Dr Minh Alexander retired consultant psychiatrist 9 May 2023
This is a post to spell out the stark numbers behind the unethical and exploitative US bounty model of “whistleblowing” rewards that the whistleblowing APPG is trying to introduce.
All Party Parliamentary Groups have no official status whatsoever.
Some do good work.
Many are shady lobbying devices for wealthy and powerful private interests that subvert our democratic process.
They positively abuse parliament’s dignity, flinging the portcullis about as a branding and marketing tool.
The APPG sleaze story is a long running and ongoing scandal. These are the typical concerns about APPGs:
WhistleblowersUK has advocated for whistleblower rewards, and latterly has euphemistically dressed this up as “compensation” but in contexts which indicate rewards are being posited. Members of the APPG have also advocated for whistleblower rewards and “incentives”.
The trouble with the US bounty model is that it is utterly ruthless. It is focussed on recovering money for the State, from the financial sector. It is not about other forms of whistleblowing in the public interest. It does not care about the welfare of all whistleblowers. It wishes only to identify those who will recover the most money for the State, be they genuine whistleblowers, or criminals who rat on other criminals.
Indeed, a lawyer from the US firm which funded the whistleblowing APPG publicly compared whistleblowing to the use of paid informants in law enforcement at a Bylines festival.
Bona fide whistleblowers who report wrongdoing, and suffer for it, are discarded by the US bounty system if their disclosures do not result in recovery of a sum beyond a target threshold, (a million dollars under the US Security and Exchange Commission rules). Some whistleblowers wait years under this system to receive nothing.
And what of the cold mathematics of SEC’s whistleblowing hunger games?
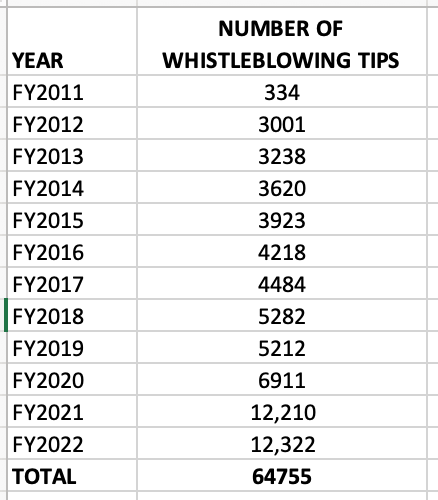
Since 2011, the US Securities and Exchange Commission (SEC) says its whistleblower programme has received a total of 64,755 whistleblowing tips about financial wrongdoing.
Source: SEC annual reports from SEC’s Dodd-Frank whistleblower programme
SEC says that from all of these tips, it has made 328 awards to individuals under its whistleblower programme:
Although there are complexities, that roughly gives a conversion rate of only 0.5%.
That is, 99.5% are junked. Some after many years of waiting.
And bear in mind that investigators have discovered that scandalously, SEC have given some of the awards to individuals who did not even meet SEC’s own definitions of a whistleblower.
Here is an example of a genuine whistleblower who failed to qualify under SEC’s Byzantine process:
Gene Ross discovered the theft of $175K from a client and reported it. He suffered serious detriment. After seventeen years, he was told that he would not qualify for a SEC award, although his report eventually led to SEC recovering more than $50 million from a fraud.
“What has moved far more slowly is the story of Gene Ross, father of three, who, in the process of voluntarily cooperating with government prosecutors and regulatory agencies in the criminal and civil actions against Amerindo, lost his job at Bear Stearns, which strongly discouraged his participation in the legal reckoning that followed, cut his pay, took away his sales team, and subjected him to unchecked harassment and retaliation. After leaving Bear, Ross was forced to sell his home to cover mounting legal bills that eventually bankrupted him. Yet he continued to provide evidence, documents, and testimony as a star witness in the 2008 criminal case that put Vilar and Tanaka behind bars.”
Ross commented of the SEC decision: “It kind of made me feel like a victim again.”
The real winners from the cruel SEC and other related US programmes are the lawyers and other middlemen.
And the obscene bounties that are paid out in the few, select cases are excessive set against losses suffered by victims who remain uncompensated.
Occasionally, some whistleblowers have refused SEC awards out of conscience:
“I request that my share of the award be given to Deutsche and its stakeholders,”
The whistleblowing APPG and its secretariat WhistleblowersUK have waged a clearly well-resourced and increasingly glossy media campaign about UK whistleblowing reform which camouflage their intentions and their vaguely and worryingly drafted law to replicate SEC’s much maligned Office of the Whistleblower.
One of the APPG’s MPs is now in power and has wasted no time in calling for a review of UK whistleblowing law:
The Whistleblowing APPG have used poster boys and girls from health and social care in their campaigns, when whistleblowing about poor care is the last thing that would attract bounties. It is the financial sector that is the real prize. And even then only a few whistleblowers would benefit.
The great risk is that the APPG’s proposed vision would quickly descend into a racket, with the whole system trained on money making rather than public protection, with the great majority of whistleblowers discarded. The more lowly paid and disenfranchised, the more neglected. Nursing and care assistants have little enough voice already.
We have already seen quite enough degradation of our public life with greed, chumocracy and misconduct in public office.
We don’t need anymore.
No thank you to failed US policies or the bounty hunting sharks and their companions.
RELATED ITEMS
A much better US model is that of the Office of Special Counsel which looks after public sector whistleblowers – federal employees – it works on a lean model, seeks to apply redress during employment rather than after dismissal and works on the principle of restoring a whistleblower to the position they would have been in but for the whistleblowing. Most valuably, it can address non-financial detriment, such as restoring lost seniority and erasing unfair performance and disciplinary records. The principle is of more justice, not incentivising greed, stoking wasteful conflict or feeding a legal industry.
UK whistleblowing law, PIDA, is hopelessly weak, wasteful and was explicitly drafted to appease industry. It benefits the lawyers. It has caused no end of suffering to whistleblowers and contributed to countless public protection failures:
The law needs urgent replacement, but in that space, opportunists will exploit any chance they can to make money or build careers.
Those who have earned their daily bread from not rocking the boat and selling whistleblowing products from the last twenty years of PIDA’s jurisdiction will want to continue their business in a newly configured form. The bounty hunters will obviously want their taste. The academics will want to preserve their access to power and grants, and some may not be too discriminating about which tables they sit at. Some politicos will expect a berth in the Pullman carriage of the gravy grain.
It falls to un-captured and genuine whistleblowers with no personal agendas, seeking no personal gain, to speak up for the public interest and for future whistleblowers.
For any journos who want a quick primer on the legislative intentions of the whistleblowing APPG and the now Parliamentary Under Secretary of State at the Department for Business and Trade, here is a summary:
The care quality and governance scandal at University Hospitals Birmingham NHS Foundation Trust blew up in early December 2022 when BBC Newsnight broadcast concerns about poor culture at the trust.
Within days, on 8 December 2022 the commissioner of the acute hospital service, Birmingham and Solihull Integrated Care Board announced three reviews into UHB.
The first review undertaken was a rapid review of clinical safety by Dr Mike Bewick a GP and former deputy Medical Director of NHS England, who set up a private consultancy after leaving NHS England, IQ4U Consultants Ltd.
Bewick was deputy to Bruce Keogh, who was formerly a consultant at UHB prior to becoming Medical Director at NHSE. Keogh’s wife remained at UHB as a medical manager.
Bewick through his company IQ4U Consultants Ltd, which appears to have no website that I could find, has undertaken a number of investigations and reviews for the NHS.
Bewick’s latter role as a purported expert in safety and governance is somewhat at odds with the fact that he and others were criticised in Bill Kirkup’s report on the Morecambe Bay maternity disaster. Bewick was the then medical director for the local PCT and chaired an odd “Gold Command” response to the trust’s governance problems, under SHA directions. The Kirkup team saw little value in this misapplication of an emergency major incident procedure to ongoing governance issues, which served to burden the trust. For example:
“1.95 On 3 October 2011 the SHA, which had continued to regard the supposedly coincidental nature of the previous incidents as evidence that there was no systemic problem up to 10 September 2011,100 called a ‘Gold Command’. The intention appears to have been to offer support to the Trust in responding and accessing additional staffing, but the evidence we heard suggested that it served as much to distract senior staff in the Trust, who had to brief twice-weekly Gold Command meetings. We could find no evidence of defined exit criteria to underpin the closing down of Gold Command by Cumbria PCT, and it was not clear exactly what had been achieved when this was done. Overall, we were unconvinced that this represented the best way to address the situation.”
The Rosser Fiction
On 18 November 2022, UHB and the ICB both announced that David Rosser the controversial former CEO of UHB was stepping down for a new regional role as strategic director of digital health and care.
This was a fiction.
Rosser may have relinquished his role as UHB CEO, but he never left UHB and remained an UHB employee. He was merely “hosted” by the ICB, answering to the ICB’s CEO.
Through an FOI response of 16 February 2023, the ICB eventually admitted that Rosser had never departed and had remained employed by UHB all along.
This fact was not revealed until it was briefly alluded to in a BBC Midlands clip days before Bewick’s phase one report was published on 28 March 2023, and then covered on BBC Newsnight on the day of publication.
Information shared with Mike Bewick by the ICB
I asked Birmingham and Solihull ICB for clarification on whether Mike Bewick was informed of the fact that Rosser had NOT left UHB as publicly announced by UHB and the ICB.
The ICB answered evasively and avoided my questions.
After I pressed the matter, the ICB finally replied “Yes” to all three of the following elements of this question:
“Did the ICB inform Mike Bewick upon appointing him, to undertake the phase 1 rapid review into UHB, that David Rosser:
a) Was still employed by UHB?
b) Was “hosted” by the ICB?
c) Was reporting to the ICB CEO?”
That is to say, Mike Bewick has apparently known since early December 2022 that David Rosser was still a UHB employee, and had not left the trust as claimed by UHB and the ICB.
I am not surprised that the ICB was reluctant to reveal this information.
A number of questions arise.
Has Bewick investigated the misleading claims by UHB and the ICB?
If not, why not?
This is in the context that Bewick’s investigation terms of reference were unlimited and allowed him to go where the evidence took him.
Why did Bewick not comment on the irregularity in his rapid review report on UHB?
Was he unwilling to criticise the ICB, who commissioned his services?
Or did Bewick see nothing wrong in the way that UHB and the ICB misled the public and partner agencies?
For example, Healthwatch Birmingham have indicated to me that they received only the official briefings that Rosser was stepping down from UHB and knew nothing of Rosser’s continued employment by UHB.
Does the fact that Bewick did NOT report the Rosser fiction raise a concern about his role as an investigator of UHB’s governance?
The word “any” is troubling given issues such as recurrent haematology never events, A&E delays and such unsafe staffing that the CQC issued a warning notice in December 2022 at Good Hope Hospital. Revisiting Bewick’s report, it is clear that he knew about the warning notice, page 27: “Good Hope Hospital is the only one with a CQC regulatory notice at present (S29a for quality of healthcare requiring significant improvement, issued in Dec 2022”, but he claimedthat mitigation was in place.
Bewick also did not call up medical staff suspension, NCAS(PPA) referral stats or quote full GMC referral and outcome stats in his report, despite major concerns in these areas.
But fiction did become fact in one respect. Rosser’s retirement was announced on the day that Bewick’s report was published.
In a theatrical flourish, Bewick told the BBC that there might be more departures. This was not in his report.
But then neither was a reported claim that Bewick would be happy for his family to be treated at UHB, parroted by the hapless ICB CEO David Melbourne at a Joint Health Overview and Scrutiny Committee in February after briefing by Bewick.
What is needed is not theatre and misdirection, but facts and the whole truth.
Which would likely lead us to bad government policy and unsafe staffing.
Which is ultimately what so many NHS staff have been whistleblowing about. And so many compromised senior NHS managers with fat salaries and pensions have been trying to obstruct them, and are often richly rewarded for such efforts.
So, the ICB confirmed that Bewick knew from early December 2022 that Rosser had NOT left UHB’s employ. But Bewick kept mum.
Does that suggest that the reviews are a face-saving confection?
Dr Minh Alexander retired consultant psychiatrist 3 May 2023
I was interested in Healthwatch as a source of patient intelligence after Bewick declared University Hospitals Birmingham NHS Foundation Trust safe overall without mentioning patient complaints.
Local Healthwatch services support local communities to make use of health services.
They are ultimately funded by the Department of Health and Social Care. The funds are routed through local authorities. There are currently 152 local Healthwatch organisations which collectively receive £250,400,000 via local authorities to carry out their statutory activities for year 2022/23.
(i) advising the Care Quality Commission through information supplied to Healthwatch England – a subcommittee of the CQC, and of
(ii) providing local communities with information about access to local services.
The government also intended that local Healthwatch organisations should:
“…act as local consumer champion representing the collective voice of patients, service users, carers and the public, on statutory health and wellbeing boards”
However, Healthwatch Birmingham does not publish data on concerns received from the public.
It has an online feedback page where some comments by the public can be seen, good and bad, and some organisational responses can also be seen.
I asked Healthwatch Birmingham for its data on complaints and concerns.
I also asked if there was any restriction on whether this data could be routinely published, and whether commissioners request that the complaints and concerns data is reserved only for commissioners and regulators. This is because Healthwatch Birmingham informed me that despite not publishing the data, it did in fact collate it and routinely sent a report to commissioners and regulators on a quarterly basis.
Healthwatch Birmingham has now shared the numbers of concerns received from the public since 2018, but with no qualitative summary about these concerns. It has also not answered the question about whether its contract requires it to reserve data on complaints and concerns for commissioners and regulators only.
Notwithstanding, HW Birmingham has indicated that due to escalating concerns received from the public in 2021 about UHB, it asked to meet with the CQC and has continued to do so on a monthly basis.
“Over the course of 2021, we raised additional concerns with the CQC on several occasions following an increase in negative feedback and concerns from the public received by Healthwatch Birmingham and Healthwatch Solihull, and intelligence personally received by our Chair. We had also noted UHB’s poor performance in published NHS waiting list statistics and we raised these issues with the CQC. As a result the CQC agreed to meet us monthly to update us on their monitoring of UHB. These meetings continue.”
CQC conducted an unannounced inspection of UHB in June 2021 when it concluded that: “Managers shared feedback from complaints with staff and learning was used to improve the service.”
Although CQC dropped the overall UHB trust rating to “Requires Improvement”, its inspection report implied that much of the turmoil at the trust was COVID-related.
CQC maintained, despite several FPPR referrals on UHB’s then CEO David Rosser, the trust was “Good” under the Well Led domain.
In July 2021, the CQC was additionally warned by UNISON who submitted a formal dossier of staffside concerns about mismanagement at UHB.
The figures now released by HW Birmingham show that concerns from the public spiked even more sharply in 2022.
Figures for 2023 so far suggest that the rate of concerns remains much elevated.
According to HW Birmingham, although Healthwatch England is a sub-committee of the CQC and the Chair of HW England is a CQC board member, local Healthwatch organisations do NOT have the power to trigger CQC’s Emerging Concerns Protocol. So there is structural inequality – the patients’ champions may report upwards but they have no hands on any levers. Supplication only.
Neither did the PHSO think to alert the local Healthwatch, the nearest thing to the official local voice of patients, when it triggered the Emerging Concerns Protocol.
HW Birmingham’s Chair is a member of the external reference group which has the role of maintaining independent oversight of the ongoing Bewick reviews of UHB governance.
HW Birmingham has through its Chair made a number of statements about the UHB scandal:
In none of these statements is it disclosed that there was a very marked spike in concerns received by HW Birmingham, or that HW Birmingham has been holding frequent meetings with the Care Quality Commission in consequence. I appreciate there may be contractual constraints on Healthwatch organisations.
There is an expression: The truth, the whole truth, and nothing but the truth.
The scandal at UHB was allowed to happen. It did not spring forth fully formed. It was conceived when government policy failed to protect clinical quality, it was nourished when certain directors were appointed. It was incubated when whistleblowers were ignored and thrown back to the wolves, when safe staffing was deemed an optional extra. As at MidStaffs, poor care was normalised and regulators did not put patients first. Poor culture was not addressed and was instead perpetuated when abusive executives were excused and protected.
Taking the microscope, and not a very good microscope at that, to UHB alone is not enough. What happened at UHB happens elsewhere still, and there will be more UHBs.
It is the central governance of the NHS and government policy that needs proper examination, as acknowledged by the HW Birmingham statement of 9 December 2022.
But how likely is that? Rather, secrets and Bewick’s Bendy Hall of Mirrors prevail.
UPDATE 7 MAY 2023
I have written to Mike Bewick to formally ask that he reviews UHB patient complaint data as part of his reviews:
BY EMAIL
Dr Mike Bewick
4 May 2023
Dear Mike,
FOI data from Healthwatch organisations on concerns received from the public about UHB
Please find attached FOI data from local Healthwatch organisations which shows escalation in concerns received from the public about UHB since 2021, which was such that Healthwatch has been holding monthly meetings with CQC since 2021.
I hope your reviews into UHB will now include some examination of patient complaints data, with both quantitative and qualitative analysis.
With best wishes,
Minh
Dr Minh Alexander
Cc BBC Newsnight Nancy Cole ITV Becky Johnson Rob Behrens PHSO Preet K Gill MP external reference group Dr Chaand Nagpaul external reference group
It is a political instrument of control and helps to serve whatever master is in power. Workforce intimidation can help to hide failures of policy and lack of resources.
In the last thirteen years, we have seen particularly extreme manifestations of this suppression, especially during the pandemic, and we now see unprecedented NHS strikes as a point of no return is reached in government’s ransacking of the public purse and public services.
I hope the letter below to the CEO of the General Medical Council pressing for active measures to identify rogue employers who abuse referrals to the GMC as an improper way to punish doctors, sometimes whistleblowers, is self-explanatory.
LETTER 1 MAY 2023 TO CHARLIE MASSEY CEO GENERAL MEDICAL COUNCIL
BY EMAIL
Charlie Massey
Chief Executive
General Medical Council
1 May 2023
Dear Charlie,
After the Hooper Review and UHB: GMC’s wider system for identifying rogue employers
I write to ask about the General Medical Council’s systems for early identification of rogue employers and thus for protecting doctors from abuse by such employers.
At University Hospitals Birmingham NHS Foundation Trust it has emerged that the consultant body raised a concern with the trust board about cronyism at every level of medical management.
Obviously this would be a grave issue both in terms of safe working environment for doctors and patient safety, as it would create an atmosphere that is unconducive to raising public interest disclosures and it would more likely result in arbitrary treatment of any doctor who raised concerns.
Unsurprisingly, alongside the concerns about cronyism affecting UHB medical management, there have also been reports of arbitrary application of discipline and rapid escalation of disciplinary procedure and GMC referrals.
UHB last year issued inaccurate FOI data about its pattern of GMC referrals and outcomes which caused alarm.
From December 2022 onwards I made several requests for corrected data, after I noticed that UHB’s FOI response could not be true.
The trust has now corrected the record and claimed that these are the true facts:
RESPONSE BY DAVID BURBRIDGE, UHB CHIEF LEGAL OFFICER, 13 APRIL 2023
Dear Dr Alexander
Please find below a response to your email to Dame Yve Buckland, dated 29 March.
For the period 1 April 2012 to 31 March 2022:
– How many doctors the trust referred to the GMC ?
At UHB (prior to and post the merger with Heart of England NHS Foundation Trust (“HEFT”)) there were 22 referrals
At HEFT (prior to the merger with UHB) there were 16 (3 of these are dated just after the date of merger 1.4.2018, but are attributed to HEFT – we believe this may be because there was contact before the change of RO)
– How many of these referrals were signed off by the medical director?
At UHB 14/22, the remainder were signed off by Deputy Medical Director or acting Medical Director At HEFT 6/16 were signed off by the Medical Director and the remainder were by Deputy or Associate Medical Directors.
– How many of these referrals resulted in no further action by the GMC?
UHB – 4 were concluded at triage, 7 were investigated and concluded with no action, 11 were subject to advice, warning, undertakings, suspension or erasure HEFT – 3 were concluded at triage, 4 were investigated and concluded with no action, 9 were subject to advice, warning, undertakings, suspension or erasure
– How many doctors died whilst under GMC investigation or monitoring? None
– How many doctors died by suicide whilst under GMC investigation or monitoring? None Regards
David Burbridge Chief Legal Officer
As you can see, this still leaves 18 out of 38 GMC referrals by UHB which ended in cases being dropped at triage or no further action being taken by the GMC, in a ten year period.
Information request
With respect to UHB:
I would be grateful if the GMC could verify if the most recent data supplied by UHB is indeed the correct picture.
Could the GMC additionally clarify in the 20 cases where it reportedly took action, in how many of these UHB cases did the action consist only of advice given to the referred doctor?
Where the GMC action comprised solely of advice given to the referred doctor, was a GMC referral really necessary or would a less formal and drastic route of addressing concern have been possible and/or preferable?
More generally:
What mechanism(s) does the GMC have in place, if any, to detect whether individual employers are making inappropriate or abusive GMC referrals?
What early warning signs does the GMC track, if any, to alert itself of poor employer practices with respect to GMC referrals?
Has the GMC estimated at national level what proportion of GMC referrals annually by employers are inappropriate and/or could have been dealt with another means?
If so, please give the total percentage of GMC referrals annually which the GMC believes could have been avoided.
What policies and strategies does the GMC have in place to address inappropriate referrals, and how does it measure the effectiveness of these policies and strategies?
What quality indicators does GMC monitor, if any, on each employer’s GMC referrals?
What comparative data does GMC collate centrally, if any, to track differences between employers’ behaviour, in terms of quality and outcomes of GMC referrals?
Can the GMC, based on its current systems and data collection, tell whether some employers are outliers in terms of higher rates of GMC referrals which end in no case to answer, no further action, or only advice given?
Does the GMC collate central data on whether it raises concerns with individual employers about poor referral practice or gives formal warnings to individual employers and medical managers about poor practices such as vexatious GMC referrals or GMC referrals which are suspected to be vexatious?
Has the GMC in the last five years disciplined any senior doctor for abusing power and vexatiously referring a doctor under their line management to the GMC, for example, by carelessly or knowingly making a false allegation?
If so, on how many occasions has this happened and what was the GMC sanction(s) applied, for example, undertakings, warning, suspension or erasure etc?
If the GMC currently has no system for tracking poor GMC referral practice by individual employers, and for publishing such comparative data, will it give consideration to doing so in future?
If the GMC does currently track this data but does not publish it, will it give consideration to doing so in future?
Will it also consider a change to Good Medical Practice guidance to specifically make it a proscribed practice for doctors in leadership positions to carelessly or knowingly make unsubstantiated or false GMC referrals or PPA referrals on doctors whom they manage?
Lastly, GMC previously kindly shared a status update on its Hooper implementation project. Could it do so again?
I copy this to Mr Reuser and to Mr Watkinson who as the GMC will be aware, were proven to have been mistreated by UHB. They were referred to the GMC based on very flawed governance processes. This included UHB supplying NCAS (now PPA) with false information.
PPA has since kindly changed its processes, and is now considering strengthening more processes. I hope GMC will do the same.
I am aware of other doctors who have been referred by UHB to the GMC under contentious circumstances, and I hope they will in due course have some resolution of their issues.
As you will know only too well, a GMC referral is a massive upheaval in most doctors’ lives and will cause the majority huge distress and major health consequences. This will be compounded when the referring employer acts in bad faith and is not only unsupportive but actively persecutory.
I also copy this letter to Chaand Nagpaul who is on the external reference group for the ongoing reviews into UHB’s governance.
Dr Minh Alexander retired consultant psychiatrist 29 April 2023
The Parliamentary and Health Service Ombudsman told BBC Newsnight that it triggered this protocol for the first time ever at University Hospitals Birmingham NHS Foundation Trust in the summer of 2022 because of concerns about UHB’s culture and leadership, with respect to learning from serious incidents.
PHSO advised me it attended multi-agency meetings about its concerns on UHB on 4 August 2022, 12 October 2022, 10 January 2023 and 7 February 2023.
A 65 year old man died avoidably at UHB in 2019 of intestinal obstruction after doctors failed to interpret clinical signs and read an abdominal x-ray correctly.
His sister was wrongly told that he had constipation and dehydration.
His family were awarded compensation in the higher PHSO range of £10,000.
I asked CQC if it had ever triggered this protocol at UHB.
CQC’s FOI reply of 28 April 2023 revealed that it had never done so, not even after receiving the dossier from UNISON in July 2021 about extensive UHB staffside concerns regarding unsafe staffing and poor management behaviour. Or the FPPR referrals on Rosser the former UHB CEO or the blood products never events.
Consistent with this lack of action upon the UNISON dossier, CQC indicated that it had not attended any regulatory risk summit meetings on UHB in the four years prior to 31 March 2022.
“CQC did not attend, and does not hold information about, any regulatory risks summit meetings (or similar) held about UHB in the 4 years up to 31/03/2022”.
CQC refused to say what regulatory risk summit meetings it had attended since then:
“CQC will not disclose whether or not we have attended any regulatory risks summit meetings (or similar) about UHB since 01/04/2022 as disclosing recent information about this type of activity would be likely to be prejudicial to the exercise of our regulatory functions.”
The regulator implied that information sharing had occurred outside of its emerging concerns protocol:
“It should be noted that the ECP is not the only mechanism or legal framework for regulators to share information. Nor is it designed as a mechanism for sharing only the most serious or substantial information of concern.”
However, the lack of any regulatory risk summit meetings in the four years up to 31 March 2023 suggests that CQC simply did not consider there were serious problems at UHB (or alternatively did not wish to acknowledge them).
It was not until after the first BBC Newsnight broadcast that CQC carried out the unannounced inspections in December 2022 which led to the recent issue of a warning notice about unsafe staffing, which UHB have been whistleblowing about for years now.
Trust board papers show that falls with serious or catastrophic injuries are a regular occurrence.
Why is CQC simply issuing a warning notice and not conducting a Regulation 12 investigation given the history of repeated unsafe staffing and regular falls with serious patient injuries?
Probably for the same reason that it did not act on UHB staff concerns in the first place and continued to rate the trust as ‘Good’ until the problems were exposed by the media.
Dr Minh Alexander retired consultant psychiatrist, 27 April 2023
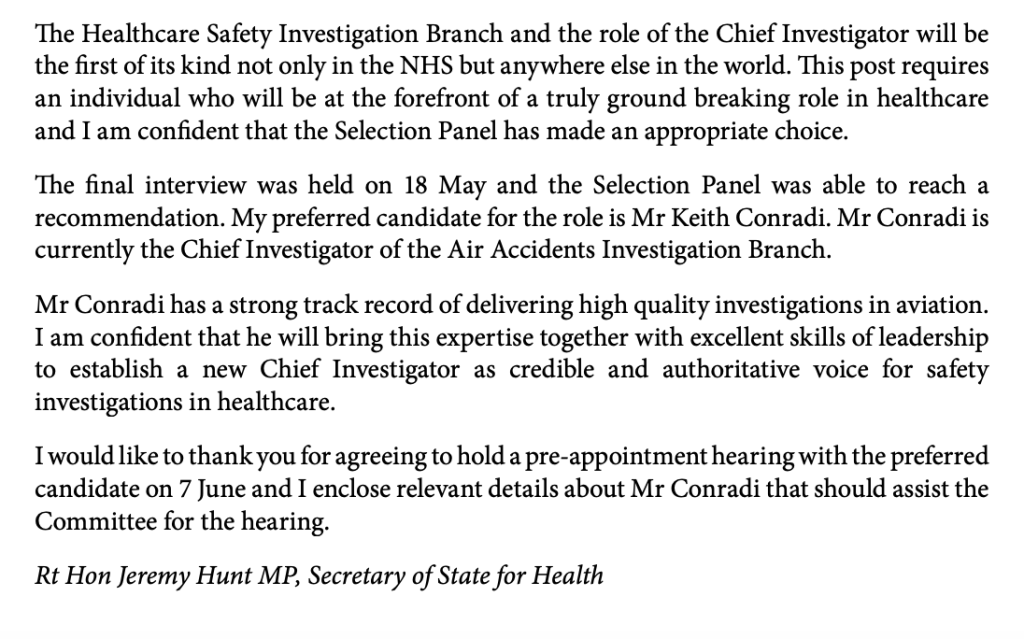
On 20 April 2023 the principal author of a HSIB report appeared courageously at the current NHS England Employment Tribunal at Reading as a witness for the claimant.
HSIB’s Chief Investigator Keith Conradi asked her to undertake this review in her then capacity as Acting Head of Investigation Education, Learning and Standards.
She led the 2020 review, working with two other colleagues.
They found a number of disturbing shortcomings in the regionally based HSIB maternity programme, including issues of bullying.
In her witness statement to the Employment Tribunal, she corroborated the claimant’s report of being victimised for raising concerns about HSIB’s maternity investigations. She gave evidence of a recognisable pattern of bullying in the organisation, that other staff had also reported after raising concerns.
In response to questions from Tribunal members, she observed that the claimant had been bullied to the point of being “traumatised”.
I will leave it to the media to report in more detail about these matters.
The issue that I wish to highlight is from documents disclosed in the Tribunal bundle.
Until now, NHS England had only released a redacted copy of the 2020 Benson report, which was provided under FOI in May 2022.
Contained in the current ET bundle are two un-redacted slides from the report, revealing some of what had hitherto been concealed:
Reported messages from the HSIB senior team to the HSIB workforce that “jobs will be threatened” if the maternity report backlog was not cleared, and that staff were consequently pressured to produce reports
Some staff had left HSIB because they felt compromised by the investigation process, but were also fearful of reprisal by HSIB once they were back in clinical roles
How can there be just culture if investigators are coerced into hurried investigations that fail to fairly identify all contributory factors?
The slides support the claimant’s contentions that there was an unsafe management drive to churn out investigation reports at a cost to thoroughness.
It is troubling that the message about the threat to jobs and pressure to churn out reports reportedly came from the HSIB senior team.
Would that explain Keith Conradi/ HSIB’s later reluctance to deal properly with the claimant’s whistleblowing about management pressure to produce reports and poor handling of maternity investigations, as found by the Susan Newton investigation?
Was there a conflict of interest?
If Conradi was ultimately responsible for any undue, top down pressure to clear the maternity report backlog without proper regard for safety, he should have recused himself from dealing with the claimant’s case.
The two slides from the ET bundle, along with the redacted versions for comparison, are provided below.
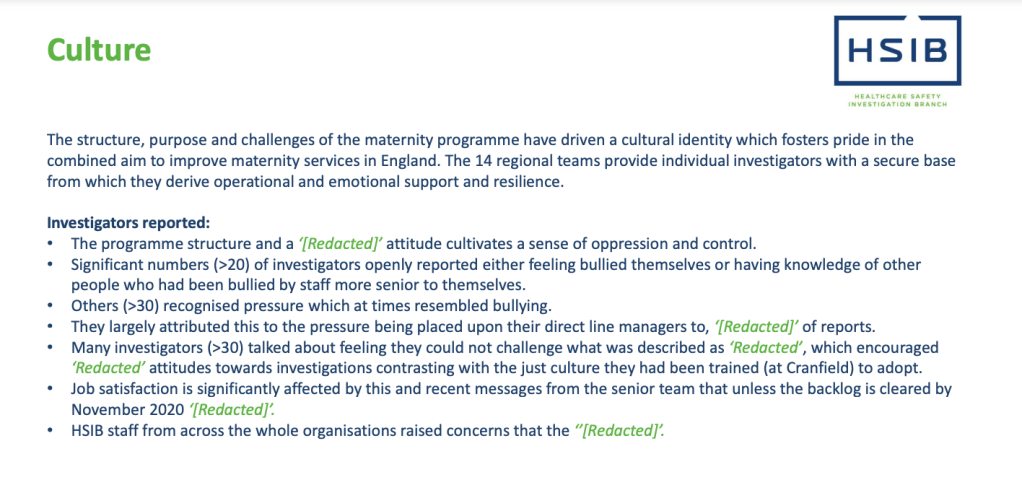
PREVIOUSLY UNDISCLOSED SLIDE (1)
The content of this slide is copied from the ET bundle. There was highlighting on the slide, which is reproduced below.
“Culture
The structure, purpose and challenges of the maternity programme have driven a cultural identity which fosters pride in the combined aim to improve maternity services in England. The 14 regional teams provide individual investigators with a secure base from which they derive operational and emotional support and resilience.
Investigators reported:
Significant numbers (>20) voluntarily reported either feeling bullied themselves or having knowledge of other people who had been bullied by staff more senior to themselves.
Others (>30) recognised pressure which at times resembled bullying.
They largely attributed this to the pressure being placed upon their direct line manager to ‘reduce the backlog’ of reports
Many investigators (>30) talked about feeling they would not challenge what was described as ‘clinical dogma’, which encouraged ‘blamey’ attitudes towards investigations contrasting with the just culture they had been trained (at Cranfield) to adopt
Job satisfaction is significantly affected by this and recent messages from the senior team that unless the backlog is cleared by November 2020 – ‘jobs will be threatened’ (MI)
HSIB staff from across the whole organisation raised concerns that the ‘culture within the maternity programme could tarnish the reputation of the whole organisation’
This is the redacted version of this slide which appeared in the Benson report
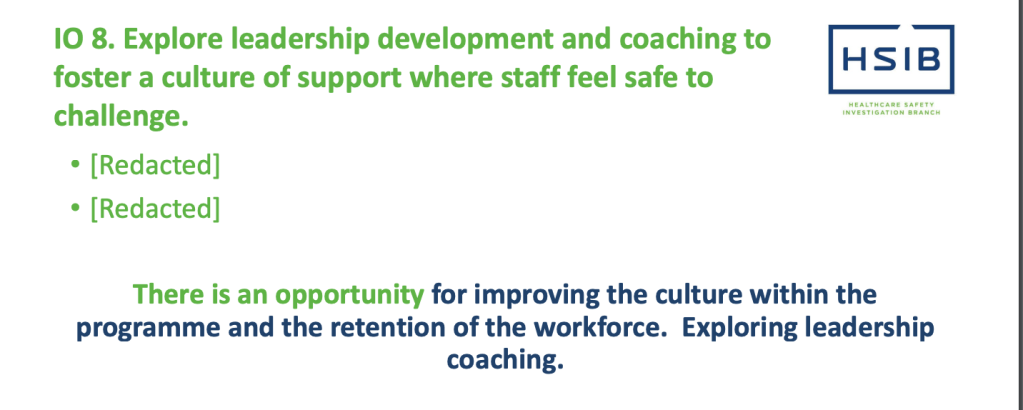
PREVIOUSLY UNDISCLOSED SLIDE (2)
The content of this slide is copied from the ET bundle. There was highlighting on the slide, which is reproduced below.
10.8 Explore leadership development and coaching to foster a culture of support where staff feel safe to challenge
Staff talked about feeling ‘bullied’ or others being ‘bullied’ or targeted if they ‘put their head above the parapet and challenge the senior team’
Staff were not asked about being bullied, some staff volunteered this information
The evaluation team recognise this has not been explored across the whole maternity structure
Staff, who have left HSIB because they felt the investigation process compromised their integrity, reported fear of reprisal from the HSIB maternity programme senior management once they were working back in a clinical environment
This is the redacted version of this slide which appeared in the Benson report
There had in fact been another highly significant investigation, by an external consultancy, Susan Newton Ltd. This took place in early 2021.
It was commissioned as a Freedom To Speak Up investigation by the central whistleblowing team at NHSE/I, to look into a whistleblowing case that is the subject of the current NHS England Employment Tribunal at Reading.
So NHS England tried to mislead me by omission. What’s new.
Susan Newton herself posted CV details of an investigation that she undertook in 2021 as follows:
March to June 2021: “Conducting a wide ranging investigation into whistle-blowing allegations relating to management culture and work practices. Findings and recommendations presented to the Board.”
NHS England’s lawyers delayed my access to the Reading ET case bundle, and it was not until after several rounds of correspondence to the Tribunal and Tribunal Judge that access was finally facilitated on 24 April 2023, at which point I was finally able to see the Newton report.
For any journalists covering the case, the Newton report starts at page 622 of the ET bundle.
As might be anticipated, the Newton report was not flattering of HSIB leadership.
I will leave the media to pick up the bulk of the details.
But in terms of the crucial whistleblowing governance, Newton found it unfathomable that the organisational response was to apply a grievance process to what was “clearly a whistleblowing complaint”.
Moreover, the decision to apply a grievance process was apparently not recorded.
But Newton suspected that senior managers influenced the decision.
Keith Conradi HSIB’s Chief Investigator received the claimant’s disclosure after disclosure to local managers was thwarted, and he was responsible for the central response.
Newton suspected that the grievance process was in part an attempt to keep the issues contained within HSIB:
“….there appears to have been an unwillingness to identify the complaint correctly and a desire to keep the whole process within HSIB”
Newton noted that a grievance process was applied despite advice by the HSIB Director of Corporate Affairs that it was a whistleblowing matter.
Newton expressed surprise that although the grievance process was very flawed, failed to follow the grievance policy and was full of omissions, it was deemed “very thorough”.
“The process deviated so far from policy that [the claimant] thought she had been referred to a different policy”
Newton pointed out in her report that this was despite Conradi reviewing the grievance documents himself, and thus omissions should have been evident to him.
“The Chief Investigator, as the Commissioning Officer, reviewed all the relevant documents so it is even more surprising that the investigation was deemed “very thorough” as it might have been assumed he would have easily identified the flaws given his role.”
Newton concluded that the whistleblower was not properly protected as a result of the organisational response.
Importantly, Newton took the claimant’s disclosures about conflicts of interest arising from HSIB maternity teams being regionally based very seriously and agreed entirely with her that this needed to be rigorously managed.
It is in the legal directions for HSIB that the independence of HSIB and its investigations must be maintained. Therefore, conflicts of interest would be incompatible with this legal obligation and breaches would be a matter that would fall under PIDA.
Newton’s professional response to the claimant’s concerns is in stark contrast to the response of local HSIB managers, who had told the claimant that she should not disappear down “rabbit holes” and who had sent emails discrediting her, including derogatory remarks about her “fixated” and “unstable” mental state.
It seems strange that NHS England was willing to pay good money for the advice from Newton and acted upon it by commissioning the King’s Fund external review of culture and leadership at HSIB, a further significant expense, but now apparently rejects the notion that the whistleblower was a whistleblower.
In an amended ET3 (Grounds of Resistance) of 31 January 2022 and throughout cross examination of the claimant. NHS England’s representatives have disputed that the claimant made protected disclosures:
“It is not accepted that the alleged disclosures at paragraph 2.1.1 of The Issues amount to protected disclosures.”
I have not finished by any means looking at the trail of disclosure correspondence in the bundle between the claimant and HSIB managers. I doubt that I will in the restricted time remaining. However, from what I have seen, I am perplexed by NHS England’s contention that no protected disclosures were made. Or perhaps I am not.
Importantly, in correspondence to Tom Grimes NHSE/I head of whistleblowing, Susan Newton reported to NHS England that during the course of her investigation, other HSIB staff also started whistleblowing to her.
Importantly, Newton also recommended at the end of her investigation that there should be an independent investigation into the claimant’s unresolved patient safety concerns:
“The safety concerns by [the claimant] should be investigated by a qualified and experienced person outside of the Maternity programme, and appropriate action taken internally and if appropriate, externally to satisfy all parties that this has been appropriately investigated and action taken.”
What happened to that?
The claimant does not believe her concerns were addressed and in fact has pointed out that NHS England seems to have lost some of the evidence relating to her clinical concerns.
NHS England made the claimant wait months before it gave her the Newton investigation outcome.
Susan Newton wrote to NHSE in September 2021 about this delay, to say she had “huge sympathy” for the claimant and that she could not believe that the claimant had not yet been told of the investigation outcome.
“I can’t believe she still hasn’t heard anything”
Prior to giving the claimant the Newton report outcome, Tom Grimes wrote an emollient email to KeithConradi Chief Investigator of HSIB:
Email dated 5 November 2021, headed “[Name of claimant] summary report”
“Dear Keith,
I hope your recovery is going well.
I am sure you will have been expecting to receive the attached finalised summary report regarding the [name of claimant] FTSU case. It’s not been shared with anyone else at HSIB but we will need to share it with [claimant] very shortly.
I understand you are due to speak to Aidan today, and so you will have an opportunity to discuss it with him.
If you can confirm receipt, I will then share the password with you, or you can obtain it from Aidan.
With very best wishes,
Tom”
The tone of the NHSE correspondence to the increasingly distressed claimant is in contrast to this.
Email dated 26 November 2021, headed “Confidential – Susan Newton’s report” from Tom Grimes to the claimant
“Dear [Claimant],
Thanks for your email. I will respond to your email in order.
Yes. This is a summary of Susan’s report.
Sophie Ellis was an NHS Improvement legal director at that time. To be clear, referencing her role does not waive legal privilege in respect to any legal advice she gave. There was no formal escalation process to the NHSI Legal Team because HSIB HR and Legal is separate to NHSE/I. Sophie did not formally oversee HSIB HR matters but was available for ad hoc advice. It was in that way that your case was raised with Sophie. Sophie responded to one brief, high level query and no further input was sought by HSIB. HSIB continued with the conduct of the case. It is not clear that Sophie’s advice was interpreted accurately by HSIB staff.
The delay was clearly regrettable and there is a limit to how much explanation I can provide. However, the report’s findings impacted on others and as I explained on 28 April, before we could release the summary report to you we needed to consider carefully how the findings of the report were shared with you and others. Recognising the impact on you of the delay, I informed you on 28 May that, in relation to each of element of the ToR of the FTSU investigation, the investigation found flaws in handling of your grievance and in responding to the original concerns themselves.
I hope that’s helpful.
With best wishes.”
What is quite obviously missing in the NHSE response is the fact that the claimant was not immediately told of Susan Newton’s recommendation that her unresolved patient safety concerns should be independently investigated.
Patients. What are patients? What do they look like, these things called “patients”? Has anyone seen one?
But as all whistleblowers, patients and families know, the D’s prevail.
Delay, deny, defend.
And of course, the most important names are usually kept out of the picture.
I have written to Dr Aidan Fowler NHS England National Director of Patient Safety in England and a Deputy Chief Medical Officer at the Department of Health and Social Care, who oversaw this matter, and also oversaw the King’s Fund review and the HSIB maternity schism.
I have asked him more precisely what elements of the Newton report’s findings were accepted by NHS England, with reference to NHSE’s current rejection of the claimant’s protected disclosures.
I have also asked for clarification of whether NHSE acted upon Susan Newton’s recommendation that the claimant’s unresolved patient safety issues should be investigated.
LETTER TO AIDAN FOWLER
BY EMAIL
Dr Aidan Fowler
National Director Patient Safety, NHS England
Deputy Chief Medical Officer, Department of Health
25 April 2023
Dear Aidan,
Action upon 2021 Whistleblowing investigation into Healthcare Safety Investigation Branch/ NHS England by Susan Newton
As you will be aware, this investigation took place in the Spring of 2021 but the affected whistleblower was not provided with a summary report by NHS England until November 2021.
This is of huge concern because one of the most important recommendations from this report was that an external investigation was required into the whistleblower’s unresolved patient safety concerns. Susan Newton recommended:
“The safety concerns by [the claimant] should be investigated by a qualified and experienced person outside of the Maternity programme, and appropriate action taken internally and if appropriate, externally to satisfy all parties that this has been appropriately investigated and action taken.”
As a far as I can see, this has never been acted upon, or if has been acted upon, it has been done secretly and without involving the whistleblower, against the terms of the recommendation.
The whole safety of the HSIB maternity investigation programme has since come into serious question and has had to be remodelled nationally.
I should also point out that NHS England has been improperly hiding the existence of this 2021 whistleblowing investigation and misled me by omission in an FOI response, which adds to the impression of suppression.
The report is now in the public domain at page 622 of the bundle of an Employment Tribunal claim currently being heard at Reading, and shows shocking governance failures in a safety agency.
Susan Newton the investigator clearly accepted the validity and seriousness of the whistleblower’s public interest disclosures and made a slew of recommendations flowing from this, which as far as I can see NHS England broadly accepted in that it commissioned a review of HSIB’s culture and leadership as advised.
However, NHS England has since reversed and has claimed to the Employment Tribunal that the whistleblower has NOT made protected disclosures, which seems a disturbing position. I have been observing the Tribunal proceedings and have been very surprised by some of NHSE’s barrister’s contentions, such as an assertion that a concern about tampering with medical records is not a qualifying disclosure under UK whistleblowing law. This implies that NHS England does not consider tampering with medical records is unlawful, even though an investigation of records falsification by a predecessor body in 2012 determined that tampering breached a number of legal obligations. There are also other ways in which medical records tampering may be relevant to UK whistleblowing law.
NHS England might wish to review how it instructs counsel generally, but in particular in the conduct of whistleblowing cases, given its recent defeat in Cox v NHSE. Also the Care Quality Commission’s recent defeat in Kumar v CQC, where CQC defamed the whistleblower repeatedly.
It tends to have a chilling effect on the workforce and is contrary to national Freedom to Speak Up strategy to see these cases play out in this way.
I would be very grateful for the following clarification:
1. Which of the findings of the 2021 Susan Newton whistleblowing investigation report did NHS England accept?
2. Which of the findings of the Susan Newton whistleblowing investigation report did NHS England reject?
3. What follow up actions did NHS England take pursuant to the Susan Newton whistleblowing investigation report?
4. What actions did NHS England take in relation to Susan Newton’s recommendation that NHS England arrange an external investigation into the whistleblower’s unresolved patient safety concerns, as per the terms above?
5. If NHS England did NOT undertake an external, independent investigation into the whistleblower’s unresolved patient safety concerns, what was the recorded decision for this, assuming a decision was recorded?
I copy this to Mr Vineall at the Department of Health whom I understand has oversight of these matters and to the relevant parliamentary committees.
For parliament’s information, I should point out that in a five year period including the 2021 HSIB whistleblowing investigation, NHS England indicated via FOI that it paid Susan Newton Ltd over £140K for several pieces of complex Human Resources work.
One imagines from the recurrent commissions that NHS England was satisfied with the quality of the work commissioned.
Many thanks,
Minh
Dr Minh Alexander
Retired consultant psychiatrist
Cc William Vineall Director of NHS Quality, Safety, and Investigation DHSC
Public Accounts Committee
Health and Social Care Committee
UPDATE 27 APRIL 2023
I have today shared disclosed documents from the ET which reveal previously withheld data from the Benson review. The un-redacted extracts from the Benson report show reports that the HSIB senior team told the HSIB workforce there would be a “threat to jobs” if the maternity report backlog was not cleared. Staff told Dr Dawn Benson and her co-reviewers of related pressure to churn out reports. Some left HSIB because they felt investigation integrity had been consequently been compromised, but feared reprisal by HSIB senior management after they returned to clinical roles. Issues about staff inability to challenge HSIB senior managers were identified.
If Keith Conradi HSIB Chief Investigator had ultimate responsibility for the undue pressure on HSIB maternity investigators to churn out investigation reports without due regard for safety, he should have recused himself from dealing with the claimant’s whistleblowing case about these issues.
Dr Minh Alexander retired consultant psychiatrist 24 April 2023
Background
The HSIB maternity investigation programme was commenced as a political vanity project, against professional advice, under Jeremy Hunt’s tenure as Health Secretary.
Its ambitious brief was to replace local NHS maternity investigations, a huge task.
These are the legal directions for establishment of the programme in 2018, which emphasised unequivocally that HSIB investigations must“identify all contributory factors that led to that outcome”:
HSIB a tiny, centralised specialist investigative agency mushroomed rapidly into a sprawling body with maternity branches based in the regions, that operated on different directions.
Who could have predicted that things would go wrong?
It is thanks to HSIB maternity whistleblowers that the public became aware of serious deficiencies in what should have been a vital safety service.
With great reluctance, NHS England later released some of the relevant reviews about these matters, which it had previously suppressed from public view:
In a later interview he claimed that senior leadership at NHS England did not prioritise patient safety, in a seeming attempt to justify his own position.
Slow and incomplete HSIB maternity investigations, Death of baby Theo Young and Coroner’s serious criticisms of HSIB
In a current Employment Tribunal case against NHS England, the claimant said in oral evidence last week, that she was concerned both that HSIB was not turning investigations around fast enough and that management tried to restrict the scope of her investigations.
This was set against the 2018 HSIB directions which required investigators to identify ALL contributory factors.
A corroborating piece of information about the general concerns about HSIB’s maternity investigations already lies on the public record.
This is the findings from the 2020 inquest of baby Theo Young who died under the care of Surrey and Sussex Healthcare NHS Trust (SASH) in 2018 (not to be confused with the well publicised and also avoidable death of baby Theo Ellis at Frimley).
The Surrey Coroner, Karen Henderson, found that baby Theo died of perinatal hypoxia contributed to by neglect. He was allocated to an inexperienced midwife who did not recognise a pathological CTG reading and did not escalate to a more senior midwife or obstetrician, and he would probably have survived if help had been sought appropriately.
Notably, the coroner was very concerned about the actions of HSIB in this case and issued a Prevention of Future Deaths notice that solely related to the actions of HSIB in forbidding the trust to undertake a local investigation whilst exceeding its own target six month target, and not producing an investigation report until eighteen months later, which was substandard.
The MATTERS OF CONCERN are in relation to the role of the HSIB in their conduct, investigation and conclusion:
1. The HSIB specifically requested the Trust not to undertake their own investigation effectively preventing the recognition of causes of concern and therefore being unable to undertake any immediate and necessary remedial action at the earliest opportunity to prevent future deaths.
2. HSIB indicated to the Trust at the outset that their investigation would take approximately six months which is highly likely to delay the introduction of any immediate necessary measures by the Trust to prevent further deaths.
3. The initial draft report contained factual errors and inaccuracies requiring considerable input by the Trust to resolve. The final report is insufficiently detailed and was completed 18 months after the death, during which time further deaths could have resulted.”
It is quite something that an agency that is supposed to help prevent deaths was found to have obstructed learning and so endangered the public.
The coroner added in her PFD notice that she had other concerns about HSIB which did not fall under PFD remit, but which she would be taking up.
“Other matters were brought to the attention of the court outside of PFD matters which raise considerable concern as to the role and actions of HSIB which I will deal with in a letter to them in due course and will be shared with other relevant bodies.”
Keith Conradi replied on behalf of HSIB to the Coroner’s PFD in what did not appear in my opinion to an especially conciliatory tone and did not demonstrate measurable learning with respect to evidence of improvement.
HSIB made similar comments to the Health Service Journal.
The Department of Health through Nadine Dorries also replied but did not appear to take any effective action to hold HSIB to account.
These are the various organisational responses to the Surrey Coroner’s PFD on baby Theo Young:
I have asked Ted Baker about what evidence HSIB subsequently tracked on the timeliness of its investigations, such as how soon after incidents did interviews with involved staff take place.
I have also asked him about the “other matters” that caused the Coroner considerable concern.
The Employment Tribunal against NHS England continues, with substantial media presence.
The Claimant’s evidence is expected to resume today.
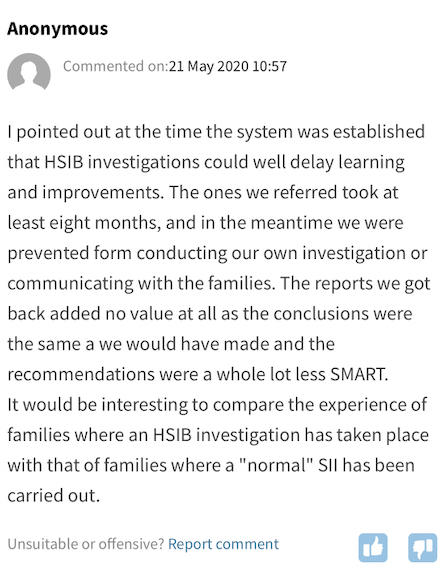
This is a comment left anonymously under the article in HSJ about the Coroner’s criticisms of HSIB in the Theo Young case. It seems that other trusts, unsurprisingly, may have had similar misgivings, lending further credence to the concerns currently being aired in the NHS England ET:
Dr Minh Alexander retired consultant psychiatrist 23 April 2023
Yesterday I reported on an issue that arose from a current Employment Tribunal against NHS England, in the context of the weakness of UK whistleblowing law.
This implied that such a disclosure did not fall under any of the following categories of qualifying disclosure:
“a)that a criminal offence has been committed, is being committed or is likely to be committed,
(b)that a person has failed, is failing or is likely to fail to comply with any legal obligation to which he is subject,
(c)that a miscarriage of justice has occurred, is occurring or is likely to occur,
(d)that the health or safety of any individual has been, is being or is likely to be endangered,
(e)that the environment has been, is being or is likely to be damaged, or
(f)that information tending to show any matter falling within any one of the preceding paragraphs has been, is being or is likely to be deliberately concealed.”
In response to this assertion, I posited how tampering with medical records might fall under the categories of “a breach of a legal obligation”, “endangerment of an individual’s health or safety” or “a crime”.
In this additional post, I now share an additional example of whistleblowing about medical records tampering which was recognised by an NHS England commissioned investigation to be a breach of legal obligations.
The whistleblowing took place at Avon and Wiltshire Mental Health Partnership NHS Trust (AWP) in 2012 and was reported by Community Care and by the BBC:
In February 2012, a group of social workers reported to the Wiltshire Council that they believed that false entries had been made to electronic patient records (RiO) at AWP.
It was alleged that “a number of social workers employed by Wiltshire Council but working in Avon and Wiltshire Mental Health Partnership Trust (AWP) that they had been instructed to falsify or alter service user records and/or that records had been amended by NHS staff without the knowledge of council employed staff.”
The Council investigated and found that nearly thirty social workers based in either the adult community, liaison or later life services of AWP shared these concerns.
The South of England Strategic Health Authority ie. NHS England, commissioned an investigation into the irregularities on the 28 May 2012, under DH guidance (2005) concerning the conduct of independent inquiries into mental health services, replacing paragraphs 33- 36 in HSG(94) 27 (LASSL (94)4).
The investigation terms of reference included a review of any breach of legislative requirements, and impact on safety, care, treatment, welfare, safeguarding, and risk assessment and management of patients.
The investigation team reported that they found a top down senior management culture focussed on meeting financial targets, which in turn middle managers translated into falsification of patient records to meet targets and avoid financial penalties:
“4.2.3 Both NHS and social care staff described working in a bullying and intimidating environment with a relentless focus on achieving targets, avoiding breaches and ‘staying green’ (the scorecard) and threats of fixed penalties being applied to team budgets for breaching targets. We were shown an email from a care team administrator to a social worker that confirmed a £3000 fine would be applied to the team for breaching a referral to assessment target for a single patient. The email went onto confirm that despite the fact that the social worker had recorded multiple telephone contacts with the client, the administrator had added a face to face contact visit to the social workers RiO diary to avoid the breach.”
The investigation concluded that most of the records falsification did not result in direct patient harm but work done to input data and manage performance diverted away from face to face clinical care.
Records also did not always give an accurate clinical contact history.
This is potentially of relevance to clinical risk assessment.
The investigators considered that there was no intention to defraud commissioners, only to survive. But that might not be a persuasive defence in law.
Importantly, the investigators noted that the records falsification at AWP was likely in breach of legal obligations because under the Data Protection Act 1998:
1) False data breached the accuracy principle of data protection
2) Covertly processing fabricated data breached fair processing principles.
AWP had also not taken adequate systemic measures to safeguard against unauthorised and unlawful personal data processing.
“5.5 The organisation is unlikely to be processing information in accordance with the Data Protection Act. Three specific breaches should be considered. Firstly in relation to the recording of data about ‘carers’ without their express knowledge or agreement of the individual concerned which does not satisfy fair processing requirements. Secondly as patient records contain entries and information that is incorrect it is questionable whether the records meet the accuracy principle Thirdly AWP should consider whether it is in breach of the requirement to take appropriate technical and organisational measures against unauthorised or unlawful processing of personal data.”
This is a copy of the investigation report into the records falsification, as disclosed by AWP via the What Do They Know FOI website, to a member of the public who identified themselves as a harmed patient:
So in short, these are more arguments as to why a concern that is raised about tampering with medical records is likely to be a qualifying disclosure under UK whistleblowing law, the Public Interest Disclosure Act (PIDA).
Let us hope that NHS England will in the longer term recognise the importance of protecting disclosures about medical records tampering, and acknowledge (once more) that tampering breaches a number of legal obligations.
Let us also hope that NHS England remembers that its own investigation at Avon and Wiltshire upheld that whistleblowing disclosures about medical records tampering amounted to disclosures about breaches of legal obligations…….which are a category of “qualifying disclosures” under the Public Interest Disclosure Act.
Dr Minh Alexander retired consultant psychiatrist 22 April 2023
UK whistleblowing law is very weak.
It offers no protection.
No one is legally required to proactively protect a whistleblower.
Not employers, not regulators nor other public bodies.
The law only entitles whistleblowers to claim for post hoc compensation after serious harm. Even then the odds of success are very slim and the compensation usually inadequate.
A whistleblower can be blameless, determined to be so, and yet still dragged through several years’ ordeal of disciplinary procedures, dismissal, litigation and end up out of pocket after paying legal fees. I know of such a recent case.
Those representing themselves as litigants in person have even worse outcomes.
A great weakness of UK whistleblowing law is the threshold and number of legal tests that whistleblowers face, which were explicitly set high to appease industry and disadvantaged workers when the law was originally drafted.
For whistleblowers, the law is a fragile chain of flickering fairy lights. Knock out any one of those lights and the case is lost.
A UK whistleblower has to make the right sort of disclosure (qualifying disclosure) and they have to make the disclosure in the right way to the right person or body, in the right circumstances, to qualify for protection (“protected disclosure”).
Lawyers make hay out of endlessly arguing about the niceties, and establishing a professional hegemony from specialist knowledge of ever-evolving case law.
How on earth is a litigant in person supposed to cope in this minefield, from the first critical step of framing their claim? One error and the fairy lights go out.
Take the first hurdle for whistleblowers: what is a qualifying disclosure under the law?
(1) In this Part a “qualifying disclosure” means any disclosure of information which, in the reasonable belief of the worker making the disclosure, tends to show one or more of the following—
(a)that a criminal offence has been committed, is being committed or is likely to be committed,
(b)that a person has failed, is failing or is likely to fail to comply with any legal obligation to which he is subject,
(c)that a miscarriage of justice has occurred, is occurring or is likely to occur,
(d)that the health or safety of any individual has been, is being or is likely to be endangered,
(e)that the environment has been, is being or is likely to be damaged, or
(f)that information tending to show any matter falling within any one of the preceding paragraphs has been, is being or is likely to be deliberately concealed.
(2) For the purposes of subsection (1), it is immaterial whether the relevant failure occurred, occurs or would occur in the United Kingdom or elsewhere, and whether the law applying to it is that of the United Kingdom or of any other country or territory.
(3) A disclosure of information is not a qualifying disclosure if the person making the disclosure commits an offence by making it.
(4) A disclosure of information in respect of which a claim to legal professional privilege (or, in Scotland, to confidentiality as between client and professional legal adviser) could be maintained in legal proceedings is not a qualifying disclosure if it is made by a person to whom the information had been disclosed in the course of obtaining legal advice.
(5) In this Part “the relevant failure”, in relation to a qualifying disclosure, means the matter falling within paragraphs (a) to (f) of subsection (1).”
Case law has evolved such that there are several strands about which whistleblowers are usually grilled by Tribunals and employers’ barristers.
Disclosure of information
The disclosure should contain information of “sufficient factual content and specificity”.
Nature of the worker’s belief
The worker should have a reasonable belief that the information tends to show one of the “relevant failures” and “is made in the public interest”;
Employers’ barristers try to attack via any and all of these angles.
For example, questioning of claimants about whether they made their disclosures with the public interest in mind.
Barristers may posit that this is as narrow as making a disclosure with the employer’s whistleblowing policy in mind, when the law does not even require employers to have a whistleblowing policy.
Another legal tactic is to ask claimants if they ticked a box on the ET application form to consent to their claim being shared with a regulator, on the premise that this demonstrates a public spirit. This question is naturally asked of claimants who do not tick the box.
Employers’ barristers may also question whether claimants’ disclosures fit the defined categories (a) to (f) under Section 43B of PIDA.
Imagine the shock that a lay person, especially those of limited resources and/or who are unrepresented, may experience after raising what most reasonable people would think is a public interest disclosure, only to discover that lawyers have a very particular meaning.
In the NHS, this is compounded by permissively written policies and procedures which on the face of it invite maximum disclosure because the NHS is a safety critical sector.
The national template whistleblowing policy for the NHS:
set by NHS Improvement (now absorbed into NHS England) is applied by many NHS bodies. It states:
“You can raise a concern about risk, malpractice or wrongdoing you think is harming the service we deliver/commission [delete as appropriate]. Just a few examples of this might include (but are by no means restricted to):
· unsafe patient care
· unsafe working conditions
· inadequate induction or training for staff
· lack of, or poor, response to a reported patient safety incident
· suspicions of fraud (which can also be reported to our local counter-fraud team [insert contact details])
· a bullying culture (across a team or organisation rather than individual instances of bullying).”
Crucially, the NHS national whistleblowing policy urges staff to err on the side of caution and to raise concerns even if they are not sure if the concern is proven:
“Remember that if you are a healthcare professional you may have a professional duty to report a concern. If in doubt, please raise it. Don’t wait for proof. We would like you to raise the matter while it is still a concern. It doesn’t matter if you turn out to be mistaken as long as you are genuinely troubled.”
The NHSI 2016 national policy was replaced in 2022 with the NHS England version:
This did not even specify what sort of concerns NHS workers could or should raise. Instead, this replacement policy states in bold letters:
“This policy is for all workers and we want to hear all our workers’ concerns”
All concerns? Remarkable.
But at the very end of the 2022 policy there is an appendix B which states:
“Making a ‘protected disclosure’
A protected disclosure is defined in the Public Interest Disclosure Act 1998. This legislation allows certain categories of worker to lodge a claim for compensation with an employment tribunal if they suffer as a result of speaking up. The legislation is complex and to qualify for protection under it, very specific criteria must be met in relation to who is speaking up, about what and to whom. To help you consider whether you might meet these criteria, please seek independent advice from Protect or a legal representative.”
Why is this caveat in the small print, especially after urging the workforce to spill all?
“Whistleblowing does not apply to personal grievances, including employment issues, which should be dealt with through internal organisational policies. It would generally be applied to:
• Concerns about unsafe patient care;
• Poor clinical practice or other malpractice which may harm patients;
• Failure to safeguard patients;
• Maladministration of medications;
• Untrained staff;
• Unsafe working conditions
• Lack of policies;
• A bullying culture;
• Staff who are unwell or stressed and not seeking help.
These types of concerns are sometimes referred to as ‘Protected Disclosures’ under the Public Interest Disclosure Act 1998.”
This would seem a reasonable list to most health service workers, who can appreciate that these are all matters which could affect the health and safety of patients.
But in the parallel world of litigation, it is far from straightforward, as I will discuss below.
NHS England’s contention that raising a concern about tampering with medical records is not whistleblowing
An ongoing employment tribunal against NHS England (or more specifically, the Healthcare Investigation Branch which is located within NHS England but overseen by NHS England and subject to its HR and governance systems), which I am currently observing, demonstrates how bewildering litigation can be for whistleblowers.
An experienced worker made a disclosure about unauthorised alterations of medical records.
To all healthcare professionals, this is an issue that sets off huge alarm bells on probity, patient safety, culture, safeguarding and a good many other matters.
But NHS England’s barrister questioned whether the matter amounted to a qualifying disclosure under whistleblowing law.
I struggle to see how a concern about tampering with medical records is not a health and safety issue.
Tampering with records may be done to cover up a care failure, which would fall under both the health and safety and concealment provisions of Section 43B PIDA.
It prevents learning from serious incidents, may allow unsafe practitioners to continue harming patients and impacts on trust in healthcare workers, which is an important part of safe care at a public health level.
Tampering with health records impacts on patients’ rights to seek legal redress for care failures and it can potentially obstruct regulatory activities and statutory Health and Safety provisions.
“Risks can relate to a wrongdoing, patient safety or malpractice which the organisation oversees or is responsible or accountable for. In a health setting, these concerns could include, for example:
patient-safety issues
patient-care issues
poor practice
unsafe working conditions
fraud (theft, corruption, bribery or embezzlement)
changing or falsifying information about performance
breaking any legal obligation
abusing authority
deliberately trying to cover up any of the above.”
“maintain securely an accurate, complete and contemporaneous record in respect of each service user, including a record of the care and treatment provided to the service user and of decisions taken in relation to the care and treatment provided;”
That is, maintaining the integrity of contemporaneous care records is a statutory, legal obligation.
Post hoc tampering with health records is likely to represent a failure of this legal obligation, and thus would bring a disclosure about such wrongdoing under the category of a legally “qualifying disclosure”.
For completeness, this is CQC’s guidance to the staff of provider bodies who wish to whistleblow to the CQC. It advises health and care workers that whistleblowing can encompass a wide range of issues: “The concerns don’t have to be restricted to people using the service. Whistleblowing can cover any risk, malpractice or wrongdoing that affects patients, the public, other staff or the provider itself.”
Regardless of whether NHS England prevails in its above legal argument at the ET, it will need to explain to the NHS workforce, patient groups, fellow regulators and parliament, why the most powerful NHS body does not accept that raising a concern about tampering with medical records is whistleblowing.
NB If there are any lawyers reading this blog who think I have got anything wrong or left anything out in this important matter, please do let me know. Best wishes.
Related miscellaneous
NHS England itself has not responded to me yet about its practice of its General Counsel routinely attending operational meetings about the management of internal whistleblowing at NHS England, and whether the affected NHS England whistleblowers will be allowed as a matter of policy to access meeting minutes as personal data. This was first raised in June 2022.
On a similar theme, NHS England through its representatives was supposed to give me electronic access to the case bundle from the above ET, as an observer. I understand that NHSE informed the Tribunal that it did so yesterday morning. However, I received no correspondence from NHSE with the necessary link to give me access, and will take the matter up again with the Tribunal next Monday when the hearing resumes.
It was noteworthy that NHS England’s barrister elected not to question several of the claimant’s senior witnesses, even with a caveat by the barrister that this did not mean that NHSE agreed with their evidence or accepted it.
This further post shares a 2012 investigation report commissioned by South England Strategic Health Authority (the nascent NHS England in other words, which became fully operational on 1 April 2013), on records falsification by a mental health trust, Avon and Wiltshire Partnership (AWP). This investigation concluded that AWP had likely been in breach of legal obligations as a result of falsifying medical records to avoid financial penalties for not meeting performance targets. It follows from this finding that the whistleblowers who made disclosures about the records falsification had by implication raised qualifying disclosures under the Public Interest Disclosures Act.
RELATED ITEMS
We have seen examples of NHS regulators not only failing whistleblowers who approach them as Prescribed Persons under PIDA, but their own regulatory staff who whistleblow.
There has been the case of Mr Shyam Kumar at the Care Quality Commission, where the CQC behaved in the most extraordinary manner. It defamed him, unfairly dismissed him, abused its power as a regulator to (unsuccessfully) seek adverse information about him that could be used in ET proceedings and then maintained a narrative throughout the ET hearing that he was a bully, which was rejected by the ET.
We have also seen a case of race harassment by senior NHS England managers as well as whistleblowing detriment in the case of Ms Cox.
The Tribunal judgment noted that NHS England’s submission in this case focussed on uncoupling detriment from protected acts:
“the respondent’s case focusses on causation and whether the treatment complained of arose from the protected acts or protected disclosures”
This illustrates that where employers think they have lost the battle on disproving protected disclosures, they move on to the next fairy light, which is to disprove a causal link between protected disclosures and detriment.
It is a shabby trick to play on the NHS workforce, to invite whistleblowing disclosures through fine words, and then waste public money on tripping staff up and blocking them with a massive, well-oiled legal machinery and expensive barristers.
What is more, current UK whistleblowing law enables this state of affairs.