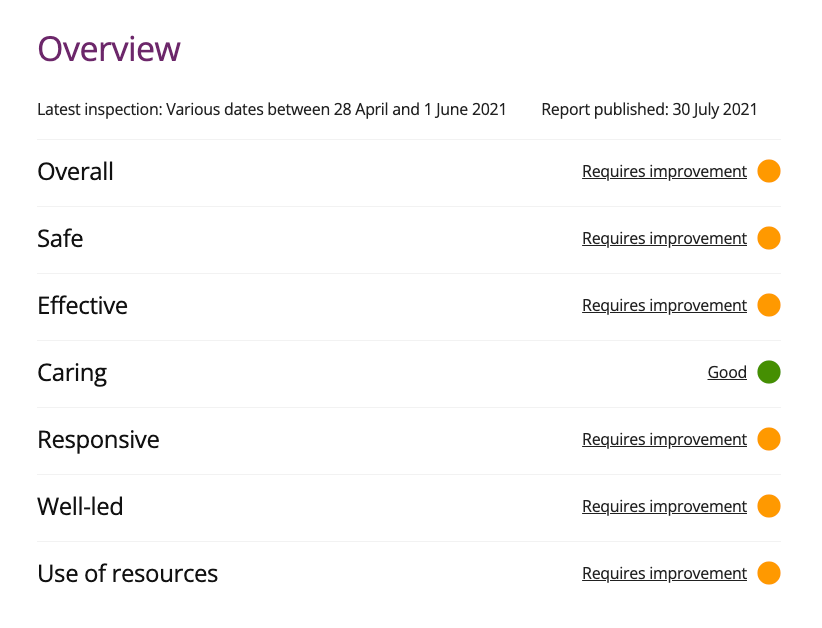
There have been multiple failures of whistleblowing governance at Brighton and Sussex, now acknowledged by the Care Quality Commission. A CQC inspection at the Royal Sussex County Hospital which took place during September to October 2021 resulted in a highly critical inspection report.
A police investigation is now also taking place into untoward trust deaths that whistleblowers have been raising concerns about for years. Some of the deaths being investigated occurred during Black’s tenure as Chief Operating Officer at Brighton and Sussex.
It was revealed yesterday by The Guardian that the police investigation is widening and that there is evidence of continuing risk to the public. Disturbing details of harm suffered by patients, and families’ difficulties in getting the truth about loved ones, are now coming into the public domain:
Of note, George Findlay the medical director and now Chief Executive of University Hospitals Sussex NHS Foundation spent a short period at Medway, as CEO, preceding Black’s appointment. These are the relevant details from his LinkedIn entry:
I have asked Jayne Black for information on why Medway NHS Foundation Trust failed to respond to the ET claim by Mr Prew.
Medway NHS Foundation Trust is currently rated “Requires Improvement” overall by the Care Quality Commission, and also “Requires Improvement” on the Well Led domain.
“There have been significant cultural, relationship and leadership issues within urgent and emergency care which have had a demonstrable negative impact on patient outcomes. The trust had commissioned mediation for staff and had relied on external intervention from the NHSE/I’s Emergency Care Improvement Support Team (ECIST) to help to engage staff and deliver improvements in performance on length of stay and ambulance handovers.
Our conversations on the Freedom to Speak-Up agenda, focus groups with Junior Doctors and discussions with others with roles intrinsically linked with cultural change reflected a lack of engagement with staff. As did the trust’s 2020 staff survey results with the majority of relevant indicators falling below the national average, with many falling significantly below.
These cultural issues, along with a lack of meaningful clinical engagement had created a disconnect between management and clinical staff. A clinical summit was held in February 2021 to bring these groups together to look to bridge the gap and work together to make improvements and to begin to reform the medical model. However, a recent follow-up to this summit, around the time of our inspection, showed that this work had proved unsuccessful and the pace of delivery (and reform) had not been improved through this process.”
That’s something to chew on, for the pro management lobbyists who have been criticising the Secretary of State for suggesting that poor managerial performance may be grounds for disbarring NHS managers.
“Serious mismanagement” is a ground for action under CQC Regulation 5 Fit and Proper Persons, as it should be, because serious mismanagement of healthcare services can kill thousands.
CQC Regulation 5 states:
“5(3)(d) the individual has not been responsible for, been privy to, contributed to or facilitated, any serious misconduct or mismanagement (whether unlawful or not) in the course of carrying on a regulated activity or providing a service elsewhere which, if provided in England, would be a regulated activity.” [my emphasis]
NHS healthcare management is critical to the wellbeing of millions. It should be professionalised and consistent with Nolan Principles of public service, and not a morass of club culture.
PETITION FOR REGULATION OF NHS MANAGERS
This is a Westminster petition calling for regulation of NHS managers:
Francis suggested on Newsnight that NHS employers are unaware of errant managers’ histories. By doing so, he drew a veil over what is an organised system of mutual protection and recycling, which has NHS regulators at its heart. The system even has a nickname, “The Donkey Sanctuary”.
The case of Paula Vasco-Knight exemplifies the collusion running throughout the system:
The broadcast viewed the issues through the prism of a yet-to-be-tested case of allegations against The Christie NHS Foundation Trust by Rebecca Wight, a nurse who reports that she experienced reprisal after raising concerns about another nurse’s practice. The concerns included an allegation of records alteration after a patient death.
The Christie accepted that concerns were legitimately raised but denied that there was patient harm or improper records alteration. The NMC is investigating. Newsnight reported that Wight has filed a claim of wrongful dismissal to the Employment Tribunal.
Ahead of the Newsnight broadcast, The Christie took the step of issuing an internal statement to its staff, denying the veracity of Wight’s allegations.
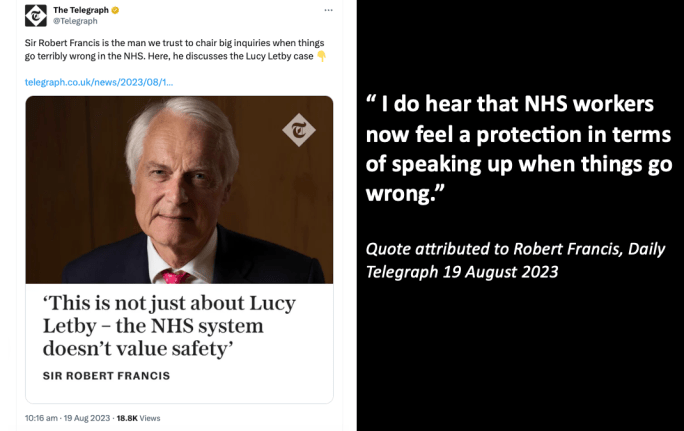
Newsnight interviewed Francis about the need for NHS managerial regulation in the context of the Wight case and other matters, such as the scandal at University Hospitals Birmingham NHS Foundation Trust and the Letby killings at the Countess of Chester Hospital.
Francis recently supported the government’s initial stance of resisting a public inquiry into the Letby killings. He gave an interview to the Telegraph which resulted in a comically adulatory article about The Patrician:
Francis now hums a similar tune and told BBC Newsnight that he thinks it is time for NHS managers to be regulated. However, he said that there is no need for strict equivalence to a body such as the General Medical Council. Francis espoused only a reactive system which will respond to complaints. This is the case for teachers.
Although Francis spuriously claimed that such a reactive system would level the playing field for clinicians, his suggestion means that non clinical NHS managers would not be held to the same level of proactive professional standards, skills, aptitudes and continuing professional development that clinicians are expected to meet.
This effectively ignores past reviews of NHS management capability, which have criticised the poor training of NHS managers.
All whilst the government and General Medical Council dream up ever more absurd ways in which to control doctors. For example, a newly introduced, mandatory requirement for “kindness”. I have written to the GMC’s medical director about this and have not yet received a response.
At that point, Francis agreed with Kark’s proposal of a disbarring mechanism and he suggested that the disbarring function could be given to the Health and Care Professions Council. The HCPC is the most incompetent professional regulator that I have ever come across. It does not even collate basic data about referrals by referring employer.
A transcript of Francis’ comments about managerial regulation to BBC Newsnight is provided below:
18.07
Robert Francis: Well on the point of confidentiality, I appreciate that there is always a need for some degree of confidentiality. But too often in my view, and I can’t comment on this individual case, but too often it’s used as an excuse not to give explanations either to the members of staff or indeed to patients about what has happened to them. And I think that needs to be revisited.
Victoria Derbyshire: Time and again when someone raises a concern, whether it’s Rebecca Wight an experienced nurse, whether it’s senior consultants in the Letby case, who had to apologise to Lucy Letby for raising concerns. Or the statistical data at Stafford Hospital showing deaths were higher than they should have been, managers attacked the messenger, the data. Rather than focussing immediately on patient safety. It’s still happening. Why do you think that is?
Robert Francis: I think that there is a, an absence unfortunately in the National Health Service of a proper system of investigating things that might have gone wrong. And I don’t think…you shouldn’t have to wait until you prove that something’s gone wrong before it can be looked into. And I think that needs to be done by qualified and trained people who can undertake an objective inquiry, one that’s independent. And one that produces an authoritative result. At the moment I’m afraid, most investigations, if there’s one at all, are undertaken sometimes by Human Resources officers who frankly they don’t have the expertise, or by people who have a preconceived agenda. So I think there needs to be a serious look at how we look at concerns that are raised, whether it be by staff or patients or indeed into serious incidents which are known to have happened.
Victoria Derbyshire: In our film the question was about why doctors and nurses can be struck off yet not hospital managers. Do you think that should change?
Robert Francis: I think the time has come for that to be considered very seriously. I recommended the Fit and Proper Person Test, which is not very surprisingly a requirement that managers are Fit and Proper People to do the job. It seems to me that if they don’t treat whistleblowers correctly that raises an issue about whether they’re Fit and Proper People. But that hasn’t worked and I think the time has come where there should be a level playing field between managers and healthcare professionals in relation to regulation. And I don’t think that means a new sort of manager’s General Medical Council. What is needed is a register of people who are managers and a Tribunal of some sort which can listen to complaints about them and investigate them properly. At the moment, when a manager’s done something bad, at one trust goes to another, the new employer has very little means of finding out what happened before. And the only way of dealing with that is to have a system of disciplinary investigation, similar to doctors and nurses. And until that happens, I’m afraid that there won’t be what the outside world would think of as accountability.
RELATED ITEMS
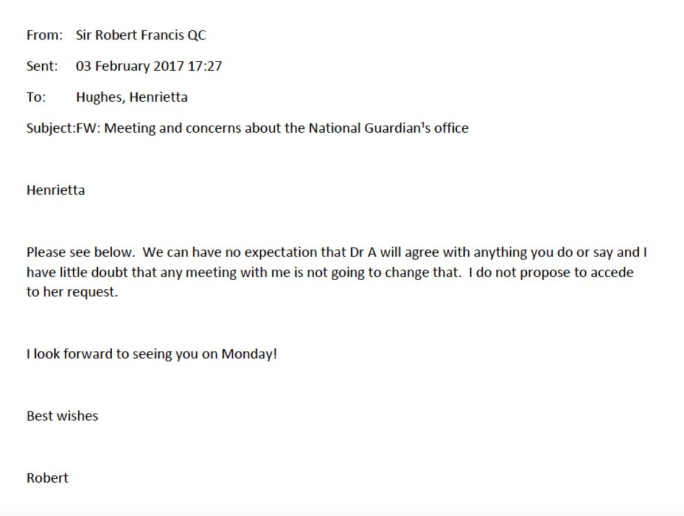
For those who are old enough to remember, Robert Francis once recommended criminal sanctions against NHS managers who suppressed and mistreated whistleblowers:
Also, Francis knows full well that UK whistleblowing law is hopelessly weak, but he declined to recommend law reform when he had the chance to do so in 2015. He instead gave us the useless and non evidence based Freedom To Speak Up model, and he refused to listen to concerns that the model was being further diluted by the second National Guardian and her funders, CQC and NHSE/I:
Francis’ comment to BBC Newsnight that new employers do not know what NHS managers did wrong in previous posts draws a veil over endemic collusion amongst the manager classes who protect each other. Quid pro quos are commonplace, and NHS regulators are at the heart of a system of organised recycling of erring NHS managers.
The case of Paula Vasco-Knight former NHS CEO and convicted fraudster is an excellent example of what happens:
Dr Minh Alexander retired consultant psychiatrist 11 September 2023
Who wrote the Whistleblowing APPG’s pro bounty Bill?
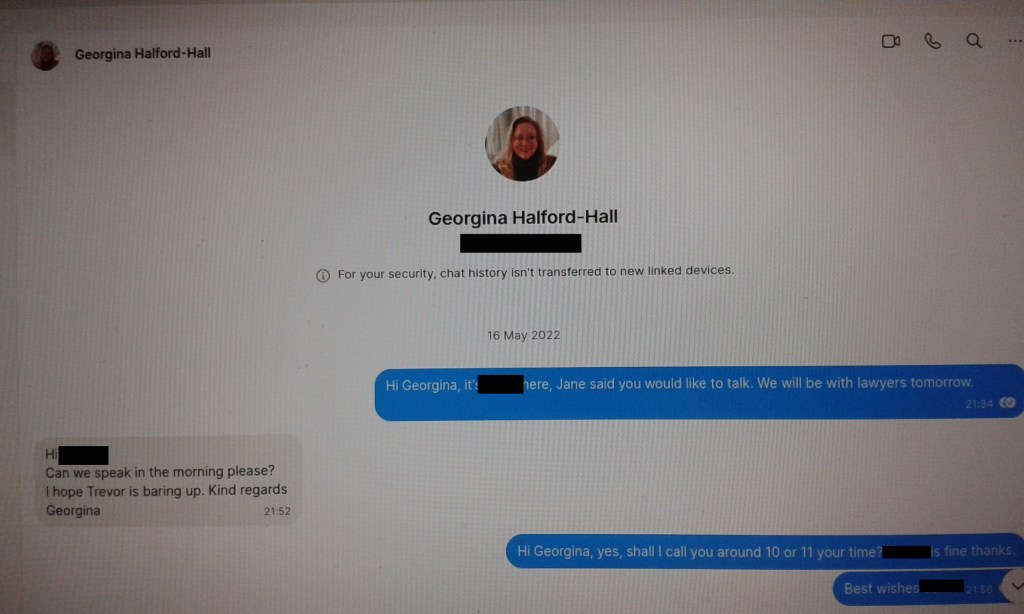
An individual who had dealings with WhistleblowersUK sent me photos of May 2022 Signal messages which appeared to be from Georgina Halford-Hall the CEO of WhistleblowersUK.
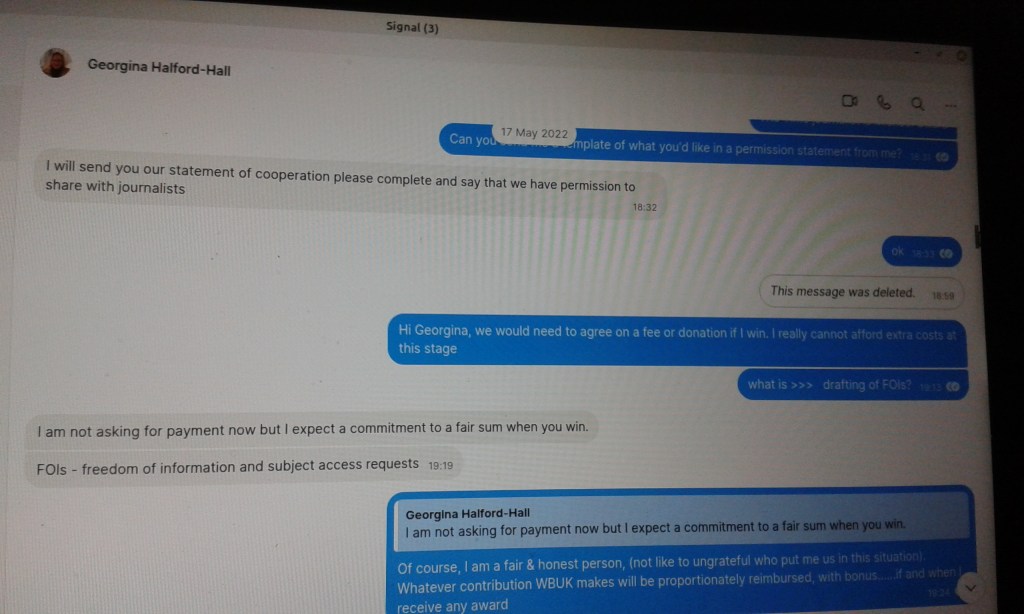
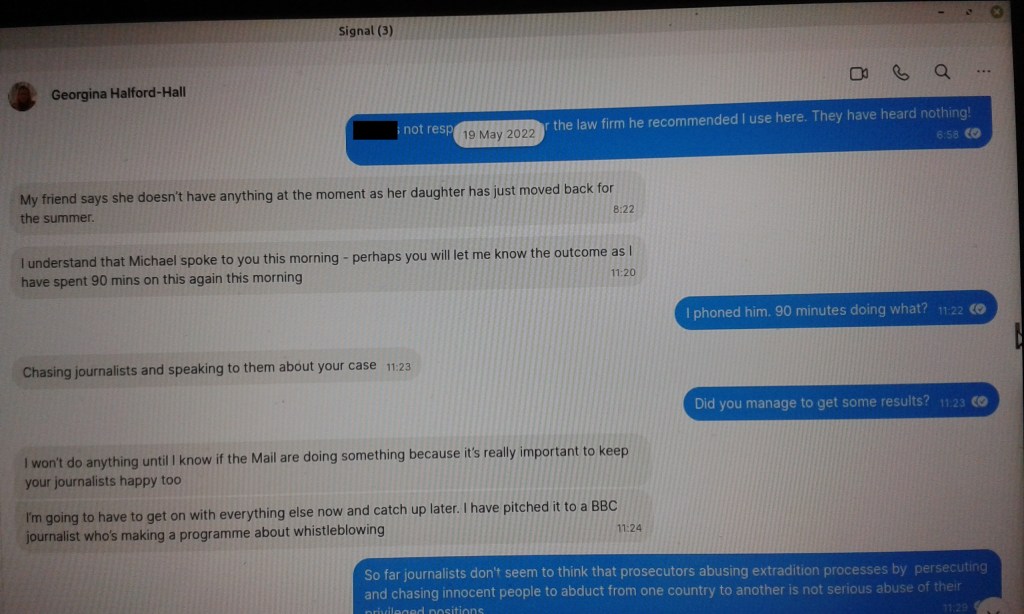
In the Signal messages, shared below, Halford-Hall appeared to document in detail how much time she was spending on the person’s case, as though it was a business service for which payment would be claimed (see photos 3 and 4).
The parties eventually agreed in these messages that payment for help would be deferred and eventually made in the form of a percentage of any financial award (see photo 2).
This is consistent with WhistleblowersUK documents which ask whistleblowers for money and a percentage of any settlements and awards.
Importantly, in the course of the exchanges, Halford-Hall appeared to compose a draft press statement to accompany this case, which claimed that WhistleblowersUK had written the pro bounty Bill which the Whistleblowing APPG and former APPG members have been repeatedly presenting to parliament:
“The Whistleblowing Bill written by WhistleblowersUK is working its way through parliament…..” (see photo 5)
If true, does this support concerns that the Whistleblowing APPG is a vehicle for private interests?
The US lawyers certainly funded the establishment of the Whistleblowing APPG, with Constantine Cannon LLP donating money which paid for WhistleblowersUK’s services as an external secretariat, and links continue to be evident. For example, a partner of Kohn, Kohn and Colapinto spoke at an APPG event earlier this year.
Moreover, in the Signal messages, Halford-Hall appeared to offer to “coordinate political help” (see photo 6).
Would it be right that services, for which WhistleblowersUK seeks to be paid, are entangled with our democratic processes?
There are strict rules which prevent members of parliament from representing anyone who is not a constituent. Does the Whistleblowing APPG in any way breach this principle, through its relationship with WhistleblowersUK, and any brokering of political influence by WhistleblowersUK?
WhistleblowersUK previously publicly stated on 22 July 2023 that whistleblowers who wanted their evidence to be presented to the government should submit via WhistleblowersUK, implying a special relationship:
I asked the Whistleblowing APPG Chair Mary Robinson about this and she denied that WhistleblowersUK had any special, formal role:
“Neither the APPG or WhistleblowersUK have any formal role in the collection of submissions or the terms and would submit their own evidence as they see fit to assist and inform the review.” From email 11 August 2023
I sent the photos of the May 2022 Signal messages on 4 September 2023 to Mary Robinson MP Chair of the Whistleblowing APPG copied to Baroness Susan Kramer, a former APPG member who employs Halford-Hall as a parliamentary researcher, to ask for confirmation and comment.
Neither have responded despite a reminder.
In the absence of a response, I am making key photos public and leave it with others to form an opinion:
WhistleblowersUK are now revealed as one of the parties who have been treated preferentially by Hollinrake’s department. WhistleblowersUK had a meeting with the Department of Business and Trade BEFORE official evidence gathering had begun.
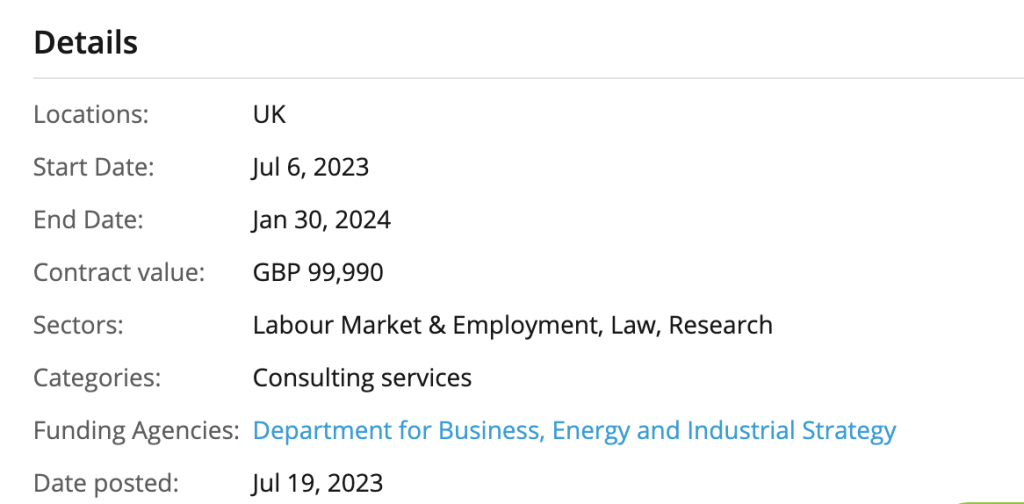
Because of months of government silence following the March 2023 announcement of Hollinrake’s review, and government failure to provide a means for whistleblowers to contribute, despite an announced intention to do so, whistleblowers started asking questions. These revealed that the government had outrageously outsourced the law review to a company, Grant Thornton. Not only this, Grant Thornton had prior contacts with the Whistleblowing APPG, WhistleblowersUK and US bounty hunting law firms.
The government also delayed a response to an FOI request about its review process, that was made two months ago, claiming that it needed time to consider possible exemptions to disclosure.
It has now responded (FOI2023/03987) revealing that the usual suspects were treated preferentially and met with the Department for Business and Trade (DBT) in the Spring, soon after the law review had been announced.
WhistleblowersUK, Protect and Parrhesia all had meetings with DBT about the law review.
WhistleblowersUK met with DBT officials on 6 April 2023, only ten days after Hollinrake announced the government’s law review.
Protect and Parrhesia met with DBT officials later on 4 May 2023.
Did these meetings in any way pre-determine the conduct of the government’s review, especially the first and very early meeting with WhistleblowersUK?
The Department also met with representatives from various institutions: TUC, Law Society and several Prescribed Persons.
Published material indicates that the closing date for the bid was 19 May 2023:
Astonishingly, there has been no formal announcement of the decision to hire Grant Thornton for this very important exercise.
When I asked Protect if they knew, they replied that they did not know and in the words of their CEO: “We had not heard any announcement about the appointment of a consultant to conduct the review and had hoped to meet with them first.”
It told me that I MIGHT be invited to contribute. Three days later I received an invitation from Grant Thornton, but that was not the point.
The government has disclosed via the above FOI response FOI2023/03987 that Grant Thornton will stop taking evidence in December 2023.
On 4 September 2023 I asked Grant Thornton for a copy of the questionnaire they said they would use to gather evidence. In response, Grant Thornton stated that their questionnaire had not been finalised:
From: Ali Crotch-Harvey <REDACTED>
Subject: RE: Invite to participate in the research study into the effectiveness of the whistleblowing protections in Great Britain
Date: 4 September 2023 at 10:16:03 BST
To: REDACTED
Hi
Of course.
We are just finalising testing the questionnaire through our internal quality controls to ensure it works, that we are happy with the wording of questions and its security, given the nature of what we are asking whistleblowers to share with us. We are aiming for this to be the case by the end of the week, so I will send you the invite link then.
In the meantime, let me know if you have any further questions or thoughts.
Kind regards
Ali
I have again asked for the questionnaire and await a response.
If Grant Thornton will stop taking evidence by December 2023, that does not leave much time for whistleblowers to be informed of the process and to contribute evidence.
How sound will this law review be, given that it is being conducted on a relatively limited budget, without proper publicisation and without being open to all whistleblowers?
Grant Thornton’s governance has been criticised by regulators and the company has been repeatedly sanctioned. There is also a question of conflict of interest arising from the fact that Grant Thornton sells whistleblowing compliance services.
The review is appears to be dominated by those with an institutional and/or market perspective from the whistleblowing compliance industry and by the bounty hunters.
Will the public interest be foremost?
Will evidence from whistleblowers whom the government would rather not hear be discarded?
Whistleblowers from non-financial sectors will be disadvantaged if the bounty hunters prevail in replacing current UK whistleblowing law with a model that is designed for and focussed on lucrative bounties from the financial sector. Will non-financial whistleblowers’ voices be muted? Is that what we really need after endless health and care scandals, such as the Letby killings at the Countess of Chester Hospital?
If free range whistleblowers, who have eschewed membership of the government’s favoured organisations, wish to submit evidence, I advise that you send it direct to the Secretary of State.
WhistleblowersUK’s website, on the “What We Do” page, states that the company advances dialogue through its community of associate members:
The company’s coffers may also benefit, as according to WhistleblowersUK’s associate membership application form, such membership costs a minimum of £120 per annum. Applicants are asked to agree to pay “donations”:
“I agree to make a minimum donation of £10 per calendar month [£120 per annum] to further the Company’s work to support whistleblowers.”
At the end of the document it is stated that people who cannot afford this can apply to WhistleblowersUK’s directors for a waiver.
Associate membership entitles individuals to be non-voting participants at WhistleblowersUK’s general meetings:
“I acknowledge that as an Associate Member I am afforded the right to attend and be invited to speak at General Meetings, but not to vote. I acknowledge that I am not a Member of the Company as defined in Section 112 of the Companies Act 2006.”
Associate membership of WhistleblowersUK also purportedly entitles individuals to a range of other benefits, including “Priority application to other services”, whatever that is.
Let us hope it does not relate to benefits in terms of access to power and “political help”.
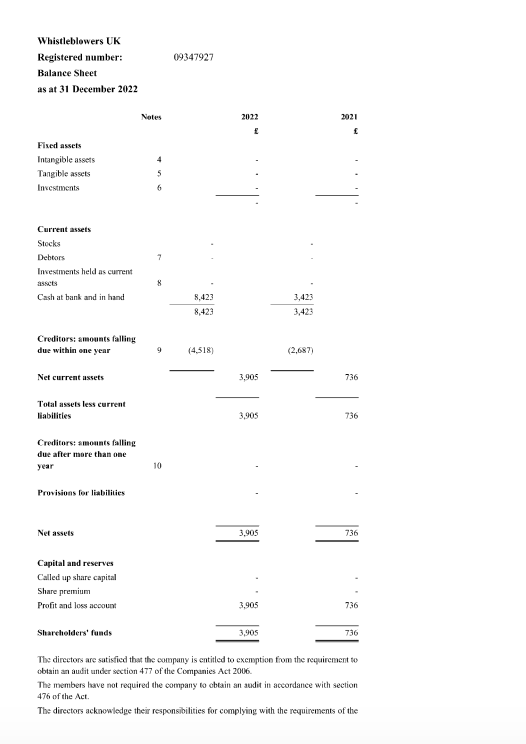
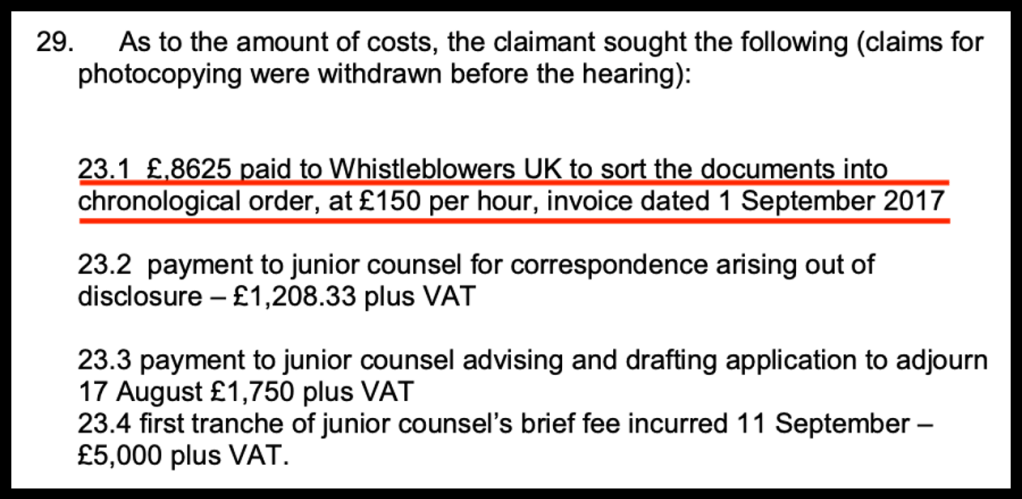
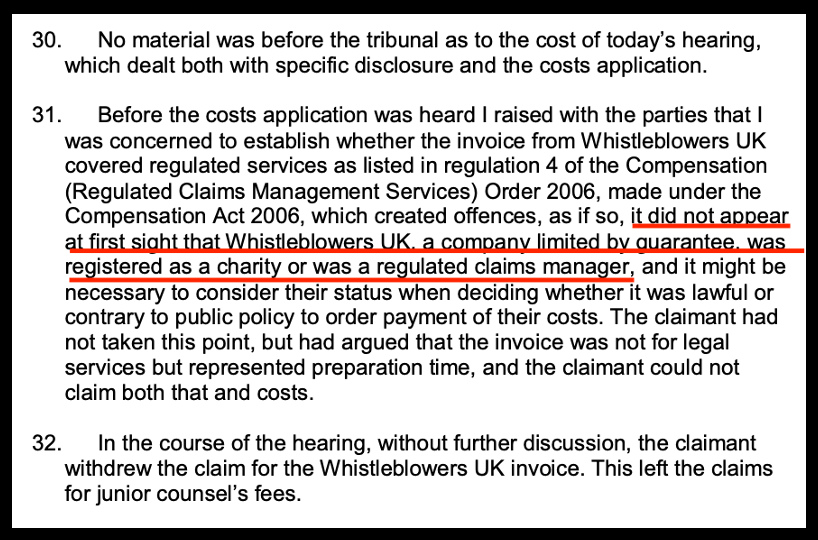
An invoice by WhistleblowersUK was submitted to the Employment Tribunal in a financial whistleblower’s case (Banerjee Case number 2200415/2017) which consisted of charging £150 per hour for arranging the whistleblower’s documents in date order, with a total bill of £8625.
The judge questioned the claim on the grounds that WhistleblowersUK is not legally recognised as a regulated claims manager, and the invoice was withdrawn by the claimant:
The government has also outsourced its review to a private contractor, Grant Thornton, which has been repeatedly sanctioned by the Financial Reporting Council in recent years. This seems a curious choice of reviewer for such a sensitive governance task.
There has finally been a partial response by the Department of Business and Trade.
I have responded to this. The hopefully self explanatory correspondence and uploaded supporting documents are provided below.
BY EMAIL
Kemi Badenoch
Secretary of State
Department of Business and Trade
4 September 2023
Dear Secretary of State,
Serious concerns about the government’s review of UK whistleblowing law, after the Letby killings
I write to respond to a letter from your department which was the first and only substantive response to issues that I have been raising since early July about the government’s review.
I write to express concern about the probity and transparency with which the government is currently conducting this review of UK whistleblowing law. Whilst such an exercise is well overdue, as existing UK law is highly flawed and has enabled cover ups for over twenty years, the current review is being conducted in a closed and unaccountable manner.
The Letby killings at the Countess of Chester Hospital have shown we truly cannot afford yet more flawed UK whistleblowing law.
The key parties controlling the government’s current review of whistleblowing law are Kevin Hollinrake MP and Parliamentary Under Secretary of State (Minister for Enterprise, Markets and Small Business) since 7 February 2023and Grant Thornton, who have been hired to undertake the review.
Grant Thornton had prior links with both the APPG and US bounty hunting lawyers, hosting an event by the APPG and its secretariat WhistleblowersUK earlier this year.
“The relevant minister is Parliamentary Under Secretary of State (Minister for Enterprise, Markets and Small Business) Kevin Hollinrake, whose Ministerial Portfolio includes whistleblowing.”
The Department claimed to me that its review will consider the experiences of whistleblowers:
“I would like to reassure you that the government believes it is vital that the experiences of whistleblowers are considered when examining the effectiveness of the whistleblowing framework”.
However, it has not made its review process open to all, and it has taken two months to answer any questions about the review process.
In reply to my question on how I or other whistleblowers can give evidence to the review, The Department replied that it is not publicly consulting.
The Department stated only that:
“The research study will include (i) a review of recent academic and relevant literature, (ii) examination and analysis of data related to employment tribunals and whistleblowing reporting by prescribed bodies, and (iii) undertaking several interviews and focus groups with various stakeholders to gather a broad range of perspectives, views and experiences surrounding whistleblowing.”
The Department suggested that IF I am contacted by Grant Thornton, I should engage with them:
“If approached, we encourage you to engage with them as fully as possible.” [my emphasis]
“We continue to welcome proposals for potential research participants, and we have flagged your interest to Grant Thornton.”
This is undemocratic and wholly unacceptable process. It smacks strongly of predetermination, controlled by vested interest.
I had already contacted Grant Thornton directly to ask them if I and other whistleblowers could contribute evidence to them, and I have been ignored for a month.
It is unedifying to watch the Department and Grant Thornton playing whistleblower football in this manner, especially as some whistleblowers may still be in a vulnerable state.
Moreover, the Department has both ignored and failed to answer my questions on whether there have already been meetings with and evidence accepted from other parties such as from Kevin Hollinrake’s former associates, the Whistleblowing APPG and its external secretariat WhistleblowersUK. This silence by the Department only adds to concerns about whether the review is an exercise in cronyism. This is especially as there are particular concerns about WhistleblowersUK, some of which I briefly address in the appendix below.
Most recently, I have been sent photos of messages, purportedly from WhistleblowersUK, which claim that WhistleblowersUK in fact wrote the Bill that the Whistleblowing APPG has been repeatedly presenting to parliament. I have passed these to the APPG chair for her comment. It is a concern if the claim is true, and equally a concern if it is not true.
The whole country has had the most painful reminder of what goes wrong when whistleblowing concerns are mishandled. The government has been forced to upgrade from a non-statutory to a statutory public inquiry into the Letby killings because of the level of public disgust and outcry. It is deplorable that the government is conducting a review of vital, vital whistleblowing law behind closed doors in this manner.
Whilst hiring Grant Thornton may have given the government an element of plausible deniability, it does not absolve the government of its basic duties. I attach a discussion document by whistleblower colleagues and I which comprehensively set out what an improved UK whistleblowing law could look like. Substantial elements of this were adopted by Philippa Whitford MP in the Public Interest Disclosure (Protection) Bill. Please accept this as an evidence submission to the review of UK whistleblowing law, on what changes should be made to the law.
For convenience, I set out in the appendix below highly summarised principles and key characteristics of the law changes which colleagues and I proposed. I also submit as evidence to the government’s review, various summaries and documents which show why the US bounty hunting model espoused by Kevin Hollinrake and his former APPG colleagues is harmful to the majority of whistleblowers and the public interest. The bounty model gives little value to life (such as in the Letby case) and is designed for recovering vast bounties from the financial sector. Its main effect is to generate huge profits for the private, lawyer-led bounty hunting industry.
In the context of a campaign in recent years to open up the UK market to US bounty hunting law firms, there has been a noticeable media presence linking Whistleblowing APPG members, WhistleblowersUK and US bounty law firms. For example, this is a 2018 piece quoting both Kevin Hollinrake and Constantine Cannon, the US bounty hunting law firm which funded the establishment of the Whistleblowing APPG in 2018, by paying for WhistleblowersUK’s services as external secretariat.
Please be under no illusion that lawyers advocating for a bounty model are acting in the public interest. They act in their own financial interest.
Whether or not Grant Thornton continues to ignore me and other whistleblowers who oppose the activities of the Whistleblowing APPG, WhistleblowersUK and the bounty hunting agenda, I expect the government to take our evidence into consideration. Please advise me if you will do so.
I would also appreciate it if the Department of Business and Trade could answer my questions that it has so far ignored, about parties with whom it (or its contractors) has already met and from which it has already accepted evidence. I think the silence so far speaks volumes, but my request for information requires either disclosure of this information or the production of a valid exemption under FOIA as to why the information cannot be disclosed. This is especially as my questions touched on whether Kevin Hollinrake’s former associates and fellow pro bounty players, have been treated preferentially. If so, the question arises of why this is the case.
The worst of all worlds for whistleblowers would be to end up with a model that is driven by perverse incentives due to monetisation, that is operated by actors with vested interests and who would not only not be independent from the government but even possibly complicit with it. That would be a terrible bear trap and not a safe harbour, which would utterly fail the public interest and permit more gross NHS scandals.
In my view, for any whistleblowing mechanism to have a prospect of success, it should not be under the government’s line of management. (For example, I reject some of the proposals that have been made for UK whistleblowing governance to be controlled by the Home Office or by a police agency).
There is no protection for whistleblowers without probity and trust, and the government’s current approach to its review of the law is not building any trust.
Public Accounts Committee and Health and Social Care Committee have reported on many failures of whistleblowing governance over the years, and also on the weakness of the law. It is time for genuine improvement.
UPDATE At the time of writing this letter, a letter has just arrived from Grant Thorntoninviting my participation. This does not change my above views. I think the government should make its review open to any whistleblower who wants to contribute. The government should also give whistleblowers the option of submitting directly to the Department if they do not wish to entrust any sensitive personal data to a private contractor which sells whistleblowing compliance services and has links with the Whistleblowing APPG and WhistleblowersUK.
Yours sincerely,
Dr Minh Alexander
Cc
Philippa Whitford MP
Kevin Hollinrake MP Parliamentary Under Secretary of State (Minister for Enterprise, Markets and Small Business)
Gareth Davies Permanent Secretary Business and Trade
Sarah Wallin Department for Business and Trade
Steve Donaghy Director Forensic, Grant Thornton
Ali Crotch-Harvey, Manager FSG, Grant Thornton
Standards Committee
Business and Trade Committee
Health and Social Care Committee
Public Accounts Committee
Keir Starmer Leader of the Opposition
Jonathan Reynolds Shadow Secretary Business and Industrial Strategy
Wes Streeting Shadow Secretary Health and Social Care
Steve Barclay Secretary of State Health and Social Care
Rishi Sunak Prime Minister
APPENDIX – EVIDENCE TOWARDS THE GOVERNMENT’S REVIEW OF UK WHISTLEBLOWING LAW
Summary of the attached, new proposed whistleblowing law
The document is set out in plain English and accessible to all. The principles and key elements of the new proposed law are to:
Promote and enforce good whistleblowing governance with early intervention and prevention, or at the very least, early arrest of reprisal;
Re-focus the system onto properly responding to the whistleblower’s concern and correcting wrongdoing, instead of making the whistleblower the problem, as the current law does;
Resolve conflict expeditiously and to minimise litigation and related waste;
Ensure fair restitution for loss but not rewards, and to deter reprisal with meaningful dissuasive measures that hold individuals to account, including criminal penalties for reprisal and failures to act;
Introduce a legal concept from other jurisdictions of “mobbing” in the workplace
Extend protection to third parties affected by reprisal against the whistleblower, such as family members;
Limited extension of protected groups to those who are not workers, but who may suffer significantly as a result of making public interest disclosures, such as patients and families in a healthcare setting. Suppression of concerns by patients and families, as well as staff whistleblowers, has contributed to many NHS scandals. We have most recently seen that families’ concerns about deliberate harm at the Countess of Chester were rebuffed.
Our proposal includes establishment of a central whistleblowing body outside of the government’s line of management, answering to parliament, with sufficient powers to execute and enforce the above.
The US bounty hunting model was originally a civil war exigency. When first introduced it was acknowledged that the Lincoln administration had to do business with criminal elements, if necessary, to protect its wartime procurements. Since introduction, the law has waxed and waned. For example, it fell into disfavour when abused in the past by scavenger parties launching “parasitic” claims on the back of government actions.
The current US bounty model is literally a type of lottery which abandons the majority of genuine whistleblowers who experience reprisal. It excessively rewards a tiny majority whose disclosures lead to recovery of large enough sums of money. Lawyers take a cut of the enormous winnings.
The model is designed for the financial sector but Kevin Hollinrake and his former associates on the Whistleblowing APPG proposed to introduce a pro bounty Bill to apply to ALL sectors, whilst repealing existing UK whistleblowing law. This is a threat to whistleblowers from health and care, and other non-financial sectors, who are already seriously exposed but would be even more at risk:
WhistleblowersUK and US bounty hunting law firms are now explicitly linked and united in their pursuit of a rewards model in the UK, as revealed in a recent joint paper.
The modern US bounty hunting model has, due to the vast sums involved, spawned regulatory corruption:
The CEO of Whistleblowers UK has pressed for all to be rewarded, including wrongdoers, if they provide information.
In the Deutsche Bank scandal, a whistleblower declined a reward and asked that it be passed to shareholders whom he believed had been unfairly punished for executive wrongdoing:
This is an example of a genuine whistleblower who suffered deeply from reprisal, including through bankruptcy, but perversely got nothing from the US bounty hunting system:
Please also be aware that WhistleblowersUK, the external secretariat to the APPG of which Kevin Hollinrake was a member, tries to charge whistleblowers money for services and to obtain a percentage of their awards and settlements. This is a recent version of the contract that WhistleblowersUK asks whistleblowers to sign:
These requests for payment are not mentioned on WhistleblowersUK’s website, other than a recently added fragment of a sentence which indicated that WhistleblowersUK’s services are “affordable”
I have been sent copies of messages from a case in which WhistleblowersUK apparently repeatedly and precisely told the individual how much time was being racked up on their case, implying that this was a business service. In the same exchanges, there is also discussion of future payment in the form of a percentage of any award. I have sent this material to Mary Robinson MP Chair of the Whistleblowing APPG for comment, copied to Susan Kramer peer and former APPG member, who employs the CEO of WhistleblowersUK as a parliamentary researcher.
Another individual informed me that they received an unsolicited call from WhistleblowersUK out of the blue, just prior to the publicised award of remedy in their case.
WhistleblowersUK has also publicly approached bereaved members of the public, which seems related to its bid to widely expand the definition of whistleblower to all members of the public. This is a necessary prelude to the introduction of US style bounty hunting.
I asked the Chair of WhistleblowersUK if the organisation would make its charging policy more transparent, but I was ignored.
I have also raised concerns with the Whistleblowing APPG about WhistleblowersUK’s handling of whistleblowers’ personal data, but I never received a response.
WhistleblowersUK have never addressed questions about finances and conflicts of interest that I put in 2019. This refusal to answer led to Normal Lamb’s resignation from the Whistleblowing APPG:
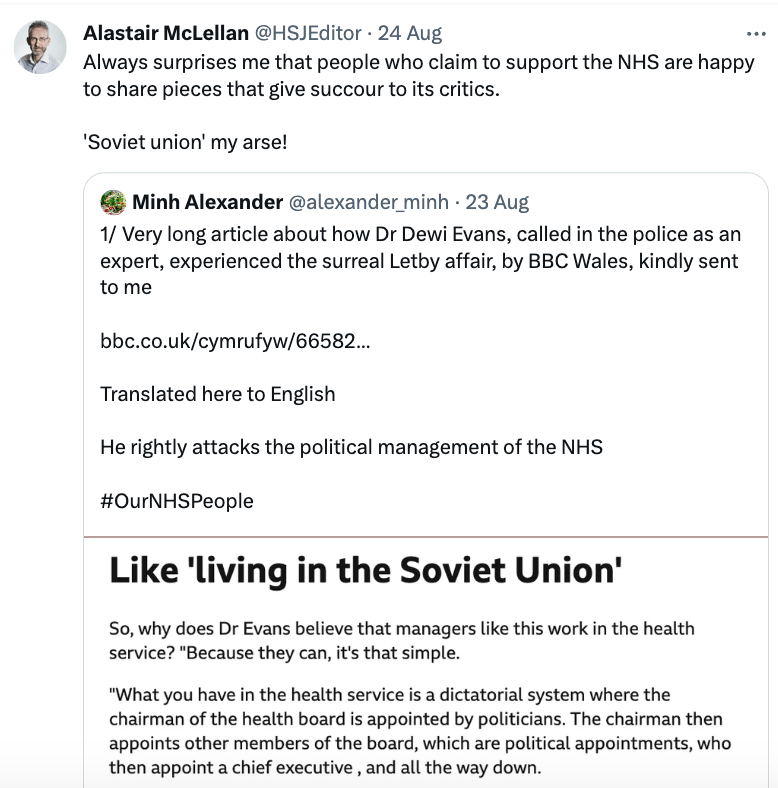
They believed it was a more profound criticism of the way our NHS is run than had been seen in any English media coverage. The article featured Dr Evans’ forthright comments about the problematic political management of our NHS, in which doctors suffered. He compared this with suppression of dissidents in the Soviet Union.
Other reviews have noted how NHS managers “look up”, ultimately to the Department of Health, instead of looking “out” to patients and communities.
I posted the BBC Wales article on social media, with an English translation of Dr Evan’s comments on the Soviet-like nature of a politically controlled NHS management culture:
“What you have in the health service is a dictatorial system where the chairman of the health board is appointed by politicians. The chairman then appoints other members of the board, which are political appointments, who then appoint a chief executive , and all the way down.
“So, the system is something I believe anyone who lived in the Soviet Union would understand very well.
“That’s what’s happening – they’re completely out of control, and I’m sorry to say that people I know, like doctors and consultants, have lost their jobs because they challenged our management, and of course the health service is a monopoly so if you lose your jobs in Wales or Britain, that’s the end of your career unless you’re willing to go work abroad.
“How in heaven can something like this happen? This is something very unusual. But in terms of system, things don’t work and there are problems in every department, in every hospital where there is a lack and negligence in terms of how we are looking after patients.
“And if you make a complaint and say that the system is not good enough (the whistleblowers) there is a risk of losing jobs, as their feelings are a threat to the managers who want to keep things quiet.”
Importantly, the BBC piece also noted that Dr Evans was strongly in favour of regulating NHS managers:
“Is it necessary to regulate Health Service managers as a result of this? “Without a doubt,” said Dr Evans.”
The government has now given in to overwhelming public pressure and announced a STATUTORY public inquiry into the Letby killings, so NHS managers will be compelled to give evidence. This should ideally include those who were party to a decision to apply an NDA to Tony Chambers the former CEO of the Countess of Chester Hospital NHS Foundation Trust.
Unexpectedly the Titanic editor of the Health Service Journal, then descended from the clouds to elegantly respond:
“Always surprises me that people who claim to support the NHS are happy to share pieces that give succour to its critics.
‘Soviet union’ my arse!”
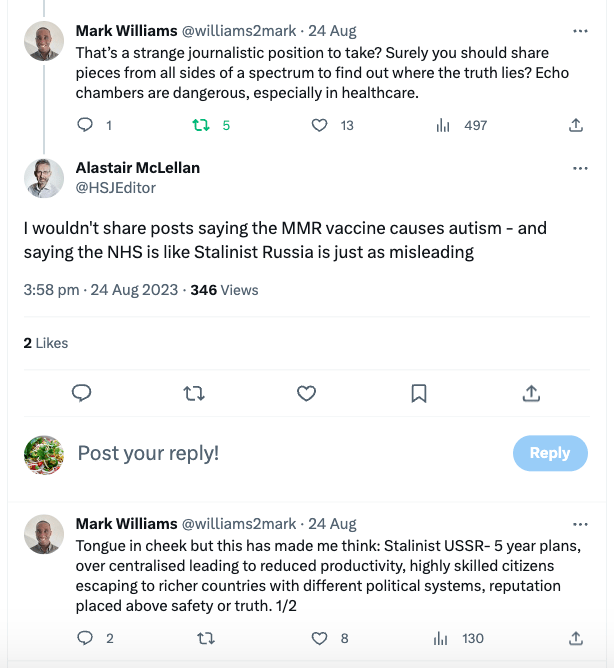
I responded with candour but sans anatomical references. Various other parties also stepped in to engage with the buttock waver. Some tried to reason, another compassionately sent him a suggestion for haemorrhoid relief.
Sadly, the buttock waver only added:
“I wouldn’t share posts saying the MMR vaccine causes autism – and saying the NHS is like Stalinist Russia is just as misleading”
The Tory politician Jacob Rees Mogg had similarly made such a comparison when publicly attacking another doctor in 2019, and subsequently had to apologise in the glare of national media coverage.
The buttock waver then fell silent and emitted no more.
As the Healthcare Service Journal describes itself as a product for healthcare leaders, one can understand that Buttock Waver might need to be attuned to his constituency.
It is ironic that an article which criticised NHS Stalinism was followed by a repressive response.
As in all self-respecting totalitarian regimes, the NHS hunts down and neutralises dissidents through unfair dismissals, gagging, and blacklists. Whilst along with the government, senior NHS managers have resisted a tracking database about their own misconduct, such as suggested by the 2019 Kark review, they have not objected to sharing information that results in NHS whistleblowers being blacklisted.
Between those who would tear down our NHS, and those who think they defend it by deterring debate about its faults, lies a reasonable ground of open learning, efficiency and improvement.
The NHS should stop using the blunt instrument of crude terror against its workforce, and should also dispose of its unfair disciplinary processes which have more in common with the Spanish Inquisition than modern HR practice.
Gulags need to give way to glasnost.
Part of the instruments of terror is the public protection of senior wrongdoers, which sends a very chilling message the workforce.
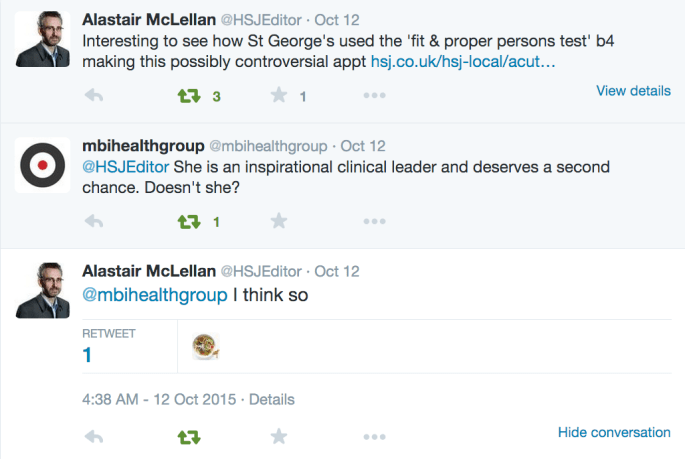
In a past social media exchange, the buttock waver agreed with another party that Vasco-Knight should be given a second chance:
Very shortly after being appointed as interim CEO at St. Georges, Vasco-Knight was charged and later convicted alongside her husband Stephen of defrauding the NHS. Vasco-Knight and her husband claimed they could not repay the full amount stolen. According to the NHS Counterfraud Authority, a proceeds of crime investigation revealed “assets that the couple had not previously volunteered to tell NHSCFA about, namely personal pensions”.
The cycle in Devon appears to continue.
Clare Sardari has asked her local ICB, Devon, to confirm reports of a controversial interim ICB CEO appointment, Allison Williams.
The RCOG concluded there had been “suboptimal” management, under-reporting of serious incidents and a lack of “basic governance”.
An important prior investigation report was not properly disclosed to RCOG investigators by the Health Board:
“An earlier report, prompted by the identification of the unreported SIs, was submitted to the Health Board in September 2018. This review was undertaken by a consultant midwife. The report provides an in depth review of the shortfalls of the service and has produced very similar findings to this report. The existence of this 2018 report was only discovered and made available to the assessors when on site. The significance attached to this report by the Executive Team and what actions have been initiated remains unclear.”
The RCOG found concerns about poor team working and probity in how managers were appointed, which the Health Board had reportedly ignored:
“They [staff] were also concerned about senior managerial posts being filled without advert or interview. They felt they had raised their concerns many times with no apparent response from the senior midwifery team or the Health Board Executive team.”
The RCOG baldly reported:
“The culture within the service is still perceived as punitive. Staff require support from senior management at this difficult time.”
Devon ICB has not responded so far to Clare Sardari’s enquiries, despite chasing. This is a reminder that she sent to the ICB on 30 August 2023:
“Please see my email below.
I am a Devon resident and would therefore would be grateful for an answer to my question below please.
– Has Alison Williams been appointed as the interim CEO of Devon ICB?
As you have stated your commitment to a citizens-led approach to health and care, I assume this also means that you will be open and transparent in your approach to questions and queries asked of you, by the residents of Devon, of which, I am one.
I look forward to your response.
Clare”
UPDATE: At the time of publication the ICB has finally responded and simply stated:
“We wanted to confirm that we have received your messages and colleagues will be in touch with a response as soon as possible.”
If it is correct that Allison Williams was appointed as interim CEO of Devon ICB, what does it say about NHS culture that the commissioning bodies are willing to recycle managers who have been criticised for presiding over punitive cultures, feared by staff?
Is that a little….Stalinist? Da.
And why has there been no announcement of Williams’ appointment?
Did NHS England realise, in the face of the public outcry over NHS managerial probity after the Letby verdict, that appointing yet another failed NHS executive would attract political shrapnel?
An FOI has been submitted.
I have also shared my recent experiences with BBC Wales and Dr Evans.
I did wonder about pitching this article to HSJ but on mature reflection decided against it.
UPDATE 1 SEPTEMBER 2023
Devon ICB Comms have today written to Clare Sardari to confirm that the ICB did indeed appoint Allison Williams the former CEO of Cwm Taf Healthboard who left in storm of controversy over badly handled baby deaths and bullying in maternity services, as the new interim CEO of the ICB. HOWEVER, it is reported that she has decided not to take up the post. It also revealed that Williams has in fact been working for Devon ICS for the past two years:
“Allison Williams has been working with the Devon system on a part-time basis for the past two-years supporting the recovery programme. In the interest of continuity of delivery and with the full support of the NHS Devon Board and local NHS Trusts, Allison agreed to extend her support to cover the interim CEO responsibilities for the brief period between Jane leaving and the new substantive CEO starting.
The proposed arrangements were communicated internally to staff in mid-August but no external announcement was made pending confirmation of the shortlist for the substantive post and the full suite of interim arrangements.
In the intervening period, circumstances have changed, which mean that Allison, who lives in Wales, is regrettably unable to commit to being present in Devon full-time as required of her in the role and as such will not be taking up the interim CEO position. Allison has been discussing this with colleagues over the last couple of weeks. Interim cover arrangements will be confirmed in due course.”
Was the Letby verdict and public outcry about poor NHS management appointments in any way a contributing factor?
There has been a cacophony of panicky messaging following the Letby murder verdict. Folks rushing about claiming that a statutory public inquiry is not needed, then swaying in the winds of public opinion, others U turning on trenchant resistance to disbarment of NHS managers for serious misconduct and managerial regulation. Some deflected attention to a voluntary charter for candour in public life after the Chester families signalled that they are seeking mandatory reporting. Fortress Department of Health has skilfully seen off many a past serious challenge and crisis. But will the naked failure of managerialism at the Countess of Chester prove too much even for the Denial Machine to contain?
Dr Minh Alexander retired consultant psychiatrist 30 August 2023
I have today responded to an article yesterday in the British Medical Journal by Bill Kirkup and James Titcombe which stated:
“Despite increased protection under the Freedom to Speak Up policy, introduced to improve staff confidence to raise concerns following a report in 2015…”
The following letter should hopefully be self explanatory.
1.Your comment: “Despite increased protection under the Freedom to Speak Up policy, introduced to improve staff confidence to raise concerns following a report in 2015…”
Could you kindly point me to what you believe has been the increase in protection conferred by the Freedom To Speak Up policy?
I am not aware of any policy of increased protection.
This is because:
a) The National Guardian has indicated that it is not the role of local NHS trust Freedom To Speak Up Guardians to advocate for NHS whistleblowers.
The National Guardian has gone so far as to publicly correct Freedom To Speak Up Guardians who interpreted their role to be one of advocacy. Two embattled Freedom To Speak Up Guardians at North West Ambulance Service NHS Foundation Trust were implicitly criticised in the National Guardian’s case review report for trying to advocate for and to protect NHS trust staff from the usual toxic ambulance management culture.
The situation has been something of a dog’s dinner as other Freedom To Speak Up Guardians have understandably also seen the role as one of advocacy, reflecting what was originally written in the report of the Freedom To Speak Up review about Guardians being appointed to support staff who had suffered detriment for whistleblowing. For example, this is a flyer from Shropshire Community Health NHS Trust referring to Freedom To Speak Up “Advocates”.
b) The National Guardian by policy does not help whistleblowers with detriment, despite this being a recommendation of the original 2015 Freedom to Speak Up policy by Robert Francis.
In fact, the National Guardian’s Office usually tells whistleblowers to go back to their trusts (as in the cases of Shyam Kumar and Dr Julian Campbell to name but two), or to go away and to only come back when their case processes (such as litigation in the Employment Tribunal) have concluded, before it will even consider their case for case review. This is what happened to Dr Jasna Macanovic, who went on to be fully vindicated, but without any help or protection from the National Guardian. And when the National Guardian conducts a review, this looks at systemic issues and by policy does not investigate whistleblowers’ concerns.
This system basically favours power and whitewashes whistleblowers out of the picture.
And of course, you will probably be aware of the appalling revelation that the Director of Nursing and Medical Director, who failed staff who raised concerns and the babies and their families at the Countess of Chester, were at one point the trust’s Freedom To Speak Up Guardians. I had in fact documented these appointments in 2017, as whistleblowers had been concerned that inappropriate appointments to Guardian posts would be made, as part of the power abuse that was likely with Robert Francis’ model. The relevant 2017 spreadsheet of NHS trust executives acting as Guardians can be found here. But the trouble is that whistleblowers are ignored, including when they raise concerns about bad whistleblowing governance.
If you are aware of any evidence of increased protection of NHS whistleblowers since 2015, please let me know.
But equally, in your own words, please also “listen to whistleblowers” when they say that the Freedom To Speak Up model is not fit for purpose.
In considering any response, please also be aware that the majority of issues raised with NHS Freedom To Speak Up Guardians have been confirmed by research to be low level gripes, and they do not meet the accepted definition of whistleblowing. Therefore, the information on detriment experienced by NHS staff contacting Freedom To Speak Up Guardians, as published by the National Guardian, is not a clean sample that relates only to whistleblowing. It is also data that does not come directly from whistleblowers but has been filtered and anonymised by trusts and has not been verified at source.
I consider based on research over the last eight years, that the NHS Freedom To Speak Up initiative has caused harm because it has delayed real reform. In some cases, it has allowed abusive organisations to pretend to be something that they are not, resulting in NHS staff putting themselves in harm’s way.
c) The NHS national whistleblowing policy refers to “protected disclosures”. This is merely a technical term which means that the whistleblower is potentially entitled to claim for retrospective compensation if they suffer reprisal as a result of making such disclosures. It does not mean they are actually legally protected from reprisal or that there is a mechanism to stop any reprisal.
2. Your comment:“Regulation of health service managers has been recommended but not implemented. The proposed Public Authorities (Accountability) Bill would place an enduring duty of candour on organisations and staff that is currently lacking; pending that possibility, health bodies’ adoption of the voluntary charter currently being signed by police forces and other bodies would be a start.”
I am unsure what such a voluntary charter would add, as we already seen that a statutory Duty of Candour under CQC Regulation 20 has self-evidently failed to give reliable transparency, because of the all the ongoing scandals in which there have been cover ups.
It is also worth noting that the 2017 Public Authorities (Accountability) Bill (more commonly known as the Hillsborough law) has a well-intentioned but not very strong clause on whistleblowing. An experienced fellow whistleblower and I in fact contributed to a symposium at the School of Law and Social Justice, Liverpool University, which was held to generate refinements to the Bill, including on whistleblowing. I was surprised at the published end result, which was:
“All public authorities shall have and publish a “Code of Ethics” which …provides reasonable protection for whistleblowers”
No non statutory code has ever provided protection for whistleblowers against a determinedly abusive employer. The NHS national whistleblowing policy, adopted as a result of the Freedom To Speak Up review, is living proof of that.
With best wishes,
Minh
Dr Minh Alexander
Retired consultant psychiatrist and NHS whistleblower
Cc Kamran Abbasi BMJ Editor in Chief
Editorials editor
RELATED ITEMS
Bill Kirkup told the media that in his experience non compliance was not an issue with non statutory investigations and that people were “ready and willing”. Review of the records shows that key witnesses did not cooperate with his investigations at Frimley and Liverpool Community Health. The relevant Department of Health director has been asked for definitive confirmation but has not so far replied. Why would the Department pursue a non statutory inquiry into the Letby killings if it has relatively recent experience of non-cooperation by key witnesses?
The conviction and imprisonment of Lucy Letby for killings at the Countess of Chester has set off a wider debate about the how the NHS is run.
A key issue is how NHS managers should be held accountable, given many scandals about failed managers evading accountability, being rewarded, and most crucially of all, being recycled repeatedly across the NHS to repeat harms.
The Labour Shadow Health and Social Care Secretary Wes Streeting has declared in favour of regulating managers.
Will this stand the test of time?
In 2007, Alan Johnson Labour Health Secretary placated the public, in response to a terrible NHS deaths scandal at Maidstone and Tunbridge Wells from poor infections control, by proposing to rid the NHS of incompetent NHS managers:
“…we need to ensure proper accountability throughout the system. In particular and as the hon. Gentleman suggests, we should be spotting these issues much earlier and getting rid of incompetent chief executives or chairpersons who, fortunately, are in the minority, rather than waiting for a report such as this, by which time, frankly, most of the damage has been done.”
This is the Healthcare Commission report on that disaster, which concluded that Clostridium difficile infections escalated without any managerial grip:
“….from October 2005 to September 2006 more than 500 patients developed the infection, and we estimate that there were approximately 60 deaths where C. difficile was definitely or probably the main cause.”
However, in 2009, Johnson appointed Cynthia Bowers the CEO of the notorious West Midlands Strategic Health Authority which was responsible for overseeing Mid Staffordshire NHS Foundation Trust, as the CEO of the newly formed Care Quality Commission.
Perhaps he should have taken his own advice from 2007.
I have written to Wes Streeting to ask for more information about Labour’s current position on NHS managers, such as whether Labour will support full regulation, and for ALL NHS managers, so that no room for evasion is left.
I have also flagged the need to address all the other regulatory failures in the NHS, including the CQC, Labour’s legacy.
BY EMAIL
Wes Streeting MP
Shadow Health and Social Care Secretary
28 [sic] August 2023
Dear Wes,
Your comments about regulation of NHS managers under a future Labour government
The Guardian yesterday quoted you thus:
“The case for a proper system of accountability has been made again and again. Labour will introduce this in office, and make sure those found guilty of serious misconduct are disbarred.”
The Guardian also wrote:
“The party said it would consult on the details of the regulatory system once in power, including the roles it should cover, the most appropriate regulatory body, and the competencies themselves. These would include responding to whistleblowing and empowering staff to raise concerns.”
“Any system will be proportionate and supportive and aim to deliver excellent management and leadership throughout the NHS,” the party said.”
I am glad to hear that in principle you support the concept of regulation for managers. May I ask if you have any policy outline in mind yet, as this is a subject dear to many people’s hearts.
For example, do you commit to a principle that any regulation of managers should be as rigorous as that applied to clinicians, and not a diluted affair?
“She has told health chiefs she wants an urgent meeting next week to consider whether formal regulation is the right response to the Letby case and look at whether systems for overseeing teachers and bankers could be models to follow.” [my highlight]
Teachers and bankers
From the 2019 Kark report, my understanding of the regulation of teachers and bankers, which Amanda Pritchard proposes to possibly adopt in the NHS, is that it is not equivalent to the stringent level of regulation applied to clinical healthcare professionals. Professional regulation of clinical healthcare staff requires compliance with standards and ongoing revalidation. Instead, the regulation for teachers seems to be a reactive model that primarily responds only to reports of the most serious wrongdoing. The Teachers Regulation Agency deals only with the very most serious misconduct and reflecting this, it can only recommend permanent prohibition. This means that if this model is followed, a number of NHS managers guilty of lesser degrees of misconduct, even if repeated, would still slip the net.
Also, I see that the Financial Conduct Authority’s Fit and Proper Person test does not define what training is “applicable” for a suitable senior manager. This is a far cry from the way in which the competency of clinical healthcare professionals is strictly defined and regulated.
Importantly, Kark also recommended that if a simple disbarment arrangement proved to be insufficient, the government should proceed to full regulation of NHS managers:
“On the evidence currently available to us, we have not at this stage recommended that the HDSC [Health Directors’ Standards Council – a body proposed by Kark] becomes a full ‘regulator of directors’, accrediting training, registering and regulating directors, and operating a form of revalidation process. But we do recommend that the design of the HDSC allows for a more extensive remit should that prove necessary”.
I would very grateful to understand more about Labour’s policy position and whether you will seek full regulation as opposed to the partial models for regulating teachers and bankers that NHS England is scrabbling to offer as appeasement post Letby.
The lack of a level playing field between clinicians and non-registered managers is a significant part of what has fuelled managerial abuse against doctors, nurses and other frontline practitioners.
Indeed, some abusive professionally registered managers have taken themselves off register to evade accountability.
Unregulated managers have been free to enact unsafe political orders and to provide useful plausible deniability for the Department of Health by suppressing evidence of failures to resource the NHS safely and failures of bad policy. They have not been bound by a statutory professional code to put the public interest and the needs of patients first.
If NHS managers are to be regulated, why should they be regulated to a lesser degree? Real action is needed, not the semblance of action.
Also, all grades of managers should be regulated, and not just directors, giving parity with the way in which clinicians are regulated.
If you leave some managers unregulated, it is quite conceivable that more of the dirty work will simply be commissioned lower down the chain of command.
Is Labour committed to regulating ALL NHS managers?
We have already seen some profound failures of the Care Quality Commission that was established by Alan Johnson, which seems to have done everything in its power not to investigate the concerns of patients, families and whistleblowers on the spurious pretext that it does not have a remit to investigate individual “complaints”. CQC in fact has power to investigate serious incidents under CQC Regulation 12.
As a serious example, CQC has still not explained itself properly in the case of Sally Lewis, whose terrible death by neglect (as determined by the coroner) it failed to investigate for two years. There is still a need to fully understand the catastrophic systems failures at CQC which led to this appalling, mission-critical departure from its regulatory duties. The CQC has so far simply said it does not know how it happened, and refuses to disclose more information. This is just not good enough.
The CQC is hard to distinguish from the NHS which it is supposed to regulate. There is an endless revolving door between the two, and routine use of specialist inspection staff drawn from the NHS in the form of “specialist advisors” and importantly, NHS trust executives advising on CQC’s Well Led inspections as “executive reviewers”. The latter are appraising their own peers in a small community. (There are just over 200 NHS trusts). Such a lack of separation is surely very damaging to regulatory impartiality and public confidence.
The CQC has handled Regulation 5 Fit and Proper Persons (FPPR) most shockingly. It has accepted the most dubious assurance evidence from regulated bodies and it has also misrepresented this to parties who have referred directors under FPPR. For example, CQC told me that it closed down an FPPR referral on David Rosser the former CEO and medical director of University Hospitals Birmingham NHS Foundation Trust, based on an “independent” report. This turned out to be a report by a subordinate trust employee who was not even a board member, assisted by a lawyer from a firm retained by the trust. The CQC later admitted that it should not have claimed that it was an independent report.
I think based on all the evidence to date, it would be fair to ask if club culture masquerades as regulation in the NHS.
The charade has seriously failed the public and harmed patients and staff.
It is of critical importance that regulators are properly designed to be effective.
It is also of vital importance that regulators are properly overseen and that existing regulators are cleaned up.
There is a yawning chasm of trust and probity to be repaired.
I hope to hear from you.
Yours sincerely,
Minh
Dr Minh Alexander
Retired consultant psychiatrist and NHS whistleblower
APPENDIX
These are the relevant excerpts from Tom Kark and Jane Russell’s 2019 review of the Fit and Proper Person test in the NHS, for Steve Barclay, which relate to the FCA and the TRA:
“Teaching Regulation Agency
11.30 We met with Alan Meyrick (Chief Executive Officer).
11.31 The TRA regulates the teaching profession by conducting misconduct hearings
and maintaining a database of qualified teachers.
11.32 The TRA takes action on receipt of allegations of serious misconduct pursuant to
the Teachers’ Disciplinary (England) Regulations 2012 as amended by the
misconduct is conduct that is fundamentally incompatible with being a teacher or
could lead to the teacher being prohibited from teaching. The TRA does not
concern itself with cases of less serious misconduct, incompetence or underperformance
(which it leaves for the teacher’s employer to deal with).
11.33 An allegation of serious misconduct is heard by a three-person panel who decide
whether there has been: (1) unacceptable professional misconduct, (2) conduct
likely to bring the profession into disrepute, (3) a conviction, at any time, of a
relevant criminal offence. If the panel decides that there has been conduct falling
into any of those three categories it makes a recommendation to the Secretary of
State and a senior TRA official decides whether a prohibition order is appropriate.
A prohibition order applies for life and where an individual is prohibited, their
details will appear on the prohibited list.
11.34 In very serious cases, an interim prohibition order is imposed whilst the case is
being investigated. There is a right of appeal against a prohibition order via the
Queen’s Bench Division of the High Court pursuant to Part 52 of the Civil
Procedure Rules. Under some circumstances and after a minimum period of 2
years, the Secretary of State may allow a teacher to apply for the prohibition order
to be removed following a recommendation from another TRA panel. The test
applied by that panel is whether the individual has demonstrated “clear and
unequivocal insight into misconduct that led to prohibition and the extent to which
they can demonstrate a clear commitment to adhere to and exhibit the personal
and professional conduct elements of the Teachers Standards”.
11.35 The TRA does not have the power to impose lesser sanctions than a permanent
prohibition order save for the possibility of review after 2 years.”
Kark gave this account of Financial regulation:
“Financial Conduct Authority
11.10 We met with Richard Fox (Head of Cross-Sectoral & Funds Policy) and David
Blunt (Head of Conduct Supervision).
11.11 The FCA regulates financial firms providing services to consumers and maintains
the integrity of the UK’s financial markets. It regulates 58,000 financial services
firms and financial markets in the UK and is the prudential regulator for over
18,000 of those firms.
11.12 Under the Financial Services and Markets Act 2000 (FSMA), the FCA can prohibit
any individual from performing a ‘specified function’. In 2014 and 2015 prohibition
orders were issued to 25 and 27 individuals respectively. The kinds of behaviour
that have in the past resulted in prohibition have been: providing false or
misleading information to the FCA (including information relating to identity, ability to
work in the UK and business arrangements); failing to disclose material
considerations on application forms such as details of County Court Judgments,
criminal convictions and dismissal from employment for regulatory or criminal
breaches; serious acts of dishonesty (for example which may have resulted in
financial crime); and serious lack of competence.
11.13 The FCA applies a statutory ‘fit and proper person’ test to assess whether
individuals are suitable to perform a controlled function. When considering fitness
and propriety the FCA assesses the individual’s honesty, competence and
capability and financial soundness. For senior positions, when assessing fitness
and propriety, regard must be had to the individual’s qualifications, competence,
their personal characteristics and whether they have undergone training. The FCA
may withdraw an approval where it considers that a person is not a fit and proper
person to perform the relevant function.
11.14 Individuals must submit a detailed application to the FCA in order that their fitness
and propriety can be assessed. The application form’s fitness and propriety
section asks questions of fact requiring a ‘yes’ or ‘no’ answer about particular
actions. Some questions include the word ‘ever’, meaning that the required
answers are not restricted to a specified period.
11.15 The FCA has mandatory requirements about regulatory references which came
into force on 7 March 2017 (referred to in Chapter 8). Regulatory references must
cover the past 6 years from current or previous employers including overseas
employees. Further, matters to be disclosed include breaches of the FCA Conduct
Rules, the PRA (Prudential Regulation Authority) Conduct Rules and the Conduct
Standards and Statements of Principle and Code of Practice for Approved
Persons where such breaches resulted in disciplinary action (which is limited to
formal written warnings, suspensions as a disciplinary sanction and dismissal).”
UPDATE 16 SEPTEMBER 2023
Wes Streeting has not yet replied to the question about whether he will commit to regulating NHS managers as rigorously as clinicians are regulated.
He appeared on BBC Newsnight on 13 September 2023, when he stated that Labour would implement existing recommendations. This suggests that he is only looking to implement simple, reactive disbarment as recommended by Kark.
I have written to Streeting with evidence of serious middle management misconduct against a whistleblower and asked him to consider full regulation of ALL NHS managers, which will control training, accreditation and ongoing professional development.
My letter and Streeting’s comments to BBC Newsnight and a letter by him to the NHS Confederation and NHS Providers can be found here:
Francis suggested on Newsnight that NHS employers are unaware of errant managers’ histories. By doing so, he drew a veil over what is an organised system of mutual protection and recycling, which has NHS regulators at its heart. The system even has a nickname, “The Donkey Sanctuary”.
The case of Paula Vasco-Knight exemplifies the collusion running throughout the system: