By Dr Minh Alexander retired consultant psychiatrist 16 June 2022
| Summary: The Employment Tribunal (ET) has been very critical of governance by University Hospitals Birmingham NHS Foundation Trust (UHB) in the whistleblowing case of Mr Tristan Reuser, surgeon. Misleading, inaccurate information was given to an advisory body to justify Mr Reuser’s suspension. David Rosser the medical director, now CEO, made a misleading declaration in referring Mr Reuser to General Medical Council. Other concerns have added to governance failings identified by the ET. There are questions about whether the General Medical Council and Care Quality Commission have taken robust enough action against those who treated Mr Reuser unfairly. The GMC at least issued Dr David Rosser with a warning for making a misleading declaration to the GMC. Twenty five of twenty six GMC referrals by the trust since 2012 had medical director sign off. It is therefore important to ensure that doctors are fairly treated. The CQC is especially open to criticism because it has deemed UHB is compliant with CQC Regulation 5 Fit and Proper Persons despite the ET’s criticism of David Rosser. FOI material from the trust has revealed an apparent conflict of interest in the trust’s Fit and Proper Person process (FPPR). A non executive director who worked with David Rosser as MHPS Designated Board member, overseeing the trust’s suspension and disciplinary action against Mr Reuser, later helped to oversee the trust’s FPPR review on David Rosser’ detrimental actions against Mr Reuser. CQC also misleadingly claimed to have received an “independent” Fit and Proper Person (FPPR) review report on Rosser. However, the report was in fact jointly written by a UHB trust employee and a solicitor from a law firm that had a prior commercial relationship with the trust. When CQC was challenged, the chair of the CQC FPPR panel Rosie Benneyworth Chief Inspector of Primary Care tried to brazen it out. She has so far not accepted that CQC has done anything wrong. In response to an FOI request, CQC admitted to accepting at least three FPPR investigation reports that were written partly or entirely by NHS trust staff. CQC has also admitted that it in fact asked UHB to carry out an external FPPR review. Through hindsight goggles, CQC excused its failure to enforce acceptable practice by UHB by denying it has powers to insist that providers follow better FPPR process. This is despite numerous references in CQC’s published and internal guidance to its intention to ensure “robust” FPPR process by providers. As a small concession, CQC apologised in its FOI response for its previous misleading claim that the Rosser FPPR review was “independent”. But CQC still insisted that support to the FPPR review from a law firm which was an existing UHB supplier was “independent”. Shockingly, there is evidence that CQC was informed of the above conflicts of interest which compromised the Rosser FPPR process before the CQC decided to rubber stamp the trust’s governance. I will be making a fresh FPPR referral to CQC on the board of University Hospitals Birmingham NHS Foundation Trust and the trust’s former chair Jacqui Smith based on several matters, including the abuse of process by the trust board in asking a subordinate to determine a senior’s fitness. Natural justice and common decency would tell anyone – except it seems the CQC – that the latter is very, very wrong. Evidence of CQC’s further failures on FPPR will also be submitted to parliament. |
Background and the GMC’s findings
Mr Tristan Reuser was an experienced senior surgeon at University Hospitals Birmingham NHS Foundation Trust who the Employment Tribunal determined was unfairly dismissed after he whistleblew about patient safety issues of safe staffing and theatre cover.
The ET also found that his then medical director Dr David Rosser, now the trust CEO, made a misleading referral to the General Medical Council omitting the fact that Mr Reuser was a whistleblower. This was in contravention of GMC’s procedures to protect whistleblowers. Under guidelines produced for the GMC by former Court of Appeal judge Sir Anthony Hooper, an incorrect declaration of this sort should trigger a review of the referring senior doctor’s Fitness to Practice.
The ET’s criticism was serious and raised doubts about whether Dr Rosser made an inadvertent mistake.
| These are the relevant passages from the Employment Tribunal judgment of 8 October 2018 which raised doubt about whether Dr Rosser’s failure to inform the GMC that Mr Reuser was a whistleblower was a matter of simple oversight. “Misleading the GMC 23.1 The GMC were given inaccurate and misleading information and those failings were serious. 23.2 The respondent suggested that these failings were both inadvertent and after the decision to dismiss and hence irrelevant. However, it seems to me that I am entitled, and required, to consider all the circumstances when, for example, considering whether to draw adverse inferences in the whistle-blowing claim. It is also potentially relevant in the context of assessing the independence and neutrality of Dr Rosser. 23.3 In his referral to the GMC Dr Rosser’s failure was far more than the omission of a piece of insignificant information. He was required to address whether the claimant had raised protected disclosures and asserted positively that, “To my knowledge Mr Reuser has not been involved in any whistleblowing episode or other attempt to raise concerns within the organization.” 23.4 It may well be that Dr Rosser was unaware of the full details of the Hooper Review on the handling by the GMC of cases involving whistle blowers but, as the responsible officer, he was required to be aware of the main principles and purpose. For example: “If a doctor being referred to the GMC has raised concerns about patient safety or the integrity of the system with the organization making the referral, then the necessary steps should be taken to obtain from the organization material which is relevant to an understanding of the context in which the referral is made.” “Investigators assessing the credibility of an allegation made by an organization against a doctor who has raised a concern should take into account, in assessing the merits of the allegation, any failure on the part of an organization to investigate the concern raised and/or have proper procedures in place to encourage and handle the raising of concerns.” 23.5 In relation to that latter quote, it was not in dispute that the respondent had failed to properly investigate and respond to the claimant’s concerns. It is possible that, irrespective of any link to the reasons for the claimant’s dismissal, Dr Rosser wanted to conceal this failure. 23.6 The Hooper review continues: “Failure to answer the question truthfully would no doubt lead to the signing doctor’s fitness to practise being investigated and, if discovered during the course of the investigation, would be an important factor in assessing the credibility of the allegation.” 23.7 Dr Rosser was taken in re-examination to the GMC response to Hooper and confirmed that he believed all documents from the GMC were given to him by the GMC liaison officer. 23.8 Dr Rosser initially suggested that he must have overlooked the claimant’s whistleblowing letter when writing to the regulator. That appears surprising given that the letter was included with, and referred to in, the Claimant’s Statement of Case and emailed separately to the disciplinary panel before the hearing. It was also referred to at the hearing just 4 days before Dr Rosser wrote to the GMC. 23.9. Dr Rosser accepted that he was required to consider the documents on both sides before reaching a decision. The decision was reached and written on the same day as the GMC referral was made. Dr Rosser wrote both letters. It is unlikely, therefore, that he had forgotten the protected disclosure. 23.10. In response to this challenge, Dr Rosser’s second, somewhat contradictory, explanation was that he misunderstood the legal terminology and did not consider that the letter should be treated as a protected disclosure. 23.11 It seems to me surprising that the Respondent’s Responsible Officer would not understand what amounted to a whistle blowing episode, not least because he asserted that he had focussed on encouraging reporting of concerns. He certainly ought to have enquired about any whistle blowing episodes before making an express representation about them to the regulator. 23.12 In any event his assertion was that there had been no “other attempt to raise concerns within the organisation.” If Dr Rosser had not identified the claimant’s letter as containing protected disclosures it remains difficult to understand how he did not view them as “concerns”. 23.13 Dr Rosser has not written to the GMC to inform them that he misled them. He asserts that he told the liaison officer but there is no record of that discussion. If Dr Rosser did inform the GMC it is, at best, surprising that they did not write to Mr Reuser to inform him of the new information received, nor was there any mention of it in their findings” |
David Rosser’s referral did not result in any GMC action against Mr Reuser.
Instead, I and others referred David Rosser to the GMC for his misleading GMC referral and he subsequently received a warning on 22 July 2021 for his misleading referral.
An FOI request by fellow NHS whistleblower Maha Yassaie @Lady_yassaie has revealed that 25 of 26 of GMC referrals by UHB since 2012 were signed off by the medical director:
University Hospitals Birmingham FOI disclosure 14 April 2022 GMC referrals Request No 2141 2022/23
NB UPDATE 14 APRIL 2023 Some of the data in this UHB FOI response is inaccurate – please cross reference with this article: Bewick, the ICB, misinformation by UHB about GMC referrals and a late correction
It is important therefore that doctors are treated fairly by the medical director.
Shortly after the GMC warning, Rosser relinquished his GMC registration. This coincided with challenges to the GMC from some referrers about the veracity of the regulator’s claims that Rosser’s error in misleading the GMC was an isolated incident.
I have seen correspondence from a year prior to the July 2021 GMC warning, about an earlier concern raised with the GMC about incorrect evidence by Dr Rosser on another occasion. The individual who raised this concern with the GMC also wrote to the then UHB chair Jacqui Smith in October 2019 raising this issue and they questioned Rosser’s fitness. Smith reportedly never replied.
Another referrer had raised concern with the GMC about David Rosser signing off a incorrect declaration on maternity safety at his trust, which had to be retracted. His personal sign off was revealed by an FOI request to NHS Resolution. The incorrect declaration was amongst several made by a number of trusts, which resulted in wrongly paid discounts on insurance having to be repaid to NHS Resolution, as reported in an Independent story of 7 March 2021.
This is a screenshot from the FOI of the 2019 sign off in Dr Rosser’s name, taken from the trust’s declaration document for year two of NHS Resolution’s maternity incentive scheme:
According to the GMC’s record of the investigation hearing on 22 July 2021, David Rosser’s barrister Fiona Horlick QC argued that his incorrect declaration to the GMC:
“was clearly an isolated incident in a previous unblemished career”
The GMC record indicated that David Rosser was in attendance when this submission was made on his behalf. Did he at this point recall that he had also made a mis-declaration to NHS Resolution, a mis-declaration publicised by the press four months before the GMC investigation committee hearing? If he did, should he have disclosed this to the GMC?
Although the GMC claimed in its warning of July 2021 that David Rosser was “developing” insight, he later gave an interview to the Health Service Journal which seemed to minimise his actions in misleading the GMC. He stated in the interview:
“At the end of the day, after two and a half years of intensive investigation, the accusation was that I made a mistake on the GMC referral. I can live with that frankly, that I made an administrative error,” he added.”
University Hospitals Birmingham NHS Foundation Trust withheld damaging documents from the Employment Tribunal
UHB withheld documents which revealed that it had suspended Mr Reuser based on false information. It should in fact have given Mr Reuser the documents at the time of his suspension as a matter of policy.
The trust later failed to produce the documents during the legal disclosure process for the Employment Tribunal and it also failed to disclose the documents in response to a subject access request by Mr Reuser.
Mr Reuser only managed to obtain the revealing documents through a subject access request to the National Clinical Assessment Service (NCAS), to whom UHB had provided the false information which had led to NCAS agreeing his suspension.
The ET judge noted:
“25.1 The Respondent disclosed no documents at all from NCAS, either in
the litigation or via the SAR. Mr Reuser obtained them direct from NCAS. I was
invited to draw the inference that they were withheld intentionally.”
In the ET judge’s view, the information given to NCAS by the trust was seriously misleading:
“25.2 It appears that Dr Ryder gave NCAS seriously misleading and inaccurate information as identified earlier in my findings. This further supports my view on apparent bias and/or incompetence at a senior management level.”
UHB’s disreputable behaviour during ET proceedings resulted in a cost order for £20,000 against the trust.
Cost orders against NHS trusts are very rare. Tribunals do not like to impose costs on cash strapped public bodies.
The fact that a cost order was made represented a significant criticism of UHB.
Does the CQC which need a dictionary to understand the word ‘independent’?
Despite the specific criticisms by the original ET judgment against David Rosser regarding his reliability as a witness;
Despite his misleading GMC referral on Mr Reuser;
Despite his ultimate responsibility as medical director for the unjustified suspension and unfair dismissal of a medical whistleblower;
CQC last year typically concluded that David Rosser was a Fit and Proper Person under Regulation 5 (FPPR).
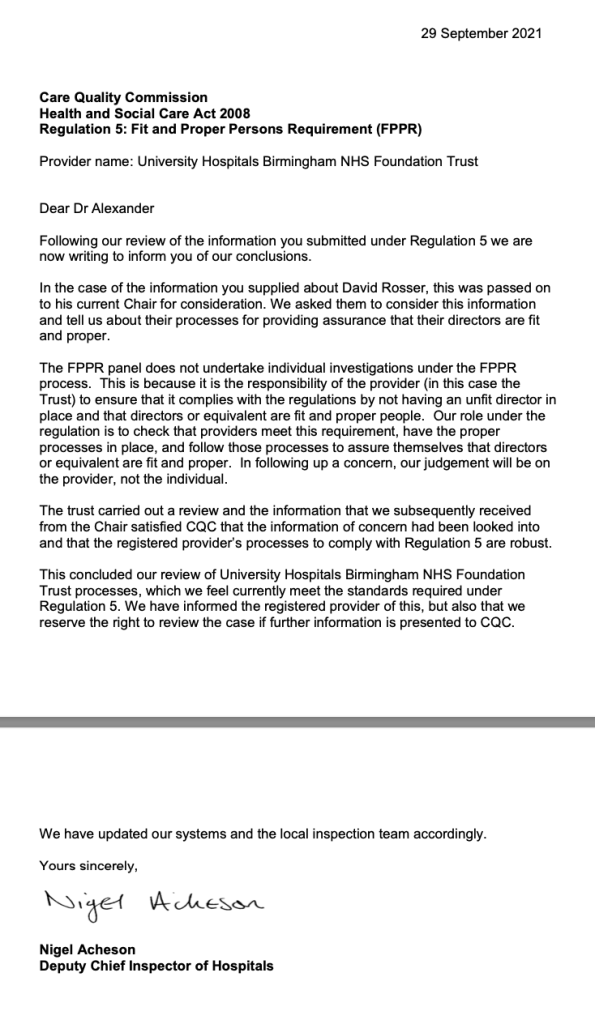
CQC accepted assurance by UHB that Rosser had been thoroughly investigated in this respect and had passed.
Because of concerns about the independence of the FPPR process undertaken by the trust, I asked CQC to confirm that it had reviewed primary documents itself and that it had satisfied itself that there was no conflict of interest in the trust’s process.
The CQC replied that it had satisfied itself that UHB’s process was sound and that its FPPR panel had received a copy of an “independent” FPPR report by two individuals, Berit Reglar and James Gutteridge.
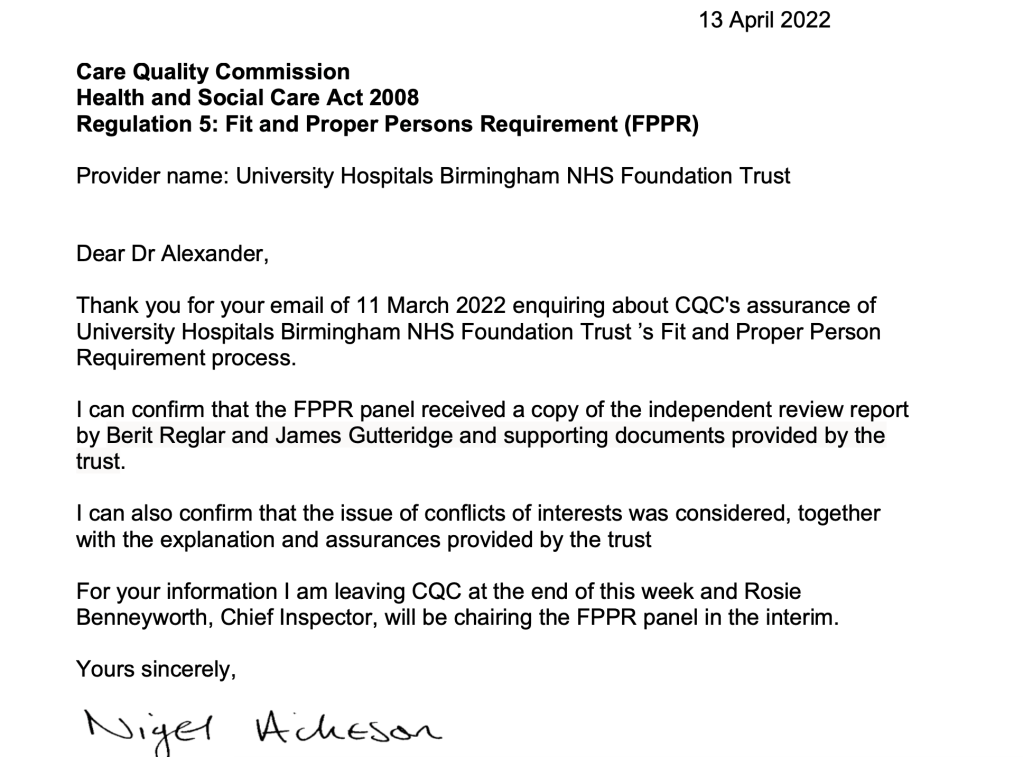
The problem with this is that, astonishingly, cursory checking revealed that Berit Reglar is a longstanding trust employee, and that James Gutteridge is a partner at Bevan Brittan LLP, a law firm that had done recent work for UHB and which in some of its promotional material had listed UHB as a “key client”.
Furthermore, I have now seen correspondence in which Berit Reglar stated that she was in joint charge of the Rosser FPPR investigation process.
When I confronted CQC about its false claim that UHB’s report was “independent”, the regulator through Rosie Benneyworth Chief Inspector of Primary Care and current Chair of CQC’s FPPR panel, firmly stuck its chin out. Benneyworth insisted that CQC had done nothing wrong. In doing so, Benneyworth appeared to tear up the CQC FPPR rule book to justify what her panel had done, claiming that CQC had no say over a trust’s FPPR process:
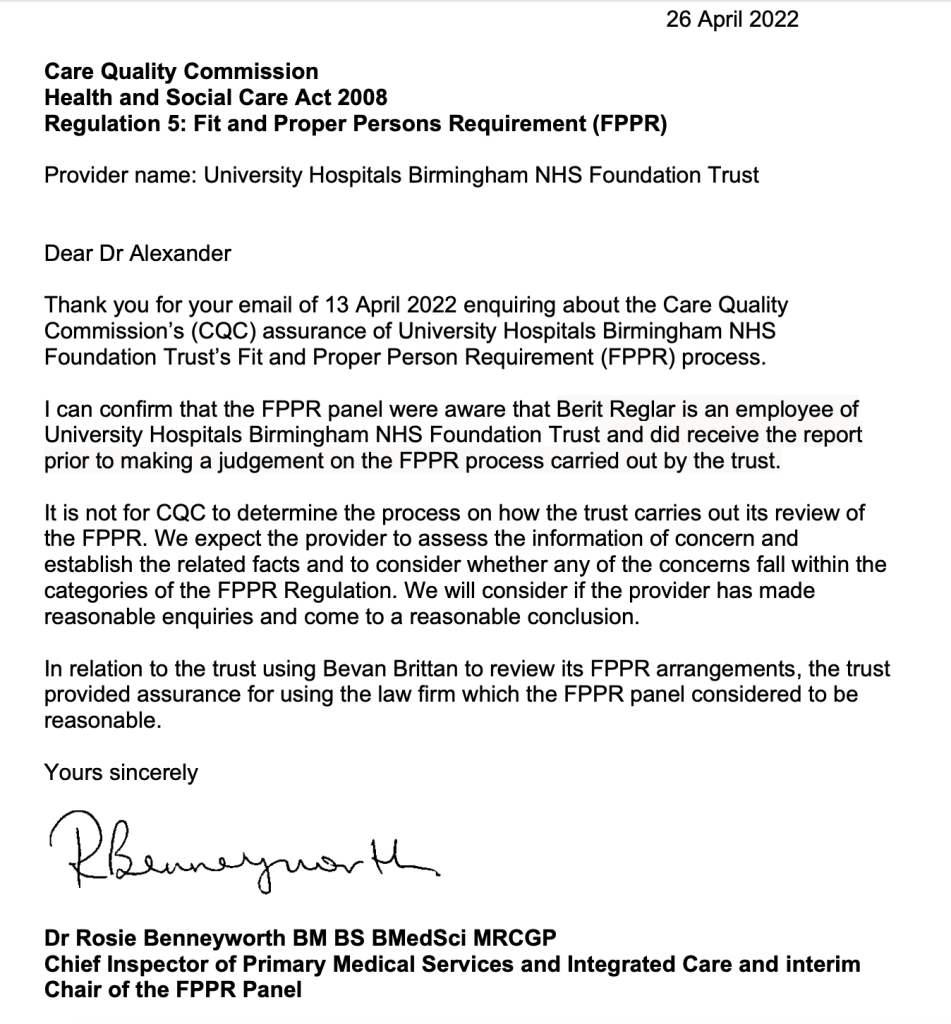
I have challenged Benneyworth’s response:
Based on past experience I imagine her letter could well have emanated from CQC’s regrettable legal department. CQC has not yet responded to my challenge.
It transpired on further checking that the CQC had been warned of the conflict of interest regarding Bevan Brittan, an existing supplier, acting as an “independent” FPPR investigator. This was before CQC shut down the FPPR.
| University Hospitals Birmingham NHS Foundation Trust spending on Bevan Brittan Oddly, although it is routine for public bodies including NHS bodies to publish details of financial transactions above £25K, the published transparency trail for UHB stops after 2017. The ICO’s records show that UHB unlawfully tried to resist an FOI request for details of spending over £25K in 2018, citing a “prevention of crime” and a “commercial interests” exemption. This is the ICO decision notice overruling UHB’s refusal: ICO Decision Notice 26 July 2019 Ref FS50810179 ordering University Hospitals Birminghan NHS Foundation Trust to disclose details of spending over £25K Why did UHB stop routine publication of this financial information? Why would it not wish to be held accountable or to allow the public to scrutinise the record for any matters of possible concern? Most recently, UHB was asked by NHS whistleblower Clare Sardari @SardariClare for information on its spending on Bevan Brittan’s services, but has failed to supply this so far, resulting in an ICO order to disclose. Strikingly, it has been alleged that UHB met David Rosser’s full legal expenses, and that a statement to this effect was made by trust officers at a governors’ meeting in July 2021. The trust has been asked to clarify if there is any basis to this allegation, and has not yet responded. |
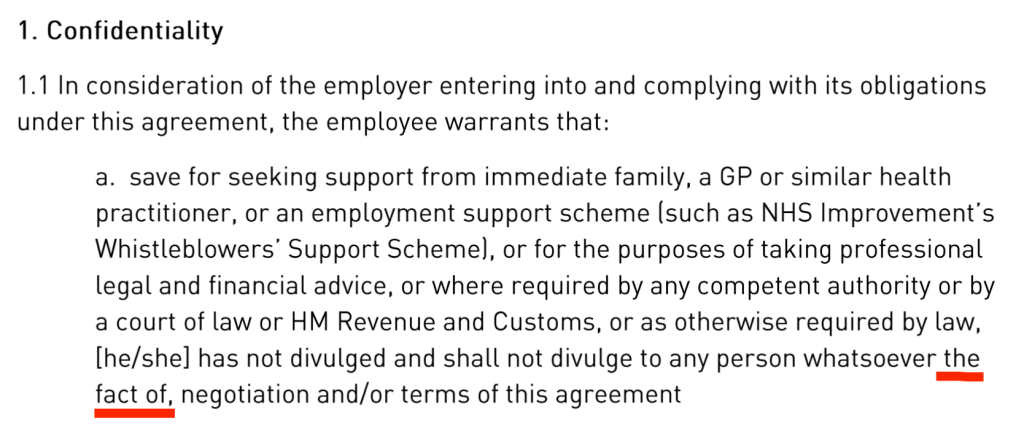
Additionally CQC had been sent evidence that the trust, through Berit Reglar the internal FPPR investigator, gave Mr Reuser false information that Bevan Brittan had no prior connection with the trust:

The loss of trust arising from this and other matters was such that Tristan Reuser decided not to take part in the trust FPPR process.
Moreover, Mr Reuser became concerned about an issue of impartiality because Berit Reglar made an incorrect assumption about him in the course of correspondence. She admitted that she wrongly assumed he had made a GMC referral:

[NB It is relevant to note here that the GMC decided to only pass a single anonymous referral to its investigators, but withheld my earlier referral on identical grounds. One possible explanation is that this circumvented the requirement to provide feedback to a named referrer.]
FOI data on CQC’s handling of FPPR
I requested update data on whether CQC had ever made a finding of breach of regulation 5 Fit and Proper Persons and to see how many of the “independent” FPPR reports CQC has accepted had in fact been written by NHS trust personnel from the very trusts under investigation.
Shocking, but no surprise to many NHS whistleblowers who are familiar with the whiff of collusion between CQC and abusive employers.
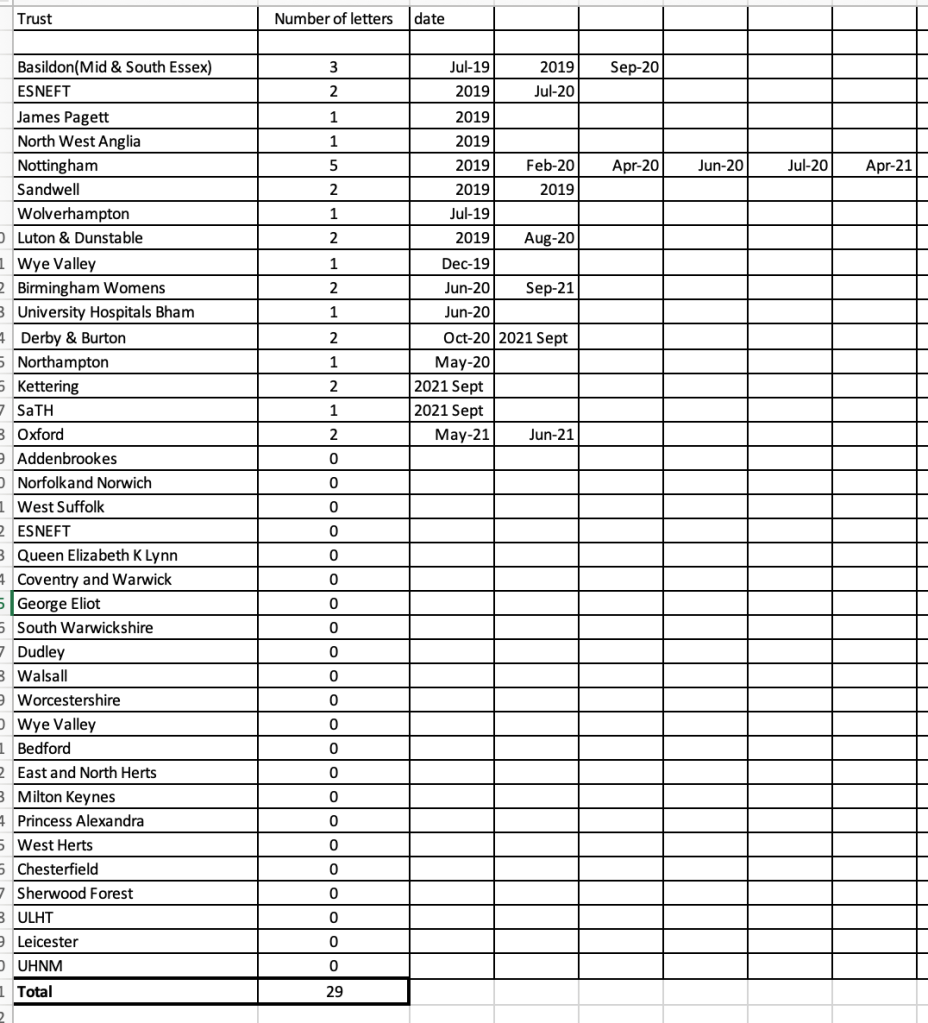
According to the FOI disclosure, CQC’s FPPR panel has accepted 95 FPPR referrals for consideration since 2014 but only 29 formal FPPR investigation reports were produced arising from this, raising questions about the rigour of CQC’s regulatory process.
The CQC claimed that three of the 29 formal FPPR investigation reports produced were authored partly or wholly by NHS trust staff, one of which would have been the Rosser FPPR investigation.
Significantly, CQC claimed that that it originally advised University Hospitals Birmingham NHS Foundation Trust to commission an external FPPR report:
“In the case of the review for the FPPR referral made for University Hospitals Birmingham (UHB) we suggested to the trust that they may benefit from an external independent review.”
CQC made post hoc excuses for not ensuring that UHB followed a suitably “robust process”, despite all its guidance, internal and published, indicating that CQC expects providers’ FPPR process to be “robust”. CQC gave these mealy mouthed excuses for letting UHB get away with a flawed and conflicted FPPR process:
“CQC are not in a position to insist on how the trust carries out their review of the fitness of an individual when an FPPR referral has been made.”
“there is scope for the trust to do a proper review without going out to someone independent.”
In UHB’s case, CQC tried to whitewash UHB’s flawed process thus:
“The trust gave their reasons for carrying out the review lead by a member of UHB staff (who is a qualified and practising solicitor) supported by an independent HR lawyer. The panel accepted that their decision was reasonable.”
CQC did at least apologise for misleading me by initially claiming that the UHB FPPR investigation into Rosser was “independent”:
“You asked if CQC reviewed any primary sources of information such as independent review reports on Dr Rosser’s fitness as a trust director (as opposed to any summarised information provided by the trust Chair) and in response to your question we referred to the Berit Reglar and James Gutteridge review as the independent review. We should have stated this was an internal review with independent support. Please accept our apologies for the error in our reference.”
Note that CQC still maintains that support to UHB’s FPPR review from the law firm Bevan Brittan, which was an existing trust supplier, was “independent”.
So conflict of interest would seem to be a highly plastic concept in the CQC-verse.
Cutting through all of CQC’s self interested squirming, CQC has had the power all along to force NHS trusts to remove unfit directors if it pleased.
It has simply chosen not to do so.
FOI data from University Hospitals Birmingham NHS Foundation Trust on the FPPR process on David Rosser
The trust did not respond to an FOI on this issue despite several reminders, including to its Chair, until ordered to do so by the Information Commissioner.
In a response of 6 June 2022, the trust disclosed terms of reference of September 2020 which showed the FPPR review into David Rosser was conducted because of:
- The dismissal of Mr Reuser and the related ET findings against the trust and David Rosser
- Allegations concerning MHPS process and GMC referral of another individual
The terms of reference stipulated that it would be an internal process supported by an external lawyer.
Importantly, UHB stated that the terms of reference were drafted by David Burbridge the trust’s Chief Legal Officer, “with CQC input and approval”.
There was also a letter from the trust Chair Harry Reilly responding to some concerns and questions that I had raised, which contained data that I had requested.
In this letter Harry Reilly responded to my concern that the trust had not recognised what a grave step a GMC referral was, in relation to ET criticisms of trust process. Reilly maintained that referral to the GMC “should not be seen as a punitive measure”.
This is so devoid of empathy that it is hard to comment on. There is no acknowledgment here of the damage done to doctors, regardless of intent.
Doctors have died of suicide and suffered acute illness such as heart attacks and strokes whilst under GMC investigation. After the GMC’s recent bizarre pursuit of Dr Arora over trivia, Chaand Nagpaul the BMA Chair went to war on the dysfunctional GMC process, calling for radical reform with the comment:
“Being notified and being investigated by the GMC can be one of the most traumatic experiences in a doctor’s life”.
But the rigid, stonewall attitude by UHB perhaps explains why it has kept digging itself into HR holes and does not seem to learn.
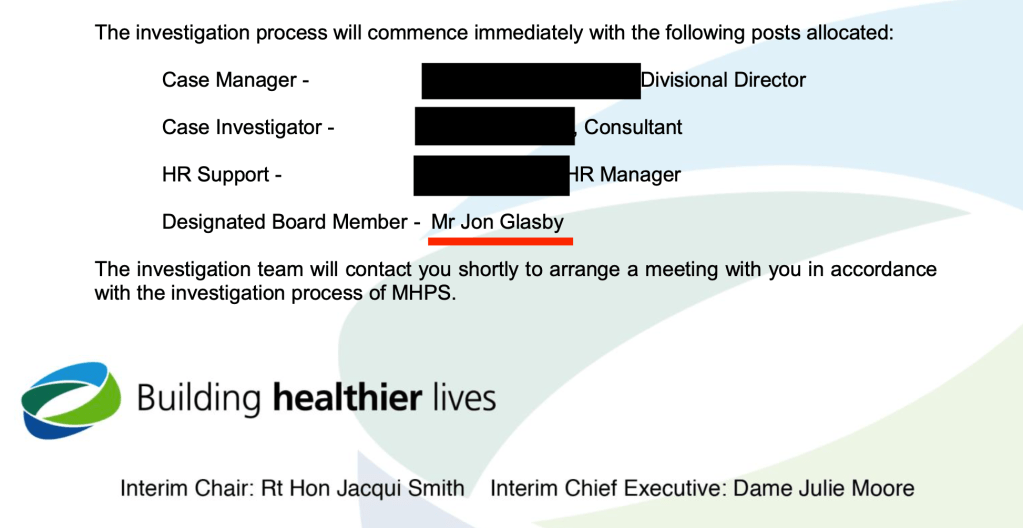
In addition, the trust claimed to me in its FOI response that there was no known conflict of interest in its FPPR process on David Rosser. However, the FOI response revealed that one of the trust’s non executive directors, Jon Glasby a social worker by background, acted as a support to the former trust Chair Jacqui Smith in the Rosser FPPR process:

This raised an additional issue of conflict of interest because Glasby had previously worked with David Rosser (then as Medical Director) to oversee the trust’s suspension of and disciplinary action against Tristan Reuser, in Glasby’s capacity as MHPS Designated Board Member:
The apparently incorrect denial of conflict of interest in a statutory disclosure under FOIA has to be noted as another example of the trust providing unreliable information.
I have written to Harry Reilly trust chair to ask for the trust’s response to the apparent conflict of interest concerning Jon Glasby. There has been no response so far.
And should the CQC have detected this clash when it assessed the soundness of the trust FPPR process?
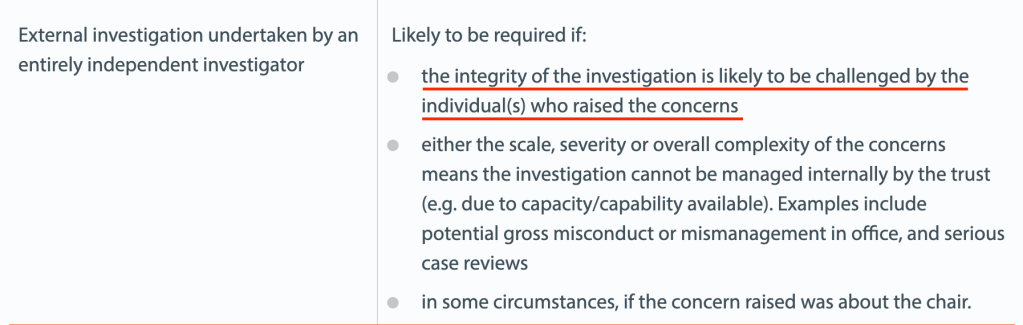
The trust maintained in its letter of 6 June 2022 that it adhered to NHS Providers’ guidance on FPPR. This is debatable given that NHS Providers’ criteria for triggering a fully external FPPR review is contentiousness. In the context of the Reuser litigation, that would seem to be fulfilled. Also, if the whistleblower at the centre of the matter did not have confidence in the process and had already withdrawn, the process had de facto been disputed.
Shockingly, I have now seen correspondence which shows that the CQC was informed that Jon Glasby was inappropriately involved in the Rosser FPPR review, BEFORE CQC decided to accept the trust’s FPPR evidence as satisfactory.
Separate to this, Mr Reuser wrote to Jon Glasby himself in November 2020, after the conclusion of his case in both the ET and the EAT. He asked if Jon Glasby had been kept properly informed of trust actions under MHPS, in the light of the ET and EAT’s serious criticisms of his suspension by the trust.
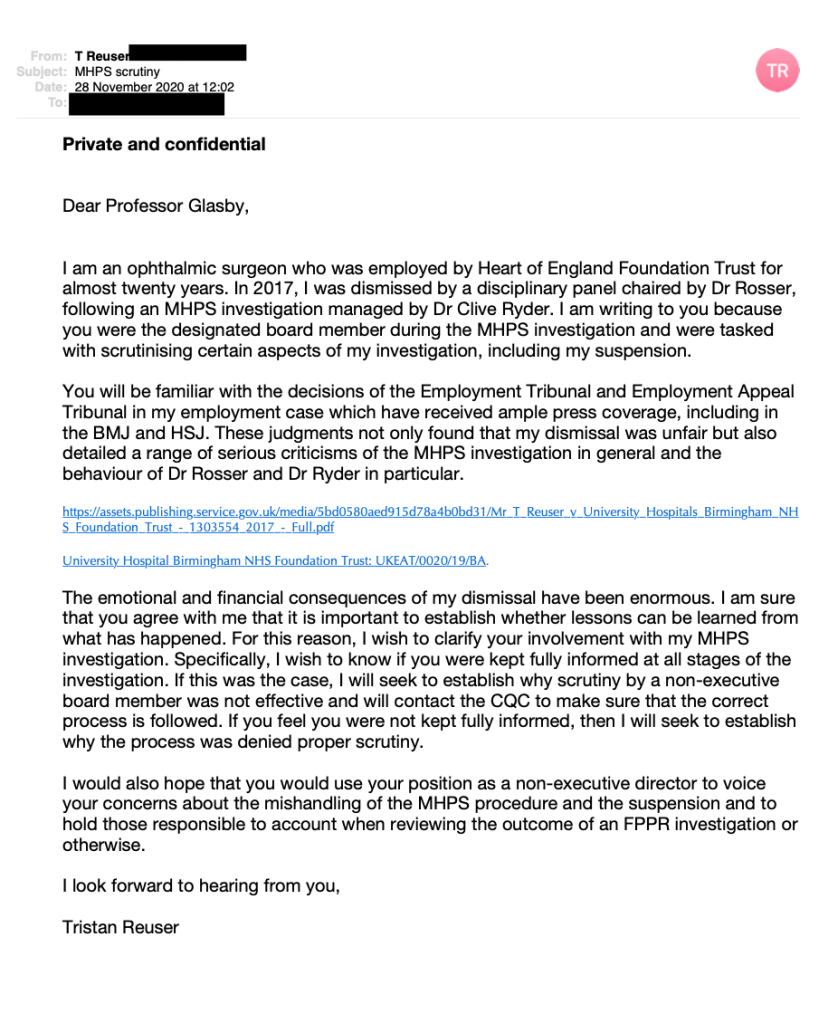
Glasby reportedly never responded to this letter. But by this point, the trust had drafted the terms of reference for the Rosser FPPR review. Did Glasby fail to respond to Tristan Reuser’s letter because he had already been appointed to the Rosser FPPR process and was conscious of the tension arising?
Trust learning from the Reuser case
UHB seem to have taken a cherry picker’s approach to the NHS Providers’ guidance on FPPR. This guidance emphasised the importance of retaining public confidence and it recommended publication of the outcome of FPPR investigations. It is unclear whether UHB has ever done so. I have asked Harry Reilly UHB chair to clarify if a summary outcome was ever published, and it not, whether the trust intends to publish a summary.
A previous enquiry that I made to the former trust chair Jacqui Smith about trust learning was repeatedly ignored. The trust eventually cursorily admitted in a seven month overdue FOI disclosure of 30 March 2022 that some level of wrongdoing was acknowledged, as board training was undertaken:
“The Trust has reflected upon the errors made in relation to the disciplinary process concerning Mr Reuser and the subsequent Employment Tribunal and has undertaken related training with all Board members, including the Trust’s current Responsible Officer (RO). This includes consideration of all relevant factors and advice when making a referral to the GMC.”
The reluctance to admit even this is not reassuring evidence of genuine learning or a change in attitude by the trust board. And there is no note of empathy.
I will be re-referring the UHB trust board and its former chair Jacqui Smith, now chair of Barts Health NHS Trust and Barking, Havering and Redbridge University Hospitals NHS Trust to the CQC under FPPR. This will include grounds of what I believe is the serious abuse of process in instructing a subordinate to determine the fitness of a senior. Although CQC is hardly fit to adjudicate given its part in rubber stamping UHB’s impropriety in its FPPR process.
Overall, the whole matter may look to some like CQC collusion with the trust.
How many other FPPR referrals have been processed in this shady way by the CQC, behind closed doors?
Ultimately, the ongoing evidence of CQC failure on FPPR will be submitted to the relevant parliamentary committees.
The regulation of NHS managers
If we revisit the original reasons for FPPR – the horrors of MidStaffs – and we contrast this against CQC’s obvious inaction, the question arises of what patient harm has CQC enabled in the last eight years of FPPR non-enforcement, in concert with cover ups and poor quality management of the NHS?
It has been a decade since the MidStaffs public inquiry, and the senior ranks of the NHS have continued to fiercely resist accountability, let alone regulation. The senior NHS ranks have been increasingly stuffed with government cronies, many of whom are financiers with little obvious connection to healthcare.
Instead of accountability, we see endless, incestuous recycling of the same individuals, revolving between provider and regulatory bodies, and sometimes the Department of Health. Shaking hands with a knowing wink as they keep swapping seats.
| An example of CQC’s troubling proximity to the providers that it is supposed to regulate, and the fast-spinning CQC revolving door Ellen Armistead was CQC Deputy Chief Inspector of Hospitals CQC disclosed that she chaired the CQC’s FPPR panel between February 2016 and June 2019 Armistead left CQC in June 2019, and became Chief Nurse and Deputy Chief Executive of Calderdale and Huddersfield NHS Foundation Trust in July 2019. |
The Kark review report on managing NHS managers’ fitness was carried out four years ago but remains unimplemented. Kark stopped short of full regulation but did recommend a central database and a barring mechanism, with full future regulation if these initial partial measures were not enough.
When I enquired again for the umpteenth time recently, I was told that there were still no implementation terms of reference to share with me because the work on the Kark report was still at an early stage – after four years!
A telephone meeting was held with NHS England/Improvement on 18 May 2022 and brief meeting minutes have now been agreed. It was revealed that there had not been Ministerial authorisation to go ahead with Kark implementation, but that was anticipated. A question about whether the Kark register will be retroactive has not so far been answered. If not, some will doubtless be pleased to delay the register’s establishment for as long as possible. It is anticipated that it will be at least a year before any Kark database is operational.
In the meantime, the odd report of the Messenger review of NHS and social care leadership which seems to come with no supporting evidence or references, has been published to a tepid welcome.
If patients are to be effectively protected, and frontline clinicians given the proper professional independence to care for them, the senior NHS management cabal must be tackled.
So of course must be the malign political influence of the Department of Health which sits at the apex of the pyramid of bullying and suppression.
| Another example of the CQC revolving door Mike Richards was a former CQC Chief Inspector of Hospitals who chaired CQC’s FPPR panel between December 2014 to February 2016. He personally shut down the FPPR referral on the notorious Paula Vasco Knight who was recycled back into the NHS with the help of Monitor despite an ET finding of whistleblower reprisal. Richards was severely embarrassed when she was shortly after charged with a criminal fraud. Upon his retirement from the CQC Richards was rewarded with a seat as a non executive on the Department of Health and Social Care’s board. He also took up some positions in the private sector with PwC and Incisive Health. |
UPDATE 11 DECEMBER 2022
Since the above was published, UHB’s performance continued to give cause for concern.
UHB’s CEO and Chair resigned.
BBC Newsnight has commenced an investigation into the trust.
Dozens of UHB staff have also contacted Preet Gill MP Birmingham, Edgbaston with concerns about poor culture.
I have made transcripts of two Newsnight interviews with proponents of the awful Freedom To Speak Up project, and of a revealing BBC interview with the UHB Freedom To Speak Up Guardian:
Under the microscope: The Freedom To Speak Up model and University Hospitals Birmingham
What the UHB Freedom To Speak Up Guardian told the BBC
I have also written to the new interim Trust Chair to challenge leaked internal trust communications which implicitly denigrated current and former staff who have spoken to the BBC:
Letter to Yve Buckland interim UHB Chair 11 December 2022 about unfortunate messaging by trust board
UPDATE 16 DECEMBER 2022
I have come across data which suggests that UHB’s above FOI disclosure of April 2022 about the outcomes of its GMC referrals was incorrect.
I have written to the interim Chair Yve Buckland requesting clarification.
Letter to Yve Buckland UHB interim Chair 16 December 2022
PETITION
Please click and add your signature to this petition to reform UK whistleblowing law – whistleblowers protect us all but weak UK law leaves them wholly exposed and it is a threat to public safety
Replace weak UK whistleblowing law and protect whistleblowers and the public
RELATED ITEMS
Is there a ‘club culture’ at the heart of the NHS’s quality regulator?
Whistleblowers have continued to emerge at UHB:
Multiple whistleblowers flag ‘heartbreaking’ incidents at major trust
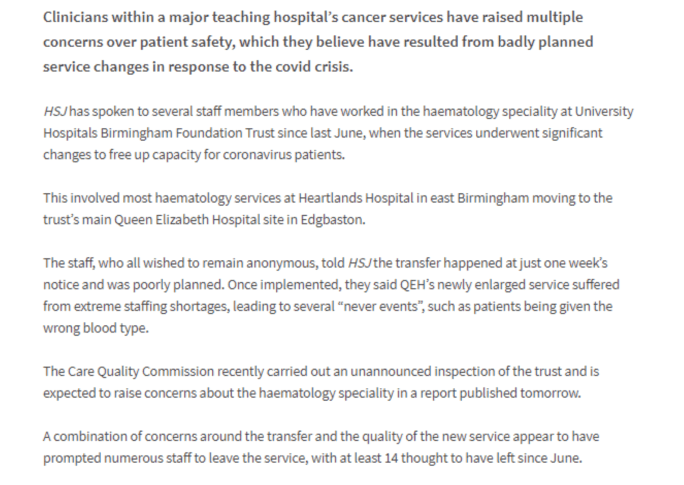
A FIFTH never event of the wrong type of blood given has just been reported at UHB:
Major trust records fifth never event at troubled department
University Hospitals Birmingham NHS Foundation Trust also made the headlines on 5 June 2022 because of reportedly poor treatment of doctors in training in obstetrics and gynaecology, requiring regulatory intervention:
Trainee doctors in ‘meltdown’ at major hospital maternity department
Based on Tristan Reuser’s case and others, NHS Resolution agreed that NCAS’ successor body will consider safeguards against being fed false information by unscrupulous employers:
In true NHS musical chairs style, it was announced on 7 June 2022 that Rosie Benneyworth current chair of the CQC FPPR panel is being posted to HSIB:

Dr Rosie Benneyworth appointed interim Chief Investigator
“We know that most people get good care in the NHS, but sometimes they don’t get the outcomes they need or things go wrong. In these circumstances, it is vital that as a system we reflect and learn from these events to improve the safety of care”
“Rosie takes up her post with HSIB on 1 August 2022.”
Let us hope that Benneyworth does not take to tearing up any rule books at HSIB.
A particularly gross example of CQC conflict of interest and failure on FPPR was when it passed its notorious former Chair Jo Williams as a Fit and Proper Person, removing obstacles to her recycling back into the NHS fold:
Jane Archibald’s shocking whistleblowing case about a cover up of an unqualified assistant being allowed to run epilepsy clinics and vary complex epilepsy medication featured a failure by her former CEO Stephen Eames to respond to her disclosures. He simply did not respond to her correspondence. NHSE/I has been asked to review his suitability for his current post as CEO of the Humber region ICS.
Dr Jasna Macanovic’s recent NHS whistleblowing case adds to the pile of managerial recycling scandals. John Knighton the medical director found by the ET to be centrally involved in her premeditated unfair dismissal has been protected by the trust and Mark Cubbon the trust CEO who failed to ensure her protection as a whistleblower has been promoted to a senior post at NHS England.
An FPPR referral has now been made arising from the executive failures in this matter.
The Flexible CQC, FPPR & Kettering General Hospital NHS Foundation Trust\
Sorry is the hardest word: CQC, Paula Vasco-Knight and Regulation 5 Fit and Proper Persons
Steve Trenchard, NHS regulators & FPPR
FPPR: CQC has lost all moral authority, but what will the National Guardian do?
Postscripts on Paula. NHS England’s apologia & regulatory reticence