By Dr Minh Alexander NHS whistleblower and former consultant psychiatrist 10 August 2018
Summary: I have been asked to comment on HSIB investigations. HSIB is purportedly based on aviation models of accident investigation and has been parachuted into the NHS, but there are very considerable difficulties in attempting a straight translation. Healthcare is a much, much more complex, human endeavour. There are many more actors, a greater range of tasks, greater relational complexity, including different ethical, regulatory and political contexts. HSIB has also been under the Department Health thumb in the early stages of its establishment, with the embedment of a DH deputy director as its director of corporate affairs, who was in charge of comms.
I have looked at HSIB’s second published investigation report, on a mental health case as this is territory with which I most familiar. I concentrate on HSIB’s silence about failures to deliver a central plank of government mental health policy for almost thirty years – the Care Programme Approach (CPA). A young person died in the transition between two services. HSIB spins a line that CQC haplessly lacked a mechanism for regulating such transitions. In truth, since CQC’s inception its regulations and protocols have required it to inspect the interface between services and providers, and to ensure safe transitions. CQC has repeatedly reaffirmed these principles. The question is why policy failed. The government short changed the public and oppressed the mental health workforce by superficially standing by quality standards such as CPA, but not giving the NHS the resources to properly implement them. If HSIB is truly independent, it should be highlighting these issues more robustly.
The Care Programme Approach
In the NHS, CPA was introduced into mental health services in 1990 after an asylum closure programme to ensure that de-institutionalisation did not result in neglect in the community:
Continuing high profile failures of care in the community of people with serious mental illness, and a string of inquiries into serious incidents, avoidable deaths and homicides by mentally unwell people emphasised the need for joined up mental health care. The disturbing images of Ben Silcock in the lions’ pen at London Zoo on New Year’s Eve 1992 where he was gravely mauled, the revelations of his serious mental illness and the fact that he had been turned down for hospital admission prior to the incident, prompted a public outcry.
As did the unprovoked, fatal attack by Christopher Clunis on Jonathan Zito, a complete stranger, at Finsbury Park Tube station in December 1992. An inquiry revealed that Clunis passed through several mental health services before the killing, with missed opportunities to care for him and to protect the public. Clunis later sued his Health Authority for neglect.
CPA has been revised several times. Some mental health staff perceived its structure as an imposition. There have also been controversies around later attempts to tier and then restrict CPA to the most complex cases. Confusion persists about who should be cared for under CPA:
|
The CQC has acknowledged in its statistical releases that the proportion of patients on CPA varies greatly between trusts. For example: 2015: “…it is worth noting that there is enormous variation in the proportion of people on CPA between trusts: for respondents to the 2015 survey this ranged from 10% to 61%, which suggests that there are systematic differences in how trusts interpret and apply the CPA policy locally.” 2017: “…it is worth noting that there is a large variation in the proportion of people on the CPA between trusts, which suggests that there are systematic differences in how trusts individually interpret and apply the CPA policy.”
|
In general terms, CPA applies to patients with the most complex needs and risks. It is possible that more patients would be assigned to CPA if mental health services were under less resource pressure.
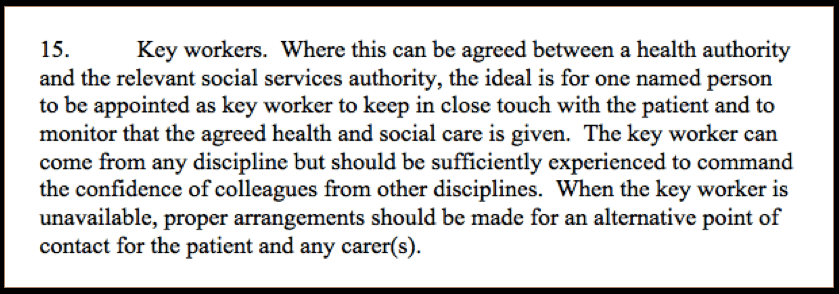
CPA is just common sense and a formalisation of good practice. It seeks to prevent blind spots in care planning and risk assessment by providing a comprehensive framework under which such activities take place. CPA provides for a key role – that of the key worker or ‘care coordinator’ whose job it is to drive the care plan and ensure that it is properly carried out, and that all of the patient’s needs are met:
 Health Service Circular/Local Authority Circular HC(90)23/ LASSL(90)11
Health Service Circular/Local Authority Circular HC(90)23/ LASSL(90)11
Crucially, CPA also serves to ensure safe handovers within and between teams and services, because poor communication and badly managed transitions lie behind many serious mental health failures. Lost information and risk assessments based on incomplete information, or risk assessments made without due multi-disciplinary process or senior oversight are classic factors in serious mental health incidents.
Importantly, CPA seeks to ensure that the patient, family and or carer voice is heard by giving a structured means of consulting and recording their views, and providing them with a transparent, written record of therapeutic commitments by the treating service.
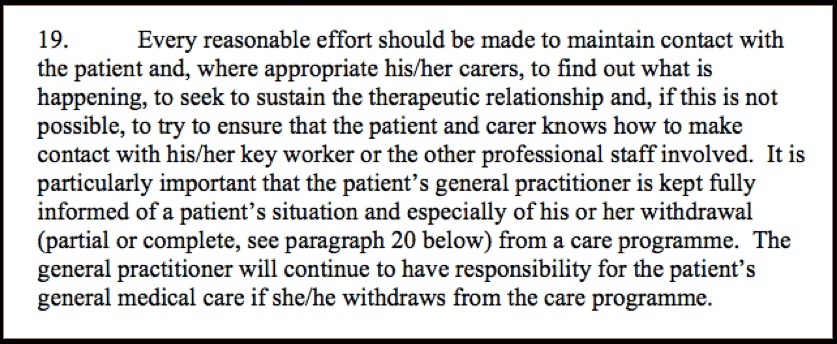
CPA emphasised the great importance of the therapeutic relationship and of not letting people fall through the safety net:
 Health Service Circular/Local Authority Circular HC(90)23/ LASSL(90)11
Health Service Circular/Local Authority Circular HC(90)23/ LASSL(90)11
In short, CPA was intended to be a failsafe that ensured thorough, supportive, patient-centred and safe care.
It follows that breaches of CPA may put basic care standards at risk. Inquiries, coroners’ warning reports and independent mental health homicide reports commissioned by Health Authorities, Strategic Health Authorities and NHS England have repeatedly cited care planning/ CPA failures as contributory factors.
For example, this coroner’s report to Prevent Future Deaths (PFD) was recently sent to Jeremy Hunt, about the death of Robin Richards who was on CPA but in whose case there were a number of care planning and communication breakdowns:
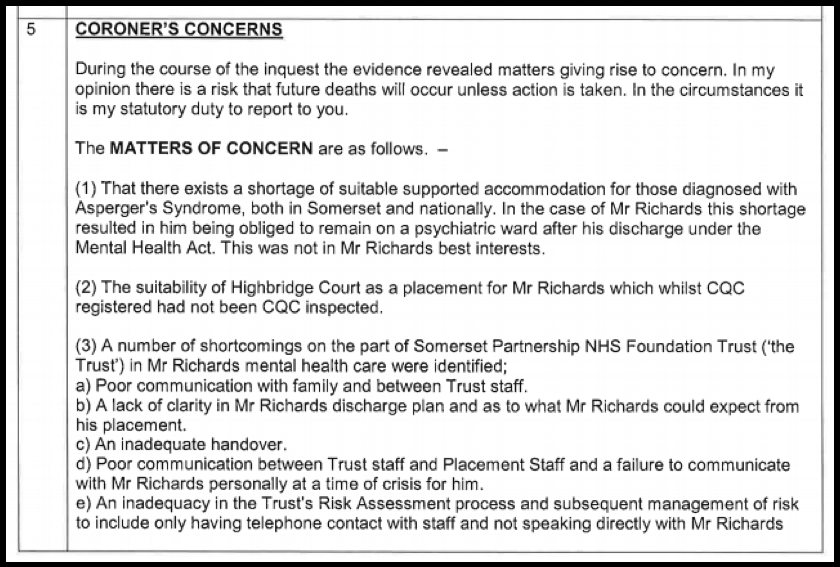
This PFD was issued on 25 May 2018 and there is still no published response by the Department of Health and Social Care.
Under the strain of austerity and de-funding, immense service pressures make it harder for mental health services to meet CPA standards or to meet them well. Care coordinators may not be replaced when they leave or go off sick , or patients may be passed repeatedly between care coordinators, resulting in an impersonal experience with loss of continuity.
Proactive crisis planning is a core part of CPA, and relies on staff who understand early warning signs. This clearly works better when there is a relationship and staff know the patient, as opposed to someone walking in on a crisis and checking off a list. Patients are also more likely to be comforted by and work more easily with staff whom they trust, than a relative stranger.
Under the pressure of staffing shortages and de-funding, the care coordinator role may be delegated to inappropriately inexperienced and inadequately supervised staff. Care planning may also be dictated by service pressures instead of led by patients’ needs. Serious shortages in mental health beds result in premature, chaotic discharges and sometimes emergency re-admissions in short succession. The CPA process may be reduced to hurried, tokenistic form filling or alternatively it runs behind playing catch up, when it should be a meaningful, proactive process.
It is also possible to have perfect CPA paperwork but awful care that is based on poor assessment and is badly prescribed.
The signs of extreme pressure on mental health services have been writ large for some time, but CQC has not revealed the full extent of the failures. CQC rates most mental health trusts as “Good’ or ‘Outstanding’:
“As at 31 May 2017, we had rated 68% of NHS core services as good and 6% as outstanding.”
This is despite systemic failures across the board to meet patients’ needs, as evidenced for example by daily placement of NHS patients in private sector beds sometimes hundreds of miles from home, because the NHS does not have enough beds of its own.
HSIB’s investigation on ‘The Transition from Child and Adolescent Mental Health Services to Adult Mental Health Services’
The Healthcare Safety Investigation Branch’s second investigation report of July 2018 into the unsafe interface between child and adolescent mental health services (CAMHS) and adult mental health services (ADMHS) leaves much unsaid.
It focuses on the case of Ben. These are the salient facts of his case according to HSIB:
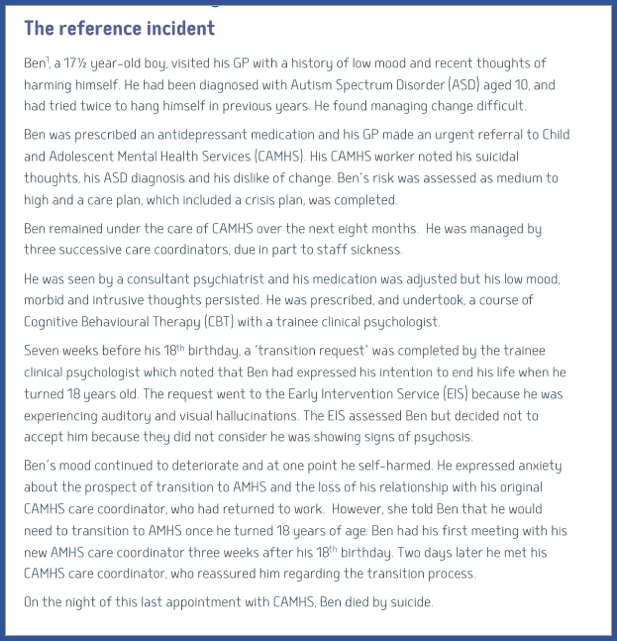
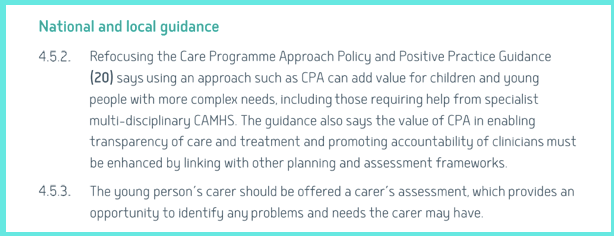
HSIB’s report did not fully map Ben’s care against accepted CPA standards and national guidance, but it identified that no CPA meeting had taken place in the months that Ben was nominally subject to CPA, that no carer’s assessment had been offered when this was indicated and that there were failings in risk assessment and management.
Almost 30 years after CPA was introduced, HSIB could have said a lot more about the significance of any failure of CPA process. Why are there still frequent failures in this core process for people with serious conditions, that is supposed to ensure safe care? What have the government and NHS regulators been doing in response to the inquiries, coroners’ warnings and mental health homicide investigation reports that have flagged failures in CPA process?
In 2008 the government indicated that it expected NHS regulators to police CPA. CQC’s predecessor the Healthcare Commission examined CPA and in March 2009 concluded:
‘However, marked variations between trusts remain and the national averages against which they are compared are relatively low, suggesting that some trusts have been far more successful than others in ensuring that the infrastructure for the CPA is embedded within routine practice.”
CQC took over from HCC in April 2009. What has CQC done since about patchy CPA implementation, including precarious CAMHS to AMHS handovers? If CQC had been regulating CPA effectively, this would have encompassed the transition between CAMHS and AMHS, because safe handover is exactly what CPA was designed to govern.
For decades now, data on CPA compliance has been centrally collated. A critical transition is that between hospital and community. This has been linked time and again to suicides. It remains unreliable. National policy is that patients should be seen within 7 days of discharge from hospital but some still slip through. The data showing the breaches is routinely published by NHS digital. In the last quarter of 2017/18, , ‘Outstanding’ East London NHS Foundation Trust had the second worst rates of 7 day follow up: only 1006 out of 1154 (87.2%). Leicestershire Partnership NHS Trust had the lowest 7 day follow up rate, at 68.8%.
Year in, year out CQC has received intelligence from patients via the annual (adult) community mental health survey of poor experiences of care planning, crisis planning and of being insufficiently involved by services in devising their own care.
Patients’ response rates to the CQC’s annual community mental health surveys have been low and are falling:
| CQC annual community mental health survey of patients receiving specialist care | Response rate to survey |
| 2012 | 32% |
| 2013 | 29% |
| 2014 | 29% |
| 2015 | 29% |
| 2016 | 29% |
| 2017 | 26% |
Source: CQC annual community mental health surveys
It is possible that the results would be worse if data from patients who did not respond was included. Interpretation of survey results is hampered by a change in methodology in 2014, which limits comparability with earlier results. Comparability is also limited by inconsistency in CQC’s presentation of results.
Nevertheless, the surveys have suggested that patients do not reliably receive a care plan or that a care plan is consistently agreed, even when some are deemed ill and disabled enough to require CPA:
| Year of CQC community mental health survey | Question 27 Have you been given (or offered) a written or printed copy of your NHS care plan? |
| 2012 | 24% patients on CPA replied ‘No’ |
| 2013 | 24% patients on CPA replied ‘No’ |
| Question 12 Have you agreed with someone from NHS mental health services what care you will receive? | |
| 2014 | 23% of all patients replied ‘No’* |
| 2015 | 15% of patients on CPA replied ‘No’ |
| 2016 | 14% of patients on CPA replied ‘No’ |
| 2017 | 24% of all patients replied ‘No’* |
*Specific statistics for patients on CPA not available
The surveys have suggested that crisis care planning has not been reliable enough, even though this is vital to risk management. Recent figures suggest that about a fifth of patients on CPA do not know how to seek help in a crisis:
| Year of CQC community mental health survey | Question 26 Does your NHS care plan cover what you should do if you have a crisis (e.g. if you are not coping or if you may need to be admitted to a mental health ward)? |
| 2012 | 14% patients on CPA replied ‘No’ |
| 2013 | 14% patients on CPA replied ‘No’ |
| Question 21: Do you know who to contact out of office hours if you have a crisis? | |
| 2014 | 32% of all patients replied ‘No’* |
| 2015 | 19% of patients on CPA replied ‘No’ |
| 2016 | 20% of patients on CPA replied ‘No’ |
| 2017 | 29% of all patients replied ‘No’* |
*Specific statistics for patients on CPA not available
The survey has also suggested that some patients’ care plans are infrequently reviewed, even when they are considered to have serious enough needs to merit being placed on CPA:
| Year of CQC community mental health survey | Question 28 In the last 12 months have you had a care review meeting to discuss your care? |
| 2012 | 24% patients on CPA replied ‘No’ |
| 2013 | 26% patients on CPA replied ‘No’ |
| Q14: In the last 12 months have you had a formal meeting with someone from NHS mental health services to discuss how your care is working? | |
| 2014 | 26% of all patients replied ‘No’* |
| 2015 | 17% of patients on CPA replied ‘No’ |
| 2016 | 18% of patients on CPA replied ‘No’ |
| 2017 | 26% of all patients replied ‘No’* |
*Specific statistics for patients on CPA not available
NHS England acknowledged some of these core failures in its 2016 Five Year Forward report:
“Almost one-fifth of people with care coordinated through the Care Programme Approach (for people with more severe or complex needs) have not had a formal meeting to review their care in the previous 12 months.”
HSIB’s report did not mention these wider, persisting problems in national CPA delivery, nor did it explore what action CQC had taken in response to this.
HSIB’s report made no reference to specific provision for handover between CAMHS and AMHS that appeared in national Department of Health CPA guidance from 2008:
| “Child and Adolescent Mental Health Services
The importance of having a system similar to CPA for children and young people with mental health needs is increasingly recognised. In the Report on the Implementation of Standard 9 of the National Service Framework for Children, Young People and Maternity Services, 68 in delivering good practice for young people it is noted that “The Care Programme Approach, modified to meet the needs of younger people, is used to plan transition, and transition is supported by agreed protocols.” A similar point is made in Standard 9 of the NSF for Children, Young People and Maternity Services, namely “When children and young people are discharged from in-patient services into the community and when young people are transferred from child to adult services, their continuity of care is ensured by use of the care programme approach.” However, it is important that where CPA is considered relevant for children and young people it is tailored to their requirements. Guidance on how this can be achieved is set out at Annex B.” This Annex B is found on page 45 of the DH 2008 guidance and provides guidance on the special needs of children and young people when care planning. It specifically addresses: – A need for more frequent review than in adult cases – Very careful coordination between professionals and agencies – The particular need to involve families and carers given the developmental stage of children and young people – A need for age appropriate communication and documentation, and special support to participate in care planning |
HSIB only summarises the 2008 DH guidance very briefly thus:
CQC actually acknowledged that there was unsafe practice around transition from children’s to adult health services in a specific 2014 report. This focussed largely on physical health services but touched on mental health services as well. The question was what happened next.
Instead of confronting the question of CQC’s and other central bodies’ oversight of existing CAMHS-AMHS transition policy, HSIB proffered this wriggly explanation for CQC’s failure to get a grip of CAMHS-AMHS handover issues:

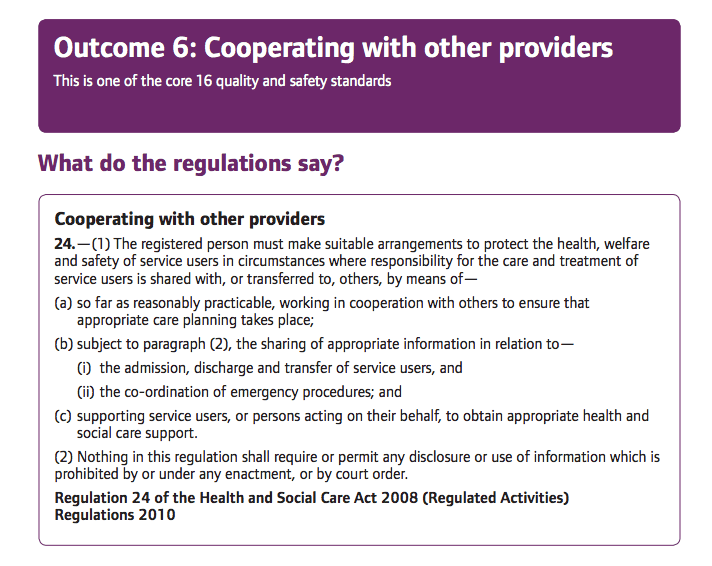
This is a bizarre claim by HSIB. Since CQC’s inception, the regulations underpinning its operations have included a requirement for it to regulate co-operation between providers and transfer of service users between providers as part of assessing service safety:
HSIB’s report also omitted to mention that in 2013, CQC issued a framework for inspecting mental health services which specifically emphasised the importance of safely managed transitions between services and providers:
| “A fresh start for the regulation and inspection of mental health services Working together to change how we regulate, inspect, and monitor specialist mental health services
· Focus on transitions, care pathways and joint working, including where people move between services and where care is provided in an integrated way. Transitions between services will include moving between services within the provider – such as between children and young people’s and adult services or between adult and older adult services – as well as between providers – such as the transition between primary and secondary care or between independent sector and NHS services. · For the providers we regulate, this will mean looking at the timeliness of responses and the way they work with other providers to achieve positive outcomes for people who use services. This includes integrated working to address physical as well as mental health needs; to promote recovery, health and wellbeing; to prevent or respond appropriately to crisis; and to achieve quality of life, including in relation to housing, employment and social participation.”
|
HSIB omitted to mention that in 2015, CQC issued guidance to providers on meeting regulations which reaffirmed the need for safe transitions:
|
“12(2)(i) where responsibility for the care and treatment of service users is shared with, or transferred to, other persons, working with such other persons, service users and other appropriate persons to ensure that timely care planning takes place to ensure the health, safety and welfare of the service users.”
|
HSIB did not mention that in 2017 CQC issued an inspection framework for children and young people which repeatedly specifies assessment of transitions between services. There are plenty of other CQC publications from all the years since CQC’s inception in 2009 which make it clear that CQC has been aware of its duty to inspect the critical care pathway changes between services and providers. For example, CQC’s monitoring reports on the use of the Mental Health Act frequently examine high risks aspects of transfer between services. It would have taken a miracle for HSIB to have missed them all.
And if HSIB had examined CQC inspection reports – and I make no assumptions about whether HSIB did or not – it would have found that CQC does at least occasionally inspect transitions. The difficulty is that CQC does not provide evidence that it does so reliably. A quick and dirty check of the most recent CQC inspection reports on mental health trusts by searching under the term ‘transition’ reveals that CQC commented on service interfaces in only 21 out of 54 of the inspection reports, and in 14 of these instances this was in the context of CAMHS services.
Strikingly, HSIB’s report does not actually describe what regulatory action CQC took at the trust where Ben died, in contrast to its detailed description of clinicians’ actions. That does not seem the even handed, fearless approach that we were promised.
But maintaining the artifice, HSIB recommended:

So in short, a face saving exercise and a slight slap on the wrist for CQC which allows HSIB to claim that it is holding even regulators to account.
And as for HSIB’s claim that it will investigate if problems are widespread and systemic, why is HSIB’s investigation report silent on the full extent of CPA failures in mental health services?
HSIB confines itself to the CAMHS-AMHS interface, whilst reinventing the CPA wheel:
This HSIB recommendation appears to be little more than the final step in a highly choreographed dance. CQC had already tidied up the loose ends some months ago in two new publications. One was a thematic review report in March 2018 waxing lyrical about the importance of person-centred care planning and describing the poor transition between CAMHS and AHMS.
The other publication was a March 2018 specific guide for CQC inspectors on how to inspect the CAMHS-AMHS transition:
| “Evidence required
1. Providers have to provide the following information to their commissioners: a) A case note audit to assess the extent of Joint-Agency Transition Planning b) A survey of young people’s transition experiences ahead of the point of transition (Pre-Transition / Discharge Readiness); c) A survey of young people’s transition experiences after the point of transition (Post-Transition Experience) 2. The CQUIN also specifies a transition meeting, which should include: a) The young person; b) The appropriate key worker from the sending service; c) Where applicable, a dedicated point of contact for transition from the receiving service; and d) Where appropriate and the young person agrees, the young person’s parent(s) /carer(s). Ask young people and staff about whether these meetings occurred and their experiences of the meetings 3. Review case notes of young people transitioning to adult services or about to leave CAMHS.” |
HSIB’s report states theatrically that HSIB has ‘directed’ its recommendation to CQC and that CQC must respond in 90 days. But it is patently obvious that the next dance step will be the usual heart-warming reassurance that CQC has already acted to safeguard patients etc etc..
HSIB additionally makes the recommendation that NHS England should ensure that money earmarked for CAMHS is spent as intended. HSIB also makes a rather timorous ‘observation’ rather than a recommendation, that it would be ‘beneficial’ if NHS England identifies CCGs that spend less on CAMHS than ‘expected’.
HSIB supports NHS England’s incentivisation of safe handover process between CAMHS and AMHS with the use of Commissioning for Quality and Innovation (CQUIN) targets. These may be self-defeating if the fundamental problem is that trusts are not given enough money for basic operations and that is the reason for unsafe practices
HSIB seeks to manage disparities between CAMHS and AMHS by proposing that younger people should be able to remain within CAMHS up to the age of 25 if necessary instead of 18, citing long waiting lists and steep eligibility criteria in AHMS as part of the case for this proposal.
For anyone who knows anything about the relative length of CAMHS waiting lists compared to AMHS waiting lists, HSIB’s observations about AMHS waiting lists are perplexing.
It is of course common sense that there should be needs-led flexibility at service interfaces, particularly if this is needed for management of serious risk.
However, the more muscular recommendation that HSIB could have made was that the government should provide all mental health services with the necessary funds to implement the government’s policies and the quality standards that the government says it expects for mental health services, such as safe care planning under CPA. But that would be calling the government’s bluff.
So far, HSIB looks less like the professional investigator that we were promised, and more like another, expensive go-faster stripe on the denial machine.
The element of trust is crucial given all the very serious concerns about abuse of the ‘safe space’ provision in the legislation that will govern HSIB’s operations.
The last word belongs to those most deeply affected, but it is not clear what Ben’s family think of the system response. HSIB offered to meet with Ben’s parent but at the time of publication, it reported that the offer had not been accepted.
RELATED ITEMS
Safe in their hands? Government’s response coroners’ warnings about the NHS


Your points are well made.
LikeLike