By Dr Minh Alexander NHS whistleblower and former consultant psychiatrist 8 April 2017
There is a big hole at the heart of NHS whistleblowing governance that is most likely there by design.
In reality, it’s nobody’s job to investigate whistleblowers’ concerns.
Of course, employers are supposed to.
But no one makes them do so.
Current UK whistleblowing law, the Public Interest Disclosure Act (PIDA) 1 , does not compel them to do so.
Instead, PIDA is focused on employment disputes. 2 This only serves to support poor employers’ main tactic of hiding whistleblowers’ concerns by focussing on – and sometimes manufacturing – employment disputes.
NHS regulators pay lip service to the need for investigation of concerns, but very often look the other way when whistleblowers report failures by their employers. 3
For good measure, the NHS regulator the Care Quality Commission also repeatedly maintains that it has no remit to investigate individual whistleblowers’ concerns. 4
When the government was embarrassed into ‘doing something’ about recurrent NHS whistleblower scandals, it came up with local Freedom to Speak Up Guardians and the National Freedom to Speak Guardian. Unsurprisingly, they too were specifically designed not to investigate whistleblowers’ concerns. 5
Sir Robert Francis, through his report of the Freedom to Speak Up Review, left investigation firmly in the hands of employers. 6
This was with a fig leaf proviso that employers could arrange external investigation where appropriate. 7 But investigations commissioned by and paid for by employers are hardly guaranteed to be independent.
There have been too many examples of such ‘independent’ investigations that proved to be little more than public relations exercises.
As a typical example, NHS whistleblower Hayley Dare reported that she was offered an ‘independent’ investigation by her former chief executive, but discovered that the investigator was in fact her employer’s solicitors’ hireling.
NHS whistleblower Hayley Dare’s statement to the Employment Tribunal:
https://www.dropbox.com/home?preview=Hayley+Dare+Witness-Statement.pdf

So, was this edifice of non-investigation arrived at by pure accident and incompetence?
That is most unlikely. Those clever folks at Whitehall know that investigation of whistleblowers’ concerns – about matters for which the government is ultimately responsible – is crucial to the public interest and to protecting whistleblowers.
Power protects itself. It follows then that if the status quo is to be maintained, investigation of concerns must be resisted and potential political embarrassment contained.
Genuine reform requires an enforceable legal duty upon employers to properly investigate whistleblowers’ disclosures.
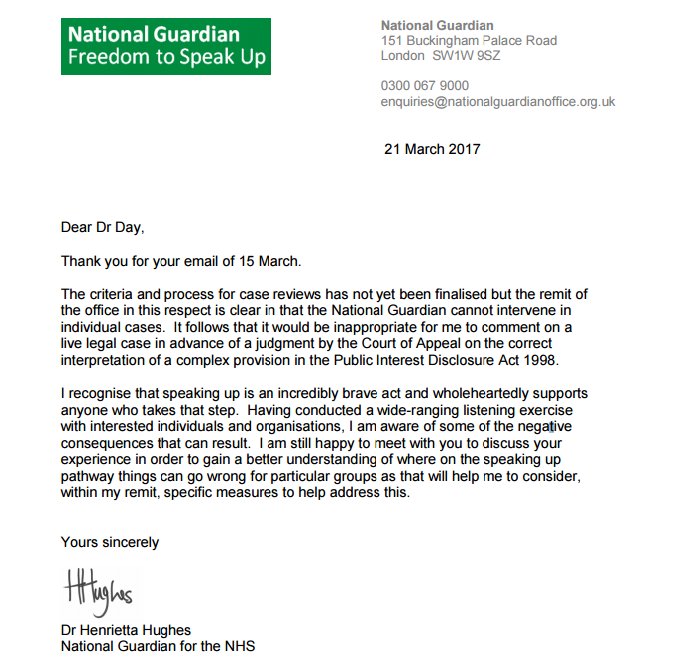
Will the much criticised National Guardian help ensure that concerns are investigated? Unlikely. Her current position is that her office will not seek law reform 8 and her office has quickly become part of the problem.
Will the just-launched Healthcare Safety Investigation Branch (HSIB) fully discharge its remit to ensure good investigative practice in the NHS 9 10 11, including of whistleblowers’ concerns?
After all, the Department of Health promised us:
“The Service [HSIB] will have the capacity to investigate only a small proportion of the many safety incidents that occur each year, and therefore a key part of its role will be to champion the need for good quality local investigations and lead on approaches that will enhance the capabilities of providers to conduct their own investigations. 9
I’ve seen little sign so far of serious interest and expertise at HSIB regarding whistleblowing. HSIB resisted meaningful engagement on whistleblowing and a meeting was only offered after lengthy correspondence.
I have put it to HSIB that it should closely examine failures to investigate whistleblowers’ concerns, and that it needs to openly consult with whistleblowers to tap into an important part of the NHS organisational memory on cover ups.
However, at the time of writing, there is no confirmation from HSIB that it will do so.
Also, HSIB indicated that it would publish its protocols for “dealing with whistleblowers” and repeatedly refused to share this material prior to publication. However, when HSIB became operational on 1 April and published its materials, I could find no specific documents on whistleblowing.
HSIB has also not yet responded to repeated questions about how it will discharge its Prescribed Person functions under the Public Interest Disclosure Act. HSIB has not even acknowledged its status as a Prescribed Person, which it must certainly have given that it is currently constituted as part of NHS Improvement, a Prescribed Person.
This is the relevant correspondence, which includes agreed records of a telephone meeting with the head of the HSIB intelligence unit about these matters on 24 March 2017.
Click to access hsib-correspondence-on-whistleblowing-records-of-meetimg-24-03-2017.pdf
HSIB’s hesitance to embrace whistleblowers is perhaps not surprising given that it seems to be under the DH thumb: a DH Deputy Director is currently seconded to HSIB as HSIB’s Director of Corporate Affairs.
Despite this DH embedment, HSIB claims:

Do note that HSIB seems to be whittling down its already restricted quota of 30 investigations a year. The official, public HSIB wording is “up to 30 healthcare safety incidents in England each year”. The conversation with HSIB on 24 March reveals that the intention is to carry out 25 investigations.
Until the gaping investigative breach – that literally swallows whistleblowers whole – is closed by effective law and a willing enforcement structure, expect more whistleblowing failures.
RELATED ITEMS
(1) Edna’s Law, proposed by the campaigning charity Compassion in Care, seeks to enforce investigation of whistleblowers’ concerns:
http://www.compassionincare.com/node/162
(2) https://minhalexander.com/2017/03/03/white-elephants/
(3) https://minhalexander.com/2017/03/12/national-guardian-behan-replys/
REFERENCES
1 Public Interest Disclosure Act 1998
http://www.legislation.gov.uk/ukpga/1998/23/contents
2 The Public Interest Disclosure Act does not protect whistleblowers and only gives them the right to sue for compensation after they have been harmed. It does not include any requirement upon employers to investigate concerns.
3 Whistleblowers unheard by the CQC. Alexander, Linton, Sardari and a fourth NHS whistleblower, December 2016 https://minhalexander.com/2016/12/05/whistleblowers-unheard-by-cqc/
4 Complaints matter, CQC report December 2014
https://minhalexander.com/wp-content/uploads/2016/09/cqc-20141208_complaints_matter_report.pdf
“People [whistleblowers] with historic cases also contact CQC in the hope that we can help resolve their concerns or hold a provider to account for its actions. While each case provides learning for us about the problems that can occur, and how we need to mould our new methods of inspection to detect similar problems and take effective action, we do not have the remit to resolve an individual case. As with complaints, we believe there is a regulatory gap in this area and we welcome the Freedom to Speak Up review, including its focus on historic cases.”
5 Robert Francis’ report of the Freedom to Speak Up Review February 2015
Page 19:
“78 The INO [National Guardian] will have discretion to consider how an existing case is being or has been handled, and to advise an organisation on any actions they should take to deal with the issues raised. The officer would need to operate in a timely, non-bureaucratic way. He/she would not take on the investigation of cases themselves, but would challenge or invite others to look again at cases and would need sufficient authority to ensure that any recommendations made were taken seriously and acted upon.”
Page 169:
“7.6.13 I want to emphasise that I am not proposing an office to take over the investigation of concerns. As I have already said, this needs to remain the responsibility of the local organisations.”
“7.6.17 The INO would in essence fulfil a role at a national level similar to the role played by effective Freedom to Speak Up Guardians locally. They would not take on cases themselves, but could challenge or invite others to look into cases which did not appear to have been handled in line with good practice or where it appeared that a person raising a concern had experienced detriment as a result of raising the concern.”
6 Robert Francis’ report of the Freedom to Speak Up Review February 2015
Page 167:
“7.6.2 There was considerable discussion in the written contributions about the potential role of an independent body to manage disclosures by whistleblowers. Some contributors were supportive of this option, others were unsure but thought it at least worthy of consideration. Most of the reasons given in support of this idea were related to mistrust of managers and internal processes which led to concerns that treatment of whistleblowers would be biased and prejudicial. “ Trusts cannot be left to mark their own homework.” 7.6.3 We were also told about the risks associated with establishing such a body. In particular, removing responsibility for dealing with the concern from local level to a more remote organisation could create delays, affect local ownership of issues, and require the establishment of potentially bureaucratic systems to allow the external organisation to investigate concerns. Equally importantly, there would be a real risk that serious patient safety issues may not be addressed sufficiently quickly locally, if someone reported them to an external body for investigation rather to their own organisation
7.6.3 We were also told about the risks associated with establishing such a body. In particular, removing responsibility for dealing with the concern from local level to a more remote organisation could create delays, affect local ownership of issues, and require the establishment of potentially bureaucratic systems to allow the external organisation to investigate concerns. Equally importantly, there would be a real risk that serious patient safety issues may not be addressed sufficiently quickly locally, if someone reported them to an external body for investigation rather to their own organisation.
7.6.4 These risks seem to me to be powerful arguments. It is certainly not my intention to propose anything which could in fact make the practical handling of patient safety concerns more complex rather than less so. I am therefore not minded to propose establishment of an external body to consider and investigate concerns. Primary responsibility for investigating concerns should remain with the local organisation taking into account the good practice set out in 6.4.”
7 Robert Francis’ report of the Freedom to Speak Up Review February 2015
Page 25:
“Principle 8
Investigations: When a formal concern has been raised, there should be prompt, swift, proportionate, fair and blame-free investigations to establish the facts.
Action 8.1: All NHS organisations should devise and implement systems which enable such investigations to be undertaken, where appropriate by external investigators, and have regard to the good practice suggested in this report.”
8 Letter from Henrietta Hughes National Freedom to Speak Up Guardian 16 February 2017
9 Learning not Blaming. Department of Health, July 2015
10 The National Health Service Trust Development Authority (Healthcare Safety Investigation Branch) Directions 2016
https://www.gov.uk/government/uploads/system/uploads/attachment_data/file/514217/HSIB_directions.pdf
11 Healthcare Safety Investigation Branch, website: http://www.hsib.org.uk/
“We investigate up to 30 health safety incidents each year in order to provide meaningful safety recommendations. We share what we learn across the whole of the healthcare system for the benefit of everyone who is cared for by it and works in it.
In this way, we can raise standards, improve patient safety and support learning across the healthcare system in England.
In essence we are here to:
- conduct thorough, independent, impartial and timely investigations into clinical incidents
- engage patients and relatives, NHS staff, and medical organisations in the investigation process
- treat the patients and relatives of incidents sympathetically and help them understand ‘what happened?’ and what’s being done to prevent similar events in the future
- produce clearly written, thorough and concise reports with well-founded analysis and conclusions that explain the circumstances and causes of clinical incidents without attributing blame
- make safety recommendations to improve patient safety
- improve patient safety by sharing the lessons learned from investigations as widely as possible
- raise the standard of local investigations of healthcare safety incidents by establishing common standards and skills development
In the future, we will act as global ambassadors for safety investigations.”