To Mike Mire CQC Chair, 26 November 2015
Dear Mr Mire,
CQC’s approach to whistleblowers and whistleblowing
We write to raise concern about these issues. Public Accounts Committee, at its recent hearing with the CQC and Dame Una O’Brien on 28 October, noted the CQC’s continuing ineffectiveness. [1] Specifically, we believe that the CQC has failed and continues to fail whistleblowers. We have the following unresolved concerns about the CQC’s discharge of its responsibilities for ensuring good whistleblowing governance:
1) The CQC’s poor treatment of its own staff who whistleblow and its role modelling of good practice as an employer.
2) The CQC has done little or nothing to challenge the gagging of whistleblowers by the organisations that it regulates.
3) The CQC is not sufficiently transparent about whistleblowing issues.
4) The CQC is failing to act appropriately upon whistleblowers’ disclosures.
5) The CQC still has no structured inspection methodology for assessing regulated organisations’ whistleblowing governance.
6) The CQC has not made serious efforts to engage with whistleblowers.
7) The CQC has shown little will to address serious misconduct by senior managers who engage in reprisal
8) The CQC has advised whistleblowers that they can complain to PHSO about CQC’s response, but in six years PHSO has not upheld a single complaint about the CQC
9) Whistleblowers continue to be sacked or forced to move on, and this is supporting evidence of insufficient support for whistleblowers and insufficient deterrence of reprisal.
We provide the basis for our concerns in the appendix below. We ask you to ensure that the CQC rapidly improves its whistleblowing governance and that the shortcomings that we have described are rectified. In particular, we ask that the CQC’s handling of FPPR is appropriately scrutinised and corrected. To borrow from the CQC’s Board, we believe that the CQC’s poor whistleblowing governance is a “fraying rope” which poses a risk to patient safety. We look forward to hearing whether you will be able to help resolve our concerns.
Yours sincerely,
Minh Alexander
Kevin Beatt
Fiona Bell
Sharmila Chowdhury
Eileen Chubb
David Drew
Narinder Kapur
Gary Walker
Maha Yassaie
cc Health Committee
Public Accounts Committee
Secretary of State for Health
Shadow Secretary of State for Health
APPENDIX: The basis for our concerns:
1. The CQC’s treatment of its own staff who whistleblow and the CQC’s role modelling of good practice as an employer. The CQC has a history of gagging [2] and treating its own whistleblower staff poorly. It has also still not apologised to several of its own whistleblowers. Additionally, a CQC member of staff recently made a serious external disclosure.[3] This suggests that CQC is still not properly handling concerns raised by its own staff. This does not set a good example to the organisations that the CQC regulates.
2. The CQC has done little or nothing to challenge the gagging of whistleblowers by the organisations that it regulates. The CQC’s inspection reports do not explicitly deal with this key issue of whistleblowing governance. Despite the CQC acknowledging that confidentiality clauses can be seen as gagging clauses [2], the CQC seems to have turned a blind eye to the widespread and continuing use of such clauses by regulated organisations. This allows employers to continue forcing whistleblowers into silence.
3. The CQC is not sufficiently transparent about whistleblowing issues. Despite Public Account Committee’s recommendations that public bodies make proactive and transparent use of whistleblowing data [4], the CQC has failed to analyse and publish meaningful whistleblowing activity data. This is despite the fact that the CQC holds an unparalleled national database on health and social care whistleblowing, which could clearly be powerfully used to drive learning and care quality. It is a hugely wasteful, major governance failure that the CQC has not made better use of this data. The CQC has also declined to make a definite commitment to publishing such whistleblowing data in the future [5], even though the government says that it plans to make it compulsory from April 2016 for prescribed bodies such as the CQC to publishing whistleblowing data. [6]We are also concerned that the CQC has refused to publish the outcome of an external review of its whistleblowing governance, which was conducted at a cost of £150,000 to the public purse. The cost of this exercise was revealed only through an FOI request. [7]
4. CQC’s failure to act appropriately upon whistleblowers’ disclosures. The CQC has repeatedly failed to give due weight to whistleblowers’ concerns, and has repeatedly failed to investigate their concerns either singly or as part of wider thematic review, despite the fact that the CQC acknowledges it has powers of thematic review. In the few instances where the CQC has undertaken thematic reviews, it has not been adequately supportive of whistleblowers. [8] The CQC has also far too readily accepted “independent” investigations that regulated organisations arrange to manage concerns raised by whistleblowers. These investigations are not truly independent, and there is evidence in some cases that employers have unhealthy if not clearly corrupt control of such investigations. The CQC must surely be aware of the shortcomings of such investigations, but it still permits and in some cases, encourages their use. In essence, the CQC divests itself of responsibility, does not take whistleblower intelligence seriously, and allows regulated organisations to waste public money on superficial and sometimes false assurance.
5. The CQC still has no structured inspection methodology for assessing regulatedorganisations’ whistleblowing governance. [9] We have written to the CQC about this issue. [9]Sir Robert Francis concluded the CQC was not making sufficient use of its powers to protect whistleblowers, and that it could do more. He recommended that regulatory action should be taken where organisations have poor whistleblowing practice. [10] However, it is hard to see how this will be achieved until the CQC sets clear, auditable inspection standards and measures its adherence to such standards. The CQC does notseem to have adopted Sir Robert Francis’ recommendations in any measurableway and appears to be carrying on regardless.
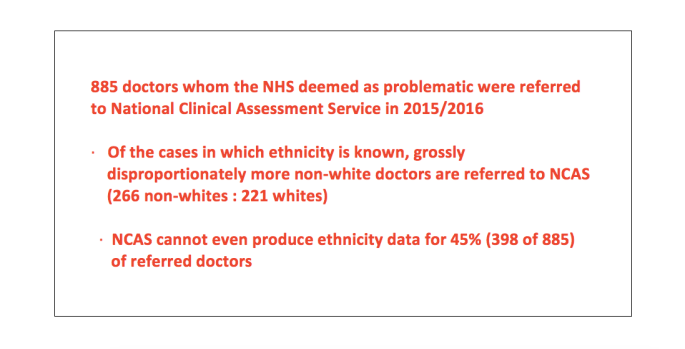
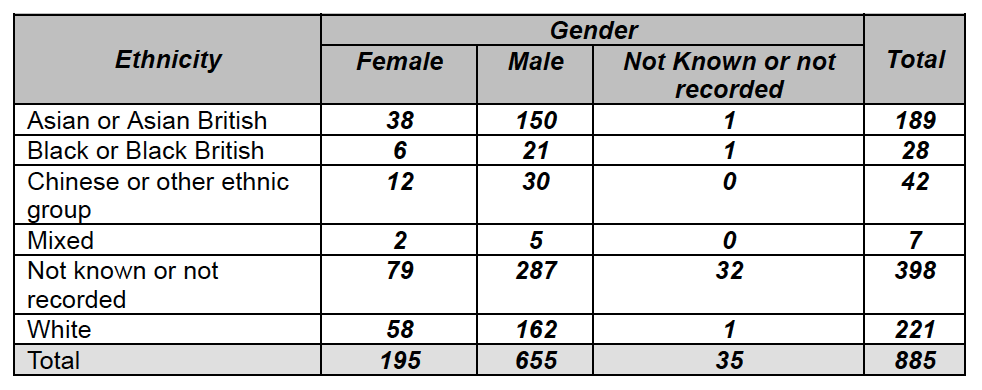
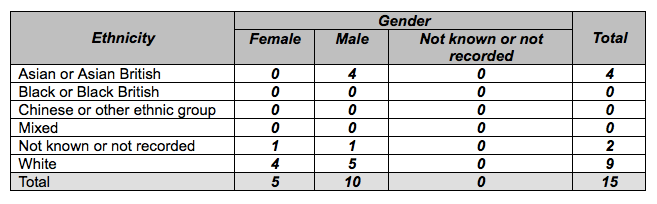
6. The CQC has not made serious efforts to engage with whistleblowers. It has only held two whistleblower listening events in two years. This is despite the CQC’s promise to keep whistleblowers regularly involved and informed. The CQC’s approach has been tokenistic, and it continues to postpone discussion of the real issues that concern whistleblowers. Also, the CQC stated last year that it was reviewing its customer care, including its approach to whistleblowers, but it has not yet taken an evidence-based approach and measured whistleblowers’ experience of the CQC. One important consequence of the CQC’s failure to measure whistleblowers’ experience is that it is failing its duty of Equality. The CQC has no data to evidence that it is treating protected groups as well as others, and CQC has admitted that it is not collecting data on the ethnicity of whistleblowers. This is despite the fact that the Freedom To Speak Up Review demonstrated that BME whistleblowers have a worse experience of whistleblowing. The CQC also set criteria for a recent CQC whistleblowing post which disadvantaged whistleblowers, and meant that many whistleblowers would not be eligible to apply even though they were the individuals with the very knowledge and expertise that were relevant to this post. [11]
7. CQC has shown little will to address serious misconduct by senior managers who engage in reprisal against whistleblowers. Not one director who has been referred under Regulation 5 Fit & Proper Person (FPPR) has so far been removed from office as a result of the CQC’s actions. [12] [13] Whistleblowers have in fact noted a tendency by the CQC to spare such managers. Professor Sir Mike Richards, who chairs the CQC’s FPPR panel, has stated that only certain levels of reprisal would be considered for regulatory action, although there is no clarity and transparency about the determining levels of reprisal. Professor Mike Richards has also stated to whistleblowers that it will not be possible to remove too many managers for reasons of public opinion. In our view, the CQC’s application of FPPR has been arbitrary and its position contradictory. The CQC claims that it is up to Trusts to make determinations of fitness, but the CQC itself has declared a number of FPPR referrals to be meritless and has not even passed these referrals to the relevant Trust Boards. This brings to mind recent comments by Professor Mark Baker of NICE: “I think the reason they don’t want it is if you don’t like the answer to the question, you don’t ask the question” [14] It seems logical to ask if the CQC is not allowing FPPR questions to be raised with Trusts, because it wishes to avoid the answers. This is particularly disappointing to whistleblowers as FPPR is currently the sole mechanism for holding managing victimising whistleblowers to account. This is because in his report of the Freedom To Speak Up Review report, Sir Robert Francis eschewed managerial regulation in favour of a trial of FPPR. It seems logical to ask if the CQC is not allowing FPPR questions to be raised with Trusts, because it wishes to avoid the answers. This is particularly disappointing to whistleblowers as FPPR is currently the sole mechanism for holding managing victimising whistleblowers to account. This is because in his report of the Freedom To Speak Up Review report, Sir Robert Francis eschewed managerial regulation in favour of a trial of FPPR. We do not believe that the CQC have shown robust will to deter whistleblower reprisal. Another government agency has overseen the successful barring of a company director responsible for whistleblower suppression at Winterbourne view [15], but the CQC have failed to remove other directors for even worse reprisal using FPPR. Mr Behan and Professor Mike Richards recently claimed that although no director has yet been removed under FPPR, they believed that FPPR is now having a “deterrent” effect. [13] Their view was not supported by the recent appointment by St. George’s hospital of a high profile director, who was previously found by an Employment Tribunal to have victimised whistleblowers. [16] Sir Robert Francis referred to this specific case as an example of “oppressive” employer behaviour that should not be tolerated. [17] Yet it seems to us that the CQC has tolerated many such instances of oppressive behaviour. The resulting injustice to whistleblowers and impunity for “oppressive” managers is, as Health Committee has noted, a serious patient safety issue. [18] In the case of Hayley Dare whistleblower, her former employer West London Mental Health NHS Trust has now finally admitted in EAT proceedings and after prosecuting a ferocious campaign against her, that she raised concerns in good faith. [19] Yet such is the licence afforded to employers that we have no expectation that the Trust board will be held to account for unlawful reprisal, sacking a whistleblower or for gross waste of public funds.
8. The CQC has advised whistleblowers that they can complain to PHSO if they are unhappy with its response, but this is likely to be an ineffective means of appeal.However, it is clear from the statistics that a complaint to PHSO is unlikely to beupheld. Based on FOI disclosure by PHSO, of 354 complaints to PHSO about the CQC since the CQC’s inception in 2009, none have yet been upheld. [20] An appeal to PHSO is likely to be just another journey between pillar to post for whistleblowers. So in short, whistleblowers are obstructed by the CQC’s failures to discharge its responsibilities, and in effect have nowhere else to go.
9. Whistleblowers continue to be sacked or forced to move on, and this is supporting evidence of insufficient support for whistleblowers and insufficient deterrence of reprisal. In the continuing case of whistleblower Dr Kevin Beatt illustrates the fact that even when whistleblowers are fully vindicated by Employment Tribunals, employers may still subject them to further harrowing appeals. The Employment Tribunal found that Dr Kevin Beatt was a genuine whistleblower, that he was blameless and that he suffered serious detriment which included being vexatiously referred by his employer to the GMC. However, Dr Beatt’s former employer has appealed against the ET judgment despite the recommendations of Sir Robert Francis’ whistleblowing review and his advice that employers should reflect on current legal action [21], and despite Mr Hunt’s promises to protect whistleblowers. Furthermore, the CQC arbitrarily rejected Dr Beatt’s FPPR referralabout the actions of his employer. It is clear to us that poor employers continue to victimise whistleblowers because there is a palpable lack of deterrence, and they have no fear of consequences.
References
[1] Public Accounts Committee, oral evidence on the CQC 28.10.2015
[2] Health watchdog put 20 gagging orders on staff, Patrick Sawer and Laura Donnelly, Telegraph 30 June 2013
[3] DH audit of the CQC’s procurement process in response to a CQC whistleblower’s disclosures to DH
https://www.gov.uk/government/publications/review-of-2-cqc-procurements-made-in-2013
[4] House of Commons Public Accounts Committee, Whistleblowing, Ninth report of session 2014-2015, 1.08.2014
[5] Correspondence about the CQC’s analysis and publication of its whistleblowing data
[6] Correspondence from Sir Jeremy Heywood, Cabinet Secretary 20.10.2015
[7] Correspondence about the publication of a review of the CQC’s performance as a prescribed body under the Public Interest Disclosure Act
[8] Joint review by the CQC and Monitor into whistleblowing concerns at the Christie NHS Foundation Trust
Click to access Christie_Review.pdf
[9] Letter to Mr David Behan, CQC Chief Executive 19.10.2015
[10] Report of Freedom to Speak Up Review by Sir Robert Francis QC, 11.02.2015
[11] Correspondence to Mr David Behan about National Guardian Set Up Manager post 10.10.2015 and 22.10.2015
CQC’s processes leaves exiled whistleblowers in the cold
CQC slams door on whistleblowers
[12] More than 60 managers have faced Fit and Proper complaints, Shaun Lintern, Health Service Journal 29.06.2015
http://www.hsj.co.uk/news/more-than-60-managers-have-faced-fit-and-proper-complaints/5087202.article
[13] Chief inspector: Fit and proper regulation having ‘deterrent effect’, Will Hazel, Health Service Journal, 24.09.2015
[14] NHS leaders ‘didn’t like answer’ they got on staffing levels, Shaun Lintern, Nursing Times 7.07.2015
[15] Nursing home director disqualified for failing to act on whistleblower concerns
[16] Ex-South Devon Chief joins London trust, Sophie Barnes, Health Service Journal, 12.10.2015 http://m.hsj.co.uk/5091013.article
[17] Francis criticises Vasco-Knight trust, Judith Welikala, Health Service Journal, 7.02.2014 http://www.hsj.co.uk/news/acute-care/francis-criticises-vasco-knight-trust/5067807.article
[18] House of Commons Health Committee, Complaints and Raising Concerns, Fourth report of session 2014-2015, 21.01.2015
[19] NHS Mental Health Trust accepts whistleblower who spoke out about bullying acted in good faith, Paul Gallagher, Independent on Sunday 8.11.2015
[20] FOI disclosure 21.09.2015 by PHSO on the handling of complaints about the CQC.
[21] NHS to get whistleblower guardians, Hugh Pym, BBC 11.02.2015