
| Please sign and share:
Petition to replace weak UK whistleblowing law to protect whistleblowers and the public |
By Dr Minh Alexander NHS whistleblower and former consultant psychiatrist 25 August 2020
The CQC has shamed itself deeply once more in its failure to raise the alarm quickly enough on COVID-19 deaths of highly vulnerable people in residential care or who receive care in their own homes from domiciliary care services.
CQC is by law notified of the deaths of all users receiving care from regulated providers:
CQC Regulation 16: Notification of death of service user
CQC should have proactively anticipated the risks posed by the pandemic to vulnerable people and raised the alarm about any failures to protect them from COVID-19.
CQC certainly received a much elevated number of Safeguarding concerns from care workers during the pandemic (2,043 Safeguarding referrals by care workers to the CQC 1 March -21 May 2020 compared to 1,230 in the prior year period).
Instead, it took CQC months after the World Health Organisation warnings of COVID-19 threat to even ask care home and domiciliary care providers to report whether COVID-19 was a factor in service user deaths – the regulator only did so on 9 April 2020, and the reporting obligation has only been in force since 10 April 2020.
There has been a great deal of media coverage on the COVID-19 devastation in our care homes resulting from gross UK government negligence, its much damned herd immunity strategy, and its lies that it threw a protective ring around care homes.
There has been less coverage of the failure to protect domiciliary care service users, even though peripatetic care staff pose an obvious virus transmission risk.
I asked the CQC to provide statistics on COVID-19 deaths of people who receive care at home, and evidence that the CQC is actively tracking and learning from these events.
A delayed FOI response has been issued which reveals that as of 20 August 2020:
- There have been 892 confirmed or suspected COVID-19 service user deaths
- 474 domiciliary care providers had notified CQC of at least one confirmed or suspected COVID-19 death
- Some care providers did not report any such deaths
- One care provider reported 17 confirmed or suspected COVID-19 service user deaths, which is the highest number
Of great concern, the CQC has not produced actual written evidence of analysis of trends and lessons learned. It only says that it is working with ONS.
The regulator cannot or will not even say if any domiciliary care service users died or may have died of COVID-19 as a result transmission from care workers.
The FOI response is reproduced below in the appendix.
I will pass the information to parliament to feed into both scrutiny of the government’s response to the COVID-19 crisis and the CQC’s regular accountability hearings with the Health and Social Care Committee and the Public Accounts Committee.
The CQC is an example of UK regulatory capture and failure to properly champion the public interest, or importantly, to defend the rights of vulnerable people.
It continues to ignore and silence whistleblowers, including its own whistleblowers, with impunity partly because UK whistleblowing law is so weak.
Please sign the petition and share to call for law reform to make UK whistleblowing law fit for purpose and to serve the interests of the public and not the powerful.
Thank you
| Please sign and share:
Petition to replace weak UK whistleblowing law to protect whistleblowers and the public |
UPDATE 27 AUGUST 2020
The Healthcare Safety Investigation Branch has today published an intelligence report which reveals that it was informed of a case of a vulnerable service user being fatally infected with COVID-19 by domiciliary care workers who did not wear PPE during the pandemic:

This raises very serious questions about CQC’s above claim in its FOI response that it held no data on transmission from domiciliary care workers to vulnerable clients.
HSIB and CQC have a memorandum of understanding which includes sharing risk and safeguarding information. It is very hard to believe that information was not shared on the above issues.
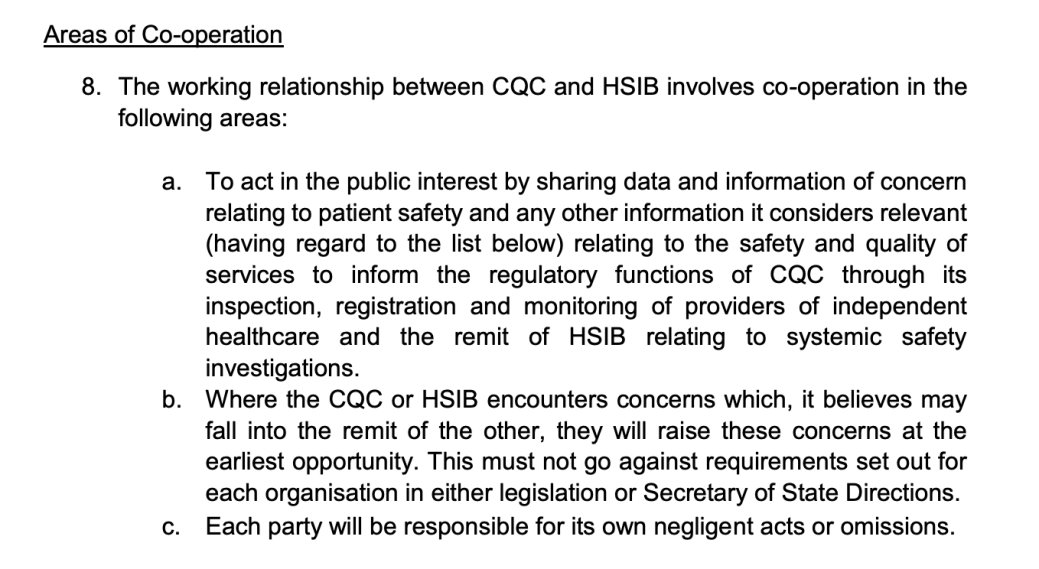
However, if there was a failure to share information, that too would be very serious.
I will pursue more answers from HSIB and CQC.
APPENDIX
CQC FOI response
From: Information Access <REDACTED>
Subject: CQC IAT 2021 0126
Date: 25 August 2020 at 11:21:16 BST
To: Minh Alexander <REDACTED>
Dear Dr Alexander
Our Ref: CQC IAT 2021 0126
I write in response to your request under the Freedom of Information Act 2000 (FOIA) of 3 July 2020. I apologise again for the delay in this response.
You asked:
- What data does CQC hold on COVID-19 deaths of service users who receive domiciliary care services (home care)?
Does CQC collate such data on a database/ spreadsheet? If so, what data fields does CQC operate on this database/spreadsheet (column and row titles)?
Regulation 16 of the Care Quality Commission (Registration) Regulations 2009 requires that care providers must notify CQC of the death of a service user.
You can access the notification form on our website at:
We are able to run reports from the information we receive in the notifications, however we don’t have a standing spreadsheet containing the information at any one time. We would however be able to pull a report to collate the specific data on numbers of notifications that we required for a particular purpose.
Providers are only required under the regulation to submit a notification to CQC where:
- the person died while a regulated activity was being provided
- their death may have been a result of the regulated activity or how it was provided
Therefore CQC will not be notified of all deaths of people who use domiciliary care services.
2/ The total number of COVID-19 deaths of service users who receive domiciliary care services that have been notified to CQC since the start of the pandemic
Since 10 April 2020, providers submitting notifications under regulation 16 have been required to state whether the death was confirmed or suspected as being a result of coronavirus.
On 3 July, the ONS published data on deaths of recipients of domiciliary care in England. See section 8 of this report –
This report is based upon regulation 16 notifications received by CQC between 10 April and 19 June. As of that date, 819 deaths of people who use domiciliary care service had been reported to CQC as being confirmed or suspected to have resulted from coronavirus.
Since that data was published, we have been reviewing how we register hospices which provide community services (to support people with end-of-life care in their own homes). This work is ongoing but three of these services are no longer reported as domiciliary care services in the figures provided in this response.
As of 20 August, 892 deaths of people who use domiciliary care services had been notified by providers to CQC as being confirmed or suspected to have resulted from coronavirus.
3/ The total number of domiciliary care providers who have reported COVID-19 deaths of service users to CQC since the start of the pandemic
As of 20 August, 474 domiciliary care providers had notified CQC of at least one death that they recorded as being either confirmed or suspected of resulting from coronavirus.
4/ The lowest and the highest number of COVID-19 deaths of service users notified to CQC by individual domiciliary care providers since the start of the pandemic (ie. the range in number of COVID-19 deaths reported by domiciliary care providers)
As of 20 August, the lowest number of notifications received from any individual domiciliary care services is 0.
308 providers had each notified CQC of a single death.
The highest number (other than for a hospice that provides community services) is 17. This figure relates to a provider that has a number of services (locations) in different areas. The highest number for a single service is 8.
The majority of deaths reported by domiciliary care services as being related to Covid-19 occurred in hospital.
5/ Has CQC reviewed the pattern of notified COVID-19 deaths of service users who receive domiciliary care?
If so, please share a copy of any related report and or findings
CQC has supported ONS in publication of the report linked above. We are monitoring notification data on an ongoing basis and are working with provider organisations and with other organisations to understand the data. CQC has not produced findings or a report.
6/ What evidence does CQC hold on actual or potential COVID-19 transmission by domiciliary care workers to vulnerable service users?
7/ Please advice in summary of the number of confirmed or suspected instances of transmission of COVID-19 by domicilary care staff to domiciliary care service users, of which CQC is aware
CQC does not hold the information requested in questions 6 and 7.
Kind regards
Information Access Team
Governance and Legal Services
Customer & Corporate Services Directorate
Care Quality Commission
RELATED ITEMS:
A new UK whistleblowing Bill and a petition to the UK government to strengthen protection
Replacing the Public Interest Disclosure Act (PIDA)
Two years of national CQC whistleblowing data on health and social care services
Prescribed Persons or the Pretence of PIDA. How UK whistleblowers are ignored


Just a very brief but sincere thank you for continuing to scrutinise and record the indifference that the great and the good have to their duties.
I think the world has always been wicked but, it is sobering to see it so vividly portrayed.
Thank you and wishing you well.
LikeLike
Reblogged this on | truthaholics.
LikeLike
So the CQC received 813 more safeguarding concerns from care home whistle blowers as the prescribed person in the pandemic than they did at the same time last year. It appears sat on their hands and did nothing other than perhaps issue a standard response to these care workers.
I’m guessing, based on previous experience, that standard response will be along the lines of we do not deal with safeguarding concerns and/or we have noted the information for future inspections.
The post evidences they have also failed miserably in the area of home care in capturing any meaningful data which could have highlighted the problems in that sector as well.
Makes you wonder what purpose they actually serve as a care regulator and prescribed person and how they continue to exist?
LikeLike