
By Dr Minh Alexander, NHS whistleblower and former consultant psychiatrist 7 November 2019
Clad in off-the-shoulder-black-hole-noir, Servalan Supreme Commander of the Freedom to Speak Up Division has rewarded NHS Trust Rotherham, Doncaster & South Humber NHS Foundation Trust (RDASH) with the ‘Freedom to Speak Up Organisation of the year award’.
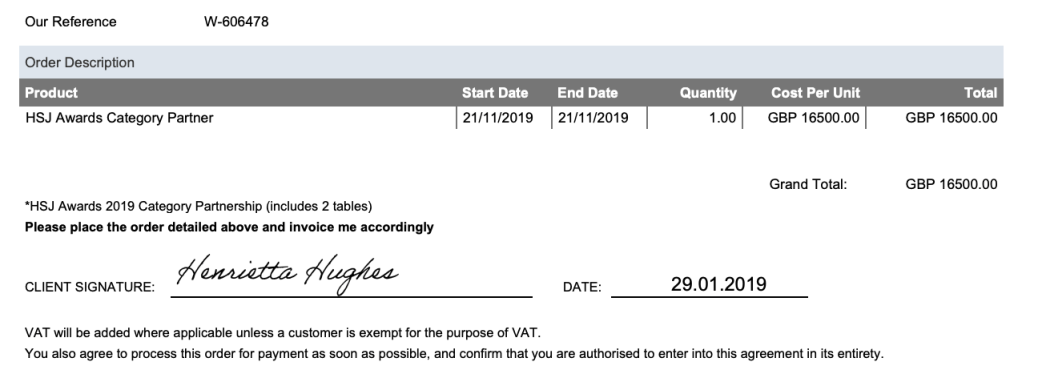
The Supreme Commander pays the Health Service Journal 16,500 Terran Federation credits a pop to sponsor this award, with the following benefits:
“…it comes with a range benefits including being involved in the criteria creation, judging panel and the publicity and platform which goes with that”
Yup, Servalan weighs in on the award of her own award.
| No expense spared on the latest reality-altering devices
National Guardian’s Office HSJ Award Sponsorship Partnership agreement
|
So how has RDASH pleased the Supreme Commander and what services has RDASH contributed to the Terran Federation?
Unfairly sacking a worker with post-natal depression:
Ms K Payne v Rotherham, Doncaster and South Humber NHS Foundation Trust Case No. 1800475/2016
Handling 63 Speak Up cases in 2017/18 and 2018/19 with only 2 reported instances of detriment
| Reporting period | No of cases raised with RDASH Speak Up Guardians | Cases with an element of patient safety | Cases featuring detriment, as reported by RDASH Speak Up Guardians |
| Q1 2017/18 | 2 | 2 | 0 |
| Q2 2017/18 | 8 | 2 | 2 |
| Q3 2017/18 | 12 | 3 | 0 |
| Q4 2017/18 | 3 | 1 | 0 |
| Q1 2018/19 | 10 | 5 | 0 |
| Q2 2018/19 | 13 | 5 | 0 |
| Q3 2018/19 | 12 | 3 | 0 |
| Q4 2018/19 | 3 | 1 | 0 |
| Total | 63 | 22 | 2 |
Source: Speak Up data published by the Supreme Commander, reported to her by NHS Trust Freedom To Speak Up Guardians, subject to no verification
https://www.cqc.org.uk/national-guardians-office/content/speaking-data
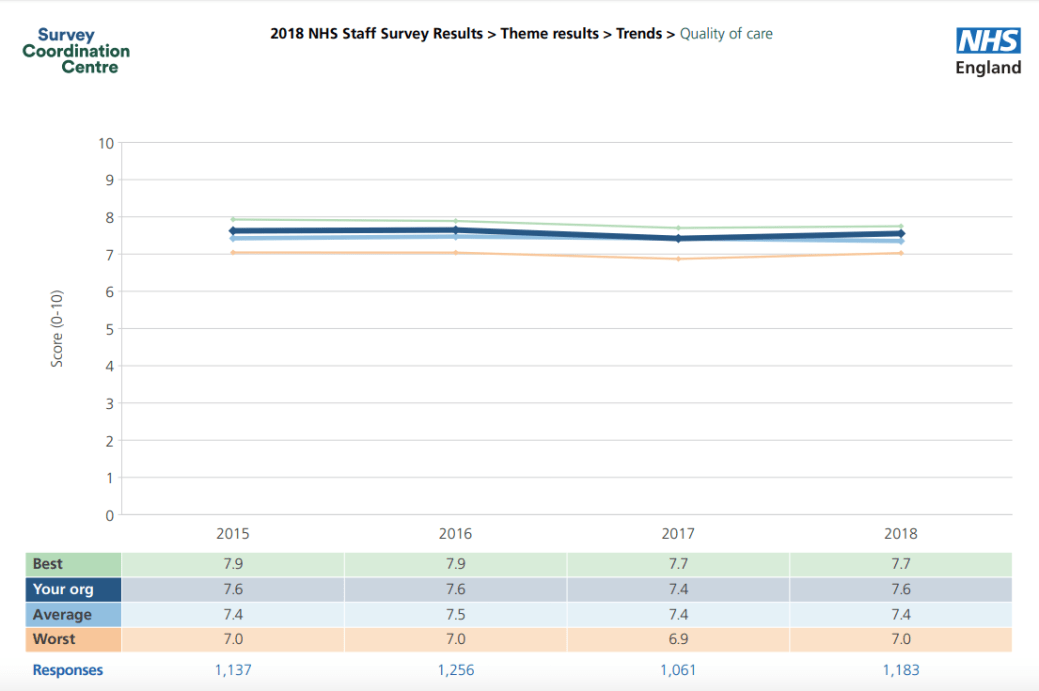
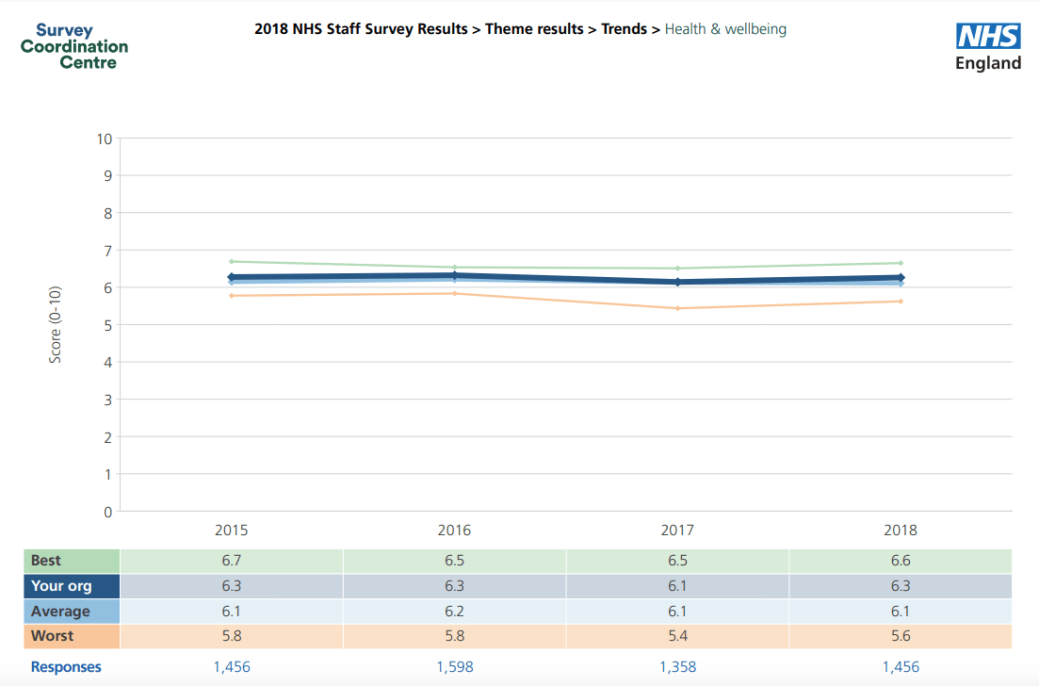
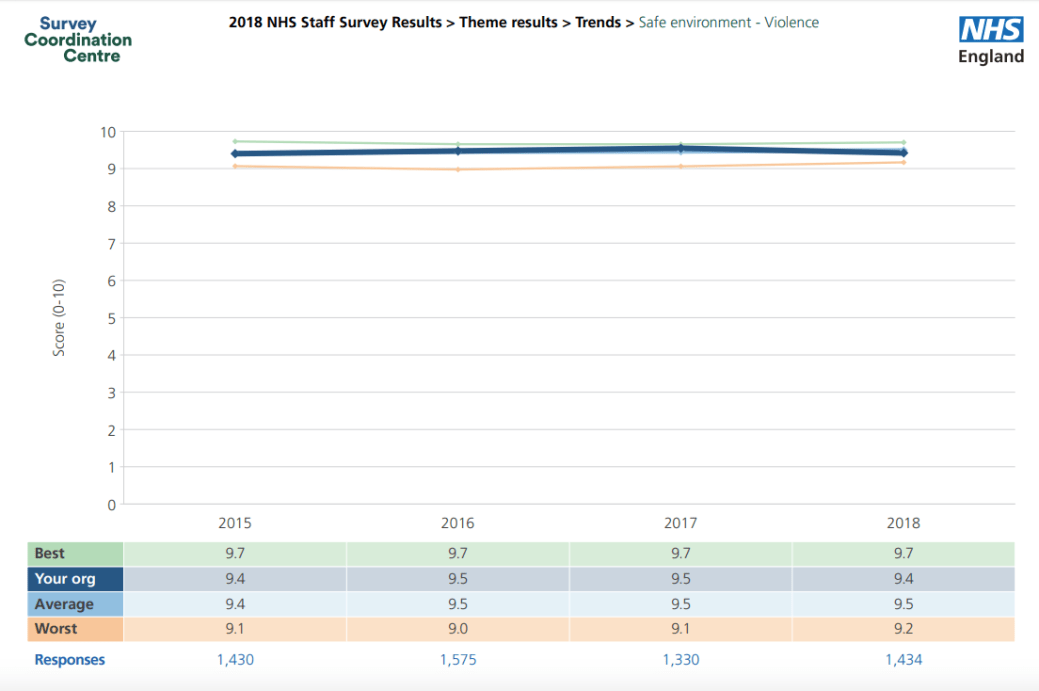
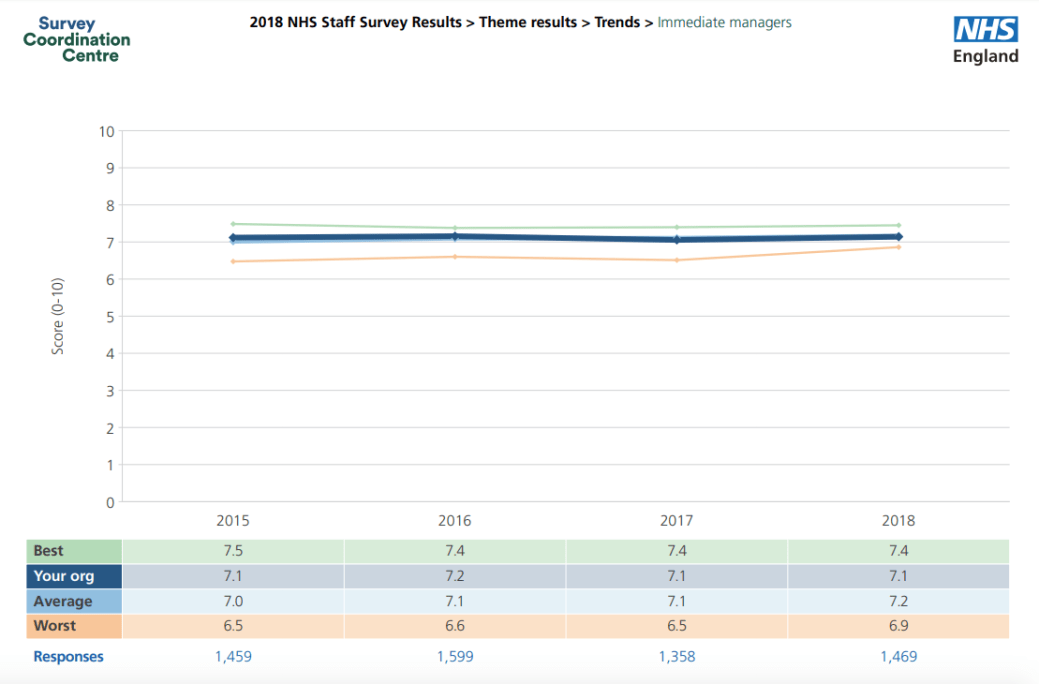
Making no apparent difference to trust staff feedback metrics as measured on the annual NHS staff survey since Freedom To Speak Up Guardians were established at the trust
The RDASH staff survey 2018 report can be found here.
According to Federation agents, RDASH colony morale has shown no troublesome blips following the introduction of Freedom To Speak Up Guardians.
In fact, central control notes there has been a pleasing, slight deterioration in scores on speaking up and overall score on safety culture.
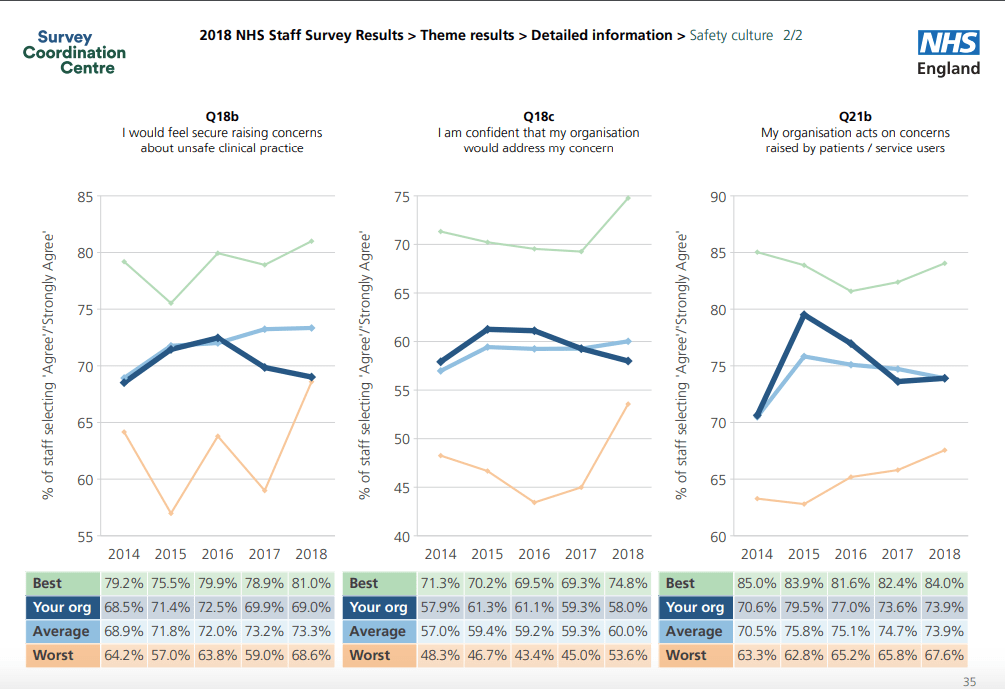
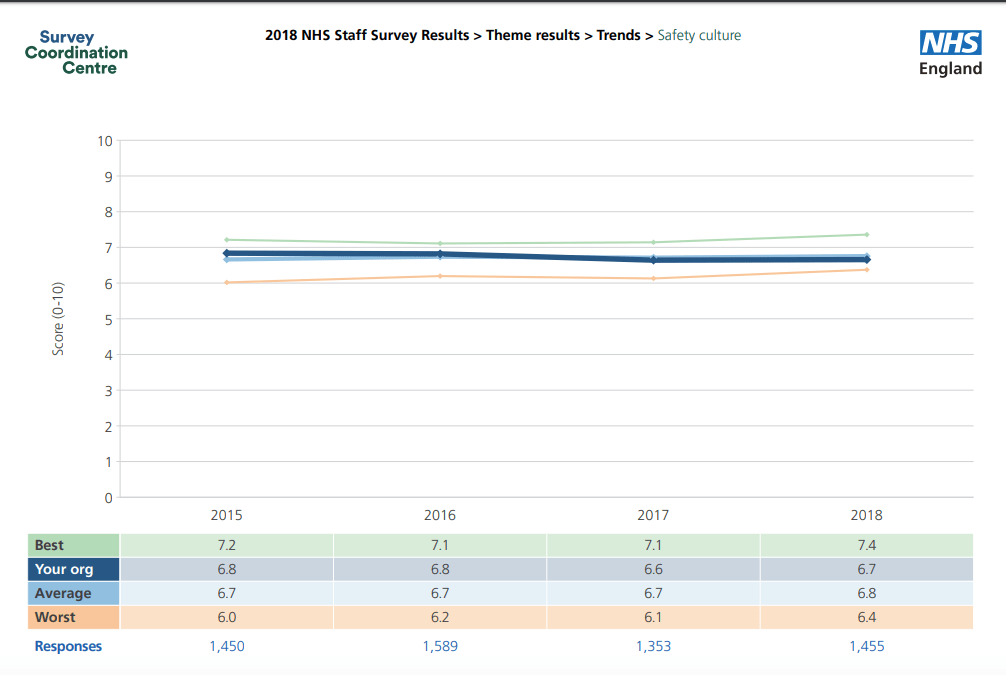
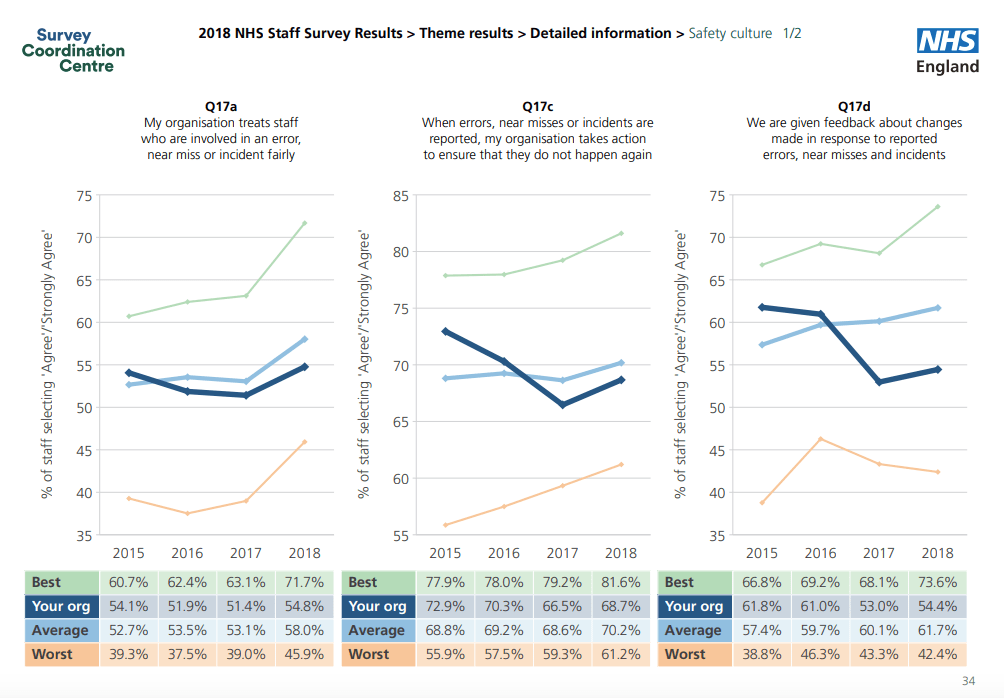
Other domains are calmly flat.
Not acting on staff concerns about safe staffing
A trust patient Robert McNeill, 60, died at Great Oaks Hospital in Scunthorpe after being attacked by fellow patient Jamie Reed in January 2017.
Staff had raised concerns about inadequate staffing levels before the killing.
A BBC report 4 September 2019 gives summarised details:
Great Oaks Hospital: Staff had safety fears before patient killed
“In a statement, RDaSH said: “We are sorry that staff felt anxious.”
This is the homicide investigation report by the company Niche, commissioned by NHS England and published September 2019:
“1.23 It is our view that the staffing levels and skill mix on the ward had a significant impact on the conditions in place at the time of the incident. However, the most significant was the observation policy. If the observations had been carried out differently it would have reduced the likelihood that Mr A would have been able to go into Mr O’s room and be undisturbed for 15 minutes.
1.24 We heard that staff had been anxious about risk assessment and risk levels within the unit. There were examples of:
- patients being brought to the unit without adequate consideration of their motivations for admission or previous criminal activity;
- staff raising concerns that a particular part of the ward was not safely staffed;
- differences in how risk assessments and risk ratings were applied.
1.25 This in practice meant that risks were not adequately controlled and caused staff to be anxious about their own and patients’ safety. Staff reported that they did not feel safe, particularly on nights and on the part of the ward where they had raised concerns about staffing.
1.26 In our view the most significant contributory factor is the culture of safety on the ward. The tolerance of uncontrolled risk meant that staff did not have the resources or plans in place to manage risks effectively. We cannot say that Mr A would not have subsequently killed someone, but we can say that promoting a culture that is less tolerant of risk will reduce the likelihood of patient harm in the future.”
The Niche investigation was critical of the trust’s own investigation:
“7.25 The internal investigation was asked to consider previous safety concerns regarding MHU2, and whilst the report discusses progress made since concerns were historically identified, it does not draw any correlations between what was said in previous reports and what happened in this case. Despite many attempts being made to address previous safety concerns it is apparent that staffing levels, clinical leadership, record keeping, and risk assessment remained problems on the ward in 2017. The report does not make this clear.”
7.26 Our review of the report indicates that there was no comment on how the unit complied with national statutory obligations, guidelines or policies and procedures, although the report does have some references to internal protocols not being followed. There is no mention of whether Mental Health Act paperwork was correctly applied or updated, no consideration of either patients’ treatment compared with Care Quality Commission regulations (for example regarding seclusion records or safeguarding practice), National Institute of Health and Clinical Excellence guidelines, British National Formulary prescribing guidance, Royal College of Psychiatrists, Royal College of Nursing recommendations or otherwise.
7.27 Because of these omissions, the investigation report does not make clear what went wrong, what happened that should not have happened and what did not happen that should have happened in chronological order. The investigation report does not clearly identify issues as care or service delivery problems and does not draw out issues specifically as contributory factors.
7.28 There is a statement that there was nothing that the staff did not do that could have prevented the incident (paragraph 15.5 page 70). We disagree with this statement in that if staff had not been congregating in the communal area, one member of staff may have been patrolling the bedroom areas which may have meant that Mr A may have been seen entering Mr O’s room. In addition, if observation practice had been less routine and predictable to Mr A he may not have taken the risk of entering Mr O’s room at that time. In essence both those points are possibilities, rather than certainties, however this does not make either situation unlikely.
7.29 Predictability and preventability are subjective judgements, often applied in a legal sense associated with accountability and blame. In cases where it has been made clear that a death was preventable there are often legal repercussions. The purpose of root cause analysis is to examine systems so that the circumstances that allow a serious incident to arise are less likely to happen.
7.30 The internal investigation report made recommendations that may improve practice in the future. However, the report states that (page 60 paragraph 12.59) the investigation team could not identify any material contributory issue or root cause in Mr A’s clinical management and care which could have prevented the incident.
7.31 Because of this the report does not make clear the linkages and consequences of each of the issues identified. The report also does not identify which of the recommendations are the most significant or most important to address.
7.32 The lack of focus on what went wrong and why, and the lack of risk assessment of each of the recommended actions, means that in practice the gravity of not meeting the recommendations is not made clear.
7.33 The action plan lacked clarity about which recommendation was being addressed in each section. We do not consider it to be wrong to group or theme recommendations but there must be a clear line of sight of recommendations made in internal investigation reports and where they are subsequently addressed in an action plan.
7.34 The Trust must ensure that serious incident investigation reports make clear the links between the issues identified and the recommendation being made, ensuring that the most important or significant recommendations are identified. See our Recommendation 2.”
But enough of boring Nolan Principles like duty selflessness, accountability and evidence. Let’s have some selfies and evening wear:



What does RDASH say?
If readers wish to see what RDASH claims about itself, HSJ has obliged by printing the trust’s eulogy of its Speak Up practices under HSJ Solutions.
It includes the word “passionate”.
But based on the Niche homicide report’s criticisms, one must wonder how capable RDASH is of rigorous self-appraisal.
And how capable the National Guardian’s Office is of doing its duty.
RELATED ITEMS


