By Dr Minh Alexander, NHS whistleblower and former consultant psychiatrist 26 September 2016
Robert Francis has u-turned on accountability for reprisal against NHS whistleblowers, even though he acknowledged it constitutes serious misconduct.
The public inquiry by Robert Francis into grave care failings at Mid Staffordshire NHS Foundation trust, published February 2013, saw harrowing examples of negligence and wilful blindness. There were many warnings about the failings, which were not heeded. A culture of fear was reported and staff who raised concerns experienced reprisal and suppression.
Arising from his findings, the then Mr Robert Francis was originally bullish about the need to protect NHS whistleblowers.
He recommended that it should be a criminal offence for any health worker to obstruct others trying to fulfil their duty of candour to patients and families. [1]
He emphasised in an interview with the Nursing Times that it was necessary to be absolutely firm in deterring whistleblower reprisal:
“I have called for a statutory duty of candour that trusts tell the truth to regulators and that there should be criminal sanctions if there’s willful obstruction of anyone performing their duties and informing their trusts about concerns to patients.
“That is about as rigorous protection of whistleblowers as you can imagine, and that’s what I intended,” he said.” [2]
In January 2014, the theme continued when he publicly commented that “oppressive behaviour” and whistleblower reprisal at Paula Vasco-Knight’s former trust, South Devon Healthcare, should not be tolerated:
“It is important that no tolerance is afforded to oppressive managerial behaviour of the sort identified only last week by an employment tribunal in the South West, which victimises staff who raise honestly held concerns.
“Every such case is hugely damaging to the confidence of other staff who are contemplating raising concerns. It is clear that there is much to do in this area.” [3]
The bullishness continued when Francis gave evidence to Health Committee in February 2014:
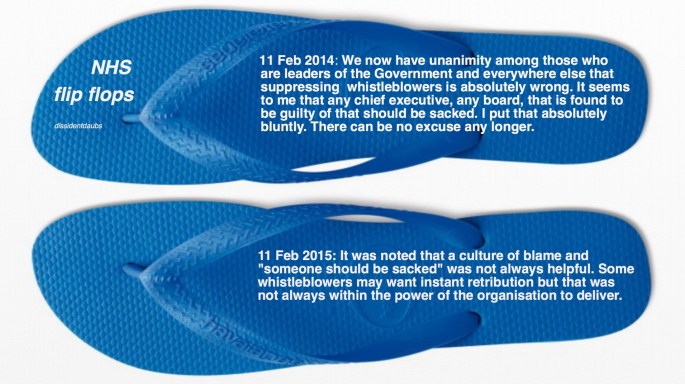
“In so far as whistleblowers are concerned, I am afraid my answer is very blunt about that. We now have unanimity among those who are leaders of the Government and everywhere else that suppressing whistleblowers is absolutely wrong. It seems to me that any chief executive, any board, that is found to be guilty of that should be sacked. I put that absolutely bluntly. There can be no excuse any longer. If you want culture change, if a step or two like that could be taken—and it is far from me to comment, but it may be there are some opportunities out there—then I would suggest that that ought to be done.” [4]
By 4 June 2014, it was announced that Francis had been appointed to the Care Quality Commission as a Non Executive Director. [5]
On 13 June 2014 we were told that Mr Francis would become Sir Robert. [6] (In March 2013, Private Eye had been critical of Francis regarding the lack of individual accountability for the grave failings at Mid Staffs, and had baldly asked: “Knighthood for a whitewash?”). [7]

On 24 June 2014, Jeremy Hunt announced that Francis would be heading a review of NHS whistleblowing, dubbed the Freedom to Speak Up Review.
By 11 February 2015, when the Freedom to Speak Up Review was published, Francis had softened considerably.
He suggested that the system response to managers who victimised whistleblowers should not be too harsh, and he replaced his previous comments that leniency was bad for culture with a claim that holding erring managers to account might add to blame culture:
“7.5.5 A number of the contributors suggested that if people were seen to be held to account this would send a powerful and positive message to other staff.
7.5.6 However, there is another side to this which must be considered. Managers are just as vulnerable as other staff to the effects of the culture in which they work, and the pressures which are imposed on them. As stressed by some employers and their representatives a ‘just’ culture is equally as necessary for managers and leaders as it is for staff raising concerns. The consequence of an uneven approach could be a worsening blame culture for staff and a loss of talented managers from the NHS.” [8]
These comments misrepresented the concept of ‘just culture’, which in fact requires sanctions for recklessness, cover ups and other deliberate wrongdoing.
Francis even appeared amnesic of his own past recommendations for criminal sanctions [1], when he made this comment about some contributors’ calls for whistleblower reprisal to be criminalised:
“A small number even wanted to see criminal and custodial sentences.”
Instead of hard reform, Francis essentially opted for trust in the power of persuasion and appealing to people’s better nature to change culture.
This was despite the fact that Robert Francis acknowledged that reprisal against whistleblowers should be seen as a form of “serious misconduct”. It was also despite the fact that his lead researcher for the Freedom to Speak Up Review Prof David Lewis, Professor of Employment Law and a whistleblowing expert, is a proponent of criminal sanctions to deter reprisal. Of note, Prof Lewis robustly and publicly reiterated his views four days after Francis’ report was published. [9] On the tail of a recent conference on whistleblowing and blacklisting, at which much sobering evidence of establishment wrongdoing was presented, Prof Lewis again spoke out publicly on the need for criminal sanctions. [10]
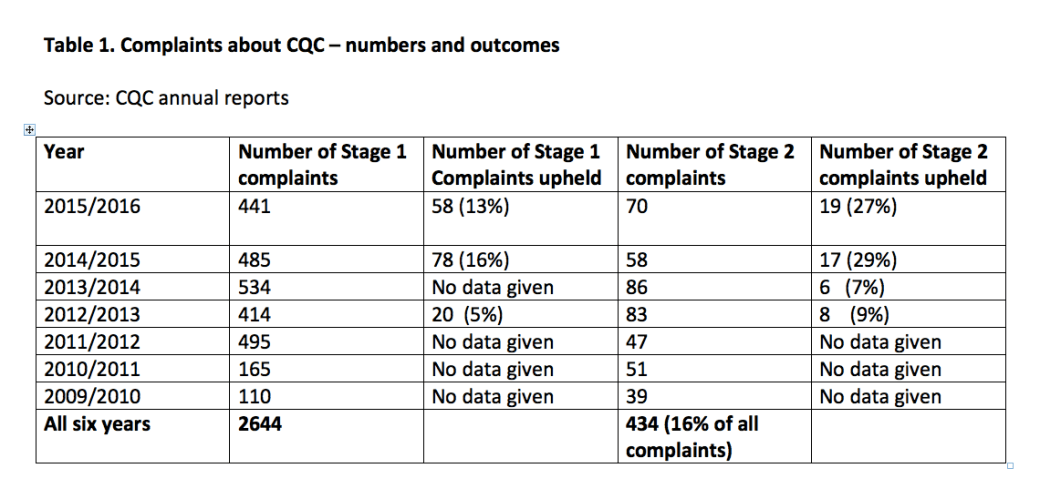
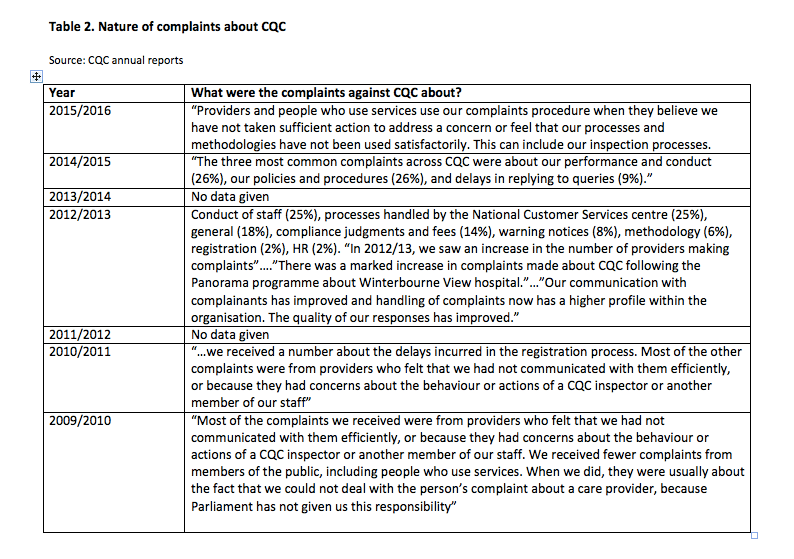
Instead of substantive reform of the law, Francis entrusted oversight of managerial misconduct against whistleblowers to the CQC’s prosecution of the new Fit and Proper Person Regulation (FPPR). In the hands of the CQC, this has proved to be a monumental flop, [11] such that the inept CQC was compelled four months ago to announce a review of itself on this matter. [12]
What we may never know is the extent to which the Department of Health interfered with the Freedom To Speak Up Review. I and other whistleblowers who participated were certainly conscious of Whitehall minders, assigned and omnipresent, right up to the day of publication and launch. Francis’ researchers were not invited to the launch. Whistleblowers were invited but were separated from the press conference by a matter of some miles, and only given a copy of the report at the very last minute. Francis was whisked in and out for a brief audience, and left us to attend the discussion about his report in parliament. To my mind, when Francis was challenged by whistleblowers that he had not done enough, he seemed uncomfortable.
In the face of ongoing and serious CQC failure, with concerns emanating from all quarters, Francis is now making more pointed comments again:
“Non-executive director Sir Robert Francis QC asked if the regulator should “reflect… on whether there is a wider mismatch or not between the policies that emanate from this board and the executive team and what is actually happening on the ground, as that is what we look for when we inspect a hospital”. He added that it was “probably not only in this field” that such a mismatch was happening.”[13]
It would have been wise to acknowledge this before abandoning the hard reform, which he had originally and correctly identified was essential.
In November 2013, Francis chided clinicians for ‘self-interest’ in failing to report concerns, and he called on frontline NHS workers to reassert their professionalism:
“This requires a visible and sustained commitment on the part of all medical and clinical staff to re-assert their professionalism.” [14]
These are fine but empty – and ultimately unfair – words if the system totally fails frontline staff when they dare to ask for safe standards of care. However, by focussing on front line staff, they do serve to distract from the culpability of politicians and senior officials who are ultimately responsible for suppression.
Items to cross-reference
Take a look at some of these Employment Tribunal judgments and witness statements about notorious NHS whistleblowing cases, and see if you think it’s right for senior NHS managers to be let off for serious cover ups:
Dr Kevin Beatt v Croydon Health Services NHS Trust
Click to access home
Clare Sardari and Penny Gates v South Devon Healthcare NHS Foundation Trust and Torbay and Southern Devon Health and Care NHS Trust
Click to access home
Hayley Dare’s ET witness statement
Click to access home
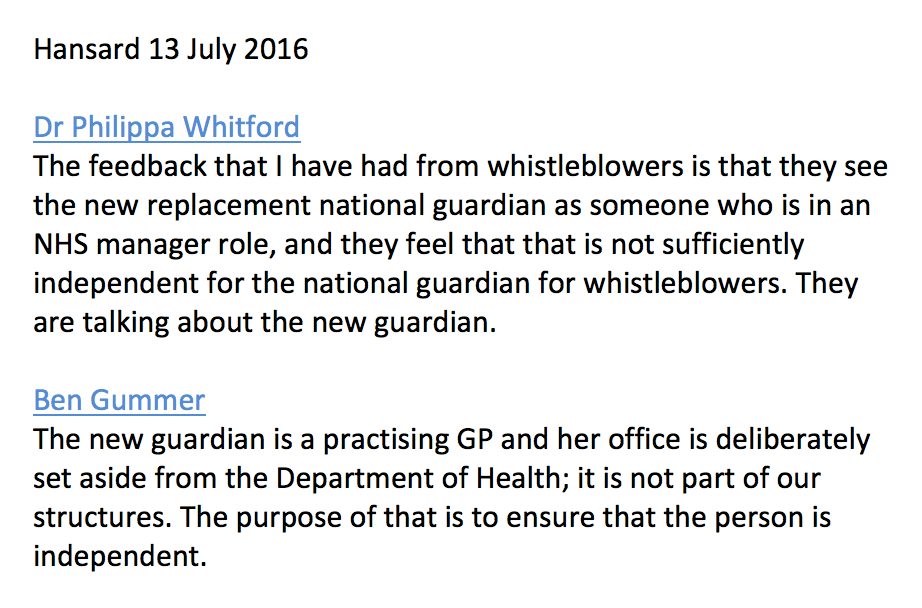
If you want details regarding the ineffectiveness of the centre piece of Francis’ and Hunt’s plans for persuading the NHS to do better, the toothless National Guardian’s office, you can find them here:
https://minhalexander.com/2016/09/24/no-one-believes-jeremy-hunt-on-patient-safety-or-whistleblowers-not-even-his-own-appointees-unmasking-the-faux-national-guardian-office/
UPDATE 20 NOVEMBER 2018 – OTHER RELATED ITEMS:
A Serious Health Warning about the Freedom To Speak Up Project: What all NHS staff should know before they whistleblow
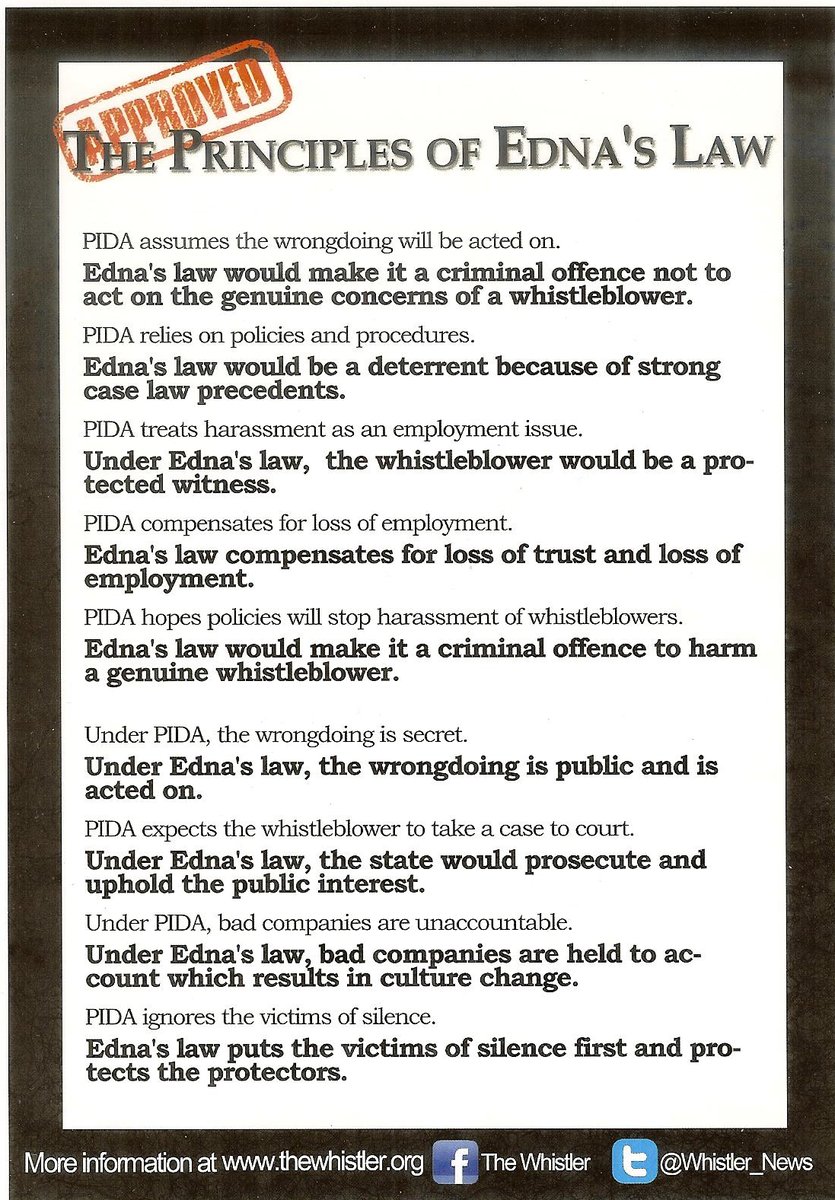
Replacing the Public Interest Disclosure Act (PIDA)
UPDATE 21 DECEMBER 2018
In his report of the Freedom To Speak Up Review, Robert Francis eschewed managerial regulation in favour of a trial of CQC Regulation 5 Fit and Proper Persons, which is supposed to be enforced by his own organisation the Care Quality Commission. However, this has failed conclusively and the PHSO has partially upheld a complaint about CQC’s mishandling of the Paula Vasco-Knight FPPR. CQC protected and enabled the recycling of Vasco-Knight as an NHS director, even though Francis had told parliament that wilful obstruction of whistleblowers by chief executives was a sacking offence.
PHSO has pulled its punches and covered the government’s back by claiming that Vasco-Knight might still have passed the FPPR test if CQC had applied a fair process, despite a damning Employment Tribunal judgment. The latest events are summarised here:
Sorry is the hardest word: CQC, Paula Vasco-Knight and Regulation 5 Fit and Proper Persons
References
[1] Recommendation 183 of the Report of the Public Inquiry into Mid Staffordshire NHS Foundation Trust
“Criminal liability
It should be made a criminal offence for any registered medical practitioner, or nurse, or allied health professional or director of an authorised or registered healthcare organisation:
- Knowingly to obstruct another in the performance of these statutory duties;
- To provide information to a patient or nearest relative intending to mislead them about such an incident;
- Dishonestly to make an untruthful statement to a commissioner or regulator knowing or believing that they are likely to rely on the statement in the performance of their duties.”
Click to access 0947.pdf
[2] Francis calls for new protection for whistleblowers, Shaun Lintern, Nursing Times 11 February 2013
https://www.nursingtimes.net/news/reviews-and-reports/francis-report/francis-calls-for-new-protection-for-whistleblowers/5054780.article
[3] Francis criticises Vasco-Knight trust, Judith Welikala, Health Service Journal, 7 February 2014
https://www.hsj.co.uk/sectors/acute-care/francis-criticises-vasco-knight-trust/5067807.article
[4] Oral evidence by Robert Francis to Health Committee 11 February 2014
francis-oral-evid-hsc-11-feb-2014
[5] CQC welcomes new board members 4 June 2016
http://www.cqc.org.uk/content/cqc-welcomes-new-board-members
[6] Robert Francis knighted in Queen’s birthday honours, Judith Welikala, Health Service Journal, 16 June 2014
https://www.hsj.co.uk/home/robert-francis-knighted-in-queens-birthday-honours/5071974.article
[7] Return to the killing fields. A chronicle of deaths foretold. Dr Phil Hammond, Private Eye March 2013
private-eye-mid-staffs-final
[8] Report by Robert Francis of the Freedom to Speak Up Review 11 February 2015
http://webarchive.nationalarchives.gov.uk/20150218150343/https://freedomtospeakup.org.uk/wp-content/uploads/2014/07/F2SU_web.pdf
[9] Lack of support for whistleblowers is a disgrace. Letter by Prof David Lewis to Guardian, 15 February 2016
“The Guardian has a laudable track record of supporting whistleblowing. However, in commenting on the impact of the Francis report on the culture of speaking up in the NHS (Editorial, 12 February), you demonstrate a rather conservative approach to legislative reform. First, there is no mention of possible criminal sanctions. Citizens who break the Official Secrets Act commit an offence, so why shouldn’t those who victimise people raising concerns in the public interest? TheProtection from Harassment Act can be invoked if the narrow definition of harassment is fulfilled, but, in my opinion, outlawing any form of retaliation against whistleblowers would send out a valuable message about what society expects.
Second, you do not point out that only “workers” are covered by our whistleblowing legislation. However, it is clear that those who are in a position to raise concerns may not have this status – for example, patients and their families. Other countries now recognise the role that the public can play in exposing wrongdoing; in this important respect, the UK no longer provides an international model.
Professor David Lewis
Director, Whistleblowing research unit, Middlesex University”
https://www.theguardian.com/society/2015/feb/15/whistleblowers-should-law-punish-hospital-bosses
[10] ‘Whistleblowers should be encouraged, protected by law’, Antonia Filmer, Sunday Guardian, 18 September 2016.
“Prof Lewis proposes… the outlawing of discrimination against whistleblowers at the point of hiring and making retaliation against whistleblowers a criminal offence. Prof Lewis also believes there is a case for establishing a specialist body such as a Public Interest Disclosure Agency. Such a body might receive disclosures, arrange for their investigation by an appropriate authority and ensure that advisory and counselling services are available, protect whistleblowers from reprisals”
http://www.sundayguardianlive.com/world/6512-whistle-blowers-should-be-encouraged-protected-law
[11] CQC’s Fit and Proper Parade. Dr Minh Alexander, 29 July 2016
https://minhalexander.com/2016/09/24/cqcs-fit-and-proper-parade/
[12] CQC to review whether fit and proper person rule ‘needs to change’, Will Hazel, Health Service Journal 24 May 2016
https://www.hsj.co.uk/topics/policy-and-regulation/cqc-to-review-whether-fit-and-proper-person-rule-needs-to-change/7005046.article
[13] CQC told to change culture after data loss ‘never event’, Sharon Brennan, Health Service Journal, 23 September 2016
https://www.hsj.co.uk/topics/technology-and-innovation/cqc-told-to-change-culture-after-data-loss-never-event/7010763.article
[14] Mid Staffordshire – some reflections for clinicians, Robert Francis QC, Trends in Urology and Men’s Health, November/December 2013
francis-mid-staffordshire-some-reflections-for-clinicians-362_ftp