By Dr Minh Alexander retired consultant psychiatrist 20 May 2022
Summary: The Practitioner Performance Advice Service (formerly the National Clinical Assessment Service or NCAS) has a history of enabling NHS employers’ victimisation of medical whistleblowers by rubber stamping unjust suspensions and disciplinary action. PPA issues advice based on what it is told by employers, which is sometimes false. Employers manipulate the process to obtain the advice that they want from PPA, in order to seriously mistreat staff who may be blameless. This poses serious health risks to the mistreated staff and represents a gross waste of precious medical personnel. NHS Resolution has now agreed to consider safeguards against being fed false information by employers, such as requiring a statement of truth from employers.
PPA, formerly NCAS, is an NHS oddity which supervises the operation of the much criticised Maintaining High Professional Standards process in the NHS – a disciplinary process for senior doctors. In recent years NCAS (PPA) has come under the control of NHS Resolution.
Maintaining High Professional Standards (MHPS) 2005
MHPS was seen as an own goal by the BMA which accepted this provision in place of much more rigorous and fair processes for disciplining senior doctors.
The well-known case of Wendy Savage obstetrician, who was successfully defended under the old procedure, would most likely have turned out quite differently if she had been at the mercy of MHPS.
Consultants used to have rights of appeal to the Secretary of State. Nowadays, whistleblowers’ letters just pile up on the floor of the Minister’s office, assuming they are even allowed to get that far. Part of the game is to block contact, to preserve plausible deniability.
For the little that it is worth, this is a link to official NHS guidance for employers on the competencies required of case investigators and case managers:
PPA has no powers, it is merely a consultative service with which employers must liaise in order to trigger suspensions and disciplinary action on grounds of incapability or misconduct.
In the experience of practitioners at the receiving end of this service, employers easily manipulate this arrangement by feeding whatever information is necessary to NCAS to get a desired outcome and a rubber stamp for their actions.
Those who are entirely blameless can be easily suspended and disciplined by abusing the MHPS/PPA mechanism.
And so many NHS whistleblowers have been roughed up by this route.
The unnecessary suspension of doctors is both traumatic for the individuals, constituting serious threat to health, and also a great waste of precious personnel resource for the NHS.
Surgeons in particular are easily de-skilled and it is very wrong that precious, expensively trained medical resource can be so easily flushed down the drain by corrupt managers covering up and protecting their own interests.
After continuing examples of baseless whistleblower exclusions such as those of Mr Tristan Reuser and, Dr Jasna Macanovic, I pressed NHS Resolution, to ensure that PPA implements safeguards against employers’ lies about whistleblowers.
This is a letter of 27 March 2022 to NHS Resolution’s CEO Helen Vernon about the issue:
Today, NHS Resolution has responded in a letter about various matters, with the relevant extract as follows:
“Turning to the first and the query about declarations from managers (including medical managers) who request advice and interventions (including assessments) from Practitioner Performance Advice. You will be aware that we already ask at the point of an initial contact with Advice whether the practitioner is a whistleblower or has made public interest disclosures and are able to offer advice within the context of that. We would anticipate this would be considered routinely throughout the lifetime of a case.
We are currently reviewing our approach to cases which go to the Assessment Consideration Group which determines whether or not a case is suitable for a behavioural or clinical performance assessment or professional support and remediation plan (and is being extended to consider team reviews and assisted mediations). This is equivalent to the type of decision making forum where the GMC have implemented Hooper’s recommendations as part of the fitness to practice referrals. We will be considering with stakeholders (including practitioners) how we can incorporate a statement of truth regarding their referral and whether we need to do something in addition to our current practice to consider whether or not the practitioner has made public interest disclosures. In our referral documentation the practitioner has space to write about the referral from their perspective and this currently provides an opportunity for practitioners to record if they consider themselves to be a whistleblower.” [my emphasis]
So we may in due course see a requirement for medical managers to make a statement of truth when referring doctors to PPA and when seeking PPA’s agreement for exclusions and disciplinary action under MHPS.
This would not stop victimisation but it would add a small safeguard that can be levered if necessary. As was a similar GMC safeguard in the case of Mr Reuser, when a false GMC referral ended in a GMC warning against his former medical director.
I have asked NHS Resolution to:
Advise of the timescale for the above work and to feed back the outcome of its deliberations.
Ask referring medical managers to make a formal declaration about whether the referred doctors are whistleblowers. It is not enough just to ask referred doctors to self-declare. The whole point is that referring organisations must be made to take responsibility and be held accountable for how they treat whistleblowers, in full awareness of a person’s status as a whistleblower.
I have emphasised that insufficient protective action, by not deterring employers’ abuse of process, would mean that NHS Resolution risks contributing to the serious personal injury of blameless whistleblowers. Which would be rich for the agency that oversees the NHS’ compensation of staff for work-related injuries.
Petition
UK whistleblowing law is currently unfit for purpose and allows employers to cover up and persecute whistleblowers with impunity.
If you wish to protect UK whistleblowers and to help stop their concerns being covered up, please click on this link and lend your signature to this petition for much better UK whistleblowing law:
By Dr Minh Alexander retired consultant psychiatrist 16 May 2022
Summary: The NHS trust which employed a bogus doctor Zholia Alemi as a consultant psychiatrist also allowed an unqualified healthcare assistant Samantha Robinson to practice far outside her scope for years as a specialist epilepsy ‘nurse’, running clinics and advising on specialist medication without any input from specialist doctors, sometimes for years. This was despite the situation being known to qualified clinicians and trust managers. When Jane Archibald a specialist nurse joined the trust, she was horrified to discover the situation. Her whistleblowing about this matter and other issues of concern was not met with a safe response by the trust. She experienced reprisal and an Employment Tribunal ultimately found that she had been unfairly constructively dismissed. A poorly executed grievance process was found to be a whistleblowing detriment, with a trust manager falsely claiming to the grievance investigator that the records of the whistleblowing disclosures were not available for inspection. The trust denied that Jane Archibald had made protected disclosures, right up to the last minute until the Tribunal ruled that she had. A disclosure letter that she sent to Stephen Eames the trust Chief Executive asking for his help with the unresolved patient safety concerns and her experience of reprisal was met only with silence. The Care Quality Commission was equally unhelpful and reportedly told her that the issues were an internal matter for the trust. Many issues remain to be resolved.
On 13 May 2022 the Employment Tribunal published a most shocking judgment in the case of Jane Archibald, an unfairly sacked whistleblower. This is the judgment against North Cumbria Integrated Care NHS Foundation Trust, which sacked her:
The Tribunal determined that she had been unfairly constructively dismissed and that the poor handling of a grievance by her constituted a whistleblowing detriment:
“The complaints of protected disclosure detriment in relation to the complaints about the outcome of the grievance and the grievance appeal are well founded.”
Jane Archibald’s whistleblowing concerns and the trust’s poor response
Jane Archibald worked at Cumbria Partnership NHS Foundation Trust, a mixed mental health trust, between 2015 and 2020 as a Senior Nurse Practitioner/Specialist Epilepsy Nurse.
In her time at the trust, she discovered extraordinarily poor clinical practice.
The most striking discovery was that an unqualified healthcare assistant Samantha Robinson had been allowed to work for years without adequate supervision. She ran epilepsy clinics and advised general practitioners on specialist medication. Sometimes the patients were not seen by a specialist doctor, a neurologist, for years.
Epilepsy medication is powerful and sometimes toxic, and it is of great concern that an unqualified person was in a position to make changes to patients’ medication.
Example
This extract from the Employment Tribunal judgment gives the type of disclosure made by Jane Archibald via the trust incident reporting procedure, and the management response to the report:
“Patient attended the Epilepsy Nurse Clinic for review at Hilltop Heights. Noted from the EMIS notes patient had not been reviewed by a Neurologist since attending the Neurology Department, patient transferred in November 2011.
“Only person to have reviewed patient was SR Epilepsy Advisor.
“SR [Samantha Robinson] had made reference to patient’s medication that she would make “no changes to patient’s medications”.
“No evidence of a referral letter on transfer letter in 2011”.
33. Jonathan Kenworthy inserted in the outcome details:
“SIRI investigation has identified the root cause of the incident – many lessons learnt including Sam Robinson no longer employed as Epilepsy Advisor. A lack of supervision and governance was historically cause of the issues. Investigation has resulted in epilepsy safety plan with clear guidance of appropriate service governance that is underwritten by Registered practitioners working with the patient group”.
Robinson was referred to by some as a “neurology specialist” and or “epilepsy nurse”, as noted by the Tribunal, who also noted the trust management’s denial of the extent of the governance failures:
“24. In or around February 2015, soon after the claimant started her role, the claimant had a meeting with Samantha Robinson. Samantha Robinson told her that she had her own clinics. We find that she told the claimant that she prescribed medicines. Fiona Dixon [Senior Network Manager for the Neurology Service] did not think that an investigation found that she had done that; however, the document at page 217 indicates that she made recommendations about medication.
25.The claimant also discovered that Samantha Robinson was described on correspondence as a nurse. An example of this is at page 217. Samantha Robinson was not a registered nurse. There are various references in documents to Samantha Robinson as a “Neurology Specialist” (p.216), and “Epilepsy Nurse” (pp.224, 226).
26. We consider it more likely than not that Samantha Robinson described herself in this way with the knowledge of at least some managers and clinicians. This appears to be supported by the evidence of Fiona Dixon, who describes the concerns the claimant raised about Samantha Robinson being the “product of the historic structure” and why there was no disciplinary action against Samantha Robinson (para 25).”
One of Jane Archibald’s peers had reportedly supervised Samantha Robinson:
“21. It appears that Graham Bickerstaff may, at some time prior to the claimant’s appointment, have had some supervisory responsibility for Samantha Robinson. In her letter to the Chief Executive dated 8 August 2019 (p.559), the claimant wrote that she had been told by Graham Bickerstaff that he used to be her supervisor. The claimant, in submissions, also relied on the document at page 763, on which Graham Bickerstaff is described as Team Leader, of the neuroscience service”.
Very worryingly, Robinson saw many vulnerable patients with a Learning Disability. She also saw patients who were women of child bearing age, with regards to the teratogenic effects of some anti-convulsant medication, especially sodium valproate. The latter can cause devastating harm to developing babies in the womb, resulting in major congenital malformations, developmental delay, intellectual disability, neurological and psychiatric disorders:
When Jane Archibald raised concerns about this surreal situation, she was met with an equally surreal organisational response. According to Archibald, no rigorous investigation was mounted and those responsible for allowing this situation oversaw the organisational response to her concerns.
The Employment Tribunal noted that Fiona Dixon the Senior Network Manager for Neurology suggested in incident forms that Samantha Robinson was removed from her post for malpractice. But the Tribunal found that the reality was that Robinson went off sick and was simply allowed to leave the trust via redundancy. An astonishing failure of Safeguarding:
“28. Samantha Robinson went on sick leave and remained on sick leave until she left the trust. Her employment was terminated by reason of redundancy and no disciplinary action was taken against her. We consider that this is contrary to the impression given on incident forms, which suggest she was removed from post because of concerns about her practice e.g. as referred to in the incident form completed 21 December 2015 on which Fiona Dixon wrote: “The unregistered member of staff was investigated and is no longer with the Trust.”
This saga of Samantha Robinson being allowed to masquerade as an epilepsy specialist is all the more concerning because Cumbria Partnership NHS Trust is where the bogus doctor Zholia Alemi, who posed as a psychiatrist for years. This first came to light through the diligent investigation of a local press reporter.
Jane Archibald also found serious problems with the use of buccal midazolam for epilepsy by nurses, mainly within the Learning Disability section of the trust. This drug is a sedative and can cause respiratory arrest. Archibald found that midazolam was not used within protocol, placing patients at risk, and that some nurses acted outside of their remit.
Reprisal and lack of protection
As a result of raising concerns, Jane Archibald found herself increasingly ostracised.
Managers started focussing on the manner in which she raised concerns, rather than the concerns. They asserted that her communication style was poor, when audit information indicated no such communication problem. It was also despite the fact that Jane Archibald’s record was hitherto unblemished. As the Employment Tribunal noted, although trust managers criticised Archibald’s communication style, they did not actually offer her any help or training with the alleged issue. When her immediate colleagues were hostile or unsupportive, managers suggested that it was her manner of raising concerns that caused problems.
One manager even suggested that the alleged communication problems were due to Jane Archibald’s diagnosis of epilepsy (which had been well controlled):
“135. On 7 June 2019, Fiona Dixon was interviewed in the grievance investigation. The interview included Fiona Dixon saying: “I have no concerns of her clinical knowledge but the impact of not being able to communicate with MDT and patients it then gets fractured, I do feel sorry for her because it is not deliberate, I think it may be linked with her epilepsy but how do you raise that?”
It was a particular disappointment to Jane Archibald that the Tribunal made no finding of discrimination on this point.
There was even a complaint which related to Archibald wearing a cardigan and refusing to take it off because she was cold. Many whistleblowers will relate to this type of ridiculous non-complaint, that arise when employers struggle to find dirt on conscientious, competent employees.
As a well-controlled epilepsy sufferer herself, Archibald’s health began to deteriorate. After eighteen years symptom free, she began experiencing breakthrough symptoms again.
Jane Archibald wrote to the then trust Chief Executive Stephen Eames in August 2019. At that point, Cumbria Partnership was in the process of merging with North Cumbria to create the current North Cumbria Integrated Care NHS Foundation Trust. The merger was completed in October 2019.
In the letter to Eames which I have seen, Archibald very clearly set out the history of her concerns and difficulties at the trust, especially her shock at the trust’s response to the issue of an unqualified healthcare assistant working as a senior specialist nurse.
Archibald reports that she did not even receive the courtesy of a response from Eames. This was cited in Tribunal proceedings and not disputed by the trust.
“147. On 8 August 2019, the claimant wrote to the Chief Executive of the respondent Trust. She wrote that she was writing to highlight concerns which she believed were in the public interest. She wrote about concerns she raised about Samantha Robinson working outside her scope of practice and about lodging other incidents regarding controlled medication, most of which involved Learning Disability Nurses, who she found to be working outside their scope of practice…. The claimant received no response to her letter to the Chief Executive.”
This is not the first time that a concern has arisen regarding Stephen Eames’ interaction with a whistleblower. On this I will provide more at another time.
Stephen Eames
Stephen Eames has held many management posts in the NHS.
This is a most detailed and harrowing account by UNISON of the grievous impact on staffing, beds and services caused by a PFI financial black hole at Mid Yorkshire Hospitals NHS Trust, where Stephen Eames was CEO from 2012 to 2016, and reportedly received a salary of approximately £300K:
Most recently, he has been appointed as Chief Executive of the Integrated Care System in the Humber region.
He was Chief Executive of the Mid Yorkshire Hospitals NHS Trust between 2012 and April 2016 when the trust’s handling of whistleblower cases gave cause for concern.
One of these cases was that of Gillian Wright a manager in the trust Occupational Health Department who raised concerns from 2013-2015 about corrupt practices of nepotism, fraud, breach of the Medicines Act and covert monitoring of her email.
Gillian Wright experienced reprisal after raising concerns and later sued the trust. The Employment Tribunal found that she had been unfairly constructively dismissed and that the trust subjected her to whistleblowing detriment by claiming that she “ might be the problem in her relations with three of her interim managers.”
This obviously has similarities with Jane Archibald’s case.
This is the Employment Tribunal judgment in Gillian Wright’s favour against Mid Yorkshire Hospitals NHS Trust:
I will provide more information about another whistleblowing matter at Mid Yorkshire Hospitals NHS Trust in due course.
Instead, the usual dreadful NHS whistleblower playbook rolled on. Jane Archibald was isolated and vilified. Her grievance about mistreatment was extraordinarily poorly handled and the grievance report joined the chorus about her alleged communication problems, despite Archibald’s previously unblemished record.
Moreover, Jane Archibald was later offered support from a Freedom To Speak Up Guardian who had given evidence against her during the grievance investigation.
The trust’s compromised Freedom To Speak Up process
According to the Employment Tribunal, Linda Turner Quality and Safety Lead gave hearsay evidence against Jane Archibald to the grievance investigation:
“133. Fiona Dixon suggested Martin Daley [the grievance investigator] should speak to Linda Turner. Linda Turner said that she personally had never had an issue with the claimant but a lot of people had told her that they had less than positive experiences of working alongside the claimant. Linda Turner said that a lot of the claimant’s concerns were based on clinical evidence and some of the things she had raised had been brilliant and led to improvements being made. She said the claimant appeared to struggle with email communication and she was aware that other clinicians had been upset by the tone and content of some emails the claimant had sent. She said that the claimant had raised a number of incidents and it was positive that she had picked up on service gaps in development and training. The notes record: “She concluded that Jane has demonstrated some good work and identified issues well but that the main concerns noted come back to communication and people feeling that she doesn’t value them or doesn’t recognize their skills.”
The Tribunal noted that in December 2019 the trust offered Jane Archibald the option of support from Linda Turner in her capacity as Freedom To Speak Up Guardian, but she understandably declined this.
“She was invited to speak to the Freedom to Speak Up Guardian, Linda Turner, but refused to do so.”
The Tribunal concluded that Jackie Molyneux Team Lead for Neurology, who was one of the subjects of the grievance, misled the grievance investigator:
“Martin Daley [the grievance investigator] asked Jacquie Molyneux whether there were copies of the incident forms. Jacquie Molyneux replied “we don’t keep a copy of the incidents”. When asked about this in cross examination, Jacquie Molyneux acknowledged that she could get the incident forms from the computer system. She did not volunteer this information to Martin Daley. No one subsequently corrected the misleading information given by Jacquie Molyneux to Martin Daley, so he did not obtain the relevant incident forms as part of his investigation.”
The trust’s response to Jane Archibald’s grievance about whistleblower reprisal
The grievance investigation into Jane Archibald’s concerns about her experience of whistleblower reprisal was fundamentally flawed because the investigator made no examination of her whistleblowing disclosures, which were mostly in the form of formal incident reports.
There were also other procedural failures in the grievance investigation. The grievance instead focused on her colleagues’ allegations about her manner of communication.
The Employment Tribunal determined that not only was the grievance procedure fundamentally unfair and a whistleblowing detriment, but that the subsequent grievance appeal process was also detrimental:
“The appeal was not a rehearing. We conclude that it was, therefore, tainted by the original flaws in the grievance investigation. We conclude that the claimant was subjected to a detriment by receiving a grievance appeal outcome relying on a flawed grievance process.”
Occupational Health advice to Archibald’s employer was not taken seriously. She went off sick, with stress exacerbating her epilepsy. She eventually resigned, without a job to go to, when it was clear to her that all hope of any fair resolution was gone. The detriment continued when the trust gave her an indefensibly poor reference for a new job with another organisation. This was later criticised by the Tribunal and recognised as a detriment.
Her claims to the Employment Tribunal were partially upheld. Remarkably, the Tribunal accepted that she had suffered whistleblower detriment, a rare finding. It also agreed that she had been unfairly and constructively dismissed.
One of the most egregious aspects of the case is that right up to the end, North Cumbria Integrated Care NHS Foundation Trust refused to accept that Jane Archibald was a whistleblower. Despite her many, serious protected disclosures.
Farcically, the trust argued during Tribunal proceedings that her disclosures were not protected because they were just part of her job:
“219. The respondent also suggested that the claimant was not making protected disclosures because she was raising matters as part of her day to day job.”
The Tribunal gave this short shrift and determined that Jane Archibald had made serious protected disclosures.
“We conclude that it does not matter that it was part of her job to flag up such concerns and complete incident forms where appropriate; the statutory test does not prevent concerns raised as part of a person’s day to day job satisfying the statutory test for protected disclosures.”
“….the incident forms we have seen which all raise legitimate concerns, most of a serious nature.”
Damningly for the trust and reflecting very badly on its persistent denial, the Tribunal accepted all of Archibald’s pleaded disclosures as protected disclosures:
“221. We conclude that all the disclosures relied upon were protected disclosures.”
But the trust has inadvertently impaled itself on a sharpened stake of its own making: it has publicly recognised that Jane Archibald was being a professional and just doing her job in raising concerns.
Small vindication though for all the suffering and lost years.
Regulators and the governance aftermath
Jane Archibald raised concerns with the Care Quality Commission but was told it was an internal matter for the trust.
The correspondence is no longer available as she sent the email from work and she does not have access to it.
The Care Quality Commission and North Cumbria
The Care Quality Commission has a deeply worrying history of helping to minimise patient safety problems at North Cumbria University Hospitals NHS Trust, a predecessor body of North Cumbria Integrated Care NHS Foundation Trust.
A later FOI response from the CQC showed that the CQC reacted reluctantly to numerous North Cumbria whistleblowers’ disclosures, often effectively just putting even the most serious disclosures in a drawer.
Many questions remain from this unedifying tale. The trust can clearly not be trusted to put right the mess of the unqualified healthcare assistant unsafely treating patients for years. Neither can the CQC it seems. Much more rigorous scrutiny is needed. In the first instance, I have asked NHS England/ Improvement to look into the matter and to review Stephen Eames’ role in particular with respect to his current post as Chief Executive of the ICS Humber, Coast and Vale Health and Care Partnership, copied to his Chair Sue Symington.
Elaine Middleton was a senior psychologist. who raised concerns about the trust adopting a cheaper model of staff support for staff coping with traumatic events at work, against NICE guidelines for trauma.
I asked York about its learning from this matter. York Teaching Hospital NHS Foundation Trust CEO’s response of 18 March 2022 was not overly remorseful in tone: “Dear Dr Alexander,
Thank you for your email.
As with any Employment Tribunal outcome we gain learning from the judgement.The learning from the judgement is used to improve our systems and processes. This was the case for the Tribunal you reference below.
The Tribunal clarified for us the need for the Trust to ensure the accuracy of job descriptions and this has now been implemented.
I feel it helpful to clarify that the tribunal confirmed the whistleblowing concern was handled appropriately and there was no connection between that and the dismissal.Kind Regards
Simon Simon Morritt Chief Executive”
I have raised concerns with Sean O’Kelly the new CQC Chief Inspector of Hospitals about the local CQC inspection team’s response to Jane Archibald’s disclosures. I have asked him to ensure that CQC reviews the trust’s compliance with regulations, especially Duty of Candour to all the patients and families affected by the trust’s negligent failure to supervise Samantha Robinson properly.
I have also asked the current trust Chief Executive Lyn Simpson for comments and information. One of the questions I have asked the trust is whether those responsible for supervising and managing Samantha Robinson have been investigated, disciplined or referred to the Nursing and Midwifery Council by the trust. I have also asked the trust for evidence of any trust Safeguarding actions arising from the Samantha Robinson matter. At the time of writing, no comments have been received.
Whilst Jane Archibald was suffering whistleblower reprisal, the National Guardian’s Office was helping to legitimise and publicise the trust’s whistleblowing governance:
This is the trust Freedom To Speak Up Ambassador, who gave hearsay evidence against Jane Archibald, discussing the importance of giving staff confidence to speak up when things go wrong:
By Dr Minh Alexander retired consultant psychiatrist 12 May 2022
Staffsuicidesat ambulance trusts in recent years
It is well known that ambulance services have been troubled organisations with higher levels of staff stress and reported bullying. This is reflected annually in the NHS Staff Survey.
Staff deaths were much publicised at East of England Ambulance Service NHS Trust, where serious leadership failures were also reported.
Media reports about the troubled East of England Ambulance Service NHS Trust
In October 2021 it was reported that an inquest had determined a “self-inflicted” death of David Cullum a paramedic at another trust, West Midlands Ambulance Service NHS Foundation Trust. The coroner considered intent was not clear. Prior to his death David Cullum had a disagreement with a manager:
“We’ve had eight suicides in the past four years. It’s just not sustainable….I’m having phone calls with paramedic friends who are saying, ‘I just want to quit, I just want to quit’….I’m turning up and I’m seeing this many 999 jobs and I know I’m going to have to do everything, I’m driving a four and a half tonne vehicle all night, I’m having to do everything and I can’t carry on. We’re not wimps as paramedics, we get on with it….The thing that annoys me is that the Service always has a get out clause, that ‘it’s the demand’ that’s to blame...…”I cannot and my colleagues cannot continue to work 15 to 17 hour shifts…
….But they couldn’t give two tosses about the staff that are run into the ground.
…I am very concerned that so many friends and colleagues are leaving the system because there’s so much pressure on them.… Lower management knows how bad things are. But the higher management… all they are doing is working the rota harder and that is killing us all.”
In particular, the whistleblower was concerned about downgrading of skill mix:
“The ACAs [Ambulance Care Assistants] are coming out with us in an ambulance uniform, but they can’t drive an ambulance on blue lights or normal conditions…The paramedic has to drive there, do all the care, all the paperwork. We can’t drive the person to hospital because if the patient needs paramedic intervention, the person we’re working with (ACA) can’t provide it….If the patient needs to be taken to hospital, the paramedic cannot do anything apart from request another crew – so literally they’re sending ambulances to people for nothing.”
Contrasting with this picture of life on the frontline, with diluted skill mix, is the trust board’s plan to build new headquarters.
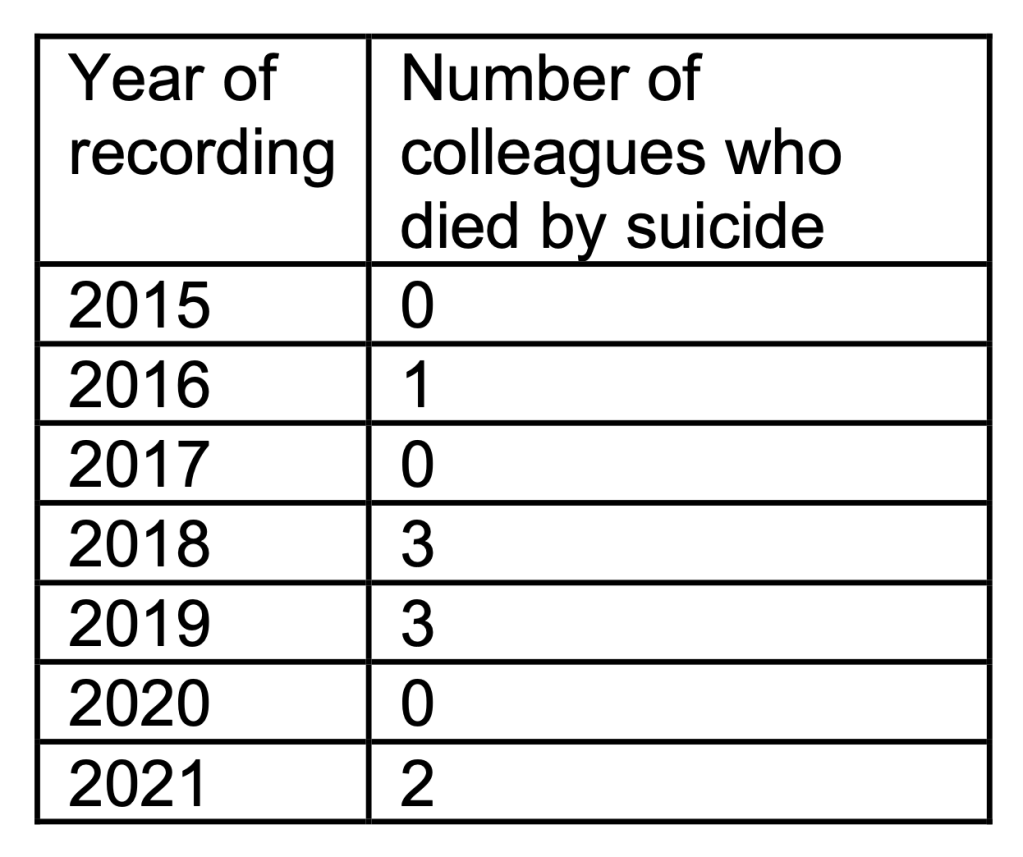
I asked the trust about the eight suicides reported by the whistleblower and related matters. This is the full FOI response by the Trust:
“Late shift finishing, reduced training opportunities through reduced patient contacts, concern about safety for deteriorating patients, moral hazard from dealing with deteriorating patients on the phone, as well as violence and aggression being experienced by crews when they attend patients who have been waiting sometimes for hours on end.”
The trust does give a lengthy description of its approach to staff mental health.
I asked for reports and equivalent documentation showing learning and action arising from deaths. The trust stated there had been much learning, but it disclosed no documents. The trust stated:
“Much learning has been taken from the deaths of our colleagues, mental health awareness training and additional support services have been embedded directly as a result.”
West Midlands Ambulance Service NHS Foundation Trust and the Care Quality Commission
The CQC has rated the trust as “Outstanding” since 2017.
Safeguarding referrals were sent but not followed up by the organisation. When hundreds of emails failed to “send” due to an IT glitch, the referrals were never made, with referrers unaware of this.
After the failures became evident, CQC changed tack and advised that systems changes were needed: “The service should consider how to alert staff that safeguarding reports to the central contact point have been actioned.”
Should CQC’s effusive claims about the trust’s leadership and support for its staff now be in doubt too?
I found no reference to staff suicides in CQC’s last report of 2019. Instead, CQC emphasised the quality of staff support:
“Staff had access to support for their own physical and emotional health needs. The trust positively promoted the well- being of staff. The trust valued the well-being of its staff. There was wide range of well-being options and resources available”
CQC was effusive about trust leadership in general and the trust CEO in particular:
“There was strong, clear leadership in place, led by a chief executive who wasregarded as inspirational by every staff member and service trust wide.”
Did the CQC inspection team in question, led by Victoria Watkins, CQC Head of Hospitals Inspection, speak to every member of staff at this trust in order to justify making this expansive claim?
Certainly, the staff who sued the trust in the Employment Tribunal in recent years did not seem to feel inspired:
CQC also claimed: “Every level of the trust had sustained a highly positive culture that supported and valued staff, creating a sense of common purpose based on shared values. Staff felt supported, respected and valued and were exceptionally proud to work for and represent the trust.”
Somewhat dispelling this rose-tinted view, an FOI request previously showed that the trust failed to keep records of a meeting held by the trust CEO with whistleblowers about racism, because the meeting was not considered “formal”:
Is West Midlands Ambulance NHS Foundation Trust a specially protected organisation?
Is the National Freedom To Speak Up Guardian taking effective action to support ambulance staff?
An earlier FOI to the National Guardian’s Office (NGO) revealed that the Office had been discussing a thematic review of Speaking Up in ambulance trusts since June 2020 – around the time that public concern about East of England intensified – but had not actually done much to progress the project.
Thematic reviews often hide a multitude of sins, may diffuse accountability and shield individuals.
Notwithstanding, a request to the NGO for documents relating to the planned thematic case review was met with a blanket refusal under Section 22 FOIA (material intended for future publication), when not all the material requested was intended for publication.
In its FOI response of on 6 April 2022. The National Guardian’s Office asserted that it would be publishing information about its proposed review “in the near future”.
I enquired a month later on 4 May about timescales for publication of the withheld information about the review and timescales for the review itself.
On 10 May the National Guardian’s Office replied off the point as follows:
“In your email of 3rd May, you asked for any update on our Speaking Up review on Ambulance Trusts. We are working on the co-design of this review with the Ambulance Trusts and will deliver updates on this piece of work in due course.”
I have repeated the request for clarification of timescales for publication of information and for conducting the review and have forwarded the FOI response from WMAS confirming staff suicides to the National Guardian.
The correspondence follows below:
BY EMAIL
Dr Jayne Chidgey-Clark
National Freedom To Speak Up Guardian
11 May 2022
Dear Dr Chidgey-Clark,
Information about and progression of your planned thematic case review of Speaking Up in Ambulance Service NHS trusts
I asked you on 10 March 2022 for information on this planned review and for clarification and assurance that the relevant whistleblowers would be invited to participate, whether currently or formerly employed by ambulance trusts.
On 6 April your Office refused my request for relevant documents and declined to answer my questions about how the review would be conducted, citing exemption Section 22 FOIA (material intended for future publication). Your Office asserted that the withheld information was scheduled for publication in the “near future”.
When I asked on 4 April if there was an identified timescale yet for publication of the withheld information, and a timescale for the review itself, your Office simply stated in reply yesterday (see below):
“We are working on the co-design of this review with the Ambulance Trusts and will deliver updates on this piece of work in due course.”
I wonder if it is possible to have timescales as requested, even if they are only rough and provisional.
Also, I am a little concerned that you are co-designing with employers but do not appear to be including relevant whistleblowers at this stage. Could they be included if they wished to be?
Underlining the necessity to progress the review, please find an FOI response from West Midlands Ambulance Service NHS Trust at this link:
This very sadly confirms that there have also been nine staff suicides at this trust, including two deaths last year, in addition to those more widely reported at the East of England Ambulance Service NHS Trust.
This has been accompanied by WMAS staff whistleblowing to the media.
Although I asked the trust to disclose documents showing evidence of learning and action arising from any staff deaths, none were disclosed.
Yours sincerely,
Dr Minh Alexander
Condolences
My condolences to families, loved ones and colleagues affected by the above tragic losses of ambulance staff.
In a broken system for whistleblowing, with unreliable regulators, I would advise whistleblowers to consider going directly to the press as a means of protecting themselves and the public. It can be empowering if done carefully and responsibly, choosing your media outlet wisely to protect your confidentiality and identity, and the accuracy of reporting. Each case needs to be weighed on its own merits. A record of going directly to the press may count against you in any subsequent employment dispute, because there are legal tests for going to the press under employment law. It is accepted under the rules in some circumstances. But equally, an untraceable disclosure to the press can reduce the risk of reprisal and an employment dispute, and reduce delay in bringing very serious risks to attention. It is very important that accuracy is maintained in order to preserve confidence, credibility and fairness. A drawback of anonymous whistleblowing is that you may not be able to disclose all relevant details. Seek the best advice you can before deciding what to do.
PETITION
Please click and add your signature to this petition to reform UK whistleblowing law – whistleblowers protect us all but weak UK law leaves them wholly exposed, lets abusers off the hook and it is a threat to public safety.
Late on 21 May 2022 the Sunday Times published an investigation on management cover ups of care failings in patient deaths at North East Ambulance Service NHS Trust, which has resulted in staff whistleblowing. Some of the details of this affair are provided in this blog, which examines how the matter has been hijacked to augment Jeremy Hunt’s political fortunes, coinciding with the re-launch of his Tory leadership bid.
By Dr Minh Alexander retired consultant psychiatrist 9 May 2022
My apologies for this late posting of FOI material from March 2021. It came through at a time last year when I took a break from campaigning work due to personal commitments.
East London NHS Foundation Trust, a recent darling of regulators and the trade press, was embarrassed after the export of its executive paratroopers into stricken Norfolk and Suffolk NHS Foundation Trust came to a sticky end.
Marie Gabriel the ELFT Chair led the way as NSFT Chair, and following her, Mason Fitzgerald ELFT Deputy CEO was due to be crowned as NSFT CEO. But he fell at the last furlong when he was discovered to have faked a qualification on his CV. He withdrew his NSFT application and was eventually dismissed by ELFT.
Mason Fitzgerald and the Good Governance Institute
Astonishingly, despite the scandal, Fitzgerald was hired by of all people, the Good Governance Institute.
A month ago, I asked the Institute to comment but it has not done so.
Caveat emptor.
But the business once more raised questions about the NHS’ due diligence when appointing senior managers. Both ELFT and the CQC were in the frame – ELFT for its recruitment practices in not checking primary qualifications, and CQC for failures to do the same under Regulation 5 Fit and Proper Persons.
I therefore asked CQC for information on its processes, guidance to inspectors and quality assurance of its regulation of FPPR.
This was the CQC FOI response, along with disclosed guidance to inspectors and a single FPPR audit from November 2016 entitled “Quality Sampling Report, Fit and Proper Persons Requirement”:
The disclosed guidance to CQC inspectors describes a largely tick box, administrative exercise but it does include ensuring that qualifications are checked.
CQC ducked a question that I asked on the minimum number of directors’ files that are checked during inspections, giving only this answer:
“Our assessment of trust-wide leadership, governance, management and culture will be the starting point for the trust-level rating for well-led. We also consider improvements and changes since the last inspection. A small team of inspectors and specialist advisors with appropriate experience will look at a range of evidence applicable at the overall trust board level. This includes interviews with board members and senior staff, focus groups, analysis of data, strategic and trust-level policy documents, and information from external partners. The scope and depth of our assessment of the well-led question varies for each provider. Our approach depends on factors such as the size of the trust, the findings of previous inspections, and information gathered from the provider, external partners and other sources on performance and risks in the trust across our five key questions”
The November 2016 audit of CQC’s regulation of FPPR shows that there was much confusion and a dog’s dinner of how different CQC staff approached the task. This was two years into the Regulation taking effect.
The paper, unsigned, was critical of CQC’s then guidance for inspection staff:
“There is also a lack of clarity about what is considered to be serious mismanagement, what to do if a breach of regulation 5 is determined and how the information and any proposed action should be escalated.”
“Although staff have received some training in FPPR there remains a lack of confidence and awareness about regulation 5, what type of evidence indicates a potential breach and what to do if a breach is found.”
The report notes:
“Our current management information on FPPR cases and records of action taken in relation to FPPR is not complete or correct. There are a lack of processes to follow when FPPR information is received by CQC The way we record and manage information relating to FPPR is inconsistent and as a result we are unable to track referrals or provide an audit trail of decision making and action taken .”
“There is a lack of clarity on how we will gain assurance of FPPR from some organisations.”
Private providers may have had an easy ride:
“Inspectors are unsure when FPPR is applicable to some corporate providers…In NHS inspections FPPR is proactively inspected….Across all other providers FPPR is only addressed reactively when specific issues arise.”
The report recommended more training for inspection staff, better guidance and processes and ongoing audit.
In its response to my FOI request CQC did not disclose any other audits of its handling of FPPR other than the audit undertaken in 2016. Therefore, CQC has failed to implement the 2016 recommendation on completing the audit cycle with re-audit. A fundamental failure.
In its FOI response letter, CQC also admits:
“No central data is held on how well CQC inspectors check provider compliance with CQC Regulation 5 Fit and Proper Persons.”
which underlines the complacency and lack of ongoing audit.
But an important admission is contained in the 2016 document:
“It is not the responsibility of CQC to ensure fitness although we can take action against the provider if we believe an unfit person to be in a directorship position.”
This is what Mike Richards the then CQC Chief Inspector of Hospitals said to whistleblowers at a telephone meeting in 2014.
It is a question of whether CQC has the will to do so.
There is not much evidence of that to date.
It is also important to note that CQC’s FOI response letter is also liberally peppered with phrases such as:
“robust process”
“proper processes”
“thorough processes”
when referring to its judgments of providers’ processes for assuring directors’ fitness.
This is important because CQC recently tried to claim that it has no role in determining how providers should assure directors’ fitness. More on that another time.
CQC clearly does have responsibility to ensure that providers’ FPPR processes are fit for purpose.
If the CQC waves any silly FPPR excuses at you to justify inaction, wave these papers back.
RELATED ITEMS
Dr Jasna Macanovic’s recent NHS whistleblowing case adds to the pile of managerial recycling scandals. John Knighton the medical director found by the ET to be centrally involved in her premeditated unfair dismissal has been protected by the trust and Mark Cubbon the trust CEO who failed to ensure her protection as a whistleblower has been promoted to a senior post at NHS England.
By Dr Minh Alexander retired consultant psychiatrist 7 May 2022
On 28 January 2014 an Employment Tribunal ruled that South Devon Healthcare NHS Foundation Trust had harmed two whistleblowers, Penny Gates and Clare Sardari, who had raised concerns about nepotism by the trust’s then CEO, the infamous Paula Vasco-Knight.
The Employment Tribunal concluded that Vasco-Knight had breached the NHS managers’ code of conduct.
The regulator Monitor later helped to recycle Vasco-Knight as an NHS director to a locum post at St Georges.
The Care Quality Commission was asked to review Vasco-Knight’s fitness under CQC Regulation 5 Fit and Proper Persons (FPPR). It did so cursorily and Mike Richards the then Chief Inspector of Hospitals personally shut down the FPPR:
The CQC’s actions allowed Vasco-Knight’s promotion to the post of interim CEO at St. Georges, completing her rehabilitation despite the whistleblower reprisal and nepotism.
The CQC was severely embarrassed when shortly after this, Vasco-Knight was charged with and eventually convicted of a criminal fraud against the NHS from her tenure as CEO at South Devon.
The CQC never took any responsibility for this FPPR botch, despite a subsequent PHSO finding against it in this matter. It issued a non-apology to Clare Sardari but then undermined even this with its further public statements excusing itself:
NHS England and NHS Improvement who had also been complicit in building up the Vasco-Knight brand also evaded taking proper responsibility for their part in these matters.
Vasco-Knight was not the only director of South Devon Healthcare NHS Foundation who was criticised by the Employment Tribunal that found whistleblower reprisal.
The trust chair Peter Hildrew was criticised for an extraordinary cover up of Vasco-Knight’s misconduct.
The trust Human Resources Director Adrienne Murphy was also found guilty of whistleblower reprisal, for trying to dissuade Gates and Sardari from pursuing their concerns and making them feel intimidated. Not only did Murphy make the whistleblowers feel intimidated, but according to the ET, Murphy tried to convince the trust Chair not to investigate the whistleblowers’ concerns about her behaviour and that of Paula Vasco-Knight. The ET also determined that the trust’s procedural response to the whistleblowers had been unfair. The HR director’s role in this must be in question.
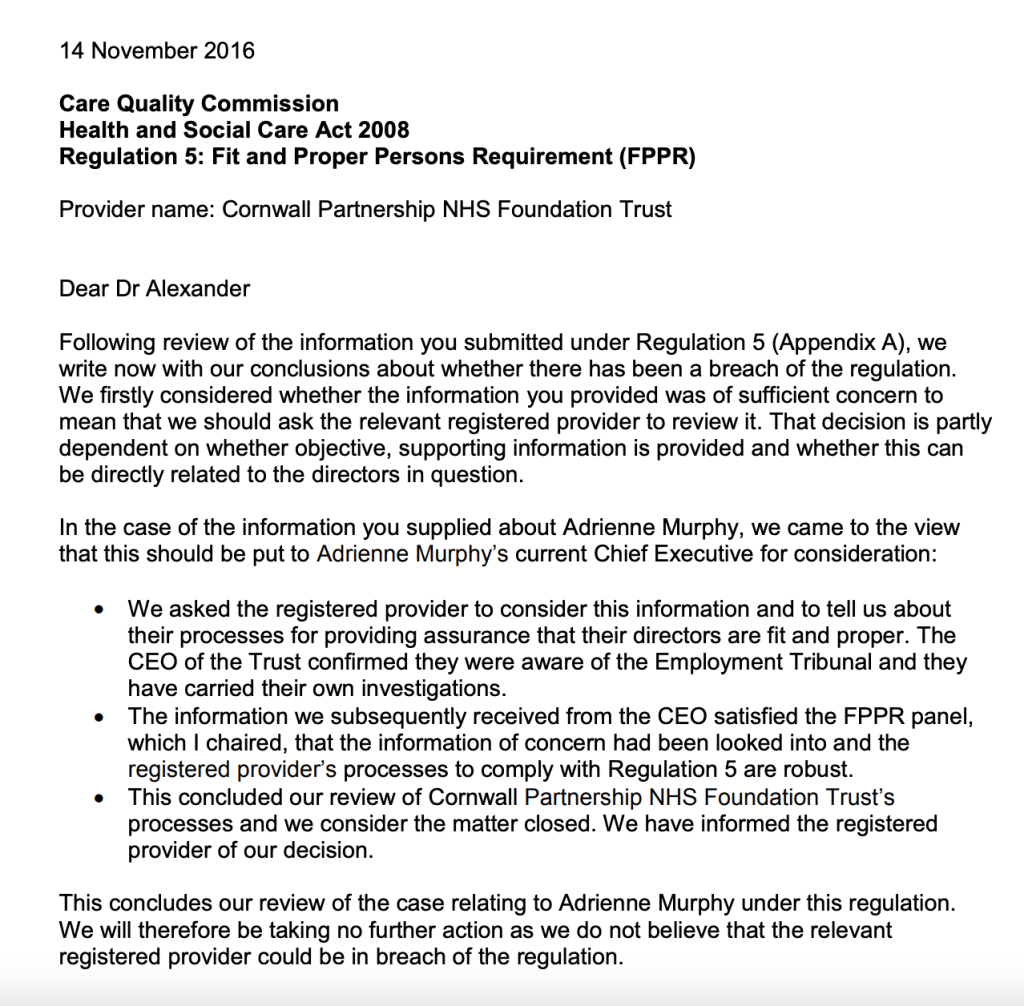
Parallel to the FPPR process on Vasco-Knight, another FPPR referral was made to the CQC on Adrienne Murphy. She had been given a job as HR director by the mental health trust Cornwall Partnership NHS Foundation Trust, despite (or perhaps it was even because of?) the history of ET proven whistleblower reprisal.
Biog taken from Cornwall Partnership NHS Foundation Trust website
The usual CQC prestidigitation resulted in a declaration in November 2016 that all was well and that the trust was compliant with FPPR.
Fast forward to 2021 and a significant scandal emerged of four trust directors at Cornwall Partnership NHS Foundation Trust being overpaid, reports of an ongoing NHS Counterfraud investigation and resignation of long served trust CEO Phil Confue.
According to Companies House, Phil Confue was a director of a company, with the former medical director of Cornwall Partnership NHS Foundation Trust 2000-2019, who is now the Chief Clinical Information Officer of the trust:
Companies House records indicate that Confue resigned his directorship of this company on 22 June 2021.
The former medical director of Cornwall Partnership NHS Foundation Trust 2000-2019
There is woefully little information about the executive overpayments in the public domain. We know that the four directors had to repay the monies, but despite their seniority and the legitimate public interest, we do not know with any certainty who they are.
Normally such arrangements are made with advice from the most senior Human Resource officer. What senior HR advice, if any, contributed to this ill-advised overpayment?
I asked the trust for more information about investigations in recent years and about the executive overpayments.
The trust indicated that there had been a flurry of activity:
“There have been eleven external reviews/ investigations commissioned by the trust in the last three years.”
“The issues covered relate to the following areas:
Governance
Trust culture
Human resources matters
Matters raised through Freedom to Speak Up”
“Four are in progress and seven have been completed. Information relating to the findings of the cultural review, carried out as part of the trust’s undertakings, have been shared in a number of forums, internally and externally and with staff.
Of the reviews/investigations that have been completed, none have been published. The nature of reviews/investigations are such that details would not be appropriate for publication, even in a heavily redacted form, and would be covered by several exemptions to the right of access under the Freedom of Information Act 2000.”
This is unwarranted secrecy by the trust, especially as the broad outcome of one of these reviews is in the public domain. The March 2022 trust board papers revealed an audit of trust complaints was undertaken by Audit South West. The audit found gross failings in trust governance underlying a huge backlog, such as lack of staff training to handle complaints, lack of complaints tracking, lack of proper investigation and breaches of regulations. The matter was reported in the Health Service Journal recently:
Moreover, minutes of a trust board meeting in December 2021 refer to actions arising from the cultural review mentioned in the trust’s FOI response, albeit I could not find the report itself amongst published trust papers:
“HR, workforce, and organisational development
Adrienne Murphy said that there was a backlog in the agenda for change job matching process and this was being prioritised. The winter offer for staff health and wellbeing was being revisited and the HR team was meeting with the leadership academy to take on the actions from the cultural review. It was also noted that a business case was being written for substantive resources to be allocated to inclusion and diversity work”
Regarding the executive overpayments, the trust made these comments in its FOI response:
“A single flat rate of payment was made to four members of the board.”
“All four payments have been repaid.”
“This information is exempt from release by virtue of Section 40 (2) of the Freedom of Information Act 2000.”
So it seems implicitly from all the above that Human Resources, including whistleblowing governance, is not a roaring success at the trust.
Who could have predicted that? Not the CQC anyway.
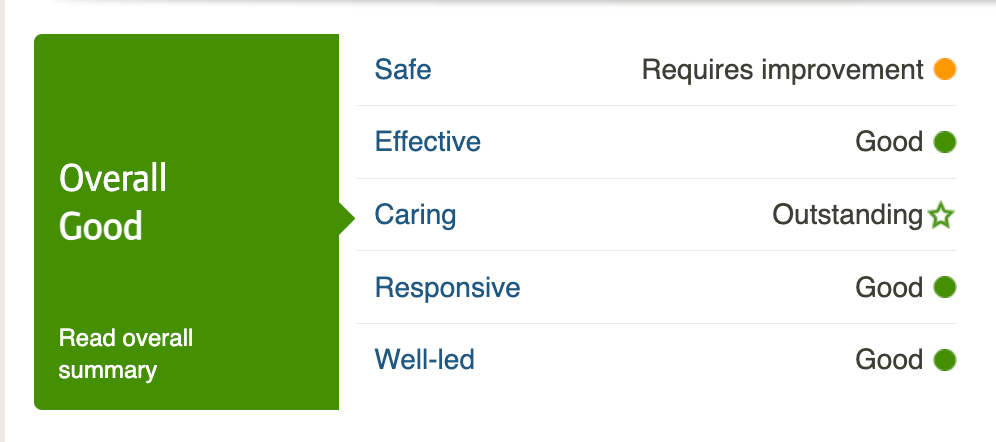
CQC made many nice comments about the trust board, such as:
“The culture of the trust had improved with high morale in the majority of services. Staff felt respected, supported and valued by their managers and the trust.”
“The board and senior leadership team had set a clear vision and values that were at the heart of all the work within the organisation.”
The effusive CQC inspection report authors were:
“Karen Bennett-Wilson chaired this inspection and Gary Risdale led it. An executive reviewer, Jan Bergman, supported our inspection of well-led for the trust overall.”
Jan Bergman was formerly an NHS trust CEO and has also worked as Director of Transformation and Deputy CEO at the Rotherham NHS Foundation Trust.
As a local Tory councillor for Weymouth Bergman’s current declaration of interests states that he is a “Transformation Consultant, NHS (3days/week)” as well as a CQC specialist adviser.
Despite the trust’s flashing neon “Keep Out” signs, I will ask Cornwall Partnership for more information about the extraordinary number of external reviews and investigations of the trust’s governance in the last three years, and the process by which the four directors came to be over paid. I will also challenge the decision to withhold their names on the basis of their seniority and the very legitimate public interest in the governance of an organisation responsible for so many vulnerable patients.
PETITION
Please click and add your signature to this petition to reform UK whistleblowing law – whistleblowers protect us all but weak UK law leaves them wholly exposed, lets abusers off the hook and it is a threat to public safety.
Dr Jasna Macanovic’s recent NHS whistleblowing case adds to the pile of managerial recycling scandals. John Knighton the medical director found by the ET to be centrally involved in her premeditated unfair dismissal has been protected by the trust and Mark Cubbon the trust CEO who failed to ensure her protection as a whistleblower has been promoted to a senior post at NHS England.
By Dr Minh Alexander retired consultant psychiatrist 2 May 2022
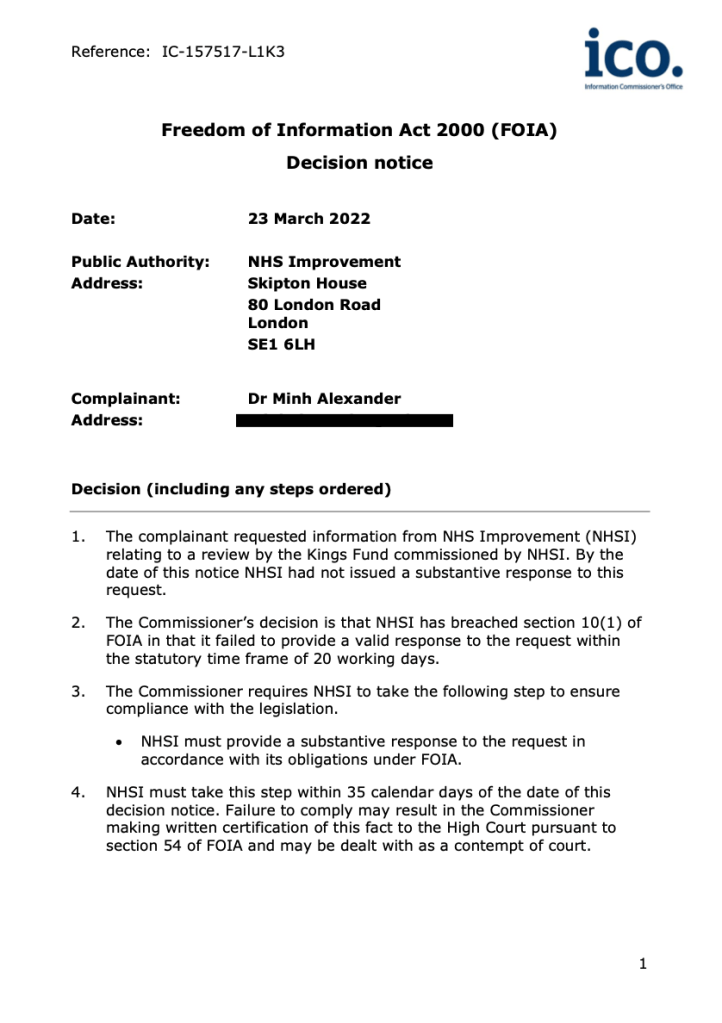
Summary: NHS England/ Improvement has reluctantly disclosed a copy of the secretly commissioned King’s Fund review report on poor culture at the Healthcare Safety Investigation Branch, under threat of possible certification to the High Court by the Information Commissioner. The King’s Fund report is a poor affair with little real factual content, and fails to deliver much transparency and accountability. It may be that is what was ordered. Related disclosed correspondence and terms of reference show that the review was never intended to look for hard evidence and it was expressly instructed to avoid specific issues of compliance against standards and policies, performance and culpability. The report’s authors’ identities have been withheld. But the report does nevertheless paint a picture of poor culture in broad strokes. The poor culture and the secrecy pervading the review process are particularly unacceptable given HSIB’s role as a safety agency. Importantly, the Department of Health and Social Care was involved throughout. It remains to be seen whether the DHSC’s related decision to strip HSIB of maternity investigations and set up a Special Health Authority under direct government control will serve patients well, or is just a pretext for controlling the maternity liability bill.
Background
The creation of the Healthcare Safety Investigation Branch was part of Jeremy Hunt’s patient safety theatrics, whilst defunding the NHS and refusing to implement core recommendations from the MidStaffs public inquiry such as safe staffing. He sold HSIB as a safety culture panacea that was based on aviation safety models. This rested on claims that everything was wonderful in aviation and at the Air Accident Investigation Branch from whence HSIB’s chief investigator came. The truth is things may not have been all peaches at AAIB. Indeed, the Department of Transport have fought tooth and nail to avoid releasing AAIB staff survey results that I first requested in 2018 and it is still a matter of litigation with the ICO opposing the government. Moreover, there are questions about aviation safety culture arising from matters such as the Boeing regulatory capture scandal and problems at the Civil Aviation Authority:
HSIB was established with heavy input from a clique of Hunt’s anointed associates. As a political instrument, it was initially protected, and was located as a sub-committee of NHS Improvement.
Shortly after the small agency was created, Hunt roped HSIB into his maternity crusader narrative. HSIB was tasked with a national maternity investigation programme which far outstripped its original capacity. Rapid expansion was required and HSIB ended up with satellite regional maternity investigation teams linked to local NHS trusts. The maternity investigation programme grew like Topsy and about a thousand cases were processed annually.
This exposed a large volume of care failings and helped victims establish liability. It had substantial financial implications nationally because liability for maternity cases is high. Injured babies and their families must be compensated for a life time of disability and care.
To complicate matters, HSIB was also supposed to be transitioning to independence, subject to the passage of the Health and Social Care Bill. The legislation passed on 28 April 2022 and HSIB is now expected to become an independent non departmental DHSC body within a year.
HSIB whistleblowers started emerging from at least June 2019:
Fast forward to January 2022. The press reported a scandal about very poor leadership at HSIB and the findings of a related King’s Fund review that had been quietly commissioned by NHSE/I and which had not been published. The headlines were lurid – “Rasputin-like characters”.
The secrecy was a concern.
Also of note, shortly after the leaks to the press, the Department of Health announced that it would strip HSIB of its maternity investigation programme. In its stead, the government would create a Special Health Authority under direct DHSC control, for only up to 5 years, to take over maternity investigations.
The purported reason for the time limit being that it expected that NHS trusts would become good enough at investigations to take back control within that time. Sigh.
FOI disclosure about the King’s Fund review
I asked NHSE/I, under FOIA, about the context in which the King’s Fund review was commissioned and for a copy of the report itself.
NHSE/I mostly ignored me, requiring two formal ICO interventions and deadlines of 10 and then 35 days, with a threat of possible certification by ICO to the High Court about non-compliance and contempt of court.
This was despite Andrew Morris NHSI Chair assuring me twice that he would liaise with the NHSE/I FOI department. On the very last day of the 35 day tranche, after I wrote and tweeted to Amanda Pritchard NHSE/I CEO, the regulator finally responded.
This is NHSE/I’s formal FOI response letter, and disclosed correspondence between NHSE/I and the King’s Fund and the review terms of reference:
In the disclosure there was correspondence exchanged between NHSE/I and the King’s Fund about prices and services as early as March 2021, and a proposal for the review by the King’s Fund dated April 2021 was included.
NHSE/I indicated that the review was commissioned in May 2021. The actual correspondence commissioning the review was not supplied, but NHSE/I informed me that Aidan Fowler, National Medical Director for Patient Safety commissioned the review in response to HSIB staff whistleblowing to the NHSE/I Freedom To Speak Up Guardian. Upon checking, it became apparent that Aidan Fowler has been both a senior manager at NHS Improvement AND Deputy Chief Medical Officer at the Department of Health and Social Care since 2018.
Bizarrely, the five authors’ identities were redacted. They were described as exceptionally senior for the purposes of the King’s Fund’s sales pitch to NHSE/I, but they were purportedly not considered senior enough for the purposes of overriding section 40 FOIA (personal data). Hey ho.
This is an excerpt from the KIng’s Fund’s proposal to NHSE/I for conducting the review of HSIB’s culture
I do wonder which senior NHS managers or former senior managers NHSE/I was so reluctant to name. Not perchance any miscreants trailing a history of scandal or any with conflicts of interest?
Of interest, the King’s Fund report revealed that this was not the first review on HSIB. It showed that HSIB staff complained that previous reviews had been carried out but were perceived to have been spiked and swept under the carpet. I have asked NHSE/I for more information about these other reviews.
The correspondence from the King’s Fund is rather ingratiating in tone, emphasising the commercial nature of the relationship with NHSE/I.
The April 2021 King’s Fund proposal for the review includes the agreed narrow terms of reference focused on soft perceived culture, with prohibitions to stay away from hard examination of compliance with policies, performance or conduct and culpability of any individuals.
For example:
“(c) Assess whether people wanting to raise a concern were aware of or had
access to appropriate policies and support identifying any actual or perceived barriers to reporting, making complaints, FTSU or other mechanisms of raising concern – although the quality of the policies and their application is outside of the scope of this review.”
“(c) The Review will not make any findings nor make any comment on the conduct, performance or competence of any individual who has raised a concern or is the subject of a concern”
There was a keenness to shut down specific cases examples, old or new:
“(b) The Review will not reopen individual cases, concerns or investigate new reports or complaints against specific individuals. Those wishing to raise or discuss any new concerns will be advised of the pathways for the resolution of such concerns.”
Additionally, the King’s Fund team were steered by a reference group composed of NHSE/I, including Aidan Fowler, and someone else from the DHSC. Steered to what end?
A draft version of the King’s Fund report was shared with NHSE/I. An email and attached comments by Aidan Fowler on this draft report were redacted and omitted from the disclosure bundle by NHSE/I under FOIA Section 36 exemption. That is on grounds that it might prejudice the effective conduct of public affairs. Or in plain English, embarrass important people.
One can only speculate on what was said that made it necessary to withhold this information.
Mr Aidan Fowler
This is Mr Fowler’s interesting CV according to his LinkedIn entry, a UCL graduate then surgeon at a DGH for ten years, followed by a rise through the management ranks via the NHS Fast Track Executive Development Programme:
The final King’s Fund report of the review dated January 2022 is an opaque piece of work with the flowery, imprecise language of appreciative inquiry technique.
Appreciative inquiry
is a cuddly technique of quality improvement based on inspiration, positivity, being your best you and all that. It is used by NHS organisations and a document posted by NHS England illustrates some of the nature of this technique:
“The Power of the Positive Image:
Dreaming
o Working in groups. Remember back to the best experiences you described earlier today.
o Its 2021 ask each other ’How’s it going? What are you doing these days?’ Be interested and co-create the story
o Create something using the materials here that expresses your positive images of the future in some way”
There is a veneer of superficial empathy by the King’s Fund team.
But their report actually contains very few facts and so fails to respect the subject matter and the people concerned.
As perhaps reflected in the way that aggrieved HSIB staff continued to whistleblow to the press after the review concluded, to expose specific examples of what happened to them. Secrecy is not conducive to justice and accountability, and the leaks were perhaps an inevitable consequence of NHSE/I’s handling of the matter.
Even survey results collected as part of the King’s Fund review were not factually reported. There was no excuse for this, because: the data was aggregated and anonymised. The results should have been clearly provided. But the King’s Fund only gave details in the appendix about response rate: “Concurrently, an anonymous staff survey was run. This was compiled of quantitative and free text questions. The response rate was 172 people, 68.5 per cent of the organisation population.”, but no specific survey results.
The technique of hiding facts and data from reports, to avoid embarrassment
An astonishing example of this was revealed when correspondence between senior managers at the Care Quality Commission surfaced.
It showed them plotting to make a CQC inspection report on Basildon hospital services appear tough, but to strip it of any real data:
“Being hard hitting without presenting critical data will I suspect be more politically acceptable than criticising with evidence”
Several months of work by the King’s Fund team of five were summed up in these meagre core findings:
HSIB has a very committed and skilled staff team who do great and important work.
The organisation exists in a very uncertain current and future context, with confusing accountability and the added complexity of being subject to legislation currently going through Parliament.
Unclear governance and accountability are compounded by confusion about organisational policies and processes not being followed, while HR support has been lacking.
We heard mixed views about leadership and culture in different teams. Many staff report poor behaviours from the executive team, individually and collectively, and the team’s leadership is regarded by many as poor.
This manifests itself through a perceived command-and-control approach to leadership, lack of openness to challenge, hierarchical approaches to management and behaviour that is out of step with the organisation’s values.
Bullying, sexism, racism and other forms of discrimination and unprofessional behaviours appear to be prevalent and tolerated – this goes right to the top of the organisation.
The national and maternity teams retain different identities and ways of working, with widespread perceptions of unfair treatment and favouritism.
All of this is very damaging to the health and wellbeing of staff, diminishes the culture and undermines the potential of the organisation.
There is a breakdown in trust and lack of confidence that these issues will be addressed by the executive team.
These findings were shared with HSIB staff in November 2021, after which HSIB’s Chief Investigator announced his retirement.
The King’s Fund report stated that not all staff perceived problems, and some were surprised to hear of them. Some thought the executive team had been unfairly blamed.
In maternity investigation teams, some managers were reportedly seen positively, but there was serious concern about others:
“There was a very strong voice from staff regarding senior maternity investigation team leaders not being held accountable for behaviours that had a very negative impact on staff.”
Irritatingly, there is no quantification of those who had concerns and those who did not, and so there is no solid factual basis on which to understand the scale of the reported problems.
HSIB staff asked for acknowledgment from the leadership of its failures, for better culture, for close supervision of HSIB by NHSE/I and DHSC and for a clear transition plan to HSIB independence.
The King’s Fund made recommendations in terms of external organisational development and HR support.
Of relevance in the disclosed correspondence, NHSE/I had noted eight months previously in correspondence of 25 March 2021 that HSIB wanted Mersey Care NHS Foundation Trust to fulfil this role, so it seems the King’s Fund plan for external support was in reality a foregone NHSE/I conclusion:
“Aidan has just flagging with me that HSIB may want to use MerseyCare NHS Trust to do the actual support/improvement element.”
There is a hint that whistleblowing arrangements were not fully satisfactory at NHSE/I as there is a recommendation to improve them. Could this relate to any failure to act sufficiently to earlier episodes of whistleblowing about HSIB?
NHSE/I have tried to draw a veil over the exact number of whistleblowing disclosures that were made, claiming small numbers and privacy arguments for not telling me more. I have asked them about the numerical threshold that they have applied.
The King’s Fund was emphatic on discrimination:
“This must be supported by some immediate actions on equality, diversity, and inclusion in the first six months of 2022.”
“Direct and urgent action must be taken in response to the racism, sexism and discrimination experienced by people in HSIB. This work must be a priority for the executive team and senior leadership of HSIB. NHS England and NHS Improvement as the employing organisation has a responsibility to support this, while the Department of Health and Social Care should be responsible for overseeing progress against this recommendation.”
The King’s Fund claimed that the issues of racism and sexism were particularly severe:
“We heard some acknowledgement and sadness regarding racism and sexism in people’s response to the findings. These are not issues that are unique to HSIB and are found in many organisations. However, the level to which they were prevalent in HSIB means inclusion needs to be at the centre of organisational development work going forward”
It is a great pity there was no specific evidence provided to demonstrate how the King’s Fund arrived at this conclusion, which had such toxic implications for HSIB’s leaders.
Despite the reluctance to report facts, there seemed to be some overreaching of competence and remit when the King’s Fund diagnosed that some HSIB staff had “trauma”, which would need workplace supplied counselling:
And finally, this being a King’s Fund paper, there was the typical exhortation:
“A sense of common purpose and drive to improve health care bound many in the organisation together. These are strengths to build on.”
All told, the King’s Fund report seems unsatisfactory in its vagueness and low information content, for what was doubtless a steep fee. (In the disclosed correspondence, NHSE/I asked if it would cost above or below £25K.)
On top of this is the hypocrisy of NHSE/I judging HSIB for poor culture when it harbours failed NHS managers, and the hypocrisy of NHSE/I and the King’s Fund not publishing their own staff survey results. Some of this was covered in this recent blog:
We know there were clearly problems at HSIB, but there are insufficient facts for real accountability and transparency. This seems unfair to both victims and accused.
And we do not know if the HSIB situation has been exploited by the DHSC.
But it is clearly unacceptable to have such poor culture at a safety agency.
We have yet to see if the DHSC’s excision of the maternity programme from HSIB will serve patients well – or if the proposed Special Health Authority will be operated as a gatekeeper to control maternity liability. The Secretary of State’s current behaviour towards bereaved families at Nottingham raises additional concerns about his intentions:
In the meantime, I have sent the King’s Fund report to the Department for Transport Permanent Secretary in case the Department may wish to review its systems for detecting failures of culture, or to comment on the reference that it likely provided for the HSIB Chief Investigator. I have yet to receive any comments.
UPDATE 31 MAY 2022
I asked NHSE/I for the earlier reviews on HSIB that were cited by the King’s Fund report of culture and leadership at HSIB. NHSE/I have disclosed a single, partially redacted 2020 report about failings in maternity investigations and cultural issues of bullying, target driven/ production line approach to reports:
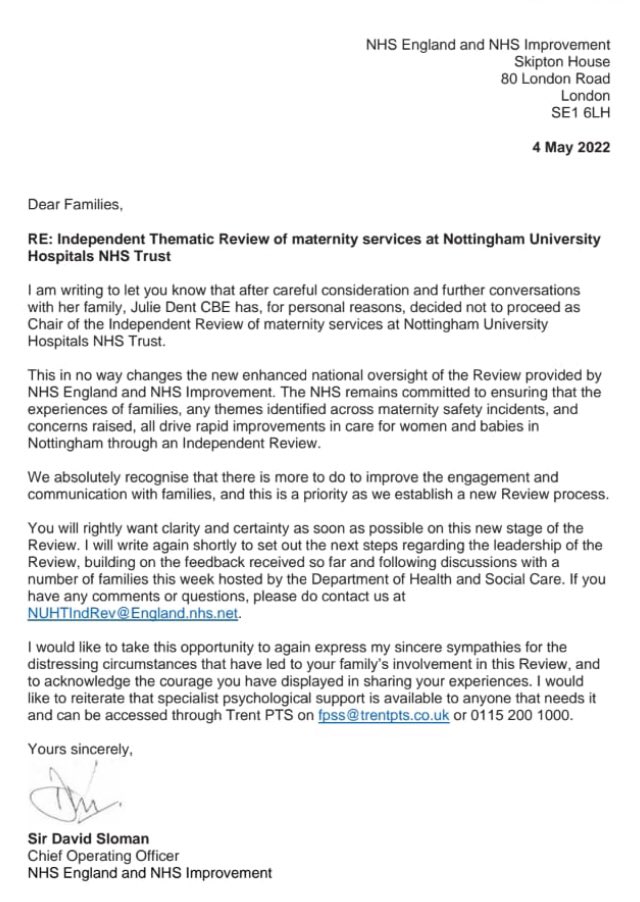
Julie Dent is Sajid Javid’s controversial appointment for heading the Nottingham Maternity Review. This post is about various governance failures at the NHS trust where Julie Dent was previously the Chair:
This post is about the recycling of the disgrace former CQC Chair Jo Williams back into the NHS, quite possibly with the assistance of a former King’s Fund Chair who failed to answer questions about his role:
This about whistleblowing governance failures, made worse by collusion between the National Guardian’s Office with an NHS trust board, and failings in maternity care:
By Dr Minh Alexander Retired consultant psychiatrist 30 April 2022
Hot on the heels of widespread concern about the government’s seizure of control over the formerly independent Electoral Commission, its Anti Corruption Champion John Penrose MP is now backing a proposal to create a whistleblowing regulator that will be under the government’s control.
Penrose, a Tory backbench MP for Weston Super Mare, better known by some as the husband of Dido Harding, formerly Chair of NHS Improvement and head of the £37 billion Test and Trace programme which reportedly ran out of money.
BACKGROUND INFORMATION ABOUT THE ANTI CORRUPTION CHAMPION This is a link to information on the Home Office website about John Penrose’s role as The PrIme Minister’s Anti Corruption Champion: https://www.gov.uk/government/people/john-penrose
This is an article about the role of the Anti Corruption Champion based on released documents:
The Telegraph reported that Penrose was backing the Bill read into parliament on 26 April 2022 by the controversial Whistleblowing All Party Parliamentary Group and its even more controversial secretariat, the organisation WhistleblowersUK.
This Bill, which has still not been made transparently available despite numerous requests to the APPG Chair and the leadership of WhistleblowersUK, reportedly set out to establish an Office of the Whistleblower.
“[The Office of the Whistleblower] will …report back to the Government.”
This fatally undermines its independence and sinks many future whistleblowers, public sector whistleblowers in particular, who raise concerns about government failures.
A concern held by many experienced whistleblowers and respected senior academics in the field is that the Bill is a Trojan horse to allow the billion dollar US bounty hunting industry to finally break through into the UK market, after many years of repeated rebuffs.
Penrose gave a little reported interview to GB News on 26 April. I apologise for giving any oxygen to this channel but I do so here in the public interest. Penrose seemed to imply that he was speaking as the Anti Corruption Champion and that “we”, as in the government, thought the Robinson Bill a “good set of suggestions” but that alternative good ideas would be considered:
“I’m sure we’d be all ears”
The timeline of events raises some questions about political tactics and gameplay to shoe-in bounty hunting that is targeted at lucrative financial recovery from the financial sector – the real target and prize for the bounty hunting lawyers. Bounties in the US financial sector can be huge – up to hundreds of millions in some cases. A vast proportion of this goes to the lawyers.
The middlemen, the lawyers, always win. Whistleblowers and the public not so much. The bounty hunting model abandons many genuine whistleblowers, it wastes vast sums in obscene rewards to individuals that could be spent for the common good and it gives whistleblowers and whistleblowing a bad name.
Robinson’s Bill had its first reading on 26 April with a note in Hansard that the second reading would take place on 6 May, however, parliament was then prorogued.
WhistleblowersUK gave an undertaking before the first reading that the Bill would be published as soon as Robinson had made her speech. But the Bill still remains withheld despite numerous requests.
A careful examination of John Penrose’s interview to GB News on 26 April 2022 may reveal the reason why the second reading of Robinson’s Bill was curiously scheduled, and why the fabled Bill has not materialised:
“John Penrose MP5.01: Yeah, I’m waiting for a government minister to say mañana at the dispatch box, that would be a parliamentary moment. But you’re right, it’s always a problem of timing, of getting space in the legislative timescale to do this sort of stuff. There is however, some legislation coming up, there’s an Economic Crime Bill which will we’re hoping will be coming up in the next couple of months. We could put some whistleblowing clauses in that to solve some of the problems that you and I are talking about here. So the time is now, the moment is available and so even if we can’t get a full blown Whistleblowing Bill Act stand alone, we may be able to get some of these things that I’m talking about into another piece of legislation quite soon if the government is willing. That’s the reason why I’m supporting Mary Robinson’s Bill today. And I hope it will attract some attention and perhaps get a bit of a following wind.”
So, was Robinson’s ten minute motion just a political device by the bounty hunting industry for creating some media noise, using mainly unsuspecting whistleblowers from all sectors as camouflage? When in fact the target was the rich bounties from the financial sector?
This is the full transcript of Penrose’s interview for those who are interested:
Penrose’s grasp of whistleblower detriment seems a little tenuous. Perhaps he misspoke but he seemed to suggest that whistleblowers are pursued in the Employment Tribunal by their former employers and colleagues:
“…you may find yourself being pursued for.. through an Employment Tribunal effectively for what your colleagues think of as betraying secrets”
Penrose gave excessive emphasis to the importance of “guidelines” associated with Robinson’s Bill, as if the acres of guidelines that we have had for over twenty years have ever protected any whistleblower.
There was also a hint of sympathy for the Devil in his comments that whistleblower reprisal is “understandable” and “human”, although he does acknowledge that it is “really unacceptable”.
There is an implication running through his interview comments that his focus is on crimes and the police.
This is interesting because WhistleblowersUK have in the past suggested that the Office of the Whistleblowers should be located in the Home Office, which is where John Penrose’s role as Anti Corruption Champion is also located. So who knows for how long these conversations have been going on? And what a horrendous thought: whistleblower welfare under the control of the highly suppressive Home Office.
Penrose is not alone in welcoming the Robinson Bill. A number of whistleblowers who are not from the financial sector have been gulled into supporting the Robinson Bill, when the bounty hunters have little interest in helping them. There is no money in poor healthcare or social care quality or child abuse. Some have definitely not seen the Bill. I have been sent correspondence which shows this, and thank those who shared it with me. It seems likely that many others have not seen it either. This reflects badly both on the credulity of those who have acted uncritically and also on the APPG’s undemocratic manipulation and its lack of accountability. A deep irony when whistleblowing is the issue, but perhaps not so much if this is in fact just about lucre. And of course, a few parties may be fully complicit with the venture. Some have literally been dining out on it.
Notwithstanding, if you are opposed to profiteering from whistleblowing, why not make your feelings known to the The Prime Minister’s Anti Corruption Champion, and suggest that he listens to all voices and not just industry lobbyists with a financial interest? After all, he is the Anti Corruption Champion and ought to recognise a conflict of interest when he sees one.
I have written to Mr Penrose as follows:
BY EMAIL
John Penrose MP
The Prime Minister’s Anti Corruption Champion
Home Office
30 April 2022
Dear Mr Penrose,
Protecting the public interest in the reform of UK whistleblowing law, discouraging profiteering and conflicts of interest and influence by lobbyists
I write to you in your Home Office role as The Prime Minister’s Anti Corruption Champion.
I note with thanks that you have taken an interest in reform of UK whistleblowing law, which as you say is well overdue for reform.
UK whistleblowing law was in fact fatally flawed from inception over twenty years ago because it was designed to ignore whistleblowers’ concerns and it treated whistleblowing as an employment dispute rather than a matter of public protection. It placed the whole burden on whistleblowers and placed virtually no responsibility on the State.
I see that you have backed Mary Robinson’s Bill as read into parliament on 26 April 2022. I am afraid that the Bill remains unpublished despite an undertaking by her APPG secretariat to publish it on that same day, so there has been no opportunity for real debate or scrutiny. Notwithstanding., my view is that the Bill is fatally flawed by Ms Robinson’s proposal that the whistleblowing regulator should be under government control. This creates unacceptable conflicts of interest and great dangers for the many whistleblowers who raise concerns about government failures.
There are also concerns that the legislation is intended to generate litigation and business for bounty hunting lawyers, which is not a lean or efficient manner of running public services. You indicated that the government would be “all ears” regarding better ideas, and as such I refer you to the US Office of Special Counsel for federal whistleblowers which has nimble powers of redress at a stage of an earlier stage whistleblower’s journey, before all has been irreversibly laid to waste. This Office can restore unfairly lost career progression or expunge unfair disciplinary records, and allow whistleblowers to return to their lives in a way that financial compensation after the event cannot. This Office is run with a much stronger public interest ethos than the hybrid model espoused by the Robinson Bill which gives entry to private interests.
In the same vein, please see this paper, now published in International Journal of Law and Management on non-financial redress for whistleblowers in the form or redeployment and re-employment. Very large public sector employers such as the NHS have no good reason not to run a re-deployment scheme across the range of its organisations. This would ensure efficient retention of expensively trained workforce, instead of the wasteful dismissals and de-skilling that we currently see in whistleblower cases. At present there is only a very unsatisfactory post-dismissal employment-finding support scheme for NHS whistleblowers.
Please see this letter to Margaret Hodge MP which contains more details about the need for public interest principles in any reform of UK whistleblowing law, to prevent hijacking by those who would profiteer from it.
The letter references the Public Interest Protection Bill by Dr Philippa Whitford MP which was written with principles of early conflict resolution and minimisation of destructive and wasteful litigation in mind. I hope those principles would be attractive to any government interested in efficiency and in rooting out conflicts of interest that the Robinson Bill is likely to create.
May I also emphasise that it is not a want of guidelines that have failed UK whistleblowers. We have been awash with guidelines for over twenty years. What has been lacking is a legal duty to act on disclosures, a proactive legal duty to protect whistleblowers (as opposed to a facility for retrospective compensation), and fit for purpose enforcement including criminal penalties for individuals. Those are the three critical pinch points that new legislation should address.
I would be very grateful If you could set up a listening exercise to formalise receipt of evidence from all interested parties who might wish to share good ideas with you on whistleblowing law reform, with respect to your comment to GB News that you and the government would be “all ears” for good alternative proposals to those of the Whistleblowing APPG.
I do hope that the APPG’s proposals will not be inserted into the Economic Crime Bill without fair and democratic consideration of other view points, especially from those with no economic interest in the policies.
Lastly, I submitted an FOI to the Home Office (see below) essentially to find out more about the Bill that Mary Robinson and her APPG have purportedly drafted, due to the failure by the APPG to be transparent about what it is they are asking the public support. If you are minded to simply let me have a copy of the APPG Bill and some of the contextual information that I have asked for, I would be extremely grateful.
With best wishes,
Dr Minh Alexander
Retired Consultant Psychiatrist and NHS whistleblower
FOI REQUEST TO HOME OFFICE 30 APRIL 2022
From: Minh Alexander <REDACTED>
Subject: The Prime Minister’s Anti Corruption Champion’s support of a whistleblowing Bill to establish an Office of the Whistleblower
Date: 30 April 2022 at 00:12:57 BST
To: FOI Requests Home Office <REDACTED>
Reply-To: REDACTED
Dear Sir,
The Prime Minister’s Anti Corruption Champion’s support of a whistleblowing Bill to establish an Office of the Whistleblower
The Prime Minister’s Anti Corruption Champion John Penrose MP recently lent his support to a Bill proposed by Mary Robinson MP to establish and Office of the Whistleblower which was read in under the ten minute rule on 26 April.
Mr Penrose gave an interview to GB News about this matter and his support for the Bill was also reported by other media outlets.
Please can the Home Office disclose:
– What consultations took place between Mr Penrose and Ms Robinson and or the Whistleblowing APPG which she chairs, or its secretariat the organisation WhistleblowersUK, which led up to Mr Penrose’s decision to support the Bill?
Were there meetings and or correspondence? Please give details
– Please indicate at what point Mr Penrose had sight of the proposed Bill in question, and which version of the Bill informed his decision to support the proposed legislation?
– Please disclose a copy of the version of the Bill of which Mr Penrose had sight
– If Mr Penrose did not actually see the Bill proposed by Mary Robinson, please also disclose this
– Please disclose if Mr Penrose discussed the possible future location of the proposed Office of the Whistleblower with Ms Robinson and or the Whistleblowing APPG or its secretariat, WhistleblowersUK
– Please advise if any possible government Departments were identified to oversee the putative Office of the Whistleblower, for example, was the Home Office discussed as a possible location for the new whistleblowing regulator?
Yours sincerely,
Dr Minh Alexander
RELATED ITEMS
These posts relate to concerns about the organisation WhistleblowersUK, which has a history of charging whistleblowers for services:
By Dr Minh Alexander retired consultant psychiatrist 28 April 2022
This is a very brief post to share the High Court judgments from the important and widely reported case brought by two grieving daughters against the UK government for its deplorable handling of care homes during the pandemic.
Our government of extremists and law breakers has a track record of holding life very cheap. Especially life that is of colour, life that is economically unproductive and life that it generally deems unworthy of life, to coin a phrase from an egregious era of the twentieth century.
The current mass COVID denial that the government has engineered and its modelling of callous disregard for hundreds of daily continuing COVID deaths perhaps numbs some people to earlier deaths in the pandemic.
Notwithstanding, the government policy of recklessly seeding COVID into care homes via hospital discharges has now been examined by the High Court and found wanting.
The High Court recognised this as “an important and legitimate claim” and it noted that staggeringly, about 20,000 care home residents in England alone died in the first COVID wave.
This is the core of the Court’s finding which has determined that the government acted unlawfully:
“The common law claim succeeds against the Secretary of State and Public Health England in respect of both the March Discharge Policy and April Admissions Guidance documents to this extent: the policy set out in each document was irrational in failing to advise that where an asymptomatic patient (other than one who had tested negative) was admitted to a care home, he or she should, so far as practicable, be kept apart from other residents for 14 days.“
That is to say, whilst some some care home staff made great sacrifices, locked themselves away from their families and lived on site at work to protect their vulnerable residents, HM Government undermined their efforts and recklessly sent infection into their care homes.
There are few details publicly available about the law.
I have today written to Margaret Hodge and some other senior parliamentarians, who have taken an interest in whistleblowing matters, about concerns that the public interest should be properly safeguarded in any process of law reform, and not hijacked by private interests.
The correspondence follows:
BY EMAIL
Dame Margaret Hodge MP
House of Lords [NB This should state House of Commons]
25 April 2022
Dear Dame Margaret,
Discouragement of financial incentives for whistleblowing in the UK and profiteering from whistleblowing
I write to you in acknowledgment of your longstanding support of whistleblowing and work on whistleblowing as former Chair of Public Accounts Committee and more recent interventions, and to ask for your help in ensuring that future reforms are guided along a steady path of public interest. This is with respect to your continuing interest in much needed reform of UK whistleblowing law.
There has unfortunately been steady pressure in recent years for a breakthrough from the US legal market into the UK of the bounty hunting model, most applicable to the financial sector, for recovery of enormous sums and commensurate rewards for reporters. This is a billion dollar industry for litigators.
The US bounty hunting model serves the State’s narrow financial needs for recovery of large sums lost to fraud but it does not promote a healthy whistleblowing culture or justice. It does not reliably protect most whistleblowers and leaves many genuine whistleblowers in the cold. It also puts the good name of whistleblowers and whistleblowing in jeopardy, which adds to the difficulties that whistleblowers already face with credibility.
Of huge importance, the US bounty hunting model does not concern itself with whistleblowing that is about protecting the person, if there is no money to recover. Thus it neglects swathes of important whistleblowing such as that in health and social care.
The UK Whistleblowing APPG originally proposed an Office of the Whistleblower such as that in the US which recovers money for the State using the bounty hunting model. The APPG’s model had the added feature that this Office would effectively act as a broker for approved private law firms and other entities – passing on business to them:
“…form and maintain a panel of accredited legal firms and advisory bodies to advise and support whistleblowers”
I am very uneasy about this, given that the Whistleblowing APPG was established with the involvement of and funding from a major US bounty hunting law firm from the outset. This is in the context of the longstanding general concerns about APPGs serving as lobby groups for private interests and hostile State interference.
A litigation heavy model is also wasteful for the public purse and traumatic for whistleblowers, because it implies prolongation of conflict.
A much leaner and more just model, with a better public interest ethos is that operated by the US Office of Special Counsel for federal whistleblowers. This Office has powers to direct non-financial redress such as restoration of lost career progression and expunging of unfair disciplinary records. This is much more in line with what most whistleblowers want and need – nimble, proactive protection to get back to their lives rather than retrospective compensation after everything lies in smoking ruins, whilst lawyers profit the most.
There are moreover concerns about WhistleblowersUK the secretariat of the Whistleblowing APPG, which have been raised a number of times with parliament. I copy below in the appendix links to some of the evidence that has been submitted to APPG members. This includes a thorough due diligence review by well known corporate whistleblower Wendy Addison, which raised concern about WhistleblowersUK’s direct role in supporting the bogus Westminster paedophile ring whistleblower Carl Beech.
Some of the other evidence that has been submitted is more sensitive and not suitable for sharing in the public domain. You may be aware that Norman Lamb resigned as APPG Vice Chair because he was unable to get reassurances from the CEO of WhistleblowersUK to questions that I raised with the APPG. He also received other evidence of concern.
Please note this WhistlebowersUK document, from a whistleblower who contacted the organisation – it shows that WhistleblowersUK asks whistleblowers for a fee of £100/hour for services and 5% of settlements and awards.
Please also note this ET judgment which revealed a bill by WhistleblowersUK for services charged at £150 per hour for sorting “documents into chronological order” in a whistleblower case. This claim was withdrawn after the ET Judge queried the status of the organisation under regulations for claims management.
“These actions that benefit society should be encouraged and recognised by way of financial compensation, and other forms of recognition, separate from that awarded by the tribunals. The amount can be determined by the Office of the Whistleblower.”
WhistleblowersUK penned a flyer in March 2022 about “compensating” whistleblowers which was a response to John Penrose MP discouraging financial incentives for UK whistleblowers. This WhistleblowersUK flyer in fact promoted the US reward system and it claimed “almost every whistleblower becomes dependent on compensation because of the catastrophic impact on their lives and those around them”. The point here is that well designed whistleblowing law should prevent catastrophic harm. It is only weak whistleblowing law that results in distraction from whistleblowers’ public interest disclosures and ends up with a secondary quagmire of employment dispute and a legal circus.
I note the press reports that the Whistleblowing APPG is proposing criminal penalties – which are welcome – but also fines of up to £18 million against organisations for whistleblowing breaches. I would be concerned if such fines are applied to the public sector because of the impact on public services. I would also be concerned if such monies are ultimately transferred from the public purse to private law firms or other private entities via the Office of the Whistleblower.
If any law maximises conflict, disruption and litigation and if that benefits middlemen the most, it will hardly serve either the public interest or whistleblowers.
There should be no inappropriate closeness between any putative whistleblowing regulator and private law firms or other private entities, nor conflicts of interest in the establishment of any new whistleblowing regulator. The creation of a new whistleblowing regulator should not be a Trojan horse for bounty hunting nor in effect construct a front door for the private whistleblowing litigation and compliance industry.
There should be no end effect of targeting resources on financial recovery and any lucrative bounties which that may net for some parties, at the expense of protecting the health and safety of the public.
A dysfunctional whistleblowing regulator would be the very worst of all worlds for the public and for whistleblowers. It would compound the serious deterioration we have seen in UK governance, not relieve it.
Lastly, may I refer to you the principles of the Public Interest Protection Bill originally laid in parliament by Dr Philippa Whitford.
Importantly, this gives primacy to the system response to whistleblowers’ concerns and therefore the public interest.
It also seeks as a principle to minimise both harmful employment consequences and related litigation, and so to avoid waste.
Dr Whitford’s Bill ensured that a whistleblowing regulator should be fully independent of government. This is crucial. I emphasise it because WhistleblowersUK at one point proposed that the Office of the Whistleblowers should be located in the Home Office, one of the worst Departments for suppression:
I believe WhistleblowersUK has now deleted this post about the Home Office.
Dr Whitford’s Bill also contained a principle of active review by parliament to ensure that any whistleblowing regulator does not stray or go stale, as can easily happen, and has happened in other jurisdictions.
I ask you and other parliamentarians to safeguard these public interest principles in any endeavour to reshape UK whistleblowing law.
I hope you can help.
With best wishes,
Dr Minh Alexander
Retired consultant psychiatrist and whistleblower
Cc Dr Philippa Whitford MP
John Penrose MP Prime Minister’s Anti-Corruption Champion
Lord Hendy QC
Lord Sikka
Lord Morse
Meg Hillier Chair PAC
Whistleblowing APPG Vice Chairs and member Lisa Cameron, Rosie Cooper, Rebecca
Long Bailey
Correspondence and evidence submitted to parliament about WhistleblowersUK has included:
Ahead of the debate on the new Bill, a member of the whistleblowing APPG Kevin Hollinrake Tory MP has pushed in parliament on 25 April 2022 for financial rewards:
He was also quoted in a recent article which pressed for financial rewards:
“The problem is this touches the wider perception of whistleblowing, and whether it’s worth coming forward,” Hollinrake said…..Campaigners are pointing to this broader push, arguing that the U.K. also needs to bring more monetary incentives to the mix as it sets to overhaul its approach to economic crime…”
UPDATE
Mary Robinson briefly read her new Bill into Parliament on 26 April. It remains unpublished. But from the Hansard record of her speech, it is clear that the intention is that the proposed Office of the Whistleblower will NOT be independent. It will report to the Government. This will be far worse than useless. It will be seriously harmful and set up grievous and corrupt conflict of interest in all the cases where whistleblowers raise concerns about government failures, directly or indirectly.
“It [the Office of the Whistleblower] will set standards and report back to the Government” [my emphasis]
I wrote on 28 April 2022 to Mary Robinson to ask for a copy of the Bill has it had remained unpublished despite the drip feed of selective accounts to the press.
Wendy Addison fellow whistleblower has on the same day pointed out an email of 22 April 2022 from the CEO of WhistleblowersUK, the APPG’s secretariat, which claimed that the Bill would be uploaded as soon as Mary Robinson had given her speech in parliament on 26 April:
WhistleblowersUK have organised a webinar on the Bill on 29 April 2022, the tickets for which cost £10. Perhaps the expectation is that one must pay for information that would normally be freely available as a matter of democracy.
RELATED ITEMS
This is a matter relevant to the current row about Sajid Javid’s controversial decision to override bereaved families’ wishes and to appoint a former NHS manager to chair a review into maternity failings at Nottingham. This is a post about governance failings at her former NHS trust:
By Dr Minh Alexander retired consultant psychiatrist 24 April 2022
This is a post about an Employment Tribunal judgment against Devon Partnership NHS Trust, a mental health provider, against a worker with a mental health condition.
I had intended to write it up as it has implications for all mental health providers. It has since become especially significant following the Secretary of State’s controversial decision to override bereaved families’ wishes, with an announcement late on a Friday that an NHS management old hand would chair a review into the maternity failings at Nottingham University Hospitals NHS Trust – Julie Dent, former Chair of Devon Partnership NHS Trust.
Rhiannon here as you & I know K, the compounding of harm through badly timed, often harmful or contradictory communication is a deliberate form of abuse for complainants. As is always ensuring the 1st incident investigation is appalling. It’s then hidden behind aggressively 1/2 https://t.co/wMRYj5MGJI
“Julie Dent CBE was Chief Executive of South West London Strategic Health Authority until 1 July 2006. She left the NHS in March 2007 after 22 years to take up a new portfolio career including being Chair of the London Probation Board from April 2007 to March 2012.
She became Chair of Torbay NHS Care Trust in December 2009, and since March 2013 has been Chair of Devon Partnership NHS Trust.
Prior to this she established her own consultancy/coaching company coaching chief executives, chairs and directors in the NHS. She has worked extensively across London and the South East with clinical commissioning group leaders, and in the past year has coached senior leaders in the third sector.
She is a trustee of the School Food Trust and the Children’s Food Trust. She is Chair of User Voice, a ground-breaking charity for offenders.
Julie was awarded the CBE in 2005, after the London bombings, for services to the NHS.”
Dent retired as Chair of Devon Partnership NHS Trust in February 2020
NHS Whistleblower scandals
Dent was reportedly one of several senior NHS officials who denigrated Ian Perkin St. Georges NHS whistleblower for not being a “corporate player”.
She was also Chair of Torbay and Southern Devon Health and Care NHS Trust when it was sued by whistleblowers who raised concerns about nepotism by the notorious Paula Vasco-Knight. The ET held that the other respondent trust was the guilty party, but did Dent push hard enough against the cover up by the chair of the other NHS trust?
On 18 March 2022 the Employment Tribunal ruled that Devon Partnership NHS Trust was found guilty of disability discrimination against a peer support worker, Mrs Zena Cockles.
The events in question started during Julie Dent’s tenure as trust Chair. Mrs Cockles was hired by the trust in 2019 as a peer support worker, someone with lived experience of mental ill health employed specifically to use that experience to support mental health patients.
Mrs Cockles attended Occupational Health before starting work, resulting in advice to the trust that she had a disability, was symptomatic but was fit for work, and in need of structured weekly discussions:
“Mrs Cockles has underlying psychological condition. She is not completely asymptomatic and feels that this is triggered by some ongoing difficult personal circumstances. I have advised her to continue to monitor her mood and should she feel that it continues to dip to contact her GP.
I feel that she is fit for work with adjustments mentioned below.” ….
“It is advisable that regular structured support under the form of weekly discussions is considered for the first month of her starting the job and regularly thereafter.”
The post was not at all structured as Mrs Cockles was left to define what the new role would be. She started work in November 2019. Not all trust staff were aware of her arrival, and there was awkwardness fitting in because her role was not clear. Structured weekly supervision did not take place, admittedly initially with Mrs Cockles’ agreement as she had asked for more frequent ad hoc contact. However, structure was still not provided long after it was clear that she was struggling without it, and had herself indicated that she needed structure:
“I feel lost at the moment. As anyone would feel with no routine or structure I cant function properly”
There was a disconnect noted between how her line manager saw the situation – desirable flexibility in how the role could be developed – and how Mrs Cockles described her experience of it.
The line manager recounted: “the role was new to the Directorate, but that this was exciting because it means the successful candidate would work with DPT to shape the role and identify what would work best.”
Mrs Cockles in fact felt at sea and not secure or properly welcomed. For example,
“Emailed EE again about my laptop as it was so hard trying to get into Rougemont all the time as I had no ID, no name badge, no keys or fobs to get in and around the place. EE replied 13/01 saying she will chase them up.”
The difference in perception between Mrs Cockles and her line manager was so great that the Employment Tribunal commented:
“This is in stark contrast to the position Mrs Cockles portrayed in the Grievance and we are left wondering if they had been in the same meeting”
A change of her role by managers from face to face work to telephone surveying of post discharge patients met with difficulty. Mrs Cockles reported a lack of guidance and information, and she was not happy with the major change:
“No one has been in touch with me to explain that this would now be my job role and this is the first I am hearing about it I said to her it has changed so much and that I had no idea what I was supposed to be doing anymore. I told her it was starting to stress me out and I just wanted a job role….I said but I don’t have a job role. I was supposed to be seeing patients and talking to them on peer level of someone who has that understanding of what they are going through and so far I’ve not seen 1 patient in 3 months.”
When there was a change of line manager after fourteen weeks due to maternity leave, there was reportedly no evidence of handover about Mrs Cockles’ disability or the Occupational Health report and its recommendations. Mrs Cockles reported that her new line manager did not return her messages. She applied for a new peer support worker post. In the process, critical correspondence between managers was inadvertently copied to her.
The correspondence described Mrs Cockles as “unboundaried [sic] and confrontational” and questioned “that she has the self-awareness, insight and diplomacy required for this key role.”
This in itself was likely to be an act of discrimination because it displayed a lack of awareness that the behaviours criticised might be due to a relapsing or sub-optimally controlled mental illness ,(the ET noted a diagnosis of Bipolar illness, which is indeed a relapsing-remitting illness). Had this been better managed and supported, it might be no barrier to the post in question. Surprising that this did not seem to occur to a mental health organisation.
Indeed, a later consultation with a support service for trust workers during the pandemic noted a deterioration in Mrs Cockles’ mental health, and she was eventually signed off sick.
The employment arrangements continued to be sketchy, with a brief transfer to a non-peer support worker role. After a grievance process, the trust apologised for her poor experience and the lack of adequate support. Mrs Cockles accepted a new post but the ET noted that she withdrew her acceptance after she made a request that the learning about her experience to be shared and something be done about the “inappropriate” email that was copied to her. It is not clear what the trust response to her two requests was, but the ET implied it was not affirmative.
The ET noted: “Mrs Cockles reluctantly changed her position again, however, when it was explained to her that the extension of her contract was conditional on the acceptance of a post.”
If I understand this correctly, the trust left her with no real options.
Ultimately, “Mrs Cockles’ employment with the Trust ended on the expiry of the fixed term of her contract, on 24 February 2021.”
This is an uncomfortable story. Trusts should not employ vulnerable peer support workers as a matter of tokenism or virtue signalling, without thought and preparation. The idea of peer support workers of itself carries a kernel of stigma – the subtle implication being that “ordinary” staff do not have lived experience of mental ill health – when statistically, due to the frequency of mental ill health in the general population, many are bound to.
But where peer support workers are employed explicitly to use their own valuable experiences to help others, trusts have a special duty of care to ensure that the working environment is safe and supportive, and that the managers supervising such workers understand their task.
The fact that Mrs Cockles met with such an “unboundaried” [sic] organisational response to the employment of a peer support worker is ultimately a failure of board leadership to recognise and proactively manage the serious risks of any failure to support peer support workers. The trust board failed to ensure the delicate balance of empowering a user perspective without abrogating all responsibility as an employer, and in fact causing injury. Mrs Cockles should have had a very different reception and experience.
The tokenistic and undoubtedly ham-fisted organisational behaviour, which led to the Employment Tribunal awarding Mrs Cockles £10,613.59 just for injury to feelings, adds to the questions about whether the Trust’s former Chair is the best person to conduct a sensitive review and to understand and meet the needs of bereaved families at Nottingham.
This is Julie Dent pictured with the peer support worker project team, at a 2018 trust awards ceremony. The person in the top hat is Melanie Walker, trust CEO.
Julie Dent has decided not to chair the review into maternity safety at Nottingham after family opposition, citing personal reasons, as reported by NHSE/I:
RELATED INFORMATION
Coroner’s findings
Devon Partnership has been rated “Good” by the Care Quality Commission, but mental health trust ratings are unreliable when all are seriously under resourced and operating under serious, chronic bed pressure.
Listed below are published coroners’ Prevention of Future deaths reports – usually issued only exceptionally – that have been issued against the trust. They include a number of inpatient suicides. The case of Diane Knight revealed shocking practices of patients being allowed to cover observation windows – implying that it was commonplace not to carry out observations at night.
This was of particular concern because an earlier coroner’s PFD had highlighted the inpatient suicide of Elaine Jobe, in which lines of sight for observation were an issue:
There have also been a steady stream of serious incidents reported in the press.
These have included allegations by a whistleblower following an inpatient death, that trust managers repeatedly ignored concerns about unsafe staffing levels:
“An urgent probe has now been launched at The Haldon, part of Wonford House Hospital in Exeter after bosses were allegedly warned of the dangers that something like this could happen due to cuts in staffing levels.
The whistleblower said: “I am aware that staff have repeatedly raised concerns that the ward was unsafe due to insufficient staffing.
“It had been repeatedly flagged up by ward staff as a major risk factor.”
These are a sample of other media reports about serious incidents at the trust:
“Barrister Catherine Oborne, on behalf of the O’Sullivan family, cross examined both Mr Cole and Devon Partnership Trust’s Carolyn Crowe about why he had been discharged from the crisis team on December 5 and about the use of the diagnosis as a ‘malingerer’.
“The family of Alan Prettyjohn, 44, is calling to not judge people who suffer from mental health conditions and for better help to be made available to them in Devon….Alan did not even receive a mental health assessment.”
For followers of medical politics, Adrian James the President of the Royal College of Psychiatrists and former medical director of the trust is a consultant psychiatrist based at Devon Partnership NHS Trust. Prior to becoming President, he represented the Royal College as Chair of the Westminster Parliamentary Liaison Committee of the Royal College of Psychiatrists.
As Chair of the Health Select Committee she declined for years to hold a follow up hearing into the government’s failures to meet the recommendations of her own Committee on NHS whistleblowing and the related failures of the NHS Freedom To Speak Up project.
Safe Staffing in the NHS
It is clear that maternity failures are widespread across the NHS and that there are systemic issues that have not been adequately tackled. One crucial matter is safe staffing – a recommendation from the MidStaffs Public Inquiry that has been resisted by successive Tory governments over the last decade, because they do not wish to fund it. NHS staff whistleblowing about safe staffing is not well handled, as it is a matter that sits in the “too difficult” box.
A recent whistleblowing matter at Sussex, where staff were told to stop raising concerns about unsafe staffing levels, illustrates this: