
By Dr Minh Alexander, NHS whistleblower and former consultant psychiatrist 22 October 2019
|
Summary: NHS Improvement has started a process of deciding which of several recommendations from the Kark Review will be implemented and how. Incomplete information has been publicly shared to date, but some more information has been obtained and the relevant documents are provided below. The documents shared so far show an attempt by NHS Improvement to water things down with an emphasis on “light touch”. NHS Improvement and other bodies have a history of not consulting openly enough with whistleblowers or making adequate use of their extensive knowledge of system failure. Certain voices may be selected without transparent, sufficient justification, and some may also be paid. Some FOI data giving a past example of the latter is provided. There is also a tendency to rely on intermediaries such as the National Guardian’s Office, about which many whistleblowers have significant reservations, adding to reduced representativeness and further lack of whistleblower confidence. Documents and other information provided by NHS Improvement show that many of the organisation and players that have been part of the problem have the most seats at NHSI’s Kark implementation table. Links to the documents follow. I encourage whistleblowers, patients or families who have not been invited to contribute to the Kark implementation process to do so and to ensure that NHS Improvement listens to all voices, even if they do not say what it wants to hear.
|
Background
There have been very serious, repeated failures by the CQC to fulfil its responsibilities under Regulation 5 Fit and Proper Persons, and to ensure that the public is Safeguarded from managers guilty of serious misconduct.
In response to mounting criticism of CQC’s blatant FPPR failures, the government eventually conceded and commissioned the Kark FPPR Review which took place last year.
Kark’s review report was published in February and largely let CQC off the hook for its misconduct and mishandling of FPPR, but it did criticise the present FPPR provisions and made a range of recommendations.
The government handed final decisions about implementation of the Kark recommendations to NHS Improvement.
NHSI fell silent in the subsequent months despite occasional whistleblowers’ enquiries as to progress.
NHS Improvement’s behaviour regarding Kark implementation
I wrote on 6 September 2019 to Dido Harding NHSI Chair cc parliament with an example of continuing, characteristic CQC failure on FPPR – including failures to feedback to the referrer, excessive delay and refusal to share adequate information.
A reply of 25 September 2019 Dido Harding gave the following update:
“As you know, the Department of Health and Social Care accepted the first two recommendations of the Kark Review and asked that NHS England and NHS Improvement engage with a wide range of stakeholders to consider the remaining five. We have subsequently agreed with the department that we should also implement the third recommendation (to introduce a mandatory reference requirement for NHS directors) and that the department would consider the final recommendation (which concerns the application of the FPPR in social care).
We intend to write to the department, setting out our implementation approach to the entire Kark Review alongside publication of the People Plan later this year. My team is currently speaking to a range of people to inform the best approach to implementation and I have passed your contact details on to a colleague, who will be in touch with you separately so that you have an opportunity to inform on our next steps.”
This colleague, a policy adviser, proved to be an DHSC employee, previously attached to the Freedom To Speak Up review and currently seconded to NHSI.
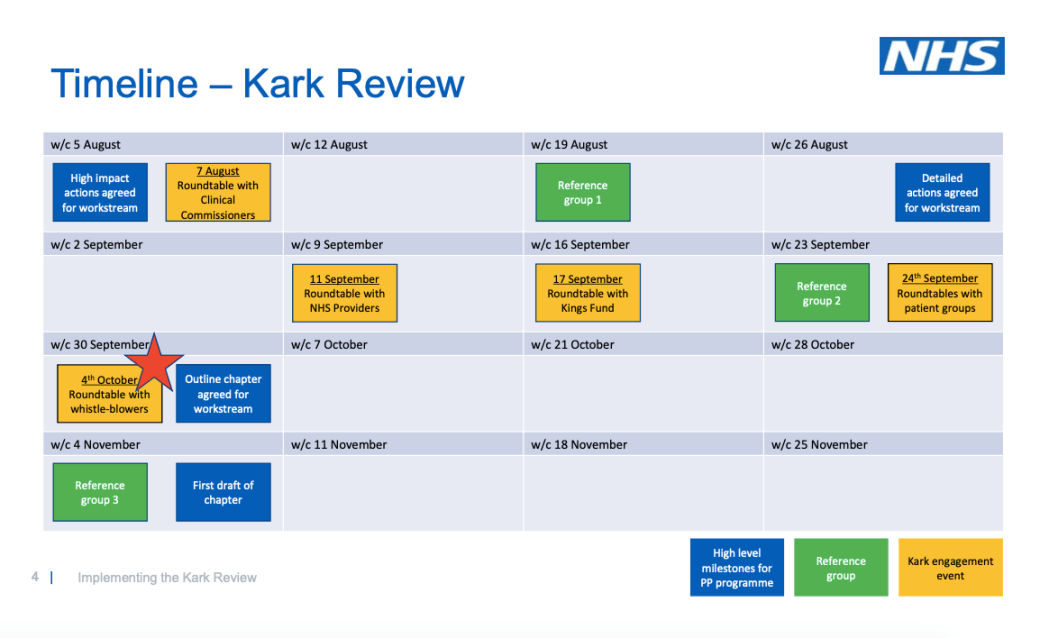
Upon request for relevant NHSI Kark consultation documents, the policy adviser shared the following document, which are the slides from an NHS Leadership Academy event that took place in Leeds on 4 October 2019:
‘Transforming Leadership Culture: Implementing the Kark Review’ NHS Improvement 4 October 2019
Some whistleblowers had been notified in early September of this event, but it was not clearly badged as an official NHS Improvement event. There was the usual, rather patronising invitation to contribute experiences:
“Session
Facilitator
11:00am – 12:30pm
As part of wider Speak Up Month activities, we invite you to a Lessons Learnt/Shared Experiences session – TBC by Bernie
Bernie Rochford, Russ Parkinson (TBC)
12:30pm – 1:15pm
Lunch – (supplied by the Academy)
N/A
1:15pm – 3:15pm
Focussed Kark session, exploring the themes of your experiences regarding Directors in whistle-blowing incidents
Karl Roberts, Bernie Rochford, Sally Scales (TBC)”
Seeing the involvement of the National Guardian’s Office and not having been advised that this was an official NHSI event on policy, I had decided not to attend.
I questioned NHSI about the fact that whistleblowers were just invited to contribute ‘experience’, and NHSI has clarified that it will accept submissions about policy.
In terms of publicising the 4 October event, NHSI said it asked the National Guardian’s Office and NHS Leadership to send out invitations. Only some whistleblowers received an invitation. Some of those who were not invited had in fact been participants in the Kark FPPR review.
NHS Improvement advised me that about 14 whistleblowers attended the Leeds Kark session on 4th October.
I noticed that the 4 October 2019 event slides mentioned a Reference group.
The DHSC/ NHSI contact explained that this group was set up to help steer NHSI’s Kark implementation.
The Reference group appears to the real business end of NHSI’s consultation process and the key point at which influence is on the process is exerted.
Further enquiry NHSI revealed there was a single whistleblower on this NHSI Kark Reference group. This person was previously a PCT manager, who unsuccessfully claimed for constructive dismissal and whistleblower detriment, against Southwark PCT and currently works as a Freedom to Speak Up Guardian for Mersey Care NHS Foundation Trust including covering the now defunct Liverpool Community Health NHS Trust which was absorbed by Mersey Care.
The presence of a solitary whistleblower took the gloss off a recent expansive claim by Chris Hopson CEO of NHS Providers that the consultation was robust:
“More happily, there is a strong and effective consultation process on the other Kark Review recommendations as part of the work on the NHS People Plan. NHS Providers, frontline trust leaders and a broader group of stakeholders, including whistleblowers are contributing to this exercise and we are having a quality discussion on some highly complex issues. That is how to create the right decisions that can be implemented successfully to deliver the desired outcome.”
Upon enquiry about how the single whistleblower member of the Kark Reference Group was selected, the NHSI response was one of initial uncertainty followed by the following explanation:
“I have also been through my records and confirm that the whistleblower member of the Kark reference group was drawn from the wider membership of the Improving Leadership Culture reference group.”
I have challenged the lack of transparency and equality of opportunity in NHSI’s selection of a whistleblower representative for the Kark Reference group, and pointed out that NHSI previously acted in a similar manner during the establishment of its much criticised NHS whistleblower employment support scheme.
|
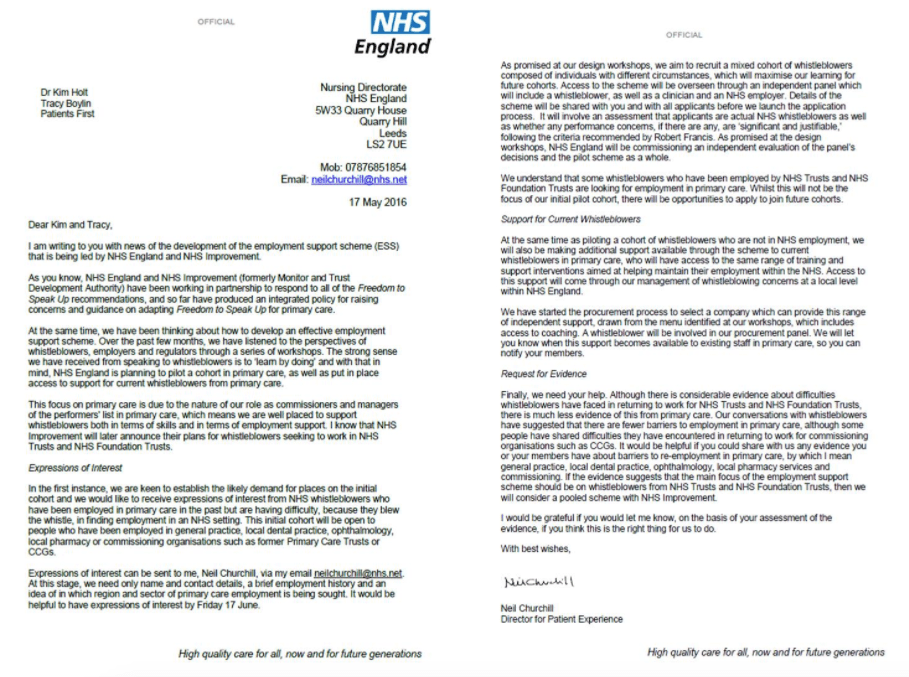
NHS Improvement’s anointed figurehead for the whistleblower employment support scheme Without any transparency or equality of opportunity, an individual who was previously an NHS trust HR manager who as far as I am aware had not established in law that they had a whistleblowing case, and who was the subject of conflicting medical evidence about possible factitious illness, was selected as an adviser for the much criticised NHSI whistleblower employment support scheme. Moreover, NHS England had originally approached two individuals at the (now defunct) organisation Patients First, regarding establishment of the NHS whistleblower employment support scheme:
FOI enquiries later revealed that 1. NHS England made payments totalling in excess of £18K to one of these individuals, the person selected as an adviser by NHSI, through their company: “Payments totalling £18,536.64 were made to TAB HR Limited between September 2016 and June 2017. These payments were for a range of contractor/consultancy services.” NHS England FOI disclosure 23 February 2018 Ref 055603 2. NHS Trust Development Authority, one of NHSI’s constituent bodies, paid the same individual £4,893 for their part in development of NHSI’s whistleblower employment support scheme: “The NHS TDA spent £4,893.85 on the services of TAB HR Limited which covered services for up to 16 days between February and April 2017. This was to provide support for the development of the Employment Support service.” NHS Improvement FOI disclosure 7 February 2018
|
But the failures to be transparent and to ensure equality of access for all are not new on the whistleblowing scene.
It is a cycle that repeats ad nauseam. Power typically seeks out that with which it feels comfortable, finds familiar and or believes it can exploit or mould to its own purpose, providing trouble-free public relations and photo ops, without the nuisance of dissent and robust scrutiny.
Power may deny that it does so, and sometimes this denial may be sincere and the selectivity is based on subconscious bias, but the actions have the same effect.
Controlling tokenism undervalues dissent as a healthy part of normal governance.
The usual suspects
I asked for the terms of reference and minutes of the meetings of NHSI’s Kark Reference group.
Minutes of the first Kark Reference group meeting, and Terms of Reference for the overarching ‘Improving Leadership Culture’ Reference group have been provided:
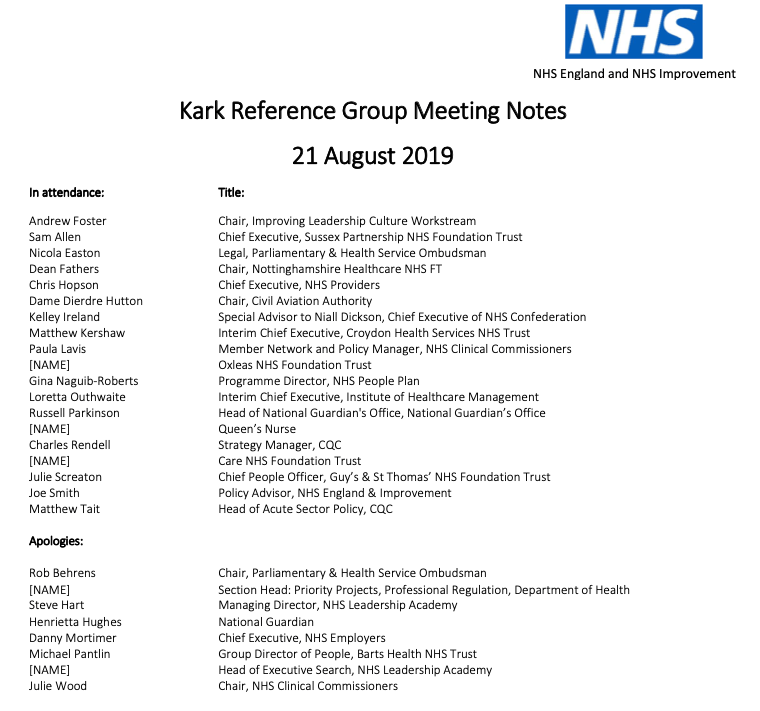
Minutes of NHSI Kark Reference group meeting 21 August 2019`
NHSI Improving Leadership Culture Reference group terms of reference
Minutes of a second meeting have also been promised and will be posted here when available.
A glance at the list of attendees at the Kark Reference group’s first meeting on 21 August 2019 [redacted by NHSI of junior officials’ names] shows many familiar faces, representing organisations that have firmly been a part of the problem:
The principles put forward by the Kark Reference group after two meetings convey inertia and low expectations:
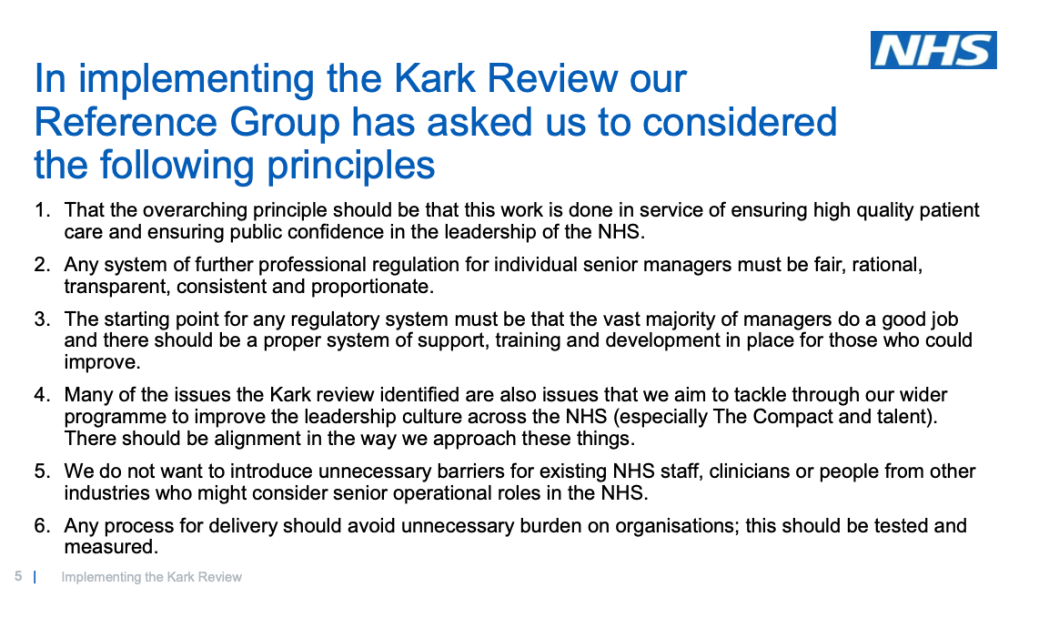
Upon questioning, NHSI admitted that the above assertion that “the vast majority of managers do a good job” was not based on any evidence whatsoever, but merely a wish to avoid negativity.
I contended that the assertion was improper and provocative in the absence of evidence, especially given the history of recurring avoidable deaths, and that such attitudes were the reason the Kark Review was necessary in the first place.
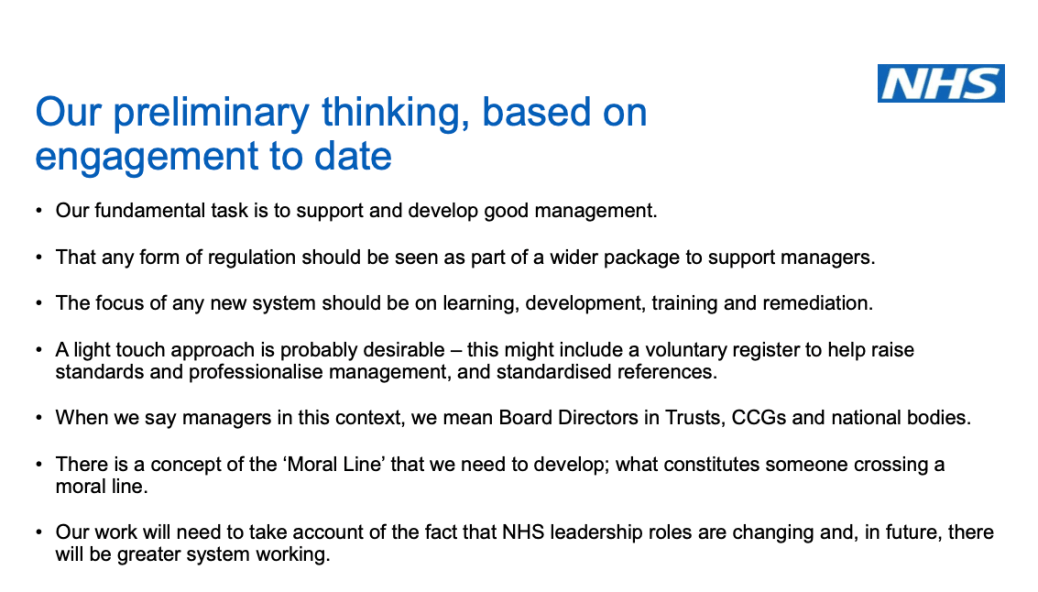
On that theme, NHSI is trying its best to nudge the Kark implementation process in the direction of doing as little as possible – the words ‘light touch’ stand out:
Granted, NHSI has yet to update its slide based on the outcome of the 4th October 2019 event.
NHSI admitted that whistleblowers who attended on 4th October pushed back on the light touch gambit. I have now added my opposition.
This is the agreed record of two telephone meetings with the DHSC policy adviser seconded to NHSI, who is handling the Kark review implementation:
My formal written submission to NHSI on implementing the Kark review is also provided below in the appendix.
Any whistleblowers or patients and families who wish to challenge NHSI and DHSC’s attempt to water down what were already compromise solutions by Kark should also add their voices as a matter of urgency, because NHSI plans to finalise a draft of its plans by early November:
The Kark review came after years of serious government failure following Jeremy Hunt’s glib and insincere promises of culture change following MidStaffs.
The issues are at their heart simple and are about decency and honesty. Everybody is qualified to comment. If you feel strongly, just write in however briefly and simply, FAO Joseph Smith Policy Adviser, NHS England and NHS Improvement.
RELATED ITEMS
Sorry is the hardest word: CQC, Paula Vasco-Knight and Regulation 5 Fit and Proper Persons
Twiddling at the edges will not be safe substitute for much needed reform of unfit UK whistleblowing law:
Replacing the Public Interest Disclosure Act (PIDA)
APPENDIX
SUBMISSION TO NHS IMPROVEMENT’S KARK IMPLEMENTATION PROCESS
22 October 2019
Dear Joe,
Thanks for your help, all the information provided and the documents shared.
As promised, this is my formal submission to NHSI’s Kark implementation process.
- Firstly, I should say that I do not believe that the mistreatment of whistleblowers In the NHS or any other UK sector will reduce until there is substantial reform of UK whistleblowing law, which should include meaningful deterrence of whistleblower reprisal in the form of sanctions for individuals, civil and criminal, as opposed to sanctions for organisations.
- The government said it might consider changes to UK whistleblowing law after the publication of the Gosport inquiry report, and meetings between DHSC and BEIS have been held, but little has update has been provided. I doubt that there are present government plans to make the necessary degree of change for safe governance.
- At present, some senior NHS managers corruptly squander public money on legal services to intimidate, settle and gag whistleblowers because they know there is almost zero chance that they will suffer any personal consequence.
- The fact that regulators such as NHSI rubber stamp some of these payments, help shelter and redeploy senior abusers and avoid taking action in even the most egregious cases is permissiveness of a scale that is tantamount to encouragement of the misconduct. Similar arguments apply regarding the DHSC, the ultimate culture carrier and pace setter.
- At present, the DHSC resists even the proper investigation of whistleblower’s concerns, so the Kark implementation exercise is somewhat hollow, no disrespect to you personally.
- I also note from the Kark review report that there is understandable fear by managers that any system of managerial regulation will be abused by the centre to unfairly dismiss individuals who are unwanted, as opposed to wrongdoers. Also that there are reports that not only FPPR has been blind to some misconduct but has been improperly weaponised against managers who are not in favour.
- Nevertheless, those caveats apart, I make the following summarised points and address some issues that you asked me to.
- As I understand it, the government has so far accepted the following recommendations from the Kark review:
- The introduction of a national competency framework for NHS board roles
- The creation of a central database about NHS managers’ training and employment history, including upheld grievance and disciplinary issues
- NHSI has informed me that it accepted a third recommendation:
- The introduction of standardised, mandatory references
I understand this should be along the lines of a sample reference form provided by the Kark review report, and a recommendation that mandatory references are signed off by directors who are subject to FPPR (and thus can be held accountable for any false references).
Please let me know if the government and NHSI are not fully implementing any of the above three Kark recommendations as I have understood them.
- This leaves much a number of other recommendations to be decided, including:
- Extension of FPPR to commissioners and ALBS
- A power to disbar directors for serious misconduct, with a disbarring service located within NHSI
- Removal of the clause which makes being ‘privy’ to misconduct a criterion under FPPR
- The application of FPPR in social care provision.
- Overall, I believe that there needs to be a step change in the quality of NHS management, commensurate with the gravity of the task in hand. Professionalisation is needed, with clear, explicit, regulated standards, as for all other health professions.
- I reject any attempts to lower standards based on concerns that barriers should be lowered for access, as implied by the guiding principles generated by the Reference group steering NHSI’s Kark implementation. It is low expectations, poor controls which have allowed unchecked managerialism and unsuitable senior managers appointing in their own image that have got us to this state.
- Patients and the wider public deserve a high standard of management in a vital, safety-critical public service. That should be the core expectation, with no compromise on quality, the latter being short termism which stacks up disproportionate trouble for the future.
- It is essential that DHSC and NHSI face up to the need to remove corrupt senior managers from the DHSC, ALBS and provider bodies. Until this is done, there will be little change because these individuals will not change behaviour. They will operate corrupt cultures where meritocracy, safe governance and patients cannot flourish.
- Beyond that, I agree with the need for a supportive, proactive system of talent development and supportive remediation where things go wrong due to issues of competency.
- However, I also suggest that much more emphasis is given to recruitment of the right individuals, with the right values and character. This is less wasteful than appointing unsuccessfully and throwing resource at managing failure.
- The Kark review emphasised competency and proposed that NHS directors should have understanding of the importance of the following:
- Board governance;
- Clinical governance;
- Financial governance;
- Patient safety and medical management;
- Recognising the importance of information on clinical outcomes;
- Responding to serious clinical incidents and learning from errors;
- The importance of learning from whistleblowing and ‘speaking up’;
- Empowering staff to make autonomous decisions and to raise concerns;
- Ethical duties towards patients, relatives and staff;
- Complying and encouraging compliance with the duty of candour;
- The protection, security and use of data;
- Current information systems relevant for health services;
- The importance of issues of equality and diversity both within the hospital in workforce issues and in relation to appointments to the Board; and
- The importance of complying on a personal basis with the Nolan principles
Whilst understanding of these matters is obviously necessary, the issues in the worst breaches have been deliberate non-compliance, collusion and conspiracy to misconduct, not inadvertent blunders.
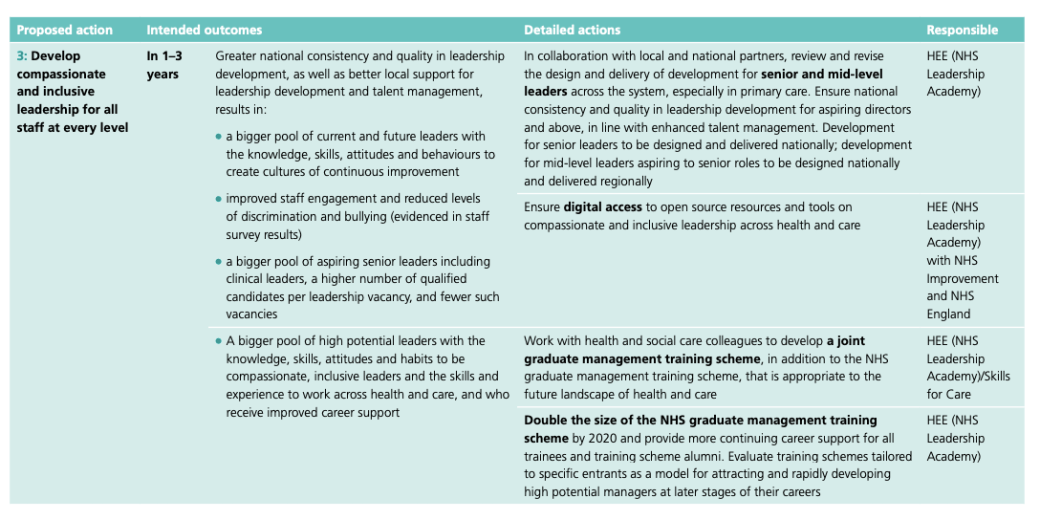
- You asked me to comment on NHSI’s competency frameworks.
- Regarding “Developing People – Improving Care A national framework for action on improvement and leadership development in NHS-funded services”
https://improvement.nhs.uk/documents/542/Developing_People-Improving_Care-010216.pdf
- Page 20 gives the following as the action plan for ensuring “Compassionate, inclusive and effective leaders at all levels”:
“A variety of frameworks are used across the NHS to develop, assess, select, promote and regulate leaders and leadership, and they are often incongruent. People across the system need to agree on ‘what good leadership looks like’ at different levels and develop consistent descriptions, using language common to all organisations and systems.”
- Page 23 gives a little more detail:
- The emphasis here is on development and training. Whilst these interventions may augment, they cannot substitute for wise, kind, honest character. If the NHS fails to recruit managers with sound character, the rest falls. As cited in the Kark review report, the PSA has observed that: “Technical competence to serve on a Board is as nothing without personal commitment to the public interest”
- Looking at NHS Improvement’s resources for “Creating a culture of compassionate and inclusive leadership”
https://improvement.nhs.uk/resources/culture-leadership/
This leads to sample documents from several trusts, some of which briefly nod to “recruiting for values” but give little detail on definitions and methodology.
- The Kark review noted huge variation in how NHS directors are recruited:
“The variation in how executives are recruited is huge. At one end of the scale, there is a ‘full service’: full stake holder discussions are held with each candidate, applicants are filmed in order to test media training etc. At the other end of the scale, there is just an interview panel for between 45 and 60 minutes with little other than CVs and references.”
- If the NHS does not have sufficient expertise on this subject of recruiting for the right values, it has the options of buying in suitable expertise and of commissioning research to inform future policy decisions. The Kark Review directed the government to the Institute of Directors’ Director Competency Framework which emphasises the importance of evidence of suitable “attitude and disposition that shapes a director’s responses and behaviour”.
- Regarding models of regulation, I have looked at the regulation of teachers as you suggested:
https://www.gov.uk/government/collections/teacher-misconduct
- I do not think this model offers adequate protection to patients because it only deals with misconduct so serious that it is wholly incompatible with the role and may require a life ban. The model leaves any misconduct short of this extreme level to employers to deal with:
“They [the regulations] cover cases of serious misconduct. This is when a teacher’s behaviour:
- is fundamentally incompatible with being a teacher
- uld lead to them being prohibited from teaching
The regulations don’t cover the cases of less serious misconduct, incompetence or under-performance. A teacher’s employer should deal with these cases.”
- I think it would be unacceptable for employers to be left wholly in the control of NHS managers’ misconduct that merits serious but lesser sanctions. There is a conflict of interest for employers to cover up failure, and that conflict of interest becomes acute and unmanageable when it is the directors of the organisation who are the accused.
29. The full model of professional regulation as operated by health and social care professional regulators is preferable and safer, partly because it is in principle proactive and preventative through the basic requirements of standardised qualification, accreditation and registration. It is required for the proper professionalisation of NHS management as a discipline. I believe the additional expense of full regulation is justified to keep patients safe.
- Therefore, I would prefer full professional regulation of NHS managers to give parity with the way clinicians are managed, not least to stem the abuses of unchecked managerialism against patients’ interests which have resulted in horrors such as MidStaffs, Gosport and Liverpool Community Health NHS Trust.
- I appreciate that the Kark recommendation is only for a disbarring council broadly similar to that which operates for teacher, but with less formality. I do not feel this goes far enough. I also do not agree that a disbarring service should be under NHSI’s control, given political conflicts of interest and the potential for abuses. As I write I am mindful that NHSI currently employs as a director a trust manager who had been personally criticised for causing serious detriment to a whistleblower.
- Needless to say, I think this preliminary suggestion by NHSI is wholly unacceptable and I reject it:
“A light touch approach is probably desirable – this might include a voluntary register to help raise standards and professionalise management, and standardised references.”
- It is hopeless to expect that the worst offenders who have cheated, lied, fabricated false allegations against staff, referred staff vexatiously to regulators and misled regulators, dismissed honest investigators, committed fraud, perjured themselves, covered up, and knowingly endangered patients out of self-interest would comply reliably with, and act in the spirit of, voluntary arrangements.
- The current failure of FPPR and the farce of self-declaration under FPPR are I believe sufficient evidence to show that NHSI’s hopes of a light touch, voluntary system are doomed.
- I agree with the proposal to extend FPPR to commissioners, regulators and other ALBs. I also think the DHSC should be included.
- NHSI has characterised Kark recommendation 7 as: “That the FPPT be extend [sic – extended] to cover social care provision”
- As discussed, I believe from my reading of Regulation 5 and CQC’s supporting material that FPPR already applies to social care (and at the time of writing it occurred to me that I made an FPPR referral to CQC on a director of social care some time ago, about which I had forgotten). On checking the wording of the Kark review report, it says: “We recommend that further work is done to examine how the test works in the context of the provision of social care and whether any amendments are needed to make the test effective.”
I would support this.
- You asked about definitions of misconduct and red lines – or as NHSI puts it: “what constitutes someone crossing a moral line”.
I think there should be clear definitions of types of serious misconduct that would result in disbarment from senior office. I agree with the suggested red lines set out in the Kark review report, and I would particularly emphasise:
- Covering up safety issues
- Suppressing whistleblower concerns
- Reprisal against whistleblowers or complainants
- Misuse of public funds in the pursuit of any of the above, including aggressive, meritless appeals by NHS organisations that been the subject of successful claims, and respond by punishing and ruining whistleblowers through vexatiously prolonging the legal process
The Kark review emphasised “deliberate” bullying:
“Deliberate bullying, particularly victimising those who raise concerns should in our view be regarded as ’red line’ behaviour and serious misconduct.”
I am concerned that this might provide a loophole.
I suggest that any bullying of whistleblowers is a red line, whether proven to be deliberate or not, but that if deliberate bullying is found, this should be viewed as an aggravating factor when sanctions are decided.
- The Kark review suggests removing the clause which makes being privy to serious misconduct a criterion for consideration under FPPR:
“Amending the Fit and Proper Person Test to remove the reference to directors ‘being privy to’ mismanagement which we do not think promotes clarity”
- I am concerned that this will remove proper liability for executive negligence in the form by-standing. Whistleblowers very commonly encounter a wall of silence when after being blocked they anxiously explore more and more avenues to resolving concerns or seek protection from reprisal. It is often concerted failure to respond, to act and to protect that sinks whistleblowers as much as active victimisation. Indeed, in a rare glimpse, it became evident that officials planned to warn a DH minister not to respond to a whistleblower.
- I think that if the clause about being ‘privy’ is removed, it must for clarity be replaced with a clause that makes it clear that offences of omission are just as serious, and that failing to act appropriately upon knowledge that fellow directors are guilty of serious misconduct is itself classed as serious misconduct.
- There is a note along these lines on page 132 of the Kark review report about red lines: “Victimisation or knowingly allowing the victimisation of whistleblowers”
I think the principle of “knowingly allowing” other forms of serious misconduct should also apply.
- The Kark review sets out to prevent unfit managers from moving around the NHS:
“Our recommendation in relation to mandatory references and an independent disbarring service are intended to prevent those proved to have been guilty of misconduct moving around the NHS system.”
- I think NHSI should give consideration to wider Safeguarding issues, and set out how it would ensure that other agencies are apprised of risks posed managers who are barred from the NHS and who may seek employment in other areas where they may also pose a risk to the public, especially vulnerable people.
- With regard to proposed exceptions in the public interest from a five year statutory time limitation for serious misconduct, I think the principles by which exceptions are made should be explicitly provided in guidance, to avoid arbitrary and widely varying responses.
- I recommend that NHSI takes note of resources on the organisational management of seriously sociopathic behaviour. This is one example, which describes how psychopathic individuals may impact on institutions, and what institutions can do to manage this risk:
Tackling psychopathy: a necessary competency in leadership development?
As the author comments, psychopathic individuals excel at kissing up and kicking down, and may manage upwards in a manipulative way, to please regulators such as NHSI:
“The problem for leadership development16 is that psychopathic individuals can achieve most of the key competencies including getting others to follow them, being politically astute, relating to senior colleagues with charm, and possessing excellent communication skills. If the person can muster sufficient ‘charisma’ and achieve set targets (for example, in cost cutting), affective instability and the tendency to damage others could be overlooked by organisations”
- Accordingly, as my last word to NHSI, I would stress the importance of valuing voices that the regulator finds less comfortable, whether it is trust executives who honestly say they cannot do the impossible, frontline staff who report the consequences of provider organisations being asked to the impossible or whistleblowers who are more challenging and less complaisant regarding NHSI’s policies. In terms of future policy consultations that may involve whistleblowers, I advise open calls for contributions and publication of consultation papers at an early stage, without reliance on intermediaries such as the National Guardians Office who have any control of the communication.
With best wishes,
Minh
Dr Minh Alexander
Cc Tom Kark QC
Dido Harding NHS Improvement Chair


Reblogged this on | truthaholics and commented:
Tackling psychopathy: a necessary competency in leadership development?
As the author comments, psychopathic individuals excel at kissing up and kicking down, and may manage upwards in a manipulative way, to please regulators such as NHSI:
“The problem for leadership development16 is that psychopathic individuals can achieve most of the key competencies including getting others to follow them, being politically astute, relating to senior colleagues with charm, and possessing excellent communication skills. If the person can muster sufficient ‘charisma’ and achieve set targets (for example, in cost cutting), affective instability and the tendency to damage others could be overlooked by organisations”
LikeLike