By Dr Minh Alexander, NHS whistleblower and former consultant psychiatrist 8 October 2016
Summary
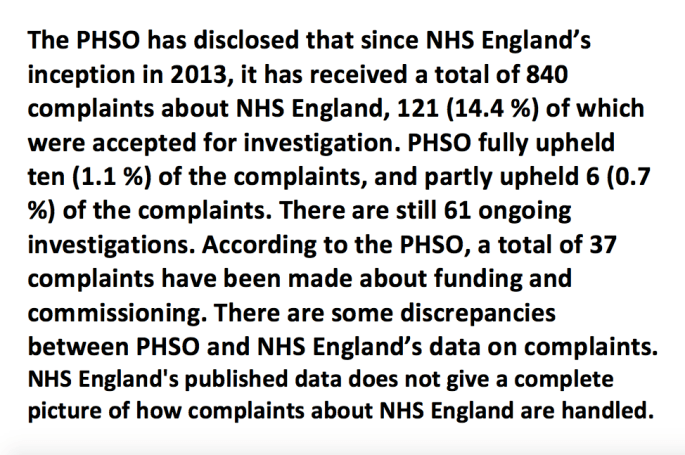
CQC continues to fail to protect vulnerable people. As an example of this, and despite revelations of failings a year ago, there is still no evidence that CQC responds in a consistent way to coroners’ warnings about care homes failures. CQC has been sent about half (31 of 66) of the coroners’ warnings issued about care home deaths since July 2013. There have sometimes been lengthy gaps between coroners’ warnings and subsequent inspections by CQC. In 18 (27%) of the 66 cases, there is no evidence yet that a coroner’s warning has triggered a CQC inspection. CQC inspection reports rarely refer to deaths or to coroners’ warnings. There are only two published CQC responses to coroners’ warning reports. There is no published response by CQC to a criticism that it failed to inspect medicines management prior to the death of a patient who was given the wrong medication. There is also no published CQC response to two coroners’ warnings which concluded that there was neglect, and which noted an allegation of physical harm by care home staff. A year ago, after CQC’s poor response to coroners’ warnings about care homes was criticised, David Behan promised that CQC would improve and undertake analyses of coroners’ data. There is still no published evidence that analyses have been undertaken.
Introduction
Social care is in even worse trouble than the NHS, with dire under-funding [1], under staffing, exploitation of staff who are sometimes not even paid the legal minimum wage [2] [3] and general pressures that increase the risk of error and abuse.
Care workers paid less than minimum wage who are taking legal action:

http://www.bbc.co.uk/news/uk-37350750
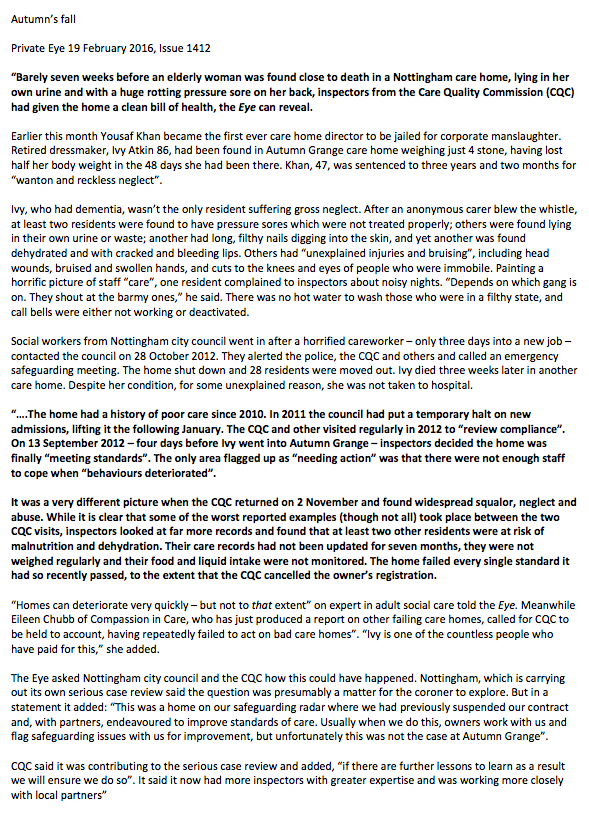
However, the CQC has been repeatedly and copiously criticised for failures to detect and respond to poor care, and failures to listen to care home whistleblowers. [4] [5] Over the last year, there have been five Private Eye articles exposing the CQC’s poor regulation of the sector, including repeated failures to be fully transparent about poor care homes’ histories, despite this being pointed out since 2010. In total, Private Eye has featured 22 articles about CQC’s care home failures and obfuscation since 2010. The sorry history can be found summarised in the report “CQC an ongoing concern” by the campaigning charity Compassion in Care, which has collaborated with many of the Private Eye investigations: http://www.compassionincare.com/node/229
The CQC has also been criticised for its closeness to the care home industry. Questions raised about CQC’s objectivity, which CQC’s Chief Inspector has dismissed:
“I am a firm believer in the value of constructive engagement between the regulator and providers and have welcomed the contribution provider representatives have made to the development of our new regulatory regime. I speak regularly at conferences organised for providers so that I can explain clearly my expectations of them and hear about their issues.” [7]
Despite the Secretary of State’s claims to be reforming services with “intelligent transparency”, the CQC is not sufficiently transparent or accountable to the public about the most crucial issues. Other analyses have shown that CQC does not present deaths and other safety data in a complete or consistent manner in its inspection reports. [8] [9]
A year ago, the Bureau of Investigative Journalism and the Independent exposed failure by the CQC to respond to serious coroners’ warnings about care homes. [10] This investigation identified 23 coroners’ warnings about care homes since July 2013. It reported that in over half of these cases, the coroners’ reports had failed to trigger an inspection by CQC.
This was of particular concern because the CQC had previously claimed that it agreed a memorandum of understanding with coroners in 2014:
“Coroners Society: In 2014 we developed a memorandum of understanding with the Coroners Society. We now receive information from individual coroners’ reports about any deaths in health and care settings and how these could be prevented in future. This information is provided to our inspection teams who use the details of the report in their work with individual providers.” [11]
Indeed, it is extraordinary that CQC only reached this joint working arrangement with coroners five years after its inception, and despite scandals such as the Harold Shipman killings.
David Behan CQC Chief Executive responded thus to the 2015 TBIJ and Independent investigation: “I am not going to defend the indefensible. We have got more to do.”
In a related CQC press release, David Behan promised that CQC would improve its response to coroners’ warnings and “ensure any concerns raised are effectively logged, analysed, managed and reviewed” [12]
Results of new analysis
I have carried out an updated search of published coroners’ Reports to Prevent Future Deaths on care homes (PFDs) and I have cross checked these with CQC inspection reports of the care homes in question, to look for evidence of improvement. The relevant data is uploaded here: care-home-rule-43s-8-10-2016
PFD reports (formerly known as Rule 43 reports) are issued when coroners identify risks that may cause future deaths. [13] Most often, PFDs relate to factors that have contributed to the deaths reviewed, but incidental risks that are discovered may also be reported. PFDs are sent to the relevant organisations with responsibility for addressing the risks identified by the coroner, with a requirement for response within a defined timescale. PFDs have been published since July 2013. The Chief Coroner advises that most PFDs, and responses by organisations that are sent PFDs, are published.
The Chief Coroner has published 71 PFD reports since July 2013 that his office has categorised as ‘care home deaths’. Five of these reports related to domiciliary and transport services rather than care homes, and were excluded from this analysis, leaving 66 PFDs about care home cases. The care homes were not identified in two of the 66 cases, so they could not be cross-referenced with the relevant CQC care home inspection reports. Links to all 66 coroners’ PFD reports are provided below.
The 66 care home PFD reports were distributed in time as follows:
|
YEAR
|
Number of coroners’ PFDs issued about care home deaths
|
|
2013, from July onwards
|
11 |
|
2014
|
24 |
|
2015
|
14
|
| 2016 year to date |
17
|
NB. 2016 figures may not be complete, as there is a lag between the issue and publication of PFDs.
In the 66 care home PFDs, coroners warned about poor staffing levels and training, poor management of falls and risk assessment, failures to safely manage urgent medical needs, poor medicines management, inappropriate placements in homes that could not meet the most complex needs, inadequate arrangements regarding resuscitation and end of life care, failures of Safeguarding and lack of incident investigation. In two cases, coroners explicitly criticised the CQC for not recognising a serious burns risk prior to a death, and for failing to inspect medicines management prior to a related death “purportedly because they [CQC] did not have anyone available to inspect and review the drugs administration system at the time”.
There was no evidence that 18 (27%) care homes have been inspected by CQC after coroner’s PFDs were issued. The time elapsed since the issue of PFDs ranged between 3 and 32 months, with an average interval of approximately 15 months. In ten of these 19 cases, a year or more had passed since a PFD was issued without evidence of subsequent inspection. Obviously, some CQC inspections may have been conducted but not yet reported, but the length of the gaps still suggests that there have been excessive delays in some of the cases. One of the 18 care homes is no longer operating, but even so, there is no evidence that CQC inspected it in the 22 months in which it continued operating after the coroners’ PFD was issued.
CQC had inspected 46 care homes after PFDs were issued. The interval between the PFDs and subsequent CQC inspections ranged between 2 days to 27 months, with an average interval of approximately 7 months. In eleven cases, a year or more passed after PFDs, without evidence of a subsequent inspection.
Since CQC acknowledged the failings highlighted a year ago by the TBIJ and Independent, a further 18 care home PFD reports have been issued by coroners. Eleven of the 18 homes were subsequently inspected, with an average gap of approximately 4 months between the PFDs and the subsequent inspections. There is no evidence that six of the 18 care homes have yet been inspected, with an average of approximately 5 months gap since the PFDs were issued. This suggests that CQC may have been responding more quickly to PFDs that were issued over the last year, but it has inexplicably still not clearly responded to older PFDs.
To check whether CQC had already responded to deaths prior to the issue of coroners’ PFD reports, the dates of all inspections after the deaths were examined. These showed similar variation and delays.
57 of the 66 homes had been inspected after the deaths, with the interval between death and subsequent inspection ranging between 0 to 37 months, with an average interval of approximately 7 months. In eleven cases, it took a year or more after a death before the care home was inspected.
There was no evidence that 6 homes have been inspected after the deaths, with a range of 10 to 41 months since the deaths, and an average interval of 17 months.
The majority of the CQC reports from inspections undertaken after the deaths, and after issue of PFDs, did not specifically mention the deaths or the coroners’ PFDs. [14]
Overall, the results raise questions about whether the CQC is reliably detecting sentinel events – or worse, detecting them but not responding and reporting appropriately.
What about the 31 PFD reports sent to CQC, and the people who suffered?
About half of all care home PFDs – 31 of 66 – had been sent to the CQC. Of these, 11 had been directly addressed to the CQC as a named respondent, as opposed to just being copied to CQC for information. See Table 1 for details of the 31 PFDs sent to CQC: care-home-rule-43s-table-1
Even when PFDs were sent to CQC the response, in terms of evidence of subsequent inspections, was still erratic and slow. See Table 2 for details: care-home-rule-43s-table-2
In the 31 cases of which CQC was notified of concerns via coroners’ PFDs, there is still no evidence that 7 of the care homes have yet been inspected. The time elapsed without inspection ranged between 3 and 29 months, with an average of approximately 12 months.
23 of the 31 care homes had been inspected, with the interval between PFDs and subsequent inspections ranging between 2 days and 27 months, with an average interval of approximately 7 months.
In only two of the 31 cases notified to CQC by coroners was there a published response by CQC. Both cases related to the physical safety of care home premises:
Death of Marjorie Keogh
https://www.judiciary.gov.uk/wp-content/uploads/2014/02/2013-0325-Response-by-Care-Quality-Commission.pdf
Death of Walter Powley
https://www.judiciary.gov.uk/wp-content/uploads/2014/05/2013-0251-Response-by-Care-Quality-Commission.pdf
Both of these CQC responses acknowledged the importance of the intelligence provided by coroners and accordingly, emphasised that the information would be cascaded to CQC staff.
However, there was a published CQC response to only one out of the 11 PFDs that were directly addressed to CQC.
There was no published response to a PFD addressed to David Behan himself in the case of Gwendoline Clarke, who sustained multiple injuries and who had made an allegation that a member of staff had hurt her.
There was no published CQC response to the PFDS about Dorothy Clarkson and Barbara Cooke, which explicitly found neglect (choking and two grade 4 pressure sores respectively) and had been addressed directly to CQC.
There was no published CQC response to the case of Derrick Rivers, in which the coroner had addressed his PFD to David Behan. This was despite findings by the coroner of unsafe medicines management and failure by the CQC to review the care home’s medication arrangements prior to the death.
There was no published CQC response to the PFD about Mary Waldron, directly addressed to CQC, in which the coroner expressed concern about failure to recognise and appropriately manage a patient with deteriorating physical health. This was despite the fact that the coroner noted that the care home had reported inaccurately to the CQC and the coroner wanted to know what investigation the CQC would undertake.
In the case of Walter Powley who suffered severe burns after falling against a radiator, the coroner was concerned that CQC had missed the fact that radiators were run at temperatures well in excess of HSE guidance, and that they were not covered. Of concern, the first recorded CQC inspection was conducted 12 months after the coroner’s PFD report, even though the PFD had been addressed to David Behan himself.
There was no published CQC response to a PFD about Stanley Ward that was addressed to CQC. This raised concerns about insufficient guidance to staff about how to manage falls and injuries where older people are on anti-coagulants, that increase the risk of intracranial bleeding. This issue featured in several other care home PFDs, which CQC would have picked up if it had systematically tracked PFD intelligence.
However, the CQC has not yet published any evidence that it has analysed the copious evidence that it has received from coroners.
One has to ask quite how much repeated failure is tolerable, from a body that must surely hold itself to the highest standards if it expects to judge others.
I am sending this additional evidence to parliament for the next CQC accountability hearing. I hope the Health Committee will wonder how many times do the same ‘mistakes’ need to be made before one asks if they are deliberate?
CQC has cost the taxpayer well over a billion pounds in just its running costs, let alone the cost of its failures. Isn’t that rather a lot of money just for political window dressing and a load of old ‘’learning by doing” rope?
In its seventh year of failure, shouldn’t CQC be blushing whenever it wheels out its habitual “work in progress” refrain?
CQC operational expenditure
Source: CQC annual reports
|
Financial year
|
CQC operational expenditure |
|
2009/2010
|
£189, 941,000 |
|
2010/2011
|
£139,089,000
|
|
2011/2012
|
£149,440,000 |
|
2012/2013
|
£163,665,000
|
|
2013/2014
|
£171,052,000 |
| 2014/2015 |
£221,706,000
|
| 2015/2016 |
£248,045,000
|
| All years |
£1, 282,938,000
|
Related items:
Do “Complaints Matter” to CQC?
https://minhalexander.com/2016/10/02/do-complaints-matter-to-cqc/
CQC Deaths Review: All fur coat
https://minhalexander.com/2016/09/25/cqc-deaths-review-all-fur-coat/
REFERENCES
[1] Social Care for Older People, Home Truths, Kings Fund, 15 September 2016
http://www.kingsfund.org.uk/sites/files/kf/field/field_publication_file/Social_care_older_people_Kings_Fund_Sep_2016.pdf
[2] Tens of thousands of care workers ‘still paid below minimum wage despite new regulations’ Jamie Merrill, Independent, 23 March 2016
http://www.independent.co.uk/news/uk/home-news/tens-of-thousands-of-care-workers-still-paid-below-minimum-wage-despite-new-regulations-a6946596.html
[3] Care workers sue council contractor in minimum wages battle, Zoe Conway, BBC, 14 September 2016 http://www.bbc.co.uk/news/uk-37350750
[4] Orchid View, Serious Case Review, West Sussex Adult Safeguarding Board June 2014
http://www.hampshiresab.org.uk/wp-content/uploads/June-2014-Orchid-View-Serious-Case-Review-Report.pdf
[5] Staff sackings and suspensions over poor elderly care. Alison Holt BBC Panorama, 30 April 2014 http://www.bbc.co.uk/news/uk-27128011
[7] Care Home Open Day, Blog by Andrea Sutcliffe CQC Chief Inspector 22 June 2015, http://www.cqc.org.uk/content/care-home-open-day-0
[8] How safe are NHS patients in NHS hospitals? Prof Colin Leys and Prof Brian Toft, Centre for Health and the Public Interest, December 2015
https://chpi.org.uk/wp-content/uploads/2015/12/CHPI-PatientSafety-Dec15.pdf
[9] CQC deaths review: all fur coat, Minh Alexander 13 August 2016
https://minhalexander.com/2016/09/25/cqc-deaths-review-all-fur-coat/
[10] Elderly people put at risk as watchdog fails to act on warnings of ‘fatally negligent’ care homes, Melanie Newman and Oliver Wright, Independent 2 September 2015
http://www.independent.co.uk/life-style/health-and-families/health-news/elderly-people-put-at-risk-as-watchdog-fails-to-act-on-warnings-of-fatally-negligent-care-homes-10483573.html
[11] CQC Annual Mental Health Act monitoring report 2013/2014
http://www.cqc.org.uk/sites/default/files/monitoring_the_mha_2013-14_report_web_0303.pdf.pdf
[12] CQC press release 3 September 2015, ‘CQC response to the story in the Independent
http://www.cqc.org.uk/content/cqc-response-story-independent
[13] Chief Coroner’s guidance on Reports to Prevent Future Deaths
https://www.judiciary.gov.uk/wp-content/uploads/2013/09/guidance-no-5-reports-to-prevent-future-deaths.pdf
[14] CQC inspection reports were key word searched.
Links to the 66 coroners’ Reports to Prevention Future Deaths on care homes since July 2013:
Betty ADDISON https://www.judiciary.gov.uk/publications/betty-addison/
Keith BARTON https://www.judiciary.gov.uk/publications/barton-2013-0330/
Malcolm BENNETT https://www.judiciary.gov.uk/publications/malcolm-bennett/
Stanley BERE https://www.judiciary.gov.uk/publications/stanley-bere/
John BIRD https://www.judiciary.gov.uk/publications/john-bird/
Eliza BOWEN https://www.judiciary.gov.uk/publications/eliza-bowen/
Ross BOYD https://www.judiciary.gov.uk/publications/ross-boyd/
Phyllis BROOMHEAD https://www.judiciary.gov.uk/publications/phyllis-broomhead/
George BROWN https://www.judiciary.gov.uk/publications/brown-2013-0230/
Edna BULMER https://www.judiciary.gov.uk/publications/edna-bulmer/
Michaela CHRISTOFOROU https://www.judiciary.gov.uk/publications/michaela-christoforou/
Gwendoline CLARKE https://www.judiciary.gov.uk/publications/gwendoline-clarke/
Dorothy CLARKSON https://www.judiciary.gov.uk/publications/dorothy-clarkson/
Violet CLOUDSDALE https://www.judiciary.gov.uk/publications/violet-cloudsdale/
Margaret CONNOR https://www.judiciary.gov.uk/publications/margaret-connor/
Barbara COOKE https://www.judiciary.gov.uk/publications/barbara-cooke/
Freda CORDY https://www.judiciary.gov.uk/publications/freda-cordy/
Norman DORN https://www.judiciary.gov.uk/publications/norman-dorn/
Thomas FARRELL https://www.judiciary.gov.uk/publications/thomas-farrell/
Margaret FLEMING https://www.judiciary.gov.uk/publications/margaret-flemming/
Beryl FRENCH https://www.judiciary.gov.uk/publications/beryl-french/
Jean GILLESPIE https://www.judiciary.gov.uk/publications/jean-gillespie/
Joseph GODFREY https://www.judiciary.gov.uk/publications/joseph-godfrey/
Harold GOULDING https://www.judiciary.gov.uk/publications/harold-goulding/
Douglas GREY https://www.judiciary.gov.uk/publications/douglas-grey/
George HULME https://www.judiciary.gov.uk/publications/george-hulme/
Lillian HURSELL https://www.judiciary.gov.uk/publications/george-hulme/
Joan JONES https://www.judiciary.gov.uk/publications/jones-2013-0234/
Janine KAISER https://www.judiciary.gov.uk/publications/janine-kaiser/
Marjorie KEOGH https://www.judiciary.gov.uk/publications/keogh-2013-0325/
Charles LAWRENCE https://www.judiciary.gov.uk/publications/charles-lawrence/
Doreen MATTINSON https://www.judiciary.gov.uk/publications/doreen-mattinson/
Dorothy MC DERMOTT https://www.judiciary.gov.uk/publications/dorothy-mcdermott/
Margaret METCALFE https://www.judiciary.gov.uk/publications/margaret-metcalfe/
Gaenor MOORE https://www.judiciary.gov.uk/publications/margaret-metcalfe/
John MORRIS https://www.judiciary.gov.uk/publications/morris-2013-0295/
Wilhelmina NEWTON https://www.judiciary.gov.uk/publications/wilhelmina-isobel-newton/
Peter NOTT https://www.judiciary.gov.uk/publications/peter-norman-nott/
Peter PATTINSON https://www.judiciary.gov.uk/publications/peter-pattinson/
Marjorie PHILLIPS https://www.judiciary.gov.uk/publications/marjorie-phillips/
Alois PISKA https://www.judiciary.gov.uk/publications/alois-piska/
Noreen PORTER https://www.judiciary.gov.uk/publications/alois-piska/
Walter POWLEY https://www.judiciary.gov.uk/publications/walter-gordon-powley
Marie QUINN https://www.judiciary.gov.uk/publications/marie-quinn/
Elsie RAPER https://www.judiciary.gov.uk/publications/elsie-raper/
Derrick RIVERS https://www.judiciary.gov.uk/publications/derrick-rivers/
James ROBERTSON https://www.judiciary.gov.uk/publications/james-robertson/
Lillian ROBINSON https://www.judiciary.gov.uk/publications/lillian-robinson/
Margaret ROGERSON https://www.judiciary.gov.uk/publications/margaret-rogerson/
Christopher ROYAL https://www.judiciary.gov.uk/publications/christopher-royal/
Maria SILKIN https://www.judiciary.gov.uk/publications/maria-silkin/
Gladys SMITH https://www.judiciary.gov.uk/publications/gladys-smith/
Vincent SMITH https://www.judiciary.gov.uk/publications/vincent-smith/
Edna SMITHER https://www.judiciary.gov.uk/publications/edna-smither/
Vera STEEL https://www.judiciary.gov.uk/publications/vera-lillian-steel/
James STEWART https://www.judiciary.gov.uk/publications/james-stewart/
Doris TAYLOR https://www.judiciary.gov.uk/publications/doris-taylor/
Pamela THURSTON https://www.judiciary.gov.uk/publications/pamela-thurston/
William TOLEN https://www.judiciary.gov.uk/publications/william-tolen/
John TUGWELL https://www.judiciary.gov.uk/publications/tugwell-2013-0319/
Mary WALDRON https://www.judiciary.gov.uk/publications/mary-waldron/
Stanley WARD https://www.judiciary.gov.uk/publications/stanley-ward/
Walter WILLOWS https://www.judiciary.gov.uk/publications/walter-willows/
Olive WILMOTT https://www.judiciary.gov.uk/publications/clive-wilmott/
Marjorie WOOD https://www.judiciary.gov.uk/publications/marjorie-wood/