By Dr Minh Alexander, NHS whistleblower and former consultant psychiatrist 15 March 2017
I am in favour of justice being seen to be done, if public servants act dishonestly and endanger the public.
For too long now, there has been impunity for senior officials who cover up failures and risks, and who victimise those who speak out.
The NHS whistleblowing organisation Patients First says that it supports just culture.
I have invited it to fully reflect this in its policy position, by supporting sanctions for whistleblower suppression and reprisal, including criminal sanctions in at least some circumstances.
A formal proposal is provided below.
RELATED ITEMS:
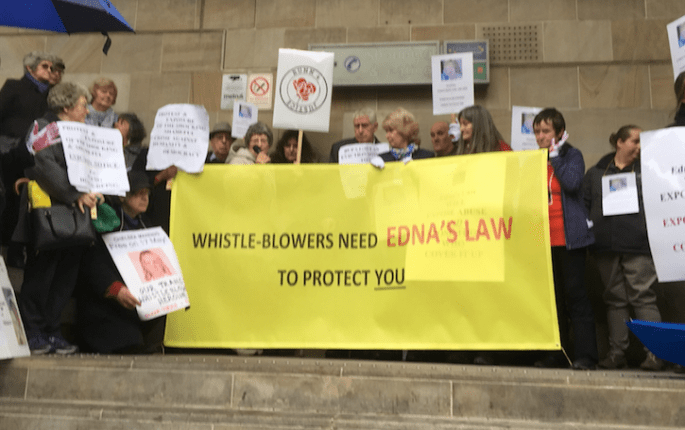
1. Edna’s Law by Compassion in Care:
http://www.compassionincare.com/node/162
2. Hillsborough Law – a bill on outlawing failures of candour by public servants:
http://www.thehillsboroughlaw.com/
3. The example of Paula Vasco-Knight, an NHS CEO who was found to have bullied whistleblowers but was protected and recycled by NHS regulators
https://minhalexander.com/2017/01/27/cqc-a-chief-inspector-doesnt-call/
PROPOSAL PUT TO PATIENTS FIRST, 15 MARCH 2017
Discussion document: Sanctions for suppression of whistleblowers’ concerns and reprisal against whistleblowers
Introduction
This brief paper has been produced to facilitate discussion within Patients First and consultation with Patients First’s membership about the charity’s policy position on sanctions for whistleblower reprisal.
In writing this paper I focus on practical aspects of deterrence of reprisal, the encouragement of safe speaking up and the communication of healthy norms, which to my mind are the key objectives.
I note the King’s Fund paper of May 2015 on ‘systems leadership’ which featured an implied view that disciplining managers who victimise whistleblowers may not help patients. 1
In this paper, I oppose this view.
Patients First’s constitution states that the charity has two core purposes, one of which is:
“…to campaign for the advancement of a just culture in the National Health Service (“NHS”) and the healthcare services generally in England, Scotland, Wales and Northern Ireland in order to foster safer patient care.” 1
That being so, the charity should arguably support proportionate and fair sanctions for deliberate wrongdoing, which are an accepted feature of just culture.
Individual accountability
As Aveling et al observed, too much focus on systems can have the effect of undermining appropriate individual accountability in healthcare:
“Individual agency is both an ethical requirement and a means of modifying systems themselves; never holding individuals to account risks normalisation of failure, fatalism, externalisation of blame and apathy, and may erode collective commitments and values. The ability to impose sanctions for culpable failures is likely to remain an important feature of any well-functioning accountability system, but legitimate and effective exercise of this ability depends on a predictable, fair and effectively operated institutional infrastructure, with proportionate consequences and alignment of the values and processes of different internal and external forums.”2
Indeed, there was a concern arising from the Mid Staffs Public Inquiry that Robert Francis failed to send a message to the most senior actors responsible, and did not deliver justice to those affected by the disaster. 3
As Shojania and Dixon-Woods have argued, there is no reason why attention to systems issues cannot go hand in hand with removing ‘bad apples’: 4
“Yet ‘bad apples’—individuals who repeatedly display incompetent or grossly unprofessional behaviours— clearly exist. While they may not account for most patient safety problems, the field has probably reached the point where we can at least name the problem of bad apples without detracting from still crucial efforts to improve the design of organisational systems and human factors”
Nevertheless, Robert Francis recognised from evidence he received during the Mid Staffs Public Inquiry, that suppressing NHS whistleblowers has serious patient safety consequences. So much so that he recommended the behaviour should be criminalised for deterrence and to ensure rigorous protection for whistleblowers. 5 6
Francis’ report of the subsequent Freedom to Speak Up Review two years later was a disappointment. His report was weak on accountability. Francis made excuses for managers who had been guilty of misconduct. He referred to “retribution” which implied motives of revenge as opposed to the accountability that most whistleblowers seek. 7
In total reversal of his original position that sanctions would be a robust deterrent, he claimed that sanctions would actually result in greater cover up. 8
The last point is a substantially flawed argument on a number of grounds. For example, Francis produced no evidence that punishment for deliberate wrongdoing (cover ups in this context) would increase wrongdoing.
Just culture and patient safety
Contrary to Francis’ claims, there is evidence that a just culture which supports workers, prioritises safety, helps workers by remedying systems weaknesses, does not blame workers for errors of good faith that anyone in the same circumstances might make, but does hold people accountable for recklessness, negligence and other deliberate wrongdoing, creates psychological safety and promotes learning and safer practices. 9
Secondly, it is perverse that Francis acknowledged that whistleblower suppression is “serious misconduct” 10, but suggested that sanctions are undesirable. This is especially so when Francis went to the effort of recommending that whistleblowers should be held to account for the far lesser sin of raising concerns in an insufficiently tactful or otherwise inappropriate manner. 11
Serious misconduct is a clearly punishable matter by any standard NHS disciplinary policy.
If having acknowledged acts of whistleblower suppression and reprisal as serious misconduct, the NHS does not apply sanctions, this would cement discrimination against whistleblowers and seriously trivialise acts of suppression and reprisal. It would be the opposite of just culture.
Failure to sanction misconduct against whistleblowers sends a chilling message to other staff. The evidence is that staff do not always report safety concerns if they believe that they will suffer repercussions, or that nothing will be done about their concerns. 12
In other words, it is impunity and lack of sanctions that helps to perpetuate the cycle of cover up and bullying.
NHS organisations that are complacent and dismiss concerns, or seek to villify and scapegoat those who raise concerns have worse mortality outcomes. 13
Sanctions for whistleblower suppression and reprisal are arguably an important part of Safeguarding patients, and promoting staff welfare.
Law reform
The law has a communicative aspect and it functions as an important barometer of social values. If the public good is to be valued over self-interest and cover ups, there is also an argument for communicating distaste for whistleblower reprisal through better legislation. Wisely drafted and used, Law can be a pivotal component of changing culture and behaviour.
Although the criminology evidence base varies depending on context, and some sources conflict, there is overall empirical evidence that sanctions against criminal wrongdoing have a general deterrent effect, especially if punishment is certain, swift and fair. 14 15
In 2014, a statutory regulatory mechanism was introduced in the NHS for removing unfit senior managers: CQC Regulation 5 Fit and Proper Persons (FPPR). Robert Francis suggested in February 2015 that this should be the route for holding those who victimised whistleblowers to account. In November 2016, after delays and repeatedly poor performance by the Care Quality Commission, Francis admitted that FPPR was not working and that managerial regulation should be considered. 16 This implied that he accepted a more effective and enforceable system of accountability and sanctions was needed.
Moreover, under current UK whistleblowing legislation, the onus is on whistleblowers to sue via the Employment Tribunal. This means that many whistleblowers are priced out of justice, or that some risk and lose much or all in their efforts to seek justice. Only 3% of PIDA claims succeed at hearing 17 and compensation is often wiped out by legal fees. Whistleblowers may be left ruined or facing very uncertain futures. And at the end of it all, unsafe NHS senior managers usually remain free to suppress failings and risks, and endanger patients all over again.
In other models and proposals, the State has a more active role and takes greater responsibility for prosecuting whistleblower reprisal and wrongdoing by individuals. 18
Some of the harassment against whistleblowers meets the existing bar for criminal harassment 19 (and harassment law has been successfully used in at least one case).
Some also feel that suppression of concerns and reprisal should be criminalised per se.
There are also arguments for treating a finding of whistleblower suppression and reprisal as an aggravating factor if it is a feature in other criminal offences.
Without being too prescriptive about the exact form that any new legislation should take, it would be very valuable if whistleblowers are united in agreeing that in at least some instances, there should be criminal sanctions for whistleblower suppression and reprisal.
In conclusion
I suggest that Patients First recognises that sanctions for whistleblower suppression and reprisal are crucial to changing culture, and that the charity explicitly supports the principle of just and proportionate sanctions for those who victimise whistleblowers.
I also invite Patients First to support the broad principle that criminal sanctions are appropriate for whistleblower suppression and reprisal, at least in some circumstances.
Dr Minh Alexander
15 March 2017
REFERENCES
1 The practice of system leadership. King’s Fund May 2015
Page 52“One part of the problem is that when things go wrong, people look for a head on the block. And it can be the whistle-blower, not just others, who is looking for a head on the block – that someone, or a certain person, needs to be fired. And that doesn’t really help the patients, you know?”
https://www.kingsfund.org.uk/sites/files/kf/field/field_publication_file/System-leadership-Kings-Fund-May-2015.pdf
1 Patients First constitution 2015
https://minhalexander.com/wp-content/uploads/2016/09/patients-first-constitution.doc
2 What is the role of individual accountability in patient safety? A multi-site ethnographic study. Aveling et al. Sociology of Health & Illness Vol. 38 No. 2 2016 ISSN 0141-9889, pp. 216–232 doi: 10.1111/1467-9566.12370
http://onlinelibrary.wiley.com/store/10.1111/1467-9566.12370/asset/shil12370.pdf?v=1&t=j09nrzgr&s=948ec47cea58c2db188f71e20d58f68c693cfdb2
3 Return to the Killing Fields. Private Eye. 2013
“One wonders what version of his report Robert Francis was reading at the press conference on 6 February. He looked like a man held hostage. The interminable delay in publication to allow for rewrites had reportedly been because those he was minded to criticise had launched vigorous legal defences. In the end he opted for a ridiculous “no scapegoats, blame the system” approach. This was endlessly debated after the Bristol Inquiry report in 2001, when a culture of “fair blame” was proposed. Ill thought-out, untested, rushed and brutally-enforced reforms undoubtedly contribute to NHS disasters, but individuals also have to be held accountable for their actions. Patients and staff trust a system that is just. But the judge delivered no justice.”
http://drphilhammond.com/blog/wp-content/uploads/2013/03/Private-Eye-mid-staffs-final.pdf
4 ‘Bad apples’: Time to re-define as a type of systems problem? Shojania and Dixon-Woods
May 2013, Shojania KG, et al. BMJ Qual Saf 2013;22:528–531. doi:10.1136/bmjqs-2013-002138
http://qualitysafety.bmj.com/content/qhc/22/7/528.full.pdf
5 Recommendation 183 of the Report of the Public Inquiry into Mid Staffordshire NHS Foundation Trust
“Criminal liability
It should be made a criminal offence for any registered medical practitioner, or nurse, or allied health professional or director of an authorised or registered healthcare organisation:
Knowingly to obstruct another in the performance of these statutory duties;
To provide information to a patient or nearest relative intending to mislead them about such an incident;
Dishonestly to make an untruthful statement to a commissioner or regulator knowing or believing that they are likely to rely on the statement in the performance of their duties.”
https://www.gov.uk/government/uploads/system/uploads/attachment_data/file/279124/0947.pdf
6 Francis calls for new protection for whistleblowers, Shaun Lintern, Nursing Times 11 February 2013
“Speaking to Nursing Times, Mr Francis said: “I have called for a statutory duty of candour that trusts tell the truth to regulators and that there should be criminal sanctions if there’s willful obstruction of anyone performing their duties and informing their trusts about concerns to patients.
“That is about as rigorous protection of whistleblowers as you can imagine, and that’s what I intended,” he said.”
https://www.nursingtimes.net/news/reviews-and-reports/francis-report/francis-calls-for-new-protection-for-whistleblowers/5054780.article
7 Report of Freedom to Speak Up Review February 2015
Page 70 “Some whistleblowers may want ‘instant retribution’ but that that was not always within the power of the organisation to deliver.”
http://webarchive.nationalarchives.gov.uk/20150218150343/https://freedomtospeakup.org.uk/wp-content/uploads/2014/07/F2SU_web.pdf
8 Report of Freedom to Speak Up Review February 2015
Page 163 “7.5.6 However, there is another side to this which must be considered. Managers are just as vulnerable as other staff to the effects of the culture in which they work, and the pressures which are imposed on them. As stressed by some employers and their representatives a ‘just’ culture is equally as necessary for managers and leaders as it is for staff raising concerns. The consequence of an uneven approach could be a worsening blame culture for staff and a loss of talented managers from the NHS.”
http://webarchive.nationalarchives.gov.uk/20150218150343/https://freedomtospeakup.org.uk/wp-content/uploads/2014/07/F2SU_web.pdf
9 A roadmap to Just Culture: Enhancing the safety environment. GAIN working group. September 2004
https://flightsafety.org/files/just_culture.pdf
10 Report of Freedom to Speak Up Review February 2015
Page 165 “Good practice….
…. Discriminating against, or victimising, an NHS worker because they have raised a concern, or turning a blind eye when other officers or employees do so, is regarded as serious misconduct or mismanagement.”
http://webarchive.nationalarchives.gov.uk/20150218150343/https://freedomtospeakup.org.uk/wp-content/uploads/2014/07/F2SU_web.pdf
11 Report of Freedom to Speak Up Review February 2015
Page 162 “7.5.1 Everyone should be held accountable for their behaviour and practice when raising, receiving and handling concerns where this is not consistent with the values of a well-led organisation. This applies to those raising concerns as well as the managers and leaders handling concerns.”
Page 142 “Good practice – Training staff in raising and handling concerns
… how to raise concerns with tact to avoid causing offence or provoking defensive behaviour”
http://webarchive.nationalarchives.gov.uk/20150218150343/https://freedomtospeakup.org.uk/wp-content/uploads/2014/07/F2SU_web.pdf
12 Whistleblowing commission Public Concern at Work 2013
https://www.tuc.org.uk/sites/default/files/Whistleblowing%20Commission%20Report%20Final.pdf
13 Culture and behaviour in the English National Health Service: overview of lessons from a large multimethod study, Dixon-Woods et al, September 2013
http://qualitysafety.bmj.com/content/qhc/early/2013/08/28/bmjqs-2013-001947.full.pdf
14 Criminal Deterrence Research at the Outset of the Twenty-First Century, Nagin 1998,
Crime and Justice, Vol. 23 (1998), pp. 1-42
http://faculty.washington.edu/matsueda/courses/587/readings/Nagin%201998.pdf
15 Deterrence in criminal justice, Evaluating Certainty vs. Severity of Punishment, Valerie Wright 2010, The Sentencing project
http://www.sentencingproject.org/wp-content/uploads/2016/01/Deterrence-in-Criminal-Justice.pdf
16 Robert Francis calls for regulation of senior managers. Health Service Journal Shaun Lintern 9 November 2016
https://www.hsj.co.uk/topics/workforce/exclusive-robert-francis-calls-for-regulation-of-senior-managers/7013089.article
17 Public Concern at Work data 2013/14: Out of 2684 whistleblowing ET claims disposed in 2013/14, 92 claimants were successful at hearing (3%)
18 US Office of Special Counsel: https://osc.gov/
Office of the Whistlebower: https://www.sec.gov/whistleblower/
Compassion in Care, Edna’s Law: http://www.compassionincare.com/node/162
19 Lack of support for whistleblowers is a disgrace. Letter by Prof David Lewis to Guardian, 15 February 2016
“The Guardian has a laudable track record of supporting whistleblowing. However, in commenting on the impact of the Francis report on the culture of speaking up in the NHS (Editorial, 12 February), you demonstrate a rather conservative approach to legislative reform. First, there is no mention of possible criminal sanctions. Citizens who break the Official Secrets Act commit an offence, so why shouldn’t those who victimise people raising concerns in the public interest? TheProtection from Harassment Act can be invoked if the narrow definition of harassment is fulfilled, but, in my opinion, outlawing any form of retaliation against whistleblowers would send out a valuable message about what society expects.
Second, you do not point out that only “workers” are covered by our whistleblowing legislation. However, it is clear that those who are in a position to raise concerns may not have this status – for example, patients and their families. Other countries now recognise the role that the public can play in exposing wrongdoing; in this important respect, the UK no longer provides an international model.
Professor David Lewis
Director, Whistleblowing research unit, Middlesex University”
https://www.theguardian.com/society/2015/feb/15/whistleblowers-should-law-punish-hospital-bosses
©Minh Alexander2017