Dr Minh Alexander retired consultant psychiatrist 29 June 2023
Summary: The Department of Health and Social Care has confirmed that its plans to set up a Special Health Authority to investigate maternity failures in the NHS are dead and buried, with no plans to resurrect. This is despite an abortive attempt to recruit a Chair for the Special Health Authority which concluded with fourteen applicants being turned away. It refuses to disclose its justification for transferring the maternity investigation programme to the Care Quality Commission or the legislation drafted for the now binned Maternity and Newborn Safety Investigation Authority.
Background
Jeremy Hunt former Health Secretary’s unwieldy vanity project the national maternity investigation programme was foisted on the Healthcare Safety Investigation Branch against advice.
It unravelled in secrecy as whistleblowers spoke out against poor management and inherent systemic problems, such as designed-in conflicts of interest from seconded staff feeling pressured to keep on good terms with the regional teams they investigated, for the sake of their long term career prospects.
NHS England and its predecessors tried to suppress the scandal but to no avail as an HSIB whistleblower’s Employment Tribunal hearing in April this year revealed crucial evidence and an investigation by Channel 4 (broadcast 15 and 16 May 2023) brought forth yet more whistleblower evidence of defective maternity investigations and cultural failings at HSIB. Importantly, HSIB staff claimed that they had been threatened with job losses if they did not churn out investigations reports quickly enough, which affected quality.
Related to these troubles, several investigations were conducted but suppressed by NHS England. Firstly the Newton report was conducted into a HSIB whistleblower’s concerns of detriment and concluded that there had been poor whistleblowing governance.
A review of culture and leadership was then conducted by the Kings Fund upon the recommendation of the Newton report, which was overseen by NHS England and the Department of Health and Social Care. The Kings Fund produced a curiously fact lite report which nevertheless found leadership failures. It also commented on the harmful effect of uncertainty about the future of the maternity division of HSIB and advised that this be resolved.
The King’s Fund review was informed by an internal review of the maternity division, the Benson report, which revealed serious dysfunction. Dawn Benson the HSIB lead author went on to give evidence at the above HSIB’s whistleblower’s ET hearing and also gave an interview to Channel 4.
Keith Conradi the head of HSIB’s retirement was announced after the King’s Fund’s conclusions were shared with HSIB staff.
On 21 January 2022 the Health Service Journal reported the findings of the leaked King’s Fund report, which was the first time the report’s existence was revealed:
Bullying, sexism and racism ‘prevalent and tolerated’ at national regulator
On 26 January 2022 Sajid Javid made a statement in parliament announcing that the government would create a short life Special Health Authority to take over the maternity investigation function from HSIB. The idea was to eventually hand maternity investigations back to NHS trusts once an example of good practice had been purportedly modelled:
“Special Health Authority will be established for up to five years from 2022-23 to enable maximum learning to be achieved and to equip NHS Trusts with the expertise, resources, and capacity to take on maternity safety incident investigations in the future.”
The post of Chair for the special health authority was advertised in autumn 2022:
Advert for Chair of Maternity and Newborn Safety Investigation Authority 2 September 2022.
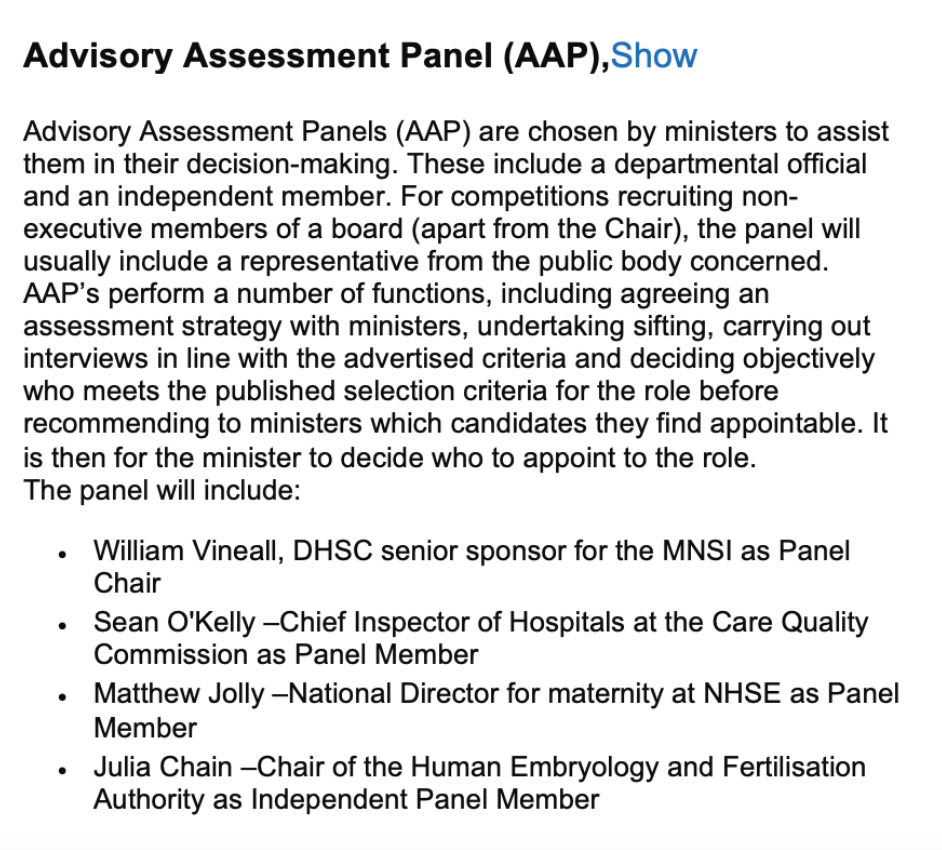
William Vineall and NHS regulators were represented on the advisory panel.
But on 30 March 2023, shortly before the HSIB whistleblower’s ET case was due to be heard, Maria Caulfield Parliamentary Under Secretary for Health and Social Care unexpectedly announced that the maternity investigation section of HSIB would be hosted by the Care Quality Commission:
“On 26 January 2022, Official Report, 25WS, by way of a written ministerial statement, the Department of Health and Social Care announced that a separate Special Health Authority would be established to continue the independent maternity investigation programme, which is currently overseen by the Healthcare Safety Investigation Branch.
The Department is committed to ensuring the continuation of independent, standardised maternity investigations that provide learning to the system and contribute to the Government’s ambition to halve the 2010 rates of stillbirths, neonatal and maternal deaths and brain injuries in babies occurring during or soon after birth by 2025.
Following careful consideration, the Department has determined that the most appropriate and streamlined mechanism for delivering the valued and independent maternity investigations is for the function to be hosted within the Care Quality Commission. The purposes of the maternity investigation programme remain as set out last January: to provide independent, standardised and family-focused investigations of maternity cases for families: to provide learning to the health system via reports at local, regional and national level; analyse data to identify key trends and provide system wide learning; be a system expert in standards for maternity investigations; and collaborate with system partners to escalate safety concerns.
We will now work with the CQC and the HSIB to complete the transition of the maternity investigation programme to the CQC by October 2023.
As announced in the written ministerial statement of 9 February 2023, Official Report, 40WS, the establishment of the new HSSIB will take place in October 2023, to enable all the necessary work to be completed to ensure a smooth transition of these investigation programmes.”
The Department of Health and Social Care’s termination of the Maternity and Newborn Safety Investigation Authority
To confirm whether this was a permanent arrangement and to find out more about the justification for locating maternity investigations within the notoriously politicised and none too competent CQC, I made an FOI request to the Department of Health and Social Care. This is the response:
The Department confirmed that it went ahead with its appointment process for a chair to the Special Health Authority, for which it received fourteen applicants:
“DHSC received 14 applications for the post of Chair/Chair designate to the Maternity and Newborn Safety Investigation Special Health Authority (MNSI).”
The government claims no appointment was made because:
“An appointment was not made, as a final decision on the appointment had not been reached before the announcement on the future of the MNSI [Maternity and Newborn Safety Investigation Authority] via a Written Ministerial Statement (WMS) on 30 March 2023.”
Well that’s a good way to do business. Advertise a job and then tell everyone “Hard cheese chaps, the job’s gone”.
The government also confirms that the Special Health Authority was never legally established.
It stands by its claims that the best option is hosting by CQC rather than a standalone Special Health Authority reporting directly to the Department of Health and Social Care:
“….following careful consideration, DHSC has determined that the most appropriate and streamlined mechanism for delivering the valued and independent maternity investigations is for the function to sit within and be hosted by the CQC.”
However, the government refuses to disclose its justification for this opinion on grounds that it might be embarrassed. Sorry, I mean on grounds of Section 35 FOIA formulation of government policy, because the transition period is not yet complete and policy is still being formulated.
The government has no plans to revisit the idea of a Special Health Authority.
This implies that the maternity investigation division will likely be allowed to wither on the vine for some as yet undetermined period until it all reverts to NHS trusts. This will do nothing for the independence of maternity investigations.
The government also refuses to disclose legislation drafted for the Special Health Authority on purported grounds that this is legally privileged.
One is left wondering what sort of governmental hissy fit led to such a major change of direction, and the bizarre Heath Robinson arrangement of the Care Quality but We Don’t Investigate Complaints Commission hosting a specialised incident investigation function.
It is left only to commiserate with the unfortunate maternity investigation staff who have been so badly managed and supported from the outset of a political misadventure.
RELATED ITEMS
Hunt’s chutzpah
Hunt skilfully dined politically off the Midstaffs and Morecambe Bay disasters whilst simultaneously wrecking the NHS, fashioning a narrative of hero crusader against the wicked NHS and recruiting a number of families to insulate himself.
He dined off Midstaffs whilst reneging on core recommendations from the public inquiry such as mandatory safe staffing and real whistleblower protection, which would have helped to prevent further maternity tragedies and any need for his disastrous national maternity investigation gimmick.
Even in 2020, Hunt was still trying to politically capitalise from maternity tragedies:
Jeremy Hunt calls for national inquiry into NHS maternity safety after repeated scandals
His handiwork on the NHS is now all around us as emergency care has collapsed, regularly causing deaths, cancer care is teetering and 7.4 million people await treatment.
And at the UK COVID public inquiry it has just been revealed that Hunt wanted to cut Public Health England’s funding by half:
Hunt wanted 50% cut to public health, says ex-PHE boss
Public health is one of the most crucial, effective and super-efficient medical specialties with profound effects on improving the health of the populace. Why would anyone except the utterly incompetent or those with malign intentions wish to cut it?
HSIB whistleblowers and the Secret King’s Fund Fact Lite report
More secret HSIB reports and failures of HSIB maternity investigations
Why is CQC not investigating UHB under CQC Regulation 12?
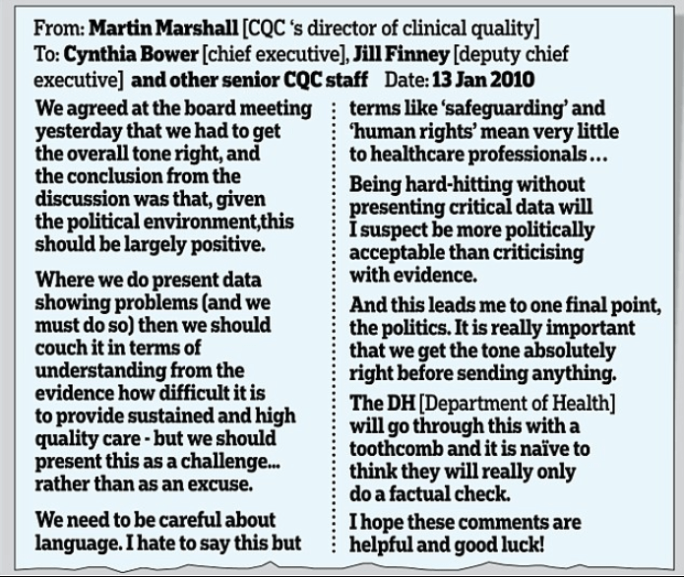
I leave readers who are less familiar with CQC’s ways with this FOI revelation about how CQC senior managers huddled and deliberated on the best way to manipulate public into thinking that they had written a “hard hitting” inspection report, but with as few facts as possible: