By Dr Minh Alexander Retired consultant psychiatrist 30 April 2022
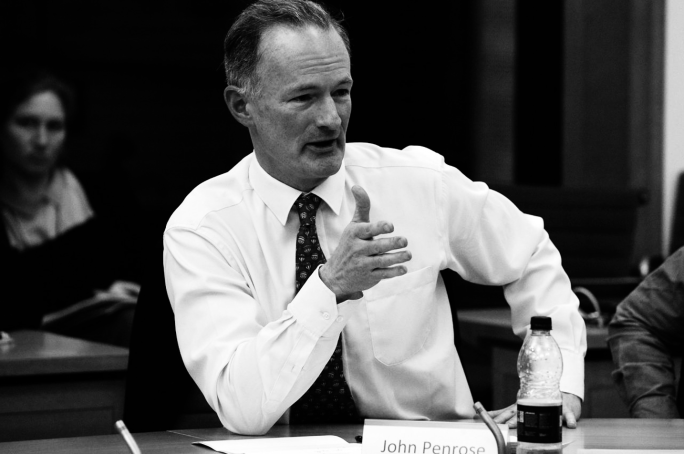
Hot on the heels of widespread concern about the government’s seizure of control over the formerly independent Electoral Commission, its Anti Corruption Champion John Penrose MP is now backing a proposal to create a whistleblowing regulator that will be under the government’s control.
Penrose, a Tory backbench MP for Weston Super Mare, better known by some as the husband of Dido Harding, formerly Chair of NHS Improvement and head of the £37 billion Test and Trace programme which reportedly ran out of money.
BACKGROUND INFORMATION ABOUT THE ANTI CORRUPTION CHAMPION This is a link to information on the Home Office website about John Penrose’s role as The PrIme Minister’s Anti Corruption Champion: https://www.gov.uk/government/people/john-penrose
This is an article about the role of the Anti Corruption Champion based on released documents:
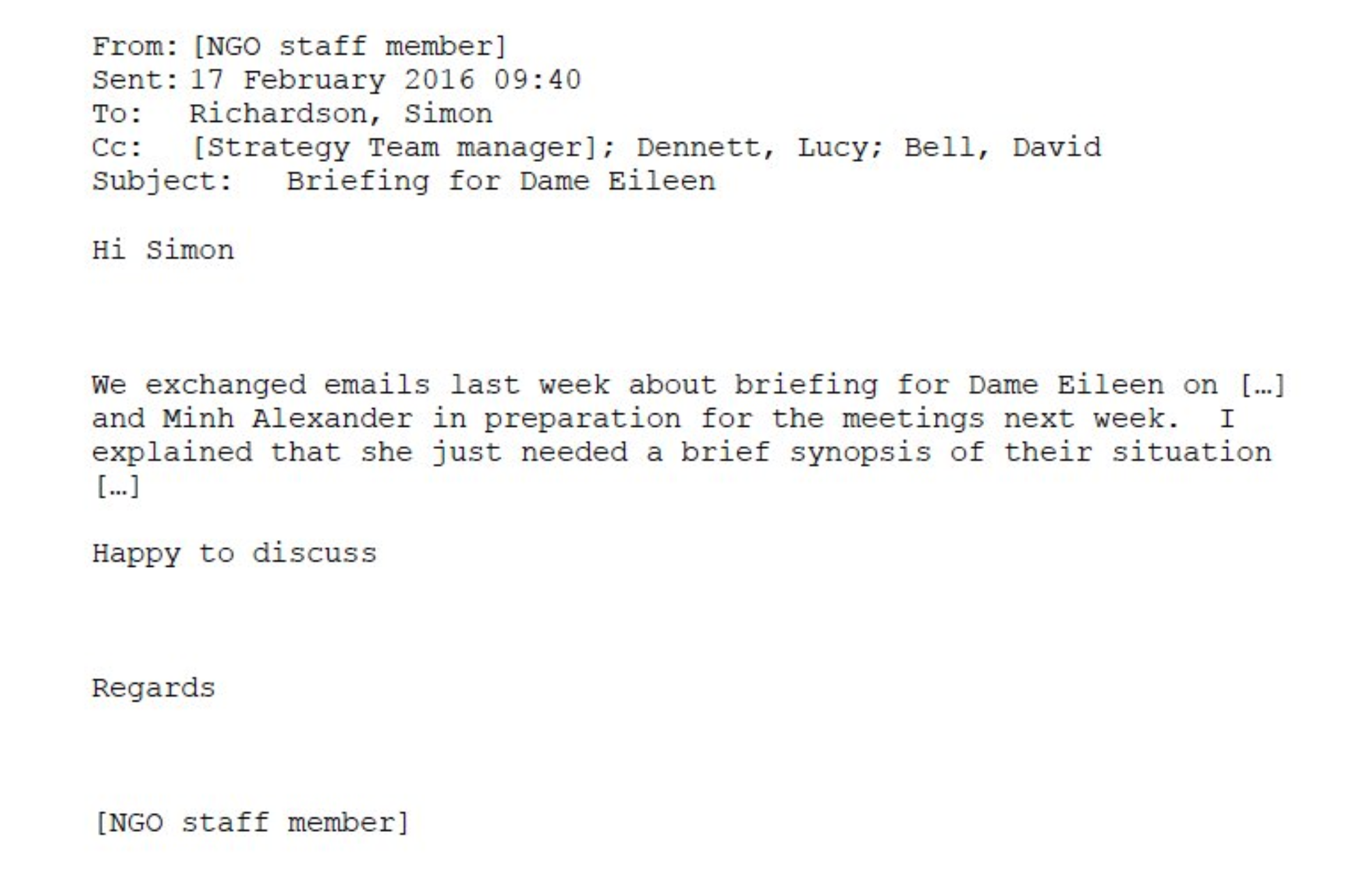
The Telegraph reported that Penrose was backing the Bill read into parliament on 26 April 2022 by the controversial Whistleblowing All Party Parliamentary Group and its even more controversial secretariat, the organisation WhistleblowersUK.
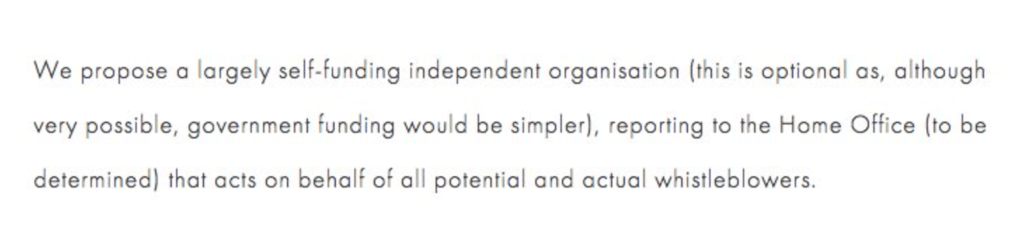
This Bill, which has still not been made transparently available despite numerous requests to the APPG Chair and the leadership of WhistleblowersUK, reportedly set out to establish an Office of the Whistleblower.
“[The Office of the Whistleblower] will …report back to the Government.”
This fatally undermines its independence and sinks many future whistleblowers, public sector whistleblowers in particular, who raise concerns about government failures.
A concern held by many experienced whistleblowers and respected senior academics in the field is that the Bill is a Trojan horse to allow the billion dollar US bounty hunting industry to finally break through into the UK market, after many years of repeated rebuffs.
Penrose gave a little reported interview to GB News on 26 April. I apologise for giving any oxygen to this channel but I do so here in the public interest. Penrose seemed to imply that he was speaking as the Anti Corruption Champion and that “we”, as in the government, thought the Robinson Bill a “good set of suggestions” but that alternative good ideas would be considered:
“I’m sure we’d be all ears”
The timeline of events raises some questions about political tactics and gameplay to shoe-in bounty hunting that is targeted at lucrative financial recovery from the financial sector – the real target and prize for the bounty hunting lawyers. Bounties in the US financial sector can be huge – up to hundreds of millions in some cases. A vast proportion of this goes to the lawyers.
The middlemen, the lawyers, always win. Whistleblowers and the public not so much. The bounty hunting model abandons many genuine whistleblowers, it wastes vast sums in obscene rewards to individuals that could be spent for the common good and it gives whistleblowers and whistleblowing a bad name.
Robinson’s Bill had its first reading on 26 April with a note in Hansard that the second reading would take place on 6 May, however, parliament was then prorogued.
WhistleblowersUK gave an undertaking before the first reading that the Bill would be published as soon as Robinson had made her speech. But the Bill still remains withheld despite numerous requests.
A careful examination of John Penrose’s interview to GB News on 26 April 2022 may reveal the reason why the second reading of Robinson’s Bill was curiously scheduled, and why the fabled Bill has not materialised:
“John Penrose MP5.01: Yeah, I’m waiting for a government minister to say mañana at the dispatch box, that would be a parliamentary moment. But you’re right, it’s always a problem of timing, of getting space in the legislative timescale to do this sort of stuff. There is however, some legislation coming up, there’s an Economic Crime Bill which will we’re hoping will be coming up in the next couple of months. We could put some whistleblowing clauses in that to solve some of the problems that you and I are talking about here. So the time is now, the moment is available and so even if we can’t get a full blown Whistleblowing Bill Act stand alone, we may be able to get some of these things that I’m talking about into another piece of legislation quite soon if the government is willing. That’s the reason why I’m supporting Mary Robinson’s Bill today. And I hope it will attract some attention and perhaps get a bit of a following wind.”
So, was Robinson’s ten minute motion just a political device by the bounty hunting industry for creating some media noise, using mainly unsuspecting whistleblowers from all sectors as camouflage? When in fact the target was the rich bounties from the financial sector?
This is the full transcript of Penrose’s interview for those who are interested:
Penrose’s grasp of whistleblower detriment seems a little tenuous. Perhaps he misspoke but he seemed to suggest that whistleblowers are pursued in the Employment Tribunal by their former employers and colleagues:
“…you may find yourself being pursued for.. through an Employment Tribunal effectively for what your colleagues think of as betraying secrets”
Penrose gave excessive emphasis to the importance of “guidelines” associated with Robinson’s Bill, as if the acres of guidelines that we have had for over twenty years have ever protected any whistleblower.
There was also a hint of sympathy for the Devil in his comments that whistleblower reprisal is “understandable” and “human”, although he does acknowledge that it is “really unacceptable”.
There is an implication running through his interview comments that his focus is on crimes and the police.
This is interesting because WhistleblowersUK have in the past suggested that the Office of the Whistleblowers should be located in the Home Office, which is where John Penrose’s role as Anti Corruption Champion is also located. So who knows for how long these conversations have been going on? And what a horrendous thought: whistleblower welfare under the control of the highly suppressive Home Office.
Penrose is not alone in welcoming the Robinson Bill. A number of whistleblowers who are not from the financial sector have been gulled into supporting the Robinson Bill, when the bounty hunters have little interest in helping them. There is no money in poor healthcare or social care quality or child abuse. Some have definitely not seen the Bill. I have been sent correspondence which shows this, and thank those who shared it with me. It seems likely that many others have not seen it either. This reflects badly both on the credulity of those who have acted uncritically and also on the APPG’s undemocratic manipulation and its lack of accountability. A deep irony when whistleblowing is the issue, but perhaps not so much if this is in fact just about lucre. And of course, a few parties may be fully complicit with the venture. Some have literally been dining out on it.
Notwithstanding, if you are opposed to profiteering from whistleblowing, why not make your feelings known to the The Prime Minister’s Anti Corruption Champion, and suggest that he listens to all voices and not just industry lobbyists with a financial interest? After all, he is the Anti Corruption Champion and ought to recognise a conflict of interest when he sees one.
I have written to Mr Penrose as follows:
BY EMAIL
John Penrose MP
The Prime Minister’s Anti Corruption Champion
Home Office
30 April 2022
Dear Mr Penrose,
Protecting the public interest in the reform of UK whistleblowing law, discouraging profiteering and conflicts of interest and influence by lobbyists
I write to you in your Home Office role as The Prime Minister’s Anti Corruption Champion.
I note with thanks that you have taken an interest in reform of UK whistleblowing law, which as you say is well overdue for reform.
UK whistleblowing law was in fact fatally flawed from inception over twenty years ago because it was designed to ignore whistleblowers’ concerns and it treated whistleblowing as an employment dispute rather than a matter of public protection. It placed the whole burden on whistleblowers and placed virtually no responsibility on the State.
I see that you have backed Mary Robinson’s Bill as read into parliament on 26 April 2022. I am afraid that the Bill remains unpublished despite an undertaking by her APPG secretariat to publish it on that same day, so there has been no opportunity for real debate or scrutiny. Notwithstanding., my view is that the Bill is fatally flawed by Ms Robinson’s proposal that the whistleblowing regulator should be under government control. This creates unacceptable conflicts of interest and great dangers for the many whistleblowers who raise concerns about government failures.
There are also concerns that the legislation is intended to generate litigation and business for bounty hunting lawyers, which is not a lean or efficient manner of running public services. You indicated that the government would be “all ears” regarding better ideas, and as such I refer you to the US Office of Special Counsel for federal whistleblowers which has nimble powers of redress at a stage of an earlier stage whistleblower’s journey, before all has been irreversibly laid to waste. This Office can restore unfairly lost career progression or expunge unfair disciplinary records, and allow whistleblowers to return to their lives in a way that financial compensation after the event cannot. This Office is run with a much stronger public interest ethos than the hybrid model espoused by the Robinson Bill which gives entry to private interests.
In the same vein, please see this paper, now published in International Journal of Law and Management on non-financial redress for whistleblowers in the form or redeployment and re-employment. Very large public sector employers such as the NHS have no good reason not to run a re-deployment scheme across the range of its organisations. This would ensure efficient retention of expensively trained workforce, instead of the wasteful dismissals and de-skilling that we currently see in whistleblower cases. At present there is only a very unsatisfactory post-dismissal employment-finding support scheme for NHS whistleblowers.
Please see this letter to Margaret Hodge MP which contains more details about the need for public interest principles in any reform of UK whistleblowing law, to prevent hijacking by those who would profiteer from it.
The letter references the Public Interest Protection Bill by Dr Philippa Whitford MP which was written with principles of early conflict resolution and minimisation of destructive and wasteful litigation in mind. I hope those principles would be attractive to any government interested in efficiency and in rooting out conflicts of interest that the Robinson Bill is likely to create.
May I also emphasise that it is not a want of guidelines that have failed UK whistleblowers. We have been awash with guidelines for over twenty years. What has been lacking is a legal duty to act on disclosures, a proactive legal duty to protect whistleblowers (as opposed to a facility for retrospective compensation), and fit for purpose enforcement including criminal penalties for individuals. Those are the three critical pinch points that new legislation should address.
I would be very grateful If you could set up a listening exercise to formalise receipt of evidence from all interested parties who might wish to share good ideas with you on whistleblowing law reform, with respect to your comment to GB News that you and the government would be “all ears” for good alternative proposals to those of the Whistleblowing APPG.
I do hope that the APPG’s proposals will not be inserted into the Economic Crime Bill without fair and democratic consideration of other view points, especially from those with no economic interest in the policies.
Lastly, I submitted an FOI to the Home Office (see below) essentially to find out more about the Bill that Mary Robinson and her APPG have purportedly drafted, due to the failure by the APPG to be transparent about what it is they are asking the public support. If you are minded to simply let me have a copy of the APPG Bill and some of the contextual information that I have asked for, I would be extremely grateful.
With best wishes,
Dr Minh Alexander
Retired Consultant Psychiatrist and NHS whistleblower
FOI REQUEST TO HOME OFFICE 30 APRIL 2022
From: Minh Alexander <REDACTED>
Subject: The Prime Minister’s Anti Corruption Champion’s support of a whistleblowing Bill to establish an Office of the Whistleblower
Date: 30 April 2022 at 00:12:57 BST
To: FOI Requests Home Office <REDACTED>
Reply-To: REDACTED
Dear Sir,
The Prime Minister’s Anti Corruption Champion’s support of a whistleblowing Bill to establish an Office of the Whistleblower
The Prime Minister’s Anti Corruption Champion John Penrose MP recently lent his support to a Bill proposed by Mary Robinson MP to establish and Office of the Whistleblower which was read in under the ten minute rule on 26 April.
Mr Penrose gave an interview to GB News about this matter and his support for the Bill was also reported by other media outlets.
Please can the Home Office disclose:
– What consultations took place between Mr Penrose and Ms Robinson and or the Whistleblowing APPG which she chairs, or its secretariat the organisation WhistleblowersUK, which led up to Mr Penrose’s decision to support the Bill?
Were there meetings and or correspondence? Please give details
– Please indicate at what point Mr Penrose had sight of the proposed Bill in question, and which version of the Bill informed his decision to support the proposed legislation?
– Please disclose a copy of the version of the Bill of which Mr Penrose had sight
– If Mr Penrose did not actually see the Bill proposed by Mary Robinson, please also disclose this
– Please disclose if Mr Penrose discussed the possible future location of the proposed Office of the Whistleblower with Ms Robinson and or the Whistleblowing APPG or its secretariat, WhistleblowersUK
– Please advise if any possible government Departments were identified to oversee the putative Office of the Whistleblower, for example, was the Home Office discussed as a possible location for the new whistleblowing regulator?
Yours sincerely,
Dr Minh Alexander
RELATED ITEMS
These posts relate to concerns about the organisation WhistleblowersUK, which has a history of charging whistleblowers for services:
By Dr Minh Alexander retired consultant psychiatrist 28 April 2022
This is a very brief post to share the High Court judgments from the important and widely reported case brought by two grieving daughters against the UK government for its deplorable handling of care homes during the pandemic.
Our government of extremists and law breakers has a track record of holding life very cheap. Especially life that is of colour, life that is economically unproductive and life that it generally deems unworthy of life, to coin a phrase from an egregious era of the twentieth century.
The current mass COVID denial that the government has engineered and its modelling of callous disregard for hundreds of daily continuing COVID deaths perhaps numbs some people to earlier deaths in the pandemic.
Notwithstanding, the government policy of recklessly seeding COVID into care homes via hospital discharges has now been examined by the High Court and found wanting.
The High Court recognised this as “an important and legitimate claim” and it noted that staggeringly, about 20,000 care home residents in England alone died in the first COVID wave.
This is the core of the Court’s finding which has determined that the government acted unlawfully:
“The common law claim succeeds against the Secretary of State and Public Health England in respect of both the March Discharge Policy and April Admissions Guidance documents to this extent: the policy set out in each document was irrational in failing to advise that where an asymptomatic patient (other than one who had tested negative) was admitted to a care home, he or she should, so far as practicable, be kept apart from other residents for 14 days.“
That is to say, whilst some some care home staff made great sacrifices, locked themselves away from their families and lived on site at work to protect their vulnerable residents, HM Government undermined their efforts and recklessly sent infection into their care homes.
There are few details publicly available about the law.
I have today written to Margaret Hodge and some other senior parliamentarians, who have taken an interest in whistleblowing matters, about concerns that the public interest should be properly safeguarded in any process of law reform, and not hijacked by private interests.
The correspondence follows:
BY EMAIL
Dame Margaret Hodge MP
House of Lords [NB This should state House of Commons]
25 April 2022
Dear Dame Margaret,
Discouragement of financial incentives for whistleblowing in the UK and profiteering from whistleblowing
I write to you in acknowledgment of your longstanding support of whistleblowing and work on whistleblowing as former Chair of Public Accounts Committee and more recent interventions, and to ask for your help in ensuring that future reforms are guided along a steady path of public interest. This is with respect to your continuing interest in much needed reform of UK whistleblowing law.
There has unfortunately been steady pressure in recent years for a breakthrough from the US legal market into the UK of the bounty hunting model, most applicable to the financial sector, for recovery of enormous sums and commensurate rewards for reporters. This is a billion dollar industry for litigators.
The US bounty hunting model serves the State’s narrow financial needs for recovery of large sums lost to fraud but it does not promote a healthy whistleblowing culture or justice. It does not reliably protect most whistleblowers and leaves many genuine whistleblowers in the cold. It also puts the good name of whistleblowers and whistleblowing in jeopardy, which adds to the difficulties that whistleblowers already face with credibility.
Of huge importance, the US bounty hunting model does not concern itself with whistleblowing that is about protecting the person, if there is no money to recover. Thus it neglects swathes of important whistleblowing such as that in health and social care.
The UK Whistleblowing APPG originally proposed an Office of the Whistleblower such as that in the US which recovers money for the State using the bounty hunting model. The APPG’s model had the added feature that this Office would effectively act as a broker for approved private law firms and other entities – passing on business to them:
“…form and maintain a panel of accredited legal firms and advisory bodies to advise and support whistleblowers”
I am very uneasy about this, given that the Whistleblowing APPG was established with the involvement of and funding from a major US bounty hunting law firm from the outset. This is in the context of the longstanding general concerns about APPGs serving as lobby groups for private interests and hostile State interference.
A litigation heavy model is also wasteful for the public purse and traumatic for whistleblowers, because it implies prolongation of conflict.
A much leaner and more just model, with a better public interest ethos is that operated by the US Office of Special Counsel for federal whistleblowers. This Office has powers to direct non-financial redress such as restoration of lost career progression and expunging of unfair disciplinary records. This is much more in line with what most whistleblowers want and need – nimble, proactive protection to get back to their lives rather than retrospective compensation after everything lies in smoking ruins, whilst lawyers profit the most.
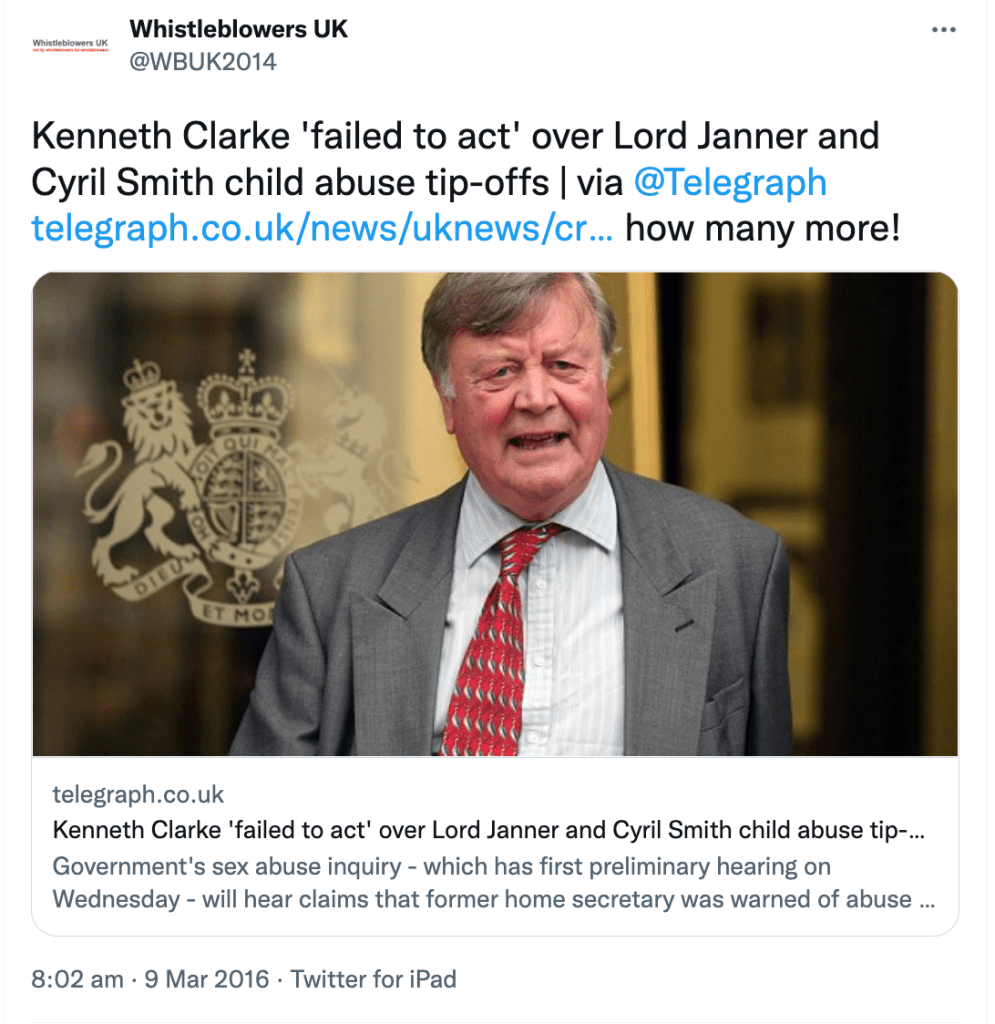
There are moreover concerns about WhistleblowersUK the secretariat of the Whistleblowing APPG, which have been raised a number of times with parliament. I copy below in the appendix links to some of the evidence that has been submitted to APPG members. This includes a thorough due diligence review by well known corporate whistleblower Wendy Addison, which raised concern about WhistleblowersUK’s direct role in supporting the bogus Westminster paedophile ring whistleblower Carl Beech.
Some of the other evidence that has been submitted is more sensitive and not suitable for sharing in the public domain. You may be aware that Norman Lamb resigned as APPG Vice Chair because he was unable to get reassurances from the CEO of WhistleblowersUK to questions that I raised with the APPG. He also received other evidence of concern.
Please note this WhistlebowersUK document, from a whistleblower who contacted the organisation – it shows that WhistleblowersUK asks whistleblowers for a fee of £100/hour for services and 5% of settlements and awards.
Please also note this ET judgment which revealed a bill by WhistleblowersUK for services charged at £150 per hour for sorting “documents into chronological order” in a whistleblower case. This claim was withdrawn after the ET Judge queried the status of the organisation under regulations for claims management.
“These actions that benefit society should be encouraged and recognised by way of financial compensation, and other forms of recognition, separate from that awarded by the tribunals. The amount can be determined by the Office of the Whistleblower.”
WhistleblowersUK penned a flyer in March 2022 about “compensating” whistleblowers which was a response to John Penrose MP discouraging financial incentives for UK whistleblowers. This WhistleblowersUK flyer in fact promoted the US reward system and it claimed “almost every whistleblower becomes dependent on compensation because of the catastrophic impact on their lives and those around them”. The point here is that well designed whistleblowing law should prevent catastrophic harm. It is only weak whistleblowing law that results in distraction from whistleblowers’ public interest disclosures and ends up with a secondary quagmire of employment dispute and a legal circus.
I note the press reports that the Whistleblowing APPG is proposing criminal penalties – which are welcome – but also fines of up to £18 million against organisations for whistleblowing breaches. I would be concerned if such fines are applied to the public sector because of the impact on public services. I would also be concerned if such monies are ultimately transferred from the public purse to private law firms or other private entities via the Office of the Whistleblower.
If any law maximises conflict, disruption and litigation and if that benefits middlemen the most, it will hardly serve either the public interest or whistleblowers.
There should be no inappropriate closeness between any putative whistleblowing regulator and private law firms or other private entities, nor conflicts of interest in the establishment of any new whistleblowing regulator. The creation of a new whistleblowing regulator should not be a Trojan horse for bounty hunting nor in effect construct a front door for the private whistleblowing litigation and compliance industry.
There should be no end effect of targeting resources on financial recovery and any lucrative bounties which that may net for some parties, at the expense of protecting the health and safety of the public.
A dysfunctional whistleblowing regulator would be the very worst of all worlds for the public and for whistleblowers. It would compound the serious deterioration we have seen in UK governance, not relieve it.
Lastly, may I refer to you the principles of the Public Interest Protection Bill originally laid in parliament by Dr Philippa Whitford.
Importantly, this gives primacy to the system response to whistleblowers’ concerns and therefore the public interest.
It also seeks as a principle to minimise both harmful employment consequences and related litigation, and so to avoid waste.
Dr Whitford’s Bill ensured that a whistleblowing regulator should be fully independent of government. This is crucial. I emphasise it because WhistleblowersUK at one point proposed that the Office of the Whistleblowers should be located in the Home Office, one of the worst Departments for suppression:
I believe WhistleblowersUK has now deleted this post about the Home Office.
Dr Whitford’s Bill also contained a principle of active review by parliament to ensure that any whistleblowing regulator does not stray or go stale, as can easily happen, and has happened in other jurisdictions.
I ask you and other parliamentarians to safeguard these public interest principles in any endeavour to reshape UK whistleblowing law.
I hope you can help.
With best wishes,
Dr Minh Alexander
Retired consultant psychiatrist and whistleblower
Cc Dr Philippa Whitford MP
John Penrose MP Prime Minister’s Anti-Corruption Champion
Lord Hendy QC
Lord Sikka
Lord Morse
Meg Hillier Chair PAC
Whistleblowing APPG Vice Chairs and member Lisa Cameron, Rosie Cooper, Rebecca
Long Bailey
Correspondence and evidence submitted to parliament about WhistleblowersUK has included:
Ahead of the debate on the new Bill, a member of the whistleblowing APPG Kevin Hollinrake Tory MP has pushed in parliament on 25 April 2022 for financial rewards:
He was also quoted in a recent article which pressed for financial rewards:
“The problem is this touches the wider perception of whistleblowing, and whether it’s worth coming forward,” Hollinrake said…..Campaigners are pointing to this broader push, arguing that the U.K. also needs to bring more monetary incentives to the mix as it sets to overhaul its approach to economic crime…”
UPDATE
Mary Robinson briefly read her new Bill into Parliament on 26 April. It remains unpublished. But from the Hansard record of her speech, it is clear that the intention is that the proposed Office of the Whistleblower will NOT be independent. It will report to the Government. This will be far worse than useless. It will be seriously harmful and set up grievous and corrupt conflict of interest in all the cases where whistleblowers raise concerns about government failures, directly or indirectly.
“It [the Office of the Whistleblower] will set standards and report back to the Government” [my emphasis]
I wrote on 28 April 2022 to Mary Robinson to ask for a copy of the Bill has it had remained unpublished despite the drip feed of selective accounts to the press.
Wendy Addison fellow whistleblower has on the same day pointed out an email of 22 April 2022 from the CEO of WhistleblowersUK, the APPG’s secretariat, which claimed that the Bill would be uploaded as soon as Mary Robinson had given her speech in parliament on 26 April:
WhistleblowersUK have organised a webinar on the Bill on 29 April 2022, the tickets for which cost £10. Perhaps the expectation is that one must pay for information that would normally be freely available as a matter of democracy.
RELATED ITEMS
This is a matter relevant to the current row about Sajid Javid’s controversial decision to override bereaved families’ wishes and to appoint a former NHS manager to chair a review into maternity failings at Nottingham. This is a post about governance failings at her former NHS trust:
By Dr Minh Alexander retired consultant psychiatrist 24 April 2022
This is a post about an Employment Tribunal judgment against Devon Partnership NHS Trust, a mental health provider, against a worker with a mental health condition.
I had intended to write it up as it has implications for all mental health providers. It has since become especially significant following the Secretary of State’s controversial decision to override bereaved families’ wishes, with an announcement late on a Friday that an NHS management old hand would chair a review into the maternity failings at Nottingham University Hospitals NHS Trust – Julie Dent, former Chair of Devon Partnership NHS Trust.
Rhiannon here as you & I know K, the compounding of harm through badly timed, often harmful or contradictory communication is a deliberate form of abuse for complainants. As is always ensuring the 1st incident investigation is appalling. It’s then hidden behind aggressively 1/2 https://t.co/wMRYj5MGJI
“Julie Dent CBE was Chief Executive of South West London Strategic Health Authority until 1 July 2006. She left the NHS in March 2007 after 22 years to take up a new portfolio career including being Chair of the London Probation Board from April 2007 to March 2012.
She became Chair of Torbay NHS Care Trust in December 2009, and since March 2013 has been Chair of Devon Partnership NHS Trust.
Prior to this she established her own consultancy/coaching company coaching chief executives, chairs and directors in the NHS. She has worked extensively across London and the South East with clinical commissioning group leaders, and in the past year has coached senior leaders in the third sector.
She is a trustee of the School Food Trust and the Children’s Food Trust. She is Chair of User Voice, a ground-breaking charity for offenders.
Julie was awarded the CBE in 2005, after the London bombings, for services to the NHS.”
Dent retired as Chair of Devon Partnership NHS Trust in February 2020
NHS Whistleblower scandals
Dent was reportedly one of several senior NHS officials who denigrated Ian Perkin St. Georges NHS whistleblower for not being a “corporate player”.
She was also Chair of Torbay and Southern Devon Health and Care NHS Trust when it was sued by whistleblowers who raised concerns about nepotism by the notorious Paula Vasco-Knight. The ET held that the other respondent trust was the guilty party, but did Dent push hard enough against the cover up by the chair of the other NHS trust?
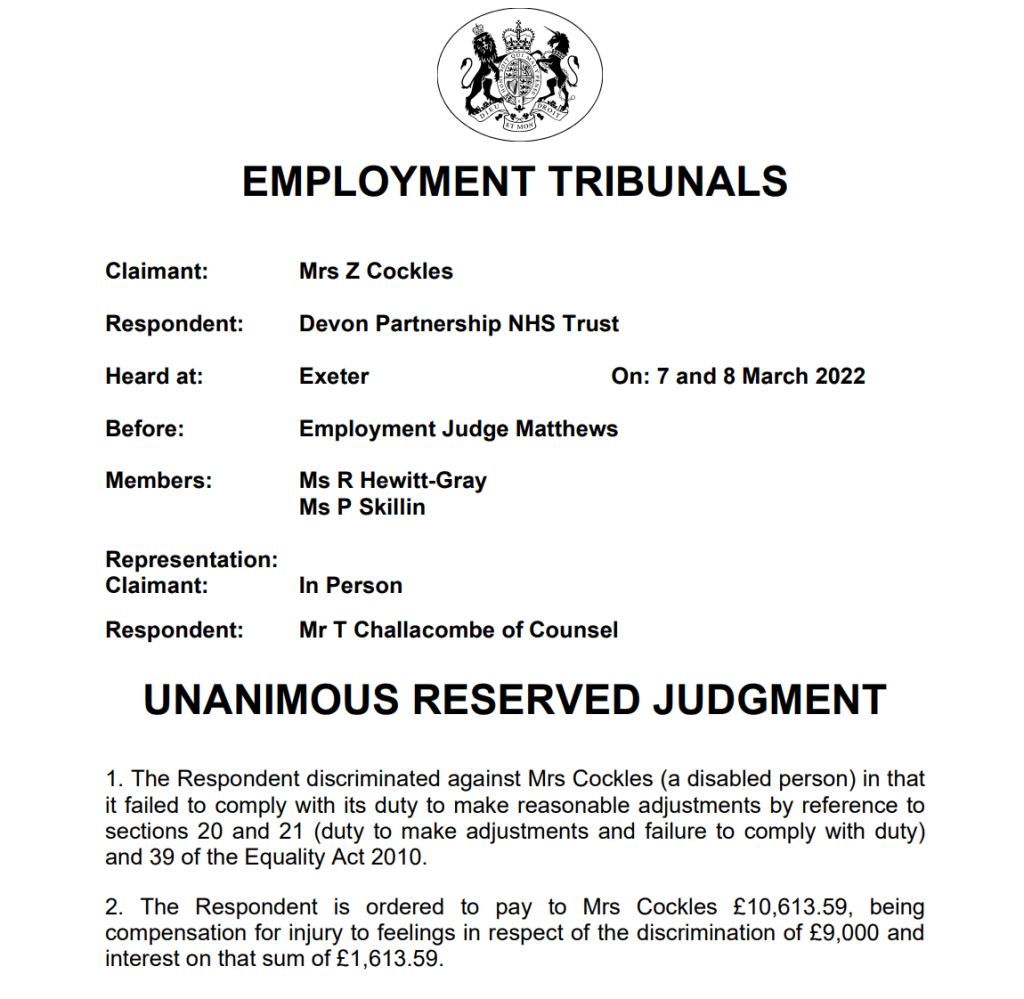
On 18 March 2022 the Employment Tribunal ruled that Devon Partnership NHS Trust was found guilty of disability discrimination against a peer support worker, Mrs Zena Cockles.
The events in question started during Julie Dent’s tenure as trust Chair. Mrs Cockles was hired by the trust in 2019 as a peer support worker, someone with lived experience of mental ill health employed specifically to use that experience to support mental health patients.
Mrs Cockles attended Occupational Health before starting work, resulting in advice to the trust that she had a disability, was symptomatic but was fit for work, and in need of structured weekly discussions:
“Mrs Cockles has underlying psychological condition. She is not completely asymptomatic and feels that this is triggered by some ongoing difficult personal circumstances. I have advised her to continue to monitor her mood and should she feel that it continues to dip to contact her GP.
I feel that she is fit for work with adjustments mentioned below.” ….
“It is advisable that regular structured support under the form of weekly discussions is considered for the first month of her starting the job and regularly thereafter.”
The post was not at all structured as Mrs Cockles was left to define what the new role would be. She started work in November 2019. Not all trust staff were aware of her arrival, and there was awkwardness fitting in because her role was not clear. Structured weekly supervision did not take place, admittedly initially with Mrs Cockles’ agreement as she had asked for more frequent ad hoc contact. However, structure was still not provided long after it was clear that she was struggling without it, and had herself indicated that she needed structure:
“I feel lost at the moment. As anyone would feel with no routine or structure I cant function properly”
There was a disconnect noted between how her line manager saw the situation – desirable flexibility in how the role could be developed – and how Mrs Cockles described her experience of it.
The line manager recounted: “the role was new to the Directorate, but that this was exciting because it means the successful candidate would work with DPT to shape the role and identify what would work best.”
Mrs Cockles in fact felt at sea and not secure or properly welcomed. For example,
“Emailed EE again about my laptop as it was so hard trying to get into Rougemont all the time as I had no ID, no name badge, no keys or fobs to get in and around the place. EE replied 13/01 saying she will chase them up.”
The difference in perception between Mrs Cockles and her line manager was so great that the Employment Tribunal commented:
“This is in stark contrast to the position Mrs Cockles portrayed in the Grievance and we are left wondering if they had been in the same meeting”
A change of her role by managers from face to face work to telephone surveying of post discharge patients met with difficulty. Mrs Cockles reported a lack of guidance and information, and she was not happy with the major change:
“No one has been in touch with me to explain that this would now be my job role and this is the first I am hearing about it I said to her it has changed so much and that I had no idea what I was supposed to be doing anymore. I told her it was starting to stress me out and I just wanted a job role….I said but I don’t have a job role. I was supposed to be seeing patients and talking to them on peer level of someone who has that understanding of what they are going through and so far I’ve not seen 1 patient in 3 months.”
When there was a change of line manager after fourteen weeks due to maternity leave, there was reportedly no evidence of handover about Mrs Cockles’ disability or the Occupational Health report and its recommendations. Mrs Cockles reported that her new line manager did not return her messages. She applied for a new peer support worker post. In the process, critical correspondence between managers was inadvertently copied to her.
The correspondence described Mrs Cockles as “unboundaried [sic] and confrontational” and questioned “that she has the self-awareness, insight and diplomacy required for this key role.”
This in itself was likely to be an act of discrimination because it displayed a lack of awareness that the behaviours criticised might be due to a relapsing or sub-optimally controlled mental illness ,(the ET noted a diagnosis of Bipolar illness, which is indeed a relapsing-remitting illness). Had this been better managed and supported, it might be no barrier to the post in question. Surprising that this did not seem to occur to a mental health organisation.
Indeed, a later consultation with a support service for trust workers during the pandemic noted a deterioration in Mrs Cockles’ mental health, and she was eventually signed off sick.
The employment arrangements continued to be sketchy, with a brief transfer to a non-peer support worker role. After a grievance process, the trust apologised for her poor experience and the lack of adequate support. Mrs Cockles accepted a new post but the ET noted that she withdrew her acceptance after she made a request that the learning about her experience to be shared and something be done about the “inappropriate” email that was copied to her. It is not clear what the trust response to her two requests was, but the ET implied it was not affirmative.
The ET noted: “Mrs Cockles reluctantly changed her position again, however, when it was explained to her that the extension of her contract was conditional on the acceptance of a post.”
If I understand this correctly, the trust left her with no real options.
Ultimately, “Mrs Cockles’ employment with the Trust ended on the expiry of the fixed term of her contract, on 24 February 2021.”
This is an uncomfortable story. Trusts should not employ vulnerable peer support workers as a matter of tokenism or virtue signalling, without thought and preparation. The idea of peer support workers of itself carries a kernel of stigma – the subtle implication being that “ordinary” staff do not have lived experience of mental ill health – when statistically, due to the frequency of mental ill health in the general population, many are bound to.
But where peer support workers are employed explicitly to use their own valuable experiences to help others, trusts have a special duty of care to ensure that the working environment is safe and supportive, and that the managers supervising such workers understand their task.
The fact that Mrs Cockles met with such an “unboundaried” [sic] organisational response to the employment of a peer support worker is ultimately a failure of board leadership to recognise and proactively manage the serious risks of any failure to support peer support workers. The trust board failed to ensure the delicate balance of empowering a user perspective without abrogating all responsibility as an employer, and in fact causing injury. Mrs Cockles should have had a very different reception and experience.
The tokenistic and undoubtedly ham-fisted organisational behaviour, which led to the Employment Tribunal awarding Mrs Cockles £10,613.59 just for injury to feelings, adds to the questions about whether the Trust’s former Chair is the best person to conduct a sensitive review and to understand and meet the needs of bereaved families at Nottingham.
This is Julie Dent pictured with the peer support worker project team, at a 2018 trust awards ceremony. The person in the top hat is Melanie Walker, trust CEO.
Julie Dent has decided not to chair the review into maternity safety at Nottingham after family opposition, citing personal reasons, as reported by NHSE/I:
RELATED INFORMATION
Coroner’s findings
Devon Partnership has been rated “Good” by the Care Quality Commission, but mental health trust ratings are unreliable when all are seriously under resourced and operating under serious, chronic bed pressure.
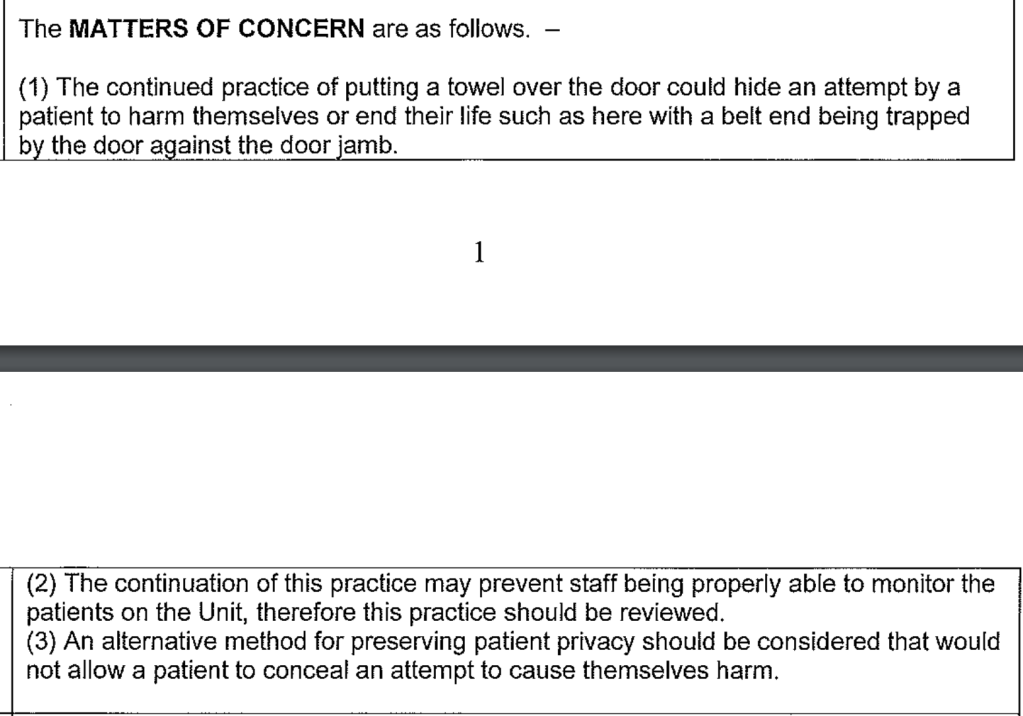
Listed below are published coroners’ Prevention of Future deaths reports – usually issued only exceptionally – that have been issued against the trust. They include a number of inpatient suicides. The case of Diane Knight revealed shocking practices of patients being allowed to cover observation windows – implying that it was commonplace not to carry out observations at night.
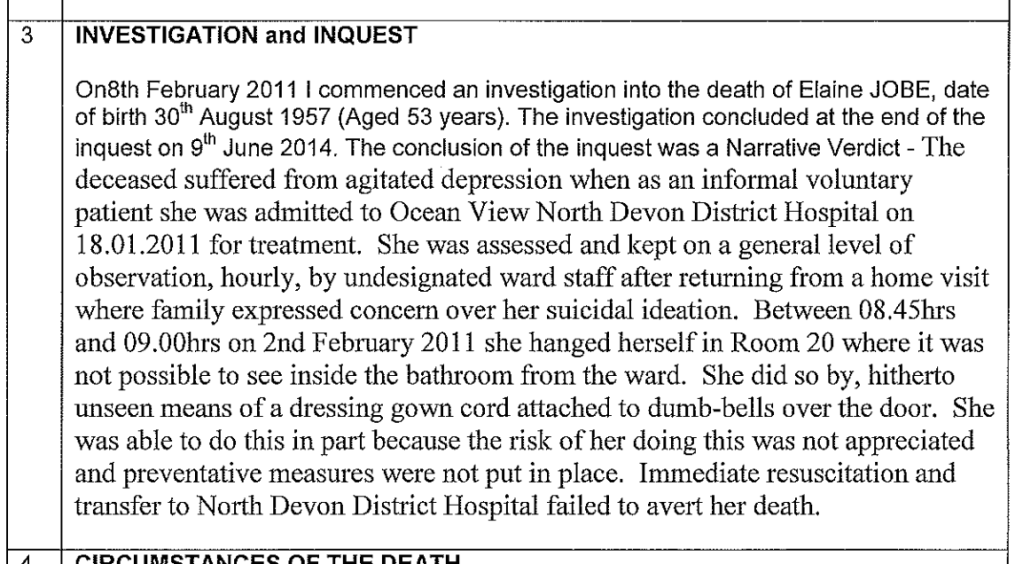
This was of particular concern because an earlier coroner’s PFD had highlighted the inpatient suicide of Elaine Jobe, in which lines of sight for observation were an issue:
There have also been a steady stream of serious incidents reported in the press.
These have included allegations by a whistleblower following an inpatient death, that trust managers repeatedly ignored concerns about unsafe staffing levels:
“An urgent probe has now been launched at The Haldon, part of Wonford House Hospital in Exeter after bosses were allegedly warned of the dangers that something like this could happen due to cuts in staffing levels.
The whistleblower said: “I am aware that staff have repeatedly raised concerns that the ward was unsafe due to insufficient staffing.
“It had been repeatedly flagged up by ward staff as a major risk factor.”
These are a sample of other media reports about serious incidents at the trust:
“Barrister Catherine Oborne, on behalf of the O’Sullivan family, cross examined both Mr Cole and Devon Partnership Trust’s Carolyn Crowe about why he had been discharged from the crisis team on December 5 and about the use of the diagnosis as a ‘malingerer’.
“The family of Alan Prettyjohn, 44, is calling to not judge people who suffer from mental health conditions and for better help to be made available to them in Devon….Alan did not even receive a mental health assessment.”
For followers of medical politics, Adrian James the President of the Royal College of Psychiatrists and former medical director of the trust is a consultant psychiatrist based at Devon Partnership NHS Trust. Prior to becoming President, he represented the Royal College as Chair of the Westminster Parliamentary Liaison Committee of the Royal College of Psychiatrists.
As Chair of the Health Select Committee she declined for years to hold a follow up hearing into the government’s failures to meet the recommendations of her own Committee on NHS whistleblowing and the related failures of the NHS Freedom To Speak Up project.
Safe Staffing in the NHS
It is clear that maternity failures are widespread across the NHS and that there are systemic issues that have not been adequately tackled. One crucial matter is safe staffing – a recommendation from the MidStaffs Public Inquiry that has been resisted by successive Tory governments over the last decade, because they do not wish to fund it. NHS staff whistleblowing about safe staffing is not well handled, as it is a matter that sits in the “too difficult” box.
A recent whistleblowing matter at Sussex, where staff were told to stop raising concerns about unsafe staffing levels, illustrates this:
“9.17 Although the existing legislation is weak, I have not recommended a wholesale review of the 1996 Act for two reasons. First, I do not think legislative change can be implemented quickly enough to make a difference to those working in the NHS today. What is needed is a change in the culture and mindset of the NHS so that concerns are welcomed and handled correctly. If this can be achieved, fewer staff will need recourse to the law.”
Instead, he proposed his go-faster option of Freedom To Speak Up Guardians, which he insisted would be effective despite inherent conflicts of interest in the model and an embarrassing lack of evidence:
If a doctor used an untested medical intervention on a wide scale without controls, they would be referred to the GMC for putting patients at risk and they would be in breach of clinical governance principles of ethical use of resources. And rightly so.
To pull his house of cards together, Francis proposed a national office. Thus, the National Guardian’s Office was established in 2016. It had no teeth. An official from the Department of Health was placed at the Office. Successive figureheads with no clear whistleblowing credentials have been appointed to head the Office.
“2) How many of these compromise agreements require staff members not to disclose the existence of the compromise agreement itself?
All of the compromise agreements contain standard wording regarding confidentiality…. …
4) How many of these compromise agreements were entered into by the Trust with staff who had previously made public interest disclosures, (whether or not these were raised by formally invoking the Trust’s whistleblowing policy)?
Two compromised [sic] agreements were entered into by the Trust with staff who had previously made public interest disclosures.”
A subject access request also later revealed that the “independent” National Guardian asked the CQC for a “briefing” about me prior to this meeting. Well, there ain’t nothin’ like a Dame!
quest
Sills resigned before she even formally took up the National Guardian post, wasting huge head hunting fees, and with embarrassing headlines for the then Health Secretary:
Dr Philippa Whitford MP: “…..what comes back from whistleblowers I meet is they are concerned that the person who has been appointed is an NHS manager. We have to have someone who is utterly outside the system.”
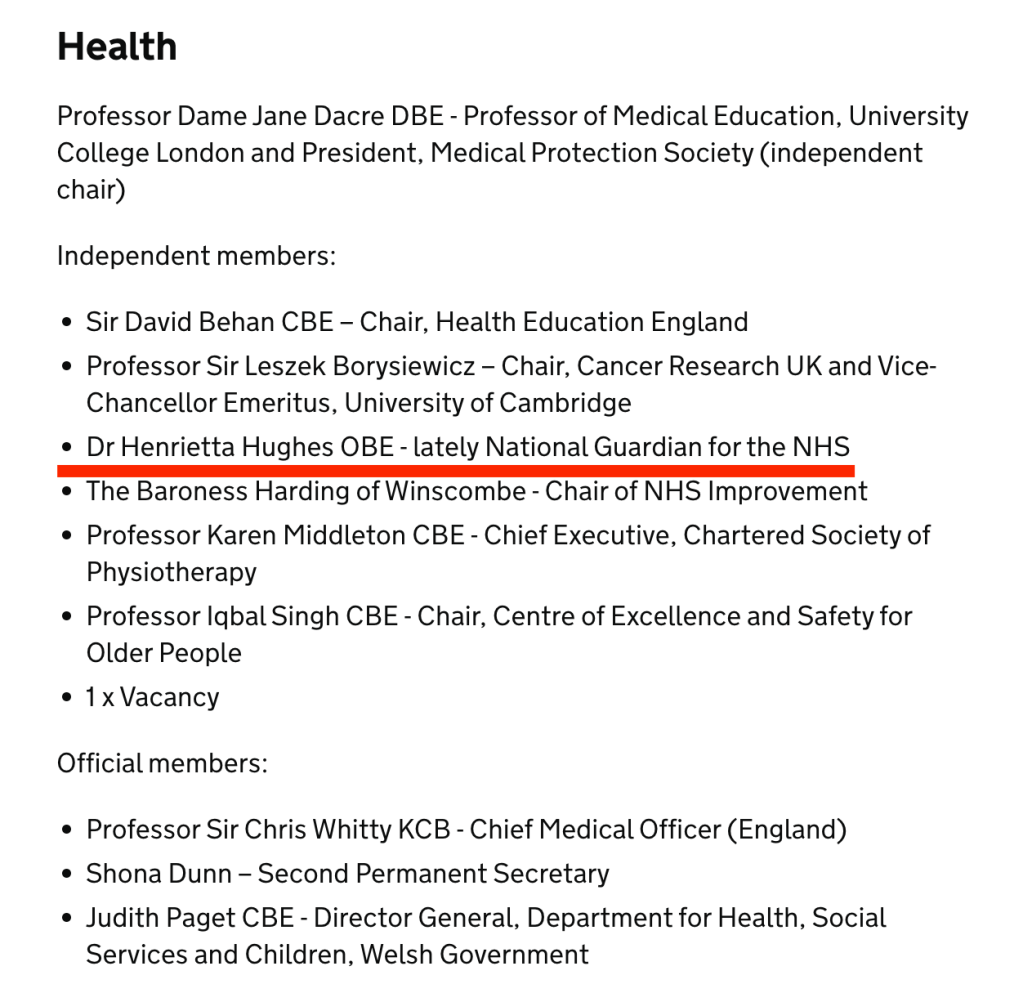
Ben Gummer, Parliamentary Under-Secretary of State for Health Services: “The hon. Lady is also wrong to say that the national guardian was an NHS manager. She is one of the leading chief nurses in the NHS, and I am sad that she felt unable to continue with that role. The hon. Lady will be pleased to know that her replacement, Dr Henrietta Hughes, is also a clinician—a practising general practitioner.”
In her previous role, Henrietta Hughes had introduced a rule which made it compulsory for staff to smile, and she wrote about it.
After appointment as National Guardian, she gave an interview to The Times in which she opined that culture in the NHS would be better if staff were more cheerful:
It was not an emotionally intelligent start to a role which is about the good governance of receiving bad news from distressed people.
Hughes also deleted her twitter account before taking up her post, obscuring her cosy past interactions as a very senior NHS manager with other very senior NHS managers. But some digital shadows remained nevertheless:
eet
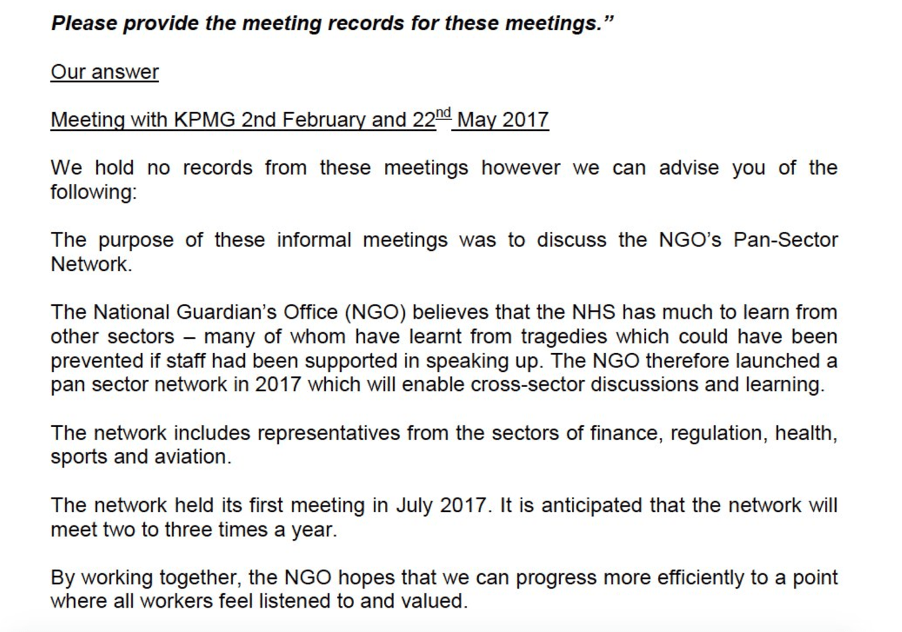
In her tenure, she paid for publicity, organised networking events which included questionable players from private industry & others and an FOI disclosure showed she did not always keep records of meetings with such players from private industry.
In 2018 she represented statistics favourably (used unpublished – against the UKSA code – by Jeremy Hunt for PR) in such a manner that the UK stats authority agreed she should be more precise:
UK Statistics Authority response 5 April 2018:
“We also note your concerns about the suggestion that some of the data are from the Freedom to Speak Up Guardian Survey Report. The presentation you referred to should have been clearer that the figures quoted on the same page as an image of the report where not in fact from this report. The report in question covers a different time period, and does not contain the information quoted.
We will write to the National Guardian’s Office to highlight areas that could be improved in their presentation and dissemination”
The latest National Guardian’s appointment was announced in November 2021. Dr Jayne Chidgey-Clark took up post on 1 December 2021. Hewn once more from the NHS management mother lode, Chidgey-Clark was previously a non executive director of Somerset CCG and also one of the CCG’s Freedom To Speak Up Guardians.
The press release about her appointment as National Guardian made sure to shake on some ‘Robert Francis secret sauce’:
“Dr Chidgey-Clark’s selection for appointment was made by a panel consisting of representatives from CQC, NHS England and NHS Improvement, as co-sponsors for the National Guardian’s Office. The panel also included Sir Robert Francis QC, whose Freedom to Speak Up Review instigated the creation of the National Guardian role.” [my emphasis]
But it is a matter of concern, not cachet, that there is a conflict of interest in Robert Francis being allowed to oversee – as a member of the NGO’s oversight board – a venture he designed and clearly continues to shape.
It contains reference to transformational and consultancy skills as follows:
“DirectorTHE JCC PARTNERSHIP LTD. · Self-employed THE JCC PARTNERSHIP LTD. · Self-employed Jul 2009 – Nov 2021 · 12 yrs 5 mos Jul 2009 – Nov 2021 · 12 yrs 5 mosServices: Transformational coaching, Interim management solutions, Health and Care Consultancy, Team development, End of Life Care Specialist
Providing consultancy solutions and interim senior management support to health and social care organisations and leading projects across health and social care. Providing exceptional executive transformational coaching and team development as well as organisational reviews.
A specialist advisor to the CQC. Able to help organisations to prepare for their CQC Inspection. [my emphasis]
Firewalk Instructor and Motivational Coach and Breath Work and Reiki practitioner.”
Of concern, it therefore appears Chidgey-Clark is one of those enterprising individuals who both offered services to the CQC as a specialist advisor for inspections and as advisor to organisations preparing to be inspected.
So how will she ensure that conflicts of interest are handled in a post that is centrally about probity?
And how many ex-CQC workers have now passed through the National Guardian’s Office?
Chidgey-Clark has written a first blog as National Guardian, which in 780 words does not say a great deal.
To find more specifics, I asked Somerset CCG for information about her previous role at the organisation.
The most startling fact which emerged from this is that Chidgey-Clark received a mere TWO whistleblowing disclosures as a Freedom To Speak Up Guardian.
This is the material disclosed by Somerset CCG via FOIA:
But do just two cases represent suitable experience for a national role?
Nevertheless, Chidgey-Clark’s experience seemed to impress Andrew Morris, who represents NHS Improvement, one of the funders of her Office:
“Sir Andrew Morris OBE Hon FRCP, Interim Chair of NHS Improvement said:“I welcome Jayne’s appointment to the National Guardian’s Office where her skills and experience will be invaluable in further developing the work of Freedom to Speak Up Guardians. On behalf of NHSE/I, we are looking forward to working in partnership with Jayne.”
In previous rounds of recruitment, knowledge and expertise of whistleblowing were not featured in the person specification for the National Guardian post, which speaks volumes.
Knowledge and expertise were probably not required this time either.
I invited comments from both the CQC about who was the appointing officer, their due diligence in the appointment process, and I also invited comments from the National Guardian’s Office, but neither have so far commented.
I had also recently renewed my enquiry to Robert Francis, post Ockenden Report revelations about gross and ongoing NHS suppression, about whether he was ready yet to withdraw the Freedom To Speak Up project and support whistleblowing law reform. I pointed out that some are calling for yet another independent review of NHS whistleblowing, which does not reflect confidence in the success of his project. I also drew his attention to the fact that the numbers of NHS staff filing whistleblowing employment tribunal claims seems to be fairly stable, disproving his suggestions in 2015 that his model would reduce the need for recourse to the law. Again, there has not yet been a reply.
Silence seems a fitting epitaph for the Freedom To Speak Up project.
Is Chidgey-Clark a master practitioner of Neuro-linguistic Programming?
I recall seeing online reference to this but did not make a note of it. Others commented online. Some posted a link to Somerset CCG’s website. The website link is no longer functioning. I asked Somerset CCG about this, who simply said they removed Chidgey-Clark’s profile entry after she moved to the National Guardian’s Office, but did not deny that it featured an NLP qualification.
NLP is a controversial coaching/ therapeutic intervention. One rating exercise carried out with mental health professionals saw NLP rated below Angel Therapy and Past Lives Therapy:
On 20 April 2022 the CQC made the following comments in response to question about Chidgey-Clark’s sum experience of two whistleblowing contacts as a CCG Freedom To Speak Up Guardian, who the CQC appointing officer was and what due diligence they took in the process:
“Hi Dr Alexander,
Please see our comment below as requested.
A CQC spokesperson said: “A multi-stage assessment process was conducted prior to the appointment of the National Guardian for Freedom to Speak Up in the NHS, to ensure the relevant knowledge, skills and experience were identified in the appointable candidate. Dr Chidgey-Clark’s appointment was made by a panel consisting of representatives from CQC, NHS England and NHS Improvement, as co-sponsors for the National Guardian’s Office. The panel also included Sir Robert Francis QC.”
Many thanks
Maryellen”
On 19 April 2022, the National Guardian’s Office made the following comment about Chidgey-Clark’s sum experience of two whistleblowing contacts as a CCG Freedom To Speak Up Guardian:
“Dear Dr Alexander,
Thank you for your email.
Dr Chidgey-Clark was recruited through the process set out by the CQC. You can find details of her announcement as National Guardian on our website here.
….Kind regards,
Ellie Staite”
PETITION
Please click and add your signature to this petition to reform UK whistleblowing law – whistleblowers protect us all but weak UK law leaves them wholly exposed and it is a threat to public safety
In his 2013 Midstaffs recommendations Robert Francis recommended that whistleblower reprisal should be criminalised. In giving evidence to parliament in 2014 he opined that CEOs who victimised whistleblowers should be sacked to set an example and discourage others. By 2015, after he was knighted and on the board of the CQC, he faintly derided contributors to the Freedom To Speak Up Review who had asked him to consider criminal sanctions.
Sir Robert changes policy on whistleblower reprisal
By Dr Minh Alexander retired consultant psychiatrist 9 April 2022
Summary: The ambiguous organisation Protect which sells whistleblowing compliance services to industry has called for yet another independent review of whistleblowing in the NHS. Such a review is fraught with risks for future whistleblowers from all sectors, and can obstruct real change. Any such review will need to be carefully negotiated. Whistleblowing touches on power and where there is power, there will be manipulation. Whistleblowers will need to be well informed and prepared, and stand their ground. The public interest is the priority. Genuine whistleblowers will need to do what they can to protect whistleblowing from more political abuse and deflection, or exploitation as a means of personal gain and profit.
Yesterday the organisation Protect which receives money from many employers including NHS organisations, for whistleblowing compliance services, issued a statement calling for yet another independent review of speaking up in the NHS.
“We are calling for an urgent review of speaking up in the NHS. NHS staff should be enabled to come forward freely and talk about their experiences in detail. In our experience, whistleblowers and would-be whistleblowers often have a clear insight into the problems, and potential solutions. Protect’s preference would be for the Health Select Committee to conduct this review, this could be done urgently, independent of Government and, if necessary, the use of Parliamentary privilege could be used to enable evidence and testimony to be gathered without legal repercussions for those involved.”
The purported trigger for Protect’s call is the report of the Ockenden Review on maternity safety failings, which is actually an obfuscatory piece of work where whistleblowing is concerned, but more on that another time.
Protect is part of the establishment whistleblowing furniture
In predecessor form, Protect was midwife to the UK’s highly flawed whistleblowing law the Public Interest Disclosure Act. Anyone can make a mistake, and law making of course always has to involve compromises, but Protect then failed to whistleblow on the law’s failures for many years. This was despite the organisation regularly hearing from whistleblowers and its seat on the Employment Tribunal national user group. Perhaps the seat was too comfortable. Protect promotes the odd high profile case, to its mutual benefit, but has been known to tell some whistleblowers not to bother and to run, even when they were shown later to have a case. Presumably Protect does so because it knows the law is weak. The law that it did not whistleblow on, that is.
Protect’s former head of legal has also been working at the National Guardian’s Office for some years now, such is the tangled web of the whistleblowing industry.
There were TWO ineffective reviews of whistleblowing in the NHS published seven years ago, which seriously failed both whistleblowers and the public.
Firstly, the well known and now much derided Freedom To Speak Up review by Robert Francis which holds no credibility amongst whistleblowers, and has failed so many patients.
The other is the less remembered but equally reprehensible review by the parliamentary Health Select Committee headed by a then Tory chair. This was released ahead of the Francis report and was little more than platitudes and pulled punches. But it provided nice headlines and a photo op:
The same committee chair was later overheard by whistleblowers sympathising with David Behan CEO of the Care Quality Commission over negative publicity due to a critical Times letter by whistleblowers. The letter was issued partly to highlight research about CQC’s whistleblowing failures – hard evidence actually submitted to the Committee, not that it seemed to cut much ice with the Chair.
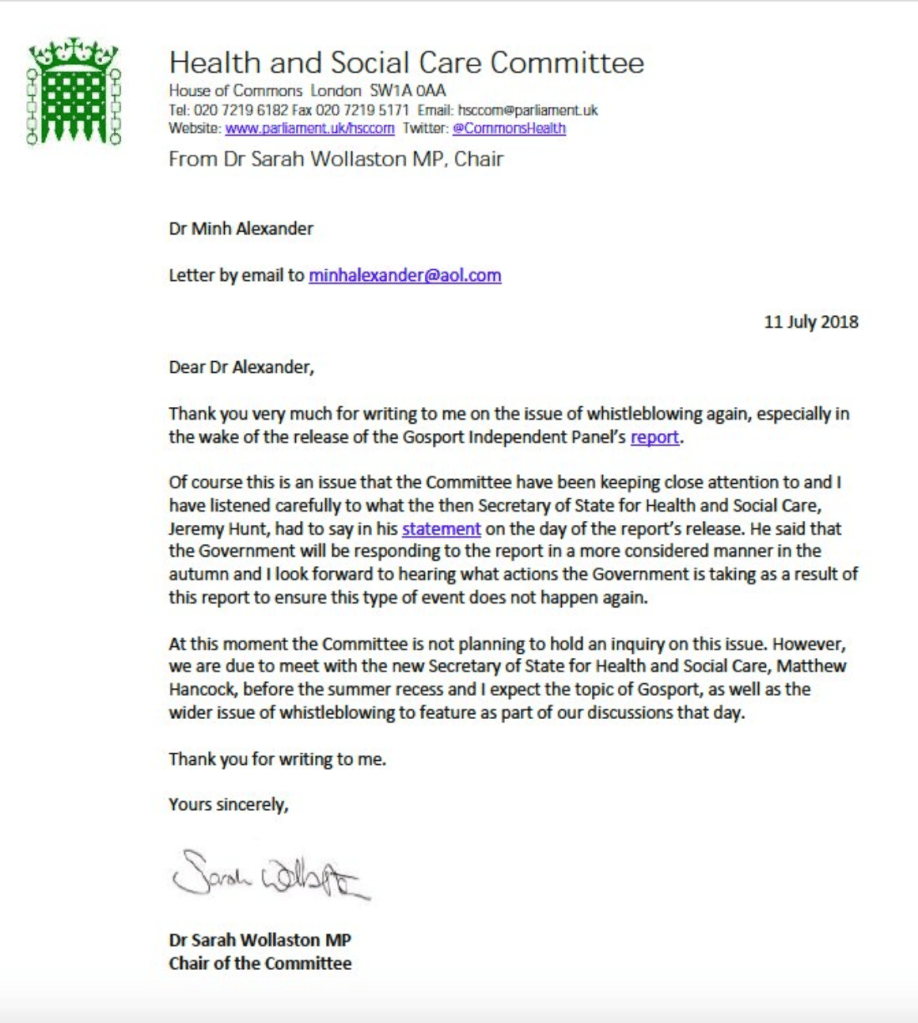
For years after the Freedom To Speak Up Review report, the same Committee Chair refused to hold any hearing into the ever more obvious failures of the Freedom To Speak Up project or the failure of the NHS to meet the sparse and loose recommendations of her 2015 review. This refusal continued after the publication of the Gosport Inquiry which showed that hundreds of killings of NHS patients could have been avoided if whistleblowers had not been intimidated and silenced early on.
Instead, friendly private meetings with the National Guardian were preferred over a public hearing with testimony from whistleblowers on an equal footing.
A Committee hearing is needed but one difficulty now is that the Health and Social Care Committee is chaired by Jeremy Hunt former Health Secretary. How will he review his own handiwork, the Freedom To Speak Up review, expressly designed to leave NHS whistleblowers entirely at the mercy of their employers? Let alone deal with the evidence from many whistleblowers who made disclosures to him but were fobbed off, as is de rigueur for the Department of Health and Social Care. Hunt should never have been allowed to take charge of the Committee due to the obvious conflict of interest as a recent past Health Secretary. Any review by him would not be truly independent.
But a parliamentary review would still be better than another flimsy effort entirely controlled by the government, in the way that the Freedom To Speak Up review was. Down to the dirty tricks on the launch day of sending whistleblowers to a different venue, miles away from the press conference held by Francis.
The great risk of any review, greatest with the latter fly by night type, is that the government will simply use it to generate another smokescreen of non-actions, to delay and to avoid real reforms. A mark II Freedom To Speak Up review will not only greatly hurt NHS whistleblowers, but whistleblowers in all sectors. It would be used by the government to avoid any discussion of UK whistleblowing law reform, which is the real solution needed.
If any review does materialise, the first wrestling match will be the terms of reference, which is where the seeds of deliberate inefficacy are usually sown.
Also, the whistleblowing scene draws a mixed crowd of secondary characters, which also poses risk to reform at times of possible change. Sometimes well meaning but temporary and ill informed actors pass through in a cloud of misdirected outrage, and ask for superficial interventions that will make little or no difference. For example, minor interventions aimed at the Employment Tribunal when whistleblowing cases should not actually be handled primarily as employment matters. And there are also carpet baggers using the whistleblowing label for publicity or seeking to profit or carve out careers, often driving debate towards financial incentivisation of whistleblowing, or models which maximise conflict and litigation and so generate income for middle men. Behind them stands a multi-billion US business trying to break through into the UK market.
Genuine whistleblowers need to tread a careful path through this morass of politics, backfires, distractions and vested interests to achieve anything of substance for those who come after. I advise that if you decide to engage, do so on clearly informed basis. Do your own research. Accept no second hand information. And do not just submit evidence into any review process and leave it with others to write the punch line.
Instead, ask the government for evidence based solutions. Ask for things that will make a measurable difference and can be auditable. Ask for specific things that the system must do. For example, I recommend that people ask for real reform of UK whistleblowing law, and set out what this means, even if briefly.
TOOL BOX AND RESOURCES FOR REQUESTING LAW CHANGE
These are some aids at varying levels of detail for those who wish to ask their MPs or submit evidence to parliament in support of whistleblowing law change
The law should: 1) Make it compulsory for whistleblower’s concerns to be investigated 2) Ensure that there is a legal duty by employers and regulators to protect whistleblowers from the point at which they whistleblow 3) Include meaningful penalties for individuals who victimise whistleblowers, including criminal sanctions for serious reprisal.
This is a detailed draft law by whistleblowers with many ideas for how an alternative model of law and whistleblowing governance could work. It borrows from the US Office of Special Counsel which is an agency for federal whistleblowers which has principles of fair restoration and proactive, lean resolution. This may include expunging unfair disciplinary findings or unfairly lost seniority. This is very different to the bloated, litigious post hoc response currently imposed by UK law on whistleblowers. Again, there are references for those who want to read more. What could a new whistleblowing law look like? A discussion document
This is a good practice example whistleblowing Bill laid on the parliamentary record by Dr Philippa Whitford MP, to serve as a resource. It introduces many of the standards that are being introduced in Europe under the EU directive, such as criminal sanctions for cover ups and reprisals. Importantly, it takes whistleblowing outside of employment law. A new UK whistleblowing Bill and a petition to the UK government to strengthen protection
Declaration of interest: It is ancient history now but I should declare that I made a disclosure to Jeremy Hunt about NHS regulators ignoring my patient safety and governance whistleblowing at that point, and pretending that all was improved. This roughly coincided with the start of a series of eating disorder deaths with common features of organisational failings that finally led to a critical inquest with national recommendations.
PETITION
Please click and add your signature to this petition to reform UK whistleblowing law – whistleblowers protect us all but weak UK law leaves them wholly exposed and it is a threat to public safety
A perfect, clear cut example of why UK whistleblowing law – PIDA – is completely unfit for purpose. The case of a gold standard whistleblowing case, Tribunal tested and fully upheld – which still resulted in a six year ordeal of persecution and harassment for whistleblower Dr Jasna Macanovic consultant renal physician and very importantly, still left patients unprotected.
By Dr Minh Alexander retired consultant psychiatrist 6 April 2022
This is a very brief post primarily for NHS Ambulance trust staff.
The National Guardian’s Office (NGO) website had a notice that it had an upcoming thematic case review on ambulance trusts but provided no details.
I submitted a Freedom of Information request to find out more.
The NGO has today responded minimally.
It is now clear that the NGO has shockingly been dragging out this piece of work since June 2020, when it seems was first discussed at its Advisory and Liaison Board. This committee consists of Robert Francis CQC NED, Andrew Morris, then NHS Improvement NED and now Chair and the National Guardian. (Incidentally, the name of this committee has been softened – it used to be the Accountability and Liaison Board – but who likes to be accountable?)
“This was first discussed with our Advisory and Liaison Board in June 2020.”
It is very hard to understand why the NGO has not given this work greater priority in view of the great difficulties faced by ambulance trust staff.
I asked the NGO for any analyses of whistleblowing in ambulance services carried out by the NGO to date. It seems none have been done save for the routine ‘Speak Up’ index material that is done for all trusts.
Moreover, the NGO has received only twelve public interest disclosures from NHS ambulance trusts in the four years from 1st April 2017 to 31st March 2021.
This is despite the well known staff relations troubles in ambulance trusts across the country and publicised staff whistleblowing to the press.
Importantly, reportedly, none of these twelve whistleblowing disclosures to the NGO came from ambulance trust Freedom To Speak Up Guardians in this period. That is, the people in ambulance trusts with responsibility for advocating for whistleblowers and escalating their concerns until they were resolved, apparently did not do so despite the severe problems and the staff deaths such as at East of England.
The NGO has for the time being ducked disclosure of all the documents that I have requested about the thematic case review by hiding behind Section 22 FOIA – documents intended for publication – even though I have asked for some documents that are not intended for publication.
As the NGO now claims it will be publishing review documentation “in the near future”, I will wait for publication and then pursue any outstanding data that the NGO fails to disclose.
The figures about ambulance staff disclosures to the NGO are not correct. There is at least one case missing from the stats. I have written to the National Guardian about record keeping by her Office.
“BY EMAIL
Dr Jayne Chidgey-Clark National Guardian
6 April 2022
Dear Dr Chidgey-Clark,
Record keeping and case files at the National Guardian’s Office
Thank you for the FOI response from your office regarding the planned thematic case review on ambulance trusts.
I believe on cross checking, including with the whistleblower in question, that your data about qualifying disclosures received by your office from ambulance trusts is incorrect, and that you are missing at least one more case from your stats.
I am rather concerned about how cases are logged and recorded. This is especially because incomplete records were an issue that arose previously in a matter of broken whistleblower confidentiality. That earlier matter was the subject of an upheld complaint against the National Guardian’s Office.
There seems to be an overlap in the NGO personnel who handled the case now missing from your stats and the earlier incompletely recorded case which led to an upheld complaint.
Is it possible to have some reassurance about the standards for record keeping and case file protocol followed by your office, including how telephone calls are logged and emails are filed? Are there written standards and expectations?
Many thanks,
Dr Minh Alexander”
UPDATE 8 APRIL 2022
I received a comment on this blog from a someone who would like to be anonymous. By agreement, this is a redacted version of what they wrote:
“Hi Minh
Very interesting article about the NGO and ambulance trusts, thank you.
[REDACTED SECTION]
You may be interested to learn that the Freedom to Speak Up Guardian at REDACTED Ambulance Service Trust has now resigned, the role has been taken over by Dr REDACTED the Medical Director. You may not be surprised to learn that Dr REDACTED will only consider Freedom to Speak Up requests if they involve patient safety – he does not think staff concerns about bullying or whistleblowing are relevant.
Surprised? No, I’m not either.
[REDACTED SECTION]
Glad that you are back campaigning again and I hope all’s well with you.
Kind regards
REDACTED (Paramedic)”
I asked the trust in question about this. After a lengthy pause, it denied these allegations and stated that it had two replacement Freedom To Speak Up Guardians in place. It denied that the types of concern that staff were allowed to raise had been restricted.
PETITION
Please click and add your signature to this petition to reform UK whistleblowing law – whistleblowers protect us all but weak UK law leaves them wholly exposed and it is a threat to public safety
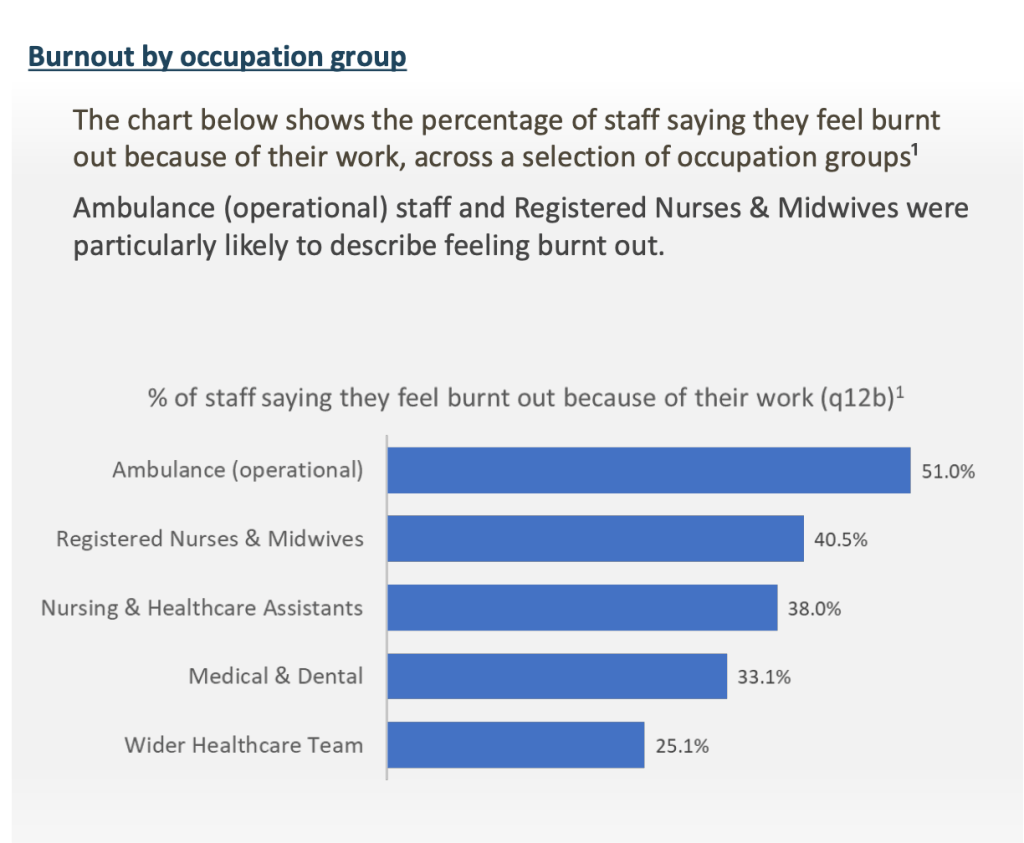
The latest NHS staff survey shows as usual that NHS ambulance trusts have the highest levels of bullying, and that ambulance staff report the greatest burnout:
This post shares an FOI response from WMAS about eight staff suicides since 2018 and further correspondence with the National Guardian:
A perfect, clear cut example of why UK whistleblowing law – PIDA – is completely unfit for purpose. The case of a gold standard whistleblowing case, Tribunal tested and fully upheld – which still resulted in a six year ordeal of persecution and harassment for whistleblower Dr Jasna Macanovic consultant renal physician and very importantly, still left patients unprotected.
By Dr Minh Alexander retired consultant psychiatrist 30 March 2022
Summary: This post looks at the National Guardian’s role in continuing poor culture at Sussex. After the former National Guardian Henrietta Hughes’ shameful treatment of whistleblowers at Brighton and Sussex University Hospitals NHS Trust, and her protection of powerful trust directors, time inevitably caught up with these improprieties. Further staff whistleblowing and patient complaints about maternity safety forced an unannounced CQC inspection late last year which revealed very serious ongoing failures of whistleblowing governance in maternity and surgical services. Staff reported that their concerns were not always acted upon. This even included serious concerns about critical care capacity. At one trust unit, inspectors found that managers had not reviewed or investigated 128 incidents. Astonishingly, staff were told to stop raising concerns about staff shortages on the basis that this was a known issue. This saga further illustrates the failure of the Freedom To Speak Up project. The National Guardian’s Office was established primarily to carry out reviews of NHS trusts but it has only completed 9 reviews since 2016 – less than two a year. Of the trusts that it has reviewed, most continue to show signs of problems with whistleblowing governance. It is time to stop wasting precious public money on sham whistleblowing agencies, and to replace them with strong, genuinely protective law and infrastructure.
Today, the long awaited Ockenden review into large scale maternity safety failings at Shrewsbury and Telford Hospitals NHS trust is due to be published. Inevitably, it has already been revealed that there was whistleblowing about the safety issues that was not acted upon by managers.
In the background is another avoidable maternity safety failing, in which the National Guardian’s Office played a part.
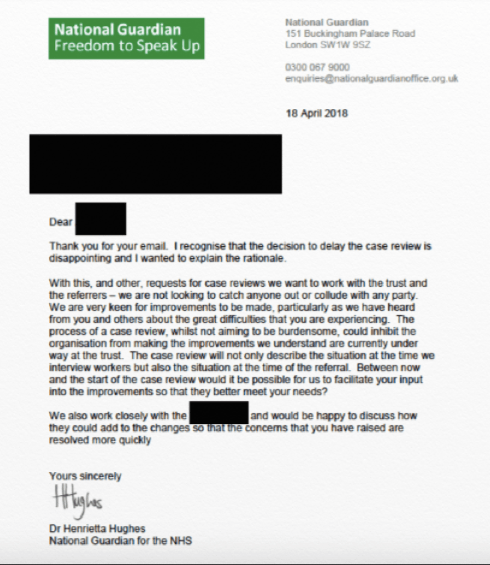
In 2017 the former National Guardian Henrietta Hughes badly failed patients and whistleblowers at Brighton and Sussex University Hospitals NHS Trust by stalling and protecting a powerful in group of NHS trust directors about whom whistleblowers raised concerns.
She deviated from her own procedures to give the trust time to cover its tracks:
Much later, in 2019, Henrietta Hughe carried out a review which came to glowing conclusions about the all the “improvements” being made in culture and whistleblowing governance.
Marianne Griffiths the trust CEO naturally crowed about this PR victory:
Praise for BSUH culture change “Trust Chief Executive Dame Marianne Griffiths said: “Since our arrival at BSUH, we have made it our absolute priority to work with colleagues and support them to help make further improvements to the culture of the organisation, particularly in relation to equality and diversity. It is extremely encouraging, therefore, to see our improvements recognised through such a comprehensive review.”
In September 2021 as a result of more staff whistleblowing and patient complaints, the Care Quality Commission carried out an unannounced inspection of maternity services at the trust , now renamed University Hospitals Sussex NHS Foundation Trust after a full merger of its two predecessor organisations.
The CQC press release emphasised poor culture and the difficulty that staff experienced with raising concerns:
“Other concerns raised with inspectors by staff, or observed by inspectors, included a poor culture – bullying and harassment was reported by some staff – and a perception that leaders were doing little to address concerns. After listening to staff about their experiences working in main theatres and recovery, inspectors had serious concerns about the culture amongst colleagues.”
Extraordinarily, trust staff had been told to stop raising concerns about safe staffing issues because it was a “known risk”:
“They told us they been instructed to stop reporting low staffing as an incident as it was a known risk”
Surgical as well as maternity services were found to have shortcomings.
This included very serious incidents about lack of critical care capacity, for example:
“We reviewed an incident form completed in April 2021, in relation to patients requiring high dependency care, being cared for in recovery. On the day the recovery unit was full and included four patients who required high dependency care one of these patients deteriorated and required intensive care. Concerns within the incident related to not being able to keep up with all the care patients needed and although some support was provided by an advanced care practitioner and anaesthetist staff did not always feel supported. The incident was not investigated by managers until 12 October 2021 we were not assured that the actions recorded, or the time taken to investigate the incident reduced the risk of further similar incidents. The only recorded action was that staffing concerns were being managed through the directorate and divisional recruitment programme. The trust also provided a narrative for this incident and stated that the care and supervision of a significantly complex post-operative recovery period was appropriate.”
Despite these very serious failings, the Dame kept her overall CQC rating of ‘Outstanding’.
So, is the National Guardian’s Office working any harder to conduct reviews? This is after all the core function for which it was established.
Sadly, the answer is ‘no’.
Since inception in 2016 the work-shy, publicity-hungry agency has only completed 9 reviews – less than two a year.
CASE REVIEWS COMPLETED SO FAR BY THE NATIONAL GUARDIAN:S OFFICE
Southport and Ormskirk NHS Trust 2017
Northern Lincolnshire and Goole NHS Foundation Trust 2017
Derbyshire Community Health Services NHS Trust 2018
Nottinghamshire Healthcare NHS Foundation Trust 2018
Brighton and Sussex University Hospitals NHS Trust 2018
Royal Cornwall Hospitals NHS Trust 2018
North West Ambulance Service NHS Trust 2019
Whittington Health NHS Trust 2020
Blackpool Teaching Hospitals NHS Foundation Trust 2021
Issues of poor whistleblowing governance have continued at most of these trusts that were reviewed by the National Guardian. For example, there has been a high rate of whistleblowing employment claims against Nottinghamshire Healthcare NHS Foundation Trust, and I am aware that whistleblowers have continued to approach the National Guardian’s office but have been very unhappy with its response. There have been similar issues with North West Ambulance Service NHS Trust. Only very recently, there has been fresh whistleblowing to the press by staff of Northern Lincolnshire and Goole NHS Foundation Trust and Blackpool Teaching Hospitals NHS Foundation Trust:
Moreover, since being reviewed by the National Guardian in 2017, Southport and Ormskirk NHS Trust has repeatedly been in the news for bullying. The trust recently lost an Employment Tribunal for causing injury after managers failed to respond to repeatedly raised concerns about bullying:
So what is the point of the National Guardian’s Office?
Does the NHS need an idle, ineffective if not harmful, sham whistleblowing agency?
Here is Marianne Griffiths the trust CEO congratulating Henrietta Hughes former National Guardian after it was announced in the New Years Honours List that Hughes was listed for an OBE:
PETITION
Please click and add your signature to this petition to reform UK whistleblowing law – whistleblowers protect us all but weak UK law leaves them wholly exposed and it is a threat to public safety
A perfect, clear cut example of why UK whistleblowing law – PIDA – is completely unfit for purpose. The case of a gold standard whistleblowing case, Tribunal tested and fully upheld – which still resulted in a six year ordeal of persecution and harassment for whistleblower Dr Jasna Macanovic consultant renal physician and very importantly, still left patients unprotected.
By Dr Minh Alexander retired consultant psychiatrist 23 March 2022
Summary: Dr Jasna Macanovic, an “extremely gifted” renal physician who provided the NHS with twenty years “excellent” service was unfairly dismissed by Portsmouth University Hospitals NHS Trust, an organisation with a troubled leadership history. The audit trail was sufficiently clear for the Employment Tribunal to firmly conclude that her dismissal was a direct consequence of her whistleblowing, which included protected disclosures to the General Medical Council about colleagues. The ET determined that her dismissal was a forgone conclusion, involving both the former Chief Nurse and current Medical Director. These two directors encouraged her to resign with a good reference during the disciplinary process that the trust mounted against her. When Dr Macanovic did not resign, she was sacked by the Chief Nurse for purported “serious misconduct” which explicitly included making referrals on colleagues to the General Medical Council, even though the regulator had already effectively said the referrals were appropriate and part of Dr Macanovic’s duty as a doctor. The ET also concluded that the trust attempted to “resist” and “deflect” Dr Macanovic’s patient safety concerns. A “substantial” number of consultant colleagues shared her concerns. Her identity as a whistleblower to the GMC was exposed in an extraordinary manner by her line manager, one of the individuals about whom she raised concerns. He read out the details of her GMC referral about him at a meeting with their colleagues. There were other notable incidents. After one meeting with the Medical Director, Dr Macanovic reportedly suffered a panic attack and required an ECG. The trust tried to retrospectively argue to the ET that it objected not to her whistleblowing but the manner in which it was done. This line is often used by some employers to rid themselves of whistleblowers under an argument of breakdown of relationships after no disciplinary charge sticks. The ET saw through this, which makes a refreshing change from fudged, equivocal judgments which end up pinning an unjustified share of the blame on already traumatised whistleblowers. Although Dr Macanovic was vindicated by the ET, it is a failure of our current whistleblowing law and infrastructure that she had to suffer this protracted ordeal, and she was not better protected from the outset. This case is also yet another failure of the Freedom To Speak Up model. The trust Freedom To Speak Up Guardian attended a meeting with Dr Macanovic, the trust CEO and Chair, but this did not stop serious reprisal and dismissal. There is no mention in the ET judgment of any escalation to the National Guardian. That is an aspect which remains to be clarified.
Introduction
The Employment Tribunal has found strongly in favour of Dr Jasna Macanovic a consultant renal physician unfairly dismissed by Portsmouth Hospitals University NHS Trust for whistleblowing, including to the General Medical Council. The judgment states:
“The unanimous decision of the Tribunal is as follows:
The claimant was unfairly dismissed for making a protected disclosure.
The claimant was subject to detriments for making a protected disclosure.
Arrangements for a remedy hearing shall be notified to the parties shortly.”
Dr Macanovic raised concerns about two unreported “red” surgical adverse events and the fact that some consultants at her trust were practising a technique known as “buttonholing” in a way that she believed was unsafe. She believed they were failing to properly report all complications and safety incidents. Several of her consultant colleagues shared her concerns about the buttonholing issue.
Buttonholing is a procedure to give access to a patient’s veins for kidney dialysis. The ET explained buttonholing thus:
“There is also an alternative process known as buttonholing (“BH”). As the Claimant explains, buttonholing is where patients cannulate (insert needles) using blunt needles. The blunt needles are placed in exactly the same holes in the fistula every time that the patient has to have dialysis. A track or tunnel is created through the skin to the fistula. Over time this may be less painful than using sharp needles because a patient is not making new holes on regular occasions. The buttonholing technique can be less painful and more convenient for patients.
It is agreed that buttonholing is a valid technique for patients with an AV Fistula, where the connection between vein and artery is constructed of tissue and can heal. The dispute is over those with an AV Graft, since the PTFE material can tear or degrade. That can cause leaks and an increased risk of infection. Patients need to be made aware of these risks to give informed consent. The probuttonholing school of thought is that using one blunt needle is better than repeated sharp needle entries, since over time these can damage the tissue and make it more difficult to find an entry site. Also, some patients prefer it to having a fresh jab each time.”
Dr Macanovic’s concern arose in part because she believed that Dr Sangala one of her colleagues had made unreliable claims that another unit had been using the novel technique, when it turned out from her own enquiries that this was not the case.
“…she had heard back from Reading and they were not doing it for AG grafts. Worse still, she said, patients had been told that the outcomes were excellent, whereas of the 14 patients using it, two had died, two had developed serious complications, and she had not had time to review the other ten.”
Her department became very polarised and the trust failed to deal appropriately with her concerns.
An example of chaotic polarisation was given by the ET as regards Dr Knighton the new Medical Director’s response to the situation in the summer of 2017:
“82….Four of the consultants met Dr Knighton urgently that day (26 June) to raise their concerns about buttonholing. Having heard them, Dr Knighton decided that the practice should cease immediately. The next day a consultants meeting was arranged at short notice, which he also attended. Some agreed with the decision to stop it, but Dr Borman and Dr Lewis put the counter case that several patients had chosen buttonholing. Mr Gibbs and Dr Sangala also emphasised that this was patient driven, and in the end Dr Knighton accepted the view that it could do more harm to reverse it immediately. So, he reversed the decision.”
On another occasion, a mediation meeting descended into chaos with all in tears. The ET determined that the “mediation” improperly focussed on pressuring Dr Macanovic to withdraw the GMC referral:
“We can only conclude that they all lost sight of the important principle that this was a protected disclosure and as such it was wrong to pressure her into withdrawing it”
Turning the focus onto the whistleblower
As often happens in whistleblowing cases, Dr Macanovic was turned into the focus of the matter. This was despite a long record as an “extremely gifted” physician, who was able to submit many statements from colleagues in all disciplines about her professionalism and patient-centredness. This in itself is remarkable, as in many whistleblowing cases, supporters are often intimidated into silence. Organisations also isolate whistleblowers, by a process of exclusion, attrition and smearing, to weaken any support they may have.
The story is a lengthy and complicated, and the whole ET judgment needs to be read for a complete picture. However, a few notable incidents follow.
One doctor about whom Dr Macanovic raised concerns behaved towards her in a way which the ET concluded was “abuse”:
“…Two days later Dr Macanovic was on the receiving end of an outburst from him. She was in her office at about 08.00 am when he arrived at the door and started shouting at her. He said that he was going home because he was too stressed, and that she was to blame. This was accompanied by a good deal of swearing, repeatedly telling her to ‘f’ off. She was left shaking and at the point of tears, and was still shaking 30 minutes later when her colleague, Dr Synodinou, came in.”
And yet Dr Macanovic’s line manager and Head of Unit, Dr Robert Lewis, wrote to her about this incident as follows:
“Over the next two weeks Dr Lewis investigated the shouting incident. He concluded (p.461A) that:
Your accusation about Mr Graetz is troubling on two counts. Firstly, you were clearly a source of great stress to him at the time and yet you categorically and vehemently state that you were not.
You have not sought to find out why Mr Graetz felt as he did and have not considered the possibility that you might be at fault. Instead you state that the fault is entirely Mr Graetz’s because he does not cope well with stress (rather unfair since you took a much longer period of stress-related leave over the same issue than he did). Secondly, and more importantly, you are clearly unable to distinguish between abuse and someone challenging you with an opinion which you find uncomfortable.”
The ET took issue with Dr Lewis’ framing of this incident and noted:
“He [Mr Graezt] accepted to us that his behaviour had been inexcusable and he apologised to her a few days later.”
The ET was not satisfied that the incident was properly investigated, and counted this as a whistleblowing detriment.
Dr Lewis was eventually one of the doctors whom Dr Macanovic referred to the GMC regarding her concerns.
The ET noted that he took the unusual step of reading out loud her referral about him to the GMC at a consultants’ meeting:
“70. The GMC referral was eventually made known to Dr Lewis. In a surprising decision, he elected to read it out in its entirety to the consultants at a meeting on 7 June (Detriment 5). Dr Macanovic was there to hear it. The exercise must have taken some time since the referral letter covers eight pages. In his evidence to us Dr Lewis said that any summary would have risked further objection from Dr Macanovic, but we see no reason why he could not just have said that she had referred him, or others, to the GMC over the buttonholing issue. In choosing to give such publicity to her complaints, he was in our view, stoking anger against her and seeking to isolate her from her colleagues. She was left shaken by this episode.”
Dr Lewis later confirmed at an interview that he had not discussed his intention to read out the referral with Dr Macanovic before he did so:
“He accepted that he had not discussed this with Dr Macanovic beforehand and maintained that that was the right approach – the others needed to know about these attempts to destroy people’s careers.”
Dr Lewis must have been highly stressed by the GMC referral but his action at the meeting seems a most extraordinary departure from what might be expected of him as Dr Macanovic’s line manager.
The referral to the GMC was an act of whistleblowing and was determined to be a protected disclosure by the ET.
23 Leading by example, you should promote and encourage a culture that allows all staff to contribute and give constructive feedback on individual and team performance. You should make sure that systems are in place to achieve this.”
Publicly exposing and inciting hostility against a whistleblower is not consistent with this.
The ET noted that after Dr Lewis’ public exposure at the above meeting of Dr Macanovic’ whistleblowing to the GMC, he followed up with emails to colleagues:
“71. Dr Lewis followed this announcement with emails to colleagues who were not there. He received many messages of support, including the one quoted at the outset (paragraph 11) from Dr Armstrong, stating that she was “shocked, enraged and very saddened.” Asked about this at the hearing Dr Lewis said words to the effect that Dr Macanovic had taught him well, this was how she operated, he needed a record of things and that by then “the gloves were off”
The ET noted other similar correspondence:
“When the unit head, Dr Robert Lewis, told the other consultants that he would have to attend a Fitness to Practice hearing, one of them emailed to say:
I am completely shocked, enraged and deeply saddened to read this email. I cannot believe that one of our colleagues would sink so low but it only goes to prove what a dysfunctional and destructive individual [Dr Macanovic] is with no thought whatsoever to the impact that her actions are having, not only on individuals but also on the whole department. …
I am sure the GMC will see this for what it is – a vindictive and purposeful attack on an individual colleague for no reason other than her own self satisfaction.”
As far as I can see from the trust website, it seems that Dr Lewis remains at the trust but no longer in a managerial capacity.
Circular assurance assisted by the CQC’s superficial regulatory method
A bizarre but familiar scenario of circular NHS assurance arose.
According to the ET, someone from the trust raised concerns with the Care Quality Commission about the novel buttonholing practice, sometime around October 2016. The trust clearly suspected Dr Macanovic because it later asked her, at a disciplinary meeting in 2018 if she was responsible:
“Dr Macanovic was asked during the subsequent disciplinary investigation if it was her and she would neither confirm nor deny it.”
This itself was another trust impropriety in terms of trying to hunt down a whistleblower.
The ET clarified in retrospect that it was indeed Dr Macanovic who had whistleblown to the CQC.
The trust response to the CQC was prepared by Mr Gibbs Clinical Director and Dr Lewis the Head of Unit.
Mr Gibbs was one of the surgeons about whom Dr Macanovic had raised concerns as regards unreported “red” adverse incidents.
According to the ET,
“Presented with this response the CQC did not carry out any further enquiry, and wrote back on 22 December 2016 (p.368) to say that they were satisfied that there were no safety concerns and that appropriate governance had been followed.”
Dr Lewis then communicated with consultant colleagues as follows:
“Dr Lewis reported this to the consultants by email on 16 January 2017 (p.375) – addressing it to “Dear Jasna and Colleagues”. But he did not attach the letter from the CQC, on the basis that this would then be “dissected or disputed”. In fact, any request to see it would, he said, be to question his probity and that of Mr Gibbs.”
An internal trust investigation report, the “Hunter report”, later relied on the CQC’s decision to take the matter no further, which of course rested on assurance given by parties under investigation.
“The Hunter report followed, after several months in the pipeline. On the buttonholing issue Mr Hunter found (p.239):
“33. Given my limited expertise within this area and given that the response provided by the Trust addressing the anonymous has been accepted by the CQC, there is a careful monitoring process in place and all significant events which were known when the investigation commenced have been investigated and this evidence provided to the CQC, I do not think any further interpretation by myself would help in this.
34. Hence, the Hunter report rested on the CQC conclusions, which rested in turn on Mr Gibbs’ letter.”
The ET judgment gives no information about who Mr Simon Hunter the report author was, but there was a consultant of Emergency Medicine of the same name at the trust, who was mentioned in 2016 trust board papers as “Chief of Service, Emergency Medicine”
The ET was critical of Dr Lewis’ decision to allow Mr Gibbs to respond to the CQC for the following reasons:
“148. One particular point raised on behalf of the Trust was that they took the buttonholing issue seriously, indicating that it was a separate matter. In fact, our view is that the consultant body in the renal unit were led by Mr Gibbs as Clinical Director, and he was a strong proponent. Dr Lewis gave Mr Gibbs his backing on this issue, and so Mr Gibbs was the one in a position to respond to the CQC. That is not so much treating her concerns seriously as attempting to resist or deflect them.”
NCAS greasing the wheels of exclusion and disciplinary action
Dr Macanovic was considered “unmanageable” by the trust as she would not be cowed and would not retract her concerns. This is often how incompetent organisations view whistleblowers.
Matters was escalated to the then Medical Director, Simon Holmes.
The ET referred to the trust “arming” itself with ritual advice from the National Clinical Assessment Service, an expensive rubber stamping service which allows NHS employers to behave abusively whilst claiming that they have sought independent advice. The truth is that trust managers can obtain whatever advice they want by tailoring the information they feed to NCAS, and they can also control the subsequent flow of information back through their organisations.
The salient passages about NCAS’ advice are given as follows by the ET.
NCAS advice 4 May 2017:
“The Trust is mindful that Dr 19339 is a whistle blower, but concerns have been expressed by her colleagues about her behaviour and you have received 3 letters of complaint alleging that she exhibits aggressive, bullying and intimidating behaviour.
…. The issue is, as you are aware, complicated by Dr 19339 whistle blowing status and it will be important to document carefully the preliminary information which has been received so that this is available for future scrutiny if required. Potentially it may be necessary for the Trust to be able to demonstrate that Dr 19339 is not being victimised for having raised concerns. I advised that to avoid any allegations of bias, it may also be useful for the role of Case Manager, to be delegated so that the person making any decision about how to proceed is free of any real or perceived conflict of interest. Likewise the Case Investigator should be suitably senior, experienced and independent.”
Further NCAS advice June 2017:
“You told me that, prior to the referrals to the GMC, the department, including Dr 19339, had requested the help of an external mediator. Everyone was keen to do this and so the Trust organised an external mediation which took place yesterday. You said you attended the start and conclusion. You described how at the end of the day everyone attending seemed stressed, anxious and some were physically shaking. One member of staff had to leave the room because he was so distressed.
There appeared to be an absolute breakdown in trust between Dr 19339 and the rest of the department and the result of this led you to be concerned for the health of all in the department. You considered that the breakdown in relationships in a team who need to have confidence in each other to ensure patient safely constitutes a risk to that safety.
However, the Trust will wish to assure itself that any action it takes to mitigate potential safety risks within the department is not construed as being a detriment to Dr 19339 as a result of her declaration to the CQC that she is a whistle blower.
…
Any prolonged exclusion from clinical work can lead to de-skilling and I suggested that the Trust might wish to look for a placement in another Trust or department while the investigation is ongoing and the GMC comes to a decision as to whether it will take any action against the colleagues of Dr 19339.”
The ET noted that the trust used NCAS’ advice to progress Dr Macanovic’s exclusion, even though it failed to follow several aspects of NCAS’ advice.
The ET also noted that at a meeting dealing with Dr Macanovic’s exclusion, a new Medical Director Dr Knighton refused to accept her concerns that she was being bullied by Dr Lewis. After this meeting with Dr Knighton, she reportedly suffered a panic attack and required an ECG:
“Dr Macanovic said that she was the victim of bullying by Dr Lewis, but he did not accept that that was the case. Dr Gast proposed that she could simply be excluded from consultants meetings and after a pause to consider, Dr Knighton agreed that that would be a better option. After that meeting Dr Macanovic was unwell and could not resume work. She had a panic attack and spent the afternoon in the outpatients department where she had an ECG. However, she was not signed off sick.”
Freedom To Speak Up mechanism made no difference
Dr Macanovic had a meeting with Mark Cubbon the Chief Executive and Mark Nellthorp the then trust Chair, attended by Jocelyn Booth the trust Freedom To Speak Up Guardian and elected trust Governor.
Dr Macanovic raised concerns at the meeting with the Chief Executive and then Chair that disciplinary action against her was in fact reprisal and bullying.
According to the ET, Mark Cubbon agreed there should be a separate investigation into Dr Macanovic’s concerns. However, he later reportedly changed his mind after talking to the trust director of workforce, Tim Powell. No one told Dr Macanovic, and Mark Cubbon reportedly did not respond to her subsequent correspondence. Such stonewalling is a common experience for whistleblowers.
Several consultants also later wrote to Mark Cubbon the chief executive on Dr Macanovic’s behalf, as disciplinary action against her proceeded, appealing to him to prevent her dismissal:
“113. In that period, on 2 March, Dr Bostock, Dr Uniacke, Dr Synodinou, and Dr Gast emailed Mr Cubbon, to ask him to step in to prevent her dismissal (p.1716). Dr Gast was the author. She said that these complaints were from a minority of staff, and were an attempt to silence and discredit Dr Macanovic as a whistleblower. He declined to intervene.”
The ET said it understood this:
“Similarly we can understand why Mark Cubbon failed or declined to intervene in the disciplinary policy at the 11th hour, as requested”.
It is a pity the ET did not elaborate.
Particularly as it concluded that the disciplinary charges against Dr Macanovic were patently flawed and that the dismissal process was blatantly predetermined.
Mark Cubbon is pictured below in 2019 with the previous National Freedom To Speak Guardian on the theme of the “authentic employee voice”. This was whilst Dr Macanovic’s Employment Tribunal claim was proceeding:
k
The General Medical Council
According to the excerpts quoted by the ET judgment, the GMC found in January 2018 that the buttonholing had not been introduced in a structured way at the trust. Oddly, the GMC concluded that because buttonholing had not been introduced under rigorous research conditions, there was no need to be concerned by the absence of the usual governance constraints, such as ethical review:
“With hindsight, it could be argued that it would have been a good idea to introduce the button holing/graft access method as a research project with a formal protocol and ethical review under the research governance framework. However, because of the gradual way in which it was introduced it was not introduced in this way. As it was not conceived as a research project, the fact that it did not follow the research governance framework does not raise any serious concerns.
The button holing/graft access method was an innovative technique, and should therefore have been introduced with appropriate controls, records and safety assurance, according to the relevant local policies.”
The excerpts indicated that the GMC identified no failing by Dr Lewis in regards to the governance of the buttonholing procedure:
“The method was introduced two years before Dr Lewis became chief of service and therefore he was not responsible its introduction. Indeed, all the governance measures that were eventually introduced were introduced as a direct or indirect result of his intervention, starting at the consultant meeting on 7 September 2016.”
Importantly, the GMC effectively concluded that Dr Macanovic fulfilled her professional obligations by referring her colleagues to the GMC:
“We are of course mindful of the findings of the independent whistleblowers review the GMC commissioned from Sir Anthony Hooper. Having considered the correspondence disclosed to the GMC by the trust and by Dr Macanovic, it appears Dr Macanovic first raised her concerns locally and that it was only after she concluded, in her view, that her concerns were not being adequately addressed locally that she made her complaint to the GMC. In doing so Dr Macanovic was no doubt aware, amongst other things, of the guidance at paragraph 25 of Good medical practice that doctors must take prompt action if you think that patient safety, dignity or comfort is or may be seriously compromised.”
In the event Dr Macanovic genuinely considered there was a risk to patient safety, and it appears to us that she did consider such a risk existed, but she had not raised her concerns through whatever mechanism was available to her locally and/or if she deemed it necessary to the GMC, she would in our view have been rightly criticised by the public and by the GMC for failing to do so.”
The ET explicitly interpreted the GMC’s remarks thus:
“In our view she did genuinely consider that there was a risk to patient safety. That is implicit in the previous finding that this referral amounted to a protected disclosure. Although it was suggested to us that this fell short of an express statement from the GMC that she was right to make this referral, that seems to us its practical effect.”
Theresa Murphy Chief Nurse explicitly sacks a whistleblower for whistleblowing
Soon after the GMC decision, the trust machinery whirred into action to dismiss Dr Macanovic. The ET concluded that this was a “predetermined” process. This was partly because, extraordinarily, Dr Macanovic was given the option by both the medical director Knighton and Theresa Murphy to resign with a good reference during the dismissal process:
“Having heard this evidence, and towards the end of the hearing, Dr Knighton referred again to his suggestion of resigning with a good reference.”
“The hearing resumed on 5 March 2018 when Professor Murphy gave her decision. At the outset, she also reminded Dr Macanovic that she could instead choose to resign with a good reference.”
A CQC specialist advisor at the trust
Dr John Knighton took up his post as medical director at Portsmouth Hospitals University NHS Trust in July 2017 and remains in this role. Prior to that he had been associate medical director. According to a local press report of 28 July 2017, at the time of his appointment as medical director, he had already been working as a CQC specialist advisor:
“During our inspection, CQC staff had to intervene to keep patients safe on several occasions, including asking staff to assess patients in the ambulance and the corridor, and to prevent a patient from leaving the department when there was not a member of staff present.”
“Inspectors praised the “exceptional resilience” of staff but said they suffered from “change fatigue” because of repeated incomplete initiatives from management.”
“Sir Mike said that “staff had now accepted a standard of care that was unacceptable” and “some of the executive team were identified as barriers to the leadership of effective change”.
The trust dismissed Dr Macanovic claiming that she was guilty of “serious misconduct”.
Despite the GMC’s effective conclusion that Dr Macanovic’s referrals were professionally appropriate – indeed, required, a dismissal letter from Theresa Murphy stated that one of the reasons for Dr Macanovic’s dismissal was the fact that she had made disclosures to the GMC:
“Despite internal and external confirmation that button holing is not contraindicated and carries no specific risks, and despite you not being an expert in vascular access, you not only continue to disagree with its use, but you also referred colleagues to the GMC for using/supporting its use and I do not feel you acted professionally in this regard”
This was a clear smoking gun linking the dismissal to protected disclosures.
Theresa Murphy’s dismissal letter also reportedly claimed:
“Relationships between you and a number of consultants in the Renal Unit have broken beyond repair as a result of your behaviour”
The ET also noted substantial issues of bias and procedural unfairness by the trust and various other whistleblowing related detriments.
Was the trust badly advised? We do not know, but the ET pointed out that the trust’s solicitors Mills and Reeve variously accused Dr Macanovic of
not acting in good faith
not articulating her concerns about the buttonholing
referring colleagues to the GMC ‘with no good reason’
Mills and Reeve act for many NHS organisations and are therefore familiar to a number of whistleblowers who have been driven to litigation.
The ET observed that the trust tried to argue that it was not so much Dr Macanovic’s whistleblowing that was the problem, but the manner in which she went about it. The ET rejected this.
The ET noted that Dr Macanovic could have been more diplomatic. However, English is reportedly her third language and there may be cultural differences in social directness to consider.
Diplomacy notwithstanding, the ET determined:
“The main plank of the respondent’s case is that Dr Macanovic was not dismissed for making these disclosures but for the manner in which she did so. But that distinction was not apparent in the dismissal letter, nor to any great extent during the disciplinary proceedings, and does not seem to us to be justified in hindsight. The plain fact is that after over twenty years of excellent service in the NHS, Dr Macanovic was dismissed from her post shortly after raising a series of protected disclosures about this one issue. It is no answer to a claim of whistleblowing to say that feelings ran so high that working relationships broke down completely, and so the whistleblower had to be dismissed.”
Quite rightly, the ET focussed on the core public interest issues – something that many Tribunals fail to do:
“Dr Macanovic was concerned with one main issue, potentially a matter of life and death. She raised her concerns against a dominant management group and at two meetings there were heated exchanges. Tempers were raised on both sides. The findings of the disciplinary process were, in our view, very one- sided, reflecting a determination to remove Dr Macanovic as the source of the problem, but that is very different from one individual making a disproportionate fuss about things that concern them. Regard must be had to the scale of the issues at stake in deciding between the message and the method used.”
Moreover, the ET made it clear that no substantive contributory fault could be attributed to Dr Macanovic:
“Given our view that the Trust have not shown a potentially fair reason for dismissal, there is no basis for a reduction on the basis that a fairer process would have led to the same result (a Polkey deduction) or to contributory fault on her part.”
This is a refreshing departure from the great multitude of ET judgments that get bogged down in spurious counter-allegations by institutions with deep pockets for legal shenanigans.
It is thus a warning to arrogant NHS trusts that may be tempted to hit the “breakdown of relationships” and “Some Other Substantial Reason” button in order to rid themselves of whistleblowers.
So, it seems that which is intended to drop whistleblowers through a hatch in the floor to shark infested waters may occasionally end up as an unwelcome eject button for trust directors.
Therese Murphy now describes herself as a former chief nurse on her LinkedIn entry.
The ET’s unequivocal finding in favour of Dr Macanovic is unusual. But she should never have suffered the ordeal she went through. Much stronger UK whistleblowing law and infrastructure are needed to ensure protection at much earlier stage of the process, to prevent both harm to the whistleblower and the public.
If you wish to protect whistleblowers and to help stop their concerns being covered up, please click on this link and lend your signature to this petition for much better UK whistleblowing law:
The body Practitioners Performance Advice (which replaced NCAS) agreed to improve its procedures following the whistleblowing cases of Dr Macanovic and Mr Reuser, to safeguard against employers feeding false and malicious information in referrals to engineer suspensions and out adverse outcomes for doctors.
2. Portsmouth Hospitals University NHS Trust scored fairly averagely on whistleblowing questions in the last NHS staff survey, but this still meant that about a quarter of staff did not feel secure in raising concerns.
2. Where disciplinary charges fail, a common method of dismissing NHS whistleblowers is by arguing an irretrievable breakdown of relationships:
3. NHS staff lack adequate procedural protection from abusive employers who make malicious use of disciplinary processes and arbitrary exclusions. The NHS has failed for twenty years to act on recommendations from the National Audit Office to strengthen safeguards:
Tom Kark QC’s 2018 review recommendations for tightening up the oversight of NHS management probity, short of full regulation, have not yet been implemented. NHS Improvement confirmed to me last week that a planned “Kark” register for tracking adverse information about managers’ fitness has not yet been established.
This laxity and impunity for whistleblower reprisal gives licence for further abuses.
5. “Mobbing” is a group dynamic by which whistleblowers are often attacked and smeared by overwhelming, concerted allegations and undermining. It is recognised in some European employment law as “moral harrassment”. Dr Macanovic’s case illustrates how the introduction of such a provision into UK whistleblowing law could more finely target and improve protection:
Summary: An as yet unpublished Kings Fund review about poor leadership at HSIB has resulted in the agency being stripped of its maternity investigations by the Department of Health and Social Care. Was the affair in any way an attempt by the government to control a mounting maternity personal injury bill, because HSIB investigations had helped to establish liability?
HSIB, the investigatory arm of the regulator NHS Improvement was one of Jeremy Hunt’s cynical and superficial ‘patient safety’ gestures created in response to pressures over unresolved patient safety issues following the Midstaff Scandal. He established it whilst he continued to defund and undermine the NHS.
Significantly, the latest scandal led to HSIB being stripped of its maternity investigations – an area which had been mushrooming with the revelations at Shrewsbury and Telford NHS Trust, with huge liability implications for the NHS and the government. HSIB had been undertaking about 1000 maternity investigations a year.
“In announcing his retirement Keith Conradi, Chief Investigator says:
“It has long been my intention to retire at 60 while my health enables me to participate in competitive triathlon.”
Other senior departures from HSIB were also reported.
When HSIB’s creation was first announced, I made attempts to obtain objective evidence of whether aviation and AAIB were truly a paragon of safety culture as Hunt had claimed. I asked for old AAIB staff survey results, but was repeatedly blocked by the government. This was despite the ICO ruling that there was no good reason for the Department of Transport to withhold the information. Litigation continues on the matter with the ICO opposing the government. It is before the Tribunal again in April.
Before HSIB became operational, I had a foretaste of things to come when I tried to engage its players in ensuring effective whistleblowing governance. They clearly knew little about whistleblowing but seemed to have minimal interest in becoming more competent. The venture seemed very insular and clubby. After being told that someone with no visible whistleblowing expertise would sort it all out, I made a challenge to the boys’ club culture. This was met with uncomprehending huffiness by one of the safety luminaries backing the project. No doubt those grand men will quickly forget their poor judgment and move on to the next vanity project dangled before them by politicians.
After the major scandal broke this January, I asked NHSI for a copy of the Kings Fund review and other information about NHSI’s handling of the HSIB affair. However, NHSI has not yet answered despite intervention from the ICO and an exchange of correspondence with Andrew Morris who said he had asked his FOI team to expedite the matter.
It is a failing by NHSI that the Kings Fund review of HSIB is not already published. It was commissioned in secret and remains withheld. NHSI bears ultimate responsibility for HSIB’s failure.
Indeed, was HSIB’s leadership substantially worse than the abusive, failing NHS trust managers than NHSI protects and recycles on a daily basis?
Indeed, how do we know if HSIB’s culture was any worse than that of NHSE and NHSI’s? Neither NHSE or NHSI routinely publish their own staff survey results and are frequently criticised for bullying provider organisations.
Notwithstanding any justified criticism of the obviously poor leadership of HSIB; was the decapitation of the agency in any way a government attempt to block transparency about NHS safety failings? Was it merely a pretext to control a huge bill from maternity injury pay outs?
And what of NHSE/I’s hireling, the Kings Fund? Did it give the HSIB leadership and its staff a fair hearing?
The King’s Fund board of trustees has traditionally been populated with the powerful, connected and sometimes recycled. I previously asked its former Chair Sir Christopher Kelly, former Department of Health Permanent Secretary, if he was one of the referees for Jo Williams the disgraced former Chair of the CQC when she applied to re-enter the NHS as Chair of Alder Hey NHS Foundation Trust:
A doctor at Smith’s trust spoke up critically about Smith’s appearance on Strictly: “Clare Gardner launched an online petition, reading: “She is the chair of the largest NHS Trust in the UK, during a time of major crisis i.e. the second Covid-19 wave.“We are already in a Tier Two lockdown. I am a haematologist within the Trust she apparently chairs.“Our Chief Executive Dr David Rosser has made numerous statements to the press recently, describing the fear and foreboding we all sense towards rising cases.”“Now that we are facing a similarly perilous situation, she has swanned off to London to dance.“This is a dereliction of duty.“If ever there was a time to have figureheads in place for NHS organisations that are struggling, it is now.“Jacqui would rather wear sequins than look after her charge.”
One can only hope that Dr Gardner is unharmed and still prospers.
Smith was also chair at UHB during Mr Tristan Reuser’s whistleblowing ordeal. She failed to answer a request in August 2021 for data about the trust’s abusive handling of the Reuser litigation and about FPPR process regarding her chief executive, despite a reminder. The matter is now with the ICO.
The Kings Fund churns out forests of prim admonishments about how NHS leaders should behave. It calls often for compassionate leadership. It positions itself in the market as a seller of advice and reviews on how to do it right.
Some of the Kings Fund’s prominent figures have sometimes worked symbiotically with the equally virtue signalling National Guardian’s Office.
So I attempted to check out the actual quality of the goods and asked the Kings Fund to share its own staff survey data. This was because the first thing noticeable is that this data is not published.
After one email to its comms team, two emails to its CEO Richard Murray and one email finally to its Chair Lord Kakkar, I received an acknowledgment from the CEO’s office. This was followed by a minimal substantive response from the Kings Fund comms team on 3 March, giving headline figures for amalgamated years and no staff survey reports:
“Dear Dr Alexander
Thank you for your emails about staff wellbeing at The King’s Fund. We don’t have a record of your original inquiry to this account so please accept our apologies for the delay in responding and treat this as a response to this and the emails you subsequently sent to Richard Murray.
The King’s Fund has been running staff satisfaction surveys since 2008, usually every other year. They are managed on our behalf by an organisation called the Leadership Factor so that scores and narrative can be provided confidentially. Between 2008 and 2015 the overall satisfaction score was between 71 per cent and 78 per cent, placing us in the top quartile of organisations the company surveyed.
In 2017, we refreshed the design of the survey and included specific questions about engagement and wellbeing. In 2018, these factors scored 8.4 and 7.6 out of 10 respectively, where 10 is very satisfied. We were due to run the survey again in 2020 when the pandemic hit. At the end of 2020, we introduced regular pulse surveys in place of the full survey which included questions about health and wellbeing, levels of optimism and morale. We will run the full satisfaction survey again in Autumn 2022.
Best wishes
Gemma Umali
Press and Public Affairs Manager”
I asked for more detail, pointing out that it would be useful for example to see how minority staff groups fared.
“Many thanks for your response and the broad percentage results extracted and aggregated from past staff surveys.
It would be more useful to have actual copies of the staff survey reports from tne years in which you say the surveys were carried out.
It is hard to make much sense of broad headline results without any contextual details.
For example, the stratified results for different staff groups, (assuming that this data is collected by the Kings Fund) and particularly minority groups are important to see – as the Kings Fund itself has emphasised in the past when passing comment on the national NHS staff survey.
Your aggregation of results from different years also obscures possible variations over time.
I would be very grateful f you would share copies of the original staff survey reports.
However, if the Kings Fund does not wish to share the actual reports, would you at least be willing to share the questionnaire forms that staff filled in on the years in question?
Mamy thanks
Minh
Minh Alexander
Cc Richard Murray CEO Kings Fund
Lord Ajay Kakkar Chair Kings Fund”
At the time of writing, I have not yet received either a copy of the questionnaire that Kings Fund staff fill in, nor the original staff survey reports. I guess the Kings Fund comms folk have still got their thinking caps on. Compassionately, no doubt.
PETITION
Please click and add your signature to this petition to reform UK whistleblowing law – whistleblowers protect us all but weak UK law leaves them wholly exposed and it is a threat to public safety
1. NHS England/ Improvement eventually reluctantly disclosed a copy of the Kings Fund report on HSIB, terms of reference and associated correspondence, which showed that a rigorous investigation was never intended:
2. As discussed above, the dispatch of undesirable senior NHS managers is the exeception rather than the rule.
The number of cases of NHS England, NHSI and its predecessor bodies covering up, protecting and recycling abusive, incompetent and or dishonest NHS managers are too many to list.
But here is a striking example of former NHS CEO Paula Vasco-Knight, unpicked to show the lengths to which the protection often extends and why the HSIB case is different:
3. After leaving UHB in October 2021, Jacqui Smith took up two new NHS Chairs at Barts Health NHS Trust and Barking, Havering and Redbridge University Hospitals NHS Trust. This looks to be system preparation for a politically sensitive merger of the two trusts, which is already stirring up controversy, with Margaret Hodge stepping in.