Dr Minh Alexander retired consultant psychiatrist 24 July 2023
This is a post to share correspondence to the Information Commissioner about a stubborn failure by NHS Resolution to fully disclose data on personal injury claims by NHS staff during the years since the pandemic started.
NHS Resolution has been handling personal injury claims by NHS workers affected by long COVID, but claimed it could not provide data about this, because it had no specific code for long COVID.
When asked to disclose data on all claims spanning the pandemic years, under all existing codes, NHS Resolution bizarrely cherry picked and supplied data relating to only a few injury codes.
It has prevaricated and delayed in supplying the withheld information, which includes claims which fall under codes such as “breathing difficulties”, sensory loss and “brain damage”.
I have referred the matter to the ICO.
The correspondence is below. The headline figures quoted from NHSR in the appendix relates to the period 2018/19 onwards. (Pre-pandemic years were included in the request for comparison).
BY EMAIL
Information Commissioner
24 July 2023
Dear ICO,
Failure by NHS Resolution to provide information about NHS staff personal injury claims during the pandemic
I have been trying to seek out information about how long COVID has affected the NHS workforce.
This is information of substantial public interest for a number of reasons.
Firstly, the government and NHS oversight bodies have indicated that they have not been collating data on the scale of harm to NHS staff from long COVID, which seems a negligent omission.
The infection of NHS staff and resulting significant disability is a reflection on infection control processes, and the government should be recording all relevant information in order to learn from the harm and to mitigate risks.
The scale of harm is a basic starting point in evaluating matters.
I therefore approached the matter from a different angle, and asked NHS Resolution on 6 March 2023 to provide me with data on all personal injury claims by NHS staff under all existing injury codes for a period spanning the COVID pandemic and the two years prior to the pandemic for comparison.
Inexplicably, NHS Resolution provided me with data on only some of the personal injury claims by NHS staff in the period in question.
NHSR limited its response to a small selection of its injury codes, and failed to disclose data relating to claims under the rest of the injury codes.
It offered no valid legal grounds for exemption of disclosure under FOIA with respect to the information that it had withheld.
When I challenged this, including with information from past FOI disclosures by NHS Resolution which showed that it held data relevant to the omitted injury codes, NHSR apologised on 10 May 2023, claimed that it was seeking advice from “subject matter experts” and indicated that it would provide me with a substantive response within two weeks.
Since then, NHSR has repeatedly failed to provide the missing data and despite further unreliable promises to do so:
NHSR email 30 May 2023:
“We hope to provide you a substantive response within 2 weeks”
NHSR email 19 June 2023:
“We hope to be able to provide you with a response by the end of next week”
I should point out that all this is very uncharacteristic behaviour by NHS Resolution, which is usually punctilious in responding to FOI requests.
I do not think it is reasonable wait any further, especially as all coded information is electronically accessible and there should be no reason why NHS Resolution could not have provided the requested information, in full, much sooner.
I would be grateful for the ICO’s help in accessing the missing data.
In the appendix below, I set out the injury codes for which NHSR has provided personal injury claims data, and the remaining injury codes for which NHSR has still provided no claims data.
The correspondence with NHSR, including the original FOI request on is forwarded below.
Many thanks and best wishes,
Dr Minh Alexander
Cc Helen Vernon CEO NHS Resolution
Baroness Heather Hallett UK COVID inquiry
APPENDIX
NHS Resolution has provided data on personal injury claims made NHS staff which fall under the following codes:
Orthopaedic Injuries
2,403
Psychiatric Damage
372
Facial Injuries
199
Head Injuries
185
Injuries to Internal Organs
96
Burns
51
Damage
50
Sickness/Disease
45
Injuries affecting the senses
33
Other
24
Fatality
15
Scarring (Except Facial)
12
Unknown
#
Damage to Hair
#
NHS Resolution has failed to provide data on personal injury claims by NHS staff which fall under the following codes:
Dr Minh Alexander retired consultant psychiatrist 22 July 2023
I am unable to do this serious matter justice and am posting in summary to share a recently published report on a surgical scandal at Salford Royal Hospital, which is now part of the Northern Care Alliance NHS Foundation Trust:
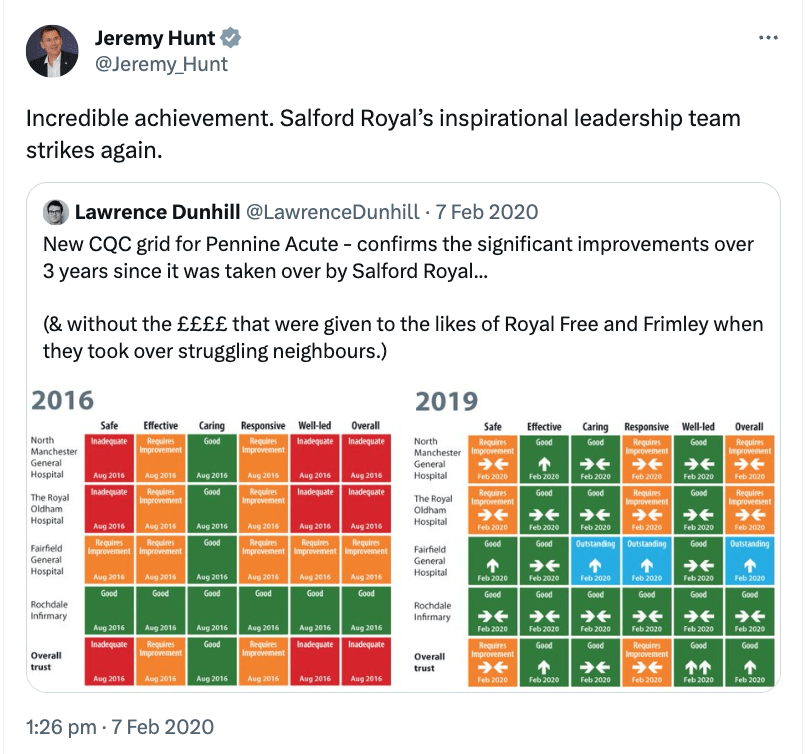
The trust’s predecessor body the Salford Royal NHS Foundation Trust was for some years practically deified by regulators as an exemplar of unimpeachable safety practice. It was one of several trusts used by Jeremy Hunt as a rod with which to batter struggling, under resourced NHS trusts.
In August 2014 an anonymous whistleblower raised concerns with:
– The trust (in predecessor form, as the then Salford Royal NHS Foundation Trust)
– The General Medical Council
– Robert Francis
– The Care Quality Commission.
The “look back review” stated:
“In August 2014, an anonymous whistleblower contacted Salford Royal NHS Foundation Trust (now known as the Northern Care Alliance NHS Foundation Trust), General Medical Council (“GMC”), Care Quality Commission (“CQC”) and Sir Robert Francis then QC, now KC, (a barrister who has chaired several high-profile medical inquiries) with concerns about Consultant Spinal Surgeon A. The letter from the anonymous whistleblower described a number of areas of concern relating to Consultant Spinal Surgeon A’s behaviour, conduct, probity and capability.
“Finally, I am announcing an independent review into creating an open and honest reporting culture in the NHS chaired by Sir Robert Francis QC, who chaired the landmark inquiry into the poor standards of care in Mid Staffordshire NHS Foundation Trust. The review is being established to provide independent advice and recommendations on measures to ensure that NHS workers can raise concerns with confidence that they will be acted upon, that they will not suffer detriment as a result and to ensure that where NHS whistleblowers are mistreated there are appropriate remedies for staff and accountability for those mistreating them. The review will consider the meritsand practicalities of independent mediation and appeal mechanisms to resolve disputes on whistleblowing fairly. It will do this by listening to and learning the lessons from historic cases where NHS whistleblowers say they have been mistreated after raising their concerns and by seeking out best practice.”
It is reasonable to surmise therefore that the anonymous whistleblower disclosed to Francis personally in expectation of a best practice system response to their concerns.
According to the just published report, what followed was that the surgeon was dismissed in January 2015.
It was not until September 2015 that the trust invited the Royal College of Surgeons to review possible harm to patients:
“In September 2015, the Trust contacted the Royal College of Surgeons to request an Invited Service Review of the Trust’s spinal surgery service and to undertake a clinical review of 10 clinical records relating to patients at the Trust who had been under the care of Consultant Spinal Surgeon A1.”
The RCS reportedly found no substantive concerns:
“…there were no overall concerns about the standard of care provided to the patients that formed part of the review, although a series of complications were acknowledged. From the information present in the clinical records, it appears that the way in which the complications were managed once identified was appropriate in each case.”
Crucially, it appears there was more whistleblowing at the trust in 2016, which was not acted upon:
“In 2016, an internal request was made to review 17 patients to determine if any required either a clinical follow up or an appointment to determine possible preventable harm. The SPSLBR has been unable to determine if this progressed as the review did not follow the usual governance processes and at the time of producing this report, it has not been possible to determine why this was the case.”
FIVE years later, processes were finally established to review patient harm:
“In 2021, a multi-professional staff support group was established under the Trust’s Freedom to Speak Up process which raised new questions and concerns around the conduct, probity and capability of Consultant Spinal Surgeon A whilst they were employed by the Trust. This group raised concerns directly with the Trust Chief Executive and following this, the concerns were triangulated, leading to the realisation that clinical notes cannot be taken as accurate and correct, and emerging themes were identified with specific concerns around Consultant Spinal Surgeon A’s conduct, probity and capability whilst they were employed by the Trust. As a result, in January 2022, the Trust commissioned the SPSLBR Investigation Group to investigate these concerns.”
Why had concerns not been “triangulated” before, to reveal that the patient records were not reliable?
Did CQC and Robert Francis diligently ensure that the original 2014 whistleblower’s concerns were properly addressed?
Did CQC and or Francis receive any further disclosures, and if so, what did they do about them?
In 2018 when CQC renewed Salford Royal Hospital’s rating of “Outstanding”, it nevertheless noted some warning signs about whistleblowing governance in surgical services:
“Not all staff were aware of the role or purpose of the Freedom to Speak up Guardians, there was some concerns about the culture in theatres.”
“Whilst most departments felt supported and valued by the executive team and senior managers, some departments did not feel recognised by their peers, for example, in oral surgery. The oral surgery department had recently accessed the Freedom to Speak Up service resulting in the division undertaking a full comprehensive review within oral surgery that was going to be presented nationally”.
The trust’s external “look back review” also identified what it considered to be culture of low reporting in the spinal surgery service:
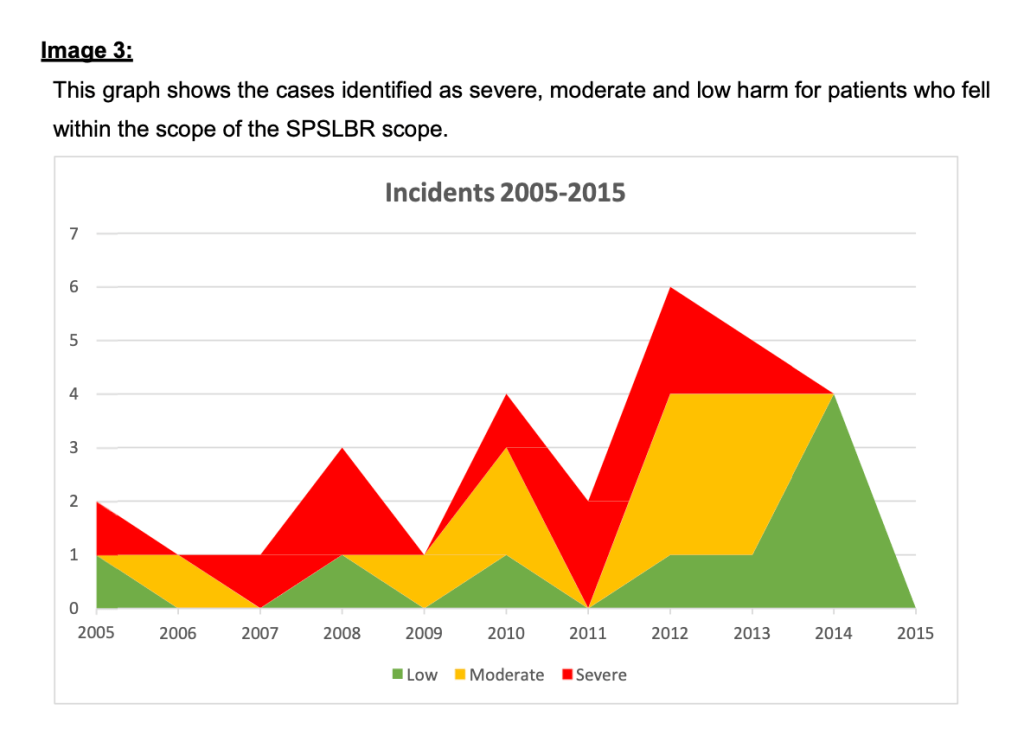
“The SPSLBR identified that there was a culture of low reporting of spinal surgical incidents within the timeframe of cases considered.”
Is this something that the CQC should have identified and followed up?
The review also concluded that there was both moderate and serious patient harm over a ten year period:
Robert Francis recommended in his report of the Freedom To Speak Up review that patients harmed by failures to manage NHS whistleblowing properly should receive redress.
Yet his model neither worked efficiently nor quickly at Salford, despite the claims that the organisation had better than average culture.
Also, until 22 December 2022, the CQC continued to rate Salford Royal Hospital as “Outstanding”.
David Dalton the CEO of the Salford Royal NHS Foundation Trust, and then the Northern Care Alliance NHS Foundation Trust 2001 to 2019, was a powerful and much feted NHS CEO.
He authored the 2014 Dalton Review for Jeremy Hunt, advising on how NHS improvements could be made. It is full of “transformation”, “ambition”, “transaction” and suggestions for how successful organisations should be allowed to “expand their reach and have greater impact”.
Importantly, Dalton was part of a group selected by Jeremy Hunt to work on the details of the Legal duty of Candour, which arose from Robert Francis’ Mid Staffs public inquiry recommendations. According to this briefing by AVMA Dalton advised as follows:
“Their report recommends that moderate as well as serious injury, or death, should be included in the new statutory duty of candour that the Government is about to introduce.”
Dalton’s joint report with Williams on Duty of Candour can be found here.
Status and hierarchy are often unhealthy in healthcare
Sirs and Dames, long letters after your name, friends rewarding friends and backscratching, beget incestuousness and circularity.
It can also impede accountability or give false assurance.
The look back review has noted:
“During the Trust’s Consultant Spinal Surgeons’ discussions with patients, a theme emerged that patients specifically sought out Consultant Spinal Surgeon A due to them holding senior roles in national professional bodies in the spinal surgical field. The patients’ interpretation of them holding such roles was that this demonstrated their clinical ability and that they were one of the leading surgeons in their field. These were non-elected roles. It is recommended that a copy of this SI report and action plan will be shared with those organisations where Consultant Spinal Surgeon A held senior roles and with their current Responsible Officer.”
Dr Minh Alexander retired consultant psychiatrist 20 July 2023
Summary: A BBC Newsnight investigation into the Good Governance Institute a private company which employs a sacked former NHS director has resulted in Companies House writing to the company to ask it to stop using a name for which it apparently had no prior approval. The word in contention is “institute”, which may not be used without permission from the Secretary of State for Business. The use of this name is usually reserved for bodies which conduct high level research or are professional bodies of the “highest standing”. Companies House has advised the BBC that use of the name “institute” without prior permission is an offence. Other concerns were unearthed. I have asked NHS England to consider whether it wishes to review whether this is a company with which the NHS should have any links.
This arose from Newsnight’s investigation into the governance and patient safety failures at University Hospitals Birmingham NHS Foundation Trust (UHB), where the GGI has been involved.
Of concern, UHB was repeatedly and favourably assessed by external reviewers, including the GGI, despite significant issues.
The review found no major concerns. The BBC concluded that there was no evidence that the GGI did anything wrong, but the remit of the review was too limited.
BBC Newsnight raised a question about the narrow scope of these types of well led reviews, which clearly do not always identify important problems, yet cost the public purse dear. In the case of the UHB, the GGI’s bill was reportedly £72,000 for the well led review and other services.
The BBC reported that the Good Governance Institute does not have permission from the Secretary of State, and that the GGI’s chief executive Andrew Corbett-Nolan instead registered a shell company in the Irish Republic under the name “Good Governance Institute”, where no special permission is needed to use the word “institute”. According to the BBC’s company research, this entity appears to have no assets, no staff and seems to conduct no business.
But is it within the rules for a UK company to use a trading name that includes the word “institute” if there is no permission from the Secretary of State?
It seems it is not: The government rules apply to any names under which someone carries on business:
Companies House told the BBC that it is an offence to use the term “institute” without prior approval, and they have written to the GGI to ask it to stop using the term.
Companies House also indicated that the registration under the name “institute” in another jurisdiction had no bearing on the matter.
The GGI responded:
2. The GGI’s chief executive used a title of “professor” based on a visiting rather than a substantive professorial post, and that he continued to use the title “professor” after the end of his time-limited, visiting position at the University of Chester.
Following Newsnight’s enquiries, Mr Corbett-Nolan stated that he had not been informed that his visiting professorship had ended, and he removed the title of professor from his website.
3. The GGI’s CEO had been previously repeatedly and publicly wrongly described as “Dr” in a number of GGI documents and other documents, when he did not hold a doctorate.
A colleague from the GGI had also previously been wrongly described as “Dr” when he only held a bachelor degree.
Andrew Corbett-Nolan explained this as error and confusion by others:
Andrew Corbett Nolan commented to Newsnight that Mr Fitzgerald was “talented and experienced”.
He also commented to Newsnight that most clients were happy to receive services from Mason Fitzgerald:
This appears to imply that Mason Fitzgerald may well be working for some NHS bodies, despite his previous dismissal by East London NHS Foundation Trust.
Mason Fitzgerald commented to the BBC:
NHS England has to date refused to confirm or deny that it hired Mason Fitzgerald to work on ICS governance AFTER his false qualification claim was discovered and he was sacked by East London NHS Foundation Trust.
“An NHS England spokesperson said: “Any money spent by the NHS on third parties for their expertise is scrutinised in accordance with our Standard Financial Instructions and in line with public contracting regulations.
“The funding cited as spent by NHS England and Health Education England adhered to these standards, while procurements led by other NHS organisations would have been managed at local and regional levels.”
Although NHS England emphasised in its most recent correspondence that it had checked its contracts and could confirm that it had no current contracts with the GGI, it did not actually say it would not hire the GGI again in the future.
Will the further investigation findings by Newsnight make any difference, or will NHS England start hiring the GGI again when the fuss has died down?
I have asked Amanda Pritchard about her plans regarding NHS commissioning of services from the GGI.
“BY EMAIL
Amanda Pritchard
CEO NHS England
20 July 2023
Dear Amanda,
In the most recent exchange of correspondence, NHS England informed me that it had checked its current contracts and none involved the Good Governance Institute (GGI).
This followed NHSE’s hiring of the GGI last autumn via the Chief Nurse’s directorate, AFTER the GGI employed the sacked former NHS trust director Mason Fitzgerald.
Companies House advised the BBC that no company should include the sensitive word “institute” in its name without permission from the Secretary of State, and that to do so is an offence. According to the BBC, Companies House has written to the GGI to ask it to stop using its current name.
There were also other matters of concern.
Will NHS England take the additional step of reviewing whether this company should ever be used again by the NHS?
As a wider point, Rachael Maskell MP questioned the usefulness and value for money in outsourcing governance reviews in this manner. Prof Andrew Sturdy from Bristol University pointed to the “demand inflation” that is driven by the self-interest of private consultants looking for repeat business, when they transact with the NHS.
Many thanks and best wishes,
Minh
Dr Minh Alexander
Cc Health and Social Care Committee”
Newsnight sought expert advice from Prof Andrew Sturdy, School of Business, University of Bristol who advised that NHS bodies are spending on average £1.2 million annually, each, on external consultancy which is making them less efficient. External consultants in his view want repeat business, cultivate friendly relationships and are reluctant to tell Emperors that they are exposed.
Prof Sturdy and colleagues’ 2020 paper on the NHS’ wasteful use of external consultancy can be found below:
Rachel Maskell MP questioned the sense of outsourcing such high-priced consultancies. She submits that governance determinations should be formal, statutory and subject to proper review of improvement.
We have of course been assured by the relevant parties that it was a fair and competitive appointment. Perhaps in the same way that the UHB gave assurances that the FPPR investigation on David Rosser was sound, but have refused to publish it.
University Hospitals Birmingham NHS Foundation Trust announces Group Chief Executive
Published on 17/07/2023
Jonathan Brotherton, Group Chief Executive of University Hospitals Birmingham NHS Foundation Trust (UHB).
“I am very pleased to announce, that following a rigorous and competitive recruitment process, Jonathan Brotherton has been appointed as Group Chief Executive of University Hospitals Birmingham NHS Foundation Trust (UHB).
“Jonathan, UHB’s interim chief executive, was successful in securing the role after a multi-staged process, involving a wide range of external and internal stakeholders, including senior clinical and non-clinical staff, governors and regulators.
“On behalf of the Board, I would like to offer our sincere congratulations to Jonathan on his successful appointment.
“I very much look forward to continuing to work alongside him and the Board, to deliver our ambitious – but fundamental – priorities, which will make real and noticeable differences to our patients and colleagues.
“Jonathan takes up his role with immediate effect.”
Speaking on his appointment, Jonathan said: “I am absolutely delighted to be chief executive of such an amazing organisation. As someone who was born in Birmingham and has worked in the area for a number of years, both clinically and managerially, it is a real privilege and an honour.
“For the past seven months – as interim chief executive – I have sought out the thoughts, opinions and concerns of many people, during what has been a very challenging time for UHB, its people and its patients. There is clearly a lot which needs to happen; we are reliant on the amazing people who work here to deliver that.
“As chief executive, I will be working hard to make sure that we have the kind of culture that allows people to flourish and thrive, to enable us all to do our very best for our patients.
“I want UHB to be a place where everyone is proud to work, where our patients are proud to be treated, and where we deliver the best possible and equitable care to each and every patient.”
Lastly, I made a small cameo appearance on the Newsnight broadcast, questioning why a governance organisation would employ someone who had been dismissed after a false qualification claim.
I see that the GGI has responded.
RELATED ITEMS
Darren Grayson was a former NHS CEO at East Sussex who resigned after a very critical CQC report. He sold services to the NHS though the Good Governance Institute, including at Sussex. Most recently, he secured a job at Sussex Uiversity Hospitals NHS Foundation Trust, as Chief Governance Officer.
Dr Minh Alexander retired consultant psychiatrist 14 July 2023
I raised concerns in a post earlier this week about NHS England’s refusal to heed concerns from bereaved families and whistleblowers about the suitability of a Jeremy Hunt favourite, Marianne Griffiths former Sussex NHS trust CEO, to investigate the North East Ambulance Service (NEAS) deaths scandal.
I also pointed out that she gave sketchy details about her investigation team, which seemed to lack clear credentials for handling complex legal issues thrown up by the matters at NEAS.
A concerned party has now contacted me to say that they believe that Griffiths’ investigation team at NEAS were in fact former trust colleagues from her days at Sussex.
I have written to Amanda Pritchard, CEO of NHS England, copied to parliament and others, seeking clarification.
The correspondence is shared below and is hopefully self-explanatory:
BY EMAIL
Amanda Pritchard
CEO NHS England
14 July 2023
Dear Amanda,
Concerns about the selection of Marianne Griffiths’ investigation team at North East Ambulance Service
I write to enquire about the composition of the team which, led by Marianne Griffiths former CEO of Sussex University Hospitals NHS Foundation Trust, which conducted NHS England’s investigation into the deaths scandal at North East Ambulance Service (NEAS).
As you can see, the credentials of the investigation team members were not clearly and fully provided.
It did not seem clear to me that there was sufficient expertise within the team to determine complex issues of whistleblowing, employment, coronial and criminal law which arose from the matters at NEAS.
It was not obvious that there were any practising lawyers on the team.
A concerned party has now contacted me to say that they believe all members of the Griffiths NEAS deaths investigation team were former colleagues of Marianne Griffiths at Sussex.
The person believes these are the relevant employment details of the NEAS investigation team members:
“Marianne Griffiths – CEO, Western Sussex Hospitals/Brighton and Sussex Hospitals/University Hospitals Sussex – 2010 – 2022
Denise Farmer – Director of Organisational Development and Leadership, Western Sussex Hospitals/Brighton and Sussex Hospitals/University Hospitals Sussex – 2010 – 2022
Lynn Woolley – Head of Midwifery and Gynaecology, Brighton and Sussex Hospitals/Western Sussex Hospitals – 2012 – 2021, Director of Maternity Services, Portsmouth Hospitals – 2021 to current (also CQC adviser on maternity)
Sian Finlay – Executive assistant to the CEO (Marianne Griffiths) and the Chair (Alan McCarthy) at University Hospitals Sussex 2017-2022”
Could NHS England kindly confirm if the individuals in the Griffiths investigation team have been correctly identified.
Concerns arise if so.
The impression of a handpicked team of Marianne Griffiths’ former Sussex NHS trust colleagues is troubling, especially from a trust which is now under police investigation into whistleblowers’ disclosures about deaths, which may amount to allegations of gross negligence manslaughter.
Dr Minh Alexander retired consultant psychiatrist 12 July 2023
Summary: NHS England resisted concerns from several parties about the fact that it had appointed Marianne Griffiths former CEO of Sussex University Hospitals NHS Foundation Trust to investigate the deaths scandal at North East Ambulance Service (NEAS). It officially stood by her AFTER the police investigation into deaths at her former trust in Sussex became public in early June, stating that it was “content” with her. Her report today has been understandably dismissed by bereaved families as a whitewash. There are other concerns about the report. The credentials and suitability of Griffiths’ investigating team are not clear, especially with regards to the complex legal matters involved at NEAS. There is also still no sign of a persistently withheld report on bullying and whistleblowing governance at NEAS, only scant summary of findings of opinion without facts. As bereaved families have commented, “This is the NHS investigating the NHS”.
NHS England’s investigation into North East Ambulance NHS trust has been published today:
It was led by Marianne Griffiths former NHS CEO despite multiple objections from bereaved families and several whistleblowers, including those who reported she failed them. I objected over a year ago, based on concerns about governance at her former trust in Sussex where she was CEO, and received the usual stonewalling from NHS England.
After fits and starts of correspondence and long silences, NHS England eventually spat out its reluctant response on 20 June 2023:
“In brief, NHS England is content with Dame Marianne Griffiths’ suitability to lead this review and expect it to conclude soon.”
This was remarkable as it came AFTER revelations about the police investigation at Griffiths’ former trust in early June.
There was nothing in NHSE’s response to address the governance issues I raised about her former trust at Sussex. Or any sign that NHSE had investigated the ongoing issues at Sussex, some of which were seeded during Griffiths’ tenure.
Importantly, NHS England confirmed in its response to me that Griffiths had received a copy of a review about bullying and poor whistleblowing governance at North East Ambulance Service, as part of her investigation into the trust.
Email from NHS England 20 June 2023:
“Hi Minh
Apologies for the delay in responding to your email. NHS England take all whistleblowing-related issues seriously and as such I have taken the time to review your concerns.
In brief, NHS England is content with Dame Marianne Griffiths’ suitability to lead this review and expect it to conclude soon.
With regards to the Stanley/Boylin report, it was shared confidentially with Dame Marianne Griffiths. NHS England does not intend to request investigation documents, nor to commence a review of the investigation contents. We await the findings of Dame Marianne’s review, and will then consider whether any action needs to be taken in response to that review.
I note you have also emailed recently about the ‘implications of governance failings at Sussex’ and I hope this response addresses the point you raise there too.
I am sorry again for the delay in responding to you. I know there is another matter I have yet to respond to you on, and will aim to do so next week.
With best wishes
Tom”
[My emphasis]
The review about bullying and whistleblowing failures at NEAS took place in 2020, and it was carried out by Jennie Stanley (née Fecitt) and Tracy Boylin.
The report has been suppressed by NEAS ever since.
Affected trust staff were only given superficial feedback about the outcome of the investigation, that concerns were partly upheld.
The trust has refused to disclose it under FOI, whether in full or as summary findings and recommendations.
Griffiths’ report on NEAS, unveiled today, is a woeful affair. It refuses, on a test of the balance of probabilities, to find that repeatedly altering original documents and withholding documents from the coroner was deliberate concealment.
Tracey Beadle, Quinn’s mother, told HSJ that the report was a “complete whitewash” due to issues including its limited scope and key details being omitted from previous investigations, and that the review failed to examine why the Care Quality Commission did not take action when concerns were raised with them. She also questioned the suitability of Dame Marianne to lead the review, given cultural problems previously highlighted at her former trusts.
“This is the NHS investigating the NHS,” she said. “Therefore no impartiality exists.”
She added NEAS “have [been] afforded protection from [CQC and NHSE], putting their reputations before the safety and wellbeing of patients”.
Griffiths’ conclusions reduce NEAS’ use of illegal and unenforceable clauses in settlement agreements, which prevented whistleblowers from pursuing public interest concerns further (applied in one case and rejected in another), to a matter of “misinterpretation” and “perception”:
“In those two cases, the circumstances were sufficiently sensitive and contentious as to make any form of proposed settlement open to potential misinterpretation. NEAS accept that there were perception issues with that, and its processes have been strengthened.”
It is unclear what specialist expertise informed Griffiths’ investigation. The full credentials of the investigation team are not supplied:
What credentials did the Griffiths investigation team have to make determinations on issues of whistleblowing, employment, coronial law and criminal law? It is not obvious that there were any practising lawyers on the team.
Griffiths’ analysis of NEAS’ general whistleblowing governance is staggeringly superficial and brief. The report’s section on Freedom To Speak Up was less than two pages long (see pages 62 and 63) and totalled 641 words. The specific section on the coronial whistleblowers tries to paint a “can of worms” type picture. This can be a technique that is sometimes used for misdirecting attention in whistleblowing matters.
I cannot find explicit mention of the Stanley/Boylin report’s outcome in Griffiths’ report.
I found this passage:
“6.34 Between 2019-20 there was a significant change in executive leadership; a new Chief Executive (CEO) (following a gap of 4 months), new Director of Quality and Safety, new Finance Director and new (and the organisation’s first substantive) Director of HR (HRD). The incoming CEO put the new executive team together including investing in Board development work. She also actioned the outcome of reports relating to behaviours and culture including meeting staff who had raised concerns.”
There were also these passages about an unspecified external Freedom To Speak Up commissioned by NEAS concluded in 2020, which would fit:
“7.38 The findings made clear that the functioning and leadership of HR, and relationships between senior staff, had been difficult for some time and had not been addressed effectively up to 2020.
7.39 Senior leaders had allowed dissent and factions to interfere with proper processes and therefore added to serious risk for HR and professional matters, and to the support given to the organisation, including to the staff raising concerns and grievances.
7.40 There was clear evidence of a lack of professional respect, and a lack of acknowledgement of professional duties and responsibilities and the consequent need to co-design processes.
7.41 There was a lack of transparency and consistency between the operational management of services and professional leadership.”
The facts supporting these opinions are not provided.
Opaquely, Griffiths gives no bibliography of the documents examined by her investigation.
A search of her report for the words “bully” and “bullying” yield zero hits, although she was tasked with examining culture.
Why has there been so much secrecy about the Stanley/Boylin report outcome?
Why has over £35K public money not been properly accounted for?
Why do private contractors undertake these types of reports without a clear condition that such reports will be openly published?
Is it because there would be no repeat customers if NHS organisations cannot cherry pick what is reputationally advantageous to publish?
Why are NHS bodies allowed to misuse public funds in the support of managerial self interest and against patients’, families’ and the workforce’s rights to transparency?
The bad, bad smell that still hangs over NEAS will likely intensify as the scandal at Sussex unfolds.
Perhaps NHS England will invite Helen Ray the NEAS CEO to review Sussex at some point. Only once CQC has confirmed improvement at NEAS and upgraded the trust to “Good” or “Outstanding”, of course.
But unaccountable senior NHS managers are bulletproof for now.
But this serves to emphasise how perfectly unfit the NHS’ governance is when things go wrong, and how only hard law reform will suffice to protect whistleblowers.
RELATED ITEMS
I have written to the Secretary of State about the missing Stanley/Boylin report.
08.07
BY EMAIL
Steve Barclay
Secretary of State for Health and Social Care
12 July 2023
Dear Mr Barclay,
Suppressed report on bullying and poor whistleblowing governance at North East Ambulance Service
Marianne Griffiths’ investigation on North East Ambulance Service for NHS England was published today and references your predecessor’s announcement last year about this investigation.
One of the NEAS whistleblowers understandably declined to cooperate with this flawed exercise. The investigation was also criticised by the bereaved families.
I write to draw your attention to the fact that NEAS paid over £35K for a 2020 report on bullying and poor whistleblowing governance at the trust, which it has suppressed ever since. This was the so-called Stanley/ Boylin report. Its findings appear to be absent also from today’s Griffiths report.
NHS England confirmed in a note to me last month that Marianne Griffiths had been provided with a copy of this report.
However, I can find no clear mention of its findings in her report today. I could find only this paragraph:
“6.34 Between 2019-20 there was a significant change in executive leadership; a new Chief Executive (CEO) (following a gap of 4 months), new Director of Quality and Safety, new Finance Director and new (and the organisation’s first substantive) Director of HR (HRD). The incoming CEO put the new executive team together including investing in Board development work. She also actioned the outcome of reports relating to behaviours and culture including meeting staff who had raised concerns.”
Marianne Griffiths also provides no bibliography at the end of her report to transparently list the documents examined by her investigation. A search of her report for the words “bully” and “bullying” brings up zero hits.
The section of her report on Freedom To Speak Up is less than two pages long and comprises of 641 words.
The report claimed it could not say that the repeated alteration of original documents and withholding of documents from the coroner, which the trust had previously been warned were potential crimes, was a deliberate act of concealment.
I really do not think that the public interest has been served by this report. It is in my opinion a sample of what we should expect if the NHS is permitted to conduct its own “exit Fit and Proper Person tests”, as currently proposed by NHS England.
I forward below the correspondence from NHS England which informed me that Marianne Griffiths had been provided with the Stanley/Boylin report.
This brief response was the culmination of over a year of my raising concerns with NHS England about Marianne Griffiths’ suitability to lead the NEAS investigation given the previous concerns about whistleblowing governance at her former NHS trust in Sussex.
Additional concerns arose over the course of that year. You will see that none of this swayed NHS England.
With best wishes,
Minh
Dr Minh Alexander
NHS whistleblower and retired consultant psychiatrist
Cc Tom Kark KC
08.54
BY EMAIL
Steve Barclay
Secretary of State for Health and Social Care
12 July 2023
Dear Mr Barclay,
My apologies.
I need to correct my earlier letter today of 08.07.
I have found a further passage in Marianne Griffiths report which seems to give a brief outcome of the 2020 Stanley/Boylin report, although the report is not explicitly identified.
It is stated that an external report commissioned by NEAS concluded in 2020 with the following:
“7.38 The findings made clear that the functioning and leadership of HR, and relationships between senior staff, had been difficult for some time and had not been addressed effectively up to 2020.
7.39 Senior leaders had allowed dissent and factions to interfere with proper processes and therefore added to serious risk for HR and professional matters, and to the support given to the organisation, including to the staff raising concerns and grievances.
7.40 There was clear evidence of a lack of professional respect, and a lack of acknowledgement of professional duties and responsibilities and the consequent need to co-design processes.
7.41 There was a lack of transparency and consistency between the operational management of services and professional leadership.”
My understanding is that affected staff were advised that their concerns were partly upheld by the Stanley/Boylin investigation, but that they were given no other information. I have seen some of the feedback correspondence from the trust.
In Marianne Grittith’s above summary, opinions are given but the specific facts supporting them are not.
She provides little comment on the issues of whistleblowing governance examined.
Information relevant to mounting an effective Fit and Proper Person challenge remains largely withheld from affected parties.
Dr Minh Alexander retired consultant psychiatrist 11 July 2023
Steve Barclay Secretary of State waffled before Health and Social Care Committee on 20 June 2023, in response to questions about the failure of the government’s Freedom To Speak Up project to protect NHS whistleblowers, after eight long and miserable years.
In consequence, I asked him some questions under FOI:
In brief, the Department says it has accepted the following four recommendations from the Kark review on Fit and Proper Persons in the NHS, but hasn’t a clue when they will be implemented, because it’s been palmed off onto NHS England:
“With regard to recommendations 1 to 4, DHSC does not hold the information you have requested. However, you may wish to contact NHS England, which may be able to provide an update on the timetable for recommendations 1 to 4.”
“Recommendation One
All directors (executive, non-executive and interim) should meet specified standards of competence to sit on the board of any health providing organisation. Where necessary, training should be available.
Recommendation Two
That a central database of directors should be created holding relevant information about qualifications and history.
Recommendation Three
The creation of a mandatory reference requirement for each Director
Recommendation Four
The FPPT [Fit and Proper Person Test] should be extended to all Commissioners and other appropriate Arms-Length Bodies (including NHSI and NHSE).“
Disbarment has been dumped
Importantly, it is also confirmed that Barclay has ditched Kark’s fifth recommendation, for a mechanism to disbar NHS managers for serious misconduct:
“The power to disbar directors for serious misconduct”
This is blamed on NHS England:
“The Government agrees with NHS England that effective safeguards are currently in place by ensuring an exit fit and proper person test is completed when directors leave employment and that any conduct issues which arise after their employment remain on the national register. These safeguards, together with a robust referencing process, will prevent unsuitable leaders being re-employed in the NHS and also act as a deterrent to misconduct itself.”
So, “an exit Fit and Proper test” has been secretly mooted but kept hidden even after publication of the NHS Workforce plan on 3 July 2023.
It sounds like a ludicrous fig leaf, that everyone knows is a ludicrous fig leaf.
Interestingly, NHS England previously blamed ministers for disbarment being dumped, telling me there was no “ministerial support” for this Kark recommendation.
How they all twist and turn.
It is worth remembering that Kark’s review reserved disbarment for matters such as criminal convictions leading to a custodial sentence, victimisation of whistleblowers or knowingly allowing the victimisation of whistleblowers, “Causing, facilitating, colluding in, or requiring any staff member to fail to comply with the duty of candour including by means of a settlement or confidentiality agreement” and “Falsification, concealment or suppression of records, data or other information which is required to be provided to any other person or organisation”.
And the disbarment mechanism also fell short of full regulation. The latter is rightly expected of hundreds of thousands of NHS staff who are responsible for patients’ lives. But so are NHS managers, who have been dodging regulation since it was recommended by the Bristol heart public inquiry over twenty years ago.
“Now Stephen Barclay, a health minister, has told The Independent he wants the “fit and proper” person test for NHS directors – introduced in 2014 – to be widened to require action on harassment and discrimination.
Mr Barclay said: “That one in four NHS staff have experienced bullying, harassment or abuse – and that more than twice as many BAME [black, Asian and minority ethnic] staff have suffered discrimination from their manager or colleagues than white staff – is deeply alarming and should be a call to arms for urgent action across the NHS.
“I am determined to put an end to this, which is why the NHS is already working to close the equality gaps and tackle bullying.”
It is also worth remembering that Barclay recently wondered out loud at Committee on 20 June 2023:
“What accountability is there for senior managers when wrong doing is established? Are they just rotated through the system? Or are people held to account?”
Really Mr B!!!!
UPDATE 23 AUGUST 2023
The Telegraph yesterday asserted that the ministerial fashion for dumping disbarrment originated with Matt Hancock:
RELATED ITEMS
NHS England’s “exit Fit and Proper Person test”
I have written to the Chief Workforce Officer at NHS England to ask for details of the “exit Fit and Proper Person test” mentioned in the Department’s FOI response:
“The Government agrees with NHS England that effective safeguards are currently in place by ensuring an exit fit and proper person test is completed when directors leave employment and that any conduct issues which arise after their employment remain on the national register. These safeguards, together with a robust referencing process, will prevent unsuitable leaders being re-employed in the NHS and also act as a deterrent to misconduct itself.”
I would be grateful if in your reply to my enquiry of 4 July 2023 you could additionally include the details of the “exit Fit and Proper Person test” that is envisaged by NHS England, and by whom it will be applied.
If no such exit test has yet been devised, please indicate the timescale within which the test will be developed and ready for use.
Would the exit test will be applied by a local employer with possible vested interest, as opposed to an independent central body, as disbarring mechanism would be?
I must say I cannot see how for example, University Hospitals Birmingham NHS Foundation Trust would have applied an exit test reliably to David Rosser, its former CEO who was criticised by the Employment Tribunal for his behaviour towards a whistleblower. He also received a warning from the General Medical Council. The trust board has still not published a flawed FPPR investigation review on David Rosser, conducted by a subordinate trust employee which it claimed cleared him. The trust board also misled the public in a bizarre fiction, claiming that Rosser stepped down as CEO and moved to a regional role, when he remained a trust employee as revealed by an FOI request. As the trust board continues to deny that its FPPR investigation found cause for concern, if left in control of an exit FPP test, I imagine it would allow him to recirculate in the NHS.
Many thanks and best wishes,
Minh
Dr Minh Alexander
NHS whistleblower and retired consultant psychiatrist
Cc Tom Kark KC
Health and Social Care Committee
Secretary of State for Health and Social Care
Is the Patient Safety Commissioner a Prescribed Person under PIDA?
Under this law, there are a number of designated bodies and individuals to whom whistleblowers may make so-called “protected disclosures”.
This too is a useless system as the Prescribed Persons sometimes are clueless about their responsibilities, and are legally obliged to do little more than to log the concerns received and to publish a superficial annual report about the numbers of concerns. No one is legally obliged to protect the whistleblower or act upon their concerns.
Barclay implied to Committee on 20 June 2023 that the Patient Safety Commissioner (for Medicines and Devices only) might be a Prescribed Person for whistleblowers’ disclosures. She is not currently listed as one. I asked him if the Department intended to give her this legal status. It did not reply.
The Patient Safety Commissioner was of course the second and particularly objectionable NHS National Freedom To Speak Up Guardian who expended most of her and her Office’s energies on PR, self-promotion and supporting an establishment narrative. Not to mention instances of failure to apologise and learn when her Office actually harmed whistleblowers:
Dr Minh Alexander retired consultant psychiatrist 6 July 2023
Disappointing BBC News coverage featured Robert Francis and the latest NHS Freedom To Speak Up Guardian Jayne Chidgey Clark on 3 July 2023.
The piece helped to legitimise the National Guardian’s Office, when it is in fact a threat to NHS whistleblowers.
The BBC team who produced the material did not balance claims by the National Guardian with evidence of her Office’s failures or with criticisms of her Office by whistleblowers.
They also chose not to include whistleblowers with the strongest cases which exposed the serious failings of the National Guardian’s Office. Whistleblowers from whom they had agreed to take this evidence were ignored.
Below is a letter to the relevant BBC team, placing my concerns about the coverage on record:
The thrust of the BBC reportage was on airing a defunct and empty argument that culture change alone is needed.
Robert Francis commented disingenuously that NHS boards need to “buy into” and “understand” about whistleblowing. He knows full well that many boards understand, but simply choose self interest and suppression. He used to advocate dismissal for abusive NHS CEOs.
Culture change is of course needed but it is not going to happen without enforcement. Road safety laws on safety belts and drink driving are an example of law changing behaviour and culture.
Power, however, naturally fears enforcement of whistleblowers’ rights to protection and action upon their disclosures.
The BBC News coverage appeared the day after The Guardian ran an item featuring the BMA’s call for reform of UK whistleblowing law:
Moreover, BBC News featured the National Guardian’s claims to purportedly support accountability for whistleblower reprisal:
“Dr Chidgey-Clark says the main healthcare regulator – the Care Quality Commission (CQC) – and NHS England itself could do more to protect individual whistleblowers and rein in rogue managers.
“I do call on them to do everything they can within their power to ensure there is accountability and these serious issues are looked into,” she says, “because without that, more high-profile cases will happen and, potentially, more patient harm and worker harm will happen. And in our society, in our healthcare system, we don’t want to see that.”
It is hypocritical of the National Guardian and her Office to call for others to ensure accountability for whistleblower reprisal and detriment, when they have done the opposite.
And why the distasteful focus on “high profile” cases? Every whistleblowing case matters, because every patient matters.
The National Guardian’s Office was primarily set up to provide independent reviews of poorly handled NHS whistleblowing cases, but has conducted a shockingly low number of case reviews since the Office was established in 2016.
Case reviews by the National Guardian since 2016:
Southport and Ormskirk NHS Trust 2017
Northern Lincolnshire and Goole NHS Foundation Trust 2017
Derbyshire Community Health Services Foundation Trust 2018
Nottinghamshire Healthcare NHS Foundation Trust 2018
Royal Cornwall Hospitals NHS Trust 2018
Brighton and Sussex University Hospitals NHS Trust 2019
Northwest Ambulance Service NHS Trust 2019
Whittington Health NHS Trust 2020
Blackpool Teaching Hospitals NHS Foundation Trust 2021
Thematic review of ambulance trusts 2023
The case reviews turned into toothless systems reviews and are now not even called case reviews anymore. They have been renamed “speak up reviews”, hiding their original purpose.
The NGO’s case reviews have avoided criticising any senior manager for harming whistleblowers.
… 1.12 Communicate that detriment for speaking up will not be tolerated, act to prevent detriment occurring, and put in place procedures that would enable cases of detriment to be looked into effectively when they are reported.”
That is hardly accountability for serious wrongdoing. It glossed over serious harm already done to the trust whistleblowers.
At North Lincolnshire and Goole, where the trust Chair publicly and notoriously attacked a whistleblower, the National Guardian made no reference to this incident in its case review report other than to say that the Chair expressed “regret” and made no recommendation for regulatory action to be taken against the trust Chair.
“We carried out this review because we had received information that the trust’s support for its workers to speak up did not always meet with good practice.”
Whitewash Central in other words.
In the latest case review by the current National Guardian, which was a thematic review of ambulance trusts, the resultant review report listed grievous examples of detriment (pages 43 and 44).
But the National Guardian did not criticise any managers responsible and kicked the can down the road by only suggesting that the Kark review recommendations should be implemented:
“One of the Kark Review recommendations called for processes to ensure greater accountability for leaders, including a focus upon behaviour which suppresses the ability of people to speak up about serious issues in the health service. This recommendation must be implemented as a matter of urgency.”
It was in fact within the National Guardian’s gift, and indeed arguably one of her duties, to request that the CQC review trust directors under Fit and Proper Persons regulation, and that NHS England should take related action. But she did not report that she did so.
Compounding these failures to hold abusive managers to account and to set the right tone, successive National Guardians have also refused to facilitate access to redress for harmed whistleblowers. This is despite the fact that this was recommended in the 2015 Freedom To Speak Up Review:
They have repeatedly taken the indefensible line that it is not part of their job.
Unsurprisingly, the National Guardian and her Office are not trusted by the NHS workforce and regularly receive only a tiny number of qualifying disclosures as a Prescribed Person under UK whistleblowing law, from an NHS workforce of 1.4 million.
BBC News reported quite wrongly that the National Guardian’s Office received over 25K contacts last year. This was actually the contacts received by local NHS trust Freedom to Speak Up Guardians and others.
Appallingly, the NGO sent 13 of these 30 staff back to their trusts:
“Signposted a worker to the Freedom to Speak Up Guardian at their organisation, so that the worker could contact them for support to raise matters relating to their disclosure”
When NHS staff contact the NGO (and some of them will be NHS trust Freedom To Speak Up Guardians who have been blocked or victimised for helping whistleblowers), they will have lost confidence in their employers.
It is unsafe and abusive to give such staff the runaround and make them go back to their employers.
Yet the NGO tried this approach in the whistleblowing case of Mr Shyam Kumar surgeon from University Hospitals Morecambe Bay NHS Foundation Trust (UHMBT), despite the fact that this trust was already notorious for several serious whistleblowing failures. This included a trust cover up of breast screening failures.
I am aware of at least seven whistleblowing cases from UHMBT, and yet the NGO has studiously avoided any case review of this organisation.
That must surely be a serious failure in the NGO’s duty of care to trust staff, and another example of the political nature of the NGO in how it sidesteps matters that are inconvenient to power.
That is hardly holding erring senior trust managers to account.
I asked Ian Trenholm CQC CEO to investigate the failure of the NGO at Sussex since the police investigation became public knowledge. He passed it to the CQC complaints team, who replied on 5 July 2023:
“After considering your email, we will not be considering this as a corporate complaint, as it goes beyond the time limit of what we would consider under our policy.”
So no accountability.
In the case of whistleblower Dr Jasna Macanovic who asked for help, the National Guardian’s Office told her to come back after her Employment Tribunal had concluded. This meant there would be no help for her or for patients for years. This too has happened to other NHS whistleblowers.
It was left to the whistleblower community to refer Dr Macanovic’s dismissing Medical Director to the CQC (the National Guardian’s employer) under Regulation 5 Fit and Proper Persons, who as usual refused to find any breach of the regulation.
I have seen correspondence supplied by an NHS whistleblower with a very serious case who was dismissed despite seeking help from their local trust Freedom To Speak Up Guardian.
They contacted the National Guardian’s Office for help. They gave the NGO a detailed account of what had happened to them, including their attempts to seek help through the local trust Guardian.
The National Guardian’s Office, under Jayne Chidgey Clark, wrote back last year suggesting:
“We understand that you were a worker at REDACTED and have attempted to speak up about a number of issues, including those around patient safety. We understand that you do not feel able to speak to the Guardian at the Trust as they are employed by them. However, we would encourage you to contact them if you have not already done so.”
The NGO correspondence continued in this incompetent and insensitive vein, such that the whistleblower questioned whether the NGO had actually read their original request for help.
This is a typical example of how the NGO operates.
The Office resists requests for help, and its first response is to try to send NHS whistleblowers back to the organisations in which they have lost confidence.
Sending victims back to abusers is not a recognised method of safeguarding.
I hope that BBC News will at some point acknowledge that the NGO’s actions smack more of collusion than accountability.
As does the disgracefully low number of case reviews conducted by the NGO.
The National Guardian’s Office simply does not protect whistleblowers.
RELATED ITEMS
The lack of evidence base for the Freedom To Speak Up project
It was reported that the prototype Cultural Ambassador role had disappointed some staff:
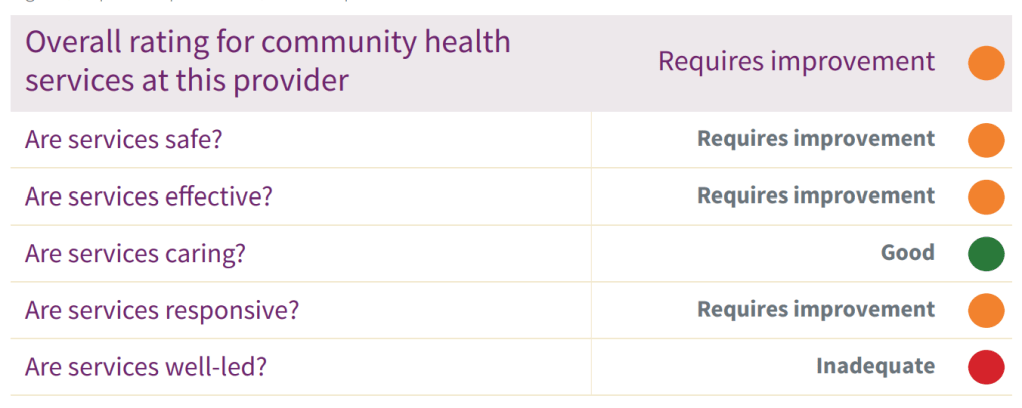
“The Staffordshire and Stoke on Trent Partnership NHS Trust created a role of ‘Ambassador for Cultural Change’. This innovative role was designed to allow the staff voice to be heard and concerns from staff to surface in a way that focused on the topic rather than the individual, protecting the identity of any staff member wanting to remain anonymous. This initiative received significant national attention. We saw that not all staff were happy with this role. They were often guarded and concerned they might not have the full protection promised. While some staff engaged with the Ambassador for Cultural Change many felt that the actions from this did not follow on as expected.”
And the trust was rated “Inadequate” on the Well Led domain partly because trust executives had not addressed staff concerns:
Francis et al did not put these salient facts in the glossy Freedom To Speak Up promotional material.
The truth, as ever, struggled to lace its boots whilst its counterpart had already been widely disseminated by government spin doctors.
Dr Minh Alexander NHS whistleblower and retired consultant psychiatrist 2 July 2023
Summary: This is a brief post to share documentation which shows that the private company WhistleblowersUK’s business model continues to be based partly on charging whistleblowers for help, and that it has linked with another company which sells services to barristers.
WhistleblowersUK also asks people for money if they wish to become “associate members”.
A statement of interests to Somerset Council by WhistleblowersUK’s Chair wrongly indicates that WhistleblowersUK is a public authority, and does not disclose that Whistleblowers seeks to influence public opinion and policy.
Background
WhistleblowersUK acts as the external secretariat of the Whistleblowing APPG. Leading members of the APPG and WhistleblowersUK seek to introduce a US model of bounty hunting.
WhistleblowersUK recently co-produced a lengthy document singing the praises of whistleblower rewards, with two major US bounty hunting law firms. However, the document omitted to mention serious drawbacks of the US bounty hunting model, such as its exploitative nature and the fact that the majority of whistleblowers are left with nothing, even if they suffer reprisal and loss. The model also siphons money into lawyers’ coffers. Bounty hunting is a billion dollar US industry led by lawyers. Lucrative cases from the financial sector generate huge bounties.
WhistleblowersUK’s document on rewards for informers also claimed that historically, the model worked well in England. Historical studies reveal that the model generated scams and corrupt practices, as has been the case with its modern successor.
I have since been contacted by someone who approached WhistleblowersUK for help and who obtained the following documents, which they have shared with me:
A revised, updated version of WhistleblowersUK’s “Statement of cooperation”
I have previously published an earlier version of this document.
Changes include the fact that this appears to be a joint document produced with another private company, the “Barrister Consultancy Services”.
The Barrister Consultancy Services’ logo also appears on this document, and the document reads:
“If appropriate we will introduce you to our trusted partner Barrister Consultancy Services (BCS), who will provide you with legal project management services enabling us to work together on your case from start to finish.” [my emphasis]
The document also indicates that WhistleblowersUK may arrange initial pro bono assistance by barristers that is not legal advice. It appears to imply that BCS may be involved in arranging access to barristers:
“We help you retain full control at all times because you know your case best.
Our specialist panel of barristers usually provide initial pro bono assistance (not legal advice) based on the chronology and supporting information that you supply. All barristers on our panel are regulated by the Bar Standards Board in England & Wales and/or Faculty of Advocates in Scotland, be assured that separate letters of agreement will be sent to you before any official legal advice is provided. You will not incur any legal costs without your agreement. WBUK & BCS does not accept responsibility or liability for any independent legal advice provided.”
The statement of cooperation links to the website of the BCS to a page about the BCS’ privacy policy.
The BCS website suggests that this company primarily provides specialist administrative support to barristers:
“Barristers in the UK often work independently in Chambers and are mostly self-employed. Therefore, they are responsible for managing their own practices and developing their business. However, managing a legal practice can be complex and time-consuming, which is why many barristers and their clerks turn to Barrister Consultancy Services for assistance.”
The “About” page of the BCS states:
“As former Barrister Clerks and Practice Managers, our primary objective is to enhance and refine internal practice management processes and procedures within barrister’s chambers.”
At the bottom of the pages of the BCS website, it is stated:
“Barrister Consultancy Services is the trading name of David Wright a self-employed consultant at DW Business Consultancy, a Company Registered at 23 Franmil Road, Hornchurch, Essex, RM12 4TR No: 10431011”
The Companies House entry for DW Business Consultancy lists Linda Wright as company secretary and David Wright as director. The nature of the business is stated to be: “70229 – Management consultancy activities other than financial management”.
According to Companies House, BCS was incorporated on 17 October 2016, and it last filed accounts last year, with “Accounts for a dormant company made up to 31 December 2021”.
These accounts state that the company was dormant in the reporting period, received no income and incurred no expenditure.
BCS also has a post on Facebook as follows:
An examination of the metadata of the revised Statement of Cooperation by WhistleblowersUK reveals that it was last edited by David Wright:
In comparing the new “statement of cooperation” with the previous version that I published, the section “What we will do for you” has been expanded, with insertion of an additional service:
“We will help you identify and instruct specialist legal advisors.”
The latest statement of cooperation indicates that WhistleblowersUK still charges whistleblowers £100 per hour for its services, albeit it now states that it will provide initial assistance without charge for up to two hours.
The latest statement of cooperation indicates that WhistleblowersUK also asks for a “percentage” of any financial award that a whistleblower may receive. It differs from the previous version of the document in that where five percent was previously specified, there is now no numerical value given, and no clear limit on what share of financial awards WhistleblowersUK propose to take.
WhistleblowersUK’s application form for associate membership
WhistleblowersUK states in the application form that it does not charge fees for membership.
However, it asks any individuals wishing to join as an associate member for a minimum donation of £120 per annum.
There is a section at the end of the document which states:
“Financial hardship is not a barrier to becoming an Associate Member. The Directors will consider applications to waive the requirement for a regular donation. Please advise WBUK in Section 2, Question 3 if you wish to apply for a waiver.”
This is the clause in the application form which asks applicants to commit to the payment of £120 and to abide by the company’s by-laws:
I could find no company by-laws on the WhistleblowerUK’s website or recorded in documents filed at Companies House.
But the application form indicates in bold text that WhistleblowersUK’s directors can terminate membership at any time:
“Associate Memberships are approved by the directors and can be terminated without notice at any time.”
WhistleblowersUK states that its objectives include expanding its associate membership:
“We Grow our community through our associate membership promoting engagement, collaboration, and sharing of ideas and perspectives among our members.”
The company publicises dates for meetings of associate members, the most recent being 26 June 2023:
However, I could find no record of the current or past number of associate members, or of the level of income generated by associate members’ required donations of a minimum £120 per annum.
I asked WhistleblowersUK through its Chair Tessa Munt former Liberal Democrat MP, now local councillor, if the organisation wished to comment on matters arising from the above two WhistleblowersUK documents, but I have not yet received a reply.
“Tessa Munt
Chair of WhistleblowersUK
29 June 2023
Dear Ms Munt,
I write to ask if WhistleblowersUK would like to comment on and/or elaborate on reports that:
i) WhistleblowersUK asks whistleblowers for £120 minimum donation per annum to be associate members
ii) WhistleblowersUK offers pro bono assistance from lawyers which is not legal advice, from a panel of specialist barristers
iii) WhistleblowersUK now works in partnership with Barrister Consultancy Services
I note in Munt’s declaration of interests to Somerset Council that she is described as “interim” chair of WhistleblowersUK, and has declared that WhistleblowersUK is a public authority when it is a private company.
I have written today to the CEO of Somerset Council and the Leader of the Council about this factual inaccuracy, and also raised an issue of whether Munt should have declared the fact that Whistleblowers is an organisation which seeks to influence public opinion and policy.
BY EMAIL
Duncan Sharkey
CEO Somerset Council
2 July 2023
Dear Mr Sharkey,
Declaration of Interests by Councillor Tessa Munt: error and omission
I am sure it is a mistake but the council currently publishes inaccurate information about Councillor Munt’s interests.
Ms Munt’s declaration of interests states under Question 9 “Do you hold membership of other Public Authorities?” that she is “director and interim chair” of WhistleblowersUK.
WhistleblowersUK is not a public authority but a private company (09347927) which had £3,905 assets by end 2022, according to documents filed at Companies House. By the end of the previous year, WhistleblowersUK only reportedly had £736 assets.
WhistleblowersUK is seeking to introduce a controversial and exploitative US model of bounty hunting, which if ever adopted as the UK national model would disadvantage the majority of UK whistleblowers and lead to only a tiny handful receiving vast rewards. The model primarily benefits bounty hunting law firms and is a billion dollar US industry, which has been trying to the break into the UK market for some years now. This model primarily targets the financial sector, where bounties from recovered monies can be huge.
Under question 11 of Ms Munt’s declaration of interests, “11. Do you hold membership of bodies influencing Public Opinion or Policy (including any political party)?”, Miss Munt has only declared membership of the Liberal Democrats.
The company states on its website that it explicitly seeks to influence public opinion and policy. It seeks to introduce an Office Of The Whistleblower, which mirrors the US Securities and Exchange Commission’s Office of the Whistleblower which handles a high profile whistleblower reward programme.
For example, WhistleblowersUK state on their website:
“We Transform the way everyone thinks about whistleblowing, educate the public, and demonstrate the importance of whistleblowers in a fair and transparent society.
We Campaign for the Office of the Whistleblower now a Bill going through Parliament that will revolutionise the treatment of concerns and the people who raise them.”
Of note, WhistleblowersUK has since 2018 acted as the external secretariat to a Whistleblowing All Party Parliamentary Group, which explicitly campaigns for the law change which would open the door to the US style whistleblowing rewards. When the Whistleblowing APPG was first established in 2018, its declarations showed that it accepted money from Constantine Cannon, a major US bounty hunting law firm. This funding was badged as payment for WhistleblowersUK’s services as external secretariat.
Sir Norman Lamb former Liberal Democrat MP was a member of the Whistleblowing APPG but resigned after the CEO of WhistleblowersUK refused to answer questions about conflicts of interest and finances which I put to the APPG:
I copy below correspondence to Councillor Munt in her capacity as WhistleblowersUK Chair, seeking greater transparency about WhistleblowersUK’s financial arrangements and the handling of whistleblowers’ highly sensitive personal data. I have received no reply to my letter of 4 May 2023, and I await a reply to my letter of 29 June 2023.
Please confirm receipt of this letter and advise what action Somerset Council will take to ensure that Councillor Munt’s declaration of interests is accurate.
Many thanks.
Yours sincerely,
Dr Minh Alexander
NHS whistleblower and retired consultant psychiatrist
Cc Bill Revans Liberal Democrat councillor North Petherton, Leader of Somerset Council and Lead Member for Governance & Communications
A Tory MP who is a pro bounty, former member of the Whistleblowing APPG secured a junior ministerial post this year and launched a review of UK whistleblowing law:
Dr Minh Alexander retired consultant psychiatrist 29 June 2023
Summary: The Department of Health and Social Care has confirmed that its plans to set up a Special Health Authority to investigate maternity failures in the NHS are dead and buried, with no plans to resurrect. This is despite an abortive attempt to recruit a Chair for the Special Health Authority which concluded with fourteen applicants being turned away. It refuses to disclose its justification for transferring the maternity investigation programme to the Care Quality Commission or the legislation drafted for the now binned Maternity and Newborn Safety Investigation Authority.
Background
Jeremy Hunt former Health Secretary’s unwieldy vanity project the national maternity investigation programme was foisted on the Healthcare Safety Investigation Branch against advice.
It unravelled in secrecy as whistleblowers spoke out against poor management and inherent systemic problems, such as designed-in conflicts of interest from seconded staff feeling pressured to keep on good terms with the regional teams they investigated, for the sake of their long term career prospects.
Keith Conradi the head of HSIB’s retirement was announced after the King’s Fund’s conclusions were shared with HSIB staff.
On 21 January 2022 the Health Service Journal reported the findings of the leaked King’s Fund report, which was the first time the report’s existence was revealed:
On 26 January 2022 Sajid Javid made a statement in parliament announcing that the government would create a short life Special Health Authority to take over the maternity investigation function from HSIB. The idea was to eventually hand maternity investigations back to NHS trusts once an example of good practice had been purportedly modelled:
“Special Health Authority will be established for up to five years from 2022-23 to enable maximum learning to be achieved and to equip NHS Trusts with the expertise, resources, and capacity to take on maternity safety incident investigations in the future.”
The post of Chair for the special health authority was advertised in autumn 2022:
“On 26 January 2022, Official Report, 25WS, by way of a written ministerial statement, the Department of Health and Social Care announced that a separate Special Health Authority would be established to continue the independent maternity investigation programme, which is currently overseen by the Healthcare Safety Investigation Branch.
The Department is committed to ensuring the continuation of independent, standardised maternity investigations that provide learning to the system and contribute to the Government’s ambition to halve the 2010 rates of stillbirths, neonatal and maternal deaths and brain injuries in babies occurring during or soon after birth by 2025.
Following careful consideration, the Department has determined that the most appropriate and streamlined mechanism for delivering the valued and independent maternity investigations is for the function to be hosted within the Care Quality Commission. The purposes of the maternity investigation programme remain as set out last January: to provide independent, standardised and family-focusedinvestigations of maternity cases for families: to provide learning to the health system via reports at local, regional and national level; analyse data to identify key trends and provide system wide learning; be a system expert in standards formaternity investigations; and collaborate with system partners to escalate safety concerns.
We will now work with the CQC and the HSIB to complete the transition of the maternity investigation programme to the CQC by October 2023.
As announced in the written ministerial statement of 9 February 2023, Official Report, 40WS, the establishment of the new HSSIB will take place in October 2023, to enable all the necessary work to be completed to ensure a smooth transition of these investigation programmes.”
The Department of Health and Social Care’s termination of the Maternity and Newborn Safety Investigation Authority
To confirm whether this was a permanent arrangement and to find out more about the justification for locating maternity investigations within the notoriously politicised and none too competent CQC, I made an FOI request to the Department of Health and Social Care. This is the response:
The Department confirmed that it went ahead with its appointment process for a chair to the Special Health Authority, for which it received fourteen applicants:
“DHSC received 14 applications for the post of Chair/Chair designate to the Maternity and Newborn Safety Investigation Special Health Authority (MNSI).”
The government claims no appointment was made because:
“An appointment was not made, as a final decision on the appointment had not been reached before the announcementon the future of the MNSI [Maternity and Newborn Safety Investigation Authority] via a Written Ministerial Statement (WMS) on 30 March 2023.”
Well that’s a good way to do business. Advertise a job and then tell everyone “Hard cheese chaps, the job’s gone”.
The government also confirms that the Special Health Authority was never legally established.
It stands by its claims that the best option is hosting by CQC rather than a standalone Special Health Authority reporting directly to the Department of Health and Social Care:
“….following careful consideration, DHSC has determined that the most appropriate and streamlined mechanism for delivering the valued and independent maternity investigations is for the function to sit within and be hosted by the CQC.”
However, the government refuses to disclose its justification for this opinion on grounds that it might be embarrassed. Sorry, I mean on grounds of Section 35 FOIA formulation of government policy, because the transition period is not yet complete and policy is still being formulated.
The government has no plans to revisit the idea of a Special Health Authority.
This implies that the maternity investigation division will likely be allowed to wither on the vine for some as yet undetermined period until it all reverts to NHS trusts. This will do nothing for the independence of maternity investigations.
The government also refuses to disclose legislation drafted for the Special Health Authority on purported grounds that this is legally privileged.
One is left wondering what sort of governmental hissy fit led to such a major change of direction, and the bizarre Heath Robinson arrangement of the Care Quality but We Don’t Investigate Complaints Commission hosting a specialised incident investigation function.
It is left only to commiserate with the unfortunate maternity investigation staff who have been so badly managed and supported from the outset of a political misadventure.
RELATED ITEMS
Hunt’s chutzpah
Hunt skilfully dined politically off the Midstaffs and Morecambe Bay disasters whilst simultaneously wrecking the NHS, fashioning a narrative of hero crusader against the wicked NHS and recruiting a number of families to insulate himself.
He dined off Midstaffs whilst reneging on core recommendations from the public inquiry such as mandatory safe staffing and real whistleblower protection, which would have helped to prevent further maternity tragedies and any need for his disastrous national maternity investigation gimmick.
Even in 2020, Hunt was still trying to politically capitalise from maternity tragedies:
His handiwork on the NHS is now all around us as emergency care has collapsed, regularly causing deaths, cancer care is teetering and 7.4 million people await treatment.
And at the UK COVID public inquiry it has just been revealed that Hunt wanted to cut Public Health England’s funding by half:
Public health is one of the most crucial, effective and super-efficient medical specialties with profound effects on improving the health of the populace. Why would anyone except the utterly incompetent or those with malign intentions wish to cut it?
I leave readers who are less familiar with CQC’s ways with this FOI revelation about how CQC senior managers huddled and deliberated on the best way to manipulate public into thinking that they had written a “hard hitting” inspection report, but with as few facts as possible:
The whistleblowing APPG and its external secretariat WhistleblowersUK are becoming more and more explicit in their pursuit of a model of financial rewards (bounties) for whistleblowing in the UK.
For a while, they toned down references to rewards in most of their written material. For example, WhistleblowersUK referred to “compensation” in contexts which made it clear that they were talking about rewards. Equally, although leading members of the APPG called for rewards and financial incentives, documents by the APPG coyly suggested that it was a matter for the government to decide if rewards were appropriate.
But last month, WhistleblowersUK produced this document with two major US bounty hunting law firms, Constantine Cannon and Kohn, Kohn, and Colapinto LLP, singing the praises of financial rewards:
Any wisps of veil are gone.This long report claimed to set out the strengths and weaknesses of whistleblowing rewards, but in reality it only knocked down straw men and it ignored elephants.
The report also makes surprising claims, such as an assertion that “qui tam” prosecutions (legal claims in the name of the King, with a share of the proceeds going to the claimant as well as the crown) “worked well for many centuries” in England.
This claim by WhistleblowersUK et al appears to be unsupported. Qui tam suits were very rough justice introduced in the 13th century only because of a lack of governance infrastructure and law enforcement resources. Citizens were effectively deputised.
“Early in Henry VII’s reign, it had become apparent that qui tam enforcement of penal statutes had created serious problems….”
False, malicious suits were sometimes pursued for personal gain. Corrupt officials “extorted” fines by imprisoning people until they “confessed” to wrongdoing. Trials without jury were held. Informers sometimes perjured themselves. Suits might be tactically and abusively filed hundreds of miles away from the accused’s home, making it nigh impossible to defend a suit.
A class of “professional informers” called “promoters” arose who made a living out of qui tam suits, and who were despised and distrusted:
“Informers were widely perceived as self-interested at best and malevolent at worst. The charge of self-interest was a natural inference from the bounty provision of a qui tam statute.”
“They were described variously as “varlets, “lewde” and “evil”…”viperous vermin”
“Indeed, informers harassed and impoverished citizens, particularly those in the lower classes, “for malice or private ends, [but] never for love of Justice.”
Some informers settled quietly and unofficially with their marks, in order to pocket more money and deprive the crown of its share, without bringing matters to the court’s attention:
“This collection of payments in return for a promise not to prosecute was, in essence, a form of blackmail or extortion.”
Informers were sometimes jailed for such scams. The worst offenders were occasionally executed.
Where justice is monetised, it is hardly surprising if the perverse incentives lead to corrupt practices. In the same way that the SEC Office of the Whistleblower became corrupted, its ancient predecessors were also sometimes corrupt.
Such was the level of abuse sometimes endured by the populace under qui tam law, that assaults and riots against informers were occasionally recorded in ye in Olde England.
Additional laws were repeatedly passed in attempts to manage the misconduct of informers.
So, hardly a picture of success as claimed by WhistleblowersUK et al.
And it is not reassuring that a claim of success was made.
Nevertheless, WhistleblowersUK, Constantine Cannon, and Kohn, Kohn and Colapinto LLP gamely argue in their report that publicity about large financial rewards increase public awareness of whistleblowers. They leap to a conclusion that this increased awareness must improve public opinion of whistleblowers, without providing the evidence to confirm this theory. (Page 20).
Notoriety for excessive whistleblower rewards, especially in scandals where victims are uncompensated, is of course an alternative explanation.
Yesterday, I observed most of a webinar by WhistleblowersUK and the Whistleblowing APPG yesterday, bar the first twenty minutes which I had to miss due to a clashing commitment. The speakers were Rory Field barrister with a specialism in organised crime and who has spoken on organised economic crime, standing in for Iain Mitchell barrister, Richard Pike of Constantine Cannon, Susan Kramer former Whistleblowing APPG Chair but still active pro-bounty politician, Folashade Adeyemo Lecturer in Banking and Company Law Reading University and a specialist in Nigerian banking regulations, a whistleblower whose full name I did not catch and Georgina Halford Hall CEO WhistleblowersUK.
The theme of the event was “restitution”.
In reality, this proved to be about financial incentivisation.
Richard Pike of US bounty hunting law firm Constantine Cannon explained the US model of bounty hunting to the audience.
He took a similar approach to that of his colleague Mary Inman in 2018 at the Bylines festival, explaining that the concept came from the “mother country”, England, when ancient custom was to take action in the name of the King, qui tam.
Pike argued that a prime benefit of bounties was to ensure legal representation for whistleblowers, because if lawyers knew that they could get a large pay out, they would be more willing to work contingently (or in plain English, on a no win, no fee basis).
Importantly, Pike did not explain to the audience the vagaries of the bounty system and the minimum financial recovery thresholds that whistleblowers have to fulfil to qualify for a reward, which in reality means that only a tiny minority are rewarded.
This leaves many genuine whistleblowers with no redress. It is possible under the US bounty system to be a bona fide whistleblower who suffers severe reprisal, who loses their livelihood and suffers longterm economic insecurity, but be left with zero redress.
Despite this reality, Pike described the model as “phenomenally successful”. This is possibly more of a comment from the point of view of the bounty hunting industry, and to an extent, the State.
Pike stated that the model is designed to recover money for the State, and indicated that it is therefore a problem when whistleblowers raise concerns about the State itself. His commented that federal whistleblowers might find themselves in prison.
He did not inform the audience of the existence of the the US Office of Special Counsel which looks after federal whistleblowers, who whistleblow about the State. This agency would be of less interest to bounty hunting law firms because it does not financially incentivise whistleblowing and operates a lean public sector model of restitution. It restores whistleblowers to the position that they would have occupied but for the whistleblowing, and no more, and it can ensure non-financial redress.
The whistleblower on the WhistleblowersUK panel suggested that bounties could perhaps be capped.
This reminded me of a past quote from Mary Inman who upon discovering Brits’ “visceral” dislike of the idea of paying whistleblowers, suggested that the bounty model could be made more culturally acceptable by capping rewards:
And will this proffer of capped rewards survive the implied intention to pursue large and eye-catching bounties, mentioned in the above joint document published only last month by WhistleblowersUK, Constantine Cannon, and Kohn, Kohn and Colapinto LLP?
Alongside Pike, Folashade Adeyemo also spoke about restitution and by this she appeared to mean financial reward. She also used the words “recognition” and “acknowledgment”.
Mostly, Adeyemo’s contribution consisted of different ways of talking about financial transaction. For example:
“Compensation, not payment for informing, but recognising the value of that information”.
There was no clear discussion of non-financial redress.
Susan Kramer former APPG chair, who employs WhistleblowersUK’s CEO as a researcher at the House of Lords spoke on how the APPG and she have garnered interest from members of parliament. She anticipated that the Bill would fall again but made it clear that the campaign would continue.
Of note, Kramer appeared not to be familiar with the details of her own Bill and initially stated that people could have their claims dealt with by either the proposed Office of the Whistleblower, or by the Employment Tribunal if they preferred.
This would actually not be possible under Kramer’s private member’s Bill, which repeals PIDA and provides no alternative path to litigate whistleblowing cases in the Employment Tribunal.
Georgina Halford Hall WhistleblowersUK CEO stepped in to state that the whistleblowing element would be dealt with by the proposed Office of the Whistleblower but other heads of claim such as discrimination would need to be presented to the Employment Tribunal.
An important question from the audience about public sector employees did not receive a satisfactory answer. The panel was asked how their Bill would benefit public sector whistleblowers and if public servants would effectively be paid for information.
Either panel members did not appreciate that or did not wish to address it, because the response did not address this principle.
Folashade Adeyemo instead replied:
“Why do we need to incentivise? Valuable information that will save lives, by our very nature as humans, if there’s no incentive, people won’t come forward”
All the talk I heard was about recovering money from frauds and SEC’s 10 to 30% bounties from recovered money.
I heard almost nothing about protecting the public from harmful health and social care, excepting a very few broad comments about saving lives, with no particularisation.
My impression was that the APPG and WhistleblowersUK wish to throw as many nice words as they can at the concept of monetising information and bounty hunting.
As in the words of WhistleblowersUK, Constantine Cannon, and Kohn, Kohn and Colapinto LLP :
“The real sticking point remains the idea of rewarding people for doing the right thing. The UK remains publicly queasy when it hears the word “reward” in the same sentence as “whistleblowing”. However, when we change “reward” to “compensate” or “restitution” attitudes change. No one can dispute the importance of fairness and that whistleblowers should not suffer for doing the right thing.”
So when you hear “restitution”, do not forget that the Whistleblowing APPG, WhistleblowersUK and the substantial corporate power behind them, are talking about financial rewards and the billion dollar bounty hunting industry led by lawyers.
Any financial reward that exceeds fair compensation for loss, and is calculated on a percentage is still bounty, capped or not.