“9.17 Although the existing legislation is weak, I have not recommended a wholesale review of the 1996 Act for two reasons. First, I do not think legislative change can be implemented quickly enough to make a difference to those working in the NHS today. What is needed is a change in the culture and mindset of the NHS so that concerns are welcomed and handled correctly. If this can be achieved, fewer staff will need recourse to the law.”
Instead, he proposed his go-faster option of Freedom To Speak Up Guardians, which he insisted would be effective despite inherent conflicts of interest in the model and an embarrassing lack of evidence:
If a doctor used an untested medical intervention on a wide scale without controls, they would be referred to the GMC for putting patients at risk and they would be in breach of clinical governance principles of ethical use of resources. And rightly so.
To pull his house of cards together, Francis proposed a national office. Thus, the National Guardian’s Office was established in 2016. It had no teeth. An official from the Department of Health was placed at the Office. Successive figureheads with no clear whistleblowing credentials have been appointed to head the Office.
“2) How many of these compromise agreements require staff members not to disclose the existence of the compromise agreement itself?
All of the compromise agreements contain standard wording regarding confidentiality…. …
4) How many of these compromise agreements were entered into by the Trust with staff who had previously made public interest disclosures, (whether or not these were raised by formally invoking the Trust’s whistleblowing policy)?
Two compromised [sic] agreements were entered into by the Trust with staff who had previously made public interest disclosures.”
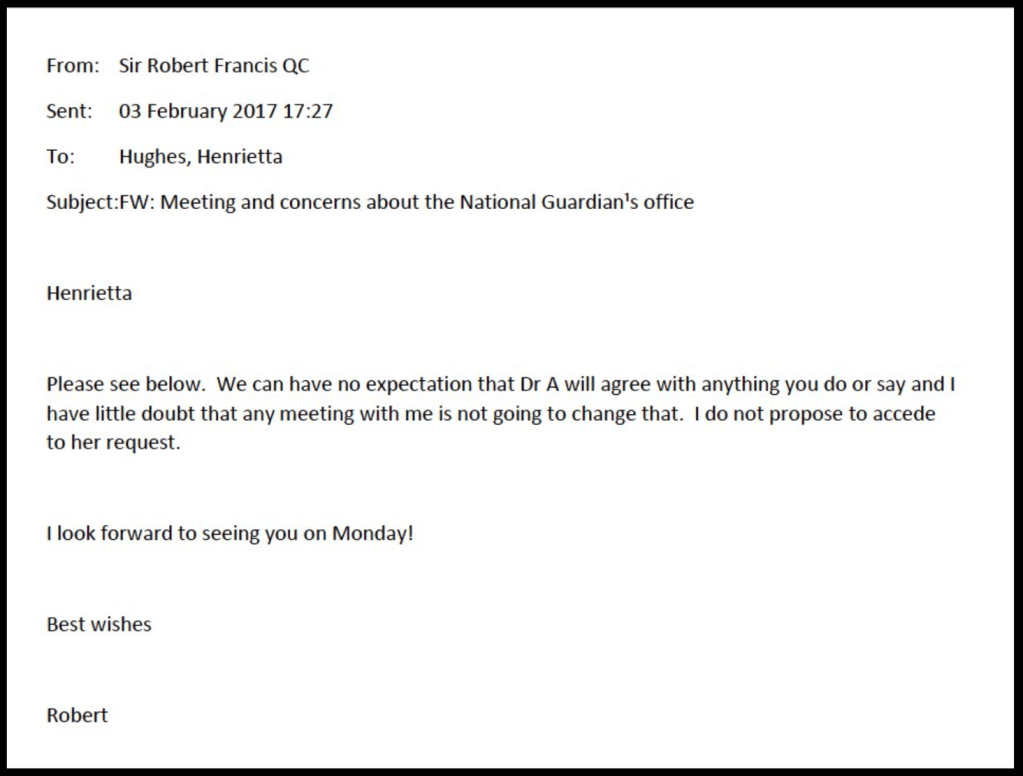
A subject access request also later revealed that the “independent” National Guardian asked the CQC for a “briefing” about me prior to this meeting. Well, there ain’t nothin’ like a Dame!
quest
Sills resigned before she even formally took up the National Guardian post, wasting huge head hunting fees, and with embarrassing headlines for the then Health Secretary:
Dr Philippa Whitford MP: “…..what comes back from whistleblowers I meet is they are concerned that the person who has been appointed is an NHS manager. We have to have someone who is utterly outside the system.”
Ben Gummer, Parliamentary Under-Secretary of State for Health Services: “The hon. Lady is also wrong to say that the national guardian was an NHS manager. She is one of the leading chief nurses in the NHS, and I am sad that she felt unable to continue with that role. The hon. Lady will be pleased to know that her replacement, Dr Henrietta Hughes, is also a clinician—a practising general practitioner.”
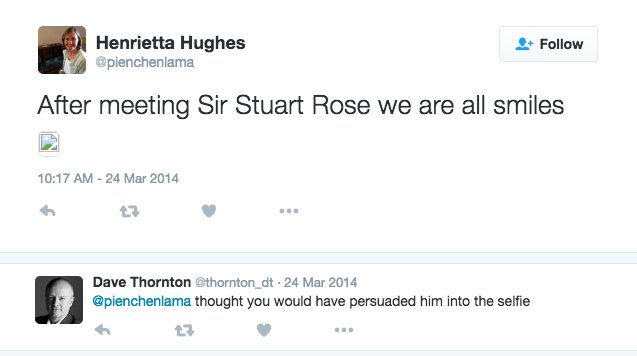
In her previous role, Henrietta Hughes had introduced a rule which made it compulsory for staff to smile, and she wrote about it.
After appointment as National Guardian, she gave an interview to The Times in which she opined that culture in the NHS would be better if staff were more cheerful:
It was not an emotionally intelligent start to a role which is about the good governance of receiving bad news from distressed people.
Hughes also deleted her twitter account before taking up her post, obscuring her cosy past interactions as a very senior NHS manager with other very senior NHS managers. But some digital shadows remained nevertheless:
eet
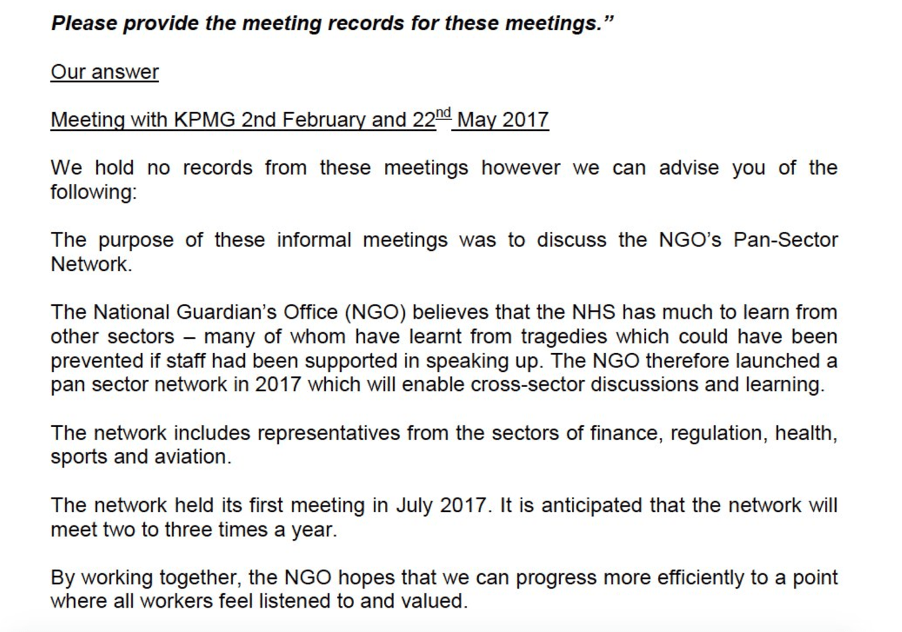
In her tenure, she paid for publicity, organised networking events which included questionable players from private industry & others and an FOI disclosure showed she did not always keep records of meetings with such players from private industry.
In 2018 she represented statistics favourably (used unpublished – against the UKSA code – by Jeremy Hunt for PR) in such a manner that the UK stats authority agreed she should be more precise:
UK Statistics Authority response 5 April 2018:
“We also note your concerns about the suggestion that some of the data are from the Freedom to Speak Up Guardian Survey Report. The presentation you referred to should have been clearer that the figures quoted on the same page as an image of the report where not in fact from this report. The report in question covers a different time period, and does not contain the information quoted.
We will write to the National Guardian’s Office to highlight areas that could be improved in their presentation and dissemination”
The latest National Guardian’s appointment was announced in November 2021. Dr Jayne Chidgey-Clark took up post on 1 December 2021. Hewn once more from the NHS management mother lode, Chidgey-Clark was previously a non executive director of Somerset CCG and also one of the CCG’s Freedom To Speak Up Guardians.
The press release about her appointment as National Guardian made sure to shake on some ‘Robert Francis secret sauce’:
“Dr Chidgey-Clark’s selection for appointment was made by a panel consisting of representatives from CQC, NHS England and NHS Improvement, as co-sponsors for the National Guardian’s Office. The panel also included Sir Robert Francis QC, whose Freedom to Speak Up Review instigated the creation of the National Guardian role.” [my emphasis]
But it is a matter of concern, not cachet, that there is a conflict of interest in Robert Francis being allowed to oversee – as a member of the NGO’s oversight board – a venture he designed and clearly continues to shape.
It contains reference to transformational and consultancy skills as follows:
“DirectorTHE JCC PARTNERSHIP LTD. · Self-employed THE JCC PARTNERSHIP LTD. · Self-employed Jul 2009 – Nov 2021 · 12 yrs 5 mos Jul 2009 – Nov 2021 · 12 yrs 5 mosServices: Transformational coaching, Interim management solutions, Health and Care Consultancy, Team development, End of Life Care Specialist
Providing consultancy solutions and interim senior management support to health and social care organisations and leading projects across health and social care. Providing exceptional executive transformational coaching and team development as well as organisational reviews.
A specialist advisor to the CQC. Able to help organisations to prepare for their CQC Inspection. [my emphasis]
Firewalk Instructor and Motivational Coach and Breath Work and Reiki practitioner.”
Of concern, it therefore appears Chidgey-Clark is one of those enterprising individuals who both offered services to the CQC as a specialist advisor for inspections and as advisor to organisations preparing to be inspected.
So how will she ensure that conflicts of interest are handled in a post that is centrally about probity?
And how many ex-CQC workers have now passed through the National Guardian’s Office?
Chidgey-Clark has written a first blog as National Guardian, which in 780 words does not say a great deal.
To find more specifics, I asked Somerset CCG for information about her previous role at the organisation.
The most startling fact which emerged from this is that Chidgey-Clark received a mere TWO whistleblowing disclosures as a Freedom To Speak Up Guardian.
This is the material disclosed by Somerset CCG via FOIA:
But do just two cases represent suitable experience for a national role?
Nevertheless, Chidgey-Clark’s experience seemed to impress Andrew Morris, who represents NHS Improvement, one of the funders of her Office:
“Sir Andrew Morris OBE Hon FRCP, Interim Chair of NHS Improvement said:“I welcome Jayne’s appointment to the National Guardian’s Office where her skills and experience will be invaluable in further developing the work of Freedom to Speak Up Guardians. On behalf of NHSE/I, we are looking forward to working in partnership with Jayne.”
In previous rounds of recruitment, knowledge and expertise of whistleblowing were not featured in the person specification for the National Guardian post, which speaks volumes.
Knowledge and expertise were probably not required this time either.
I invited comments from both the CQC about who was the appointing officer, their due diligence in the appointment process, and I also invited comments from the National Guardian’s Office, but neither have so far commented.
I had also recently renewed my enquiry to Robert Francis, post Ockenden Report revelations about gross and ongoing NHS suppression, about whether he was ready yet to withdraw the Freedom To Speak Up project and support whistleblowing law reform. I pointed out that some are calling for yet another independent review of NHS whistleblowing, which does not reflect confidence in the success of his project. I also drew his attention to the fact that the numbers of NHS staff filing whistleblowing employment tribunal claims seems to be fairly stable, disproving his suggestions in 2015 that his model would reduce the need for recourse to the law. Again, there has not yet been a reply.
Silence seems a fitting epitaph for the Freedom To Speak Up project.
Is Chidgey-Clark a master practitioner of Neuro-linguistic Programming?
I recall seeing online reference to this but did not make a note of it. Others commented online. Some posted a link to Somerset CCG’s website. The website link is no longer functioning. I asked Somerset CCG about this, who simply said they removed Chidgey-Clark’s profile entry after she moved to the National Guardian’s Office, but did not deny that it featured an NLP qualification.
NLP is a controversial coaching/ therapeutic intervention. One rating exercise carried out with mental health professionals saw NLP rated below Angel Therapy and Past Lives Therapy:
On 20 April 2022 the CQC made the following comments in response to question about Chidgey-Clark’s sum experience of two whistleblowing contacts as a CCG Freedom To Speak Up Guardian, who the CQC appointing officer was and what due diligence they took in the process:
“Hi Dr Alexander,
Please see our comment below as requested.
A CQC spokesperson said: “A multi-stage assessment process was conducted prior to the appointment of the National Guardian for Freedom to Speak Up in the NHS, to ensure the relevant knowledge, skills and experience were identified in the appointable candidate. Dr Chidgey-Clark’s appointment was made by a panel consisting of representatives from CQC, NHS England and NHS Improvement, as co-sponsors for the National Guardian’s Office. The panel also included Sir Robert Francis QC.”
Many thanks
Maryellen”
On 19 April 2022, the National Guardian’s Office made the following comment about Chidgey-Clark’s sum experience of two whistleblowing contacts as a CCG Freedom To Speak Up Guardian:
“Dear Dr Alexander,
Thank you for your email.
Dr Chidgey-Clark was recruited through the process set out by the CQC. You can find details of her announcement as National Guardian on our website here.
….Kind regards,
Ellie Staite”
PETITION
Please click and add your signature to this petition to reform UK whistleblowing law – whistleblowers protect us all but weak UK law leaves them wholly exposed and it is a threat to public safety
In his 2013 Midstaffs recommendations Robert Francis recommended that whistleblower reprisal should be criminalised. In giving evidence to parliament in 2014 he opined that CEOs who victimised whistleblowers should be sacked to set an example and discourage others. By 2015, after he was knighted and on the board of the CQC, he faintly derided contributors to the Freedom To Speak Up Review who had asked him to consider criminal sanctions.
Sir Robert changes policy on whistleblower reprisal
By Dr Minh Alexander retired consultant psychiatrist 9 April 2022
Summary: The ambiguous organisation Protect which sells whistleblowing compliance services to industry has called for yet another independent review of whistleblowing in the NHS. Such a review is fraught with risks for future whistleblowers from all sectors, and can obstruct real change. Any such review will need to be carefully negotiated. Whistleblowing touches on power and where there is power, there will be manipulation. Whistleblowers will need to be well informed and prepared, and stand their ground. The public interest is the priority. Genuine whistleblowers will need to do what they can to protect whistleblowing from more political abuse and deflection, or exploitation as a means of personal gain and profit.
Yesterday the organisation Protect which receives money from many employers including NHS organisations, for whistleblowing compliance services, issued a statement calling for yet another independent review of speaking up in the NHS.
“We are calling for an urgent review of speaking up in the NHS. NHS staff should be enabled to come forward freely and talk about their experiences in detail. In our experience, whistleblowers and would-be whistleblowers often have a clear insight into the problems, and potential solutions. Protect’s preference would be for the Health Select Committee to conduct this review, this could be done urgently, independent of Government and, if necessary, the use of Parliamentary privilege could be used to enable evidence and testimony to be gathered without legal repercussions for those involved.”
The purported trigger for Protect’s call is the report of the Ockenden Review on maternity safety failings, which is actually an obfuscatory piece of work where whistleblowing is concerned, but more on that another time.
Protect is part of the establishment whistleblowing furniture
In predecessor form, Protect was midwife to the UK’s highly flawed whistleblowing law the Public Interest Disclosure Act. Anyone can make a mistake, and law making of course always has to involve compromises, but Protect then failed to whistleblow on the law’s failures for many years. This was despite the organisation regularly hearing from whistleblowers and its seat on the Employment Tribunal national user group. Perhaps the seat was too comfortable. Protect promotes the odd high profile case, to its mutual benefit, but has been known to tell some whistleblowers not to bother and to run, even when they were shown later to have a case. Presumably Protect does so because it knows the law is weak. The law that it did not whistleblow on, that is.
Protect’s former head of legal has also been working at the National Guardian’s Office for some years now, such is the tangled web of the whistleblowing industry.
There were TWO ineffective reviews of whistleblowing in the NHS published seven years ago, which seriously failed both whistleblowers and the public.
Firstly, the well known and now much derided Freedom To Speak Up review by Robert Francis which holds no credibility amongst whistleblowers, and has failed so many patients.
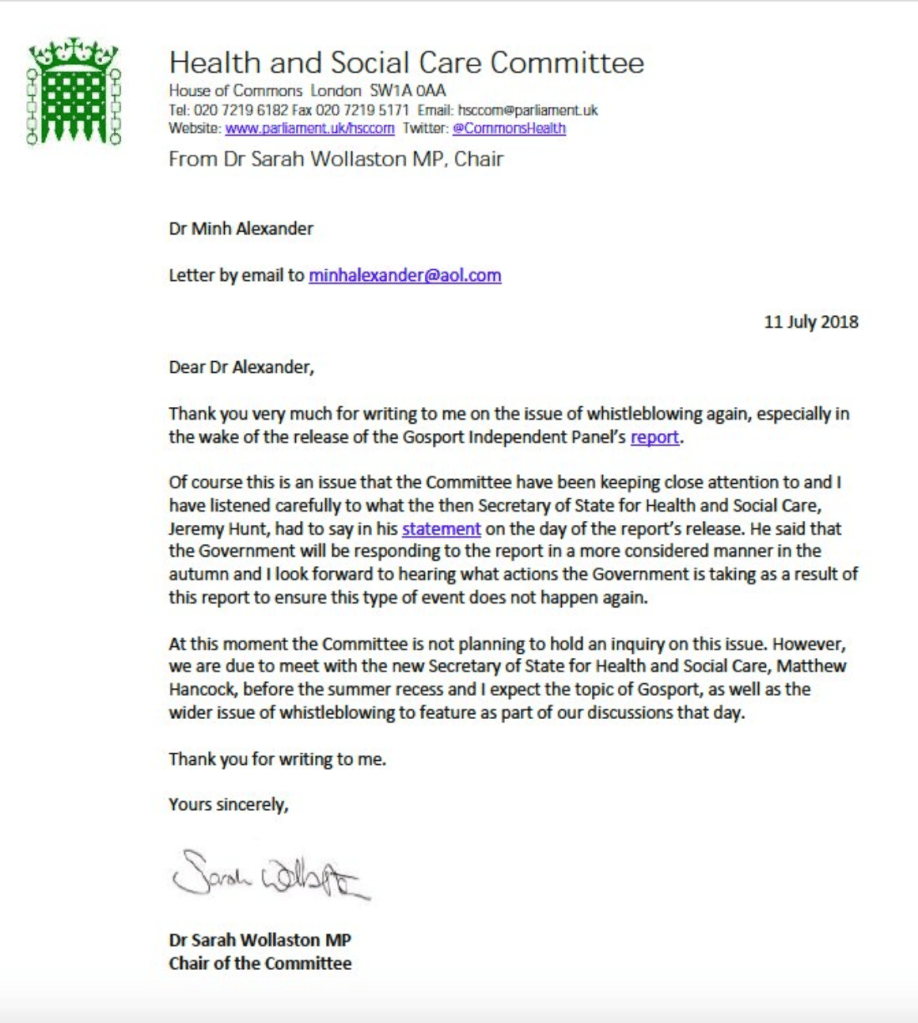
The other is the less remembered but equally reprehensible review by the parliamentary Health Select Committee headed by a then Tory chair. This was released ahead of the Francis report and was little more than platitudes and pulled punches. But it provided nice headlines and a photo op:
The same committee chair was later overheard by whistleblowers sympathising with David Behan CEO of the Care Quality Commission over negative publicity due to a critical Times letter by whistleblowers. The letter was issued partly to highlight research about CQC’s whistleblowing failures – hard evidence actually submitted to the Committee, not that it seemed to cut much ice with the Chair.
For years after the Freedom To Speak Up Review report, the same Committee Chair refused to hold any hearing into the ever more obvious failures of the Freedom To Speak Up project or the failure of the NHS to meet the sparse and loose recommendations of her 2015 review. This refusal continued after the publication of the Gosport Inquiry which showed that hundreds of killings of NHS patients could have been avoided if whistleblowers had not been intimidated and silenced early on.
Instead, friendly private meetings with the National Guardian were preferred over a public hearing with testimony from whistleblowers on an equal footing.
A Committee hearing is needed but one difficulty now is that the Health and Social Care Committee is chaired by Jeremy Hunt former Health Secretary. How will he review his own handiwork, the Freedom To Speak Up review, expressly designed to leave NHS whistleblowers entirely at the mercy of their employers? Let alone deal with the evidence from many whistleblowers who made disclosures to him but were fobbed off, as is de rigueur for the Department of Health and Social Care. Hunt should never have been allowed to take charge of the Committee due to the obvious conflict of interest as a recent past Health Secretary. Any review by him would not be truly independent.
But a parliamentary review would still be better than another flimsy effort entirely controlled by the government, in the way that the Freedom To Speak Up review was. Down to the dirty tricks on the launch day of sending whistleblowers to a different venue, miles away from the press conference held by Francis.
The great risk of any review, greatest with the latter fly by night type, is that the government will simply use it to generate another smokescreen of non-actions, to delay and to avoid real reforms. A mark II Freedom To Speak Up review will not only greatly hurt NHS whistleblowers, but whistleblowers in all sectors. It would be used by the government to avoid any discussion of UK whistleblowing law reform, which is the real solution needed.
If any review does materialise, the first wrestling match will be the terms of reference, which is where the seeds of deliberate inefficacy are usually sown.
Also, the whistleblowing scene draws a mixed crowd of secondary characters, which also poses risk to reform at times of possible change. Sometimes well meaning but temporary and ill informed actors pass through in a cloud of misdirected outrage, and ask for superficial interventions that will make little or no difference. For example, minor interventions aimed at the Employment Tribunal when whistleblowing cases should not actually be handled primarily as employment matters. And there are also carpet baggers using the whistleblowing label for publicity or seeking to profit or carve out careers, often driving debate towards financial incentivisation of whistleblowing, or models which maximise conflict and litigation and so generate income for middle men. Behind them stands a multi-billion US business trying to break through into the UK market.
Genuine whistleblowers need to tread a careful path through this morass of politics, backfires, distractions and vested interests to achieve anything of substance for those who come after. I advise that if you decide to engage, do so on clearly informed basis. Do your own research. Accept no second hand information. And do not just submit evidence into any review process and leave it with others to write the punch line.
Instead, ask the government for evidence based solutions. Ask for things that will make a measurable difference and can be auditable. Ask for specific things that the system must do. For example, I recommend that people ask for real reform of UK whistleblowing law, and set out what this means, even if briefly.
TOOL BOX AND RESOURCES FOR REQUESTING LAW CHANGE
These are some aids at varying levels of detail for those who wish to ask their MPs or submit evidence to parliament in support of whistleblowing law change
The law should: 1) Make it compulsory for whistleblower’s concerns to be investigated 2) Ensure that there is a legal duty by employers and regulators to protect whistleblowers from the point at which they whistleblow 3) Include meaningful penalties for individuals who victimise whistleblowers, including criminal sanctions for serious reprisal.
This is a detailed draft law by whistleblowers with many ideas for how an alternative model of law and whistleblowing governance could work. It borrows from the US Office of Special Counsel which is an agency for federal whistleblowers which has principles of fair restoration and proactive, lean resolution. This may include expunging unfair disciplinary findings or unfairly lost seniority. This is very different to the bloated, litigious post hoc response currently imposed by UK law on whistleblowers. Again, there are references for those who want to read more. What could a new whistleblowing law look like? A discussion document
This is a good practice example whistleblowing Bill laid on the parliamentary record by Dr Philippa Whitford MP, to serve as a resource. It introduces many of the standards that are being introduced in Europe under the EU directive, such as criminal sanctions for cover ups and reprisals. Importantly, it takes whistleblowing outside of employment law. A new UK whistleblowing Bill and a petition to the UK government to strengthen protection
Declaration of interest: It is ancient history now but I should declare that I made a disclosure to Jeremy Hunt about NHS regulators ignoring my patient safety and governance whistleblowing at that point, and pretending that all was improved. This roughly coincided with the start of a series of eating disorder deaths with common features of organisational failings that finally led to a critical inquest with national recommendations.
PETITION
Please click and add your signature to this petition to reform UK whistleblowing law – whistleblowers protect us all but weak UK law leaves them wholly exposed and it is a threat to public safety
A perfect, clear cut example of why UK whistleblowing law – PIDA – is completely unfit for purpose. The case of a gold standard whistleblowing case, Tribunal tested and fully upheld – which still resulted in a six year ordeal of persecution and harassment for whistleblower Dr Jasna Macanovic consultant renal physician and very importantly, still left patients unprotected.
By Dr Minh Alexander retired consultant psychiatrist 6 April 2022
This is a very brief post primarily for NHS Ambulance trust staff.
The National Guardian’s Office (NGO) website had a notice that it had an upcoming thematic case review on ambulance trusts but provided no details.
I submitted a Freedom of Information request to find out more.
The NGO has today responded minimally.
It is now clear that the NGO has shockingly been dragging out this piece of work since June 2020, when it seems was first discussed at its Advisory and Liaison Board. This committee consists of Robert Francis CQC NED, Andrew Morris, then NHS Improvement NED and now Chair and the National Guardian. (Incidentally, the name of this committee has been softened – it used to be the Accountability and Liaison Board – but who likes to be accountable?)
“This was first discussed with our Advisory and Liaison Board in June 2020.”
It is very hard to understand why the NGO has not given this work greater priority in view of the great difficulties faced by ambulance trust staff.
I asked the NGO for any analyses of whistleblowing in ambulance services carried out by the NGO to date. It seems none have been done save for the routine ‘Speak Up’ index material that is done for all trusts.
Moreover, the NGO has received only twelve public interest disclosures from NHS ambulance trusts in the four years from 1st April 2017 to 31st March 2021.
This is despite the well known staff relations troubles in ambulance trusts across the country and publicised staff whistleblowing to the press.
Importantly, reportedly, none of these twelve whistleblowing disclosures to the NGO came from ambulance trust Freedom To Speak Up Guardians in this period. That is, the people in ambulance trusts with responsibility for advocating for whistleblowers and escalating their concerns until they were resolved, apparently did not do so despite the severe problems and the staff deaths such as at East of England.
The NGO has for the time being ducked disclosure of all the documents that I have requested about the thematic case review by hiding behind Section 22 FOIA – documents intended for publication – even though I have asked for some documents that are not intended for publication.
As the NGO now claims it will be publishing review documentation “in the near future”, I will wait for publication and then pursue any outstanding data that the NGO fails to disclose.
The figures about ambulance staff disclosures to the NGO are not correct. There is at least one case missing from the stats. I have written to the National Guardian about record keeping by her Office.
“BY EMAIL
Dr Jayne Chidgey-Clark National Guardian
6 April 2022
Dear Dr Chidgey-Clark,
Record keeping and case files at the National Guardian’s Office
Thank you for the FOI response from your office regarding the planned thematic case review on ambulance trusts.
I believe on cross checking, including with the whistleblower in question, that your data about qualifying disclosures received by your office from ambulance trusts is incorrect, and that you are missing at least one more case from your stats.
I am rather concerned about how cases are logged and recorded. This is especially because incomplete records were an issue that arose previously in a matter of broken whistleblower confidentiality. That earlier matter was the subject of an upheld complaint against the National Guardian’s Office.
There seems to be an overlap in the NGO personnel who handled the case now missing from your stats and the earlier incompletely recorded case which led to an upheld complaint.
Is it possible to have some reassurance about the standards for record keeping and case file protocol followed by your office, including how telephone calls are logged and emails are filed? Are there written standards and expectations?
Many thanks,
Dr Minh Alexander”
UPDATE 8 APRIL 2022
I received a comment on this blog from a someone who would like to be anonymous. By agreement, this is a redacted version of what they wrote:
“Hi Minh
Very interesting article about the NGO and ambulance trusts, thank you.
[REDACTED SECTION]
You may be interested to learn that the Freedom to Speak Up Guardian at REDACTED Ambulance Service Trust has now resigned, the role has been taken over by Dr REDACTED the Medical Director. You may not be surprised to learn that Dr REDACTED will only consider Freedom to Speak Up requests if they involve patient safety – he does not think staff concerns about bullying or whistleblowing are relevant.
Surprised? No, I’m not either.
[REDACTED SECTION]
Glad that you are back campaigning again and I hope all’s well with you.
Kind regards
REDACTED (Paramedic)”
I asked the trust in question about this. After a lengthy pause, it denied these allegations and stated that it had two replacement Freedom To Speak Up Guardians in place. It denied that the types of concern that staff were allowed to raise had been restricted.
PETITION
Please click and add your signature to this petition to reform UK whistleblowing law – whistleblowers protect us all but weak UK law leaves them wholly exposed and it is a threat to public safety
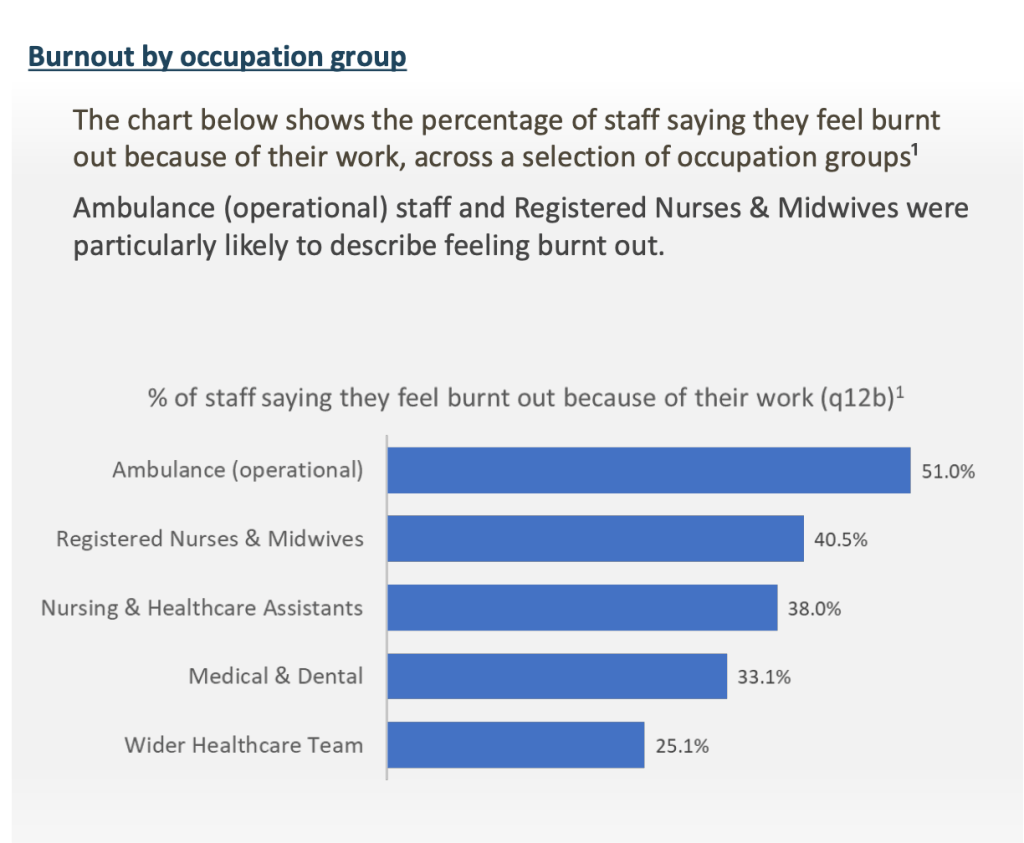
The latest NHS staff survey shows as usual that NHS ambulance trusts have the highest levels of bullying, and that ambulance staff report the greatest burnout:
This post shares an FOI response from WMAS about eight staff suicides since 2018 and further correspondence with the National Guardian:
A perfect, clear cut example of why UK whistleblowing law – PIDA – is completely unfit for purpose. The case of a gold standard whistleblowing case, Tribunal tested and fully upheld – which still resulted in a six year ordeal of persecution and harassment for whistleblower Dr Jasna Macanovic consultant renal physician and very importantly, still left patients unprotected.
By Dr Minh Alexander retired consultant psychiatrist 30 March 2022
Summary: This post looks at the National Guardian’s role in continuing poor culture at Sussex. After the former National Guardian Henrietta Hughes’ shameful treatment of whistleblowers at Brighton and Sussex University Hospitals NHS Trust, and her protection of powerful trust directors, time inevitably caught up with these improprieties. Further staff whistleblowing and patient complaints about maternity safety forced an unannounced CQC inspection late last year which revealed very serious ongoing failures of whistleblowing governance in maternity and surgical services. Staff reported that their concerns were not always acted upon. This even included serious concerns about critical care capacity. At one trust unit, inspectors found that managers had not reviewed or investigated 128 incidents. Astonishingly, staff were told to stop raising concerns about staff shortages on the basis that this was a known issue. This saga further illustrates the failure of the Freedom To Speak Up project. The National Guardian’s Office was established primarily to carry out reviews of NHS trusts but it has only completed 9 reviews since 2016 – less than two a year. Of the trusts that it has reviewed, most continue to show signs of problems with whistleblowing governance. It is time to stop wasting precious public money on sham whistleblowing agencies, and to replace them with strong, genuinely protective law and infrastructure.
Today, the long awaited Ockenden review into large scale maternity safety failings at Shrewsbury and Telford Hospitals NHS trust is due to be published. Inevitably, it has already been revealed that there was whistleblowing about the safety issues that was not acted upon by managers.
In the background is another avoidable maternity safety failing, in which the National Guardian’s Office played a part.
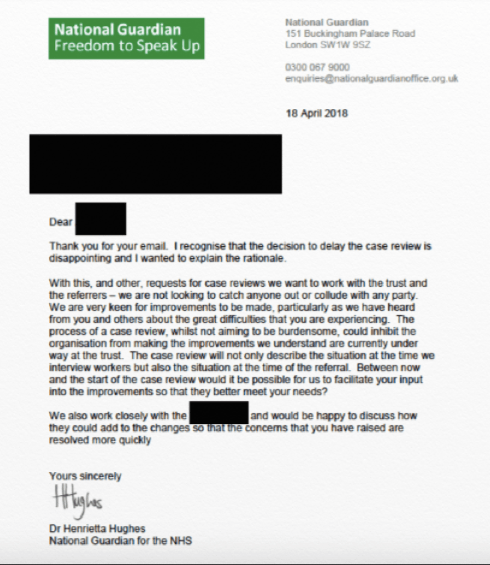
In 2017 the former National Guardian Henrietta Hughes badly failed patients and whistleblowers at Brighton and Sussex University Hospitals NHS Trust by stalling and protecting a powerful in group of NHS trust directors about whom whistleblowers raised concerns.
She deviated from her own procedures to give the trust time to cover its tracks:
Much later, in 2019, Henrietta Hughe carried out a review which came to glowing conclusions about the all the “improvements” being made in culture and whistleblowing governance.
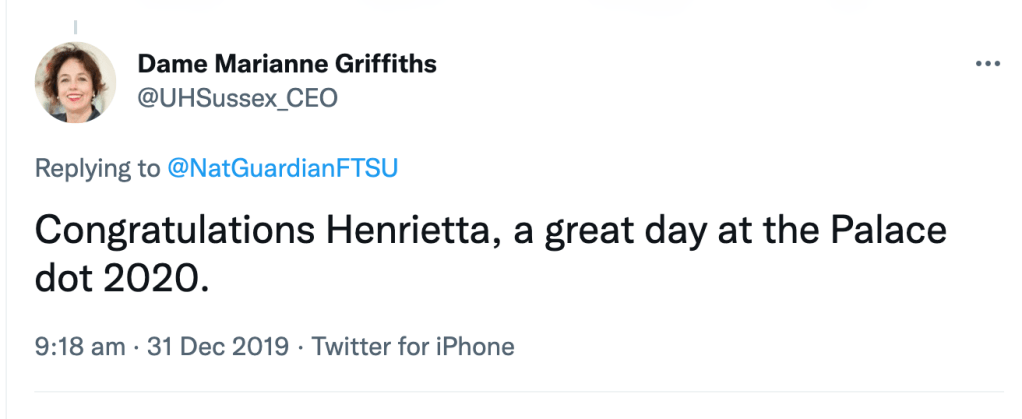
Marianne Griffiths the trust CEO naturally crowed about this PR victory:
Praise for BSUH culture change “Trust Chief Executive Dame Marianne Griffiths said: “Since our arrival at BSUH, we have made it our absolute priority to work with colleagues and support them to help make further improvements to the culture of the organisation, particularly in relation to equality and diversity. It is extremely encouraging, therefore, to see our improvements recognised through such a comprehensive review.”
In September 2021 as a result of more staff whistleblowing and patient complaints, the Care Quality Commission carried out an unannounced inspection of maternity services at the trust , now renamed University Hospitals Sussex NHS Foundation Trust after a full merger of its two predecessor organisations.
The CQC press release emphasised poor culture and the difficulty that staff experienced with raising concerns:
“Other concerns raised with inspectors by staff, or observed by inspectors, included a poor culture – bullying and harassment was reported by some staff – and a perception that leaders were doing little to address concerns. After listening to staff about their experiences working in main theatres and recovery, inspectors had serious concerns about the culture amongst colleagues.”
Extraordinarily, trust staff had been told to stop raising concerns about safe staffing issues because it was a “known risk”:
“They told us they been instructed to stop reporting low staffing as an incident as it was a known risk”
Surgical as well as maternity services were found to have shortcomings.
This included very serious incidents about lack of critical care capacity, for example:
“We reviewed an incident form completed in April 2021, in relation to patients requiring high dependency care, being cared for in recovery. On the day the recovery unit was full and included four patients who required high dependency care one of these patients deteriorated and required intensive care. Concerns within the incident related to not being able to keep up with all the care patients needed and although some support was provided by an advanced care practitioner and anaesthetist staff did not always feel supported. The incident was not investigated by managers until 12 October 2021 we were not assured that the actions recorded, or the time taken to investigate the incident reduced the risk of further similar incidents. The only recorded action was that staffing concerns were being managed through the directorate and divisional recruitment programme. The trust also provided a narrative for this incident and stated that the care and supervision of a significantly complex post-operative recovery period was appropriate.”
Despite these very serious failings, the Dame kept her overall CQC rating of ‘Outstanding’.
So, is the National Guardian’s Office working any harder to conduct reviews? This is after all the core function for which it was established.
Sadly, the answer is ‘no’.
Since inception in 2016 the work-shy, publicity-hungry agency has only completed 9 reviews – less than two a year.
CASE REVIEWS COMPLETED SO FAR BY THE NATIONAL GUARDIAN:S OFFICE
Southport and Ormskirk NHS Trust 2017
Northern Lincolnshire and Goole NHS Foundation Trust 2017
Derbyshire Community Health Services NHS Trust 2018
Nottinghamshire Healthcare NHS Foundation Trust 2018
Brighton and Sussex University Hospitals NHS Trust 2018
Royal Cornwall Hospitals NHS Trust 2018
North West Ambulance Service NHS Trust 2019
Whittington Health NHS Trust 2020
Blackpool Teaching Hospitals NHS Foundation Trust 2021
Issues of poor whistleblowing governance have continued at most of these trusts that were reviewed by the National Guardian. For example, there has been a high rate of whistleblowing employment claims against Nottinghamshire Healthcare NHS Foundation Trust, and I am aware that whistleblowers have continued to approach the National Guardian’s office but have been very unhappy with its response. There have been similar issues with North West Ambulance Service NHS Trust. Only very recently, there has been fresh whistleblowing to the press by staff of Northern Lincolnshire and Goole NHS Foundation Trust and Blackpool Teaching Hospitals NHS Foundation Trust:
Moreover, since being reviewed by the National Guardian in 2017, Southport and Ormskirk NHS Trust has repeatedly been in the news for bullying. The trust recently lost an Employment Tribunal for causing injury after managers failed to respond to repeatedly raised concerns about bullying:
So what is the point of the National Guardian’s Office?
Does the NHS need an idle, ineffective if not harmful, sham whistleblowing agency?
Here is Marianne Griffiths the trust CEO congratulating Henrietta Hughes former National Guardian after it was announced in the New Years Honours List that Hughes was listed for an OBE:
PETITION
Please click and add your signature to this petition to reform UK whistleblowing law – whistleblowers protect us all but weak UK law leaves them wholly exposed and it is a threat to public safety
A perfect, clear cut example of why UK whistleblowing law – PIDA – is completely unfit for purpose. The case of a gold standard whistleblowing case, Tribunal tested and fully upheld – which still resulted in a six year ordeal of persecution and harassment for whistleblower Dr Jasna Macanovic consultant renal physician and very importantly, still left patients unprotected.
By Dr Minh Alexander retired consultant psychiatrist 23 March 2022
Summary: Dr Jasna Macanovic, an “extremely gifted” renal physician who provided the NHS with twenty years “excellent” service was unfairly dismissed by Portsmouth University Hospitals NHS Trust, an organisation with a troubled leadership history. The audit trail was sufficiently clear for the Employment Tribunal to firmly conclude that her dismissal was a direct consequence of her whistleblowing, which included protected disclosures to the General Medical Council about colleagues. The ET determined that her dismissal was a forgone conclusion, involving both the former Chief Nurse and current Medical Director. These two directors encouraged her to resign with a good reference during the disciplinary process that the trust mounted against her. When Dr Macanovic did not resign, she was sacked by the Chief Nurse for purported “serious misconduct” which explicitly included making referrals on colleagues to the General Medical Council, even though the regulator had already effectively said the referrals were appropriate and part of Dr Macanovic’s duty as a doctor. The ET also concluded that the trust attempted to “resist” and “deflect” Dr Macanovic’s patient safety concerns. A “substantial” number of consultant colleagues shared her concerns. Her identity as a whistleblower to the GMC was exposed in an extraordinary manner by her line manager, one of the individuals about whom she raised concerns. He read out the details of her GMC referral about him at a meeting with their colleagues. There were other notable incidents. After one meeting with the Medical Director, Dr Macanovic reportedly suffered a panic attack and required an ECG. The trust tried to retrospectively argue to the ET that it objected not to her whistleblowing but the manner in which it was done. This line is often used by some employers to rid themselves of whistleblowers under an argument of breakdown of relationships after no disciplinary charge sticks. The ET saw through this, which makes a refreshing change from fudged, equivocal judgments which end up pinning an unjustified share of the blame on already traumatised whistleblowers. Although Dr Macanovic was vindicated by the ET, it is a failure of our current whistleblowing law and infrastructure that she had to suffer this protracted ordeal, and she was not better protected from the outset. This case is also yet another failure of the Freedom To Speak Up model. The trust Freedom To Speak Up Guardian attended a meeting with Dr Macanovic, the trust CEO and Chair, but this did not stop serious reprisal and dismissal. There is no mention in the ET judgment of any escalation to the National Guardian. That is an aspect which remains to be clarified.
Introduction
The Employment Tribunal has found strongly in favour of Dr Jasna Macanovic a consultant renal physician unfairly dismissed by Portsmouth Hospitals University NHS Trust for whistleblowing, including to the General Medical Council. The judgment states:
“The unanimous decision of the Tribunal is as follows:
The claimant was unfairly dismissed for making a protected disclosure.
The claimant was subject to detriments for making a protected disclosure.
Arrangements for a remedy hearing shall be notified to the parties shortly.”
Dr Macanovic raised concerns about two unreported “red” surgical adverse events and the fact that some consultants at her trust were practising a technique known as “buttonholing” in a way that she believed was unsafe. She believed they were failing to properly report all complications and safety incidents. Several of her consultant colleagues shared her concerns about the buttonholing issue.
Buttonholing is a procedure to give access to a patient’s veins for kidney dialysis. The ET explained buttonholing thus:
“There is also an alternative process known as buttonholing (“BH”). As the Claimant explains, buttonholing is where patients cannulate (insert needles) using blunt needles. The blunt needles are placed in exactly the same holes in the fistula every time that the patient has to have dialysis. A track or tunnel is created through the skin to the fistula. Over time this may be less painful than using sharp needles because a patient is not making new holes on regular occasions. The buttonholing technique can be less painful and more convenient for patients.
It is agreed that buttonholing is a valid technique for patients with an AV Fistula, where the connection between vein and artery is constructed of tissue and can heal. The dispute is over those with an AV Graft, since the PTFE material can tear or degrade. That can cause leaks and an increased risk of infection. Patients need to be made aware of these risks to give informed consent. The probuttonholing school of thought is that using one blunt needle is better than repeated sharp needle entries, since over time these can damage the tissue and make it more difficult to find an entry site. Also, some patients prefer it to having a fresh jab each time.”
Dr Macanovic’s concern arose in part because she believed that Dr Sangala one of her colleagues had made unreliable claims that another unit had been using the novel technique, when it turned out from her own enquiries that this was not the case.
“…she had heard back from Reading and they were not doing it for AG grafts. Worse still, she said, patients had been told that the outcomes were excellent, whereas of the 14 patients using it, two had died, two had developed serious complications, and she had not had time to review the other ten.”
Her department became very polarised and the trust failed to deal appropriately with her concerns.
An example of chaotic polarisation was given by the ET as regards Dr Knighton the new Medical Director’s response to the situation in the summer of 2017:
“82….Four of the consultants met Dr Knighton urgently that day (26 June) to raise their concerns about buttonholing. Having heard them, Dr Knighton decided that the practice should cease immediately. The next day a consultants meeting was arranged at short notice, which he also attended. Some agreed with the decision to stop it, but Dr Borman and Dr Lewis put the counter case that several patients had chosen buttonholing. Mr Gibbs and Dr Sangala also emphasised that this was patient driven, and in the end Dr Knighton accepted the view that it could do more harm to reverse it immediately. So, he reversed the decision.”
On another occasion, a mediation meeting descended into chaos with all in tears. The ET determined that the “mediation” improperly focussed on pressuring Dr Macanovic to withdraw the GMC referral:
“We can only conclude that they all lost sight of the important principle that this was a protected disclosure and as such it was wrong to pressure her into withdrawing it”
Turning the focus onto the whistleblower
As often happens in whistleblowing cases, Dr Macanovic was turned into the focus of the matter. This was despite a long record as an “extremely gifted” physician, who was able to submit many statements from colleagues in all disciplines about her professionalism and patient-centredness. This in itself is remarkable, as in many whistleblowing cases, supporters are often intimidated into silence. Organisations also isolate whistleblowers, by a process of exclusion, attrition and smearing, to weaken any support they may have.
The story is a lengthy and complicated, and the whole ET judgment needs to be read for a complete picture. However, a few notable incidents follow.
One doctor about whom Dr Macanovic raised concerns behaved towards her in a way which the ET concluded was “abuse”:
“…Two days later Dr Macanovic was on the receiving end of an outburst from him. She was in her office at about 08.00 am when he arrived at the door and started shouting at her. He said that he was going home because he was too stressed, and that she was to blame. This was accompanied by a good deal of swearing, repeatedly telling her to ‘f’ off. She was left shaking and at the point of tears, and was still shaking 30 minutes later when her colleague, Dr Synodinou, came in.”
And yet Dr Macanovic’s line manager and Head of Unit, Dr Robert Lewis, wrote to her about this incident as follows:
“Over the next two weeks Dr Lewis investigated the shouting incident. He concluded (p.461A) that:
Your accusation about Mr Graetz is troubling on two counts. Firstly, you were clearly a source of great stress to him at the time and yet you categorically and vehemently state that you were not.
You have not sought to find out why Mr Graetz felt as he did and have not considered the possibility that you might be at fault. Instead you state that the fault is entirely Mr Graetz’s because he does not cope well with stress (rather unfair since you took a much longer period of stress-related leave over the same issue than he did). Secondly, and more importantly, you are clearly unable to distinguish between abuse and someone challenging you with an opinion which you find uncomfortable.”
The ET took issue with Dr Lewis’ framing of this incident and noted:
“He [Mr Graezt] accepted to us that his behaviour had been inexcusable and he apologised to her a few days later.”
The ET was not satisfied that the incident was properly investigated, and counted this as a whistleblowing detriment.
Dr Lewis was eventually one of the doctors whom Dr Macanovic referred to the GMC regarding her concerns.
The ET noted that he took the unusual step of reading out loud her referral about him to the GMC at a consultants’ meeting:
“70. The GMC referral was eventually made known to Dr Lewis. In a surprising decision, he elected to read it out in its entirety to the consultants at a meeting on 7 June (Detriment 5). Dr Macanovic was there to hear it. The exercise must have taken some time since the referral letter covers eight pages. In his evidence to us Dr Lewis said that any summary would have risked further objection from Dr Macanovic, but we see no reason why he could not just have said that she had referred him, or others, to the GMC over the buttonholing issue. In choosing to give such publicity to her complaints, he was in our view, stoking anger against her and seeking to isolate her from her colleagues. She was left shaken by this episode.”
Dr Lewis later confirmed at an interview that he had not discussed his intention to read out the referral with Dr Macanovic before he did so:
“He accepted that he had not discussed this with Dr Macanovic beforehand and maintained that that was the right approach – the others needed to know about these attempts to destroy people’s careers.”
Dr Lewis must have been highly stressed by the GMC referral but his action at the meeting seems a most extraordinary departure from what might be expected of him as Dr Macanovic’s line manager.
The referral to the GMC was an act of whistleblowing and was determined to be a protected disclosure by the ET.
23 Leading by example, you should promote and encourage a culture that allows all staff to contribute and give constructive feedback on individual and team performance. You should make sure that systems are in place to achieve this.”
Publicly exposing and inciting hostility against a whistleblower is not consistent with this.
The ET noted that after Dr Lewis’ public exposure at the above meeting of Dr Macanovic’ whistleblowing to the GMC, he followed up with emails to colleagues:
“71. Dr Lewis followed this announcement with emails to colleagues who were not there. He received many messages of support, including the one quoted at the outset (paragraph 11) from Dr Armstrong, stating that she was “shocked, enraged and very saddened.” Asked about this at the hearing Dr Lewis said words to the effect that Dr Macanovic had taught him well, this was how she operated, he needed a record of things and that by then “the gloves were off”
The ET noted other similar correspondence:
“When the unit head, Dr Robert Lewis, told the other consultants that he would have to attend a Fitness to Practice hearing, one of them emailed to say:
I am completely shocked, enraged and deeply saddened to read this email. I cannot believe that one of our colleagues would sink so low but it only goes to prove what a dysfunctional and destructive individual [Dr Macanovic] is with no thought whatsoever to the impact that her actions are having, not only on individuals but also on the whole department. …
I am sure the GMC will see this for what it is – a vindictive and purposeful attack on an individual colleague for no reason other than her own self satisfaction.”
As far as I can see from the trust website, it seems that Dr Lewis remains at the trust but no longer in a managerial capacity.
Circular assurance assisted by the CQC’s superficial regulatory method
A bizarre but familiar scenario of circular NHS assurance arose.
According to the ET, someone from the trust raised concerns with the Care Quality Commission about the novel buttonholing practice, sometime around October 2016. The trust clearly suspected Dr Macanovic because it later asked her, at a disciplinary meeting in 2018 if she was responsible:
“Dr Macanovic was asked during the subsequent disciplinary investigation if it was her and she would neither confirm nor deny it.”
This itself was another trust impropriety in terms of trying to hunt down a whistleblower.
The ET clarified in retrospect that it was indeed Dr Macanovic who had whistleblown to the CQC.
The trust response to the CQC was prepared by Mr Gibbs Clinical Director and Dr Lewis the Head of Unit.
Mr Gibbs was one of the surgeons about whom Dr Macanovic had raised concerns as regards unreported “red” adverse incidents.
According to the ET,
“Presented with this response the CQC did not carry out any further enquiry, and wrote back on 22 December 2016 (p.368) to say that they were satisfied that there were no safety concerns and that appropriate governance had been followed.”
Dr Lewis then communicated with consultant colleagues as follows:
“Dr Lewis reported this to the consultants by email on 16 January 2017 (p.375) – addressing it to “Dear Jasna and Colleagues”. But he did not attach the letter from the CQC, on the basis that this would then be “dissected or disputed”. In fact, any request to see it would, he said, be to question his probity and that of Mr Gibbs.”
An internal trust investigation report, the “Hunter report”, later relied on the CQC’s decision to take the matter no further, which of course rested on assurance given by parties under investigation.
“The Hunter report followed, after several months in the pipeline. On the buttonholing issue Mr Hunter found (p.239):
“33. Given my limited expertise within this area and given that the response provided by the Trust addressing the anonymous has been accepted by the CQC, there is a careful monitoring process in place and all significant events which were known when the investigation commenced have been investigated and this evidence provided to the CQC, I do not think any further interpretation by myself would help in this.
34. Hence, the Hunter report rested on the CQC conclusions, which rested in turn on Mr Gibbs’ letter.”
The ET judgment gives no information about who Mr Simon Hunter the report author was, but there was a consultant of Emergency Medicine of the same name at the trust, who was mentioned in 2016 trust board papers as “Chief of Service, Emergency Medicine”
The ET was critical of Dr Lewis’ decision to allow Mr Gibbs to respond to the CQC for the following reasons:
“148. One particular point raised on behalf of the Trust was that they took the buttonholing issue seriously, indicating that it was a separate matter. In fact, our view is that the consultant body in the renal unit were led by Mr Gibbs as Clinical Director, and he was a strong proponent. Dr Lewis gave Mr Gibbs his backing on this issue, and so Mr Gibbs was the one in a position to respond to the CQC. That is not so much treating her concerns seriously as attempting to resist or deflect them.”
NCAS greasing the wheels of exclusion and disciplinary action
Dr Macanovic was considered “unmanageable” by the trust as she would not be cowed and would not retract her concerns. This is often how incompetent organisations view whistleblowers.
Matters was escalated to the then Medical Director, Simon Holmes.
The ET referred to the trust “arming” itself with ritual advice from the National Clinical Assessment Service, an expensive rubber stamping service which allows NHS employers to behave abusively whilst claiming that they have sought independent advice. The truth is that trust managers can obtain whatever advice they want by tailoring the information they feed to NCAS, and they can also control the subsequent flow of information back through their organisations.
The salient passages about NCAS’ advice are given as follows by the ET.
NCAS advice 4 May 2017:
“The Trust is mindful that Dr 19339 is a whistle blower, but concerns have been expressed by her colleagues about her behaviour and you have received 3 letters of complaint alleging that she exhibits aggressive, bullying and intimidating behaviour.
…. The issue is, as you are aware, complicated by Dr 19339 whistle blowing status and it will be important to document carefully the preliminary information which has been received so that this is available for future scrutiny if required. Potentially it may be necessary for the Trust to be able to demonstrate that Dr 19339 is not being victimised for having raised concerns. I advised that to avoid any allegations of bias, it may also be useful for the role of Case Manager, to be delegated so that the person making any decision about how to proceed is free of any real or perceived conflict of interest. Likewise the Case Investigator should be suitably senior, experienced and independent.”
Further NCAS advice June 2017:
“You told me that, prior to the referrals to the GMC, the department, including Dr 19339, had requested the help of an external mediator. Everyone was keen to do this and so the Trust organised an external mediation which took place yesterday. You said you attended the start and conclusion. You described how at the end of the day everyone attending seemed stressed, anxious and some were physically shaking. One member of staff had to leave the room because he was so distressed.
There appeared to be an absolute breakdown in trust between Dr 19339 and the rest of the department and the result of this led you to be concerned for the health of all in the department. You considered that the breakdown in relationships in a team who need to have confidence in each other to ensure patient safely constitutes a risk to that safety.
However, the Trust will wish to assure itself that any action it takes to mitigate potential safety risks within the department is not construed as being a detriment to Dr 19339 as a result of her declaration to the CQC that she is a whistle blower.
…
Any prolonged exclusion from clinical work can lead to de-skilling and I suggested that the Trust might wish to look for a placement in another Trust or department while the investigation is ongoing and the GMC comes to a decision as to whether it will take any action against the colleagues of Dr 19339.”
The ET noted that the trust used NCAS’ advice to progress Dr Macanovic’s exclusion, even though it failed to follow several aspects of NCAS’ advice.
The ET also noted that at a meeting dealing with Dr Macanovic’s exclusion, a new Medical Director Dr Knighton refused to accept her concerns that she was being bullied by Dr Lewis. After this meeting with Dr Knighton, she reportedly suffered a panic attack and required an ECG:
“Dr Macanovic said that she was the victim of bullying by Dr Lewis, but he did not accept that that was the case. Dr Gast proposed that she could simply be excluded from consultants meetings and after a pause to consider, Dr Knighton agreed that that would be a better option. After that meeting Dr Macanovic was unwell and could not resume work. She had a panic attack and spent the afternoon in the outpatients department where she had an ECG. However, she was not signed off sick.”
Freedom To Speak Up mechanism made no difference
Dr Macanovic had a meeting with Mark Cubbon the Chief Executive and Mark Nellthorp the then trust Chair, attended by Jocelyn Booth the trust Freedom To Speak Up Guardian and elected trust Governor.
Dr Macanovic raised concerns at the meeting with the Chief Executive and then Chair that disciplinary action against her was in fact reprisal and bullying.
According to the ET, Mark Cubbon agreed there should be a separate investigation into Dr Macanovic’s concerns. However, he later reportedly changed his mind after talking to the trust director of workforce, Tim Powell. No one told Dr Macanovic, and Mark Cubbon reportedly did not respond to her subsequent correspondence. Such stonewalling is a common experience for whistleblowers.
Several consultants also later wrote to Mark Cubbon the chief executive on Dr Macanovic’s behalf, as disciplinary action against her proceeded, appealing to him to prevent her dismissal:
“113. In that period, on 2 March, Dr Bostock, Dr Uniacke, Dr Synodinou, and Dr Gast emailed Mr Cubbon, to ask him to step in to prevent her dismissal (p.1716). Dr Gast was the author. She said that these complaints were from a minority of staff, and were an attempt to silence and discredit Dr Macanovic as a whistleblower. He declined to intervene.”
The ET said it understood this:
“Similarly we can understand why Mark Cubbon failed or declined to intervene in the disciplinary policy at the 11th hour, as requested”.
It is a pity the ET did not elaborate.
Particularly as it concluded that the disciplinary charges against Dr Macanovic were patently flawed and that the dismissal process was blatantly predetermined.
Mark Cubbon is pictured below in 2019 with the previous National Freedom To Speak Guardian on the theme of the “authentic employee voice”. This was whilst Dr Macanovic’s Employment Tribunal claim was proceeding:
k
The General Medical Council
According to the excerpts quoted by the ET judgment, the GMC found in January 2018 that the buttonholing had not been introduced in a structured way at the trust. Oddly, the GMC concluded that because buttonholing had not been introduced under rigorous research conditions, there was no need to be concerned by the absence of the usual governance constraints, such as ethical review:
“With hindsight, it could be argued that it would have been a good idea to introduce the button holing/graft access method as a research project with a formal protocol and ethical review under the research governance framework. However, because of the gradual way in which it was introduced it was not introduced in this way. As it was not conceived as a research project, the fact that it did not follow the research governance framework does not raise any serious concerns.
The button holing/graft access method was an innovative technique, and should therefore have been introduced with appropriate controls, records and safety assurance, according to the relevant local policies.”
The excerpts indicated that the GMC identified no failing by Dr Lewis in regards to the governance of the buttonholing procedure:
“The method was introduced two years before Dr Lewis became chief of service and therefore he was not responsible its introduction. Indeed, all the governance measures that were eventually introduced were introduced as a direct or indirect result of his intervention, starting at the consultant meeting on 7 September 2016.”
Importantly, the GMC effectively concluded that Dr Macanovic fulfilled her professional obligations by referring her colleagues to the GMC:
“We are of course mindful of the findings of the independent whistleblowers review the GMC commissioned from Sir Anthony Hooper. Having considered the correspondence disclosed to the GMC by the trust and by Dr Macanovic, it appears Dr Macanovic first raised her concerns locally and that it was only after she concluded, in her view, that her concerns were not being adequately addressed locally that she made her complaint to the GMC. In doing so Dr Macanovic was no doubt aware, amongst other things, of the guidance at paragraph 25 of Good medical practice that doctors must take prompt action if you think that patient safety, dignity or comfort is or may be seriously compromised.”
In the event Dr Macanovic genuinely considered there was a risk to patient safety, and it appears to us that she did consider such a risk existed, but she had not raised her concerns through whatever mechanism was available to her locally and/or if she deemed it necessary to the GMC, she would in our view have been rightly criticised by the public and by the GMC for failing to do so.”
The ET explicitly interpreted the GMC’s remarks thus:
“In our view she did genuinely consider that there was a risk to patient safety. That is implicit in the previous finding that this referral amounted to a protected disclosure. Although it was suggested to us that this fell short of an express statement from the GMC that she was right to make this referral, that seems to us its practical effect.”
Theresa Murphy Chief Nurse explicitly sacks a whistleblower for whistleblowing
Soon after the GMC decision, the trust machinery whirred into action to dismiss Dr Macanovic. The ET concluded that this was a “predetermined” process. This was partly because, extraordinarily, Dr Macanovic was given the option by both the medical director Knighton and Theresa Murphy to resign with a good reference during the dismissal process:
“Having heard this evidence, and towards the end of the hearing, Dr Knighton referred again to his suggestion of resigning with a good reference.”
“The hearing resumed on 5 March 2018 when Professor Murphy gave her decision. At the outset, she also reminded Dr Macanovic that she could instead choose to resign with a good reference.”
A CQC specialist advisor at the trust
Dr John Knighton took up his post as medical director at Portsmouth Hospitals University NHS Trust in July 2017 and remains in this role. Prior to that he had been associate medical director. According to a local press report of 28 July 2017, at the time of his appointment as medical director, he had already been working as a CQC specialist advisor:
“During our inspection, CQC staff had to intervene to keep patients safe on several occasions, including asking staff to assess patients in the ambulance and the corridor, and to prevent a patient from leaving the department when there was not a member of staff present.”
“Inspectors praised the “exceptional resilience” of staff but said they suffered from “change fatigue” because of repeated incomplete initiatives from management.”
“Sir Mike said that “staff had now accepted a standard of care that was unacceptable” and “some of the executive team were identified as barriers to the leadership of effective change”.
The trust dismissed Dr Macanovic claiming that she was guilty of “serious misconduct”.
Despite the GMC’s effective conclusion that Dr Macanovic’s referrals were professionally appropriate – indeed, required, a dismissal letter from Theresa Murphy stated that one of the reasons for Dr Macanovic’s dismissal was the fact that she had made disclosures to the GMC:
“Despite internal and external confirmation that button holing is not contraindicated and carries no specific risks, and despite you not being an expert in vascular access, you not only continue to disagree with its use, but you also referred colleagues to the GMC for using/supporting its use and I do not feel you acted professionally in this regard”
This was a clear smoking gun linking the dismissal to protected disclosures.
Theresa Murphy’s dismissal letter also reportedly claimed:
“Relationships between you and a number of consultants in the Renal Unit have broken beyond repair as a result of your behaviour”
The ET also noted substantial issues of bias and procedural unfairness by the trust and various other whistleblowing related detriments.
Was the trust badly advised? We do not know, but the ET pointed out that the trust’s solicitors Mills and Reeve variously accused Dr Macanovic of
not acting in good faith
not articulating her concerns about the buttonholing
referring colleagues to the GMC ‘with no good reason’
Mills and Reeve act for many NHS organisations and are therefore familiar to a number of whistleblowers who have been driven to litigation.
The ET observed that the trust tried to argue that it was not so much Dr Macanovic’s whistleblowing that was the problem, but the manner in which she went about it. The ET rejected this.
The ET noted that Dr Macanovic could have been more diplomatic. However, English is reportedly her third language and there may be cultural differences in social directness to consider.
Diplomacy notwithstanding, the ET determined:
“The main plank of the respondent’s case is that Dr Macanovic was not dismissed for making these disclosures but for the manner in which she did so. But that distinction was not apparent in the dismissal letter, nor to any great extent during the disciplinary proceedings, and does not seem to us to be justified in hindsight. The plain fact is that after over twenty years of excellent service in the NHS, Dr Macanovic was dismissed from her post shortly after raising a series of protected disclosures about this one issue. It is no answer to a claim of whistleblowing to say that feelings ran so high that working relationships broke down completely, and so the whistleblower had to be dismissed.”
Quite rightly, the ET focussed on the core public interest issues – something that many Tribunals fail to do:
“Dr Macanovic was concerned with one main issue, potentially a matter of life and death. She raised her concerns against a dominant management group and at two meetings there were heated exchanges. Tempers were raised on both sides. The findings of the disciplinary process were, in our view, very one- sided, reflecting a determination to remove Dr Macanovic as the source of the problem, but that is very different from one individual making a disproportionate fuss about things that concern them. Regard must be had to the scale of the issues at stake in deciding between the message and the method used.”
Moreover, the ET made it clear that no substantive contributory fault could be attributed to Dr Macanovic:
“Given our view that the Trust have not shown a potentially fair reason for dismissal, there is no basis for a reduction on the basis that a fairer process would have led to the same result (a Polkey deduction) or to contributory fault on her part.”
This is a refreshing departure from the great multitude of ET judgments that get bogged down in spurious counter-allegations by institutions with deep pockets for legal shenanigans.
It is thus a warning to arrogant NHS trusts that may be tempted to hit the “breakdown of relationships” and “Some Other Substantial Reason” button in order to rid themselves of whistleblowers.
So, it seems that which is intended to drop whistleblowers through a hatch in the floor to shark infested waters may occasionally end up as an unwelcome eject button for trust directors.
Therese Murphy now describes herself as a former chief nurse on her LinkedIn entry.
The ET’s unequivocal finding in favour of Dr Macanovic is unusual. But she should never have suffered the ordeal she went through. Much stronger UK whistleblowing law and infrastructure are needed to ensure protection at much earlier stage of the process, to prevent both harm to the whistleblower and the public.
If you wish to protect whistleblowers and to help stop their concerns being covered up, please click on this link and lend your signature to this petition for much better UK whistleblowing law:
The body Practitioners Performance Advice (which replaced NCAS) agreed to improve its procedures following the whistleblowing cases of Dr Macanovic and Mr Reuser, to safeguard against employers feeding false and malicious information in referrals to engineer suspensions and out adverse outcomes for doctors.
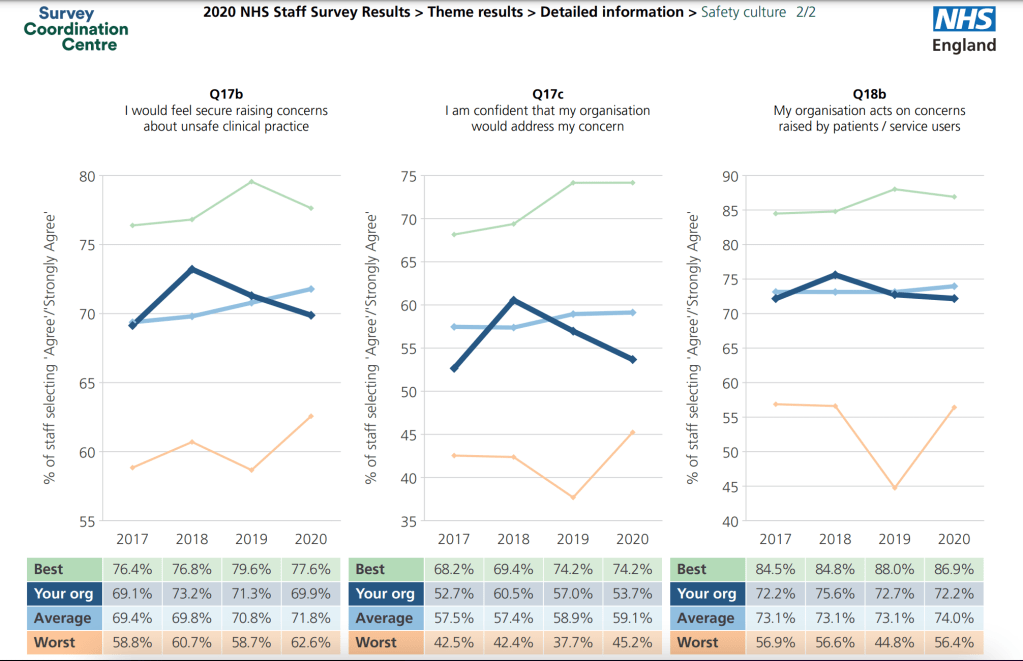
2. Portsmouth Hospitals University NHS Trust scored fairly averagely on whistleblowing questions in the last NHS staff survey, but this still meant that about a quarter of staff did not feel secure in raising concerns.
2. Where disciplinary charges fail, a common method of dismissing NHS whistleblowers is by arguing an irretrievable breakdown of relationships:
3. NHS staff lack adequate procedural protection from abusive employers who make malicious use of disciplinary processes and arbitrary exclusions. The NHS has failed for twenty years to act on recommendations from the National Audit Office to strengthen safeguards:
Tom Kark QC’s 2018 review recommendations for tightening up the oversight of NHS management probity, short of full regulation, have not yet been implemented. NHS Improvement confirmed to me last week that a planned “Kark” register for tracking adverse information about managers’ fitness has not yet been established.
This laxity and impunity for whistleblower reprisal gives licence for further abuses.
5. “Mobbing” is a group dynamic by which whistleblowers are often attacked and smeared by overwhelming, concerted allegations and undermining. It is recognised in some European employment law as “moral harrassment”. Dr Macanovic’s case illustrates how the introduction of such a provision into UK whistleblowing law could more finely target and improve protection:
Summary: An as yet unpublished Kings Fund review about poor leadership at HSIB has resulted in the agency being stripped of its maternity investigations by the Department of Health and Social Care. Was the affair in any way an attempt by the government to control a mounting maternity personal injury bill, because HSIB investigations had helped to establish liability?
HSIB, the investigatory arm of the regulator NHS Improvement was one of Jeremy Hunt’s cynical and superficial ‘patient safety’ gestures created in response to pressures over unresolved patient safety issues following the Midstaff Scandal. He established it whilst he continued to defund and undermine the NHS.
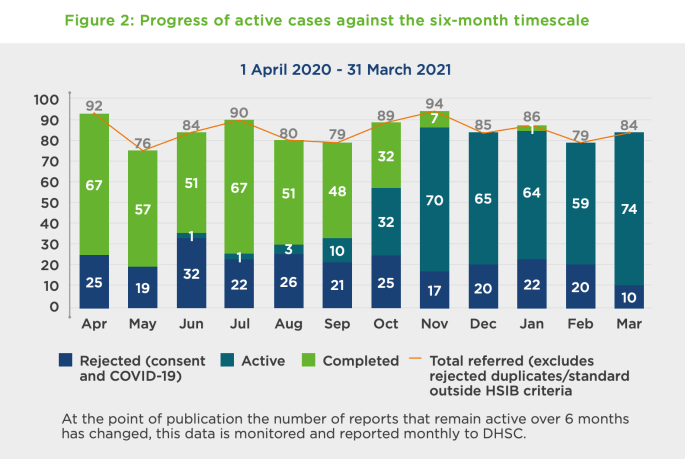
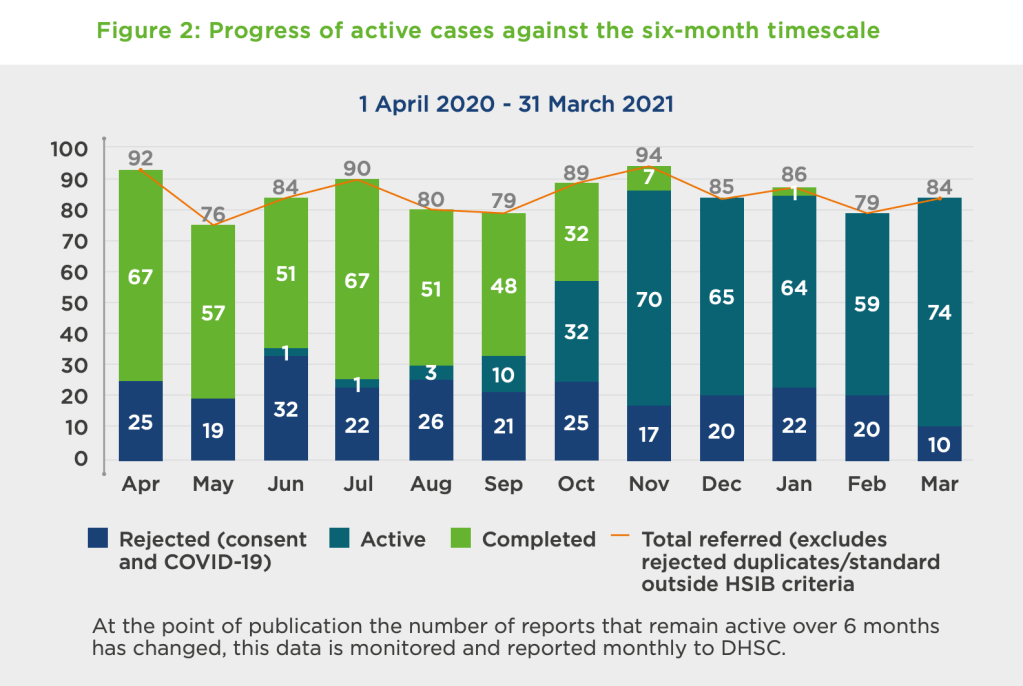
Significantly, the latest scandal led to HSIB being stripped of its maternity investigations – an area which had been mushrooming with the revelations at Shrewsbury and Telford NHS Trust, with huge liability implications for the NHS and the government. HSIB had been undertaking about 1000 maternity investigations a year.
“In announcing his retirement Keith Conradi, Chief Investigator says:
“It has long been my intention to retire at 60 while my health enables me to participate in competitive triathlon.”
Other senior departures from HSIB were also reported.
When HSIB’s creation was first announced, I made attempts to obtain objective evidence of whether aviation and AAIB were truly a paragon of safety culture as Hunt had claimed. I asked for old AAIB staff survey results, but was repeatedly blocked by the government. This was despite the ICO ruling that there was no good reason for the Department of Transport to withhold the information. Litigation continues on the matter with the ICO opposing the government. It is before the Tribunal again in April.
Before HSIB became operational, I had a foretaste of things to come when I tried to engage its players in ensuring effective whistleblowing governance. They clearly knew little about whistleblowing but seemed to have minimal interest in becoming more competent. The venture seemed very insular and clubby. After being told that someone with no visible whistleblowing expertise would sort it all out, I made a challenge to the boys’ club culture. This was met with uncomprehending huffiness by one of the safety luminaries backing the project. No doubt those grand men will quickly forget their poor judgment and move on to the next vanity project dangled before them by politicians.
After the major scandal broke this January, I asked NHSI for a copy of the Kings Fund review and other information about NHSI’s handling of the HSIB affair. However, NHSI has not yet answered despite intervention from the ICO and an exchange of correspondence with Andrew Morris who said he had asked his FOI team to expedite the matter.
It is a failing by NHSI that the Kings Fund review of HSIB is not already published. It was commissioned in secret and remains withheld. NHSI bears ultimate responsibility for HSIB’s failure.
Indeed, was HSIB’s leadership substantially worse than the abusive, failing NHS trust managers than NHSI protects and recycles on a daily basis?
Indeed, how do we know if HSIB’s culture was any worse than that of NHSE and NHSI’s? Neither NHSE or NHSI routinely publish their own staff survey results and are frequently criticised for bullying provider organisations.
Notwithstanding any justified criticism of the obviously poor leadership of HSIB; was the decapitation of the agency in any way a government attempt to block transparency about NHS safety failings? Was it merely a pretext to control a huge bill from maternity injury pay outs?
And what of NHSE/I’s hireling, the Kings Fund? Did it give the HSIB leadership and its staff a fair hearing?
The King’s Fund board of trustees has traditionally been populated with the powerful, connected and sometimes recycled. I previously asked its former Chair Sir Christopher Kelly, former Department of Health Permanent Secretary, if he was one of the referees for Jo Williams the disgraced former Chair of the CQC when she applied to re-enter the NHS as Chair of Alder Hey NHS Foundation Trust:
A doctor at Smith’s trust spoke up critically about Smith’s appearance on Strictly: “Clare Gardner launched an online petition, reading: “She is the chair of the largest NHS Trust in the UK, during a time of major crisis i.e. the second Covid-19 wave.“We are already in a Tier Two lockdown. I am a haematologist within the Trust she apparently chairs.“Our Chief Executive Dr David Rosser has made numerous statements to the press recently, describing the fear and foreboding we all sense towards rising cases.”“Now that we are facing a similarly perilous situation, she has swanned off to London to dance.“This is a dereliction of duty.“If ever there was a time to have figureheads in place for NHS organisations that are struggling, it is now.“Jacqui would rather wear sequins than look after her charge.”
One can only hope that Dr Gardner is unharmed and still prospers.
Smith was also chair at UHB during Mr Tristan Reuser’s whistleblowing ordeal. She failed to answer a request in August 2021 for data about the trust’s abusive handling of the Reuser litigation and about FPPR process regarding her chief executive, despite a reminder. The matter is now with the ICO.
The Kings Fund churns out forests of prim admonishments about how NHS leaders should behave. It calls often for compassionate leadership. It positions itself in the market as a seller of advice and reviews on how to do it right.
Some of the Kings Fund’s prominent figures have sometimes worked symbiotically with the equally virtue signalling National Guardian’s Office.
So I attempted to check out the actual quality of the goods and asked the Kings Fund to share its own staff survey data. This was because the first thing noticeable is that this data is not published.
After one email to its comms team, two emails to its CEO Richard Murray and one email finally to its Chair Lord Kakkar, I received an acknowledgment from the CEO’s office. This was followed by a minimal substantive response from the Kings Fund comms team on 3 March, giving headline figures for amalgamated years and no staff survey reports:
“Dear Dr Alexander
Thank you for your emails about staff wellbeing at The King’s Fund. We don’t have a record of your original inquiry to this account so please accept our apologies for the delay in responding and treat this as a response to this and the emails you subsequently sent to Richard Murray.
The King’s Fund has been running staff satisfaction surveys since 2008, usually every other year. They are managed on our behalf by an organisation called the Leadership Factor so that scores and narrative can be provided confidentially. Between 2008 and 2015 the overall satisfaction score was between 71 per cent and 78 per cent, placing us in the top quartile of organisations the company surveyed.
In 2017, we refreshed the design of the survey and included specific questions about engagement and wellbeing. In 2018, these factors scored 8.4 and 7.6 out of 10 respectively, where 10 is very satisfied. We were due to run the survey again in 2020 when the pandemic hit. At the end of 2020, we introduced regular pulse surveys in place of the full survey which included questions about health and wellbeing, levels of optimism and morale. We will run the full satisfaction survey again in Autumn 2022.
Best wishes
Gemma Umali
Press and Public Affairs Manager”
I asked for more detail, pointing out that it would be useful for example to see how minority staff groups fared.
“Many thanks for your response and the broad percentage results extracted and aggregated from past staff surveys.
It would be more useful to have actual copies of the staff survey reports from tne years in which you say the surveys were carried out.
It is hard to make much sense of broad headline results without any contextual details.
For example, the stratified results for different staff groups, (assuming that this data is collected by the Kings Fund) and particularly minority groups are important to see – as the Kings Fund itself has emphasised in the past when passing comment on the national NHS staff survey.
Your aggregation of results from different years also obscures possible variations over time.
I would be very grateful f you would share copies of the original staff survey reports.
However, if the Kings Fund does not wish to share the actual reports, would you at least be willing to share the questionnaire forms that staff filled in on the years in question?
Mamy thanks
Minh
Minh Alexander
Cc Richard Murray CEO Kings Fund
Lord Ajay Kakkar Chair Kings Fund”
At the time of writing, I have not yet received either a copy of the questionnaire that Kings Fund staff fill in, nor the original staff survey reports. I guess the Kings Fund comms folk have still got their thinking caps on. Compassionately, no doubt.
PETITION
Please click and add your signature to this petition to reform UK whistleblowing law – whistleblowers protect us all but weak UK law leaves them wholly exposed and it is a threat to public safety
1. NHS England/ Improvement eventually reluctantly disclosed a copy of the Kings Fund report on HSIB, terms of reference and associated correspondence, which showed that a rigorous investigation was never intended:
2. As discussed above, the dispatch of undesirable senior NHS managers is the exeception rather than the rule.
The number of cases of NHS England, NHSI and its predecessor bodies covering up, protecting and recycling abusive, incompetent and or dishonest NHS managers are too many to list.
But here is a striking example of former NHS CEO Paula Vasco-Knight, unpicked to show the lengths to which the protection often extends and why the HSIB case is different:
3. After leaving UHB in October 2021, Jacqui Smith took up two new NHS Chairs at Barts Health NHS Trust and Barking, Havering and Redbridge University Hospitals NHS Trust. This looks to be system preparation for a politically sensitive merger of the two trusts, which is already stirring up controversy, with Margaret Hodge stepping in.
Summary It appears from anonymous letters that staff at Hinchingbrooke Hospital may be whistleblowing about care failure surrounding A&E. The trust’s response so far is one of bizarre minimalisation, despite acknowledging some care failure. The trust’s CEO appears to think that anonymous letters are a sign that staff feel able to raise concerns, which hardly bodes well for organisational learning.
Like the rest of the NHS it has suffered the enormous stresses of the mismanagement of the COVID19 pandemic by the government.
It is now disturbed by anonymous whistleblowing by parties unknown. Disclosures have been made to trust managers and to at least one patient affected by a failure of tetanus management.
Unvaccinated patients presenting with injuries should have had their vaccinations histories checked and been given tetanus booster shots but allegedly, some did not.
This has been confirmed in one case, that of Marilyn Smith, reported by the BBC.
Ms Smith contracted tetanus after an injury in September 2021, for which she did not receive a tetanus shot. As a result she was severely unwell and hospitalised for 120 days and left with disabilities.
Two weeks after she was discharged from hospital, Ms Smith reportedly received several anonymous letters which claimed to come from:
“a group of current and previous A&E staff at Hinchingbrooke”
The letter described alleged shortcomings in her care and also claimed:
“the trust has been ignoring concerns about patient safety” and contained further allegations that related to an individual.”
The last NHS staff survey showed that the trust’s whistleblowing governance was on a downward trajectory:
The trust’s response to the BBC appeared somewhat self-contradictory.
It claimed that the trust had received and investigated a similar letter in October 2021and dismissed the concerns.
“The North West Anglia NHS Foundation Trust confirmed it had received a similar letter in October but after an investigation concluded there was no substance to the allegations about patient safety.”
“In a statement, Caroline Walker, chief executive of the trust, said they were meeting Ms Smith this week to discuss its investigation and report.
And yet the trust also conceded shortcomings in Marilyn Smith’s care:
“I would like to apologise to Marilyn Smith for the failure to identify her condition as quickly as we should have,” she said.“
Bizarrely, the trust CEO seemed to conclude that an anonymous letter was a sign that staff felt able to raise concerns:
“We welcome the fact that our staff feel able to raise concerns.
“We have worked hard, with the support of our Freedom To Speak Up Guardian, to encourage an environment where speaking up is something people can do with confidence.
“When issues are raised we take action to investigate and learn from them.”
That Olympic-Gold-level ostriching rather takes the biscuit.
This is therefore unlikely to be the last that we will hear about poor whistleblowing governance by North West Anglia.
Or about the woeful inadequacies of the Freedom To Speak Up project, which clearly does not provide a safe reporting channel when it really matters.
Declaration of interest: A member of my family has been injured on a number of occasions by Peterborough City Hospital, which is part of the above trust. We are wearily in conflict with the trust again over yet another episode of care failure, which they have admitted. Relevant to issues of transparency, the trust is overdue in responding to a subject access request for personal data, made directly to the trust CEO, which required a referral to the ICO.
PETITION
Please click and add your signature to this petition to reform UK whistleblowing law – whistleblowers protect us all but weak UK law leaves them wholly exposed and it is a threat to public safety
This delay included maintaining radio silence for a month even after NHS Improvement issued a final investigation report on 27 January 2021 which concluded the National Guardian’s former case review manager breached Dr Campbell’s confidentiality, and recommended that an apology be made.
NHS Improvement also recommended that the National Guardian’s Office should provide “confirmation of an improved approach to such matters in future”.
Again, no such evidence of improvement was given by the National Guardian’s Office for months despite being asked to urgently safeguard whistleblowers’ confidentiality. The request for such protection was first directed in August 2020 to Robert Francis, who has an oversight role, and then to Henrietta Hughes the National Guardian herself in December 2020. Neither responded to confirm that protective action was taken.
The lack of evidence of corrective action continued even after NHS Improvement’s recommendation of 27 January 2021 to demonstrate improvement.
A question arises of whether the silence by the National Guardian and her Office was hostile and an expression of resentment at being held to account.
On 27 February 2021 I protested about the lack of apology and learning to Ian Trenholm who is effectively the National Guardian’s line manager.
Two days later, an apology to Dr Campbell arrived from the National Guardian’s Office.
The apology did not come from the National Guardian but was delegated to her Head of Office, Russell Parkinson.
Parkinson did not acknowledge the extraordinary delay in apologising.
He also gave limited details of improvement:
“I will therefore issue a reminder to all National Guardian Office staff about the importance of preserving confidentiality and the requirement to obtain consent before the identity of individuals are disclosed, other than when there is a legal requirement to disclose someone’s identity.”
“In addition, I will strengthen the induction process and induction material for new members of the office to ensure that a full discussion of confidentiality is had with all new starters. I will also seek to strengthen our record keeping so that it is clear what level of consent has been obtained before there is any further discussion of a case.”
Of immense concern, it is implied that the National Guardian had not taken corrective action prior to this point, thereby knowingly exposing more whistleblowers to potential harm.
This is not the accountable, responsible or meticulous behaviour one would expect as standard from a whistleblowing agency.
I have written to Russell Parkinson to ask for clearer evidence of improvement and to ask the National Guardian for related policy improvements. For example, that she should make unplanned breach of whistleblower confidentiality by her Office a disciplinary matter, to underline how seriously confidentiality will taken.
It is after all a criminal matter in some jurisdictions to reveal a whistleblower’s identity.
It is not unreasonable that a whistleblowing agency should hold itself to similarly high standards.
I have copied the letter to Henrietta Hughes’ oversight board, comprising Robert Francis and Andrew Morris, woeful though they have been.
The letter to Parkinson is provided below in the appendix.
I would advise would-be whistleblowers to be cautious, to get everything in writing, to request personal data through subject access request if concerns arise about any impropriety and not to assume that those in authority will wish you well or will look after your interests.
UK whistleblowing law’s many faults include the fact that it does not specifically protect a whistlblower’s confidentiality and identity.
If you have not already done so, please help drive change by signing and sharing this petition to parliament for law reform.
LETTER 12 MARCH 2021 TO RUSSELL PARKINSON, HEAD OF OFFICE, NATIONAL GUARDIAN’S OFFICE
BY EMAIL
Russell Parkinson
Head of Office
National Guardian’s Office
12 March 2021
Dear Russell,
The National Guardian’s response to the breach of whistleblower confidentiality by her Office: corrective action
Thank you for your letter of 1 March 2021 to Dr Campbell and myself acknowledging the outcome of NHS Improvement’s investigation which concluded that the National Guardian’s Office breached Dr Campbell’s confidentiality.
I write chiefly with the aim of seeking reassurance that:
Future whistleblowers’ confidentiality will be safely protected by the National Guardian’s office and that more detail will be shared of the intended service improvements mentioned in your letter.
Unplanned breach of whistleblower confidentiality by anybody at the NGO will be treated as a disciplinary matter. The NGO will admit to any unplanned breaches immediately and it will also support any affected whistleblower and help to mitigate harm.
Planned breaches of whistleblower confidentiality will be rare, genuinely justified and properly managed, with support for the whistleblower
There will from here on be proper transparency and accountability regarding the Office’s interaction with whistleblowers’ employers. The NGO’s communications with employers will in future be fully documented and details will be shared with whistleblowers. There will be no clandestine, undisclosed communications.
In future, the National Guardian’s Office will apologise promptly as soon as it becomes aware of any failings, and in particular it will mitigate serious risks at the earliest opportunity instead of waiting months for complaints investigations to be concluded.
The National Guardian will conduct a wider review of Simon Pook’s work given the findings that he breached confidentiality and had undisclosed contact with an employer.
The National Guardian will ensure there is regular audit of the work of her office to ensure that there is adherence to operational standards.
This letter does not mean that Dr Campbell has accepted the outcome of NHS Improvement’s complaint investigation, and is without prejudice to any further steps he may decide to take.
I lay out my requests more fully as follows:
More details of proposed improvements by the National Guardian’s Office
I would be grateful for details of the planned strengthening of the National Guardian’s systems, with respect to this assurance in your letter:
“In addition, I will strengthen the induction process and induction material for new members of the office to ensure that a full discussion of confidentiality is had with all new starters. I will also seek to strengthen our record keeping so that it is clear what level of consent has been obtained before there is any further discussion of a case.”
Apologising promptly
I am glad that the National Guardian’s Office has finally apologised to Dr Campbell.
May I ask why it took so long?
Firstly, there was a shocking lack of empathy in Simon Pook’s response of 14 June 2019 to a distressed email by Dr Campbell when he discovered that his confidentiality had been breached by the National Guardian’s Office.
Breach of whistleblower confidentiality is an incredibly serious matter and the lack of apology is all the worse for this.
NHS Improvement’s investigation concluded that Simon Pook former NGO case review manager likely broke Dr Campbell’s confidentiality to his employer and Mr Pook reportedly accepted this.
Did Simon Pook inform the National Guardian or anyone else at the National Guardian’s Office in June 2019, that Dr Campbell’s confidentiality had been breached?
If he did, who at the National Guardian’s Office was aware of the breach at that point, and what was the organisational response?
Who at that point was the most senior person who was aware of the confidentiality breach?
Why was no apology provided by the National Guardian’s Office when I brought the matter to Robert Francis attention in August 2020?
I presume Robert Francis liaised with the National Guardian’s Office about the confidentiality breach at this point, but please confirm that he did so, when and whom he informed.
Why was an apology still not provided by the National Guardian’s Office when NHS Improvement’s final report was issued on 27 January 2021, with the formal finding of confidentiality breach?
An apology has only come now after I wrote to Ian Trenholm about the lack of an apology.
NHS policy is to express regret and say sorry straightaway to patients and families when things go wrong, and the NGO should act in accord with this.
Request: Please could the National Guardian’s complaint policy be amended to specifically reflect that an apology will be given promptly as soon as it is clear that there has been a failing, whether or not a formal complaint investigation has been completed.
Acting urgently on serious risks
It is disappointing that the National Guardian’s Office is only acting now to strengthen its systems to prevent unjustified breaches of whistleblower confidentiality when it has known about the breach of Dr Campbell’s confidentiality for months if not longer.
This implies that other whistleblowers have been potentially and avoidably exposed to similar risk. This not only affects the whistleblowers but the patients and co-workers who depend upon them.
Good whistleblowing governance focuses on promptly addressing the primary concerns raised by a whistleblower and not diverting into or delaying through adversarial processes. The National Guardian should act in this spirit.
Request: Please can the National Guardian’s complaint policy explicitly commit the National Guardian to correcting any future failings at the earliest stage possible, instead of waiting until a formal complaint investigation is concluded before acting.
Policy for managing breaches of whistleblower confidentiality
At present, the FAQs on the National Guardian’s website state that in all cases the National Guardian’s Office will tell whistleblowers if it decides to breach their confidentiality
“20. How will the NGO protect my confidentiality when I submit a case for review?
Wherever possible, the NGO will seek to protect the confidentiality of individuals who refer cases to it. In most circumstances the NGO will ask a referrer for their consent before discussing their case with their employer or any other agency. The office will only share information contained in a case review referral where there is a need to protect individuals from possible harm, for example where the matter relates a safeguarding issue. In all circumstances, the NGO will let referrers know when they have discussed or shared information about their case with another organisation.” [my emphasis]
However, the National Guardian’s Office did not inform Dr Campbell that it breached his confidentiality. Nor did it offer Dr Campbell any support with the consequences of its breach of confidentiality.
Request: May I suggest that the National Guardian’s policy includes an additional commitment that wherever the National Guardian’s Office breaches a whistleblower’s confidentiality, it will urgently provide the whistleblower with support to manage any risk or harm that arises from this.
Also, the policy should indicate that if a breach of confidentiality is planned and deliberate, the National Guardian’s Office should if at all possible inform the whistleblower beforehand that their confidentiality is about to breached. This would give the whistleblower the greatest chance of mitigating the harm that any breach of confidentiality might cause.
This would be consistent with NHS Improvement’s recommendation:
“In future, the NGO would benefit from taking greater care ahead of contacting individuals at an organisation about a FTSU case, by ensuring it notifies the individual who has spoken up of its intentions, and allow the individual reasonable opportunity to express any concerns they may have about the proposed course of action.”
In my view, the only valid exception to warning a whistleblower of a planned breach of their confidentiality is if they are the subject of any safeguarding concerns and non-disclosure is necessary to preserve evidence.
Where there are deliberate breaches of whistleblowers’ confidentiality, there must by policy be a full written account of the risk justification for doing so.
The National Guardian’s form, that whistleblowers complete when requesting a case review, should be amended to reflect the above policy changes.
May I also suggest that the National Guardian’s procedural documents be amended to include a clear policy statement to all who work at the NGO including the National Guardian, that breaches of whistleblower confidentiality without just cause are a disciplinary matter.
Record keeping and transparency about communication with whistleblowers’ employers
A disturbing aspect that emerged from NHS Improvement’s investigation of the breach of Dr Campbell’s confidentiality is the poor documentation of telephone calls by the National Guardian’s Office to Dr Campbell’s employer.
On 20 November 2020, NHS Improvement wrote:
“On 3 June 2019, the case review manager contacted the trust’s FTSU Guardian to arrange a telephone discussion, but the topic of conversation was not specified in the email. Shortly afterwards it appears that a phone call took place. I have not been able to locate a note of such a call.”
“On 14 June the National Guardian had a telephone call with the chief executive and Dr Campbell’s name is referred to in her note of the call.”
The fact of one of these calls and the details of both these calls by Simon Pook and the National Guardian were not disclosed to Dr Campbell.
The poor documentation and lack of transparency are unaccountable practice, which does not help with confidence nor demonstration of good faith and impartiality by the National Guardian’s Office.
Poor record keeping by the National Guardian’s Office may also disadvantage whistleblowers in any future processes such as defending themselves against retaliatory charges by employers or any legal action that they may be forced to take.
The poor record keeping is of greater significance given that the National Guardian’s Office has demonstrated that it is aware of the sensitivity and importance of good whistleblowing records through its existing guidance to trust Freedom To Speak Up Guardians:
“Be aware that your records may be requested weeks, months or even years after their creation and this should be taken into account when setting up your systems.”
In the NHS, it is now quite normal for clinical letters between health professionals to be shared with patients. The National Guardian’s Office should act in this spirit of accountability and transparency.
Request: Please could the National Guardian amend her policies to ensure that her Office’s contacts with whistleblowers employers are properly documented and that the details of such communications are routinely shared with whistleblowers.
Further investigation needed
You acknowledge that Simon Pook was sufficiently experienced and trained to be reasonably expected to know that he should not breach Dr Campbell’s confidentiality, but that he seemingly did so nevertheless.
This is particularly serious and leads to a number of difficult questions, including whether the confidentiality breach was consciously done.
Request: Please can the National Guardian trigger a review of Simon Pook’s work if she has not already done so, to check for any other possible breaches of whistleblower confidentiality and any covert, undisclosed communication with whistleblowers’ employers.
Obviously, the proper disclosures would need to be made to any other whistleblowers whose confidentiality has been breached.
If a review has already been triggered, please advise on whether it has been completed or if not, when it will be completed.
Regular audit of practice standards at the National Guardian’s Office
Related to a wider check of Simon Pook’s work, may I ask what arrangements the National Guardian has for monitoring adherence to her Office’s policies and standards?
Are quality audits regularly carried out?
If so, what audits are undertaken and what are the specifications for these audits?
You acknowledged through Simon Pook’s example that experience and training do not always prevent failure to adhere to policy.
It is important that there is quality monitoring that can pick up failures to adhere to policy.
If audits are not regularly carried out on important matters such as standards in record keeping, seeking whistleblowers’ consent for sharing information and protecting whistleblowers’ confidentiality and identity, failures may go undetected and uncorrected.
Request: If the National Guardian does not currently have a policy of carrying out regular quality audits on the work of her Office, please advise if she will adopt such a policy.
Many thanks,
Minh
Dr Minh Alexander
Cc Dr Julian Campbell
Tom Grimes NHS Improvement lead for whistleblowing
Dr Henrietta Hughes National Guardian
Robert Francis CQC NED and member of National Guardian’s Accountability and Liaison Board
Andrew Morris NHS Improvement and Chair of National Guardian’s Accountability and Liaison
By Dr Minh Alexander NHS whistleblower and retired consultant psychiatrist, 11 March 2021
Summary: NHS Improvement has decided that Andrew Morris NHS Improvement non executive director will continue in his role as chair of the National Guardian’s Accountability and Liaison Board despite an instance of proven whistleblower reprisal by Frimley Health NHS Foundation Trust, when he was trust CEO and line manager to a director criticised for their part in the whistleblower detriment. The whistleblower harmed was Donna Simmonds, an administrator who raised patient safety concerns. Moreover, the trust’s litigation in the case was signed off by another of Morris’ direct reports, the director of Human Resources. Is there sufficient clear blue water between Morris and the proven whistleblower detriment? CQC missed the whistleblower detriment at the time and instead praised Frimley’s whistleblowing governance. Most recently, CQC asked Frimley for evidence of learning from the Simmonds whistleblowing case, but the trust response was grudging and thin. Frimley Health NHS Foundation Trust serves former health secretary Jeremy Hunt’s constituency. Frimley featured prominently in Hunt’s patient safety crusader narrative and also in the National Guardian’s propaganda. However, the well known twenty year cover up of baby Lizzie Dixon death under Frimley’s care took place on Andrew Morris’ watch.
The NHS National Guardian for whistleblowing is funded and supervised by those whom she is supposed to hold to account, namely the Care Quality Commission and NHS England/Improvement.
This is not reassuring.
The supervising structure is the National Guardian’s Accountability and Liaison Board and comprises Robert Francis and Andrew Morris and Henrietta Hughes. Morris and Francis are non executive directors of CQC and NHSI respectively, and Henrietta Hughes holds the office of the National Guardian for whistleblowing in the NHS.
Francis previously chaired the Accountability and Liaison Board, and so was scrutinising a flawed project which he designed.
Francis refused to meet with me to discuss concerns about the Freedom To Speak Up project. Francis’ correspondence to the National Guardian disclosed via subject access request revealed that this refusal was based on his belief that he could not change my mind, raising questions about his objectivity about his brainchild and ability to process challenge.
Francis was replaced by Andrew Morris as chair of the Accountability and Liaison Board.
I raised concerns with NHS Improvement about this role because of knowledge of victimisation whistleblowers by of Frimley Health NHS Foundation Trust, when Morris was trust CEO.
After five months, NHS Improvement responded thus on behalf of Dido Harding on 9 March 2021:
“Hi Minh
Thank you for your email and apologies for taking so wrong [sic] to reply directly to this.
We have considered the tribunal findings and can understand why you have raised it. I have liaised with Dido, Sir Andrew Morris and Henrietta Hughes on this matter.
Having discussed with Sir Andrew, it seems that he was not directly involved in this matter. Nonetheless, NHSE/I will consider whether we might incorporate learning from this into our broader work to improve people practices in the NHS.
Sir Andrew will remain in his role on the NGO’s ALB.
Thank you again for bringing this to our attention.
With best wishes”
But the ET found that Helen Coe the then Frimley Director of Operations and Sarah Casemore Deputy Director of Operations were responsible for detriment to Donna Simmonds in terms of not allowing her to return to her original role:
“We have considered the reasons why Ms Casemore and Ms Coe reached the decisions that they did that the claimant’s working relationships had broken down so that the claimant could not return to her original role. The respondent said that the problems with the team were not limited to the claimant. It was accepted that the team as a whole was dysfunctional. We did not hear any evidence about why the respondent decided that, despite there being a problem across the whole department, it was the claimant who had to move. As set out above, there was evidence before us that the claimant was regarded by her managers as difficult and a troublemaker and we have inferred that her first two protected disclosures materially influenced that perception. We also infer that the perception of the claimant as a troublemaker by her line managers played a material part in the decisions by Ms Casemore and Ms Coe that there had been a breakdown in the working relationships between the claimant and her managers in the department and the decision that it was the claimant who had to move.”
It is hard to understand how Andrew Morris could not know about the case given that Helen Coe was his direct report. It would surely be a failure of oversight if he did not.
But NHS Improvement’s response gives comfort to NHS trust chief executives, who can heave a sigh of relief that they will not be held accountable for serious wrongdoing so long as they are not “directly involved”.
In between my letter of 26 October 2020 to Dido Harding and NHS Improvement’s reply of 9 March 2021 Andrew Morris signed off an NHS Improvement complaint investigation about the National Guardian and her Office, which interviewed only two of four key witnesses.
Morris reportedly stuck to his guns after a query. He was overruled after I appealed to Dido Harding.
Alongside querying Morris’ role as chair of the Accountability and Liaison Board, I also asked Frimley Health NHS Foundation Trust about executive responsibility for the handling of the Donna Simmonds whistleblowing case.
The trust’s reply indicated that another of Morris’s direct reports, the Director of Human Resources was ultimately responsible for signing off the trust response to Donna Simmonds’ ET claim:
I leave it with readers to judge if there is sufficient clear blue water between Morris and the victimisation of a whistleblower, to justify his continuing role in shaping the work of an agency that is supposed to help NHS whistleblowers.
For completeness, in October 2020 I also sent the Simmonds ET judgment to Ted Baker CQC Chief Inspector of Hospitals who kindly took the matter up with the local CQC inspection team. At the material time CQC had failed to either pick up or report the Simmonds case. In fact, CQC praised Frimley’s whistleblowing governance:
“Managers across the trust promoted a positive culture that supported and valued staff, creating a sense of common purpose based on shared values. The trust had a well-publicised and embedded values system developed in conjunction with its staff. Staff described and open and positive culture at the organisation. Staff demonstrated a sense of belonging and frequently talked about a “family feel” at the organisation. The trust supported effective employee relations and staff could formally raise concerns through effective human resources procedures”.
The local CQC team told me that they would ask Frimley for evidence of learning from the Simmonds case.
I asked Frimley what evidence of learning the trust gave to CQC. This is the document disclosed by the trust in response:
There are some process improvements but alas, the specific trust response to causing a whistleblower detriment is very flimsy. It consists of waffle on defining “detriment” as opposed to any action to robustly deter it.
Importantly, Frimley’s response to CQC implied that the trust did not seek to learn from the Simmonds case until approached by the CQC.
Overall, Frimley’s response to CQC reads as a reluctant document, which shows little empathy and makes little if any acknowledgment of the injustice and harm to the whistleblower.
An important contextual factor is that Frimley’s reputation has been a political issue. In June 2014 Jeremy Hunt announced that he had hired recently knighted Robert Francis to undertake the Freedom To Speak Up review on whistleblowing in the NHS as a response to pressure over scandals. Hunt also brandished a list of twelve NHS trusts which he claimed had signed up to his grandiose campaign to make “the NHS the safest healthcare system in the world.” Frimley was amongst those who were obligingly helping with Hunt’s tinselly narrative.
Andrew Morris became Frimley’s chief executive in 1991. His tenure as chief executive spanned the death of baby Lizzie Dixon under Frimley’s care on 4 December 2001, and a subsequent twenty year multiagency cover up.
An investigation by Bill Kirkup, published by the government on 25 November 2020, focussed on dishonesty by frontline clinicians but said almost nothing about the governance of their employer, Frimley Park Hospital.
The then Chief Executive of the Strategic Health Authority was interviewed but oddly, Andrew Morris was not listed amongst individuals interviewed by Kirkup’s investigation.
Buried in the investigation report appendices is the sentence:
“Allegations about the fitness to practise of medical staff involved in her death were considered by the General Medical Council, and complaints were considered by Frimley Park Hospital and Great Ormond Street Hospital”.
Kirkup made no specific recommendations for Frimley, but there is a comment that community care should be properly planned and should not discriminate against disabled people through the application of lower standards:
“Community care for patients with complex conditions or conditions requiring complex care must be properly planned, taking into account and specifying safety, effectiveness and patient experience. The presence of mental or physical disability must not be used to justify or excuse different standards of care.”
We will limp on with cover ups, subpar whistleblowing governance, conflicts of interest and ramshackle sham ‘protections’ systems for as long as there is no political will to do it properly.
If you have not already done so, please help drive change by signing and sharing this petition to parliament for law reform.
By Dr Minh Alexander, NHS whistleblower and retired consultant psychiatrist, 9 March 2021
NHS mental health beds have been unsafely slashed over the years with little of the promised re-investment in intensive community services materialising. Deinstitutionalisation has merely meant neglect in the community.
Alongside this, unsatisfactory private mental healthcare services funded largely by the public purse have proliferated.
Vulnerable NHS patients are made even more vulnerable by being shipped out of area to private care, away from the support and scrutiny of family and friends.
The quality of such private services has often been poor, sometimes dire, with frank abuse.
NHS England as the lead commissioner has failed to ensure effective, proactive commissioner oversight of the care received by these isolated, exiled patients. Scandals keep recurring.
AN EXAMPLE
Multiple mental health units operated by the private healthcare company the Priory Group have been placed in special measures by the Care Quality Commission.
St Johns House, Palgrave, Norfolk, run by Partnerships in Care Ltd which is a subsidiary of the Priory Group, is the latest to enter special measures. CQC’s inspection report of 5 March 2021 makes unbearable reading because it comprises a long, long list of serious care and governance failings. The findings amount to institutional abuse.
This is a small selection of the failings detailed by CQC’s report:
“We reviewed a random selection of CCTV footage between 17 November and 12 December 2020 to observe how staff were managing patient observations. We found that in five out of five checks, staff were sleeping on duty.”
Managers were informed that some staff had been sleeping on duty but according to the CQC “ no action was set to address this”.
CQC reported “a staff member was seen to push a patient onto the floor”.
One incident of restraint led to staff suspensions and a report to the police, but only after CQC intervened.
Staffing was often inadequate, seclusion practice was poor, there was high use of force without de-escalation, failure to report safeguarding issues, failures to mitigate ligature risk and many incidents and injuries. There were insufficient therapeutic interventions, leaving an emphasis on dreadful, custodial care.
The appalling treatment of whistleblowers by such private providers, guarding their profits, is part of the problem.
Dr Ambreen Malik’s whistleblowing case against Cygnet Health Care Ltd gives a glimpse into how far some of these private providers will go in suppressing safety concerns and mistreating whistleblowers.
Dr Malik’s case is not the first whistleblowing case at Cygnet and it will not be the last.
I have written to NHS England to ask that it:
Increases the whistleblowing governance standards required of private providers who receive public funding through contractual means.
2. Exercises its commissioning power to stop Cygnet from going ahead with a threatened appeal against the Employment Tribunal judgment in Dr Malik’s favour, which will have a chilling effect on Cygnet’s workers.
3. Ensures that any final NHS standards for Fit and Proper managers in the NHS, arising from the Kark Review implementation, are applied to private providers who receive public funding.
At present there is a fig leaf applied by NHS England in the form of a contractual requirement that private providers should appoint Freedom To Speak Up Guardians.
Cygnet appointed a Freedom To Speak Up Guardian as part of managing adverse publicity about its serious care failures.
I have disabused NHS England of any claims that a contractual requirement for a Freedom To Speak Up Guardian suffices, and provided evidence that has accumulated about the deceptive and pernicious nature of the Freedom To Speak Up project.
The letter to NHS England follows:
BY EMAIL
Noel Gordon
Non Executive Director
Chair of Specialised Services Commissioning Committee.
NHS England
8 March 2021
Dear Mr Gordon,
Suppression of safety concerns and whistleblower reprisal by Cygnet Health Care Ltd, a private contractor which provides services to the NHS and policy issues which arise
I write to you in your capacity as chair of NHS England’s Specialised Services Commissioning Committee to ask that NHS England takes action to ensure that private contractors have better whistleblowing governance and Fit and Proper Directors.
An Employment Tribunal has decisively determined in favour of Dr Ambreen Malik consultant psychiatrist and whistleblower, that there has been serious whistleblower reprisal, “a litany of bad faith”, “dishonesty” and or “less than honest” behaviour by several Cygnet Health Care Ltd directors. This included the chief executive Dr Tony Romero. The Tribunal held Dr Tony Romero responsible for most of the acts by others::
“Dr Romero was responsible in effect for nearly all of the actions taken by the other parties, through Jenny Gibson [Cygnet Director of Human Resources].”
The ET also described a retaliatory GMC referral by the then medical director as “venomous and dishonest” in tone.
The incident which sparked this whistleblower reprisal was Dr Malik’s insistence on doing her duty and giving a coroner’s inquest the full truth about the circumstances of a patient’s death.
Obvious issues of CQC Regulation 5 Fit and Proper Persons arise, and I have forwarded the ET findings to the CQC.
Cygnet relies largely on public funding, as confirmed by its 2019 annual report, and public accountability is therefore needed.
Cygnet reportedly informed the Times that it intends to appeal against the ET verdict.
Yet the Tribunal demonstrated robustly how it came to its decision, and much of its conclusions are based on clearly recorded original evidence which contradicted Cygnet’s later witness evidence.
It is hard to see how Cygnet will succeed, but an appeal will cause even more suffering to Dr Malik and her family. Very seriously, it will also have a chilling effect on any other Cygnet employee who is thinking about whistleblowing.
Dr Malik’s case is not the first Cygnet whistleblowing case in the public domain. There are also others that are not in the public domain.
NHS England has a particular duty to ensure that patients who are most vulnerable as a result of being sent out of their home area and isolated from normal sources of support are not left at the mercy of poor care and unscrupulous corporate practices.
There has been an abundance of scandals for years concerning private mental health care providers who derive most of their income from the public purse.
It is time for NHS England to significantly improve its oversight of these services to ensure the safety and welfare of these most vulnerable and isolated patients.
Ensuring better whistleblowing governance is an important part of this.
My requests to NHS England are as follows:
1. I would be grateful if NHS England could look into the ET findings of serious executive wrongdoing at Cygnet and ensure here on that any public contracts with private providers of healthcare contain robust enough standards to ensure better whistleblowing governance, and to punitively deter bad whistleblowing governance.
2. Please can NHS England use its commissioning power to deter Cygnet from appealing against such a conclusively evidenced ET judgment, and from causing Dr Malik and her family yet more suffering and intimidating other workers.
All whistleblowers are seriously harmed by the enormous stress of litigation and prolonged conflict. These processes take a substantial toll on health.
It would be a great regret if NHS England does not show that it is willing to check employers’ excesses and to protect the rights of all Cygnet’s workers to safeguard patients.
In the case of Dr Kevin Beatt another whistleblower who received a similarly decisive ET judgment in his favour, ministers and regulators all failed to restrain his former employer Croydon Health Services NHS Trust. Croydon incurred millions in costs through repeatedly appealing and then being ordered to pay about £1 million in compensation:
This was a gross waste and completely unjustified use of public money, as well as a severe injustice to Dr Beatt who suffered years of extremely stressful litigation.
I fear that if NHS England does not restrain Cygnet, yet more money that ultimately comes from the public purse will be recklessly wasted.
3. May I also ask that NHS England/Improvement considers bringing the directors of private contractors within the scope of its Kark Review implementation on NHS Fit and Proper Persons, and reflecting any final Kark standards in NHS contracts with private providers. Where public money is spent, the same standards should be expected.
I am aware that NHS contracts with the private sector contain a requirement for organisations to employ a Freedom To Speak Up Guardian but this is frankly a tissue thin device. The Freedom To Speak Up project was a weak policy design that has been badly executed, failing many whistleblowers. I provide links to relevant evidence in the appendix.
Bad employers merely exploit an appointment of a Freedom to Speak Up Guardian for cynical PR, whilst continuing with bad governance.
Cygnet announced it would employ a Freedom To Speak Up Guardian but this is in reality gives no assurance.
In general, I would urge NHS England to scrap the wasteful Freedom To Speak Up project because it adds no value where an employer is honest and only gives bad employers more tools for covering up and victimising whistleblowers, whilst maintaining a false façade of good governance.
In the meantime, I would also be grateful for information as follows:
1. Does NHS England have a system in place to track employment tribunal claims against private healthcare providers with whom it holds national contracts for specialised services?
2. What standards of whistleblowing governance does NHS England require of private healthcare providers from whom it contracts services? Please disclose or point me to the relevant documents.
3. What standards of whistleblowing governance does NHS England expect CCGs to require from healthcare providers from whom they contract services? Please disclose or point me to the relevant documents.
4. Does NHS England hold central data on complaints received about care provided by Cygnet Health Care Ltd? If so, please disclose the number and details of complaints about care provided by Cygnet Health Care Ltd in the last two years.
I copy my letter to the Joint Committee on Human Rights which held an inquiry into serious and systemic breaches of patients’ rights by private mental healthcare providers, including Cygnet.
I also copy this letter to Dido Harding, Simon Stevens and other members of NHS England’s Specialised Services Commissioning Committee, and to Tom Kark QC and Claire Murdoch NHS England’s Mental Health Tsar.
I would be grateful if this correspondence could be passed to those for whom I have no direct email address
Yours sincerely,
Dr Minh Alexander
Cc Harriet Harman Chair of JCHR
Dido Harding Chair NHS Improvement
Simon Steven CEO NHS England
John Stewart NHS England Director of Specialised Commissioning
Michelle Mitchell NHS England Non Executive Director
Moira Gibb NHS England Non Executive Director
Ian Dodge NHS England National Director of Strategy
Stephen Powis National Medical Director NHS England
Tom Kark QC
Claire Murdoch National Mental Health Director NHS England
APPENDIX
Evidence of failures of the government’s Freedom To Speak Up project
The Freedom To Speak Up model was not evidence based:
And yet millions have been wasted on this project.
The Freedom To Speak Up model is unworkable due to the central conflict of interest that it relies on employees to hold erring employers to account, and because it gives no genuinely independent channel for whistleblowers concerns to be investigated. By design, employers are left in sole control of the investigation of whistleblowers’ concerns.
The National Guardian fails to track the outcomes of concerns raised with NHS trust Freedom To Speak Up Guardians and whether NHS trust staff’s concerns are addressed:
The National Guardian has failed to carry out enough case reviews. Her Office gives poor value for the funding it receives at an average of two case reviews a year.
The National Guardian has declined to adopt the role recommended by the original Freedom To Speak Up Review of helping to ensure that harm to whistleblowers and patients is redressed. Her case reviews only make bland general recommendations:
The National Guardian and her Office havr sometimes colluded with employers and the Office has sometimes acted with the effect of covering up its failures to effect improvement as a result of case reviews: