
By Dr Minh Alexander retired consultant psychiatrist 24 February 2026
Valdo Calocane was discharged after missing appointments
The statutory inquiry hearings into the attacks by Valdo Calocane, psychiatric patient, against the public in Nottingham opened on Monday 23 February 2026.
Counsel to the Inquiry set out the areas of concern.
Agonisingly, Valdo Calocane’s loss to follow up was recounted. He was discharged from specialist mental health services in September 2022 after missing appointments and after an outreach visit was mooted but did not take place. Compounding this, there was reportedly minimal information and guidance given to primary care upon discharge. There was no further contact with health services until the attacks in June 2023.
This situation of discharge because of disengagement from mental health services is more common than it should be.
Disengagement is a precursor to suicide and homicide, but trusts vary in their approach to discharge
Patients with severe mental illness (SMI) have been poorly served in that high intensity, specialist services that are proven necessary for flexible and proactive support, were scrapped or watered down.
Generic teams cannot offer the same level of care and may struggle with patients whom they experience as “challenging”, because they are not equipped to deal with their complex needs.
In particular, when generic teams are over-burdened, de-sensitised and/or poorly managed and supervised, patients may bear the brunt in terms of therapeutic rejection, premature discharges and failures to outreach or to appropriately mitigate risk.
And thus patients may be abandoned when they are chaotic due to relapse, and are at their most vulnerable, and when some also pose greater risk to others.
Disengagement by severely mentally ill patients should trigger concern, investigation and outreach, not discharge. The National Confidential Inquiry advises:
“Non-receipt of planned care is a crucial precursor of patient suicide. Services should place priority on follow-up efforts for patients losing contact with services or who are non-adherent with medication. These patients have multiple clinical and social problems that are likely to add to risk and that need to be addressed in their care plan. Involvement of the patient’s family or carers should form part of engagement efforts.” Annual report 2025
Disengagement is similarly a precursor to homicides:
“65 (32%) patients with schizophrenia were non-adherent with drug treatment in the month before the homicide, an average of 6 per year. There had been no fall since 2008. 75 (39%) patients with schizophrenia missed their final service contact before the homicide, an average of 7 per year, and again there had been no fall since 2008. In total 116 (59%) were either non-adherent or missed their final contact with services. There was a fall overall in this group over the report period.” Annual report 2017
A glance at NHS mental health trust discharge policies in the public domain shows a range of approaches. Most contain an element of risk management when dealing with non-attendance/ disengagement. But there are differences in tone and emphasis on caution and urgency of response to a possibly deteriorating patient.
The independent homicide investigation commissioned by NHS England into Valdo Calocane’s case concluded that Nottingamshire Healthcare’s discharge processes were not sufficiently robust and that staff in any case failed to involve his family as required by trust policy.
Some trusts’ discharge/ non-attendance policies are overly complex and sometimes downright confusing. For example, one policy contains a rigid “two strikes and out” clause whilst also featuring a plethora of caveats scattered in different places in the policy:
At the end of the day, policies and flow charts cannot compensate for insufficient clinical training and experience, in the context of cost-cutting and downskilled services.
But how do policies translate into action?
DATA
A member of the public, a Ms Card, very helpfully submitted an FOI request to NHS mental health trusts in the summer of 2024 about discharges via the What Do They Know Website.
This revealed patterns of discharge due to non-attendance and non-engagement by patients. The data is incomplete for various reasons, including the fact that some trusts claimed that they did not routinely collect this data.
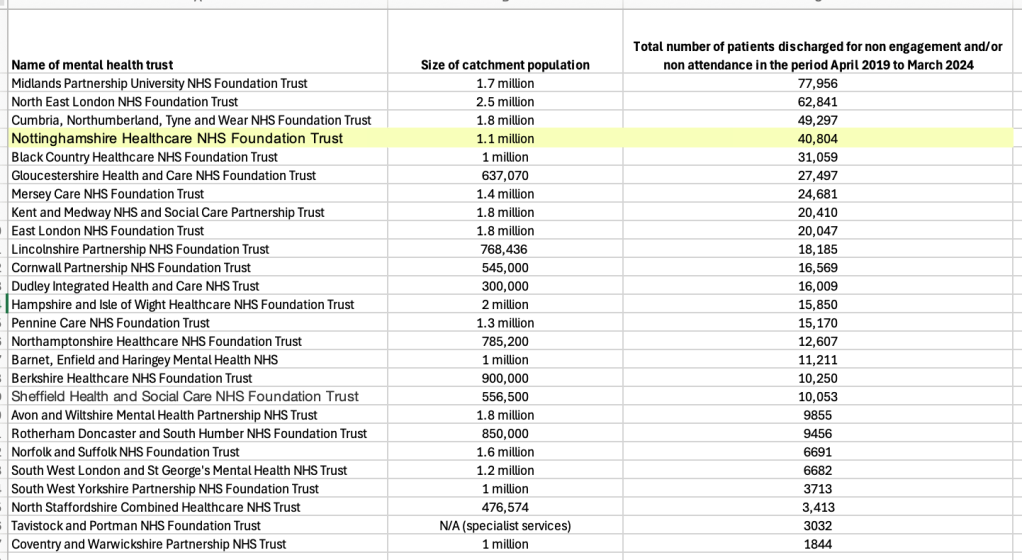
But of 26 mental health trusts that provided data for the five year period 2019-2024, there was quite a range in the number of patients discharged for non-attendance/non-engagement. The trusts vary in their range of services and comparison is rough.
According to this FOI data, Nottinghamshire Healthcare NHS Foundation Trust was at the higher end of the spectrum.
In total, the 26 trusts discharged 525,182 patients over the five year period for not attending/ not engaging.
And one trust pointed out that some patients may be discharged more than once in any given period, so the number of episodes of discharge may be slightly higher than the total number of patients discharged.
For completeness, I have loaded the more detailed results by year onto a spreadsheet. This also gives a list of the trusts which claimed not to collect data on discharges for disengagement.
Questions arise about the appropriateness of the many thousands of discharges for disengagement, and how well risk is managed and needs are met during such discharges.
Realistically, how often are such discharges clinically audited for safety, in our super-stressed NHS?
And what might the disengagement data say about the suitability of services provided?
All NHS mental health services operate under great pressure, including severe bed pressure after savage bed cuts. There is always potential for something to go badly wrong, and it is important to acknowledge that Nottinghamshire Healthcare NHSFT is not an isolated example.
One only has to glance at the immaculately maintained database of mental health homicides by the charity HundredFamilies to see that risk remains widespread and ongoing.
The issue is what will be done, if anything, to change this.
RELATED ITEMS
1) This is the independent homicide report commissioned from Theemis Consulting Ltd by NHS England into the attacks by Valdo Calocane:
Independent investigation into the care and treatment provided to VC January 2025
This concluded that discharge due to disengagement had become “normalised”:
“Based on interviews with Trust staff and from the evidence reviewed by the independent investigation, VC’s discharge due to disengagement does not appear to have been an isolated event. Pressures on the service and a lack of oversight to understand whether the service was being delivered as intended, or whether ‘as intended’ is possible within the constraints of resources, meant that this practice had become normalised and accepted within the team.”
Theemis made this important finding about the provision of Assertive Outreach Services in NHS mental health trusts:
“Finding
NHS England’s recent review and guidance indicates that assertive outreach should be a discrete resource but recognises while some ICBs may already commission ‘assertive outreach’ teams or similar, others may not currently commission a specific team or service focused on intensive and assertive approaches. This aligns with the information and evidence provided to the independent investigation that suggested the majority of dedicated assertive outreach teams as a standalone function, were disbanded over 10 years ago. Alternative models for supporting service users who do not choose to or are unable to engage with mental health services have developed but there is variation in the approach, dedicated protected resources and in outcomes for patients. VC’s clinical records and interviews with community Trust staff do, to an extent, demonstrate an element of an assertive approach. However, this was constrained by the service model and workload within the team.”
2) After the Nottingham attacks, NHS England back tracked on the dangerous dismantling of specialist assertive outreach services and directed ICBs to review their provision. The reviews have been submitted to NHSE. What happens next is the question.
3) The livestream of the Nottingham Inquiry can be found here.
This is a schedule of upcoming hearings with details of which sessions will be livestreamed:
4) This is the 1994 report of the inquiry into the mental health homicide by Christopher Clunis, who killed Jonathan Zito in 1992
The report of the Inquiry into the Care and Treatment of Christopher Clunis
The failings that it described have been repeated over the years.
The Inquiry observed that care was inversely proportional to deterioration in Christopher Clunis’ mental state, and that this was a pattern that the panel had noted over the years:

The question is how much longer society tolerates these failures, and prioritises the changes that are needed to protect the public, and also to protect patients from catastrophic deterioration that changes their lives and prognosis indelibly.
My condolences to all the affected families and surviving victims.
UPDATE 25 FEBRUARY 2026
This is a powerful opening submission to the Nottingham Inquiry by the Doughty Street Chambers team on behalf of the bereaved families.
They submit:
“This Inquiry is not only about Barney, Grace and Ian, but it is also about Jonathan Zito (who died at the hands of the Christopher Clunis; about which killing, Jean Ritchie concluded her report in 1994)’ and each of the countless other unnecessarily bereaved, whose loved ones were lost to the unmanaged risk of people who were known to be ill and known to be a risk to public safety.”
This is a moving opening submission on behalf of Valdo Calocane’s family, his mother and brother, which explains their distress at many missed opportunities to care for him and to prevent the attacks.
The Department of Health made its opening submission at the Nottingham Inquiry yesterday and its written submission has been published here.
The Department acknowledged there was a failure to manage disengagement, emphasised the need for continuity of care at several points and touched somewhat ambiguously on the issue of resources, citing a need for resources but also claiming that it has made investments.
“43.Valdo Calocane was discharged from services and at times it appeared that he may have been non-compliant with medication and was reluctant to engage with mental health services, such as in September 2022 (WITNO084001). The Department recognises that non-engagement is a recurring problem. Those with severe mental illness often live with these illnesses for their whole lives, and the support of the health services needs to reflect this in the services provided and in being able to go back into the system efficiently and quickly should deterioration occur. As a result of the lack of information sharing and the absence of access to information, professionals did not monitor Valdo Calocane’s mental health deterioration over time. This led to, for example, a failure to actively manage Valdo Calocane in transfer between the community mental health team and his GP (WITN0084001). There should have been resources to carry out this exercise. Failing to engage with services, not turning up to appointments, not answering messages, are not often in this group of patients a sign of health or a conscious decision, but a sign of mental ill health and a lack of insight into how unwell they are. Help is needed for this group even if it is difficult to deliver and requires persistence, patience, and perseverance.”

