By Dr Minh Alexander retired consultant psychiatrist 17 July 2026
Summary
This is a brief post to share a report commissioned by Cambridge University Hospitals NHS Foundation Trust (CUH) into whistleblowing governance, as applied to consultants and SAS (specialty, associate specialists and specialist) doctors at the trust.
A low response rate and disturbing insights into the experiences of doctors raising concerns paint a dismal picture. Lowlights include a universal lack of faith that raising concern will lead to action, normalised patient safety risks due to this organisational inaction, passive aggressive managerial silence in the face of concerns raised and identification of several departments as managerial trouble spots. These are neurosciences, emergency medicine, paediatrics and some surgical specialities.
The report
This has been commissioned by CUH following the Stohr orthopaedic surgery scandal .
Independent reviewers Verita who reported on the Stohr scandal previously observed:
The recent medical whistleblowing “listening exercise” ran between April and May 2026 and was conducted by Transformation Partners in Health and Care, an NHS based health consultancy.
It was a mixed method exercise, including a survey.
The key lines of enquiry for the exercise were:
“The KLOEs span eight distinct themes related to medical voice. Section five aligns qualitativeand quantitative findings to these to outline consultant and SAS doctor experience.
1. Psychological safety and voice
2. Representation, credibility and fairness of voice
3. Risk, early warning and organisational intelligence
4. Learning, prioritisation and visible ownership
5. Follow-through, trust and confidence
6. Inclusion, belonging and equity of experience
7. Blind spots, strategic gaps and unmet priorities
8. Surfacing best practice
The authors claim:
“All data collected through this process was handled with strict attention to confidentiality and ethical principles. Contributions were analysed by a small team, to reduce the number of people reviewing outputs. Anonymous quotes found within this report have been included and signed off by interview participants themselves or by written consent via the survey. No raw data has been provided to CUH.”
I could find no other information on data handling/ storage.
Results
The exercise engaged only 19% of target staff, in itself an indication of poor culture and staff hesitancy.
The data gathered represented:
128 survey responses
45 interviews
7 meetings
The survey authors noted “Many participants have had poor experiences of previous organisational leadership within CUH.”
Importantly, crude survey responses gave a better impression of whistleblowing governance than detailed qualitative responses.
This has implications for the national NHS staff survey, which relies only on a few simple questionnaire indicators about staff whistleblowing experience.
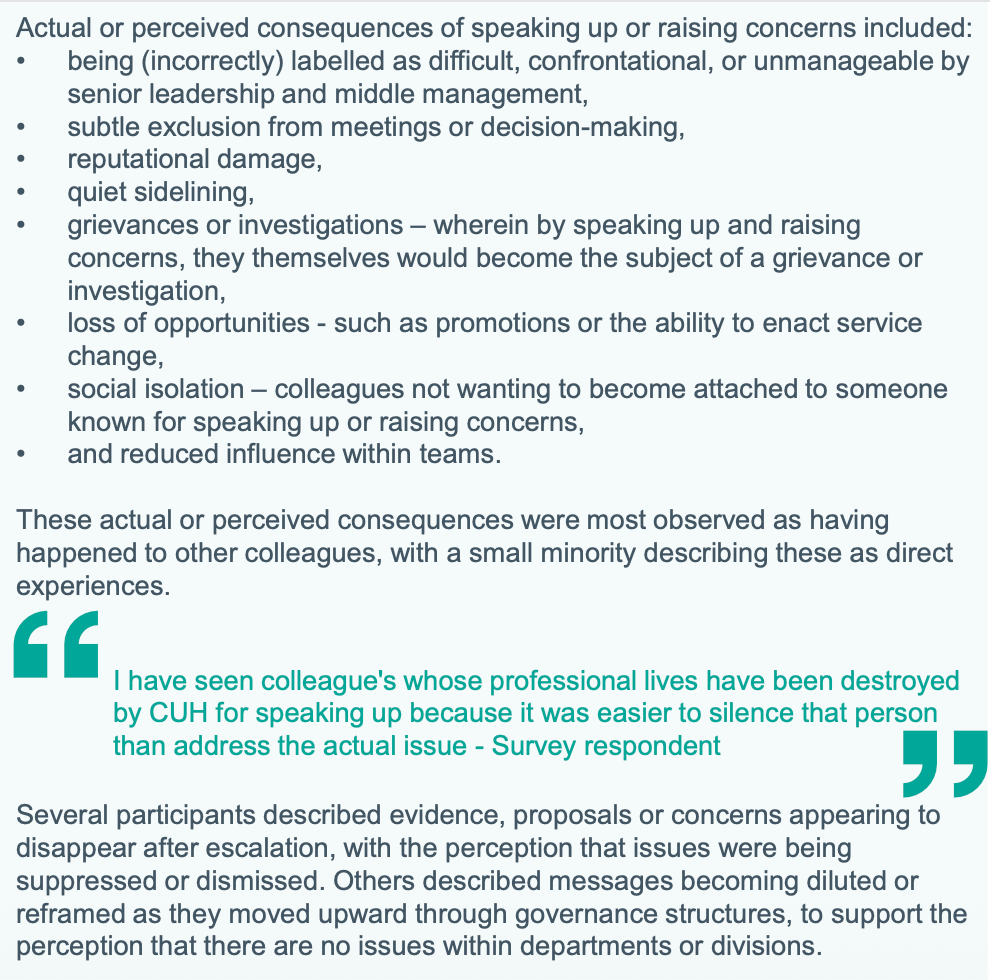
Some staff described severe symptoms of anxiety such as dissociation (feeling detached from reality and surroundings) with regards to whistleblowing. Others reported seeing colleagues “destroyed” for speaking up, as part of a range of typical whistleblower detriments.
Doctors are in an impossible situation because they are ethically obliged to raise concerns, but know that doing so carries risks, sometimes serious.
Importantly, according to respondents, CUH departments which were associated with particularly bad leadership and whistleblowing governance are neurosciences, emergency medicine, paediatrics and some surgical specialties:

Unsurprisingly, the Freedom To Speak Up model was questioned and staff expressed a lack of confidence in whether neutral support “genuinely” existed:

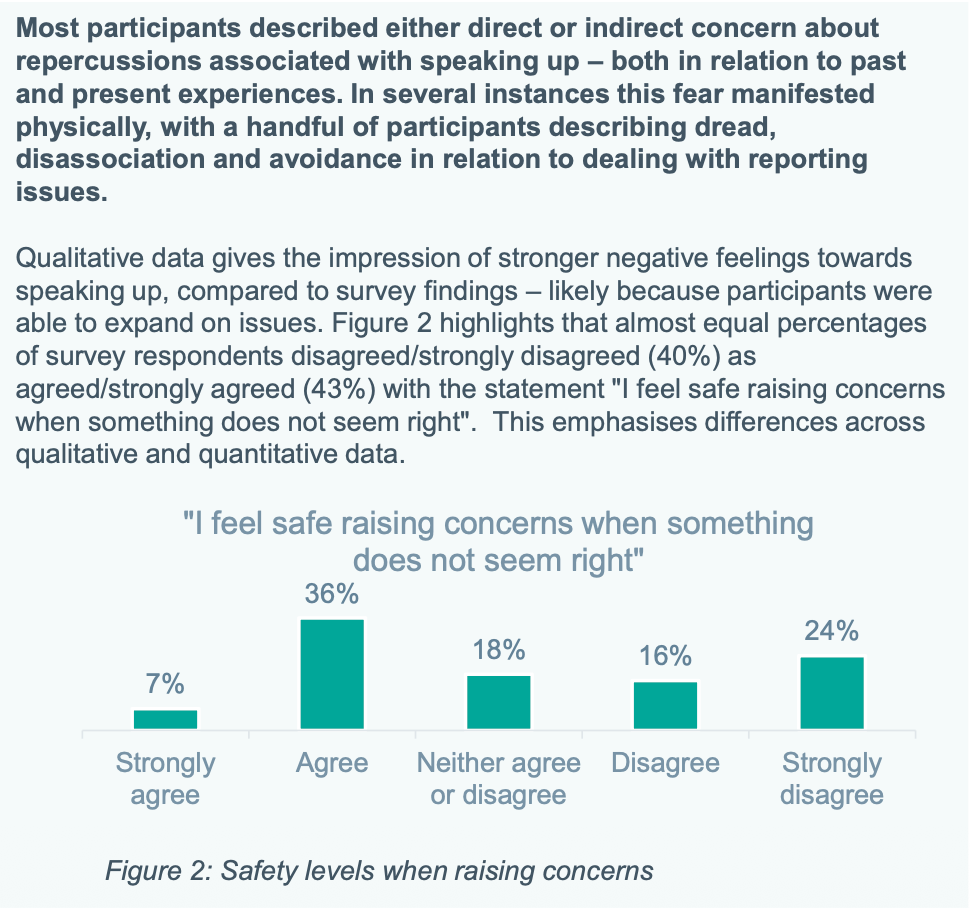
Echoing repeated national NHS staff survey findings, there was “universal” lack of confidence in whether speaking up led to change. The results at CUH were more extreme than the national staff survey:

Not unique by any means to CUH, some of the review participants reported that concerns were sometimes met with silence:
“Many talked about often not even getting a response or acknowledgement when they raised issues.”
As an aside, staff should understand that this silence is a form of passive aggression by managers, and is in effect a warning to desist.
Should the unfortunate member of staff press their concerns, the risk of active management reprisal increases.
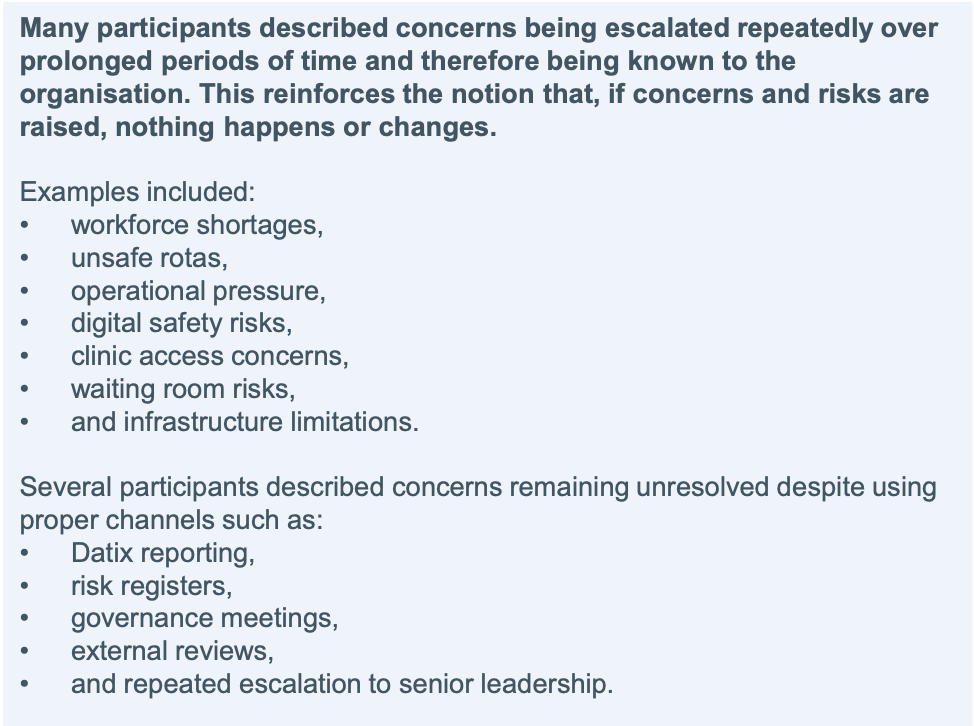
Respondents described a picture of unsafe conditions becoming normalised:
“Participants frequently linked deteriorating psychological safety with systemic workforce shortages, burnout, corridor care, service targets and on-going investigations/patient safety issues. The perception being these issues are never resolved and, worse, have become normalised.”
The typically normalised risks were as follows:
Doctors were concerned that CUH prioritised financial and reputational considerations:
“Many participants described concern that organisational prioritisation is perceived to be driven more strongly by operational, financial and reputational pressures than by frontline clinical experience.”
Related to the failures of listening up, doctors also reported serious flaws in trust consultations and investigations. For example:
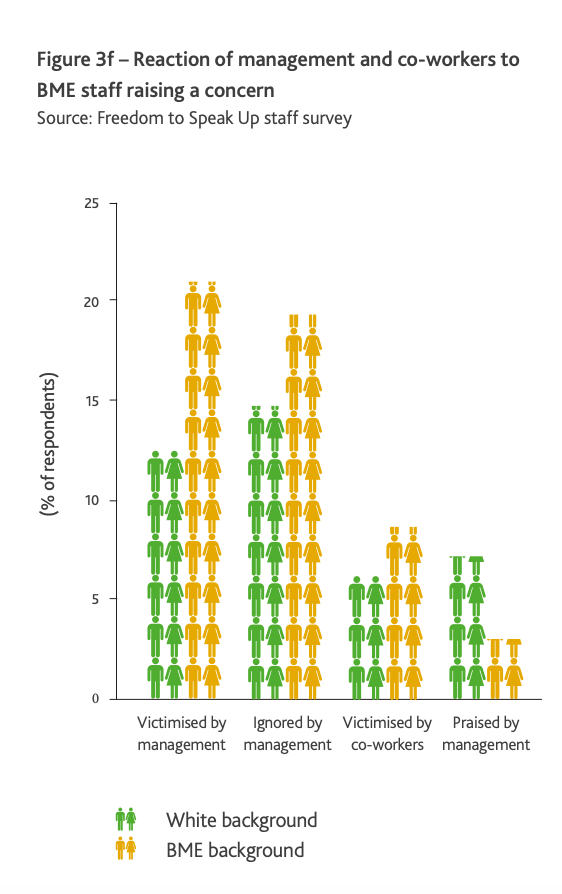
The survey found that SAS doctors and internationally trained consultants had worse experiences of whistleblowing governance:
“….SAS doctors and internationally trained consultants were perceived as less likely to feel comfortable speaking up or being heard”
This replicates findings from the original 2015 Freedom To Speak Up review, thus demonstrating that little has changed.
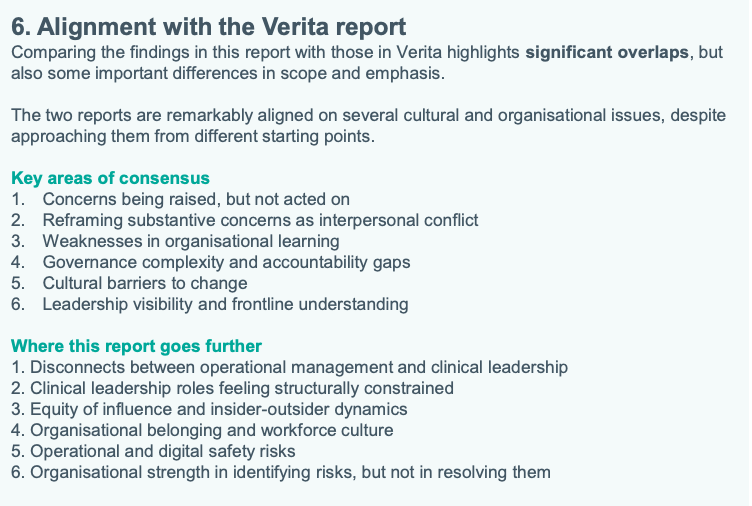
The authors felt their review uncovered additional issues that had not been identified by the Verita investigation into the Stohr scandal, and that cultural problems and organisational risks ran deeper:
Lastly, I must declare that I have fairly extensive experience of health services in this region as a carer. This includes, over the years, experience of care failures and cover ups. CUH has had its ignominious moments, but was not the worst. And at times it was much better than average. What on earth does that say about the health of our NHS?
ADDENDUM
I do not recommend that NHS staff use internal mechanisms for whistleblowing. The likely gain for the public interest set against potential harm to the whistleblower is unlikely to justify such a course. Instead, directing disclosures to the media either anonymously or with agreement of anonymity is safer. It is best to take advice as each individual’s circumstances are unique and it is a very personal decision. For example, someone earlier in their career with a young family to support has much more at stake than someone nearing retirement, who can afford to weather any financial consequences. It should also be noted that if you whistleblow externally and anonymously, and you are suspected and victimised, an employer may be able to claim that they did not know that you were a whistleblower. Take advice and consider options carefully. Equally, not all whistleblowing ends in disaster for whistleblowers, but whistleblowing about serious matters which threatens organisations or senior individuals is more likely to attract reprisal. Especially if a whistleblowers persists with their concerns.
RELATED ITEMS
At the Lampard public inquiry into failures at Essex Partnership University NHS Foundation Trust on 15 July 2026, Brian O’ Donnell clinical lead gave evidence that senior managers asked him to get rid of 4000 unresolved incident reports, dating back years:
https://www.bbc.co.uk/news/articles/c6212klngkko
He believed there was a panic as a result of the public inquiry.
4000 incident reports sitting on dusty shelves would have sent a very clear message to EPUT’s workforce.

