By Dr Minh Alexander NHS whistleblower and former consultant psychiatrist, 28 November 2017
Simon Stevens made an eye-catching promise at a Workforce Race Equality Standard (WRES) conference on 31 October 2017 that one third of NHS England’s own Speak Up Guardians would be BME staff. A throwaway soundbite perhaps, but potentially a very significant precedent in that Stevens appeared to be promoting the concept of BME quotas in recruitment.
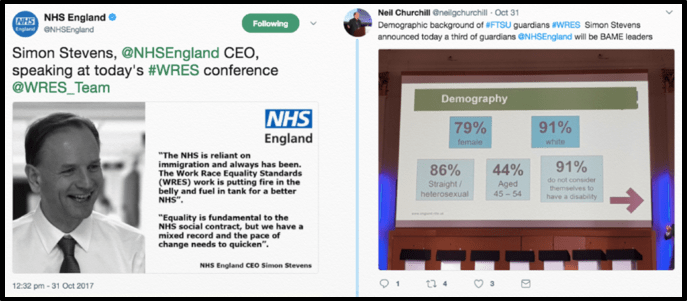
His promise followed acknowledgment by the National Freedom To Speak Up Guardian that BME staff were under-represented amongst Freedom To Speak Up Guardians.
I asked for NHS England’s intended methodology in achieving Stevens’ target of one third BME Speak Up Guardians. In response, there was an indication that NHS England was developing its process, but no details on how the quota would be achieved:
“Simon Stevens recently announced that a third of freedom to speak up guardians in NHS England will be from black and minority ethnic (BME) backgrounds and colleagues are finalising the processes for this to happen.”
From a response by the WRES Team 9 November 2017
A direct request to Simon Stevens to release national NHS Race data that is languishing under NHS England’s control, which would incur negligible cost, has been met so far with ambiguity and no clear agreement to release.
Adding to this mix, CQC revealed via a recent FOI disclosure that it is effectively looking the other way by not recording the ethnicity of provider staff who are consulted during inspections.
This is despite CQC having made a great display of enforcing WRES, through inspection:
https://www.england.nhs.uk/publication/workforce-race-equality-standard-technical-guidance-2017/
http://www.cqc.org.uk/news/stories/cqc-support-nhs-tackling-race-inequality-across-workforce
Enquiries to NHS England about whether its WRES team had actually kitemarked CQC’s inspection methodology on WRES have not so far borne fruit.
This silence is amplified by ongoing scandal about CQC’s failures at Southport and Ormskirk Hospital NHS Trust, where it failed to listen properly to the concerns of BME staff and seriously botched yet another FPPR process.
In a clear demonstration of the level of workforce mistrust engendered by such regulatory behaviour, not one of the BME doctors who raised concerns in 2015 about Southport and Ormskirk Hospital NHS Trust came forward to speak to the National Guardian’s office when it recently reviewed these matters.
The correspondence with NHS England about these CQC omissions, and supporting references, are provided below.
Millions have been spent on the NHS Race industry, with much glossy publicity and high profile events. But how much do frontline BME staff truly benefit from this largesse?
The unedifying fall of NHS England’s former poster girl for Race, Paula Vasco-Knight, equally raises questions about the conduct of the NHS Race programme.
It is not PR overdrive and endless ‘monitoring’ that are required, (albeit it is important to note that crucial issues such as Race ET claims against the NHS and NHS pay inequality are still not tracked).
It is greater accountability and effective enforcement of robust standards that are required.
UPDATE 29 NOVEMBER 2017:
One day after the above post, the NHS England WRES team has decided that despite inviting me to its event on 30 November 2017, it will not cover my travel expenses as an unwaged whistleblower. Draw your own conclusions…

UPDATE 2 DECEMBER 2017
I attended the WRES event on 30 November 2017, paying out of my own pocket to travel to London. I was approached by a member of the WRES team at the event, who repeated the statements about WRES not being able to pay me. I have now asked Simon Stevens NHS England CEO for reimbursement of my £35.20 travel expenses:
Simon Stevens Christmas card
RELATED ITEMS
Will Simon Stevens uncork ALL the NHS Race data?
https://minhalexander.com/2017/10/11/will-simon-stevens-uncork-all-the-nhs-race-data/
Postscripts on Paula: NHS England’s apologia and regulatory reticence
https://minhalexander.com/2017/10/10/postscripts-on-paula-nhs-englands-apologia-regulatory-reticence/
CQC has lost all moral authority, but what will the National Guardian do?
https://minhalexander.com/2017/05/23/fppr-cqc-has-lost-all-moral-authority-but-what-will-the-national-guardian-do/
CORRESPONDENCE WITH NHS ENGLAND ABOUT CQC & RACE
BY EMAIL
Yvonne Coghill
Director of WRES Programme
NHS England
28 November 2017
Hi Yvonne,
Academic and Data meeting 30 November 2017, and CQC inspection methodology on NHS Workforce Race Equality Standard
Thanks for the meeting agenda.
Is it possible to have confirmation of whether there is a written agreement between NHS England and CQC on inspection methodology as applied to WRES, under the Well-Led domain? As you know, I first asked for this on 30 October and again on 26 November but I have received no response.
As you may recall, I asked for this information following an FOI disclosure of 5 July 2017 by CQC that stated:
“The inspection team spoke with 219 members of staff during the inspection; we do not record their colour or ethnicity, as this does not form part of our methodology for inspection. This information is therefore not held.
https://www.whatdotheyknow.com/request/equality_and_diversity_inspectio#incoming-1001621
This seems a crucial omission.
In 2015 CQC failed BME staff who reported concerns about Southport and Ormskirk Hospital NHS Trust. CQC gave undue weight to management assurances, and to a management commissioned FPPR report which concluded that there were no serious failings. 1 However, shortly afterwards the trust Chief Executive and other trust directors were suspended. 2
A recent review by the National Guardian has revealed that CQC accepted the FPPR report, despite the fact that FPPR investigators failed to speak to the BME staff who raised concerns at Southport and Ormskirk. 3
That not a single BME doctor, who had previously raised concerns at Southport and Ormskirk, was prepared to speak to staff from the National Guardian’s office during the recent case review emphasises how damaging it is to culture when oversight bodies behave tokenistically and breach staff trust:
“Although we had hoped to speak to some of the BME doctors who had previously raised concerns none of them attended the forums or approached us in person.”
CQC and NHS England have variously issued public statements about how CQC is supporting WRES through its inspection of the Well Led domain, and CQC has appointed a few Race and Diversity specialist advisors.
However, if there is no agreed inspection methodology and or CQC’s methodology is ineffective, this is an additional weakness in failures of WRES enforcement.
Whistleblowers have seen a parallel pattern in that CQC claims a commitment to supporting good practice but resists transparent and effective inspection methodology. For example, CQC has repeatedly resisted examination of NHS providers’ compromise agreements and use of gags despite being advised to do so by the Freedom to Speak Up Review. 4
Of relevance to the main theme of the event this Thursday, I suggest that an important part of any future metrics is the measurement of WRES enforcement activity.
A pre-requisite of measurement is clear standards. I would be grateful for a response to my enquiry of 30 October as soon as possible. It looks to me as if CQC inspection methodology on Race inequality is likely to be ineffectual and discriminatory at least by omission, and if so will need substantial improvement. If it is possible to have sight of the relevant documents, this will enable a more informed discussion at our forthcoming meeting.
Best wishes,
Minh
Dr Minh Alexander
NHS whistleblower and former consultant psychiatrist
Cc David Isaac Chair EHRC
Philip Dunne Minister of State for Health
Simon Stevens NHS England Chief Executive
Peter Wyman CQC Chair
Dr Henrietta Hughes National Freedom To Speak Up Guardian, CQC
Paul Corrigan CQC NED and Board lead on WRES
Sir Robert Francis CQC NED and Chair of National Guardian’s Accountability and Liaison meeting
Marie Gabriel Chair WRESAG
Prof Mala Rao Vice Chair WRESAG
Victor Adebowale NHS England NED
Other delegates 30 November 2017
REFERENCES
1 CQC inspection report on Southport and Ormskirk NHS Trust 13 May 2015:
“As a result of the allegations the CQC initiated a regulatory challenge relating to Fit and Proper Person Regulation. In response the Trust commissioned an independent, external investigation the final report of which has ben received by the Trust Board. The investigation found no evidence or grounds for the allegations. The CQC has reviewed the report viewing it as thorough”.
https://minhalexander.com/wp-content/uploads/2017/11/cqc-southport-and-ormskirk-inspection-report-aaab8967.pdf
2 By August 2015, it was announced that the Southport and Ormskirk chief executive and other directors had been suspended:
http://www.liverpoolecho.co.uk/news/liverpool-news/southport-ormskirk-hospital-chiefs-suspended-9788193
3 National Guardian case review on Southport and Ormskirk November 2017
“In response to workers’ repeated concerns about the alleged discriminatory behaviour of one of the trust’s directors the trust commissioned an external Fit and Proper Person (FPP) review in 2015 to determine whether the director’s competence and character met those standards. However, evidence cited in the trust’s cultural review highlighted that the FPP investigation did not interview any of the staff who had spoken up about the director in question. This was despite the fact that, for a director to be a fit and proper person under the regulations, one of the requirements their employer must show is that they have ‘not been responsible for … any serious misconduct or mismanagement’ – the very type of misconduct that staff who spoke up were alleging. National Guardian’s Office 22 Southport and Ormskirk Hospital NHS Trust – A case review Upon completion the FPP review ‘found no evidence of discrimination or racial discrimination’ against the director in question.”
https://minhalexander.com/wp-content/uploads/2017/11/national-guardian-case-review-20171115_ngo_southportormskirk.pdf
4 NHS Gagging. How CQC sits on its hands.
https://minhalexander.com/2016/09/23/nhs-gagging-how-cqc-sits-on-its-hands-2/
From: “WRES, England (NHS ENGLAND)” <england.wres@nhs.net>
Subject: RE: IMPORTANT – Workforce Race Equality Standard (WRES) – Academic and Data meeting
Date: 27 November 2017 at 17:37:28 GMT
To: “COGHILL, Yvonne (NHS ENGLAND)” ********************************************************************************************************************************************************************************************************************************************************************************************************************************************************************************************************************************************************************************************************************************************************************************************************************************************************************************************************************************
Dear Colleague,
You will be aware that the WRES was implemented in the NHS in 2015, we are now in the next phase of the programme, supporting organisations to improve race equality and to become truly inclusive.
https://www.england.nhs.uk/about/equality/equality-hub/equality-standard/
We would now like to reflect on research that has been done around the subject of health and race and decide what more/else needs to be done and believe you would be instrumental in helping us to shape our thinking. Professor Mala Rao, Imperial College London, has agreed to chair a workshop where we will look at the data and work to date and decide what more needs to be done, including the possibility of establishing a race observatory.
We will be holding the workshop at Friends House, 173 – 177 Euston Road, London, NW1 2BJ on November 30th 2017 and would be delighted if you are able to attend or nominate a colleague who would be better suited to attend.
We will forward the agenda in due course and sincerely hope you can attend and help contribute to this really important discussion about health and race in the NHS.
Please accept invite to confirm your attendance and forward all dietary requirements to sniles@nhs.net ASAP.
You can stay up to date with WRES by following us on Twitter: @WRES_team.
Yours sincerely,
Yvonne Coghill, OBE
Director
Workforce Race Equality Standard (WRES) Implementation
WRES Implementation Team
NHS England
Quarry House | Quarry Hill | Leeds | LS2 7UE
www.england.nhs.uk/wres/
Twitter: @WRES_Team
********************************************************************************************************************
This message may contain confidential information. If you are not the intended recipient please inform the
sender that you have received the message in error before deleting it.
Please do not disclose, copy or distribute information in this e-mail or take any action in relation to its contents. To do so is strictly prohibited and may be unlawful. Thank you for your co-operation.
NHSmail is the secure email and directory service available for all NHS staff in England and Scotland. NHSmail is approved for exchanging patient data and other sensitive information with NHSmail and other accredited email services.
For more information and to find out how you can switch, https://portal.nhs.net/help/joiningnhsmail