Dr Minh Alexander retired consultant psychiatrist 22 June 2023
The letter below, sent today to the parliamentary Justice Committee, is hopefully self-explanatory.
BY EMAIL
Sir Robert Neill MP and colleagues
Justice Select Committee
22 June 2023
Dear Sir Robert and colleagues,
Processes for reviewing and assuring the fitness of senior officers of the Criminal Cases Review Commission
I write to raise a concern about procedures for reviewing the fitness of senior officers of the Criminal Cases Review Commission (CCRC).
I raised a concern with Helen Pitcher Chair of CCRC about the suitability of the CCRC CEO arising from actions and omissions in her ongoing capacity as a non executive board member of University Hospitals Birmingham NHS Foundation Trust (UHB).
The trust has been undergoing multiple investigations following concerns of poor governance, whistleblower victimisation, a “toxic” culture with reported “cronyism” and patient safety failings.
In particular, I was concerned about the UHB trust board’s actions in ratifying an internal Fit and Proper Person investigation of the former UHB trust Chief Executive. The investigation was launched after he was criticised by the Employment Tribunal for conduct towards a senior medical whistleblower, and related referrals were made to the Care Quality Commission by several external parties, myself included, under CQC Regulation 5 Fit and Proper Persons.
The Employment Tribunal’s criticism included the fact that the former UHB CEO made a misleading referral to the General Medical Council in which he omitted to declare as required, that the whistleblower was a whistleblower. For this he later received a formal warning from the General Medical Council, as a registered medical practitioner himself.
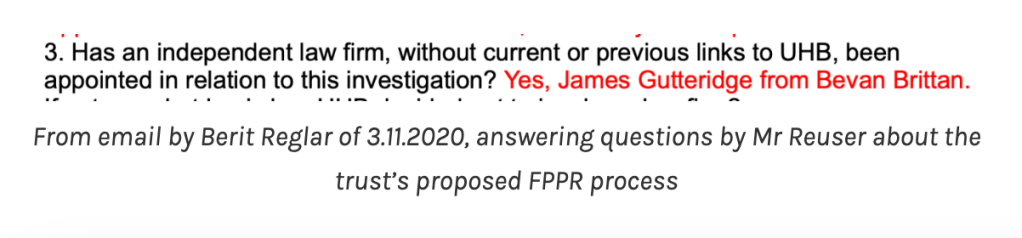
The subsequent UHB trust internal Fit and Proper Person investigation which reportedly exonerated the trust CEO (it has never been published or even shared with the whistleblower) was undertaken by a subordinate trust manager who was not a board member, assisted by a lawyer from a firm retained by the trust, which had been paid £497K for other services in the three previous years. It could not be described as an independent investigation and a probity issue arises from the fact that a subordinate employee was put in this position.
This was compounded by the fact that UHB misled the whistleblower and informed him wrongly in correspondence that the assisting law firm was independent and without current or previous links to the trust.
There were a number of procedural irregularities in the manner in which the whistleblower had been disciplined, suspended and dismissed by the trust, which were criticised by the Employment Tribunal. These breached a principle that NHS doctors should be disciplined with regards to Article 6 rights.
Documents were repeatedly withheld from the whistleblower and from the Employment Tribunal, which had the effect of concealing the fact that he was suspended on a false premise, which the Employment Tribunal determined the former UHB CEO should have known was false. The Employment Tribunal judge indicated in a costs judgment against the trust that he could not rule out “deliberate dishonesty” by the trust and key players, or that there would not be future serious governance failures of this sort.
The CRCC CEO had sight of the trust’s internal Fit and Proper Person Investigation report exonerating the former UHB CEO. She is on record as having reassured the trust governors that the investigation was sound. The minutes state at a UHB Council of Governors’ meeting on 29 July 2021:
“Karen Kneller also wished to provide reassurance to the Governors that the NEDs are particularly enquiring and have examined the situation thoroughly to their satisfaction and all are happy with the review.”
Although I am informed by an individual who actually witnessed the meeting that their recollection is that she stated there was “no smoking gun”.
The former CEO of UHB announced his retirement on the day that the first investigation report on the trust was published, on 28 March 2023.
Helen Pitcher also received information about the understandably serious impact of events on the whistleblower.
The issue I wish to raise with Justice Select Committee is this:
Helen Pitcher initially informed me via her Office on 14 April 2023 that she would consider my concerns and respond within twenty eight days.
On 18 May 2023 Ms Pitcher’s Office informed me that enquiries continued and that there was no date for completion.
On 2 June 2023, after an enquiry, the same message was given again.
There was no date set for review/ update.
I understand that serious matters take time to consider, but I am concerned by this open-ended approach to a serious matter, by an agency that is supposed to be all about fairness and accountability and should be above reproach.
It does not seem to me to be a sufficiently accountable approach.
I ask Justice Committee to note it for any future consideration of the effectiveness of the CCRC and CCRC’s governance.
I should note that parallel to this matter, NHS England’s “Well Led” investigation of UHB is expected to conclude early next month. There is reason to have modest expectations of this given that NHS regulators have repeatedly protected and helped to recycle erring NHS senior managers, which was a trigger for the NHS Kark review on the Fit and Proper Test in the NHS. The report of this review by Tom Kark KC was published over four years ago, but reflecting the recalcitrant nature of NHS senior management culture, its implementation was entrusted to NHS England and it has not yet been implemented.
I copy below the relevant correspondence from the CCRC showing its initial response and later responses with no identified timescale for completion or even review and update.
Yours sincerely,
Dr Minh Alexander
NHS whistleblower and retired consultant psychiatrist
Cc Health and Social Care Committee
From: REDACTED
Subject: FW: Concern about Karen Kneller’s role as Criminal Cases Review Commission CEO
Date: 14 April 2023 at 14:50:04 BST
To: REDACTED
Dear Dr Alexander
I confirm that your correspondence of 13 April 2023 has been passed to Helen Pitcher.
Ms Pitcher will consider the contents and respond to you within 28 days.
Please could I also ask that you direct any further correspondence on this matter to this address rather than the Commission’s general mailbox.
Yours sincerely
Kind regards,
REDACTED
Executive Assistant to the Chairman | CCRC
From: REDACTED
Subject: FW: Concern about Karen Kneller’s role as Criminal Cases Review Commission CEO
Date: 18 May 2023 at 15:51:04 BST
To: REDACTED
Dear Dr Alexander
Further to recent correspondence, Ms Pitcher has asked me to confirm that matters remain under consideration and inquiries are underway.
At this stage, we do not have a date for completion, but we will inform you of the outcome in due course.
Yours sincerely,
REDACTED
From: REDACTED
Subject: RE: Concern about Karen Kneller’s role as Criminal Cases Review Commission CEO
Date: 9 June 2023 at 10:49:39 BST
To: REDACTED
Dear Dr Alexander,
Thank you for your recent email.
Our inquiries remain underway. We do not have a specific completion date but will inform you of the outcome as soon as we can.
Yours sincerely,
REDACTED
Executive Assistant to the Chairman | CCRC
RELATED ITEMS
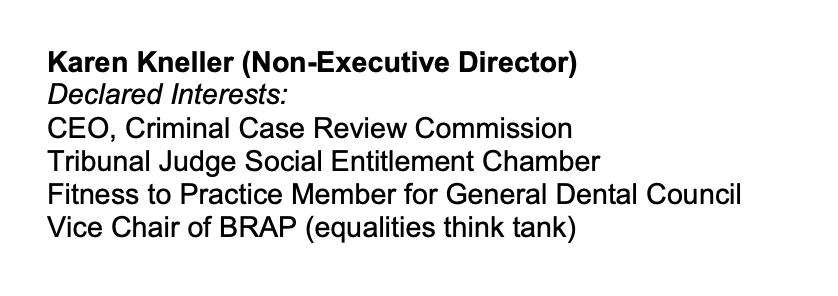
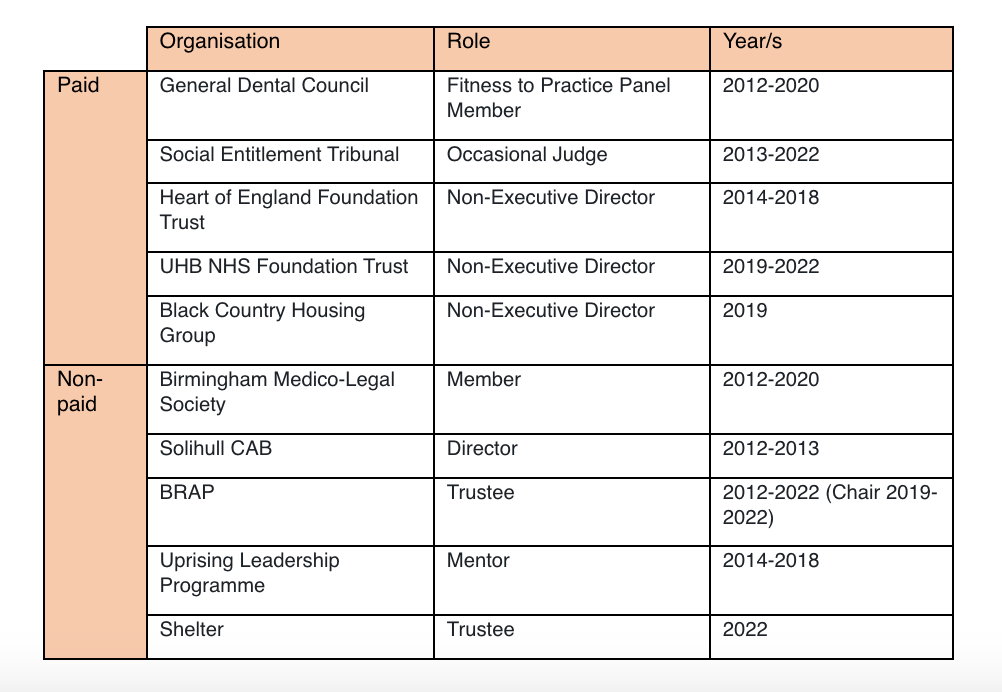
There is a difference in Karen Kneller’s declaration of interests at UHB and her declaration of interests at CCRC, which are more extensive.
This is her declaration of interests at UHB taken from a published trust document of 2020 (the most recent I could find):
By Dr Minh Alexander retired consultant psychiatrist 21 June 2023
The parliamentary Health and Social Care Committee sat on 20 June 2023 and took evidence from Steve Barclay Secretary of State.
Mr Barclay appeared to start waffling when asked about failure of the Freedom To Speak Up project.
In his verbal perambulations he wondered out loud if bad NHS managers are recycled.
He knows the answer to this, of course, having commissioned the Kark review on this topic in 2018.
But to provide cognitive support, I have reminded him of his previous commission, of two recent unanswered letters on the topic and of a topical example of an NHS exec who resigned after being criticised for poor governance, who then sold governance services to the NHS and is now back in the NHS as a Director of – you guessed it – Governance.
But it is positive that MPs are now starting to speak openly about the failure of the Freedom To Speak Up project.
The danger is that it will be replaced with something equally ineffective that will be again be used for another eight to ten years for PR and to block real change.
Actors new to the whistleblowing landscape, who are not whistleblowers, have recently been clamouring for a central route of NHS disclosure, such as at DHSC or NHS England. I have advised against that notion but it has popped up again through a Committee member. I have warned the Committee against it.
These are the relevant exchanges at Committee on 20 June 2023:
Rachael Maskell MP: If I may Chair. I’d just like to turn to the complaints system. I’m really concerned about the reports coming out of University Hospitals Birmingham. We’ve seen the reports that have come out of a number of mental health trusts. These trusts are clearly not safe for patients as the data is showing, but also not safe for many of the staff who are raising concerns.
After the Robert Francis report we thought that this would come to an end. Duty of Candour very much [inaudible] the front, whistleblowing being accepted as part of the NHS culture, however we haven’t seen the culture move on, and risk still prevails. Even looking at the PHSO insufficiency in being able to have leverage over what’s happening and in their reporting, back of what’s happening at many of these trusts, I’m really concerned that we do not have a robust complaint system.
What steps are you taking to look into that and what measures have you taken to date to move that forward?
Steve Barclay MP and Secretary of State for Health and Social Care: I think it’s a hugely important issue and I think colleagues across the house when I was on the Public Accounts Committee as a member for four years, one of the things I particularly focussed on, which is on record, was gagging of whistleblowers, particularly in the NHS. And how we have more transparency and a culture of learning where things go wrong, you know. In a Department which is allocating over £180 billion and employing as many people as the NHS does, there will be issues that go wrong. The key is how we identify them quickly and how we learn from that.
And so I know the Committee will share my concern when we heard the reports of some of the sexual abuse data that was coming out. And that was something I very urgently met with NHS leaders to discuss to ensure that was being gripped. You allude to the issues of mental health and I hope to have more to say very shortly on that specifically, particularly in the context of the Essex issues. And I know that a number of members of parliament [inaudible] have discussions with them on that, not just in Essex, but there’s been concerns more widely so I think the point you raise is a very valid one. It’s one I take extremely seriously. It’s one that colleagues can see throughout my time as an elected representative I’ve taken very seriously and it is something that I have discussed with Amanda Pritchard the chief executive of the NHS and with senior leaders such as Ruth May the lead nurse, and others, to ensure that we are learning the lessons from these issues and ensuring that where an issue is raised whether that’s by patients, whether it’s by members of staff, whether it’s by others in the community, that we’re addressing it.
Rachael Maskell MP: Just my final question. Because of what has been described as quite a bullying culture in many of these organisations and bullying being very prevalent across the whole economy (27% of workers experience bullying) but when it comes into the Health context it clearly puts the system at risk and patients at risk as well. Not to mention the impact on staff and staff retention.
Will you look at a central place where people can raise concern independently, in order to be able to whistleblow safely and to be able to raise those those concerns so that they are properly investigated? And a top down approach can be put on trusts to deal with these issues, because without it, as hard as the Robert Francis report tried to address these issues, it hasn’t delivered.
Steve Barclay MP andSteve Barclay Secretary of State for Health and Social Care: I’m keen to understand where, if there are areas where the complaints system are not working, why that is and how we learn from it. I think it is an area that has already had lots of focus so one of the issues we’ve got to understand, we have a Patient Safety Commissioner, we have er Guardians, we’ve had a number of other initiatives over many years, in this space. You touched on cases such as Birmingham which still generates significant concern. So for me it’s about understanding why when issues are known about locally, too often they’re not addressed. And how where, we’re learning from that. So that includes things like the trust Board and what visibility, what line of sight does the Board have? What accountability is there for senior managers when wrong doing is established? Are they just rotated through the system? Or are people held to account? So I think there are a number of issues. It’s an issue sadly that’s been with us for quite a while, because I’ve spent a fair bit of time on it in a previous role. But I share your absolute desire to tackle it. I think you touched on it in the context of the wider duty we have to NHS staff and things like staff absence which is why these things then often manifest themselves in falling retention, because people vote with their feet and leave. It’s a hugely important issue. It’s one that we have a number of people involved in the NHS to tackle. It is also a role for the Royal Colleges and others in the wider NHS family and I’m extremely keen to work with them on it.
This is my letter to Steve Barclay which includes a formal request for information about the DHSC’s approach to the Kark review on Fit and Proper Persons in the NHS:
“BY EMAIL
Steve Barclay
Secretary of State for Health and Social Care
21 June 2023
Dear Mr Barclay,
Kark review implementation and disbarring unfit NHS senior managers
I watched your oral evidence to Health and Social Care Committee yesterday, and in particular your answers to concerns that the government’s Freedom To Speak Up model has failed to deliver.
Your response on being asked about the failure of the DHSC’s and Robert Francis’ 2015 Freedom To Speak Up project was thus:
“Steve Barclay MP and Steve Barclay Secretary of State for Health and Social Care: I’m keen to understand where, if there are areas where the complaints system are not working, why that is and how we learn from it. I think it is an area that has already had lots of focus so one of the issues we’ve got to understand. We have a Patient Safety Commissioner, we have er Guardians, we’ve had a number of other initiatives over many years, in this space. You touched on cases such as Birmingham which still generates significant concern. So for me it’s about understanding why when issues are known about locally, too often they’re not addressed. And how where, we’re learning from that. So that includes things like the trust Board and what visibility, what line of sight does the Board have? What accountability is there for senior managers when wrong doing is established? Are they just rotated through the system? Or are people held to account? So I think there are a number of issues. It’s an issue sadly that’s been with us for quite a while, because I’ve spent a fair bit of time on it in a previous role. But I share your absolute desire to tackle it. I think you touched on it in the context of the wider duty we have to NHS staff and things like staff absence which is why these things then often manifest themselves in falling retention, because people vote with their feet and leave. It’s a hugely important issue. It’s one that we have a number of people involved in the NHS to tackle. It is also a role for the Royal Colleges and others in the wider NHS family and I’m extremely keen to work with them on it.”
A number of points arise from your comments to Committee:
1. The Patient Safety Commissioner’s role
The Patient Safety Commissioner’s remit is restricted to medicines and medical devices.
She is not currently listed as a Prescribed Person to whom whistleblowers can make protected disclosures.
But if she is to be a Prescribed Person under UK whistleblowing law, within these narrow confines, I would be grateful if you could confirm that this is so.
2. Local NHS Freedom To Speak Up Guardians
Local FTSU guardians are toothless and importantly, defenceless. They themselves may become victims of abusive NHS organisations which employ them, and that has happened in some cases. Alternatively, some Guardians are appointed because they are willing to abuse whistleblowers. The model is a logically flawed and wasteful. It contributes very little. Testimony from two whistleblowers who have been failed by NHS trust Guardians can be found here:
Oversight by NHS Boards is not the issue. It is abusive NHS Boards that are the issue, whether by actively and directly abusing whistleblowers or knowingly soliciting and/or permitting abuse.
4. Accountability for senior management wrongdoing
In your evidence to Committee you wondered out loud about whether there is accountability for erring senior NHS managers, or whether such individuals are recycled.
You personally commissioned the Kark review in 2018 on identifying unfit NHS managers and preventing their recirculation.
You will recall the immediate catalyst was the debacle in which failed trust managers were protected by NHS regulators after Mid Staffs style failures at Liverpool Community Health NHS Trust.
However, the implementation of the Kark review recommendations was entrusted to NHS England, an NHS regulator which has been responsible for much of the executive recycling and setting a culture of impunity.
There has been no sign yet of implementation of the Kark review.
Indeed, NHS England has claimed to me that there is no ministerial support for Tom Kark’s crucial recommendation of a disbarring mechanism for the worst and most unfit NHS managers.
I have written to you twice about this (7 February and 29 May 2023, forwarded below), asking you to reconsider this reported decision, but I received no reply.
A current example of NHS executive recycling
But to answer your question on whether erring senior managers are rotated through the system, the answer is ‘yes’. This is a current and topical example:
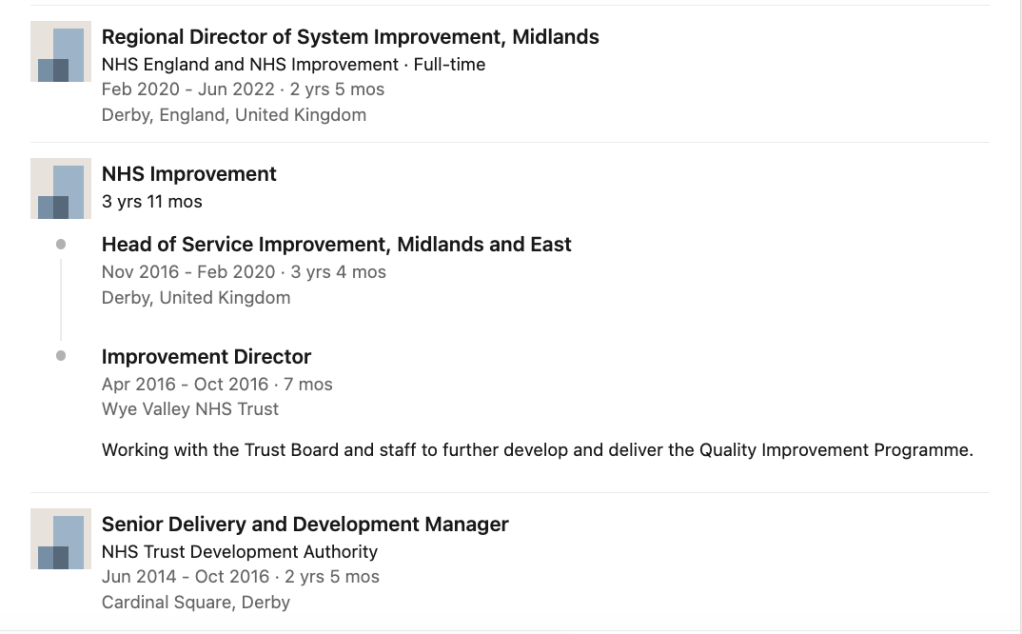
Darren Grayson resigned from a post as NHS trust CEO in 2015 after an extremely critical CQC report and allegations of management bullying and other governance failures. Mr Grayson went on to sell consultancy services to the NHS through a private company, the Good Governance Institute. This included work for a predecessor body of University Hospitals Sussex NHS Foundation trust, during Marianne Griffiths’ tenure as CEO. Partly on the basis of material produced by the Good Governance Institute, the CQC took the trust out of special measures and rated it “Good” in 2019. Last year Mr Grayson took up a substantive post at this same trust as Director of Governance. Staff whistleblowing to the CQC continued and the police are now making enquiries into concerns about patient deaths 2015-2020 that may amount to gross negligence manslaughter.
The longer the implementation of the Kark review is delayed, the more examples of such recycling will accumulate.
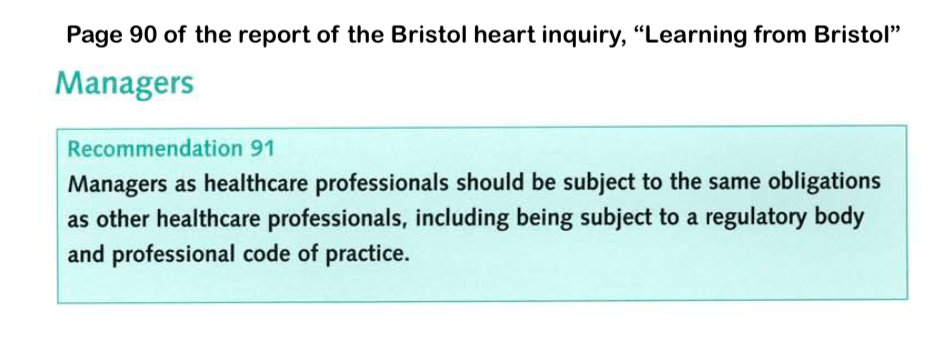
The Kark review stopped short of recommending managerial regulation, but reserved it as an option for the future. Please note that the delay in regulating NHS managers now spans decades.
The 2002 Bristol Heart inquiry recommended regulation for NHS managers:
I would be very grateful if under FOIA the DHSC could advise me of the following:
1. As of now, which of the Kark review recommendations does the DHSC accept and which does the DHSC reject?
2. Is it correct that there is no ministerial support for Tom Kark’s recommendation of a disbarring mechanism for unfit NHS managers?
3. Why did the DHSC decide not to pursue a disbarring mechanism? What directions/ instructions has the DHSC given to NHS England on this matter?
4. What is the DHSC’s timetable, if any, for implementating any of the Kark review recommendations that it has accepted?
Many thanks and best wishes,
Minh
Dr Minh Alexander”
This is my letter to the Health and Social Care Committee to register concern about the proposal for another NHS and government controlled whistleblowing body, and to ask that the Committee instead focuses on implementation of the Kark review.
By Dr Minh Alexander retired consultant psychiatrist 13 June 2023
Background
The private company the Good Governance Institute (GGI) sells consultancy services and has many links with the NHS. It lists a large group of current and former NHS managers and NHS regulatory staff amongst what it calls its “people”.
What this designation signifies seems vague.
Jacqui Smith the controversial former Home Secretary, former Chair of University Hospitals Birmingham NHS Foundation Trust (UHB) and current chair of Barts Healthcare NHS Trust and Barking Havering and Redbridge University Hospitals NHS Trust is listed amongst the Institute’s “people”.
Upon a FOI request to Barts, Smith denied that this amounted to any specific role: “Rt Hon Jacqui Smith has no formal board or management title or any ongoing role with GGI” but nonetheless Smith is listed as one of the GGI’s “people”.
Several other UHB managers are listed as GGI “people”.
The GGI carried out a “Well Led” review on UHB in 2019, but more on that another time.
What I cover here is a link between the GGI and University Hospitals Sussex NHS Foundation Trust, where it was revealed at the Employment Tribunal on 5 June 2023 that the police are investigating allegations that may amount to gross negligence manslaughter.
The Guardian reported that Mr Krish Singh, surgeon, one of the Sussex whistleblowers had raised concerns about corporate actions which resulted in deaths:
“Singh claimed the trust had promoted insufficiently competent surgeons and overused insufficiently skilled locums.”
“…he claimed that cost-saving changes at the hospital “were driven through that were grossly unsafe and ultimately drove up complication rates and patient mortality”.
Another senior trust whistleblower Mr Mansoor Foroughi, surgeon, raised similar concerns.
University Hospitals Sussex NHS Foundation Trust was formed by the 2021 merger of Western Sussex Hospitals NHS Foundation Trust, a regulatory and political favourite run by Marianne Griffiths CEO and George Findlay Medical Director, with the struggling trust Brighton and Sussex University Hospitals NHS Trust.
In the CQC’s evidence appendix for the related inspection report, CQC stated that the trust had hired the Good Governance Institute and ensured a “golden thread” of quality throughout its improvement strategy:
“Governance
The chief medical officer explained that when the current executive management team had taken over the management contract for the trust, they felt concerned about the governance and assurance arrangements in place and felt they did not have assurance about the quality of treatment and care being provided for patients. They found examples of good clinical governance and reporting in place at a service level, but this information was not being reported up to the board. The trust had therefore commissioned an external review of the governance arrangements from the Good Governance Institute.
Because of this review, a structure of five divisions was put in place where previously there had been 13 directorates. The divisional structure led by a triumvirate of a clinical director, general manager and head of nursing had provided the building blocks for the revised governance arrangements. The Good Governance Institute provided training in governance for these leaders. the non-executive directors and executive directors described the journey for the triumvirate leaders moving from a concern that more reporting was going to be required of them, to understanding governance and how the data and reporting would enable them to drive quality improvement.
The board invited the Good Governance Institute to carry out a review of the trust’s quality governance structures, which resulted in 31 separate recommendations being made. The trust acted to address these issues and the Good Governance institute carried out a further review reporting on progress against these actions. A focus of this work has been to strengthen quality governance arrangements at divisional level.
The trust had effective structures, systems and processes in place to support the delivery of its strategy including sub-board committees, divisional committees, team meetings and senior managers. Leaders regularly reviewed these structures. The trust reported regularly through its governance arrangements on progress against delivery of its strategy to the board, trust executive committee and to other relevant committees. However, the structure needed more time to become fully embedded.
In interviews with the chair of the Quality Assurance Committee, the chair of audit and the chief medical officer (the executive officer responsible for governance), all non-executive and executive directors were able to describe the governance structure and how it functioned.
The effectiveness of the governance arrangements was observed on inspection at Strategy Deployment Review meetings. Each of the three leaders of each division owned and presented the data for their breakthrough objectives. They had interrogated the data to find root causes where the objectives were behind plan and had devised action plans based on this knowledge to bring the objective back on track.
The Chair of the Audit Committee explained that under the previous administration, assurance was not provided through reporting and they were not getting the information they needed. The new structures provided a joined-up approach that provided assurance on quality and delivery against the Patient First Strategy and breakthrough objectives and delivered quality improvement.
Quality was a ‘golden thread’ running through the trust Patient First Strategy. In all the interviews undertaken on inspection the golden thread of quality was evident in the use of data both quantitative and qualitative and how this was triangulated and reported through the Quality Steering Group to the Quality Assurance Committee and the trust board.
Non-executive and executive directors were clear about their areas of responsibility. Performance against the trust’s patient first strategy, true north and breakthrough objectives was focused and reinforced through the trust’s strategic deployment review approach. There was clear ward to board line of sight through daily performance huddles, weekly driver meetings, Divisional Strategy Deployment Review, executive level Strategy Deployment Review and the board.
The Chair of the Quality Assurance Committee gave an example of challenge and holding the executive directors to account when an action plan did not evidence sufficient learning to drive improvement and required further work to be undertaken.
The quality dashboard was aligned to the quality priorities along with the quality improvement plan with actions being taken and monitored at divisional, corporate and board level through the quality governance system, Quality Assurance Committee and board. The Audit Committee evaluated the effectiveness of the trust’s structures and processes in relation to the management of risk, the management of performance and financial management and the management of quality and quality improvement.”
Well, if your quality dashboard looks good, what could possibly go wrong?
And who led the CQC inspection team that concluded BSUH should be taken out of special measures? The inspection team was led by Cath Campbell now CQC Deputy Director of Operations and a David Melbourne.
Would that be the David Melbourne who was then deputy chief executive of Deputy Chief Executive of Birmingham Women’s and Children’s NHS Foundation Trust and is now the much-criticised CEO of Birmingham and Solihull ICB, a body that has helped to protect failing UHB executives and to obfuscate the reality at UHB?
Darren Grayson formerly of the Good Governance Institute, now a University Hospitals Sussex NHS Foundation Trust director
I am informed that the Good Governance Institute’s review of BSUH in 2018 was led by Darren Grayson, executive director and partner at the Good Governance Institute 2016-2022.
The Good Governance Institute later celebrated its work at Sussex with a little blog:
In March 2022 Griffiths appointed Darren Grayson, executive director and partner of the Good Governance Institute, on to the board of the newly formed University Hospitals Sussex NHS Foundation Trust as Chief Governance Officer.
This is Grayson’s LinkedIn entry, which gives some of his CV in terms of past NHS posts prior to becoming an executive partner at the GGI. He was a local NHS executive, previously working as CEO of NHS Brighton and Hove, and then CEO of East Sussex Healthcare NHS Trust.
The CQC found evidence of managerial bullying and other signs of poor culture. For example:
“The themes identified related to the quality of staff engagement, low morale, and a bullying and harassment culture from senior management.”
“The trust board continues to state they recognise that staff engagement is an area of concern but the evidence we found suggests there is a void between the Board perception and the reality of working at the trust. At senior management and executive level the trust managers spoke entirely positively and said the majority of staff were ‘on board’, blaming just a few dissenters for the negative comments that we received.
We found the widespread disconnect between the trust board and its staff persisted. This is reflected in the national NHS Staff survey.
….The trust told us they were disappointed by the results; but we saw no direct programme to address this or to change the position. There remained a poor relationship between the board and some key community stakeholders. We found the board lacked a credible strategy for effective engagement to improve relationships.
….Within the trust, we did not see a cycle of improvement and learning based on the outcome of either risk or incidents.
• Staff remained unconvinced of the benefit of incident reporting, and were therefore not reporting incidents or near misses to the trust. the trust was not able to benefit from any learning from these. this position had not improved.
• The risk register was not capturing risks in a robust way.
• We saw a redesign of the governance structure, but were unable to yet see any significant benefits or improvements from this.”
A special meeting of the local Joint Health Scrutiny and Overview committee reached a unanimous vote of no confidence in him:
The Chair of the Committee commented: “You are the captain of the ship which has hit rocks, and it is starting to sink and I think the biggest morale boost you can give to staff is to say sorry and then offer your resignation.”
Grayson reportedly refused to resign initially but later stepped down:
“The CEO did not listen to his own staff, public opinion or GMB. Instead he openly criticised and blamed those, including GMB, for challenging him and his management style.”
This is Grayson’s biography from the University Hospitals Sussex NHS Foundation Trust’s website, which adds political detail in terms of his work at the New Labour hub, the No 10 delivery unit which ran 2001-2005.
Importantly, Darren Grayson’s partner is Jenny Procter, another director at University Hospitals Sussex NHS Foundation Trust, as revealed by trust declarations of interest:
According to her LinkedIn entry, Procter has been the trust’s Director of Improvement & Delivery since April 2021, and before that she was Director of Efficiency & Delivery from 2017 to 2021 for both its predecessor trusts.
Matters arising
So, what does it say about Marianne Griffiths’ leadership of University Hospitals Sussex NHS Foundation Trust that she hired someone like Darren Grayson to review trust governance and then later gave him an executive job, after such a disaster at East Sussex Healthcare NHS Trust?
Ironically for Griffiths et al, their enterprise with the Good Governance Institute may well tip the balance in any consideration of corporate failures in the deaths scandal. In the
“At a corporate level, we are working with Good Governance Institute to ensure clear lines of sight from the front line of service delivery through to board level on quality and safety. This means that we can identify – and resolve – issues much earlier, contributing to the improvements in patient care.”
As above, the CQC later reported that the “clear line of sight” by the trust board was in place in its January 2019 inspection report. This appears to be additional evidence supporting staff disclosures to Health Education England that the board, through Griffiths, knew about the deaths, staff concerns and lack of governance in the surgical division.
I am requesting copies of all Good Governance Institute reports undertaken for the trust under FOIA.
I will also ask CQC to confirm that David Melbourne was an employee of the CQC as an inspection chair/ executive reviewer, to disclose whether this continues and to disclose whether any other executives from UHB and Birmingham and Solihull ICB are CQC executive reviewers.
CQC’s unseemly habit of employing part time/ bank staff from regulated bodies, especially at director level, has long been a source of conflicted interests and incestuousness which has undermined the authority and legitimacy of its inspections.
Importantly, it has now been made public that shockingly, Grayson is the trust’s police liaison for Sussex police with respect to the polic investigation into police deaths.
This is despite the fact that there are questions of conflict of interest from his review of trust services in his previous capacity as a consultant for the so-called Good Governance Institute. The GGI was investigated by BBC Newsnight.
RELATED ITEMS
This is a published CIPFA profile of David Melbourne in question and answer format, from when he was CFO at Birmingham Women and Childrens, in which Melbourne sympathises with the poor and emphasises the importance of staying true to your values.
This is Birmingham and Solihull ICB’s biography of Melbourne:
Melbourne took part in a charade in which the ICB and UHB misled the public and partner agencies by claiming that David Rosser the former CEO of UHB stepped down, when he in fact remained employed by UHB:
The Kark review, commissioned by Steve Barclay five years ago made a string of recommendations for preventing the recycling of unfit managers in the NHS. The task of implementation was given to NHS England, which is notorious for running the so-called “donkey sanctuary” for failed senior NHS managers. There has been no sign yet of any implementation, and NHS England claims that Steve Barclay himself dropped Kark’s recommendation for a disbarring mechanism. Correspondence to Mr Barclay about the failure to implement Kark’s recommendations has so far gone unanswered.
The NHS National Freedom To Speak Up Guardian helped Griffiths and co by disadvantaging trust whistleblowers in 2018, when she delayed a review of whistleblowing governance. This aspect of the saga can be found here:
Dr Minh Alexander retired consultant psychiatrist 8 June 2023
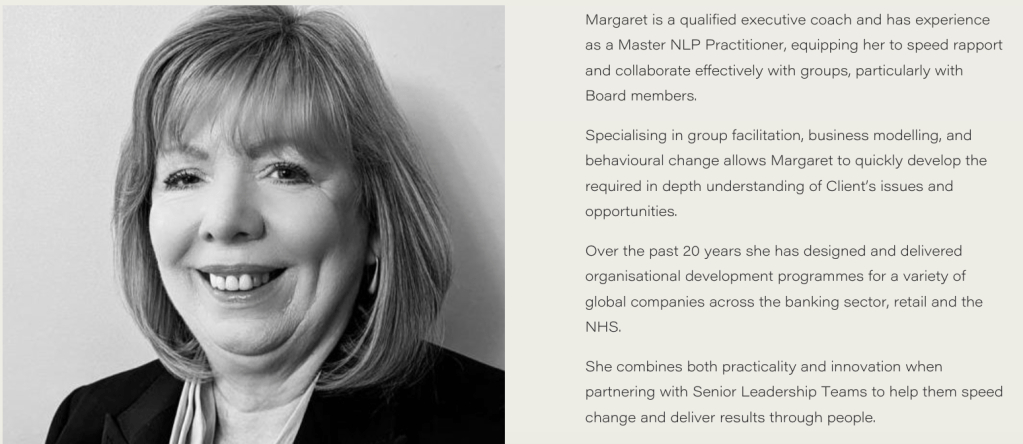
This is a brief post to share and unpack claims made by University Hospitals Birmingham NHS Foundation Trust, via an FOI disclosure, about its appointment of the private consultancy TheValueCircle to review its “toxic” culture.
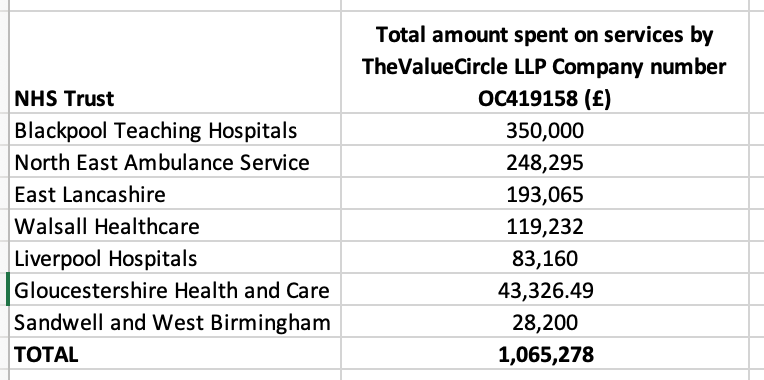
So far, other enquiries about TheValueCircle’s past work in the NHS have revealed steep fees, little evident tangible work product and much secrecy by the NHS bodies which purchased the consultancy’s services. Well Led and governance reviews etc undertaken by TheValueCircle are kept under lock and key by NHS execs:
The panel of seven included four UHB directors, including significantly Fiona Alexander the UHB Director of Comms and former editor of the Birmingham Post. Why would you want the chief spin doctor vetting a contractor for a governance exercise, unless perhaps it was more of a PR exercise?
UHB feel no shame it seems in stating that Fiona Alexander’s role is one of reputational management:
So what is she doing inside an exercise that is purportedly supposed to uncover and reveal the embarrassing truth? A silly question, no doubt.
The disclosed selection panel members:
“Dame Yve Buckland, Chair of University Hospitals Birmingham NHS FT Roger Kline, Independent Chair of UHB Culture Review Reference Group Mehrunnisa Lalani, Non-Executive Director and Chair of People and Culture Committee UHB Professor Mike Bewick, Patient Safety Review Lead and report author – identified culture themes to be carried through in to culture review Giles Peel, Patient Safety Reviewer and report contributor – identified culture themes to be carried through in to culture review Cathi Shovlin, Chief People Officer Fiona Alexander, Director of Communications“
There was no staffside representation on the selection panel, so arguably no one with a real interest and commitment was there to ask penetrating questions.
Mike Bewick who was hired by Birmingham and Solihull Integrated Care Board to oversee all of the UHB reviews, and Giles Peel one of his longstanding business associates and regular report co-authors were on the panel.
Interestingly, Bewick and Peel were appointed to the panel a month after all the others.
They were not paid by UHB so the implication is that the ICB was paying for their input.
The trust denied that NHS England was involved in the selection of panel members and maintained that it was solely directed by the trust chair Yve Buckland who both appointed and sat on the panel.
But the appearance of Bewick and his associate Peel on someone else’s tab suggests there was coordination with other bodies and external influence on this process.
Buckland also hired Roger Kline to act as “independent” chair of the panel.
In response to a question about panel members’ credentials for the task, UHB answered merely:
“Their credentials are evident from the relevance of their role to the culture review.”
A great start to a review of culture when the accused is so arrogant that it cannot even affect a small show of humility.
As for the criteria by which Buckland’s panel selected the contractor to conduct the culture review, these are the disclosed criteria:
The panel’s disclosed selection criteria for the contractor:
“1. Experience and credibility in undertaking a high quality culture review of this scale and in our current context 2. Experience in undertaking culture reviews both within the NHS and wider – important that they understand the NHS but also seek added value in what can be gained from wider sectoral experience 3. Demonstration of understanding of culture, our organisation, our values and the different stakeholder groups 4. Demonstration of understanding of equality, diversity and inclusion, and their approach to embedding this through culture review 5. Approach to the culture review – how they will maximise opportunities to hear all voices and how they will approach engagement and trust-building in our current context 6. The team – their diversity and ability to reflect our staff, and the gravitas with which they can engender trust and credibility 7. Scale – their ability to undertake the review in all its complexity and in the depth required within the timeframe 8. Value for money – price, timescale and any additional services they would include”
So how exactly did Kline et al establish that TheValueCircle had “credibility”, “gravitas” and be “value for money” when there is no work product by the company in the public domain and other organisations jealously guard it with such secrecy?
Does the hiring of TheValueCircle whiff a little of a predetermined decision because of a recommendation/ instruction from on high?
Was a selection criteria missed off the disclosed list: “favoured and tipped by other executives”?
Finally, let us remember that TheValueCircle has friends in high places. Andrew Morris a member of the NHS England board acts as a consultant for them.
Dr Minh Alexander retired consultant psychiatrist 7 June 2023
NHS England has purchased services from a private company, the Good Governance Institute, despite the fact that the Institute hired former NHS director Mason Fitzgerald. Fitzgerald was sacked after false qualification claims, including on his LinkedIn entry:
NHS England has failed to respond to concerns since last autumn and initially ignored a complaint about this. It also ignored a related FOI request until it recently received a direction from the ICO to respond.
It now refuses to confirm or deny that it has employed Mason Fitzgerald since his sacking by East London NHS Foundation Trust.
Curiously, NHS England admitted that the Good Governance Institute carried out pro bono research for it this year on “systems”. This sounds as if it could be the work on ICS governance that the GGI and Mason Fitzgerald were possibly involved with, as suggested by GGI material in the public domain.
I have asked for further information about this pro bono research and for an internal review of NHS England’s refusal to answer on whether it has employed Mason Fitzgerald since his sacking.
I have also pointed out recent evidence that the GGI’s normalisation of his behaviour and his dismissal by the NHS is leading to his re-entry into the NHS.
The FOI response and further correspondence to NHS England is provided below.
From: REDACTED
Subject: Sensitive NHS England’s relationship with the “Good Governance Institute” and possible employment of sacked former NHS director Mason Fitzgerald
Date: 7 June 2023 at 07:14:11 BST
To: REDACTED
Cc: REDACTED
BY EMAIL
Amanda Pritchard
Chief Executive
NHS England
7 June 2023
Dear Amanda,
NHS England’s relationship with the “Good Governance Institute” and possible employment of sacked former NHS director Mason Fitzgerald
I have finally received NHS England’s response to my FOI request about whether or not NHS England employed Mason Fitzgerald after he was sacked by East London NHS Foundation Trust (ELFT) in 2021, following concerns about false claims about a legal qualification which appeared in several documents and on his LinkedIn entry.
As you may recall, I was concerned that the so called “Good Governance Institute”, a private company with many links to the NHS and which lists many former and current senior NHS managers amongst its “people”, had hired Mr Fitzgerald as a senior consultant despite his sacking by the NHS. It has since promoted him to Director of Consultancy.
I became even more concerned when I saw that Ruth May NHSE England Chief Nursing Officer had engaged the Good Governance Institute late last year. I became even more concerned when I saw material by the GGI which raised questions about whether the GGI was working with NHS England on ICS governance and that Mr Fitzgerald taking part in this work.
Hence I raised concerns with Ruth and then with you about whether NHS England should have links with the GGI and whether NHS England was employing Mr Fitzgerald to work on of all things, ICS governance.
NHS England has stonewalled. The response to my eventual FOI enquiry, made in the absence of any response from you or Ruth, only came after direction by the ICO to NHS England to respond. The FOI reply is forwarded below.
NHS England has now refused to confirm or deny whether it has employed Mason Fitzgerald on grounds that this is non-disclosable personal information. It considers my request for this information “intrusive”.
But it has confirmed that it did indeed purchase services from the GGI AFTER Mr Fitzgerald was sacked by the NHS, including a purchase by Ruth May’s directorate in autumn 2022, by which time Mr Fitzgerald was working for the GGI.
Curiously, NHS England states that it received an offer of pro bono work from the GGI this year: “an offer of pro bono work with a nominal payment of £100”.
This work was vaguely described as: “consultancy services for conducting research with systems to inform the development of set of principles regarding system risk management”
1) As a fresh FOI request, I would be grateful if NHS England
– could confirm whether this research by the GGI related to ICS governance
– could disclose all documents relating to the offer and acceptance of this “pro bono” consultancy work
– could disclose whether the former CEO of ELFT who is now an NHSE director was involved in setting up this “pro bono” arrangement
– could disclose what access to NHS systems was given to the GGI in order to undertake this research, including any financial data
– could disclose the research report(s) produced as a result of this “pro bono” consultancy work
– With respect to NHSE’s advice that “We are able to generally advise that NHS England scrutinises the suppliers financial standing and capability to deliver the required services and can withhold contracts from organisations where directors have been convicted of fraud or similar offences but that power does not extend to the investigation of employees of the organisation”, please disclose the policy document(s) which sets out what due diligence NHSE should undertake regarding contractors’ governance and the circumstances in which contracts may be refused.
2) I would also be grateful if NHS England could internally review its assertion that information about whether it employed Mason Fitzgerald is personal data, that is not disclosable.
Mr Fitzgerald was a senior NHS director who was appointed as an NHS trust Chief Executive but did not take up the position at the last minute, causing a scandal and serious reputational harm and disruption to two NHS trusts because of the false claims about his qualifications.
The reasons for his eventual dismissal by East London NHS Foundation Trust have a serious impact on public trust in the NHS.
It is of great public interest whether NHS England as the body which oversees the rest of the NHS and is a regulator of NHS trusts and NHS Foundation Trusts, takes issues of probity seriously and does not employ those who have been dismissed following acts of dishonesty. It is a matter of basic Safeguarding that senior individuals whose actions impact on many, many lives should be trustworthy.
Moreover, it is important that NHS England as the body charged with implementing the Kark review recommendations on preventing unfit NHS managers from recirculating in the NHS is seen to model good practice, to live by the principles set out by the Kark review and not to actively undermine the goals of the Kark review.
NHS England maintains that it cannot investigate contractors’ employees. But the NHS has already investigated and sacked Mr Fitzgerald.
It is therefore essential that NHS England accounts for whether it has employed Mr Fitzgerald following his sacking by East London NHS Foundation Trust, and if it has done so, to explain how it will move on from this.
I should point out that the GGI’s normalisation of Mr Fitzgerald’s behaviour and dismissal is leading to his re-entry to the NHS in other contexts. According to a tweet by the Head of Risk Management of Nottingham University Hospitals, where maternity deaths are currently being investigated by Donna Ockenden, M Fitzgerald was due to speak there last month as a GGI representative, on “risk appetite”.
If NHS England is also seen to normalise the situation, and fails to account in full regarding its relationship with the GGI or to answer questions about whether it has employed Mason Fitzgerald after his sacking, this effect would be greatly amplified.
With best wishes,
Minh
Dr Minh Alexander
Cc Tom Kark KC
BBC Newsnight
Health and Social Care Committee
Steve Barclay Secretary of State
From: REDACTED
Subject: Freedom of Information Request (Our Ref: FOI-2305-1971470) NHSE:0176254
Thank you for your Freedom of Information (FOI) request dated 15 March 2023. Please accept our apologies for the delay in responding.
Your request
You requested the following information [numbering inserted by NHS England]:
“As an FOI request,
please disclose if since July 2021 when Mason Fitzgerald was sacked by East London NHS Foundation Trust, NHS England has purchased Mason Fitzgerald’s services in any capacity, whether directly or via another party such as the Good Governance Institute.
Please disclose
the number of occasions on which his services were purchased,
the total number of days work purchased,
the type of services purchased and
the total amount spent.
As part of this, please clarify if Mason Fitzgerald did indeed work on ICS governance, and if he did, on which ICS did he work.
Please also disclose
which NHSE senior managers signed off these expenses, and
under which NHSE directorate these expenses fell.
Please also disclose the total amount that NHS England has spent on the Good Governance Institute’s services since July 2021, irrespective of which directorate purchased these services.”
Decision
In respect of questions 1 and 2, NHS England is neither confirming nor denying whether the requested information is held.
In respect of question 3, NHS England holds some information in scope of your request and has disclosed all of the information that it holds.
Questions 1 and 2
Please note, from the information that NHS England would routinely hold or collect, we would be unable to breakdown this information as per parts 1(b), 1(c) and 1(e) of your request. Therefore for those parts, we confirm NHS England does not hold the information being requested.
In relation to the other parts under questions 1 and 2, NHS England neither confirms nor denies whether it holds the requested information and considers section 40(5)(b)(i) is engaged.
To determine whether section 40(5) applies, NHS England needs to demonstrate:
that confirming or denying whether the requested information is held would constitute the disclosure of a third party’s personal data; and
that providing this confirmation or denial would contravene one of the data protection principles.
Section 3(2) of the Data Protection Act 2018 (DPA) defines personal data as: “any information relating to an identified or identifiable living individual”.
In response to part a), whether NHS England has contracted or employed services from a specific individual, or did not employ a specific individual, meets the definition of personal data under the DPA. We consider that if we were to either confirm or deny we hold this information, this would in itself disclose personal data.
NHS England are required to be consistent when considering the application of section 40(5) when processing FOI requests. Therefore, it is important to apply this exemption on a consistent basis when considering requests for information under the FOI Act. The application of this exemption should not be taken as an indication as to whether the information is held or not.
In response to part b),NHS England can only confirm whether or not it holds the requested information if to do so would be lawful (i.e. it would meet one of the condition of lawful processing listed in Article 6(1) GDPR), be fair and be transparent.
The most applicable would be Article 6(1)(f) which provides that “processing is necessary for the purposes of the legitimate interests pursued by the controller or by a third party except where such interests are overridden by the interests or fundamental rights and freedoms of the data subject…”
Disclosure under FOI Act is considered to be a disclosure to the world at large, and not just to the individual applicant. Confirming or denying whether this information is held would, in our view, be unfairly disclosing information that is an individual’s personal data.
Prior to services being contracted, NHS England would scrutinise suppliers’ financial standing and capability to deliver the required services and can withhold contracts from organisations where directors have been convicted of fraud or similar offences. Therefore, we consider there are other ways in which the legitimate aim in question for this FOI can be satisfied and there are less intrusive ways of meeting this legitimate aim. We therefore consider, it would be unfair in this particular instance to disclose an individual’s personal data and we do not have a lawful basis for processing this personal data (i.e. disclosing it under the FOI Act).
Question 3
Since July 2021, NHS England can confirm that it has contracted services from the Good Governance Institute on three occasions:
Between July and October 2021, a contract was signed by Health Education England for £47,982 for consultancy services for a review of executive governance to support the Accountable Officer.
Between October and December 2022, NHS England paid £74,650 for consultancy services for an engagement exercise to support the development of the next CNO for England Professional Strategy for nursing and midwifery.
In February 2023, NHS England paid £100 for consultancy services for conducting research with systems to inform the development of set of principles regarding system risk management.
Each of these contracts were contracted through specifying the service required rather than the number of days worked. Therefore, even if a certain individual had worked on behalf of this organisation whilst the contract was in place, NHS England would be unable to breakdown the information we hold as per parts 1(b), 1(c) and 1(e) of your request.
Contract B was approved by NHS England’s Nursing directorate and was approved by the budget holder, finance account manager for the budget it was raised from, and NHS England’s Commercial Panel in accordance with our Standing Financial Instructions. The Commercial Panel includes representation from the Commercial, Financial and Legal teams. In addition, due to the value and type (consultancy services) these procurements were referred to, and approved by, the Department of Health and Social Care’s (DHSC) Procurement team.
The procurement was below the PCR (2015) threshold and as such subject to the light touch procurement process. This does not require the use of the Standard Selection Questionnaire (SQ) mandated under PPN 8/16 for above threshold work.
We are able to generally advise that NHS England scrutinises the suppliers financial standing and capability to deliver the required services and can withhold contracts from organisations where directors have been convicted of fraud or similar offences but that power does not extend to the investigation of employees of the organisation.
Contract C was approved by NHS England’s directorate for the Chief Delivery Officer and was approved by the budget holder and constituted an offer of pro bono work with a nominal payment of £100.
The total amount that NHS England has spent on the Good Governance Institute since July 2021 is £122,732 (contracts detailed above).
Copyright
NHS England operates under the terms of the Open Government Licence (OGL). Terms and conditions can be found on the following link:
We hope this information is helpful. However, if you are dissatisfied, you have the right to ask for an internal review. This should be requested in writing within two months of the date of this letter. Your correspondence should be labelled “Internal Review” and should outline your concerns and/or the area(s) you would like the review to consider. Internal Review requests should be sent to:
Please quote the reference number FOI-2305-1971470in any future communications.
If you are not content with the outcome of the internal review, you have the right to apply directly to the Information Commissioner for a decision. The Information Commissioner’s Office (ICO) can be contacted at the following weblink:
Please note there is no charge for making an appeal.
Please do not reply to this email. This message has been sent from a central mailbox. To communicate with NHS England regarding Freedom of Information (FOI) requests, enquiries or complaints we ask these are sent directly to NHS England’s customer contact centre. This is to ensure all communications are progressed correctly. Their postal address, telephone number and email details are as follows: PO Box 16738, Redditch, B97 9PT; 0300 3 11 22 33, england.contactus@nhs.net.
By Dr Minh Alexander retired consultant psychiatrist 5 June 2023
Today Croydon Employment Tribunal is scheduled to hear a whistleblowing doctor’s claim against University Hospitals Sussex NHS Foundation Trust. The hearing is set to run until 16 June 2023.
This is a post to share a relevant report from a 2020 Health Education England review of core and higher surgical trainees’ experience at the trust, carried out after trainees raised concerns:
Trainees valued the supervision of some consultants but otherwise raised many safety and governance issues with the HEE reviewers. These included:
An “unpleasant”, “toxic” atmosphere
Poor behaviour by some consultants
“Trainees informed the review team of examples of bullying and undermining by a named consultant, towards both other consultants and trainees.”
“The review team heard that some consultants frequently demonstrated undermining behaviour at the morning handover for the upper and lower gastrointestinal (GI) team, for example criticism of the registrars’ management of patients and arguments between themselves.”
“Trainees described a recent incident where the named consultant had undermined a consultant colleague in a large meeting by repeatedly accusing them of being incapable of performing a basic surgical procedure.”
High complication rates and poor recording of clinical outcomes“
“The review team heard of a case in which a patient had received surgery on the wrong part of their bowel, resulting in recurrent readmissions.”
Trainees expressed concern at the apparent increase in death rates over a period of years, to levels which they felt were unexpected considering the demographics of the local population. Trainees reported they had requested this was investigated by the Chief Medical Officer. When asked, trainees confirmed that the Medical Director and Chief Executive had been made aware of these concerns.” [my emphasis] At the time of the review, the trust Chief Executive was Marianne Griffiths.
Lack of leadership in the department
“….a lack of ownership of emergency surgery patients.”
“The review team heard that some consultants frequently refused to review patients who were not going to theatre that day, resulting in trainees feeling unsupported when asking for senior advice on managing patients. The review team were informed that core trainees were often expected to act at a registrar level in terms of decision- making.”
Poor quality clinical work by locum doctors which was not well supervised
“Trainees reported a lack of confidence in the supervision provided by some locum consultants and provided examples related to clinical decision-making and dismissal of core trainees’ concerns about an unwell patient.”
“The review team were informed there were three gaps (two non-training and one training) on the registrar rota which are currently unfilled. Trainees reported consultants were aware of concerns about the capability of some locum registrars who had covered the rota but had responded that they were required to fill the gaps.”
“…..the review team were informed of a review of the last 100 elective colorectal resections performed (taking place between September 2019 and 3 February 2020), which indicated that the anastomotic leak rate was between 10.5-11.5% depending on the definition used to classify as a leak. The review team also noted of the cases reviewed: 14% returned to theatre, 12% experienced wound infections and 15% required readmission. Trainees reported they would not want a family member operated on by some of the consultants in the department.” [my emphasis]
“Trainees reported complications were inadequately discussed at morbidity and mortality (M&M) meetings due to the volume of complications.”
“The review team heard an example of a serious incident being closed down without sufficient review.”
“The review team heard that results of an audit showing that M&M does not meet Royal College of Surgeons guidelines had been shared with the Clinical Lead for General Surgery. Trainees reported they had also raised concern at the Local Faculty Group (LFG) around the accuracy of M&M data and received the response that all departments were struggling with this. The review team were concerned to hear of the lack of systematic governance of M&M data collection. Furthermore, the review team were informed that M&M meetings were not well attended by consultants and until recently minutes of the meetings had not been recorded.”
Trainees’ hours were not appropriately controlled and in some cases exception reporting had been discouraged.
“The review team heard that trainees regularly worked additional hours. When asked, trainees reported they did not submit exception reports because some consultants had discouraged F1 doctors from doing so. The review team were informed that the Guardian of Safe Working Hours had recognised a drop in exception reporting and approached a higher trainee regarding this. Trainees reported a lack of leadership and responsibility around exception reporting.”
Of great concern, the HEE reviewers were told that trainees were discouraged from raising concerns, including with HEE.
A senior manager was reportedly one of the individuals who had discouraged the raising of concerns:
“The review team were particularly concerned to hear of behaviours apparently intended to discourage trainees from raising concerns. The review team were informed that a consultant had sent an email to trainees ahead of the review, appearing to put pressure on trainees to provide positive feedback. Furthermore, the review team heard that a trainee had been told by a senior manager that those who raised concerns needed to appreciate the consequences of their actions in terms of the impact on service provision.”
The HEE reviewers clearly believed and took what the trainees reported seriously, as reflected in their list of mandatory requirements to the trust.
These included requirements for improved governance and resolution of the cultural issues:
“HEE require the Trust to develop robust clinical governance processes, in line with NHS England and NHS Improvement (NHSE/I) requirements, in relation to patient safety, complication rates and record keeping with regards to patient outcomes.”
“HEE require the Trust to carry out work to improve the culture and reduce the number of bullying and undermining incidents within the general surgical department.”
As part of the action plan on bullying, HEE required: “the Trust to consider an external review of the department from the Royal College of Surgeons.”
I understand that this RCS external review took place only last month, three years on from the original recommendation. I am asking the trust to confirm that this is so, and about progress in general on HEE’s requirements.
The National Guardian and CQC at Sussex
So in summary, HEE found very serious dysfunction in a major trust department, with substantial patient safety implications and reports of actual care failings.
Concerns about the death rates had been raised with Marianne Griffiths.
HEE also found evidence of suppression, including by a senior manager.
And guess who carried out a review of trust whistleblowing governance in July 2019, eight months before the damning findings by HEE in March 2020?
The former NHS National Freedom To Speak Up Guardian, Henrietta Hughes.
Her July 2019 review predictably praised the trust leadership for making improvements, and reflected none of the dysfunction found by HEE the following Spring.
CQC would have been informed of the Spring 2020 HEE review findings as part of multi-agency protocols. There is no record of a CQC inspection of trust surgical services in response to the concerns.
“CQC then received concerns about the UGI surgical service from staff and other stakeholders. We carried out an inspection of the elective UGI surgical service in August 2022 and found serious safety and leadership concerns.”
“We have continued to receive concerns from staff about the safety of the surgical services at the Royal Sussex County Hospital.”
“Some staff feared reprisal for raising concerns and others had simply given up because of ‘concern fatigue.’ This group of staff felt there was little point raising concerns because no action was taken when they did. When we asked staff to describe the culture of the trust, the feedback was mostly negative. Staff also felt the trust was a ‘hierarchical’ organisation which made it hard to get their voice heard.’
CQC also admitted in its briefing, upon release of its report:
“We continue to have repeated contact from staff who tell us feel unable to raise concerns through the trust’s own internal escalation processes.”
How many Sussex staff and patients suffered because Henrietta Hughes gave Marianne Griffiths et al a free pass in 2018?
Or because the CQC failed to act quickly enough on concerns, including those raised by HEE in 2020?
What is Hughes doing as the Patient Safety Commissioner?
And importantly, what do HEE’s findings of serious governance failings and suppression, CQC’s similar findings, and Sussex’s apparent failure to organise a timely external review of surgical services as advised by HEE – despite Griffiths having already been informed of rising death rates – say about Marianne Griffiths’ current investigation of North East Ambulance Service for NHS England?
UPDATE 10 JUNE 2023
Matters took a dramatic turn at the opening of the Sussex whistleblowing ET case on 5 June 2023 when the police asked to sit on evidence, because it was relevant to a criminal investigation of gross negligence manslaughter at Sussex. The trust subsequently asked for an adjournment on grounds of prejudice to their witnesses. But it means that the skeletons in Griffiths’ (and her former medical director now successor CEO) cupboard have tumbled out:
Alongside this, NHS England continues to resist questions, raised over the last year, regarding the legitimacy of the investigation of NEAS headed by Marianne Griffiths. In its most recent letter, NHSE took the bizarre and desperate step of pretending that it had no jurisdiction over NHS Foundation trust governance, in order to avoid addressing the issue:
“Trust-wide focus on making it easier for people to speak up and raise concerns, including stronger support for the Freedom To Speak Up service. Results from the anonymous monthly “Pulse” staff survey show more people now feel confident that the trust would act upon concerns that were raised, up from 49 per cent in September 2022 to 58 per cent in March 2023, closing in on the best-performing trusts nationally.”
Having 42% staff who do not believe concerns will be acted upon is not great cause for celebration. And that is if one accepts that the trust’s report / its pulse surveys are reliable. It is hard to imagine that any patients with botched surgery, leaky bowels, post operative infections and readmissions, or bereaved families, would be uncorking any champagne.
In April 2021, shortly before he was promoted to CEO, Findlay had these commendable aspirations on quality for patients and staff, as expressed in a video posted on Facebook by the trust:
“Welcome to University Hospitals of Sussex. My name is Dr George Findlay. I am Chief Medical Officer and Deputy Chief Executive. We’re absolutely passionate about providing the highest quality care for patients every time and the best environment for our staff to work in. We’re really clear about the continued investment in services and we’ll continue to provide accident and emergency services, maternity services, trauma services and special services in all the locations we currently do. We’re absolutely passionate about research and innovation and working with our partner universities. We’ll make sure that we adopt best practice, our best roles and make the best value of evidence for our patients for the future.”
RELATED ITEMS
University Hospitals Sussex NHS Foundation Trust resisted FOI requests about their current whistleblowing claims:
Dr Minh Alexander retired consultant psychiatrist 4 June 2023
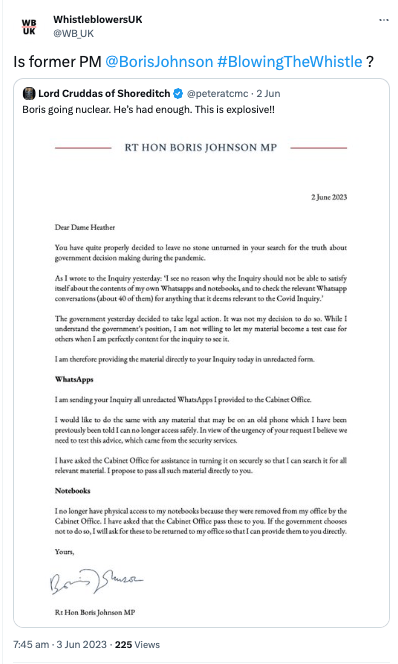
WhistleblowersUK the much criticised external secretariat of the also dubious Whistleblowing All Party Parliamentary Group (which has no official standing or powers), has publicly suggested that Boris Johnson might be a whistleblower for stating that he will cooperate with the UK COVID inquiry.
As might be expected, this has provoked strong reactions from genuine whistleblowers.
A hopefully self-explanatory enquiry to the Whistleblowing APPG is shared below.
From: REDACTED
Subject: WhistleblowersUK’s suggestion that Boris Johnson is a whistleblower, financial transparency and handling of whistleblowers’ personal data
Date: 4 June 2023 at 11:04:04 BST
To: REDACTED
BY EMAIL
All Party Parliamentary Group on Whistleblowing
4 June 2023
Dear Ms Robinson and colleagues,
WhistleblowersUK’s suggestion that Boris Johnson is a whistleblower, financial transparency and handling of whistleblowers’ personal data
I write to raise further serious concerns about your external secretariat, WhistleblowersUK.
On 3 June 2023 WhistleblowersUK tweeted to suggest that Boris Johnson was a whistleblower in respect to his claimed plans to disclose pandemic related documents to the COVID inquiry.
“Is former PM @BorisJohnson #BlowingTheWhistle?”
Mr Johnson is known for the opposite of telling truth. He was fined for a criminal breach of COVID lockdown laws, committed as prime minister. He currently faces further allegations about other breaches of the COVID lockdown.
He has been criticised for abrogation of responsibility during the pandemic. The many COVID policy failures under his premiership, such as the forced discharge of COVID positive patients into care homes, unnecessarily killed and injured thousands. The misconduct in public office that killed so many has been chronicled by Keep Our NHS Public.
Billions that could have been spent on public services, and on protecting the population from the clinical and economic effects of COVID, made their way into private pockets during his tenure.
He brought disgrace many times to his Office as prime minister.
Genuine whistleblowers find it appalling that WhistleblowersUK could suggest that Mr Johnson is any way a “whistleblower”.
It is a fundamental misapplication of the concept to apply it to the individual who was the controlling mind in our country’s tragic COVID misadventures. The many, many families whose lives have been changed forever by COVID losses deserve much better.
Moreover, it is most unfortunate to associate the term “whistleblower” with someone of Mr Johson’s character.
I acknowledge however, that under the US style bounty hunting model of financial rewards/ incentives that key members of the Whistleblowing APPG and WhistleblowersUK have sought to establish, that a criminal ratting out another criminal could be accepted as “whistleblowing” and rewarded. As in the case of Bradley Birkenfeld and other examples. If however, the APPG does not intend to replicate this aspect of the US model, please let me know.
I should add that the Chair of WhistleblowersUK has ignored a letter asking for clarification about WhistleblowersUK’s financial charges to whistleblowers seeking help, and the handling of whistleblowers’ data. Please see the correspondence forwarded below of 4 May 2023.
1. I would appreciate your comment on the tweet by WhistleblowersUK which equates purported compliance by a controlling mind with a public inquiry into gross failures with mass loss of life, to whistleblowing. Does the Whistleblowing APPG stand by the suggestion that Boris Johnson is a whistleblower?
2. I wonder also if the APPG would be kind enough to ensure that I receive a response from Tessa Munt on the outstanding questions on transparency about WhistleblowersUK’s financial charges to whistleblowers and WhistleblowersUK’s handling of whistleblowers’ highly sensitive data.
I previously raised questions of finances and conflict of interest with respect to WhistleblowersUK’s role as APPG secretariat in 2019. But this only led to Sir Norman Lamb’s resignation from the APPG because WhistleblowersUK refused to answer. The other APPG members were happy to continue with WhistleblowersUK as secretariat despite the lack of accountability and transparency. For the newer APPG members, my unanswered questions to the APPG in 2019 are documented here: Norman Lamb MP has resigned from the Whistleblowing All Party Parliamentary Group
A key issue arising from information on WhistleblowersUK’s website is: Does WhistleblowersUK share whistleblowers’ highly sensitive personal data with third parties such as NAVEX Global, and without disclosing that it does so?
Many thanks and best wishes.
Dr Minh Alexander
Cc
The Earl of Minto, Minister of State, Department for Business and Trade
Baroness Heather Hallet
Dr Philippa Whitford MP
Keep Our NHS Public
Lord Wills Whistleblowing APPG member
Lord Sikka Whistleblowing APPG member
Baroness Neville-Jones Whistleblowing APPG member
From: REDACTED Date: On Thursday, May 4th, 2023 at 4:08 PM Subject: Data processing by WhistleblowersUK To: REDACTED
BY EMAIL & Twitter
Tessa Munt
Chair of WhistleblowersUK
4 May 2023
Dear Ms Munt,
I am directing this to your council email address as I did not wish to sign into your private website, having noted the message displayed about data collected by the LibDems.
The current “Help me” section of the WhistleblowersUK website tells whistleblowers seeking help that their data is processed under the “WhistleB” process and overseen by WhistleblowersUK’s data controller. Could you kindly advise who is WhistleblowersUK’s data controller and whether any third parties have any role in processing the data of whistleblowers who contact WhistleblowersUK? For example, does WhistleblowersUK use dropboxes or digital platforms by third parties such as Navex Global? Please can WhistleblowersUk provide details of all third party involvement and also make such third party involvement clear on its website so that whistleblowers seeking help are fully informed? Also can WhistleblowersUK explain what the WhistleB process is?
Also, under“Our Purpose”, WhistleblowersUK now states that it provides “affordable” help. Can this be made be more transparent, and any financial charges for services to whistleblowers be explicitly published upfront? Also can any WhistleblowersUK’s requests for a share of financial settlements and awards be made explicit upfront? I ask as a document making indicating such charges and levies has never been published by WhistleblowersUK as far as I am aware.
Dr Minh Alexander retired consultant psychiatrist 1 June 2023
This is a brief post to share information about a disturbing failure by the Care Quality Commission to prosecute a private provider for egregious care failures. These failures led to an exquisitely vulnerable patient’s death, in a governance context of a regulatory revolving door.
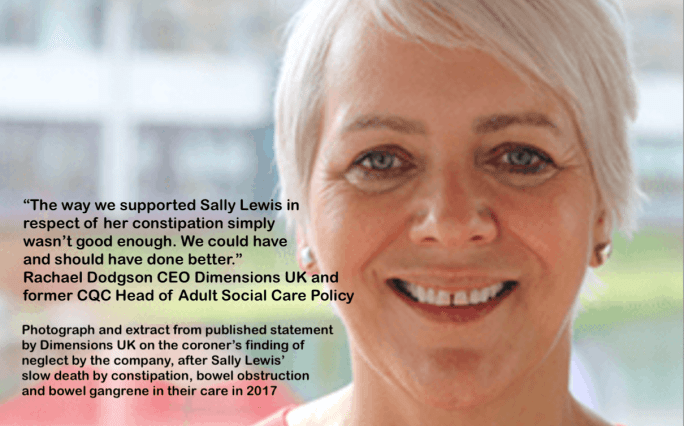
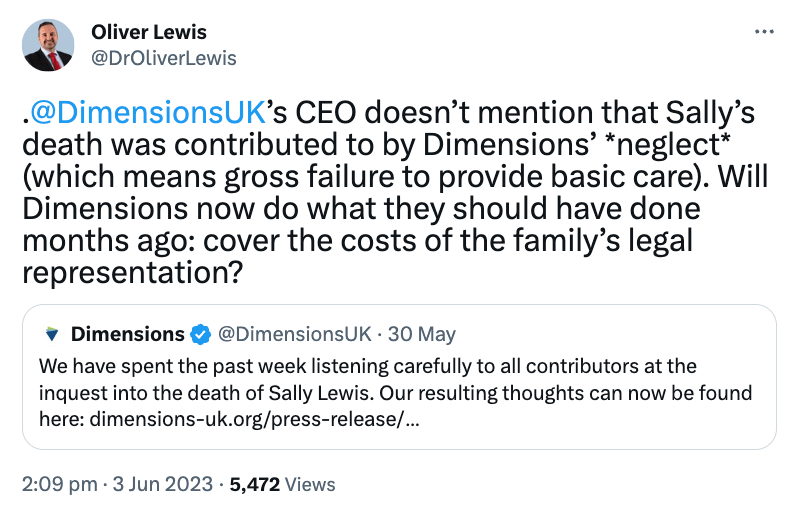
Sally Lewis had a learning disability and lived in sheltered accommodation run by the company Dimensions UK.
Sally Lewis died avoidably from constipation on 27 October 2017, a known risk in her case, because of a failure to follow a care plan to monitor her bowel function and to administer vital laxative medication. It was a very painful death, with sections of her bowel found to be necrotic (dead) at post mortem.
There were many opportunities to stop this deterioration, as her family repeatedly raised concerns with staff about a deterioration in Sally’s overall wellbeing and distension of her abdomen, but this did not prompt appropriate action.
I concentrate here on serious questions arising from CQC’s conduct.
CQC inspection background
Sally Lewis died at a Dimensions UK facility called The Dock.
A 2014 CQC inspection report gives the usual cursory, superficial account of the care one expects from CQC social care reports.
Laughably, as evidence of user choice, the CQC report produces the example:
“We heard a person being offered choice at mealtime. One staff said: “Would you like cheese or ham?””
As evidence of respect, CQC quoted what staff claimed they did:
“Staff told us how they demonstrated respect for people they were caring for. Staff said: “I knock on the doors”
CQC connection at Dimensions UK
Unattractive aspects of the CQC in recent years include the way in which some of its most senior officers have walked through the revolving door to highly lucrative jobs in the private sector, and links between the regulator and the regulated.
Months after retiring from CQC, David Behan CQC’s former CEO took up a job at the care home giant HCOne, and started arguing in parliament that people should pay a tax for their future care home care:
Even more outrageously, he was appointed by Dido Harding onto NHS England’s board despite his position on HCOne’s board, which one would have imagined created direct conflicts of interest. He also became Chair of Health Education England, raising similar concerns about conflicts.
Mike Richards former CQC Chief Inspector of Hospitals shortly after retirement walked into similar posts in the private sector but was also welcomed as a NED onto the board of the Department of Health.
Dimension UK’s annual report 2021/22 shows a turnover of over £200 million and places Dodgson’s remuneration in the pay band £180,000 to £189,999.
Was there any regulatory capture in the period following Sally Lewis’ death that affected CQC’s objectivity?
The CQC failure to prosecute for Sally Lewis death
CQC has the following legal time limits for bringing a prosecution for serious care failures:
“The CQC may bring a prosecution within a period of 12 months from the date on which sufficient evidence to warrant the prosecution came to their knowledge. However, this is limited to no more than 3 years after the commission of the relevant offence.”
“Under section 90(2) HSCA 2008 where CQC are investigating criminal offences into specific incidents under Regulation 22(2), 12, 13 or 14 RAR 2014, the statutory time-limits require that CQC prosecutions must be commenced within twelve months of the date at which sufficient evidence in the opinion of the prosecutor to justify a prosecution came to the prosecutor’s knowledge. Additionally, no prosecution can be brought where information is laid more than 3 years after the commission of the offence.”
CQC informed the BBC that it attempted to prosecute but the case was thrown out because the judge concluded that the CQC had erred in calculating dates.
Why did it take almost three years to prosecute such obvious and serious care failings, and where the link between the care failings and death were so clear?
Surely the risk to a prosecution of delaying until 2020 should have been obvious?
Rachael Dodgson’s apology
The coroner found neglect, a very serious outcome for Dimensions UK.
The company, via Counsel, reportedly tried to argue even at inquest that constipation was not a well known side effect of Sally’s medication regime of anti-psychotics (it was).
After the coroner ruled, Dodgson issued a most objectionable apology, woven with mulitple threads of organisational self-justification.
She failed to properly apologise for the fact that a vulnerable person died slowly in front of her organisation’s eyes despite frantic warnings by the family, by adding qualifications, casting blame on Sally’s behaviour, not fully acknowledging the scale of failure and importantly, not showing enough empathy or even reportedly making a personal apology to the family.
The apology was insensitively illustrated with this smiling image:
“As for suggesting you’d like to apologise to Sally’s family, if you really wanted to do that, you need to do it in person, to them, if they want to hear from you, not to the media. This is an almost carbon copy of how Southern Health behaved at the end of Connor Sparrowhawk’s inquest…”
But cutting through the distasteful corporatisation of an apology, there was some tacit if reluctant admission of the enormity of the failure: Dimensions UK admitted that serious harm from constipation is a Never Event. Although one would need to see their operationalised details to be sure that this is translated into future action.
“Our response following the inquest into the death of Sally Lewis
“The way we supported Sally Lewis in respect of her constipation simply wasn’t good enough. We could and should have done better. For that I am truly sorry and would like to apologise again to Sally’s family.
Our last CEO previously set out what had gone wrong, based upon our understanding at the time. The inquest has undertaken a deeper examination of the circumstances surrounding Sally’s death; it is clear that our processes, systems, management oversight and day-to-day support for Sally’s bowel management were not what they should have been.
That was almost six years ago and, in that time, a huge amount of organisational energy has gone into making things better. In the second half of this blog I am going to talk about what is different at Dimensions now and, just possibly, what others can learn from our experiences. But first, I want to talk about Sally, who is the most important person in all of this:
We supported Sally for 20 years. Sally was known to be at risk of constipation. Her medical records and prescriptions made that clear. And yet bowel monitoring was not done consistently and robustly. Yes, there were some ticks put into some boxes but not routinely, and whilst our colleagues verbally discussed Sally’s bowel movements between them, that wasn’t enough to make sure they, or Dimensions’ management, understood what was happening. We did not make our expectations to colleagues sufficiently clear in terms of recording. Furthermore, our systems and processes to check the quality of records and support weren’t delivered effectively. And this meant that nobody put all the pieces together. When Sally died, no-one around her realised she was constipated. And as a result, she hadn’t been receiving her PRN (“as needed”) medicine.
From the start we have said that one of the key issues here is how to balance individual dignity, privacy and rights with safety. Sally found it difficult for people to accompany her to the bathroom and this could trigger significant behaviours of distress for her. This meant that we couldn’t monitor how often she opened her bowels and the consistency, size and shape of her faeces. That issue stands but the key issue here was our acceptance of this. We should have raised this as a risk with her GP, the care manager, her family and with all those around her so we could work together to identify a way forward. I don’t think we did enough to help Sally herself understand why it was so important to be accompanied to the loo. And I don’t think we did enough to ensure our colleagues supporting her understood clearly the risks associated with long term constipation. I would like to turn to what is different at Dimensions now. Sally’s death has had a profound effect upon our organisation, and we didn’t wait for the inquest to identify the lessons we needed to learn, although following the Coroner’s findings we will reflect and consider carefully if there is any more we can do. We acted swiftly to make the necessary changes. We now have mandatory training for everyone supporting a person at known risk of constipation. We have a Bowel Toolkit which includes bowel management plans, improved bowel recording charts, a constipation screening and referral tool, guidance on how to prepare for a constipation appointment and more. It is an organisational requirement that all people we support are regularly screened for constipation and bowel health. Specialist advice is available from our Health and Wellbeing Lead.
Our electronic daily records system which is now fully embedded means it is much easier for managers to scrutinise all records relating to the people we support. And families also have access to these electronic records at any time from their own homes. There are, simply, many more pairs of eyes able to see what is going on. And we know that partnership working with families and loved ones results in better outcomes for the people we support.
Constipation is now one of seven ‘Never Events’ at Dimensions. Never events are a well-known concept in the NHS. Quite simply it means that, with the right training, behaviours, systems and processes, an incident that carries a potential risk of harm, injury or death should never happen. Specifically, at Dimensions, we say that “No one should suffer any harm as a result of a failure to administer or monitor the medication prescribed, or to follow established processes, for the relief or avoidance of constipation.” And we work to provide the right training and processes, and ensure the right behaviours, accordingly.
Our CQC registrations, previously held at Operations Director level, are now held by Locality Managers across our organisation to ensure that those directly responsible for the oversight of delivery of individual care and support are closer to the people we support. That’s a critical change; if any providers reading this have yet to make a similar change, I urge them to do so.
We have also undertaken a great deal of work externally to raise awareness of the risks and issues surrounding constipation for people with learning disabilities, to enable us and others to do everything possible to keep people at risk of constipation safe and well:
We produced an animation for our colleagues which has been used by the NHS, and this accessible book, funded by Dimensions and co-produced with Beyond Words.
Many colleagues have also devised extraordinarily creative ways of delivering what we continue to believe is a very important message, and one that we will continue to deliver. Sally’s inquest is an incredibly sad but important and timely reminder that we must always make sure support plans are clear, followed by our colleagues in how they support people, and that checks take place to ensure all those things are happening, whether that’s in relation to people’s bowels or any other areas of support.
I will end this by simply saying, to Sally’s family, I’m truly sorry. Nothing can bring Sally back but I’m determined that we will continue to do all we can to minimise the risk of this ever happening to anyone else.”
Rachael Dodgson, Chief Executive, Dimensions”
Sally Lewis’ family had no highly paid corporate lawyers or publicists.
They fought for an inquest and the truth of a loved one’s death on private means, and also endured the extra years of limbo caused by CQC’s scandalously late and unsuccessful prosecution.
They have a crowdfunding appeal for help with inquest costs:
I have asked the CQC for information under FOIA regarding its response to Sally Lewis’ death, multi-agency warnings about Safeguarding failure and its failure to mount a time prosecution. I have also asked whether in the light of Sally Lewis’ case and others, CQC should audit its application of Regulation 12 and I have sent a copy of the questions to the parliamentary Health and Social Care Committee, with a request that the committee consider CQC’s application of its responsibilities under CQC Regulation 12 at the next CQC accountability hearing.
The painful spectacle of the NHS denial machine grinding on at University Hospitals Birmingham NHS Foundation Trust (UHB) continues to embarrass us all.
Part of the prestidigitation is the performative exercise of allowing UHB to control a culture review on itself. This is akin to the useless models of internal Freedom To Speak Up arrangements for NHS whistleblowing and internal NHS arrangements for conducting Fit and Proper Persons investigations under CQC Regulation 5.
UHB, through a panel chaired by Roger Kline, has appointed a private company called “TheValueCircle” to carry out the culture review. TheValueCircle was set up by a former employee of the Good Governance Institute, another private company, which has many links with UHB managers and former managers, including Jacqui Smith former UHB Chair.
Roger Kline
Roger Kline was previously a Co-director of the now defunct organisation Patients First.
Roger Kline interacted with UHB prior to the announcement that he would chair a panel to select the organisation to conduct the UHB culture review.
A local media report confirmed in April that he had prior links with the trust:
“He confirmed he has prior links to UHB, having worked with some of the existing leadership in the past on a ‘fairness taskforce’ looking at staffing issues, but insisted he had ‘no interest’ in positioning the trust chiefs in a positive light if that was not what he found.”
It is remarkable that the UHB trust board, and ultimately NHS England where Kline was previously a director, even at this late stage, appear unconcerned about any appearance of potential conflict of interests.
TheValueCircle is notable in that one of its consultants is a CURRENT member of the NHS England board, Andrew Morris, as declared in the NHSE register of interests.
Several of its other consultants are former NHS trust directors, regulators and commissioners, some very recently stepped through the revolving door, such as Ian Hall who according to his LinkedIn entry was until June 2022 Regional Director of System Improvement, for NHS England Midlands.
This is the very NHS England region responsible for UHB and which is controlling the conduct of the UHB reviews behind the scenes, as revealed by PHSO correspondence, which is another topic for another day.
Unhealthy proximity, did I hear you say?
To understand TheValueCircle’s past work for the NHS, I looked for examples of other reviews and consultancy work. Strikingly, I found no past work product by TheValueCircle in the public domain. But I did find a comment on the company’s website about the fact that it did not produce much in the way of reports:
To find out more I requested, under FOIA, information from ten NHS bodies which appeared to have used TheValueCircle’s services in the past. They were mostly located in the West Midlands and North West regions. The results are provided below.
1)Walsall Healthcare NHS Trust
In an FOI response, Walsall reported it spent £119,232 on TheValueCircle for “Acute Partnership Development Support” and “Board Development Programme 2021/22”.
Astonishingly, the trust claimed that it held no data on which consultants from TheValueCircle carried out this work, any reports by TheValueCircle or whether NHS England had recommended the TheValueCircle.
2) Sandwell and West Birmingham NHS Trust (and false claims)
This trust and Walsall Healthcare NHS Trust are both chaired by David Nicholson, the former CEO of NHS England who was forced to resign after the scandal of the MidStaffs Public Inquiry.
He is now a major influence again in the West Midlands region, where it all started, as the chair of multiple NHS trusts.
Although Sandwell and Birmingham NHS Trust board papers recorded that Nicholson commissioned a review by TheValueCircle as one of his first acts as trust chair in, the trust FOI department bizarrely claimed to me that the trust had NEVER hired TheValueCircle.
“We have never commissioned this company for any consultancy work, advice or any services.”
When I pointed out that this was incorrect and supplied the evidence to prove this, the trust FOI department simply ignored me. Alongside this, I actually wrote to Nicholson to ask him if he had prior experience of TheValueCircle. He responded via a message from his office confirming that a review report had been produced but with a new narrative that it was not he but his CEO who had commissioned the review. He denied that NHS England had recommended TheValueCircle.
“From: REDACTED
Subject: RE: The Value Circle
Date: 18 April 2023 at 16:51:45 BST
To: REDACTED
Dear Dr Alexander
Many thanks for your email below.
Sir David has confirmed that he has not used The Value Circle previously. Sandwell and West Birmingham used them and I understand that they produced a good report which focussed heavily on the culture and behaviour elements of governance. This was requested by Richard Beeken the CEO. There is no connection with NHSE.
I hope the above is helpful.
Kind Regards
REDACTED”
Sandwell and West Birmingham did not respond properly to my FOI request until I complained to the ICO and I published my letter of complaint.
The day after, a response finally arrived indicating that the trust spent £28,200.00 on TheValueCircle’s services for a “Governance Review”.
The trust refused to disclose which consultants from TheValueCircle did the work claiming it was exempt as personal data.
Despite paying for and owning the review report on behalf of the public, the trust claimed it needed TheValueCircle’s permission to disclose it to the public:
“The report was prepared solely for the use of Sandwell and West Birmingham Hospitals NHS Trust. There is a disclaimer that the details may be made available to specified external agencies, but otherwise the report should not be quoted or referred to in whole or in part without prior consent. No responsibility to any third party is accepted as the report has not been prepared and is not intended for any other purpose. We have requested permission from The Value Circle as to what can be shared. We will respond once they have confirmed.”
The trust denied that NHS England recommended TheValueCircle and stated: “…they were chosen through a competitive bidding tender process.”
After a complaint to the ICO, Dudley Integrated Health and Care NHS Trust revealed it has spent £468K on TheValueCircle’s services since 1 April 2021. But it refuses to disclose any reports by the same, on grounds of personal privacy (Section 40).
This trust hired TheValueCircle to provide “training to our Board including a Well Led training session so that Board members would be further prepared for the then upcoming CQC inspection and also a Board Development programme.”
This cost £43,316.49 ex VAT.
The trust refused to disclose which consultants from TheValueCircle supplied the purchased services on grounds that disclosure would prejudice the conduct of public affairs. Really? Were the consultants current public servants?
The trust dubiously claimed that it could not disclose reports by TheValueCircle on grounds of commercial sensitivity.
It implied that NHS England had not recommended TheValueCircle:
“The Trust was made aware of TVC and other potential suppliers of Well Led reviews via a Trust Secretary network. TVC were appointed through a procurement exercise/tender by the Trust.”
5) Shropshire Telford and Wrekin ICB (and false claims)
ICB records clearly showed that TheValueCircle was hired to work on transformation of musculoskeletal services:
“To help shape the future ambition for MSK services, ICS organisations jointly commissioned The Value Circle to undertake a review of the current MSK transformation programme and make recommendations on next steps. The initial feedback which remains in draft form is attached in Appendix 1.”
However, the ICB claimed to me that it had never conducted any business with TheValueCircle.
This has been questioned and await a response.
6)Harrogate and District NHS Foundation Trust
No response.
I will be complaining to the ICO.
7)Liverpool University Hospitals NHS Foundation Trust
This trust spent £83,160.00 (inc VAT) by hiring TheValueCircle “work in partnership to develop a new risk management framework”.
The main man from TheValueCircle, David Cockayne, was the main consultant supplied, as is the case at UHB:
“David Cockayne, Chief Executive (The Value Circle LLP) was the senior sponsor supplied to co- ordinate the work undertaken with the Trust.”
Astonishingly, for £83,160.00 of public money spent, there is purportedly no tangible product to show for it:
“In accordance with Section 1 of the FOIA, we can confirm that the Trust does not record/collate the above information. We do not hold a final written report in order to answer Q4 of your request.”
The trust denied that NHS England recommended TheValueCircle in an interestingly worded reply:
“No external body recommended TheValueCircle to the Trust”.
8)East Lancashire Hospitals NHS Trust
This trust hired TheValueCircle to provide “Support to the development of the Provider Collaborative Strategy” and paid £193,065.90 inc VAT for this service.
The trust was reluctant to disclose which consultants from TheValueCircle provided the service, copies of their reports or whether NHS England had recommended TheValueCircle to the trust. It repeatedly gave the answer:
“The Trust does not hold this information centrally.”
I am requesting an internal review of this given reason for non-disclosure.
Until July 2021, the CEO of this trust was Kevin Mc Gee.
An apparent testimonial by Mr Mc Gee appears on TheValueCircle’s website:
I have asked Kevin McGee to kindly confirm that this comment was correctly attributed to him.
9)Blackpool Teaching Hospitals NHS Foundation Trust
This is another trust under Kevin McGee’s oversight as CEO.
The trust disclosed that it had hired TheValueCircle for the following jobs:
“From 19/20 the Trust commissioned 3 pieces of work:-
• a review of our Wholly Owned Subsidiary – Atlas • a review of our Divisional Structure and consideration of a Tertiary Division • a support piece of work for the Development of the Provider Collaborative for L&SC – this was commissioned by BTH but was for the entire PCB across Lancashire and South Cumbria.”
This all cost £350K.
David Cockayne was the main consultant for this project, as he is at UHB currently.
“David Cockayne, Chief Executive of Value Circle, was the lead contact for the projects, deploying various other consultants dependent upon the work.”
The trust refused to disclose any reports by TheValueCircle on grounds of commercial sensitivity.
Most incredibly, the trust also refused to disclose whether or not NHS England had recommended TheValueCircle on grounds of commercial sensitivity.
Shurely shome mistake?!, I hear you cry.
Surely no one at NHS England has a commercial interest in TheValueCircle getting lucrative NHS contracts?
I am requesting an internal review of these claimed exemptions.
The last but possibly the most important example:
10)North East Ambulance Service NHS Foundation Trust
As the NEAS deaths cover up and coronial misreporting scandal swirls on, compounded by the appointment of Marianne Griffiths as an investigator despite her controversial history with whistleblowers, who is found in the mix but TheValueCircle.
I discovered that TheValueCircle had been hired from NEAS financial transparency data , which showed that the trust CEO had authorised a payment to the company in December 2022 for “external consultancy”.
In response to FOI questions, the trust disclosed that it had hired TheValueCircle to undertake a “Well Led Independent Review” at a cost of £79,253 ex VAT and a “Full review of Trusts Governance and Assurance Framework” at a cost of £127,660 ex VAT.
TheValueCircle consultants who did the work were Sue Hillyard, Maggie Boyd a former NHS Improvement director in the Midlands and East Region and David Cockayne.
With desperation, and despite the massive and obvious public interest arguments, the trust claimed that it would be prejudicial to the conduct of public affairs if the reports produced by TheValueCircle were shared:
“Frankness and candour are essential for good decision-making. We believe that disclosure would be likely to prevent future reviews taking place with an honesty and candour needed to ensure that corrections can be made to improve our services.
We are therefore unable to release this information and apply section 36(2)(b)(i)&(ii) and section 36(2)(c) exemptions. This exemption states that information is exempt information if, in the reasonable opinion of a qualified person, disclosure of the information under the legislation:
(b) would, or would be likely to, inhibit – (i) the free and frank provision of advice, or (ii) the free and frank exchange of views for the purposes of deliberation, or (c) would otherwise prejudice, or would be likely otherwise to prejudice, the effective conduct of public affairs.
The documents requested and subsequently withheld contain the findings and opinions from external reviews that, if made public, would likely inhibit the future frankness and candour that we require to ensure our decisions are robust and informed.
In my reasonable opinion, this would likely damage the quality of advice and deliberation and lead to poorer decision making in the future. It would also inhibit the necessary frankness and candour of our staff if their discussions were made public.”
It is striking how the NHS will argue that night is day and vice versa when it suits.
When it is inconvenient, as at NEAS, embarrassing findings are hidden behind the wall of Section 36 exemption.
When it is less inconvenient, they may be published in full.
Here is an example of a fully public Well Led Review report on another NHS trust, of which Maggie Boyd was also a co-author:
NEAS also denied that NHS England recommended TheValueCircle:
“The Value Circle was not recommended by another body. Procurement exercise completed for Well Led Independent Review and further work on Governance and Assurance Framework required rapid completion post CQC inspection.”
So there you have it dear reader, UHB which has been severely criticised for secrecy and marking its own homework, allowing cover ups of patient safety and staff abuse, is being allowed to mark its own homework again using a private company about which there is studiously little transparency despite large amounts of hard public cash changing hands.
So far, even with three of ten trusts failing to respond to the FOI requests, over a million pounds were spent on TheValueCircle with nothing tangible in the public domain to show for it, even with a major scandal and many lives lost at North East Ambulance.
Why should highly paid NHS trust executives pay others with our money to do their jobs for them?
In times of austerity, when the lowest paid NHS frontline have to rely on foodbanks and 7.3 million patients wait for treatment, is not an obscene sight that money is frittered away in this fashion?
If these highly paid executives are incapable of doing their jobs, they should be shown the door. But oh, wait, there is still no sign of any implementation of the Kark review which the current Secretary of State himself commissioned but reportedly has stifled. He has not replied to a letter of 7 February 2023 asking him to reconsider his decision to reject Tom Kark’s recommendation of a disbarring mechanism. I have written once more:
As a little bonus feature, I should draw attention to the fact that one of TheValueCircle’s featured consultants Margaret McCabe is advertised as a NLP practitioner.
Her arrival was announced by David Cockayne himself.
NLP has been described as “pseudo-scientific”, “folk magic”, a “quasi-religion” and a New Age “psycho-religion”.
The inspection took place just after BBC Newsnight broadcast about poor culture and mistreatment of staff at the trust. The CQC claimed it inspected “due to a number of concerns raised by patients and their families around the care and treatment they had received”.
The warning notice on under-staffing was served partly as the CQC found that patient falls, some with serious harm, occurred DURING the inspection:
“Staff knew about and dealt with many specific risk issues. However, in many ward areas staff told us about their concerns over the number of falls and patients with pressure damage due to staffing pressures preventing them from taking appropriate, preventative action. On the first day of our inspection, staff reported that they had unfortunately had 2 patients fall due to being unable to provide the supervision the patients were assessed as requiring.
“The service did not have enough nursing and support staff to keep patients safe. During our inspection we found most wards were operating below national guidance for safe staffing levels. The Royal College of Nursing recommend safe staffing levels of 1 qualified nurse to 6 patients. Staff told us shifts were regularly planned for 3 qualified members on staff each shift, however this regularly reduced to only 2 qualified staff members working on the shift. Even with 3 qualified nurses on each shift, this would still have been outside of the recommended safe staffing levels. On the 13 December 2022, we found Ward 16 which had medical outlier patients admitted at the time were reduced to 1 qualified member of staff for 26 patients, at the time of our visit. The registered nurse was supported by a trained nursing associate. On the 13 and 14 December 2022, we found Ward 9 had a ratio of 1 nurse to 17 patients on both days of our inspection. Staff told us the ward had a high acuity as they had a large number of patients with complex needs, many of whom required 1:1 supervision. At the time of our inspection, staff were unable to provide this due to the unsafe staffing levels. On the first day of our inspection, Ward 9 reported 2 falls as they were unable to provide the 1:1 support for them. One patient did not sustain serious harm, however, 1 patient was awaiting a head CT scan and undergoing neurological observations due to the fall. Staff told us this was not a rare occurrence due to the challenges they faced with staffing.
We raised our concerns about staffing during and after our inspection and issued the trust with a Section 29a Warning Notice advising them of timely improvements needed to be made due to serious safety concerns.”
Another UHB hospital has now been criticised in relation to a patient fall which resulted in death.
On 19 May 2023 the coroner issued a Prevention of Future Deaths report after the death of 77 year old Norma Bruton who had an unwitnessed fall at Heartlands Hospital, resulting in a fractured neck of femur and her death seven days later.
The death occurred on 22 October 2022, shortly before the unannounced CQC inspection of Good Hope Hospital in December 2022.
“She had an unwitnessed fall on the morning of 15 October 2022 when trying to walk the short distance to her bathroom and sustained a right fractured neck of femur for which she underwent surgery on 20 October 2022. Mrs Bruton’s condition deteriorated after the surgery and she died in hospital on 22 October 2022.”
The coroner identified a concern about UHB’s falls risk assessment process and failure to take trailing attachments such as drains and drip lines into consideration as risk factors.
Bewick’s rapid review of clinical safety at UHB, published in March 2023 claimed that UHB was safe overall, despite Bewick’s awareness of the CQC warning at Good Hope Hospital. Bewick’s report maintained that mitigations were in place.
The issues of serious understaffing across all UHB sites, about which staff have been whistleblowing for years according to UNISON and others, supported by regulatory findings, long A&E waits and rates of avoidable harm from falls, are not consistent with a conclusion that clinical care at UHB is reliably safe.
I am sending the PFD on Ms Norma Bruton’s death to the Care Quality Commission with respect to Regulation 12 issues. The Coroner has already sent it to NHS England.
NB I am occupied with a family matter at present so apologies if I am slow to respond to correspondence. Best wishes.
RELATED INFORMATION
A previous UHB FOI disclosure revealed that there were 30 fractured necks of femur resulting from inpatient falls in the period 2012/13