Summary: An as yet unpublished Kings Fund review about poor leadership at HSIB has resulted in the agency being stripped of its maternity investigations by the Department of Health and Social Care. Was the affair in any way an attempt by the government to control a mounting maternity personal injury bill, because HSIB investigations had helped to establish liability?
HSIB, the investigatory arm of the regulator NHS Improvement was one of Jeremy Hunt’s cynical and superficial ‘patient safety’ gestures created in response to pressures over unresolved patient safety issues following the Midstaff Scandal. He established it whilst he continued to defund and undermine the NHS.
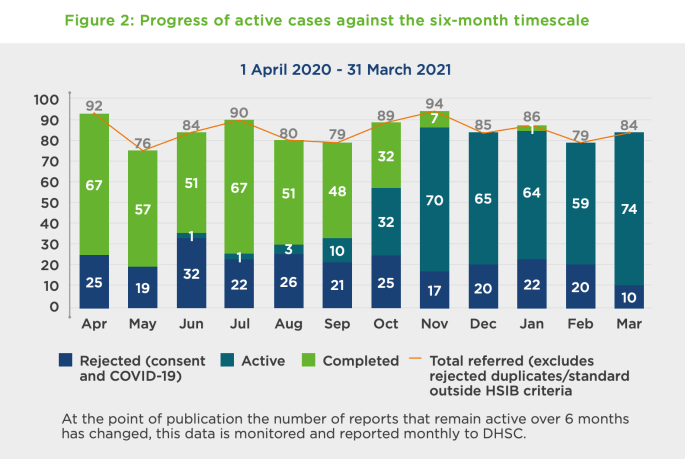
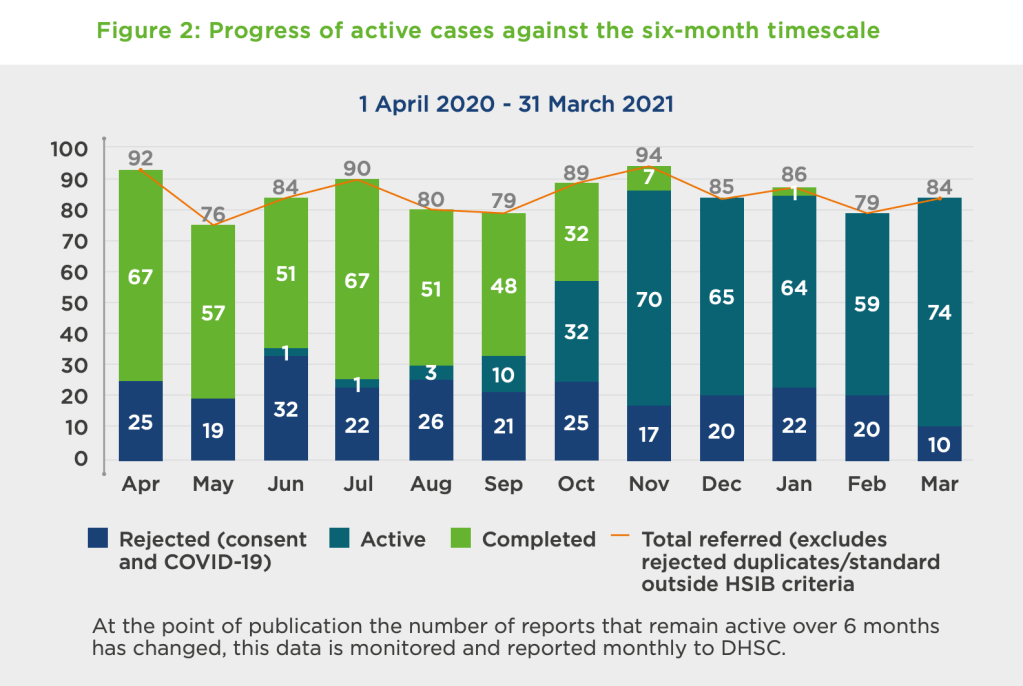
Significantly, the latest scandal led to HSIB being stripped of its maternity investigations – an area which had been mushrooming with the revelations at Shrewsbury and Telford NHS Trust, with huge liability implications for the NHS and the government. HSIB had been undertaking about 1000 maternity investigations a year.
“In announcing his retirement Keith Conradi, Chief Investigator says:
“It has long been my intention to retire at 60 while my health enables me to participate in competitive triathlon.”
Other senior departures from HSIB were also reported.
When HSIB’s creation was first announced, I made attempts to obtain objective evidence of whether aviation and AAIB were truly a paragon of safety culture as Hunt had claimed. I asked for old AAIB staff survey results, but was repeatedly blocked by the government. This was despite the ICO ruling that there was no good reason for the Department of Transport to withhold the information. Litigation continues on the matter with the ICO opposing the government. It is before the Tribunal again in April.
Before HSIB became operational, I had a foretaste of things to come when I tried to engage its players in ensuring effective whistleblowing governance. They clearly knew little about whistleblowing but seemed to have minimal interest in becoming more competent. The venture seemed very insular and clubby. After being told that someone with no visible whistleblowing expertise would sort it all out, I made a challenge to the boys’ club culture. This was met with uncomprehending huffiness by one of the safety luminaries backing the project. No doubt those grand men will quickly forget their poor judgment and move on to the next vanity project dangled before them by politicians.
After the major scandal broke this January, I asked NHSI for a copy of the Kings Fund review and other information about NHSI’s handling of the HSIB affair. However, NHSI has not yet answered despite intervention from the ICO and an exchange of correspondence with Andrew Morris who said he had asked his FOI team to expedite the matter.
It is a failing by NHSI that the Kings Fund review of HSIB is not already published. It was commissioned in secret and remains withheld. NHSI bears ultimate responsibility for HSIB’s failure.
Indeed, was HSIB’s leadership substantially worse than the abusive, failing NHS trust managers than NHSI protects and recycles on a daily basis?
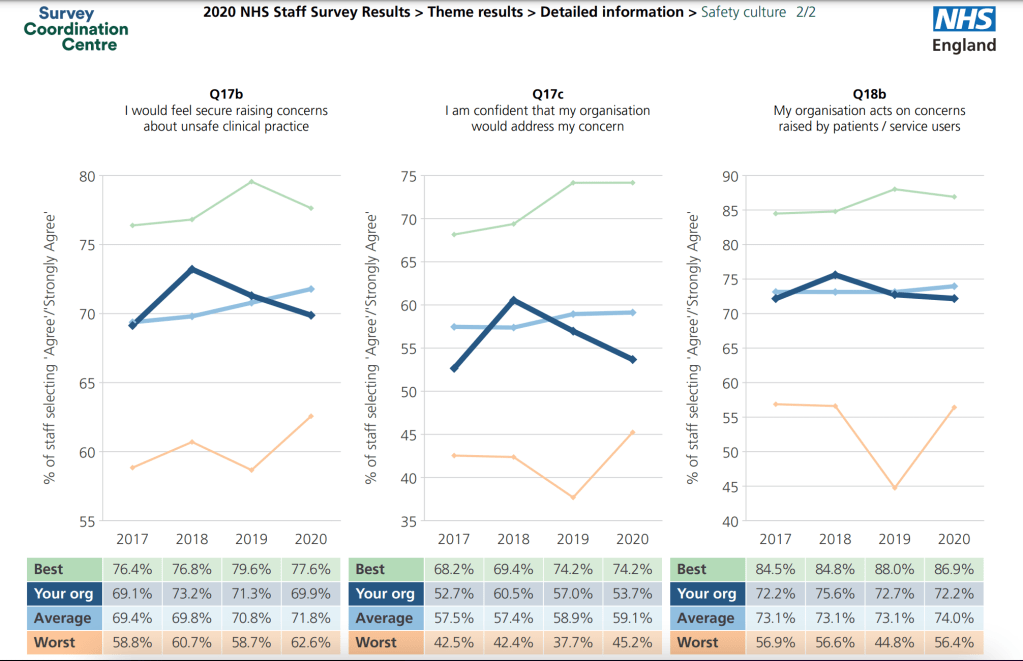
Indeed, how do we know if HSIB’s culture was any worse than that of NHSE and NHSI’s? Neither NHSE or NHSI routinely publish their own staff survey results and are frequently criticised for bullying provider organisations.
Notwithstanding any justified criticism of the obviously poor leadership of HSIB; was the decapitation of the agency in any way a government attempt to block transparency about NHS safety failings? Was it merely a pretext to control a huge bill from maternity injury pay outs?
And what of NHSE/I’s hireling, the Kings Fund? Did it give the HSIB leadership and its staff a fair hearing?
The King’s Fund board of trustees has traditionally been populated with the powerful, connected and sometimes recycled. I previously asked its former Chair Sir Christopher Kelly, former Department of Health Permanent Secretary, if he was one of the referees for Jo Williams the disgraced former Chair of the CQC when she applied to re-enter the NHS as Chair of Alder Hey NHS Foundation Trust:
A doctor at Smith’s trust spoke up critically about Smith’s appearance on Strictly: “Clare Gardner launched an online petition, reading: “She is the chair of the largest NHS Trust in the UK, during a time of major crisis i.e. the second Covid-19 wave.“We are already in a Tier Two lockdown. I am a haematologist within the Trust she apparently chairs.“Our Chief Executive Dr David Rosser has made numerous statements to the press recently, describing the fear and foreboding we all sense towards rising cases.”“Now that we are facing a similarly perilous situation, she has swanned off to London to dance.“This is a dereliction of duty.“If ever there was a time to have figureheads in place for NHS organisations that are struggling, it is now.“Jacqui would rather wear sequins than look after her charge.”
One can only hope that Dr Gardner is unharmed and still prospers.
Smith was also chair at UHB during Mr Tristan Reuser’s whistleblowing ordeal. She failed to answer a request in August 2021 for data about the trust’s abusive handling of the Reuser litigation and about FPPR process regarding her chief executive, despite a reminder. The matter is now with the ICO.
The Kings Fund churns out forests of prim admonishments about how NHS leaders should behave. It calls often for compassionate leadership. It positions itself in the market as a seller of advice and reviews on how to do it right.
Some of the Kings Fund’s prominent figures have sometimes worked symbiotically with the equally virtue signalling National Guardian’s Office.
So I attempted to check out the actual quality of the goods and asked the Kings Fund to share its own staff survey data. This was because the first thing noticeable is that this data is not published.
After one email to its comms team, two emails to its CEO Richard Murray and one email finally to its Chair Lord Kakkar, I received an acknowledgment from the CEO’s office. This was followed by a minimal substantive response from the Kings Fund comms team on 3 March, giving headline figures for amalgamated years and no staff survey reports:
“Dear Dr Alexander
Thank you for your emails about staff wellbeing at The King’s Fund. We don’t have a record of your original inquiry to this account so please accept our apologies for the delay in responding and treat this as a response to this and the emails you subsequently sent to Richard Murray.
The King’s Fund has been running staff satisfaction surveys since 2008, usually every other year. They are managed on our behalf by an organisation called the Leadership Factor so that scores and narrative can be provided confidentially. Between 2008 and 2015 the overall satisfaction score was between 71 per cent and 78 per cent, placing us in the top quartile of organisations the company surveyed.
In 2017, we refreshed the design of the survey and included specific questions about engagement and wellbeing. In 2018, these factors scored 8.4 and 7.6 out of 10 respectively, where 10 is very satisfied. We were due to run the survey again in 2020 when the pandemic hit. At the end of 2020, we introduced regular pulse surveys in place of the full survey which included questions about health and wellbeing, levels of optimism and morale. We will run the full satisfaction survey again in Autumn 2022.
Best wishes
Gemma Umali
Press and Public Affairs Manager”
I asked for more detail, pointing out that it would be useful for example to see how minority staff groups fared.
“Many thanks for your response and the broad percentage results extracted and aggregated from past staff surveys.
It would be more useful to have actual copies of the staff survey reports from tne years in which you say the surveys were carried out.
It is hard to make much sense of broad headline results without any contextual details.
For example, the stratified results for different staff groups, (assuming that this data is collected by the Kings Fund) and particularly minority groups are important to see – as the Kings Fund itself has emphasised in the past when passing comment on the national NHS staff survey.
Your aggregation of results from different years also obscures possible variations over time.
I would be very grateful f you would share copies of the original staff survey reports.
However, if the Kings Fund does not wish to share the actual reports, would you at least be willing to share the questionnaire forms that staff filled in on the years in question?
Mamy thanks
Minh
Minh Alexander
Cc Richard Murray CEO Kings Fund
Lord Ajay Kakkar Chair Kings Fund”
At the time of writing, I have not yet received either a copy of the questionnaire that Kings Fund staff fill in, nor the original staff survey reports. I guess the Kings Fund comms folk have still got their thinking caps on. Compassionately, no doubt.
PETITION
Please click and add your signature to this petition to reform UK whistleblowing law – whistleblowers protect us all but weak UK law leaves them wholly exposed and it is a threat to public safety
1. NHS England/ Improvement eventually reluctantly disclosed a copy of the Kings Fund report on HSIB, terms of reference and associated correspondence, which showed that a rigorous investigation was never intended:
2. As discussed above, the dispatch of undesirable senior NHS managers is the exeception rather than the rule.
The number of cases of NHS England, NHSI and its predecessor bodies covering up, protecting and recycling abusive, incompetent and or dishonest NHS managers are too many to list.
But here is a striking example of former NHS CEO Paula Vasco-Knight, unpicked to show the lengths to which the protection often extends and why the HSIB case is different:
3. After leaving UHB in October 2021, Jacqui Smith took up two new NHS Chairs at Barts Health NHS Trust and Barking, Havering and Redbridge University Hospitals NHS Trust. This looks to be system preparation for a politically sensitive merger of the two trusts, which is already stirring up controversy, with Margaret Hodge stepping in.
Summary It appears from anonymous letters that staff at Hinchingbrooke Hospital may be whistleblowing about care failure surrounding A&E. The trust’s response so far is one of bizarre minimalisation, despite acknowledging some care failure. The trust’s CEO appears to think that anonymous letters are a sign that staff feel able to raise concerns, which hardly bodes well for organisational learning.
Like the rest of the NHS it has suffered the enormous stresses of the mismanagement of the COVID19 pandemic by the government.
It is now disturbed by anonymous whistleblowing by parties unknown. Disclosures have been made to trust managers and to at least one patient affected by a failure of tetanus management.
Unvaccinated patients presenting with injuries should have had their vaccinations histories checked and been given tetanus booster shots but allegedly, some did not.
This has been confirmed in one case, that of Marilyn Smith, reported by the BBC.
Ms Smith contracted tetanus after an injury in September 2021, for which she did not receive a tetanus shot. As a result she was severely unwell and hospitalised for 120 days and left with disabilities.
Two weeks after she was discharged from hospital, Ms Smith reportedly received several anonymous letters which claimed to come from:
“a group of current and previous A&E staff at Hinchingbrooke”
The letter described alleged shortcomings in her care and also claimed:
“the trust has been ignoring concerns about patient safety” and contained further allegations that related to an individual.”
The last NHS staff survey showed that the trust’s whistleblowing governance was on a downward trajectory:
The trust’s response to the BBC appeared somewhat self-contradictory.
It claimed that the trust had received and investigated a similar letter in October 2021and dismissed the concerns.
“The North West Anglia NHS Foundation Trust confirmed it had received a similar letter in October but after an investigation concluded there was no substance to the allegations about patient safety.”
“In a statement, Caroline Walker, chief executive of the trust, said they were meeting Ms Smith this week to discuss its investigation and report.
And yet the trust also conceded shortcomings in Marilyn Smith’s care:
“I would like to apologise to Marilyn Smith for the failure to identify her condition as quickly as we should have,” she said.“
Bizarrely, the trust CEO seemed to conclude that an anonymous letter was a sign that staff felt able to raise concerns:
“We welcome the fact that our staff feel able to raise concerns.
“We have worked hard, with the support of our Freedom To Speak Up Guardian, to encourage an environment where speaking up is something people can do with confidence.
“When issues are raised we take action to investigate and learn from them.”
That Olympic-Gold-level ostriching rather takes the biscuit.
This is therefore unlikely to be the last that we will hear about poor whistleblowing governance by North West Anglia.
Or about the woeful inadequacies of the Freedom To Speak Up project, which clearly does not provide a safe reporting channel when it really matters.
Declaration of interest: A member of my family has been injured on a number of occasions by Peterborough City Hospital, which is part of the above trust. We are wearily in conflict with the trust again over yet another episode of care failure, which they have admitted. Relevant to issues of transparency, the trust is overdue in responding to a subject access request for personal data, made directly to the trust CEO, which required a referral to the ICO.
PETITION
Please click and add your signature to this petition to reform UK whistleblowing law – whistleblowers protect us all but weak UK law leaves them wholly exposed and it is a threat to public safety
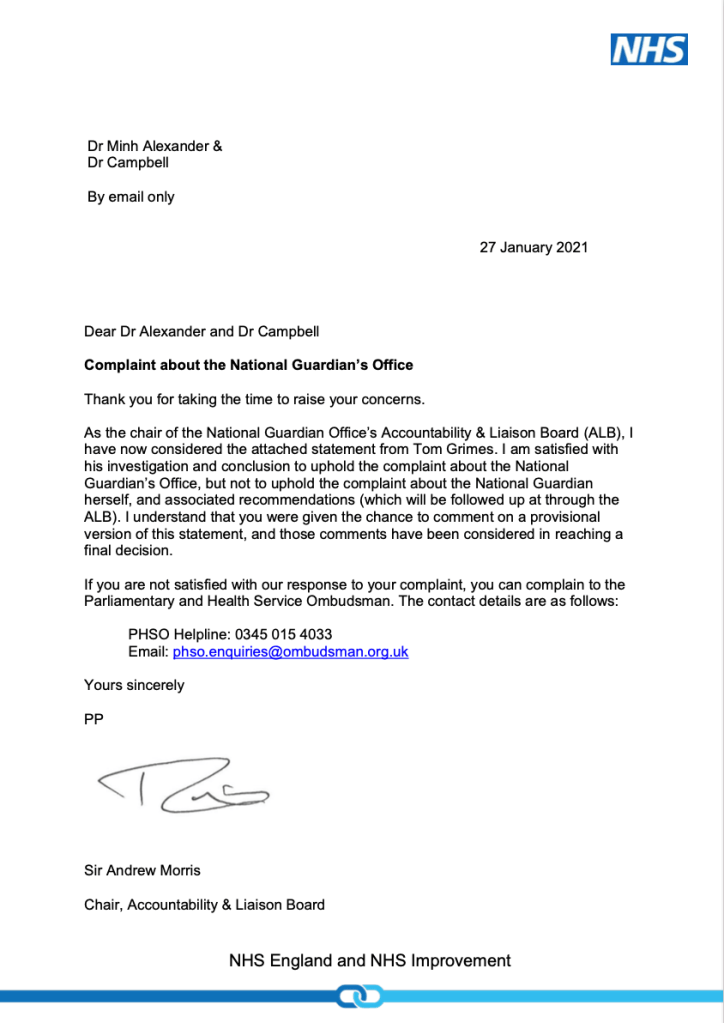
This delay included maintaining radio silence for a month even after NHS Improvement issued a final investigation report on 27 January 2021 which concluded the National Guardian’s former case review manager breached Dr Campbell’s confidentiality, and recommended that an apology be made.
NHS Improvement also recommended that the National Guardian’s Office should provide “confirmation of an improved approach to such matters in future”.
Again, no such evidence of improvement was given by the National Guardian’s Office for months despite being asked to urgently safeguard whistleblowers’ confidentiality. The request for such protection was first directed in August 2020 to Robert Francis, who has an oversight role, and then to Henrietta Hughes the National Guardian herself in December 2020. Neither responded to confirm that protective action was taken.
The lack of evidence of corrective action continued even after NHS Improvement’s recommendation of 27 January 2021 to demonstrate improvement.
A question arises of whether the silence by the National Guardian and her Office was hostile and an expression of resentment at being held to account.
On 27 February 2021 I protested about the lack of apology and learning to Ian Trenholm who is effectively the National Guardian’s line manager.
Two days later, an apology to Dr Campbell arrived from the National Guardian’s Office.
The apology did not come from the National Guardian but was delegated to her Head of Office, Russell Parkinson.
Parkinson did not acknowledge the extraordinary delay in apologising.
He also gave limited details of improvement:
“I will therefore issue a reminder to all National Guardian Office staff about the importance of preserving confidentiality and the requirement to obtain consent before the identity of individuals are disclosed, other than when there is a legal requirement to disclose someone’s identity.”
“In addition, I will strengthen the induction process and induction material for new members of the office to ensure that a full discussion of confidentiality is had with all new starters. I will also seek to strengthen our record keeping so that it is clear what level of consent has been obtained before there is any further discussion of a case.”
Of immense concern, it is implied that the National Guardian had not taken corrective action prior to this point, thereby knowingly exposing more whistleblowers to potential harm.
This is not the accountable, responsible or meticulous behaviour one would expect as standard from a whistleblowing agency.
I have written to Russell Parkinson to ask for clearer evidence of improvement and to ask the National Guardian for related policy improvements. For example, that she should make unplanned breach of whistleblower confidentiality by her Office a disciplinary matter, to underline how seriously confidentiality will taken.
It is after all a criminal matter in some jurisdictions to reveal a whistleblower’s identity.
It is not unreasonable that a whistleblowing agency should hold itself to similarly high standards.
I have copied the letter to Henrietta Hughes’ oversight board, comprising Robert Francis and Andrew Morris, woeful though they have been.
The letter to Parkinson is provided below in the appendix.
I would advise would-be whistleblowers to be cautious, to get everything in writing, to request personal data through subject access request if concerns arise about any impropriety and not to assume that those in authority will wish you well or will look after your interests.
UK whistleblowing law’s many faults include the fact that it does not specifically protect a whistlblower’s confidentiality and identity.
If you have not already done so, please help drive change by signing and sharing this petition to parliament for law reform.
LETTER 12 MARCH 2021 TO RUSSELL PARKINSON, HEAD OF OFFICE, NATIONAL GUARDIAN’S OFFICE
BY EMAIL
Russell Parkinson
Head of Office
National Guardian’s Office
12 March 2021
Dear Russell,
The National Guardian’s response to the breach of whistleblower confidentiality by her Office: corrective action
Thank you for your letter of 1 March 2021 to Dr Campbell and myself acknowledging the outcome of NHS Improvement’s investigation which concluded that the National Guardian’s Office breached Dr Campbell’s confidentiality.
I write chiefly with the aim of seeking reassurance that:
Future whistleblowers’ confidentiality will be safely protected by the National Guardian’s office and that more detail will be shared of the intended service improvements mentioned in your letter.
Unplanned breach of whistleblower confidentiality by anybody at the NGO will be treated as a disciplinary matter. The NGO will admit to any unplanned breaches immediately and it will also support any affected whistleblower and help to mitigate harm.
Planned breaches of whistleblower confidentiality will be rare, genuinely justified and properly managed, with support for the whistleblower
There will from here on be proper transparency and accountability regarding the Office’s interaction with whistleblowers’ employers. The NGO’s communications with employers will in future be fully documented and details will be shared with whistleblowers. There will be no clandestine, undisclosed communications.
In future, the National Guardian’s Office will apologise promptly as soon as it becomes aware of any failings, and in particular it will mitigate serious risks at the earliest opportunity instead of waiting months for complaints investigations to be concluded.
The National Guardian will conduct a wider review of Simon Pook’s work given the findings that he breached confidentiality and had undisclosed contact with an employer.
The National Guardian will ensure there is regular audit of the work of her office to ensure that there is adherence to operational standards.
This letter does not mean that Dr Campbell has accepted the outcome of NHS Improvement’s complaint investigation, and is without prejudice to any further steps he may decide to take.
I lay out my requests more fully as follows:
More details of proposed improvements by the National Guardian’s Office
I would be grateful for details of the planned strengthening of the National Guardian’s systems, with respect to this assurance in your letter:
“In addition, I will strengthen the induction process and induction material for new members of the office to ensure that a full discussion of confidentiality is had with all new starters. I will also seek to strengthen our record keeping so that it is clear what level of consent has been obtained before there is any further discussion of a case.”
Apologising promptly
I am glad that the National Guardian’s Office has finally apologised to Dr Campbell.
May I ask why it took so long?
Firstly, there was a shocking lack of empathy in Simon Pook’s response of 14 June 2019 to a distressed email by Dr Campbell when he discovered that his confidentiality had been breached by the National Guardian’s Office.
Breach of whistleblower confidentiality is an incredibly serious matter and the lack of apology is all the worse for this.
NHS Improvement’s investigation concluded that Simon Pook former NGO case review manager likely broke Dr Campbell’s confidentiality to his employer and Mr Pook reportedly accepted this.
Did Simon Pook inform the National Guardian or anyone else at the National Guardian’s Office in June 2019, that Dr Campbell’s confidentiality had been breached?
If he did, who at the National Guardian’s Office was aware of the breach at that point, and what was the organisational response?
Who at that point was the most senior person who was aware of the confidentiality breach?
Why was no apology provided by the National Guardian’s Office when I brought the matter to Robert Francis attention in August 2020?
I presume Robert Francis liaised with the National Guardian’s Office about the confidentiality breach at this point, but please confirm that he did so, when and whom he informed.
Why was an apology still not provided by the National Guardian’s Office when NHS Improvement’s final report was issued on 27 January 2021, with the formal finding of confidentiality breach?
An apology has only come now after I wrote to Ian Trenholm about the lack of an apology.
NHS policy is to express regret and say sorry straightaway to patients and families when things go wrong, and the NGO should act in accord with this.
Request: Please could the National Guardian’s complaint policy be amended to specifically reflect that an apology will be given promptly as soon as it is clear that there has been a failing, whether or not a formal complaint investigation has been completed.
Acting urgently on serious risks
It is disappointing that the National Guardian’s Office is only acting now to strengthen its systems to prevent unjustified breaches of whistleblower confidentiality when it has known about the breach of Dr Campbell’s confidentiality for months if not longer.
This implies that other whistleblowers have been potentially and avoidably exposed to similar risk. This not only affects the whistleblowers but the patients and co-workers who depend upon them.
Good whistleblowing governance focuses on promptly addressing the primary concerns raised by a whistleblower and not diverting into or delaying through adversarial processes. The National Guardian should act in this spirit.
Request: Please can the National Guardian’s complaint policy explicitly commit the National Guardian to correcting any future failings at the earliest stage possible, instead of waiting until a formal complaint investigation is concluded before acting.
Policy for managing breaches of whistleblower confidentiality
At present, the FAQs on the National Guardian’s website state that in all cases the National Guardian’s Office will tell whistleblowers if it decides to breach their confidentiality
“20. How will the NGO protect my confidentiality when I submit a case for review?
Wherever possible, the NGO will seek to protect the confidentiality of individuals who refer cases to it. In most circumstances the NGO will ask a referrer for their consent before discussing their case with their employer or any other agency. The office will only share information contained in a case review referral where there is a need to protect individuals from possible harm, for example where the matter relates a safeguarding issue. In all circumstances, the NGO will let referrers know when they have discussed or shared information about their case with another organisation.” [my emphasis]
However, the National Guardian’s Office did not inform Dr Campbell that it breached his confidentiality. Nor did it offer Dr Campbell any support with the consequences of its breach of confidentiality.
Request: May I suggest that the National Guardian’s policy includes an additional commitment that wherever the National Guardian’s Office breaches a whistleblower’s confidentiality, it will urgently provide the whistleblower with support to manage any risk or harm that arises from this.
Also, the policy should indicate that if a breach of confidentiality is planned and deliberate, the National Guardian’s Office should if at all possible inform the whistleblower beforehand that their confidentiality is about to breached. This would give the whistleblower the greatest chance of mitigating the harm that any breach of confidentiality might cause.
This would be consistent with NHS Improvement’s recommendation:
“In future, the NGO would benefit from taking greater care ahead of contacting individuals at an organisation about a FTSU case, by ensuring it notifies the individual who has spoken up of its intentions, and allow the individual reasonable opportunity to express any concerns they may have about the proposed course of action.”
In my view, the only valid exception to warning a whistleblower of a planned breach of their confidentiality is if they are the subject of any safeguarding concerns and non-disclosure is necessary to preserve evidence.
Where there are deliberate breaches of whistleblowers’ confidentiality, there must by policy be a full written account of the risk justification for doing so.
The National Guardian’s form, that whistleblowers complete when requesting a case review, should be amended to reflect the above policy changes.
May I also suggest that the National Guardian’s procedural documents be amended to include a clear policy statement to all who work at the NGO including the National Guardian, that breaches of whistleblower confidentiality without just cause are a disciplinary matter.
Record keeping and transparency about communication with whistleblowers’ employers
A disturbing aspect that emerged from NHS Improvement’s investigation of the breach of Dr Campbell’s confidentiality is the poor documentation of telephone calls by the National Guardian’s Office to Dr Campbell’s employer.
On 20 November 2020, NHS Improvement wrote:
“On 3 June 2019, the case review manager contacted the trust’s FTSU Guardian to arrange a telephone discussion, but the topic of conversation was not specified in the email. Shortly afterwards it appears that a phone call took place. I have not been able to locate a note of such a call.”
“On 14 June the National Guardian had a telephone call with the chief executive and Dr Campbell’s name is referred to in her note of the call.”
The fact of one of these calls and the details of both these calls by Simon Pook and the National Guardian were not disclosed to Dr Campbell.
The poor documentation and lack of transparency are unaccountable practice, which does not help with confidence nor demonstration of good faith and impartiality by the National Guardian’s Office.
Poor record keeping by the National Guardian’s Office may also disadvantage whistleblowers in any future processes such as defending themselves against retaliatory charges by employers or any legal action that they may be forced to take.
The poor record keeping is of greater significance given that the National Guardian’s Office has demonstrated that it is aware of the sensitivity and importance of good whistleblowing records through its existing guidance to trust Freedom To Speak Up Guardians:
“Be aware that your records may be requested weeks, months or even years after their creation and this should be taken into account when setting up your systems.”
In the NHS, it is now quite normal for clinical letters between health professionals to be shared with patients. The National Guardian’s Office should act in this spirit of accountability and transparency.
Request: Please could the National Guardian amend her policies to ensure that her Office’s contacts with whistleblowers employers are properly documented and that the details of such communications are routinely shared with whistleblowers.
Further investigation needed
You acknowledge that Simon Pook was sufficiently experienced and trained to be reasonably expected to know that he should not breach Dr Campbell’s confidentiality, but that he seemingly did so nevertheless.
This is particularly serious and leads to a number of difficult questions, including whether the confidentiality breach was consciously done.
Request: Please can the National Guardian trigger a review of Simon Pook’s work if she has not already done so, to check for any other possible breaches of whistleblower confidentiality and any covert, undisclosed communication with whistleblowers’ employers.
Obviously, the proper disclosures would need to be made to any other whistleblowers whose confidentiality has been breached.
If a review has already been triggered, please advise on whether it has been completed or if not, when it will be completed.
Regular audit of practice standards at the National Guardian’s Office
Related to a wider check of Simon Pook’s work, may I ask what arrangements the National Guardian has for monitoring adherence to her Office’s policies and standards?
Are quality audits regularly carried out?
If so, what audits are undertaken and what are the specifications for these audits?
You acknowledged through Simon Pook’s example that experience and training do not always prevent failure to adhere to policy.
It is important that there is quality monitoring that can pick up failures to adhere to policy.
If audits are not regularly carried out on important matters such as standards in record keeping, seeking whistleblowers’ consent for sharing information and protecting whistleblowers’ confidentiality and identity, failures may go undetected and uncorrected.
Request: If the National Guardian does not currently have a policy of carrying out regular quality audits on the work of her Office, please advise if she will adopt such a policy.
Many thanks,
Minh
Dr Minh Alexander
Cc Dr Julian Campbell
Tom Grimes NHS Improvement lead for whistleblowing
Dr Henrietta Hughes National Guardian
Robert Francis CQC NED and member of National Guardian’s Accountability and Liaison Board
Andrew Morris NHS Improvement and Chair of National Guardian’s Accountability and Liaison
By Dr Minh Alexander NHS whistleblower and retired consultant psychiatrist, 11 March 2021
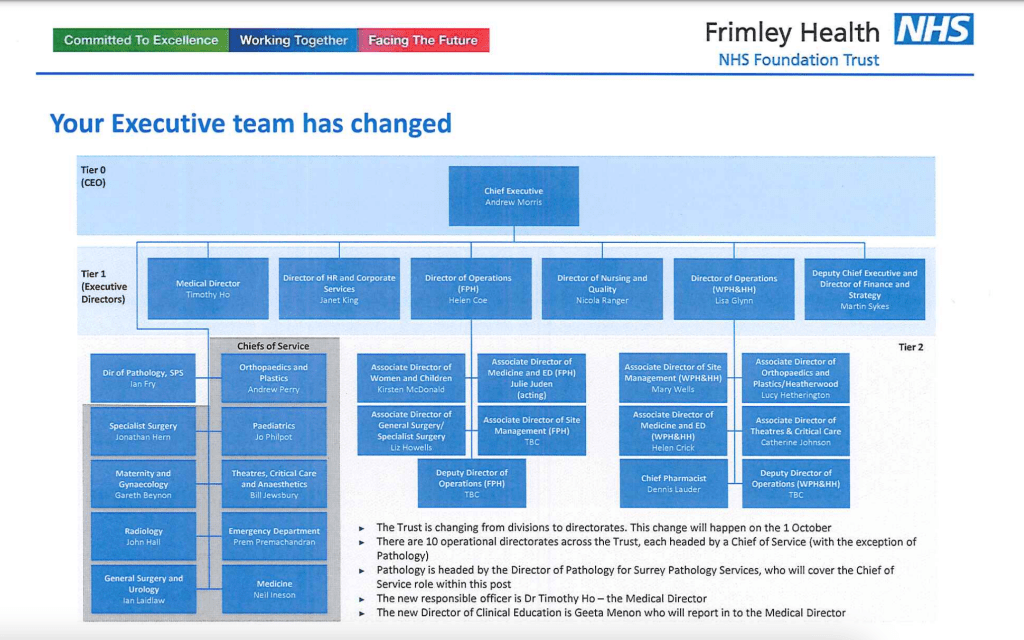
Summary: NHS Improvement has decided that Andrew Morris NHS Improvement non executive director will continue in his role as chair of the National Guardian’s Accountability and Liaison Board despite an instance of proven whistleblower reprisal by Frimley Health NHS Foundation Trust, when he was trust CEO and line manager to a director criticised for their part in the whistleblower detriment. The whistleblower harmed was Donna Simmonds, an administrator who raised patient safety concerns. Moreover, the trust’s litigation in the case was signed off by another of Morris’ direct reports, the director of Human Resources. Is there sufficient clear blue water between Morris and the proven whistleblower detriment? CQC missed the whistleblower detriment at the time and instead praised Frimley’s whistleblowing governance. Most recently, CQC asked Frimley for evidence of learning from the Simmonds whistleblowing case, but the trust response was grudging and thin. Frimley Health NHS Foundation Trust serves former health secretary Jeremy Hunt’s constituency. Frimley featured prominently in Hunt’s patient safety crusader narrative and also in the National Guardian’s propaganda. However, the well known twenty year cover up of baby Lizzie Dixon death under Frimley’s care took place on Andrew Morris’ watch.
The NHS National Guardian for whistleblowing is funded and supervised by those whom she is supposed to hold to account, namely the Care Quality Commission and NHS England/Improvement.
This is not reassuring.
The supervising structure is the National Guardian’s Accountability and Liaison Board and comprises Robert Francis and Andrew Morris and Henrietta Hughes. Morris and Francis are non executive directors of CQC and NHSI respectively, and Henrietta Hughes holds the office of the National Guardian for whistleblowing in the NHS.
Francis previously chaired the Accountability and Liaison Board, and so was scrutinising a flawed project which he designed.
Francis refused to meet with me to discuss concerns about the Freedom To Speak Up project. Francis’ correspondence to the National Guardian disclosed via subject access request revealed that this refusal was based on his belief that he could not change my mind, raising questions about his objectivity about his brainchild and ability to process challenge.
Francis was replaced by Andrew Morris as chair of the Accountability and Liaison Board.
I raised concerns with NHS Improvement about this role because of knowledge of victimisation whistleblowers by of Frimley Health NHS Foundation Trust, when Morris was trust CEO.
After five months, NHS Improvement responded thus on behalf of Dido Harding on 9 March 2021:
“Hi Minh
Thank you for your email and apologies for taking so wrong [sic] to reply directly to this.
We have considered the tribunal findings and can understand why you have raised it. I have liaised with Dido, Sir Andrew Morris and Henrietta Hughes on this matter.
Having discussed with Sir Andrew, it seems that he was not directly involved in this matter. Nonetheless, NHSE/I will consider whether we might incorporate learning from this into our broader work to improve people practices in the NHS.
Sir Andrew will remain in his role on the NGO’s ALB.
Thank you again for bringing this to our attention.
With best wishes”
But the ET found that Helen Coe the then Frimley Director of Operations and Sarah Casemore Deputy Director of Operations were responsible for detriment to Donna Simmonds in terms of not allowing her to return to her original role:
“We have considered the reasons why Ms Casemore and Ms Coe reached the decisions that they did that the claimant’s working relationships had broken down so that the claimant could not return to her original role. The respondent said that the problems with the team were not limited to the claimant. It was accepted that the team as a whole was dysfunctional. We did not hear any evidence about why the respondent decided that, despite there being a problem across the whole department, it was the claimant who had to move. As set out above, there was evidence before us that the claimant was regarded by her managers as difficult and a troublemaker and we have inferred that her first two protected disclosures materially influenced that perception. We also infer that the perception of the claimant as a troublemaker by her line managers played a material part in the decisions by Ms Casemore and Ms Coe that there had been a breakdown in the working relationships between the claimant and her managers in the department and the decision that it was the claimant who had to move.”
It is hard to understand how Andrew Morris could not know about the case given that Helen Coe was his direct report. It would surely be a failure of oversight if he did not.
But NHS Improvement’s response gives comfort to NHS trust chief executives, who can heave a sigh of relief that they will not be held accountable for serious wrongdoing so long as they are not “directly involved”.
In between my letter of 26 October 2020 to Dido Harding and NHS Improvement’s reply of 9 March 2021 Andrew Morris signed off an NHS Improvement complaint investigation about the National Guardian and her Office, which interviewed only two of four key witnesses.
Morris reportedly stuck to his guns after a query. He was overruled after I appealed to Dido Harding.
Alongside querying Morris’ role as chair of the Accountability and Liaison Board, I also asked Frimley Health NHS Foundation Trust about executive responsibility for the handling of the Donna Simmonds whistleblowing case.
The trust’s reply indicated that another of Morris’s direct reports, the Director of Human Resources was ultimately responsible for signing off the trust response to Donna Simmonds’ ET claim:
I leave it with readers to judge if there is sufficient clear blue water between Morris and the victimisation of a whistleblower, to justify his continuing role in shaping the work of an agency that is supposed to help NHS whistleblowers.
For completeness, in October 2020 I also sent the Simmonds ET judgment to Ted Baker CQC Chief Inspector of Hospitals who kindly took the matter up with the local CQC inspection team. At the material time CQC had failed to either pick up or report the Simmonds case. In fact, CQC praised Frimley’s whistleblowing governance:
“Managers across the trust promoted a positive culture that supported and valued staff, creating a sense of common purpose based on shared values. The trust had a well-publicised and embedded values system developed in conjunction with its staff. Staff described and open and positive culture at the organisation. Staff demonstrated a sense of belonging and frequently talked about a “family feel” at the organisation. The trust supported effective employee relations and staff could formally raise concerns through effective human resources procedures”.
The local CQC team told me that they would ask Frimley for evidence of learning from the Simmonds case.
I asked Frimley what evidence of learning the trust gave to CQC. This is the document disclosed by the trust in response:
There are some process improvements but alas, the specific trust response to causing a whistleblower detriment is very flimsy. It consists of waffle on defining “detriment” as opposed to any action to robustly deter it.
Importantly, Frimley’s response to CQC implied that the trust did not seek to learn from the Simmonds case until approached by the CQC.
Overall, Frimley’s response to CQC reads as a reluctant document, which shows little empathy and makes little if any acknowledgment of the injustice and harm to the whistleblower.
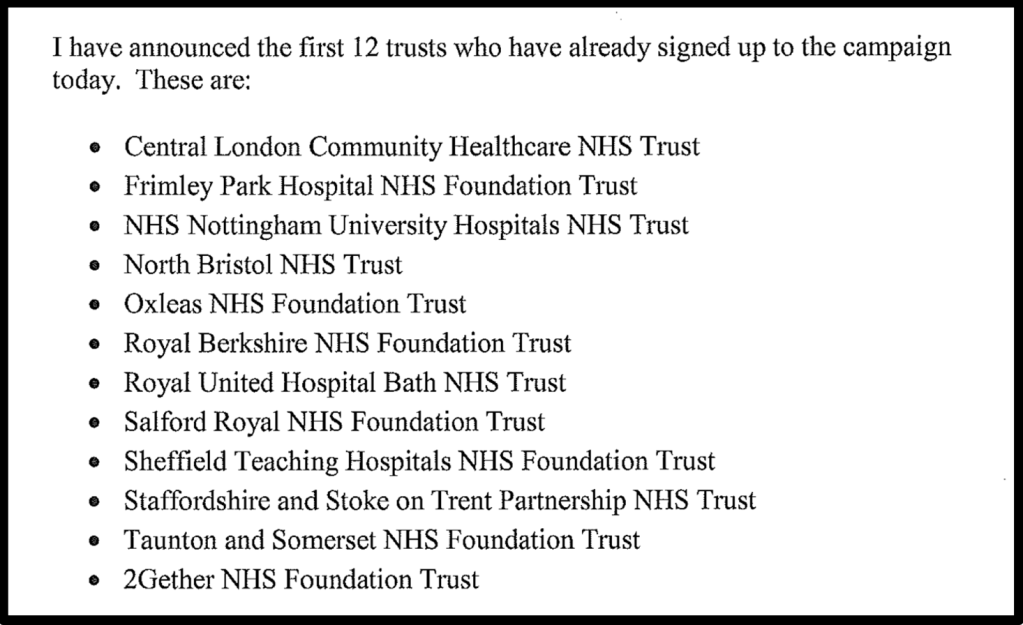
An important contextual factor is that Frimley’s reputation has been a political issue. In June 2014 Jeremy Hunt announced that he had hired recently knighted Robert Francis to undertake the Freedom To Speak Up review on whistleblowing in the NHS as a response to pressure over scandals. Hunt also brandished a list of twelve NHS trusts which he claimed had signed up to his grandiose campaign to make “the NHS the safest healthcare system in the world.” Frimley was amongst those who were obligingly helping with Hunt’s tinselly narrative.
Andrew Morris became Frimley’s chief executive in 1991. His tenure as chief executive spanned the death of baby Lizzie Dixon under Frimley’s care on 4 December 2001, and a subsequent twenty year multiagency cover up.
An investigation by Bill Kirkup, published by the government on 25 November 2020, focussed on dishonesty by frontline clinicians but said almost nothing about the governance of their employer, Frimley Park Hospital.
The then Chief Executive of the Strategic Health Authority was interviewed but oddly, Andrew Morris was not listed amongst individuals interviewed by Kirkup’s investigation.
Buried in the investigation report appendices is the sentence:
“Allegations about the fitness to practise of medical staff involved in her death were considered by the General Medical Council, and complaints were considered by Frimley Park Hospital and Great Ormond Street Hospital”.
Kirkup made no specific recommendations for Frimley, but there is a comment that community care should be properly planned and should not discriminate against disabled people through the application of lower standards:
“Community care for patients with complex conditions or conditions requiring complex care must be properly planned, taking into account and specifying safety, effectiveness and patient experience. The presence of mental or physical disability must not be used to justify or excuse different standards of care.”
We will limp on with cover ups, subpar whistleblowing governance, conflicts of interest and ramshackle sham ‘protections’ systems for as long as there is no political will to do it properly.
If you have not already done so, please help drive change by signing and sharing this petition to parliament for law reform.
By Dr Minh Alexander, NHS whistleblower and retired consultant psychiatrist, 9 March 2021
NHS mental health beds have been unsafely slashed over the years with little of the promised re-investment in intensive community services materialising. Deinstitutionalisation has merely meant neglect in the community.
Alongside this, unsatisfactory private mental healthcare services funded largely by the public purse have proliferated.
Vulnerable NHS patients are made even more vulnerable by being shipped out of area to private care, away from the support and scrutiny of family and friends.
The quality of such private services has often been poor, sometimes dire, with frank abuse.
NHS England as the lead commissioner has failed to ensure effective, proactive commissioner oversight of the care received by these isolated, exiled patients. Scandals keep recurring.
AN EXAMPLE
Multiple mental health units operated by the private healthcare company the Priory Group have been placed in special measures by the Care Quality Commission.
St Johns House, Palgrave, Norfolk, run by Partnerships in Care Ltd which is a subsidiary of the Priory Group, is the latest to enter special measures. CQC’s inspection report of 5 March 2021 makes unbearable reading because it comprises a long, long list of serious care and governance failings. The findings amount to institutional abuse.
This is a small selection of the failings detailed by CQC’s report:
“We reviewed a random selection of CCTV footage between 17 November and 12 December 2020 to observe how staff were managing patient observations. We found that in five out of five checks, staff were sleeping on duty.”
Managers were informed that some staff had been sleeping on duty but according to the CQC “ no action was set to address this”.
CQC reported “a staff member was seen to push a patient onto the floor”.
One incident of restraint led to staff suspensions and a report to the police, but only after CQC intervened.
Staffing was often inadequate, seclusion practice was poor, there was high use of force without de-escalation, failure to report safeguarding issues, failures to mitigate ligature risk and many incidents and injuries. There were insufficient therapeutic interventions, leaving an emphasis on dreadful, custodial care.
The appalling treatment of whistleblowers by such private providers, guarding their profits, is part of the problem.
Dr Ambreen Malik’s whistleblowing case against Cygnet Health Care Ltd gives a glimpse into how far some of these private providers will go in suppressing safety concerns and mistreating whistleblowers.
Dr Malik’s case is not the first whistleblowing case at Cygnet and it will not be the last.
I have written to NHS England to ask that it:
Increases the whistleblowing governance standards required of private providers who receive public funding through contractual means.
2. Exercises its commissioning power to stop Cygnet from going ahead with a threatened appeal against the Employment Tribunal judgment in Dr Malik’s favour, which will have a chilling effect on Cygnet’s workers.
3. Ensures that any final NHS standards for Fit and Proper managers in the NHS, arising from the Kark Review implementation, are applied to private providers who receive public funding.
At present there is a fig leaf applied by NHS England in the form of a contractual requirement that private providers should appoint Freedom To Speak Up Guardians.
Cygnet appointed a Freedom To Speak Up Guardian as part of managing adverse publicity about its serious care failures.
I have disabused NHS England of any claims that a contractual requirement for a Freedom To Speak Up Guardian suffices, and provided evidence that has accumulated about the deceptive and pernicious nature of the Freedom To Speak Up project.
The letter to NHS England follows:
BY EMAIL
Noel Gordon
Non Executive Director
Chair of Specialised Services Commissioning Committee.
NHS England
8 March 2021
Dear Mr Gordon,
Suppression of safety concerns and whistleblower reprisal by Cygnet Health Care Ltd, a private contractor which provides services to the NHS and policy issues which arise
I write to you in your capacity as chair of NHS England’s Specialised Services Commissioning Committee to ask that NHS England takes action to ensure that private contractors have better whistleblowing governance and Fit and Proper Directors.
An Employment Tribunal has decisively determined in favour of Dr Ambreen Malik consultant psychiatrist and whistleblower, that there has been serious whistleblower reprisal, “a litany of bad faith”, “dishonesty” and or “less than honest” behaviour by several Cygnet Health Care Ltd directors. This included the chief executive Dr Tony Romero. The Tribunal held Dr Tony Romero responsible for most of the acts by others::
“Dr Romero was responsible in effect for nearly all of the actions taken by the other parties, through Jenny Gibson [Cygnet Director of Human Resources].”
The ET also described a retaliatory GMC referral by the then medical director as “venomous and dishonest” in tone.
The incident which sparked this whistleblower reprisal was Dr Malik’s insistence on doing her duty and giving a coroner’s inquest the full truth about the circumstances of a patient’s death.
Obvious issues of CQC Regulation 5 Fit and Proper Persons arise, and I have forwarded the ET findings to the CQC.
Cygnet relies largely on public funding, as confirmed by its 2019 annual report, and public accountability is therefore needed.
Cygnet reportedly informed the Times that it intends to appeal against the ET verdict.
Yet the Tribunal demonstrated robustly how it came to its decision, and much of its conclusions are based on clearly recorded original evidence which contradicted Cygnet’s later witness evidence.
It is hard to see how Cygnet will succeed, but an appeal will cause even more suffering to Dr Malik and her family. Very seriously, it will also have a chilling effect on any other Cygnet employee who is thinking about whistleblowing.
Dr Malik’s case is not the first Cygnet whistleblowing case in the public domain. There are also others that are not in the public domain.
NHS England has a particular duty to ensure that patients who are most vulnerable as a result of being sent out of their home area and isolated from normal sources of support are not left at the mercy of poor care and unscrupulous corporate practices.
There has been an abundance of scandals for years concerning private mental health care providers who derive most of their income from the public purse.
It is time for NHS England to significantly improve its oversight of these services to ensure the safety and welfare of these most vulnerable and isolated patients.
Ensuring better whistleblowing governance is an important part of this.
My requests to NHS England are as follows:
1. I would be grateful if NHS England could look into the ET findings of serious executive wrongdoing at Cygnet and ensure here on that any public contracts with private providers of healthcare contain robust enough standards to ensure better whistleblowing governance, and to punitively deter bad whistleblowing governance.
2. Please can NHS England use its commissioning power to deter Cygnet from appealing against such a conclusively evidenced ET judgment, and from causing Dr Malik and her family yet more suffering and intimidating other workers.
All whistleblowers are seriously harmed by the enormous stress of litigation and prolonged conflict. These processes take a substantial toll on health.
It would be a great regret if NHS England does not show that it is willing to check employers’ excesses and to protect the rights of all Cygnet’s workers to safeguard patients.
In the case of Dr Kevin Beatt another whistleblower who received a similarly decisive ET judgment in his favour, ministers and regulators all failed to restrain his former employer Croydon Health Services NHS Trust. Croydon incurred millions in costs through repeatedly appealing and then being ordered to pay about £1 million in compensation:
This was a gross waste and completely unjustified use of public money, as well as a severe injustice to Dr Beatt who suffered years of extremely stressful litigation.
I fear that if NHS England does not restrain Cygnet, yet more money that ultimately comes from the public purse will be recklessly wasted.
3. May I also ask that NHS England/Improvement considers bringing the directors of private contractors within the scope of its Kark Review implementation on NHS Fit and Proper Persons, and reflecting any final Kark standards in NHS contracts with private providers. Where public money is spent, the same standards should be expected.
I am aware that NHS contracts with the private sector contain a requirement for organisations to employ a Freedom To Speak Up Guardian but this is frankly a tissue thin device. The Freedom To Speak Up project was a weak policy design that has been badly executed, failing many whistleblowers. I provide links to relevant evidence in the appendix.
Bad employers merely exploit an appointment of a Freedom to Speak Up Guardian for cynical PR, whilst continuing with bad governance.
Cygnet announced it would employ a Freedom To Speak Up Guardian but this is in reality gives no assurance.
In general, I would urge NHS England to scrap the wasteful Freedom To Speak Up project because it adds no value where an employer is honest and only gives bad employers more tools for covering up and victimising whistleblowers, whilst maintaining a false façade of good governance.
In the meantime, I would also be grateful for information as follows:
1. Does NHS England have a system in place to track employment tribunal claims against private healthcare providers with whom it holds national contracts for specialised services?
2. What standards of whistleblowing governance does NHS England require of private healthcare providers from whom it contracts services? Please disclose or point me to the relevant documents.
3. What standards of whistleblowing governance does NHS England expect CCGs to require from healthcare providers from whom they contract services? Please disclose or point me to the relevant documents.
4. Does NHS England hold central data on complaints received about care provided by Cygnet Health Care Ltd? If so, please disclose the number and details of complaints about care provided by Cygnet Health Care Ltd in the last two years.
I copy my letter to the Joint Committee on Human Rights which held an inquiry into serious and systemic breaches of patients’ rights by private mental healthcare providers, including Cygnet.
I also copy this letter to Dido Harding, Simon Stevens and other members of NHS England’s Specialised Services Commissioning Committee, and to Tom Kark QC and Claire Murdoch NHS England’s Mental Health Tsar.
I would be grateful if this correspondence could be passed to those for whom I have no direct email address
Yours sincerely,
Dr Minh Alexander
Cc Harriet Harman Chair of JCHR
Dido Harding Chair NHS Improvement
Simon Steven CEO NHS England
John Stewart NHS England Director of Specialised Commissioning
Michelle Mitchell NHS England Non Executive Director
Moira Gibb NHS England Non Executive Director
Ian Dodge NHS England National Director of Strategy
Stephen Powis National Medical Director NHS England
Tom Kark QC
Claire Murdoch National Mental Health Director NHS England
APPENDIX
Evidence of failures of the government’s Freedom To Speak Up project
The Freedom To Speak Up model was not evidence based:
And yet millions have been wasted on this project.
The Freedom To Speak Up model is unworkable due to the central conflict of interest that it relies on employees to hold erring employers to account, and because it gives no genuinely independent channel for whistleblowers concerns to be investigated. By design, employers are left in sole control of the investigation of whistleblowers’ concerns.
The National Guardian fails to track the outcomes of concerns raised with NHS trust Freedom To Speak Up Guardians and whether NHS trust staff’s concerns are addressed:
The National Guardian has failed to carry out enough case reviews. Her Office gives poor value for the funding it receives at an average of two case reviews a year.
The National Guardian has declined to adopt the role recommended by the original Freedom To Speak Up Review of helping to ensure that harm to whistleblowers and patients is redressed. Her case reviews only make bland general recommendations:
The National Guardian and her Office havr sometimes colluded with employers and the Office has sometimes acted with the effect of covering up its failures to effect improvement as a result of case reviews:
By Dr Minh Alexander NHS whistleblower and retired consultant psychiatrist, 7 March 2021
Summary: The regulator the Care Quality Commission was implicated in a case of whistleblower reprisal by a private social care provider. An Employment Tribunal case revealed CQC emails exchanged with the provider in which Emma Hatfield a CQC inspector made critical comments about a care home whistleblower. The Employment Tribunal concluded that these comments showed a lack of impartiality. In addition, the ET severely criticised Pearl Jackson a director of the provider for harming and threatening the whistleblowers, behaving in a “dishonest” manner during proceedings and showing contempt for the ET. The provider company is part of a complex web of companies which according to Companies House, appear to lead back to the Cayman islands.
I drew the ET matters to the attention of Kate Terroni CQC’s Chief Inspector of Adult Social Care but she ignored the letter. I escalated matters to Peter Wyman CQC Chair. After this I received a troubling response from Mary Cridge CQC Deputy Chief Inspector of Adult Social Care. This response minimised the failure of regulatory impartiality by Emma Hatfield and even sought to cast more aspersions on the whistleblower based on what appeared to be employer hearsay. CQC has produced no evidence to show that it has taken action to prevent future failures of impartiality. Mary Cridge herself has made public overtures to the senior managers of providers which raise questions about boundaries. She has been the CQC’s own Freedom To Speak Up Guardian since 2016.
The CQC declined to take any action against the whistleblowers’ employer under CQC Regulation 5 Fit and Proper Persons (FPPR) other than to ask if the provider was satisfied with Pearl Jackson’s fitness and expressing an intention to “monitor” services overseen by Pearl Jackson. Moreover, the CQC has declared that it will ignore any further correspondence from me on these matters because I was not directly affected. It has not taken this approach to other FPPR referrals in the past. One has to question why the CQC is so defensive in this particular case.
The public record in fact indicates that Pearl Jackson was apparently prosecuted for several counts of care home neglect and ill treatment in 2008, but the trial was halted due to CPS failure to disclose documents. I have now drawn CQC’s attention to the public record, assuming CQC is not already aware.
I have asked CQC to show that it has taken action to ensure inspectors act impartially towards whistleblowers in future, and to ensure that a proper investigation is undertaken into the FPPR issues.
Background
On 11 December 2019 the Employment Tribunal found in favour of two care home whistleblowers Karen McGuire and Tracy Skitt, whom the Tribunal determined had been subject to detriment and unfair constructive dismissal. They were both forced to resign because their identities were revealed and their positions became untenable. They also suffered post-employment detriment such as employer intimidation. Ms Skitt was according to the ET additionally victimised through a “false” letter of dismissal.
The ET summarised as follows:
“The claimants were working in a home where they were both identified as the carers responsible for making disclosures to seniors/managers alleging neglect and complaining that the other carers were not doing their jobs properly. This was a home where gossip, division blame and bad feeling towards the claimants was openly expressed and condoned by management. Instead of following the whistleblowing procedures in place to protect those who alert the employer to suspected neglect/abuse they sided with the other carers.”
The named respondents were ADL PLC, Charlton Court Care Home Ltd and Pearl Jackson, a director of both companies.
I wrote about this strange and disturbing case after a Good Samaritan drew my attention to the judgment:
The case echoes the story of Helen Rochester, who suffered detriment ultimately caused by the Care Quality Commission who should have held her employer to account, but sided with them.
Former senior police office recruited to intimidate one of the whistleblowers
The case was bizarre and included a strange tale of Bob Taylor, a former detective chief superintendent and occasional contractor to the whistleblowers’ employer, impersonating a CQC inspector in a phone call to one of the whistleblowers:
He made the call to Karen McGuire at the request of the employer, and accused her of theft. The ET concluded that his actions were a detriment carried out on behalf of the employer.
Severe criticism of a senior manager who retaliated against the whistleblowers and whose evidence was not considered reliable by the Tribunal
Moreover, the Tribunal severely criticised Pearl Jackson a director representing the employer, for both retaliating against the whistleblowers and for her conduct during ET proceedings. The ET considered that Mrs Jackson had sent a threatening letter to one of the whistleblowers, and she instructed Bob Taylor to contact the whistleblowers:
“Mrs Jacksons intimidating and threatening letter to the claimant expressly refers to the disclosures made which she describes in her letter as ‘everyday occurrences” inflated by the claimant. Her letter was a deliberate angry retaliatory response to the disclosures made. Mrs Jackson had decided at the outset before any investigation was carried out by Mr Taylor, that the claimant in making these allegations was “evidently vindictive towards senior management”. She tells her so in the first paragraph of her letter. Mrs Jackson was materially influenced in her treatment of the claimant by the protected disclosures she had made. Her instruction to Mr Taylor to contact the claimant was given in that context of protecting the home and taking ‘whatever steps were necessary’. Mr Taylor’s call to Mrs McGuire was made with that purpose in mind. It was extremely intimidating and threatening.”
Pearl Jackson claimed to Karen McGuire that her whistleblowing disclosures were malicious:
“So far, my initial investigation reveals that you have indeed inflated many of the issues using every day occurrences to fuel what I believe to be malicious activity…”
The ET noted that Pearl Jackson had not in fact carried out an investigation as claimed in this letter:
“Mrs Jackson accepts she had carried out no investigation at all before sending the letter…”
The ET also concluded that Pearl Jackson’s motivation in sending the letter was to intimidate:
“Mrs Jackson intended the letter to frighten the claimant ‘off’ by telling the claimant she would ‘take whatever steps were necessary’ backed by the board of directors threatening legal action.”
The ET noted the following about Pearl Jackson’s conduct during proceedings:
“Her first approach was that no disclosures had been made by the claimants and there were no detriments. The claimants were telling lies because the home had been ‘exonerated’ in subsequent external inspections.”
“Mrs Jackson’s second approach was to allege that the claimants were the ‘wrongdoers’ in relation to any allegations made.”
The ET found that Pearl Jackson was not honest in presenting evidence and was not a reliable witness:
“Mrs Jackson, selectively and deliberately chose to disclose only the parts of documents that supported the respondents case that subsequent inspections had ‘completely exonerated’ the home. She only disclosed parts of a Leeds City Council Inspection Report following a visit to the home on 14 February 2019 and part of an Infection Prevention and Control Report, following an audit on 18 April 2019.”
“In an email of 2 October 2019, Ms Almzedi had raised with Mrs Jackson her request for full disclosure of documents, when it became clear to her that some pages were missing. She also requested that the original reports rotas and time sheets were produced at the hearing because she queried their authenticity. She had good grounds to believe the duty rota had been altered between exchange and the version produced in the bundle, because Mrs Jackson accepted that is what had happened. Despite being forewarned of this issue the original documents were only produced very late on in the hearing.”
Arising from this the ET concluded:
“She was not being open and transparent with the claimant’s representative or with the Tribunal and her conduct of these proceedings, does not go to her credit. There were other examples in our findings of fact that informed our view that Mrs Jackson was not a reliable witness. She was evasive and was not presenting evidence openly and honestly to the Tribunal.”
In a further judgment on 19 May 2020, the ET underlined the serious harm done to the whistleblowers, and made further serious criticisms of Pearl Jackson. For example:
“She was dishonest and was prepared to go to any lengths to try and portray the claimants in the worse possible light concealing evidence that went in their favor.”
The ET also found that Pear Jackson’s conduct in proceedings amounted to contempt:
“Mrs. Jackson has chosen to continue to act as the representative until last week. For that reason, to accommodate her ‘unavailability’, the remedy hearing was delayed until 12 March 2020. It was unreasonable for Mrs. Jackson, a named respondent, to then decide not to ‘turn up’, or send any evidence or explain her absence. The conduct of the respondents since the last hearing shows complete disregard and contempt, not only towards these claimants, but also to the Tribunal and these proceedings.”
A finding of lack of impartiality by a CQC inspector
The ET judgment also revealed that Emma Hatfield a CQC inspector wrote emails to the whistleblowers’ employer which the ET concluded showed a lack of impartiality.
Emma Hatfield accepted “without question” counter allegations against the whistleblowers by Kelly Hopkinson care home manager, whom the ET found retaliated against the whistleblowers, revealed the whistleblowers’ identities, gave them bad references and concocted a false letter of dismissal against Tracy Skitt.
Importantly, by that point the CQC had received disclosures from Karen McGuire, and it should have been especially careful in weighing and filtering any counter allegations by her employer, not credulous.
The ET found that Kelly Hopkinson falsely claimed to have dismissed Tracy Skitt, who had in fact resigned:
“Miss Hopkinson’s evidence was that on 11 January 2019 before she supplied that reference she had dismissed the claimant. She relies upon a letter of dismissal (page 64). Miss Skitt never received that letter and was unaware of any ‘dismissal’. The letter in the bundle is signed by Miss Hopkinson. It states that Miss Skitt’s employment had been terminated during her trial/probationary period for not returning to work after the 9 January 2019.”
A negative reference and the false letter of dismissal by Kelly Hopkinson made it very difficult for Tracy Skitt to get further work, and reportedly affected her mental health.
The ET judgment gave this account of the email exchange between Emma Hatfield and Kelly Hopkinson, which the ET noted took place the day after Karen McGuire whistleblew to the CQC on 9 January 2019:
“External reporting to the CQC
170. Although it was not necessary to make any findings of fact about whether a protected disclosure was made to the CQC the evidence we saw produced by the respondent in the bundle (relied upon to support the ‘exoneration defence’) gave the Tribunal, some cause for concern.
171. On 10 January 2019, after Mrs McGuire had resigned informing Miss Hopkinson she would be reporting the home to the CQC, Miss Hopkinson sent an email to Ms Hatfield. The email states: “Hi Emma I just wanted to make you aware that a staff member walked out of shift yesterday due to gossiping. She has since taken to social media with immature comments. She has telephoned Pearl Jackson, the director and made some accusations about the home which Pearl is investigating and I am telephoning safeguarding to make them aware.
172. On the same day Emma Hatfield replies by email: “No problem at all. As if you haven’t got enough to do”.
173. Miss Hopkinson immediately labels the claimant as the trouble maker in this email exchange and Miss Hatfield sympathises without question. In another email on 14 January 2019, Miss Hatfield is given an update of the situation by Miss Hopkinson. Her response on the same date is “That is appalling. What is wrong with her?”. Another update follows and Miss Hopkinson apologises for ‘going on’ about it. Miss Hatfield responds “No you are not going on. It is upsetting I just don’t know what she thinks she will achieve”. In another email sent by Miss Hopkinson dated 16 January 2019, Miss Hopkinson states “I appreciate you have a process you have to follow but I really feel this is all just malicious and vindictive”. Miss Hatfield in her response of the same date states: “I’m sorry that you had to deal with all of this”.
174. Mrs McGuire having seen these emails says in her statement “I am alarmed at the inappropriate degree of empathy between the CQC inspector and the care home manager and I feel this is worrying given the nature of what was being reported. I would have expected more impartiality”.
175. Unfortunately, from the email exchange we saw (disclosed and relied upon by the respondent), we can see why the claimant has those views of the relationship between Miss Hopkinson and Miss Hatfield. From the claimant’s perspective she expected the CQC interaction to demonstrate the impartiality she had received in her dealings with the home.”
A reluctant CQC response to these ET findings
On 8 October 2020 I wrote to Kate Terroni CQC’s Chief Inspector of Adult Social Care and I asked the Care Quality Commission to:
Look into the work of Emma Hatfield the CQC inspector who was criticised by the Tribunal and to consider what further work CQC should do on ensuring that its inspectors understand the need for impartiality in whistleblower cases and their duties in responding to such cases.
Review the employer under CQC Regulation 5, with particular respect to the ET’s criticism of Pearl Jackson
My letter to CQC’s Chief Inspector of Adult Social Care was ignored. I therefore wrote to Peter Wyman CQC chair two months later, on 12 December 2020 to press the issues.
On 23 December 2020 I received a response from Mary Cridge, CQC Deputy Chief Inspector of Adult Social Care.
Mary Cridge sent me two letters, respectively addressing the concerns about Emma Hatfield the CQC inspector and Pearl Jackson the director criticised by the ET:
In brief, CQC claimed it had looked into both issues and satisfied itself there was no more to be done save for “monitoring” the organisations where Pearl Jackson was a director:
“We continue to monitor the providers where Mrs Jackson is a director and any new information that comes to us, as this will help us decide if we need to take further action in relation FPPR and plan for future inspections.”
Regarding Emma Hatfield, Mary Cridge characterised Emma Hatfield’s behaviour in the Charlton Court case as “support” for the employer, that was within the ambit of her responsibilities:
“Emma’s role as an inspector involves supporting whistle blowers to raise concerns they may have about the care people receive as well as supporting providers to improve care and support for people using their services.”
Mary Cridge seemed to imply that Emma Hatfield had reason to be critical of the whistleblower, based apparently solely on hearsay from the employer:
“Emma received a further email from the manager of the service who informed her that a previous staff member was contacting relatives by phone and they were coming to see the manager concerned and upset by what they were telling them. She told Emma that she had been able to reassure them and they were leaving happy and satisfied with what they were being told by her. Emma was concerned that contacting relatives may have caused them distress and was extremely unfortunate.”
There is no indication in Mary Cridge’s response that Emma Hatfield verified these claims by the employer.
A note of defensiveness about impartiality arises in the following comment by Mary Cridge:
“Emma feels her support throughout the process for the manager did not distract her from the core tasks as a CQC inspector given the safeguarding concerns that were raised at the time.”
This is an astonishing way to describe uncritical acceptance of allegations by a provider manager found by the ET to harmed whistleblowers and to have manufactured a dismissal letter about a dismissal that never occurred.
Mary Cridge notes that Emma Hatfield was not asked to give evidence to the ET but she did make referrals to the local safeguarding team and concluded:
“I am satisfied that Emma took all steps to ensure people living at Charlton Court were safeguarded in a timely way and in line with our policies and procedure.”
However, a question arises of what slant was put on the safeguarding discussions. Was the credibility of the whistleblowers was undermined in anyway as a result of Emma Hatfield appearing to accept a number of the employers’ assertions without evidence of critical analysis and independent verification?
Notably, Mary Cridge herself has made public comments to provider managers which raise further questions of impartiality. More information on this is provided in the appendix.
I firstly asked CQC to clarify some factual anomalies in the letters from Mary Cridge.
The letter admitted that Mary Cridge had wrongly referred to a single comment by Emma Hatfield when several troubling comments had been singled out by the ET, and the letter confirmed that CQC had reviewed the ET judgments, which Mary Cridge had previously referred to as transcripts.
CQC went on to express the following sentiments:
“While we note your intention to reply substantively, we do not intend to enter into further communication on this issue having responded in detail already. We therefore consider the matter closed as you have not been directly affected by our actions and future communication from you regarding this will be read and filed without a reply.”
Unfinished business
I have written to the CQC again to raise concerns that there is no apparent organisational learning by CQC from the Charlton Court case and to ask for more action:
CQC clearly wishes to shut down the issue of impartiality by its inspector Emma Hatfield but CQC has yet to demonstrate that its inspectors understand what regulatory impartiality requires.
Moreover, the FPPR decision is lamentable given the ET findings about Pearl Jackson’s extraordinary behaviour.
If harming and threatening whistleblowers, conspiracy to intimidate and manipulating evidence are not actionable, what is?
Integrity is essential in services that care for the extremely vulnerable who may be unable to speak up for themselves. A lack of meaningful CQC action is effectively a lack of respect for the rights of the vulnerable.
I leave it to readers to decide if CQC has acted properly in this case, or whether it has once again contributed to silence and harmed the public interest.
Alas, UK whistleblowing law does not currently recognise detriment to whistleblowers caused by regulators or any parties other than employers. This is key loophole that needs to be closed.
If you have not already done so, please help by signing and sharing this petition for reform of wholly inadequate UK whistleblowing law:
I have pointed out to the CQC that according to press reports combined with data published by Companies House, it appears that Pearl Jackson was prosecuted for neglect and ill treatment in 2008 but not convicted because of errors by the CPS in not disclosing all documents. The details are as follows.
In 2008, local press reported unsanitary environment and poor care at Newsham House care home, Stroud Road, Gloucester:
“What the Crown say was found was a lack of information regarding care plans and in many cases the non-existance of care plans.
“Photographs revealed the disgusting state of toilets in residents’ rooms. They were old, damaged and there was penetrative moisture. There was a general hygiene risk.
“In one case faeces with mould growing on it was found.
“There was no plan to address the patients’ social needs, nor was there any stimulation or diversion therapy. There was no one-on-one activity.
“Thought was given to closing the home, but the service provider ADL Ltd gave assurances that the problem was being managed.
“William Davies is the Managing Director. Pearl Jackson is the Operations Director. Derek Youds the manager, and Heather Bolton a deputy manager.”
It was reported that Pearl Jackson was charged thus:
A chief constable report at the time noted that there were five residents’ deaths of concern at Newsham House:
“Op Star
Operation Star is the investigation into the Newsham House Registered Care Home in Gloucester.
It is a joint investigation with the Commission for Social Care and Inspection (CSCI) with assistance from Gloucestershire Social Care Directorate.
In 2002 and 2003 CSCI received complaints by family members about the treatment of their relatives in Newsham House. In particular investigations revolved around the death of five patients.
Following a series of interviews with the Managing Director, Operations Director of ADL Plc, the Manager and Deputy Manager of Newsham House have been charged with a large number of offences relating to the alleged wilful neglect of a patient receiving treatment for a mental disorder. They await trial.”
“In a 42-page ruling, Judge David Ticehurst said two employees at Newsham House, in Gloucester, and two directors of ADL Plc, owners of the care home, would not have a fair trial if the prosecution went ahead.
Judge Ticehurst said his decision to halt the prosecution was sorrowful and a matter of “considerable regret”, as those who resided at the home were “the most vulnerable in society”
Tracing the ultimate ownership of these companies through Companies House leads to a company that appears to be based in the Caymans – “Oakhurst Court Holdings (Cayman) Ltd”.
More about Mary Cridge CQC Deputy Chief Inspector of Adult Social Care
Mary Cridge is the CQC’s own Freedom To Speak Up Guardian, having been appointed to that position in 2016.
Prior to that she cleared David Behan in 2013 of any serious wrongdoing when I complained that he ignored serious patient safety concerns that I escalated to him after local CQC inspectors had simply ignored me in 2012. For good measure, Mary Cridge claimed that a CQC complaints manager tried repeatedly but could not get through to me on the telephone, when this individual did not have my phone number and this was a recorded fact.
After her promotion to CQC Deputy Chief Inspector of Adult Social Care, Mary Cridge wrote an article which extolled the importance of good whistleblowing governance:
There have been other similar displays towards the powerful in various provider organisations, which perhaps give context to the lack of perturbation about Emma Hatfield’s boundaries.
By Dr Minh Alexander NHS whistleblower and retired consultant psychiatrist 3 March 2021
Summary: On 15 July 2020 Imperial College Healthcare NHS Trust issued a strange denial of wrongdoing or doubt about Revd Paula Vennells’ fitness to be chair of an NHS trust. The trust initially denied that Vennells herself helped to craft this statement. After further questions, disclosed correspondence between the Imperial director of communications and NHS Improvement throw doubts on Imperial’s claim that Vennells did not have a hand in the statement. Moreover, Imperial admits that the statement was sent to all board members before it was released, so all had responsibility. Other information obtained through FOI shows that Imperial had not agreed any terms of reference for an external review under CQC Regulation 5 Fit and Proper Persons, which the trust promised to undertake after Care Quality Commission intervention, by the time that Vennells tendered her resignation on 30 November 2020. The trust previously claimed that external legal advice concluded that its FPPR governance was “robust”. It is now revealed that this advice was provided by Capsticks LLP in February 2020. The trust now admits that it in addition to the usual administrative checks, Capsticks urged Imperial to consider more widely if Vennells was of good character. The question is whether the Imperial trust board applied itself to this consideration with good faith and any meaningful rigour. CQC’s deliberations on Imperial’s compliance with Regulation 5 Fit and Proper Persons is still awaited.
Paula Vennells was a Post Office Ltd senior manager for ten years, and the company’s chief executive for seven of these years.
She was seriously criticised for her role in the Post Office’s protracted and flawed denial that it unsafely prosecuted and convicted hundreds of subpostmasters, based on its unreliable Horizon computer system.
I referred Vennells to the Care Quality Commission under CQC Regulation 5 Fit and Proper Persons in December 2019, following a damning High Court judgment against Post Office Ltd.
BEIS ministers later questioned Vennells’ leadership of the Post Office and importantly, her fitness for her current role as Imperial chair:
On 15 July 2020, after the BEIS ministerial FPPR referral, Imperial College Healthcare NHS Trust issued a pre-prepared statement at its Annual General Meeting, read out by the deputy trust chair Nigel Acher, which was dismissive of the serious concerns about Vennells’ fitness.
Strangely, the trust’s statement claimed there were no new insights about her role in the Post Office Ltd scandal from when she was appointed as trust chair in Spring 2019:
“Sir Gerald: “Thank you, thank you very much indeed Paula. Mr Wilson, thank you for your question. [he reads] Indeed no one could follow what has happened to many of the Subpostmasters using the Horizon system without being profoundly moved, but when Paula was appointed by NHS Improvement, just over a year ago, she was open about the ongoing Horizon issues during her time at the Post Office. And following the Post Office legal ruling and settlement at the end of 2019, and subsequent developments. our board has reviewed the situation carefully and thoroughly. All of the information we have remains in line with what was understood by NHS Improvements at the time of Paula’s appointment in April 2019. And the board has no additional insight into the complexities of the Post Office issues over the past 20 years and we are only able to draw on our own direct experience of Paula’s conduct and contribution to this Trust, which has been entirely positive. Thank you Paula, back to you.”
This was very surprising given several excoriating court judgments that were issued after Vennells’ appointment as Imperial Chair. The High Court and Court of Appeal judgments lambasted Post Office Ltd’s denial of problems with the Horizon Computer system and its “mid Victorian factory owner’s” attitude towards and treatment of subpostmasters. Judges also criticised Post Office Ltd’s disreputable conduct and many incorrect claims in proceedings, aggressive litigation tactics and its extraordinary, baseless and unsuccessful attempt to boot the High Court trial judge off the case. Post Office Ltd’s behaviour during the trial helped to drive up costs, thus effectively robbing gravely harmed sub postmasters and their families of much needed compensation.
As Post Office Ltd’s CEO, it is hard to see how Vennells could reasonably escape criticism for many of these failings. She was surely either an active party to bad governance, or she did not have proper grip and failed to understand, recognise or correct bad governance. Moreover, as CEO she must have had a significant hand in shaping Post Office Ltd culture and corporate habits in her seven years as chief executive, leading up to the conclusion of the Post Office trial.
I asked Imperial College Healthcare NHS Trust which trust directors helped to draft the statement of denial issued at the 15 July 2020 AGM. The trust initially answered evasively on 14 January 2021 as follows:
“This particular outline response was developed with input from board members, though not the chair.” [My emphasis]
When challenged about this failure to answer my question, the trust remained opaque and claimed on 25 February that it could not tell me which directors were involved in the drafting because it held no records. But it did concede that the statement was shared with all directors before it was issued:
“The Trust does not hold recorded information in response to this request. The statement was drafted by the director of communications based on discussions with board members and previous responses. As is usual practice, it was shared with all board members in advance, along with other suggested responses to questions likely to arise at the AGM, including questions that may have been asked directly of the chair.”
The Imperial FOI response of 25 February 2021 can be foundhere.
Additionally, Imperial disclosed that it ran its statement on Vennells past the regulator NHS England/ Improvement. The trust disclosed its email correspondence with the regulator as part of the 25 February 2021 FOI response.
Significantly, despite the trust’s above claim of 14 January 2021 that Vennells had no part in drafting the 2020 AGM statement, the correspondence disclosed on 25 February 2021 suggests that Vennells (and the Imperial’s CEO Tim Orchard) may have been involved in preparing the trust’s AGM statement. An email by Michelle Dixon Imperial’s Director of Communications stated:
[date redacted but probably 14 July 2020] “I’ll send to Tim and Paula this evening too for any updated view.”
I have asked the Trust to clarify this apparent anomaly and explain why it originally denied that Vennells was party to drafting the denial.
Michelle Dixon like Vennells, has passed through the Cabinet Office.
Vennells got a seat at the Cabinet Office board table as a NED in February 2020 as she departed from the Post Office, but later resigned, after pressure on the government from MPs and peers mounted.
Although Imperial College Healthcare NHS Trust issued the defiant 15 July 2020 AGM statement about Vennells’ fitness, this was followed by the Criminal Cases Review Commission’s finding there had been a miscarriage of justice caused by the Post Office. CCRC referred unsafe sub-postmaster convictions to the Court of Appeal.
Imperial was then forced to agree to commission an external review of CQC Regulation Fit and Proper Person issues on Vennells, after intervention by the Care Quality Commission.
Imperial indicated in its FOI response of 14 January 2021 that it abandoned this external review of FPPR because of Vennells’ resignation from its board:
“Paula Vennells tendered her resignation from Imperial College Healthcare NHS Trust on 30 November 2020. In light of this, and bearing in mind the cost of the investigation and the fact that it is unlikely to report before 31 March, we propose to not go ahead with the review as planned.”
In the trust’s later response of 25 February 2021 it additionally admitted that it had not even agreed terms of reference for the external review by the time of Vennell’s resignation:
“The Trust approached a barrister who agreed to take on the work, but we had not agreed the terms of reference or entered into a contract at the time of Paula Vennell’s resignation. No work was commenced and we therefore do not hold any further recorded information in response to this.”
“We sought external legal advice to check our processes for reviewing our trust executive and non-executive directors’ compliance with the CQC’s Fit and Proper Persons Requirement (Regulation 5). The advice confirmed that our processes are robust.”
The trust has now supplied additional information on this reported legal advice, showing that the advice came from Capsticks LLP in February 2020 and that it focussed mostly on narrow administrative definitions of Fit and Proper Persons:
“We sought advice from Capsticks Solicitors LLP in February 2020 upon receipt of a letter from the CQC about the application of Fit and Proper Persons Requirement (FPPR) to the Trust chair.
The advice received confirmed the Trust’s view that it has robust FPPR processes in place, specifically in relation to the issues raised by the CQC letter.
On the basis of the information provided by the CQC, the requirement of the FPPR in question was whether or not the Trust chair was of good character. In that regard, none of the specific considerations referred to in part 2 of Schedule 4 of the FPPR applied.
Specifically, it was not the case that Ms Vennells:
did not have the qualifications, competence, skills and experience that are necessary for the position of chair (the CQC had confirmed at its last inspection of the Trust, that the senior leadership team had the appropriate range of skills, knowledge and experience)
had health concerns
had been responsible for, been privy to, contributed to or facilitated any serious misconduct or mismanagement in the course of carrying on a regulated activity.
The advice also noted that the regulations state that, in assessing a director’s character, the matters to be considered must include those in Schedule 4 part 2 though not exclusively. The Trust was advised to consider other matters in addition to those specified in Schedule 4 part 2 if they indicated that the chair may not be of good character, which we also endeavour to do.” [My emphasis]
A key question is whether trust directors took the last part of this legal advice seriously.
There is of course a serious flaw in the system. NHS Improvement appoints the chairs and non executive directors of non Foundation NHS trusts, but thereafter the subordinate trusts assume legal responsibility under CQC Regulation 5 Fit and Proper Persons for ensuring that directors continue to be Fit and Proper Persons. It is unfair to place trusts in this position of having to effectively overturn unsuitable appointments by the regulator.
But trust directors are nevertheless highly paid senior officials who should put their duty to the public above their self interest.
We await the outcome of the CQC’s deliberations on the FPPR referrals that it has received about Vennells’ role at Imperial.
The question that CQC must address is whether the trust’s FPPR governance is acceptable, regardless of whether Vennells is departing.
But any criticism of by CQC of FPPR issues at Imperial is a sensitive matter because it would effectively also be a criticism of NHS Improvement and Dido Harding NHSI Chair, who took part in Vennells’ selection as Imperial Chair.
UK whistleblowing law
Subpostmasters were not covered by existing weak UK whistleblowing law, so their countless disclosures to Post Office Ltd about flaws in the Horizon computer system and unsafe prosecutions were not recognised under the law as whistleblowing.
UK whistleblowing needs to be greatly strengthened to cover a wider range of whistleblowers, to prevent cover ups and to deter and sanction those who cover up.
If you have not already done so, please help by signing and sharing this petition to parliament to reform the law:
By Dr Minh Alexander NHS whistleblower and retired consultant psychiatrist 28 February 2021
Summary: A common experience amongst whistleblowers is to find that employers destroy important records in order to cover up. This is a brief post about an example of poor whistleblowing record keeping by ‘Outstanding” West Midlands Ambulance Service NHS Foundation Trust (WMAS), brought to my attention by an NHS worker who prefers not to be named. An FOI request and a related complaint to the Information Commissioner revealed that the trust allegedly held almost no records of meetings on whistleblowing about racism, and a conclusion by the ICO that some of the related correspondence had possibly been destroyed. The trust does not recruit BME staff in proportion to the diversity of its local population. The trust’s workforce race equality data showed that BME staff are disadvantaged in terms of bullying and harassment, equality of opportunity and experience of discrimination. The trust’s Freedom To Speak Up Guardian is corporate – the Head of Organisational Development – and almost no staff concerns are raised with her. The trust’s denial that it held records of an important whistleblowing event calls into question whether the trust Freedom To Speak Up Guardian is keeping adequate records of disclosures made to her.
The ICO’s decision on a complaint about whistleblowing records at WMAS
A decision notice by the Information Commissioner of 20 January 2021, kindly sent to me by an NHS employee who tellingly would prefer not to be named, now reveals that WMAS claimed to have few records of important meetings about race discrimination concerns at the trust in 2017.
On 4 August 2019 the trust was asked for documents relating to whistleblowing meetings as follows:
“Please provide the agendas and minutes of meetings held with WMAS BME staff raising concerns about racist staff, primarily at Willenhall Hub, held on the following dates; 22/07/2017 – WMAS Chief Executive, Dr Anthony Marsh. 24/07/2017 – Meeting with WMAS Emergency Service Operations Delivery Director, Nathan Hudson. 28/09/2017 – WMAS Chief Executive, Dr Anthony Marsh. 09/10/2017 – Meeting with WMAS Chief Executive, Dr Anthony Marsh. Please provide all preceding and following email correspondence relating to the agendas and actions arising from the above meetings”
WMAS claimed that it held none of this information save for two emails, request reference FOI 2782:
“That information comprised two emails associated with Trust staff who were involved in facilitating the meetings, and in which actions had been noted.”
The trust was asked by the requestor to review its response, but still concluded that it held no other information.
The requestor complained to the Information Commissioner that there were other emails (already in his possession) which the trust had failed to disclose, that replies to the two disclosed emails would exist in his view and that he believed that meetings about such a serious whistleblowing matter would have necessitated more records.
The trust told the ICO that it had approached various managers during its search for disclosable documents, including the Head of Organisational Development who was also the Freedom To Speak Up Guardian:
“In its submission to the Commissioner the Trust has told her that an independent search for relevant information was conducted by its IT Department. The Director of Corporate & Clinical Services, the Emergency Service Operations Delivery Director, Head of Human Resources, Head of Organisational Development (Freedom to Speak up Guardian), Senior Operations Manager of Willenhall Hub and the Private Secretary to the Office of Chief Executive were also approached to confirm that no further information was held.”
Astonishingly, WMAS claimed that meeting papers were never generated because the meetings – about serious whistleblowing concerns – were not “formal”
“The Trust has stated that such information was never generated and was never held, because the meetings referred to in the request were not formal meetings.”
The alternative of course is that meeting papers existed and the trust’s claims are untruthful, but that was not proven. Neither option is good.
West Midlands Ambulance Service NHS Foundation Trust’s whistleblowing policy The trust’s policy emphasises that there must be a written audit trail of the response to concerns: “Staff who have raised a concern will receive a written initial response, within 14 days of the stage meeting summarising the issues raised, how the matter will be dealt with and providing details of who will be handling it and how they may be contacted. The person raising the concern will be treated with dignity and respect at all times and kept updated as reasonably possible throughout the process.The member of staff raising the concern will be provided with written feedback at the close of the investigation, or within 28 days, whichever is the sooner advising what actions have been taken to address the concerns. There may be circumstances where it is not appropriate to provide full and detailed feedback where this may infringe a duty of confidence owed by the Trust to a patient or other third party.”
The ICO considered that some of the documents on this whistleblowing incident may have been destroyed by the trust:
“However, it might also be the case that any relevant email correspondence that one or more members of staff once held was routinely destroyed in line with the Trust’s retention schedule.”
The ICO explained that it must rule on whether organisations hold information, not whether they should hold information:
“The Commissioner’s role is not to consider whether a public authority should hold information that has been requested. She must decide, based on the balance of probabilities, whether a public authority did hold information at the time of a request for it.”
and decided in the trust’s favour:
“The Commissioner has therefore decided that, on the balance of probabilities, no information other than the two emails it has provided to the complainant was held at the time of the request. As such, she finds that the Trust has complied with section 1(1)(a) of the FOIA.”
What arises from this matter is that the Freedom To Speak Up Guardian at WMAS, according to the trust’s claims, may not have kept proper records of whistleblowing incidents, when it is part of the role to do so.
This is the national guidance on what records should be kept by Freedom To Speak Up Guardians:
The guidance requires “brief factual summary of the case”, details of action taken and related failures of governance:
“It is important to record actions taken and when and to whom referrals are made, together with a record of how, when and how often the individual speaking up wishes to be contacted. This is also another place to note anything that is encountered as the case is progressed that indicates a barrier to speaking up, or that indicates that speaking up policies are not being followed, or that policies or processes need to be improved.”
I will ask the trust specifically what records are held by the Freedom To Speak Up Guardian in relation to the 2017 allegations of racism and the related meetings.
Other material raising concerns about racism at WMAS
Alongside the above complaint to the ICO, another FOI of 29 March 2020 evident from the What Do They Know website, suggests there may have been very serious problems of racism at WMAS. This FOI request implied that Hitler had been cited as model of leadership at a trust management training centre:
“Dear West Midlands Ambulance Service University NHS Foundation Trust,
1) Please provide the disciplinary policy that applies to allegations of racist behaviour against staff.
2) What disciplinary action would be considered appropriate where allegations of racist behaviour by a member of staff were proven, for example: i) A muslim member of staff being referred to as a terrorist and having a bomb in their bag; ii) A member of the public being referred to by a racist derogatory term; iii) A member of staff declaring that they “don’t like muslims”; iv) A member of staff the dismissing concerns of a BAME student about an offensive term with the phrase slavery ended two hundred years ago; v) A member of staff telling a BAME member of staff that they only achieved because of the colour of their skin; vi) The use of Adolf Hitler as an example of great leadership in a WMAS management training assessment centre; vii) The posting of racist and white supremacist material on personal social media?
3) Does West Midlands Ambulance Service have a zero tolerance policy towards racist behaviour from staff?
4) If West Midlands Ambulance Service does have a zero tolerance policy towards racist behaviour from staff, what does that mean in practice?
5) Does West Midlands Ambulance Service consider that holding and sharing racist views is compatible with continued employment by West Midlands Ambulance Service?
6) Does West Midlands Ambulance Service consider that the employment of front line clinicians that hold racist views constitutes a risk to the BAME patients that they serve?
Yours faithfully,
Martin Waite”
WMAS’ response to this FOI request ignored the majority of the questions without indicating what legal exemption under FOIA was being applied. The trust merely supplied copies of two HR policy documents.
Whatever your views on the controversies surrounding blackface, this does seem insensitive behaviour in a senior public servant.
The Care Quality Commission
In an inspection report of 25 January 2017 the CQC noted that WMAS staff ethnicity did not reflect its highly diverse local population but it also concluded “The trust was actively involved in effective public engagement to recruit staff from Black and Minority Ethnicity (BME) population”. CQC concluded that the trust was Well-Led and Outstanding overall.
CQC also praised WMAS managers for good handling of an incident of whistleblowing:
“Staff from PTS Stoke raised concerns about lack of mental health training and felt unsupported by local leadership. The CEO and senior leaders were extremely responsive and genuinely concerned. They visited the staff the same week, engaged in open discussions and put in place extra mental health training sessions”
Presumably records were available in order for CQC to evidence its claim of good whistleblowing practice, contrasting with the disputed affair over thornier issues of racism.
Freedom To Speak Up at the trust and the National Guardian
The National Guardian’s data on Speak Up incidents at NHS trusts shows little improvement: in quarters 1 and 2 of 2020/21, there were three cases reportedly raised with the WMAS Freedom to Speak Up Guardian.
And of course, where would we be without grinning government propaganda by the National Guardian to cheer us all up and fill us with confidence:
Poor whistleblowing governance and cover ups will continue for as long as robust standards are not backed with the full force of the law.
If you have not already done so, please help by signing and sharing this petition for reform of wholly inadequate UK whistleblowing law:
By Dr Minh Alexander, NHS whistleblower and retired consultant psychiatrist, 27 February 2021
Summary: Dr Julian Campbell a consultant anaesthetist raised concerns with the National Guardian’s Office about bullying management practices at Harrogate and District NHS Foundation and a conflict of interest arising from the fact that the trust Freedom To Speak Up Guardian was married to the medical director. An independent review vindicated his concerns about poor trust governance. Dr Campbell was told by his trust chief executive that the National Guardian contacted the trust Freedom To Speak Up Guardian. This breached Dr Campbell’s confidentiality because he had not given permission for the National Guardian and her Office to contact the Harrogate Freedom To Speak Up Guardian. He was very distressed by the breach. Robert Francis was later asked to urgently protect NHS staff from any other such confidentiality breaches by the National Guardian’s Office. Francis did not address this primary concern and instead kicked the matter into governance long grass by setting off an NHS Improvement complaint investigation. This investigation has been very slow and two key witnesses were not interviewed. NHS Improvement blamed the National Guardian’s former case review manager for the breach of Dr Campbell’s confidentiality. NHS Improvement initially resisted a challenge about its incomplete investigation. However, after Dido Harding was asked to intervene, NHS Improvement made a partial concession and agreed to interview one of the two witness that it failed to question. Most troubling of all, the National Guardian and her Office have not apologised to Dr Campbell nor provided evidence of any improvement in their safeguarding of whistleblowers’ identities. The hubris and disrespect shown by the National Guardian’s Office is breath-taking. Outing a whistleblower is extremely serious. In some jurisdictions, revealing a whistleblower’s identity is a criminal matter. Current, weak UK whistleblowing law fails to specifically protect whistleblower anonymity. Law reform is badly needed.
In August 2018 Dr Julian Campbell a consultant anaesthetist made disclosures to the National Guardian’s Office (NGO) about management bullying at his workplace, Harrogate and District NHS Foundation Trust and a conflict of interest in that the trust Freedom to Speak Up Guardian was married to the medical director. He also informed the NGO that his trust Chair and Chief Executive refused to recognise this conflict of interest.
Dr Campbell was later vindicated by a Deloitte review which confirmed multiple staff reports of bullying management practices, including under the radar, arbitrary restriction of several clinicians’ practice, with management application of “informal capability plans”. The affected staff were sometimes denied representation.
Deloitte also criticised the fact that a lack of staff confidence in the trust’s Freedom To Speak Up arrangements was linked to perceived conflict of interest relating to the trust Freedom To Speak Up Guardian.
The details of the Deloitte review and the later removal of the Harrogate Freedom To Speak Up Guardian can be found here:
The NGO was slow in responding to Dr Campbell’s request for help.
Appallingly, it was not until eight months after Dr Campbell’s original request that he received a substantive response from the NGO.
Simon Pook the then NGO case review manager wrote to Dr Campbell in March 2019, suggesting that he should either “ raise a formal complaint, or request an internal review of the handling of your case”.
Dr Campbell was shocked by this:
“I came to you as the last line of support. I have been treated abysmally by HDFT. Others have been treated abysmally too, but the courage and tenacity it takes to raise a complaint with external agencies is so great that most just want to bury themselves (some quite literally) and hope that it goes away.
To be offered support to raise the issues internally when I had understood that you would be an independent reviewer of the issues that I have raised is, quite frankly, devastating. Who will hold HDFT to account if the National Freedom to Speak Up Guardian won’t?”
Things got worse when Dr Campbell learned that his confidentiality had been breached by the NGO. His trust chief executive told him at a meeting on 11 June 2019that the National Guardian herself had contacted Sylvia Wood, the trust Freedom To Speak Up Guardian.
Dr Campbell had not given the NGO permission to contact his trust Freedom To Speak Up Guardian.
He confronted the NGO case review manager about this, through an email of 13 June 2019.
“It has therefore caused me great distress to discover that the National Guardian did not contact the CEO, as your email indicated she would, but that she in fact contacted Sylvia Wood, who is now able to inform her husband.
Whilst I was happy to allow my identity to be known to the hospital in order to aid the quality of the investigation I did not expect that your first act would be to alert those whom I regard as my oppressors. I believe that the new Chief Executive would have been a more appropriate choice.”
Simon Pook’s reply of 14 June 2019 to the distressed email from Dr Campbell made no acknowledgment of the reported breach of confidentiality, offered no apology and merely stated that the National Guardian had made a telephone call to Steve Russell the Harrogate CEO that morning.
Since that time, Dr Campbell has received no satisfactory explanation for the apparent breach of his confidentiality.
I raised a concern about the reported breach with Robert Francis on 9 August 2020 in his capacity as a member of the National Guardian’s Accountability and Liaison Board, which provides scrutiny of the National Guardian’s work by her funders – the Care Quality Commission and NHS England/ Improvement.
Francis pushed the matter off his desk PDQ:
“Dear Dr Alexander
Thank you for raising for specific concerns about this case. You asked me to enquire about it and I have. I understand that this will now be treated as a complaint made by you, and no doubt you will be hearing further from the NGO.
As for the rest of your email I can only repeat what I have said before, and that I have no intention of withdrawing my support for the FTSU agenda
Kind regards
Robert Francis”
I responded to clarify that I was seeking to urgently make systems safer for NHS whistleblowers who might be forced to approach the National Guardian. I was not seeking to have the issues effectively kicked into the long grass of a complaints process which itself was marred by conflict of interest:
But Francis persisted with kicking the urgent confidentiality issue into the long grass of a complaint process, mirroring what happens to whistleblowers whose concerns are sidelined and who are pushed into adversarial processes.
“Dear Dr Alexander
Thank you.
I will forward your further concerns about confidentiality for those who speak up to the NGO to be taken into account as this matter is considered in the complaint process.
Kind regards
Robert Francis”
Unsurprisingly, NHS Improvement’s complaint process has been unsatisfactory. It has been slow, missing deadlines, and key witnesses were not interviewed.
During the course of the investigation, NHS Improvement revealed the Harrogate Freedom To Speak Up Guardian had commented in correspondence to the NGO (not disclosed to Dr Campbell) that Dr Campbell was expected to retire:
“I have not been able to locate a note of such a call, but an email reply from the FTSU Guardian to the case review manager on 7 June said:
“I have spoken to Steve Russell (CEO) this morning. I believe Dr Campbell has decided to retire but has been in touch with Steve – who had already suggested meeting.”
This is a disturbing detail as Dr Campbell’s retirement should have had nothing to do with the proper handling of his concerns. It was also disturbing that the correspondence was not disclosed to Dr Campbell,
The final NHS Improvement complaint investigation report of 27 January 2021 into the apparent breach of Dr Campbell’s confidentiality was signed off and accepted in full by Andrew Morris, NHS Improvement Non Executive director and chair of the National Guardian’s Accountability and Liaison Board.
NHS Improvement’s carefully worded report blamed the NGO case review manager for the breach of Dr Campbell’s confidentiality:“That it is more likely than not that the NGO contacted the FTSU Guardian to discuss Dr Campbell’s concerns without his specific consent. This was inappropriate in the circumstances of the case and, in any event, the NGO should have notified Dr Campbell in advance of doing this. There is no evidence of the National Guardian, Dr Hughes, contacting contacted the trust’s FTSU Guardian about this case.”
“There is no primary evidence to demonstrate that the NGO contacted the trust’s FTSU Guardian to discuss Dr Campbell’s case without his specific consent. However, the trail of emails indicates to me that it is more likely than not that there was a telephone call between the case review manager and the FTSU Guardian between 3 and 7 June 2019 which discussed his case. I have not seen evidence that the NGO had specific consent to contact the FTSU Guardian in this way.”
Yet the NHSI investigation report was unclear regarding who had been interviewed as part of the investigation and what they had confirmed or denied.
The NHSI investigation was also silent as to whether the National Guardian was party to the flawed response to Dr Campbell’s concern that his confidentiality had been breached.
Also of concern, NHSI revealed that telephone contacts between the National Guardian and her Office and Harrogate District NHS Foundation Trust were not recorded in any detail, undermining accountability.
NHSI concluded that the NGO owed Dr Campbell an apology and that the NGO should improve its safeguarding of whistleblowers’ confidentiality:
“An apology from the NGO for the distress caused, and confirmation of an improved approach to such matters in future, would be an appropriate way of resolving matters and addressing any distress caused to Dr Campbell as a result of this.”
I raised questions about NHSI’s investigation process, based on consultation with Dr Campbell and his wife:
NHSI later clarified that Simon Pook accepted that he had probably contacted the Harrogate Freedom To Speak Up Guardian:
“I have spoken to the case review manager and, although he did not specifically remember all the details, he accepted that the email trails indicate that he had spoken to the FTSU Guardian about Dr Campbell’s case.”
The facts of this case are simple. Dr Campbell flagged his fear that he could not disclose safely internally because his trust Freedom To Speak Up Guardian had a conflict of interest. He was then told by his trust chief executive that National Guardian had spoken to the trust Freedom to Speak Up Guardian without his permission, and he feared that this would have alerted her husband the medical director, with whom he was in conflict.
The key individuals in this affair were:
Simon Pook NGO case review manager – with whom Dr Campbell had negotiated the terms of any NGO contact with the trust – which did not include contacting the Freedom To Speak Up Guardian
Steve Russell CEO of Harrogate and District NHS Foundation Trust, who prior to taking up this post in April 2019 was Executive Regional Managing Director (London), NHS Improvement
Henrietta Hughes National Guardian whom Steve Russell reported had spoken to the Freedom To Speak Up Guardian about Dr Campbell’s case
Sylvia Wood the trust Freedom To Speak Up Guardian
It would have been logical to interview all four of these witnesses.
NHS Improvement clarified that it had questioned only Simon Pook and Henrietta Hughes in its complaint investigation.
The issue of NHSI’s incomplete investigation was referred back to Andrew Morris, who reportedly declined to change course:
“I have discussed with Sir Andrew and he is content that the investigation was reasonable and proportionate.”
Two subsequent emails later to Dido Harding, NHS Improvement has conceded that it will now interview Steve Russell the Harrogate CEO:
“…given your continued concern about this, I have discussed with Sir Andrew again and agreed that I will speak to the Chief Executive at Harrogate in the first instance.”
But significantly, NHSI has not yet undertaken to speak to the former Harrogate Freedom To Speak Up Guardian, who is the one person who would know exactly who from the National Guardian’s Office did or did not telephone her.
NHSI’s reluctance to carry out a straightforward investigation shakes confidence in its process.
This is an unfinished story, and I will report back on the ultimate outcome in due course.
The National Guardian’s and NHS Improvement’s complaint policies
Until now, it was not clear if any appeal mechanism existed in either the National Guardian’s and NHS Improvement’s complaint policies. It was implied that there is no appeal process, because both policies indicate that complainants may go the PHSO if they are unhappy with a complaint outcome.
This contrasts with other bodies as NHS Resolution, Public Health England and the Department of Health and Social Care, which all have a formal appeal mechanism explicitly built into their complaints process.
This seems like good practice in principle. It can potentially spare complainants the lengthy trauma of a PHSO process which may, based on track record, decide not to investigate. It also increases board accountability for complaint handling.
NHSI’s reconsideration and concession that at least the Harrogate CEO will now be reviewed establishes a principle of appeal.
It remains to be seen if NHSI and the National Guardian will formalise this in their respective policies.
The National Guardian failed to respond at all to a request for clarification of whether there was any appeal mechanism in her process, and therefore it seems unlikely that she would treat the matter seriously.
The unapologetic National Guardian’s Office
Meanwhile, Dr Campbell has astonishingly still not received an apology from the National Guardian’s Office.
The National Guardian has also not yet substantively replied to a question put to her on 22 December 2020, about whether she has made improvements to ensure that her Office does not breach whistleblowers’ confidentiality in the future.
“2 December 2020
Dear Henrietta,
The National Guardian & whistleblowers’ confidentiality
As NHS Improvement’s complaint investigation has been delayed several times and will drag on to the New Year at least, I write to ask the most pressing question:
Has the National Guardian’s Office made the necessary policy and practice changes to ensure that it does not breach whistleblowers’ confidentiality in the future?
If it has, please could you advise what changes that have been made.
Yours sincerely,
Minh
Dr Minh Alexander”
This lack of substantive response is despite further reminders.
The silence and the lack of apology are not reassuring of good governance by an agency, which given its stated purpose should be an exemplar. It is also a reflection on whether the National Guardian’s Office is – in the parlance of her employer – “Well-Led”.
I would advise any NHS whistleblowers who are forced to turn to the National Guardian’s Office to be extremely cautious, to get everything in writing and to consider making requests as needed for personal data under a Subject Access request, if they have concerns about any clandestine communication and or collusion between the National Guardian’s Office and their employer.
UK whistleblowing law and whistleblower anonymity
Current UK whistleblowing law is wholly ineffective and unlike EU whistleblowing law, it does not specifically protect whistleblowers’ rights to anonymity nor sanction those who fail to protect the identity of whistleblowers.
I have written to the CQC chief executive, the National Guardian’s de facto line manager, to raise a concern that the National Guardian’s Office has failed to apologise for the breach of confidentiality or demonstrate learning. I have also asked the National Guardian’s funders, CQC and NHS England/ NHS Improvement to examine the effectiveness of the National Guardian’s Accountability and Liaison Board given that its two key members Robert Francis and Andrew Morris were both aware of the confidentiality breach but have not ensured an appropriate NGO response to this failure.
By Dr Minh Alexander NHS whistleblower and retired consultant psychiatrist, 23 February 2021
Summary: Barts Health NHS Trust has been found guilty of victimising Jeyran Panahian-Jand a bona fide whistleblower who raised concerns that the trust was discriminating against BME staff in unfavourable allocation of work. The Times covered this story today, but missed out the most serious aspect: the trust’s cover up of investigation findings that were in the whistleblower’s favour.
Most seriously, the ET concluded that a trust manager who is an associate trust director was part of a trust cover up of investigation findings that there was race discrimination at the trust: “…we are very concerned here that the Trust went to the expense of an independent investigation but has then misrepresented and diminished the findings of that investigation to the complainant and the ward manager”.
The trust has a predominantly white trust board (fourteen of eighteen directors) despite its catchment being one of the most diverse. The trust’s own documents show that based on 2011 data, only 41% of the trust’s catchment area is composed of white people.
Barts also relies on an outsourced Freedom To Speak Up Guardian, supplied by a private company, which carries a risk of reduced trust board accountability.
The details of the case and background issues about governance problems at Barts follow.
MsJeyran Panahian-Jand v Barts Health NHS Trust whistleblowing case
An Employment Tribunal has found that Jeyran Panahian-Jand a paediatric bank nurse at Barts was victimised after she made public interest disclosures on 14 May 2019 about staff racial segregation on a ward where she had worked, and raised a concern that white staff were being treated preferentially in terms of work allocation.
Just two weeks after whistleblowing, on 30 May 2019 she was banned from working on Acorn ward, Whipps Cross Hospital on insubstantial allegations of misconduct. She was accused of continuing to talk about her concerns after the ward manager claimed they were upsetting other staff and that she should stop airing them.
Ms Panahian-Jand was not allowed back to work on Acorn ward even after an investigation found there was no case against her. The trust failed to give her the findings of the investigation and astonishingly, she had to make a Subject Access Request to obtain the investigation report.
The trust dragged out her restriction wholly unreasonably, and the ET had to make a recommendation at the time of issuing its judgment on10 February 2021 that the trust should lift the ban against Ms Panahian-Jand working on Acorn ward within 4 weeks:
“Pursuant to section 124 of the Equality Act 2010, the Tribunal recommends that, no later than 4 weeks after this Judgment is sent to the parties, the restriction on the Claimant working at Acorn Ward and at Whipps Cross Hospital be removed.”
The Employment Tribunal concluded that the ward manager handled Ms Panahian-Jand’s whistleblowing concerns unfairly and had exaggerated claims that other staff were upset and did not want Ms Panahian-Jand to return to the ward.
The ET concluded that there was only a “loud minority” who were hostile to Ms Panahian-Jand and that this should not have stopped her return after the trust found no case to answer.
“We are not satisfied that there are any more than 4 members of staff on a ward of 60 who are concerned about the Claimant’s return. They have formed a loud minority.”
The ET determined that the ward manager did not respond to Ms Panahian-Jand’s whistleblowing appropriately because she was concerned Ms Panahian-Jand’s disclosures reflected badly on her management of the ward.
“We acknowledge that Mrs Roberts was an inexperienced manager. We consider her memory of the staff response on Acorn ward is likely exaggerated because she herself was uncomfortable and upset by the allegations as a reflection on her own management. She had wanted a happy ward.”
“Mrs Roberts was plainly herself uncomfortable at hearing the allegations. She had not wished to deal with them in an informal way, contrary to both the Whistle-blowing procedure and the Dignity at Work procedure, and indeed had straightaway rejected the correctness of the allegation about allocation. We have concluded thatMrs Roberts saw them as a reflection on her management.”
The trust commissioned an internal investigation into the counter-allegations against Ms Panahian-Jand which the ET noted came to an “unambiguous” conclusion that there was no case to answer. The investigator reportedly concluded that Ms Panahian-Jand had been wrongly suspended on flimsy evidence.
The trust however delayed providing Ms Panahian-Jand with this investigation report despite several requests. Extraordinarily, Barts only gave her the report after she made a Subject Access Request for it.
“Despite the Claimant’s many, polite requests, Mrs Kara’s report was not provided to her until she made a subject access request for it.”
Barts commissioned a quasi-independent investigation into her public interest disclosures:
“The Claimant’s race discrimination complaint was investigated by Mrs Cooper-James, Head of Investigations Services at London Audit, which is hosted by the Trust and therefore to some extent independent of it.”
There was bias by the trust from the outset. The ET concluded that internal correspondence between Mrs Stephenson Associate Director of Nursing for Children and Simon Steward (then Head of Human Resources, and now Head of People at Whipps Cross) showed that Mr Steward was hoping that Ms Panahian-Jand’s allegations of race discrimination would fall apart:
“79. Mrs Stephenson asked Mr Steward whether a 6-8 week estimate was reasonable for the investigation. He answered: If a full-time investigator is on this, I think it is feasible to do this. Many of the points are at this stage, statements without evidence and we would need to clarify who witnessed them. I have added in complaints from patients and staff because if there are none, the allegations, begin to fall apart. (our emphasis) .
80. The Claimant suggests this shows Mr Steward’s wish to see the allegations fall apart. Mr Steward said he was simply adding in that complaints should be looked at as they would provide independent evidence.
81. While it may have been relevant to look for complaints, that there had been none in the past, does not necessarily suggest that this complaint would be without merit. We therefore agree with the Claimant that this wording does suggest a hope that the complaint would fall apart.”
Despite the trust’s biased approach to the investigation of Ms Panahian-Jand’s whistleblowing disclosures, the relatively independent investigator concluded there was evidence to support Ms Panahian-Jand’s concerns:
“Mrs Cooper-James did find evidence to support the three race discrimination allegations first raised informally with Mrs Roberts on 11 May 2019 (allocation; groups on the ward, and bullying)”
Ms Goldsmith the then Head of Midwifery and now commissioning manager was one of the managers handling Ms Panahian-Jand’s case. According to the ET, she and Simon Steward minimised the investigation findings of race discrimination.
In their respective witness statements to the ET, they reportedly both used the phrase “‘no real evidence of discrimination’”. The ET described their claim as “patently incorrect” and castigated their distortion of the investigation findings:
“Why have both of these witnesses told the Tribunal there was no real evidence of discrimination, when on any fair reading of Mrs CooperJames’ report there was some? We are astonished by this. The Trust has sought to hide in its summary of the report, evidence of race discrimination found in the investigation. Mr Steward plainly did not want these findings aired and it supports us in our conclusion that he hoped the allegations would fail.”
Simon Steward drafted an outcome letter for Ms Goldsmith which falsely claimed that three of Ms Panahian-Jand’s central concerns had not been upheld:
“Mr Steward drafted a letter for Ms Goldsmith, which summarised Mrs CooperJames’ findings in a letter to the Claimant on 4 February 2020 (498). We have only looked at those 3 allegations that the Claimant raised initially, but the summary is not fair as Mr Steward accepted in his oral evidence:
84.1. Allegation 6: ‘If there is evidence of racial discrimination of staff members particularly those from non-white backgrounds’. Mr Steward’s summary says that ‘No evidence was found though divisions were expressed and diversity and inclusion training was recommended.’ Whereas Mrs Cooper-James reported ‘Evidence has been found of racial discrimination against staff. Non-White staff speak of a definite divide within the Ward according to race. It is indicative that all but one of the BME staff interviewed expressed that a divide was present. However, all white staff expressed there was no such divide.’
84.2. Allegation 23: ‘If patient allocation is equitable across the Team on duty regardless of race or colour.’ Mr Steward writes ‘In order that there is clarity around the allocation of patients, it is recommended that all staff are involved (where practicable) in the allocation of patients.’ Whereas Mrs Cooper-James plainly concludes there is evidence to substantiate the allegation because all but one of the BME staff stated they felt they were given the heavier workload (376-377).
84.3. Allegation 26: in relation to staff bullying. Mr Steward writes: ‘If staff believe there is bullying on Acorn Ward. Other members of staff should be invited to make complaints if they wish to do so.’ Whereas Mrs Cooper-James stated in terms that evidence had been found to substantiate that staff believed there was bullying on the ward.”
Ms Panahian-Jand experienced retaliatory intimidation from a nursing colleague who physically blocked her path on two occasions. The trust failed to investigate her grievance about this,
“The Trust did not investigate the incident with Miss Hook even though the Claimant reported it to HR promptly and was told it would be reported. That, too, was a disadvantage because the Claimant could reasonably view it to be the Trust not taking seriously a complaint of hostile behaviour towards a whistle-blower/someone who complained of race discrimination. This was contrary to the Trust’s whistle-blowing policy, which made it clear employees should be able to challenge inappropriate behaviour without fear of reprisal.“
Yet the trust speciously justified its hostile actions against Ms Panahian-Jand, claiming it was concerned about her safety. The ET treated this with the contempt it deserved:
“90.4. Mr Steward referred to the safety of the Claimant as an issue because of her complaint. If at that point it was felt she was unsafe, then it was for the Trust to consider suspending/restricting the individuals complained about. It was not within their procedures to suspend a complainant. In December when finally asked about this the Claimant did not have safety concerns.”
Instead of protecting Ms Panahian-Jand from victimisation for raising concerns about race discrimination, the trust effectively penalised her for filing a grievance about being physically intimidated in that it used the grievance to continue her ban from Acorn ward:
“Indeed Mr Steward’s initial email shows that the hold-up is all about the fact of the Claimant bringing her grievance (a protected act) and the potential upset of other staff members. The grievance would not have caused him to restrict the Claimant and should not have caused the continuation of the restriction.”
The ET judgment ended with the following damning comments:
“217. We are concerned that the approach of managers to this complaint seems to have taken little heed of the Trust’s whistleblowing policy. And no manager, even the Director of People, appears to have fully understood the victimisation provisions of the Equality Act. Complainants should not be treated as the problem.
218. Finally, we are very concerned here that the Trust went to the expense of an independent investigation but has then misrepresented and diminished the findings of that investigation to the complainant and the ward manager. Mrs Cooper-James’ found some evidence of potential race discrimination in work allocation and divisions on the ward. These findings were diminished by the Trust’s internal summary (and in witness statements to us) to a point where it hardly appeared that there may be a problem. There is plainly still much work to be done.”
The Times covered the case today but did not acknowledge the ET’s concern about a managerial cover up of investigation findings.
Ms Panahian-Jand may have ‘won’ her ET claim and been awarded £26,083.19 compensation for her pains, but the matter has the potential to seriously affect her career, as the NHS can have a long, vindictive memory. She has also suffered a totally avoidable ordeal simply because a few individuals sought quite foolishly and unethically to manage individual and organisational reputation. There was no existing mechanism in law that she could trigger at early stage to challenge the mishandling of her case.
But will Barts’ misconduct matter? Will the managers involved be held to account, or will they be protected? Did they harm a whistleblower because they believed it was what trust senior leadership expected of them? If so, promotion may be more likely than disciplinary action, but we shall see. I will ask Barts what learning it has taken from this case.
I should say that I have found Barts to be one of the worst trusts in terms of unaccountability and blocking of FOI requests about whistleblowing governance, which points to senior leadership failure.
It is also worth noting that Barts have relied on the private services of a company which specialises in providing outsourced Freedom To Speak Up Guardians. This is a means by which some NHS boards can potentially reduce accountability.
I am not sure if the Head of People for Whipps Cross would be seen as a director for the purposes of CQC Regulation Fit and Proper Persons (FPPR). He appears on the trust website as an associate director:
But CQC has in the past indicated that it would consider whether managers’ roles were effectively director posts whatever their titles.
A gap in the current system is that middle grade managers who harm whistleblowers fly under the radar of FPPR, but may at a future point be promoted to positions of greater power where they can potentially inflict more harm on subordinates.
It is cause for concern that the NHS establishment continues to resist proper managerial regulation.
Whistleblowers need the proper protection of law and strong enforcement systems.
If you have not done so, please sign and help share this petition to parliament for whistleblowing law reform.
As ever, the National Guardian’s propaganda has given Barts a cloak of respectability, albeit somewhat threadbare and moth eaten:
Typical of many NHS organisaitions, Barts has a veneer of diversity propaganda, as evident from its public messaging. A gallery of hypocrisy and wishful thinking follows: