The poor, discriminatory treatment of BME staff in the NHS has been a long recognised stain upon the NHS’ reputation.
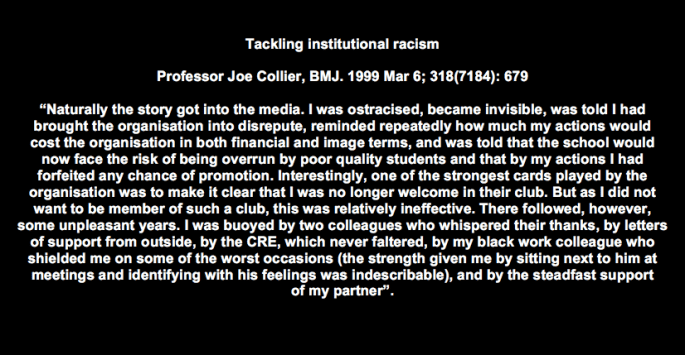
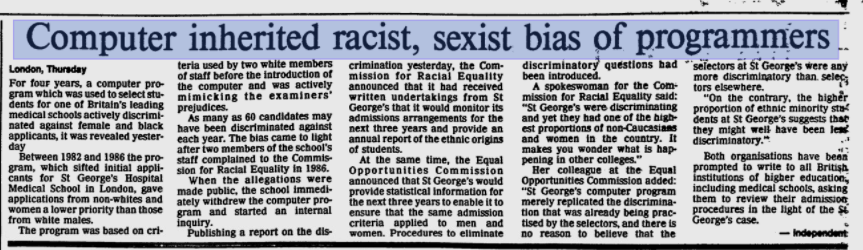
A landmark event in NHS Race history was Joe Collier and his colleagues’ whistleblowing about a racist computer programme at St Georges which weeded out foreign medical student applicants.
The classic book Racism in Medicine: An Agenda for Change, Naaz Coker et al 2001, is a very good, gripping read and still highly relevant.
NHS England commendably launched the Workforce Race Equality Standard programme (WRES) but its implementation has been a disappointment to many, with no focus on enforcement and a number of significant omissions in the parameters measured.
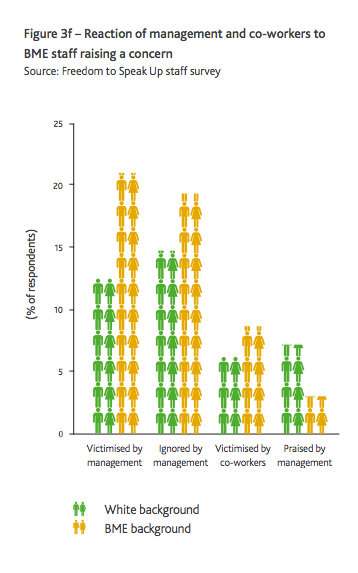
Whistleblowing and NHS racism are interlinked. Research done on behalf of the Speak Up Review showed that BME whistleblowers are more likely to be ignored and victimised.
I have asked Simon Stevens to prioritise the proper measurement of BME staff’s experience of whistleblowing through the NHS staff survey.
I have also asked him to uncork data that already exists at trust level on Race differentials for all domains of the national NHS staff survey.
I have been advised by the Picker Institute which administrates the survey for NHS England that the cost of analysing this trust level Race data is reportedly very modest:
“£1200-£1600 (excl. VAT)”
I find it perplexing that such analyses have not already been requested and published.
The letter to Simon Stevens, with supporting references, background correspondence and data, is provided below.
Dr Minh Alexander
NHS whistleblower and former consultant psychiatrist
11 October 2017
LETTER TO SIMON STEVENS
BY EMAIL
Simon Stevens
Chief Executive
NHS England
11 October 2017
Dear Mr Stevens,
Re: NHS England’s approach to Race Equality & Race analysis of NHS Staff Survey Data
I write about the rigour of NHS England’s approach and to make a request about better use of national staff survey data.
As you may be aware from correspondence to the NHS England WRES team into which I have copied you, I have concerns that the WRES programme is at this late juncture not measuring important matters such as Race Employment Claims against the NHS. Neither is it measuring Race pay inequality.
Since WRES was established, challenges to how WRES is administrated have sometimes been ignored, resisted or deflected to varying degrees. It has been indicated and or implied more than once that after any year’s WRES programme has been approved by you, no deviation is possible, whether or not this is correct. It may be that the recent shake up in WRES personnel will speed progress up.
But to give a recent example of inflexible system response:
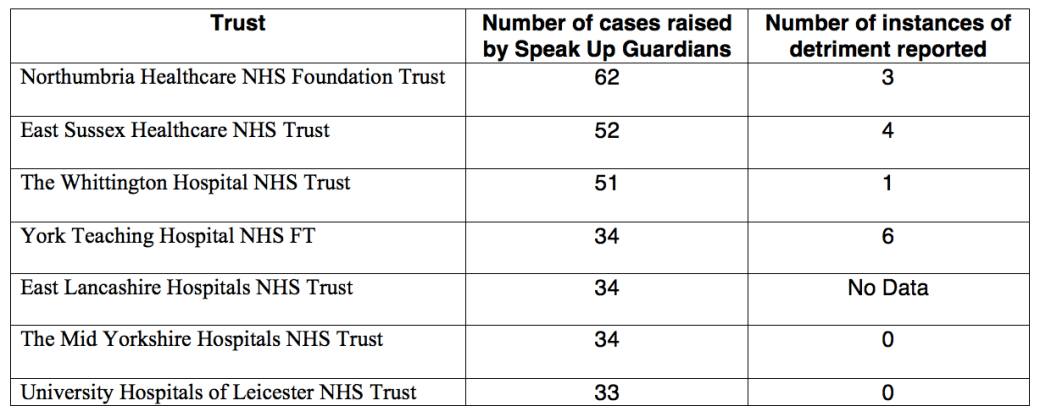
Gross bias and Race discrimination was evident from analysis of NHS Employers’ data on the appointment of Speak Up Guardians earlier this year 1 and confirmed by the National Guardian’s office subsequent analysis of its data. 2 I asked that further measures be taken, including addition of whistleblowing questions to the WRES metrics of the annual staff survey. I was told that WRES will not even consider possible changes until April 2018 at the earliest – see correspondence below. 3
This lack of urgency is a concern given the findings by Middlesex University, published in the Speak Up Review report, that BME whistleblowers are much more likely to be ignored and to suffer considerably more detriment. 4
After the last response from NHS England 3, I established for myself that the current generic whistleblowing questions in the NHS staff survey are not good at distinguishing between White and BME staff groups 5, despite the known differences in how these groups are treated. It may be that they rely too much on expectation and not on actual experience.
I do think NHS England should prioritise the better measurement of whistleblowing experience of staff in the national survey, and also include effective whistleblowing questions in the WRES metrics as soon as possible.
Most importantly, I have established that Race data is held at trust level for all questions in the national NHS staff survey and not just whistleblowing questions, and that it would reportedly cost £1200 – £1600 plus VAT to analyse the 2016 national data by white v BME scores. 6
Given this seemingly modest cost, I am surprised that this data has not already been requested and published by NHS England. This is especially as I understand the budget of millions allocated to WRES to date has not been fully spent.
Such an analysis would clearly help shine a powerful light on the shameful and still unmitigated Race inequality in the NHS. 7
I would be very grateful to know if you would authorise:
- Urgent action on ensuring that Race differences in whistleblowing are measured as part of the WRES programme
- The above Race analysis of all 2016 NHS staff survey data at trust level, similar analysis of all future annual NHS staff surveys, and the publication of such analyses.
Many thanks.
Yours sincerely,
Dr Minh Alexander
Cc
Philip Dunne Minister of State for Health
Yvonne Coghill Director of WRES Programme
Professor David Lewis Professor of Employment Law Middlesex University
Lord Adebowale NHS England NED
Prof Mala Rao NHS England WRESAG
Marie Gabriel NHS England WRESAG
Dr Henrietta Hughes National Freedom To Speak Up Guardian
Dame Moira Gibb NHS England NED and member of National Guardian’s Accountability & Liaison Committee
REFERENCES
1 https://minhalexander.com/2017/05/16/speak-up-guardians-a-whiter-shade-of-corporate-pale/
2http://www.cqc.org.uk/sites/default/files/20170915_Freedom_to_Speak_Up_Guardian_Survey_2017.pdf
3 Correspondence about Race discrimination in the appointment of Speak Up Guardians & tracking whistleblowing Race metrics:
From: “COGHILL, Yvonne (NHS ENGLAND)” <**************>
Subject: RE: Concerns about Freedom to Speak Up Guardian appointments – Race
Date: 1 October 2017 at 18:18:38 BST
To: Minh Alexander <********************>
Cc: “CE, England (NHS ENGLAND)” <****************>, mala rao <***************************>, Victor Adebowale <*****************>, *******************>, Marie Gabriel <**********************>, “NAQVI, Habib (NHS ENGLAND)” <*********************>, “WILHELM, Reg (NHS ENGLAND)” <************************>
Dear Minh,
Thank you for you e mail.
We are in the process of arranging a meeting with the National Guardian and will let you know when it will be. I will of course need to inform Dr Hughes of your request to have the meeting minuted.
With regards to the inclusion of new metrics in the WRES, we are in the process of evaluating phase 1 of the initiative and will not prior to the outcomes and recommendations of the evaluation be considering the inclusion of additional metrics in the WRES. We are hoping the evaluation to be completed by the end of April 2018.
In addition, you will be aware that Professor Dr Mala Rao is arranging a meeting to which you and other clinicians/academics will be invited, the purpose of the meeting is to discuss the WRES, research and together decide what more needs to be done in this arena.
On a final note, NHS England, the WRES team and SAG are fully committed to helping to make demonstrable, sustainable change within the system for BME staff and will continue to work towards that aim.
Kind Regards
Yvonne
Yvonne Coghill OBE
Director -WRES Implementation
NHS England
Skipton House
London SE1 6LJ
From: Minh Alexander [********************]
Sent: 29 September 2017 11:30
To: COGHILL, Yvonne (NHS ENGLAND)
Cc: CE, England (NHS ENGLAND); mala rao; Victor Adebowale; Hughes, Henrietta; Marie Gabriel
Subject: Concerns about Freedom to Speak Up Guardian appointments – Race
BY EMAIL
Yvonne Coghill
Director of WRES Programme
NHS England
29 September 2017
Dear Yvonne,
Re: Bias and Race Discrimination in the appointment of Freedom to Speak Up Guardians
Further to my letter of 19 September to the Minister of State for Health below, the Minister has informed me the WRES team will be meeting with the National Guardian’s office to
“…consider the identification of interventions that may help to improve the diversity of Freedom to Speak Up Guardians”
I wonder if it would be possible to share the minute of this meeting and any associated action plan with whistleblowers.
Also, please can you advise if NHS England is willing to include whistleblowing measures in the WRES metrics of the annual NHS staff survey, as per my request of 19 September?
Many thanks.
Yours sincerely,
Minh
Dr Minh Alexander
Cc Simon Stevens Chief Executive NHS England
Lord Adebowale NHS England NED
Prof Mala Rao NHS England WRESAG
Marie Gabriel NHS England WRESAG
Dr Henrietta Hughes National Freedom To Speak Up Guardian
From: Minh Alexander <minhalexander@aol.com>
Subject: Concerns about Freedom to Speak Up Guardian appointments – Race
Date: 19 September 2017 at 07:52:26 BST
To: philip.dunne.mp@parliament.uk
Cc: ****************, edward Jones <*****************>, Contactus England <*******************>, CE England <******************>, kate Moore <*********************>, Robert Francis, “Hughes, Henrietta” <*****************>, Dave Lewis <******************>, Yvonne Coghill <****************>, mala rao <**********************>
BY EMAIL
Rt Hon Philip Dunne
Minister of State
Department of Health
19 September 2017
Dear Mr Dunne,
Concerns about Freedom to Speak Up Guardian appointments – Race
I see that the National Guardian’s survey of Speak Up Guardians, released yesterday, has confirmed a low percentage (8.5%) of Speak Up Guardians from visible ethnic minorities. This is in accordance with my findings when I reviewed NHS Employer’s data and other sources earlier this year – see attached and previous correspondence below with Sir Robert.
This is a gross under-representation of BME staff in the NHS (at last count there were 17% non-white NHS staff and 38% non-white NHS doctors and dentists).
It is very disappointing given that research on behalf of the Freedom To Speak Up Review showed that BME whistleblowers are known to suffer greater reprisal.
This failure to appoint enough BME SpeakUp Guardians is another demonstration of the laissez-faire attitude towards and poor administration of the Freedom To Speak Up Project.
Sir Robert Francis stated in his report of the Freedom to Speak Up Review:
“I do not think it necessary to set out specific additional actions related to the raising of concerns by BME staff”
Given the latest demonstration of system bias in the form of gross under-representation of BME amongst Speak Up Guardians, I wonder if the Department of Health could review this policy and reconsider whether more specific action is needed beyond encouragement.
For example, addition of specific Speaking Up measures to the WRES metrics in the annual NHS Staff Survey.
I additionally copy this to Prof David Lewis, Middlesex University and to the NHS WRES team.
Yours sincerely,
Dr Minh Alexander
cc
Secretary of State for Health
Dame Moira Gibb NHS England NED and member of National Guardian’s Accountability and Liaison Board
Kate Moore, NHS Improvement General Counsel and member of National Guardian’s Accountability and Liaison Board
Sir Robert Francis, CQC NED and member of National Guardian’s Accountability and Liaison Board
Dr Henrietta Hughes National Freedom to Speak Up Guardian
Prof David Lewis, Professor of Employment Law, Middlesex University
Simon Stevens CEO NHS England
Yvonne Cognill, WRES Programme Director, NHS England
Prof Mala Rao, WRES Advisory Group and lead for WRES medical programme
4 Page 66 of the report of the Freedom to Speak Up Review:
http://webarchive.nationalarchives.gov.uk/20150218150953/https://freedomtospeakup.org.uk/wp-content/uploads/2014/07/F2SU_web.pdf
5 https://minhalexander.com/wp-content/uploads/2016/09/race-breakdown-of-q13-whistleblowing-nhs-staff-survey-2015-20161.pdf
6 Correspondence with the Picker Institute about NHS staff survey data:
From: Rory Corbett <***********************************>
Subject: RE: Race breakdown for question 13
Date: 10 October 2017 at 11:28:10 BST
To: Minh Alexander <**************************************>
Cc: nhsstaffsurvey <nhsstaffsurvey@surveycoordination.com>
Hi Minh,
For those analyses it would cost approximately:
1) £500-£700 (excl. VAT)
2) £1200-£1600 (excl. VAT)
The exact cost will depend on exactly what is required for each question – are you after ‘top box’ data (e.g. for q13a – the % responding ‘yes’) or data for each individual response option (e.g. for q13a – the % responding ‘yes’, the % responding ‘no’, the % responding ‘don’t know’)?
I’d also need to run this request past NHS England for approval – but I would expect there wouldn’t be a problem as no case level data is being shared.
Regards,
Rory
Rory Corbett
Senior Research Associate
Survey Coordination Centre
Picker Institute Europe
Buxton Court
3 West Way
Oxford OX2 0JB
From: Minh Alexander [*******************]
Sent: 04 October 2017 16:16
To: Rory Corbett <******************>
Subject: Race breakdown for question 13
Again, very helpful Rory, thank you.
Is it possible to say roughly how much ‘BME v White’ analyses of
1) Question 13, at trust level
2) All Questions, at trust level
for the 2016 data would cost, respectively?
BW
Minh
Minh Alexander
From: Rory Corbett <*******************>
Subject: RE: Race breakdown for question 13
Date: 4 October 2017 at 16:11:16 BST
To: Minh Alexander <*************************>
Hi Minh,
We haven’t broken down the data at trust level by white/BME for all questions – but this would be possible with the data we hold.
We do conduct additional analysis on the staff survey data for individuals & organisations but we do have to charge for our staff time in such cases.
Regards,
Rory
Rory Corbett
Senior Research Associate
Survey Coordination Centre
Picker Institute Europe
Buxton Court
3 West Way
Oxford OX2 0JB
Charity registered in England and Wales: 1081688
Charity registered in Scotland: SC045048
From: Minh Alexander [*********************]
Sent: 03 October 2017 22:19
To: Rory Corbett <*******************>
Subject: Race breakdown for question 13
Hi,
Thanks. That’s very helpful.
May I check one more thing – do you hold the trust level data, even if you don’t publish it?
Thanks,
Minh
Minh Alexander
From: Rory Corbett <**************************>
Subject: RE: Race breakdown for question 13
Date: 2 October 2017 at 15:12:15 BST
To: Minh Alexander <***************************>
Cc: nhsstaffsurvey <nhsstaffsurvey@surveycoordination.com>
Hi Minh,
If you look at this spreadsheet you will find the 2016 results for q13 for both white staff and BME staff – this is located on row 391 and 392.
The same data is available in this spreadsheet for 2015 on row 370 and 371.
Please note this is the score for staff from all organisations (including CCGs, CSUs and other small organisations that conduct the survey voluntarily).
We don’t publish this data at trust level unfortunately.
Regards,
Rory
Rory Corbett
Senior Research Associate
Survey Coordination Centre
Picker Institute Europe
Buxton Court
3 West Way
Oxford OX2 0JB
Charity registered in England and Wales: 1081688
Charity registered in Scotland: SC045048
This email and any attachments to it may be confidential and are intended solely for the use of the individual to whom it is addressed. Any views or opinions expressed are solely those of the author and do not necessarily represent those of Picker Institute Europe. If you are not the intended recipient of this email, you must neither take any action based upon its contents, nor copy or show it to anyone.
From: Minh Alexander [******************]
Sent: 01 October 2017 21:37
To: nhsstaffsurvey <nhsstaffsurvey@surveycoordination.com>
Subject: Race breakdown for question 13
Dear Sir,
Race breakdown for question 13
Can you advise me if you can provide a national overview as regards the scores for white v BME staff on the following 2016 and 2015 NHS staff survey questions?
Question 13
a) If you were concerned about unsafe clinical practice, would you know how to report it?
b) b) I would feel secure raising concerns about unsafe clinical practice.
c) I am confident that my organisation would address my concern.
Also, do you hold trust level data on white vs BME for these questions, for 2015 and 2016?
Thanks,
Dr Minh Alexander
Picker Institute Europe is a charity registered in England and Wales, registered number 1081688 and in Scotland, registered number SC045048. Registered Company number 3908160. Registered office: Picker Institute Europe, Buxton Court, 3 West Way, Oxford OX2 0JB. This email and any attachments to it may be confidential and are intended solely for the use of the individual to whom it is addressed. Any views or opinions expressed are solely those of the author and do not necessarily represent those of Picker Institute Europe. If you are not the intended recipient of this email, you must neither take any action based upon its contents, nor copy or show it to anyone.




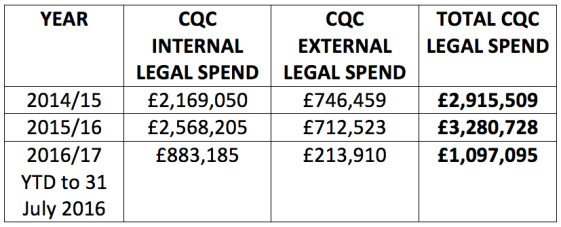
 From FOI response by NHS Protect 21 February 2017
From FOI response by NHS Protect 21 February 2017